






Languages
Pages
Legal

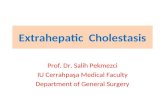
DISEASES OF THE GALL BLADDER AND EXTRAHEPATIC BILE DUCTS
Prof Orla Sheils Oct 29th 2009
GALL STONES (CHOLELITHIASIS)
Disorders of the biliary tract affect a significant portion of the worldwide population Majority of cases are attributable to cholelithiasis
(gallstones). United States, 20% of persons older than 65 years
have gallstones 1 million newly diagnosed cases of gallstones are
reported each year. 10% of the “Western” population. 20% of autopsies.
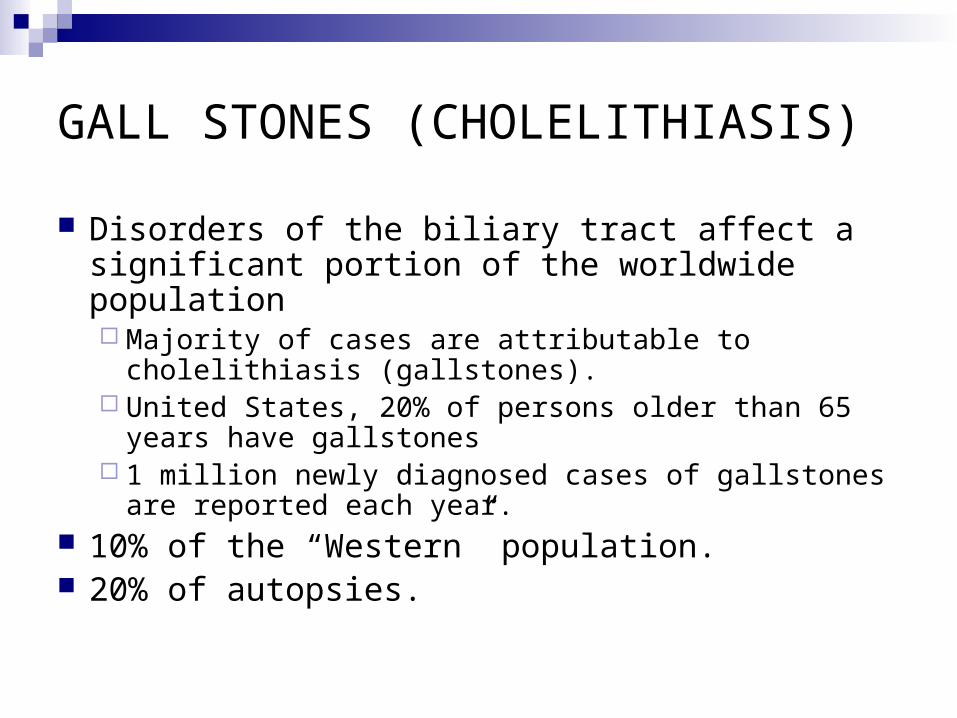
Bile exocrine secretion of the liver produced
continuously by hepatocytes. contains cholesterol and waste products,
bilirubin and bile salts, which aid in the digestion of fats.
Half the bile produced runs directly from the liver into the duodenum via a system of ducts, ultimately draining into the common bile duct (CBD).
The remaining 50% is stored in the gallbladder. In response to a meal, this bile is released from the gallbladder via the cystic duct, which joins the hepatic ducts from the liver to form the CBD.
The CBD courses through the head of the pancreas for approximately 2 cm before passing through the ampulla of Vater into the duodenum.
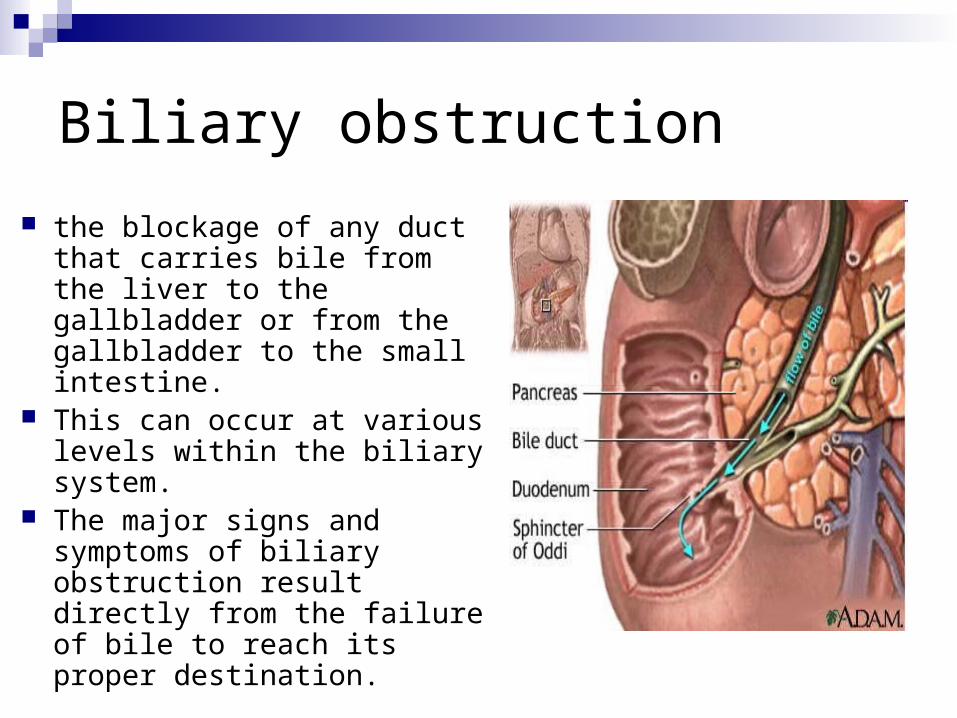
Biliary obstruction
the blockage of any duct that carries bile from the liver to the gallbladder or from the gallbladder to the small intestine.
This can occur at various levels within the biliary system.
The major signs and symptoms of biliary obstruction result directly from the failure of bile to reach its proper destination.
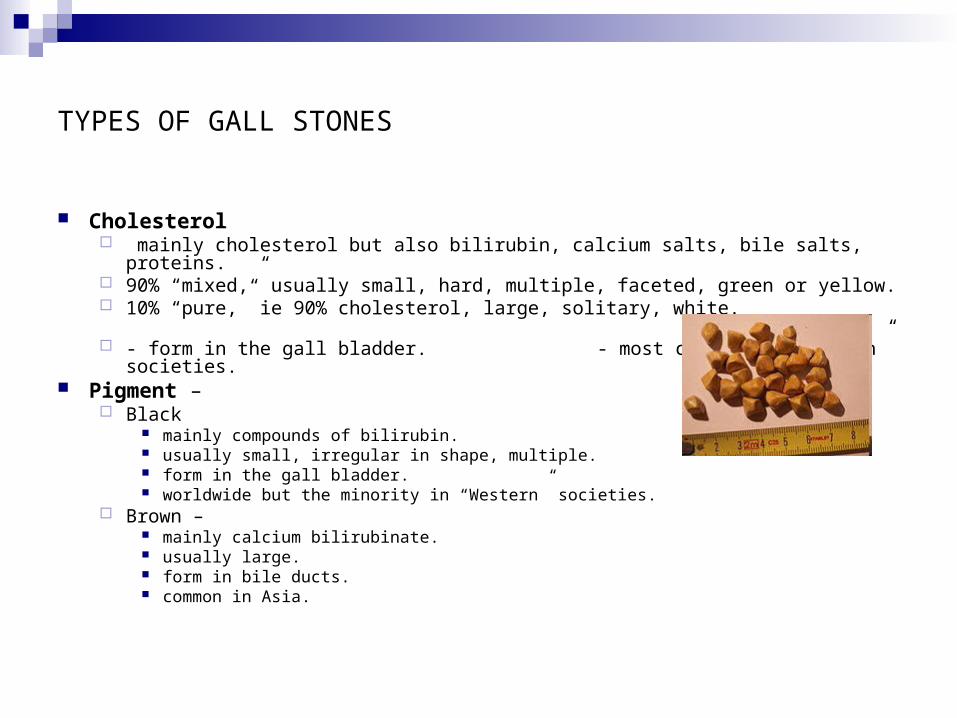
TYPES OF GALL STONES
Cholesterol mainly cholesterol but also bilirubin, calcium salts, bile salts, proteins. 90% “mixed,” usually small, hard, multiple, faceted, green or yellow. 10% “pure,” ie 90% cholesterol, large, solitary, white. - form in the gall bladder. -
most common in “Western” societies. Pigment –
Black mainly compounds of bilirubin. usually small, irregular in shape, multiple. form in the gall bladder. worldwide but the minority in “Western” societies.
Brown – mainly calcium bilirubinate. usually large. form in bile ducts. common in Asia.
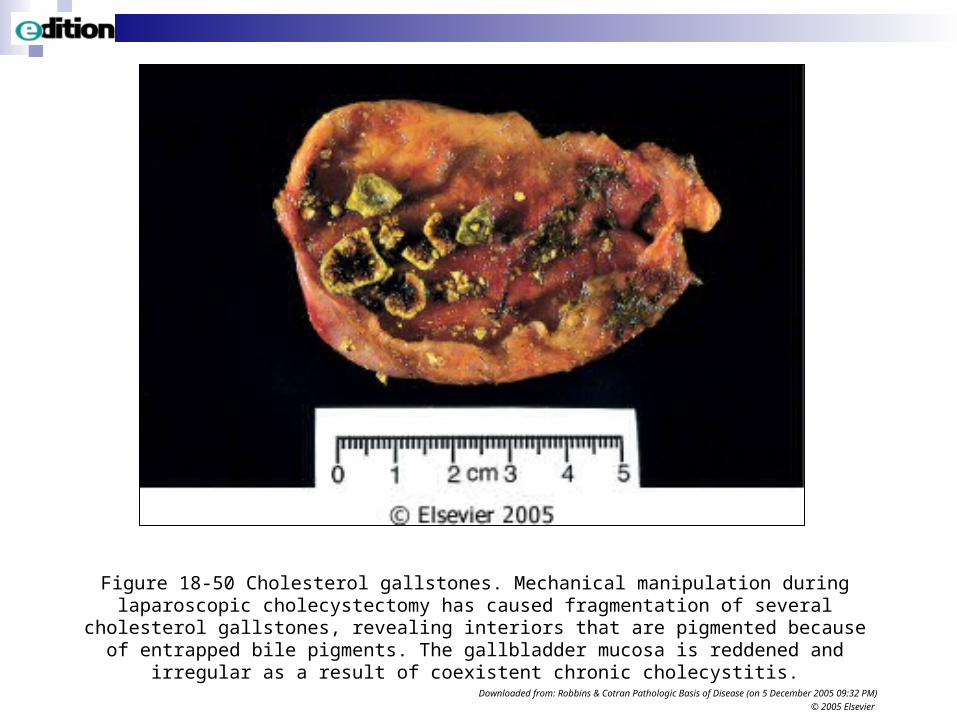
Figure 18-50 Cholesterol gallstones. Mechanical manipulation during laparoscopic cholecystectomy has caused fragmentation of several cholesterol gallstones, revealing interiors that are pigmented because of entrapped bile pigments. The gallbladder mucosa is reddened
and irregular as a result of coexistent chronic cholecystitis.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier
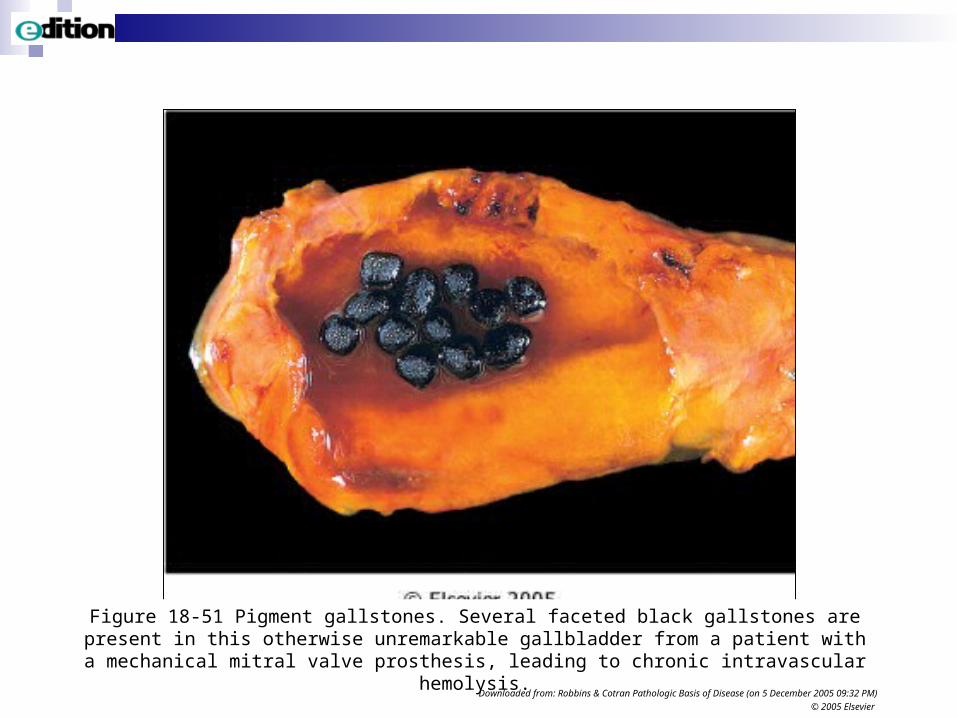
Figure 18-51 Pigment gallstones. Several faceted black gallstones are present in this otherwise unremarkable gallbladder from a patient with a mechanical mitral valve prosthesis, leading to
chronic intravascular hemolysis.Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier

AETIOLOGY AND PATHOGENESIS
Cholesterol gall stones.
Supersaturation with cholesterol (lithogenic bile). Due to increase in cholesterol, decrease in bile acids or both.
Nucleation - defect in balance between pronucleation factors (eg mucus glycoproteins) and antinucleation factors (eg apolipoproteins. Biliary sludge.
Gall bladder hypomotility. Mucus hypersecretion enables
crystals to aggregate into stones.
Risk Factors:
age sex (F:M as 2:1),
number of pregnancies,
obesity,
rapid weight loss, starvation,
hyperlipidemia,
small bowel disease/resection
lipid-lowering drugs,
inherited disorders of bile acids,
ethnic differences.
Aetiology & pathogenesis
Pigment gall stones.Black - supersaturation with unconjugated bilirubin - calcium
bilirubinate. - associated with haemolytic anaemia, cirrhosis, malaria. - bile sterile.Brown - supersaturation with unconjugated bilirubin due to
degradation of conjugated bilirubin by bacterial enzymes (beta-glucuronidase).
- bile infected and stones contain bacteria. Bile infection usually secondary to stasis in bile ducts.
- common in Asia where polymicrobial cholangitis is frequent and biliary obstruction due to flukes (eg Clonorchis, Opisthorchis) are a risk factor.
CLINICAL FEATURES AND COMPLICATIONS 90% are “silent.” 10% produce symptoms - epigastric or RUQ pain.
Complications in the gall bladder:- Acute cholecystitis
due to stone blocking the outlet; may lead to empyema, gangrene, perforation, peritonitis.
Chronic cholecystitis. Mucocoele. Biliary fistula to duodenum and gall stone ileus. Carcinoma.
CLINICAL FEATURES AND COMPLICATIONS Complications in the bile duct:- a stone exiting
the GB, passes down the bile ducts (choledocholithiasis) and may cause – Biliary colic. Extra-hepatic biliary obstruction, jaundice, ascending
cholangitis. Pancreatitis. Fibrous stricture. Obstructive jaundice with dilated bile ducts on
imaging.
ACUTE CHOLECYSTITIS 90% associated with gall stones, F>M. 10% acalculous, M>F.
Calculous cholecystitis. Clinical:-
Pain RUQ, referred to shoulder or interscapular. Anorexia, nausea, vomiting. Fever, tenderness RUQ. Neutrophil polymorphonuclear leukocytosis.
Pathology:- swollen, tense, possible exudate surface. Microscopically necrosis +/- haemorrhage; later a neutrophil polymorphonuclear infiltrate. Bacterial cultures eventually positive.
Complications:- empyema, gangrene, perforation with walled off abscess or generalised
peritonitis.
Acute cholecystitis
Acalculous cholecystitis. Following:-
Severe burns. Severe trauma. Major surgery. Prolonged labour. Ischaemia in PAN, SLE, embolism. Salmonella typhi & other organisms –
gas-forming organisms giving rise to bubbles in the wall - “emphysematous” gall bladder.
Insidious clinical features.
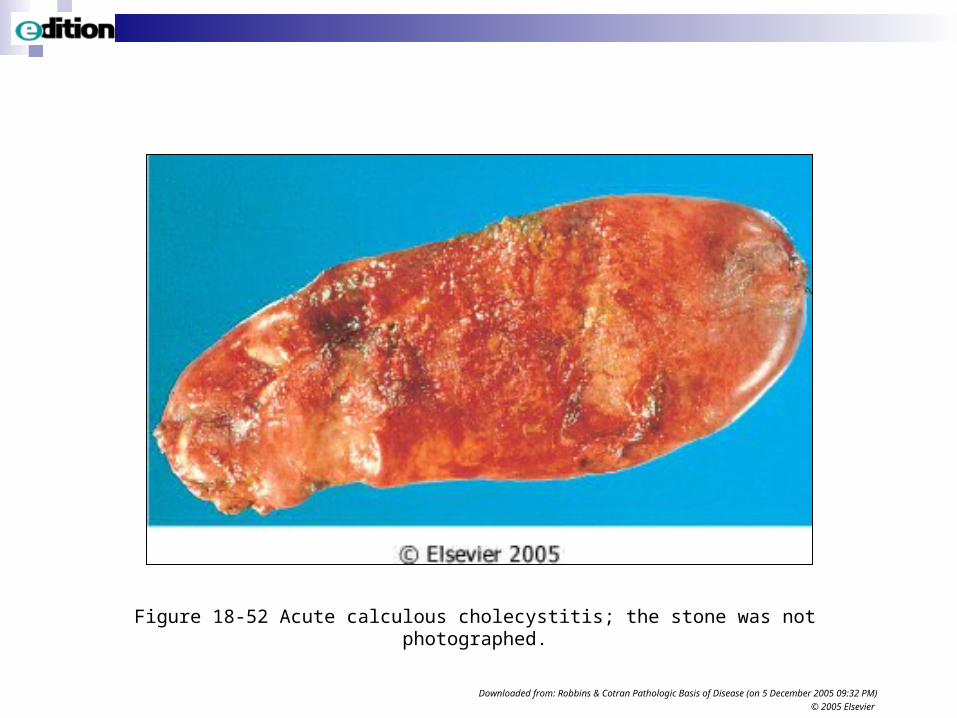
Figure 18-52 Acute calculous cholecystitis; the stone was not photographed.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier
CHRONIC CHOLECYSTITIS
Much more common than acute form. F>M. Gall stones in 95%. May be a chemical damage due to supersaturated bile. Bacteria seldom
present. Obstruction to the outlet not required. Clinical features: epigastric or RUQ pain; often at night or after a heavy
meal. Intolerance to fatty foods. Pathology: thickened firm wall; almost always gallstones in the lumen. Microscopically chronic inflammation and fibrosis.
Rokitansky-Aschoff sinuses are outpouchings of mucosal epithelium through the wall and are characteristic. Thought to be due to intra-luminal pressure effect. The wall may become calcified when it is known as a “porcelain” gall bladder and can be seen on X-ray.
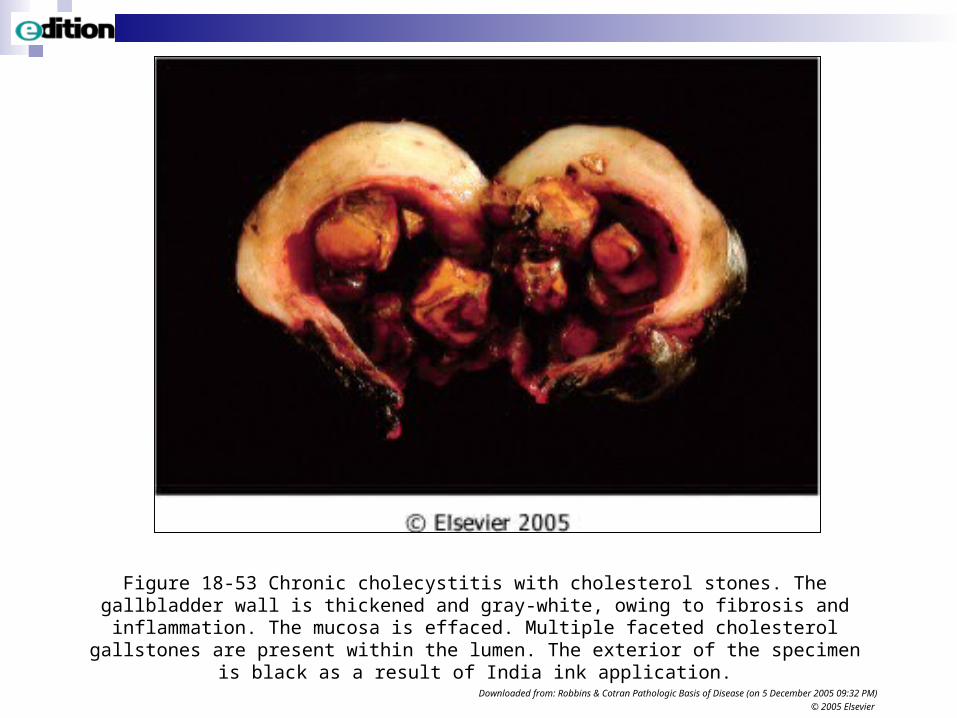
Figure 18-53 Chronic cholecystitis with cholesterol stones. The gallbladder wall is thickened and gray-white, owing to fibrosis and inflammation. The mucosa is effaced. Multiple faceted
cholesterol gallstones are present within the lumen. The exterior of the specimen is black as a result of India ink application.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier
BENIGN STRICTURES OF BILE DUCTS
Causes. Injury -
Surgery. Non-surgical trauma.
Post-inflammatory - Passage of a gall stone -> ulcer/fibrosis. Healed pyogenic cholangitis. Spread from adjacent inflammation eg DU.
Radiation. Primary sclerosing cholangitis.
Results Obstructive jaundice. Secondary biliary cirrhosis.
NEOPLASMS
Benign - very rare. Malignant - 3% of malignancies. 5th commonest in GIT.
GB to BD as 3:1. Carcinoma. GB - F>M. BD M>F. Peak age 7th decade. Aetiology unknown. Associations - GB - gall stones in 90%. BD 32%. But only 0.5% of
patients with gall stones develop carcinoma.BD - parasites (Clonorchis,Opisthorchis). - primary sclerosing cholangitis. - choledochal cyst.
Pathology - GB - diffuse or polypoid. An adenocarcinoma. Spread to regional lymph nodes, peritoneum, liver.
BD - slow growing desmoplastic adenocarcinoma. Spread to contiguous organs, lymph nodes, liver.
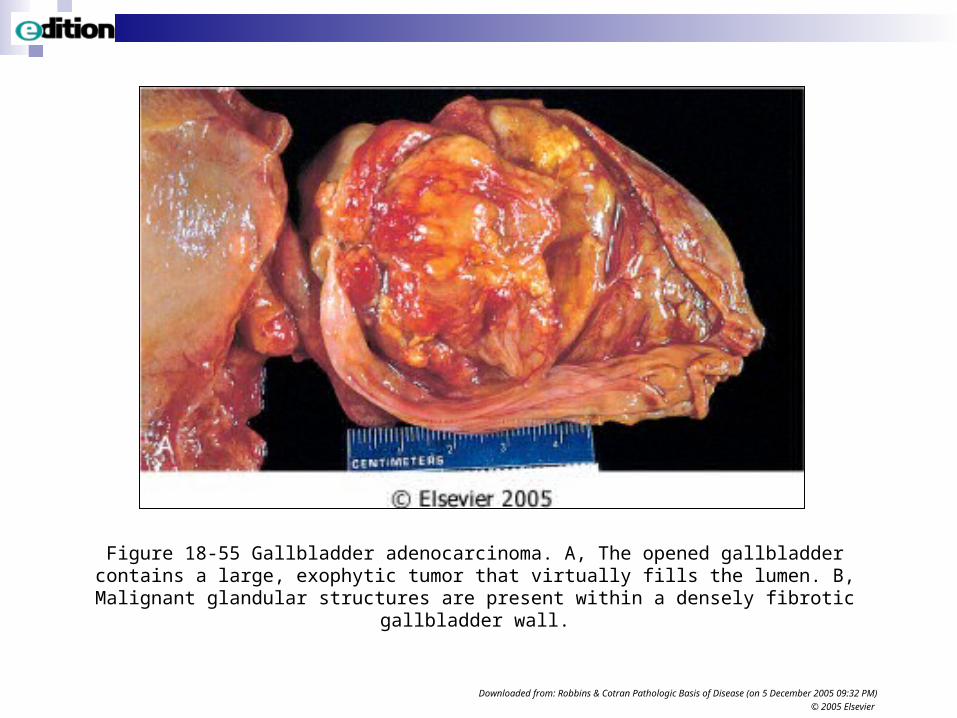
Figure 18-55 Gallbladder adenocarcinoma. A, The opened gallbladder contains a large, exophytic tumor that virtually fills the lumen. B, Malignant glandular structures are present within
a densely fibrotic gallbladder wall.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier
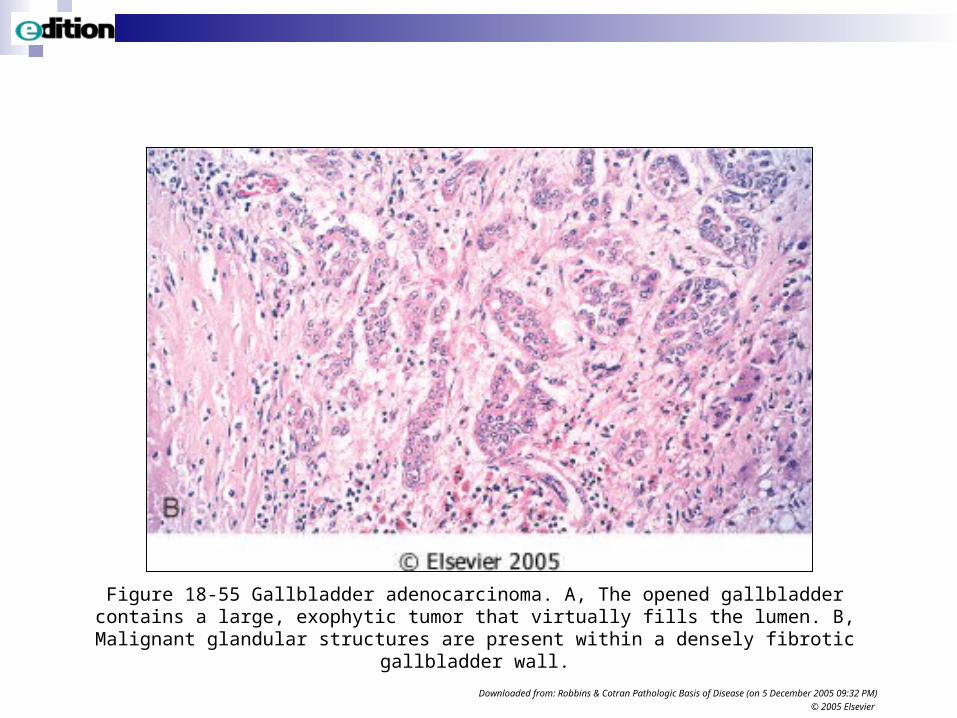
Figure 18-55 Gallbladder adenocarcinoma. A, The opened gallbladder contains a large, exophytic tumor that virtually fills the lumen. B, Malignant glandular structures are present within
a densely fibrotic gallbladder wall.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier
Neoplasms
Clinical features and prognosis - GB. A “silent area” so no symptoms until advanced. When symptomatic,
gives rise to upper abdominal pain, anorexia, weight loss. Jaundice a late feature. 5 year survival 1%.
BD. Give rise to obstructive jaundice earlier.Most die < 1 year from diagnosis. 75% have already spread to
contiguous organs or metastasised by the time of diagnosis.
Sites. Clinical and pathological findings differ in carcinomas arising at the ampulla of Vater, common bile duct, hepatic duct, or confluence of hepatic ducts at the hilum (Klatskin tumour).
Peri-ampullary carcinomas could be from the ampulla, lower CBD (both have better prognosis), duodenum, head of pancreas.
MISCELLANEOUS
Cholesterolosis.
Yellow deposits of lipid-containing macrophages in the mucosa of the gall bladder giving rise to yellow flecks grossly (“strawberry gall bladder”). Seen in 12% of autopsies and 25% of cholecystectomies. Of no clinical significance.
Congenital abnormalities.
Numerous anatomical variants. Important surgically.Extra-hepatic biliary atresia.Choledochal cyst.
DISEASES OF THE EXOCRINE PANCREAS
ACUTE PANCREATITIS
Acute onset of abdominal pain. Increased levels of pancreatic enzymes, notably amylase, in blood.
Morphology. Mild form:- interstitial oedema; no necrosis of the pancreas. - peri-pancreatic fat necrosis.
Morphology. Severe form:- extensive necrosis in and around the pancreas with haemorrhage. Extensive fat necrosis. Peritoneal accumulation of turbid brown fluid.
Incidence 10-20/100.000. 1% of hospital admissions.
Age range 30-70yrs. Mean+/- 55yrs. M=F but depends on aetiology.
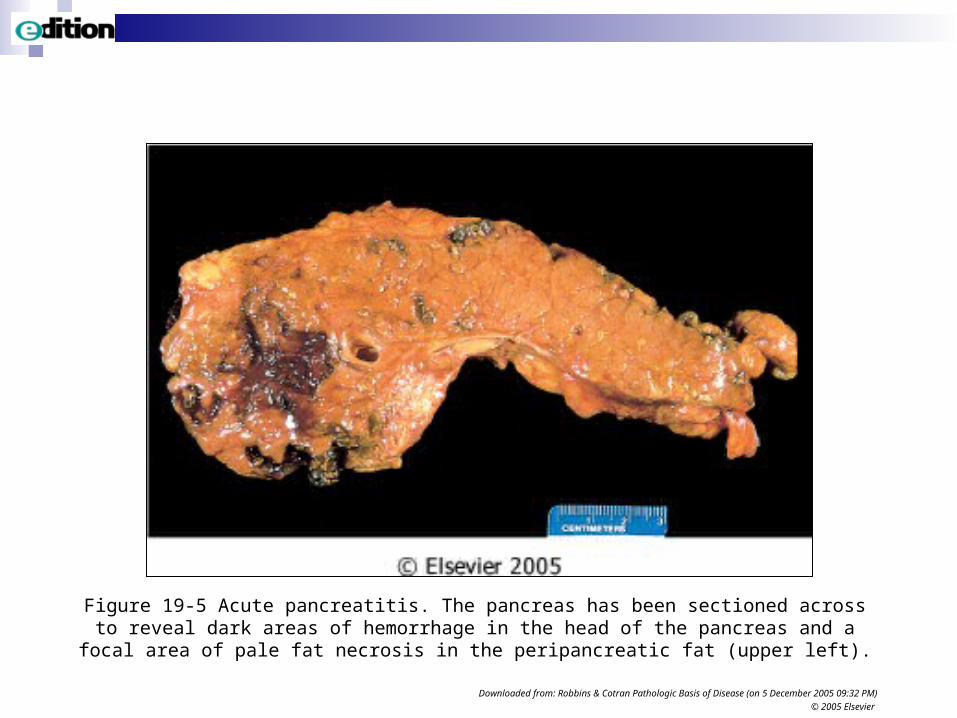
Figure 19-5 Acute pancreatitis. The pancreas has been sectioned across to reveal dark areas of hemorrhage in the head of the pancreas and a focal area of pale fat necrosis in the
peripancreatic fat (upper left).
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier
Aetiology
Gall stones most commonly in females. F:M=2:1. Alcohol most commonly in males. M:F=6:1.
Note: these 2 factors are responsible for 80% of cases. Less common mechanical causes are trauma, surgery, ERCP. Less common metabolic disorders include hyperlipoproteinemia,
hypercalcemia, drugs (eg thiazides), genetic factors. Vascular factors include shock, hypothermia, embolism, vasculitis. Infectious causes include Mumps, Coxsackievirus, Mycoplasma. Idiopathic - some hereditary forms are possibly due to mutations in germ
line genes coding for: cationic trypsinogen and pancreatic secretory trypsin inhibitor.
Pathogenesis
Acute pancreatitis is an autodigestion of the organ due to inappropriately activated pancreatic enzymes. Trypsinogen -> Trypsin causes proteolysis and activates other enzymes. Lipases cause fat necrosis. Elastase causes haemorrhage.
Kallikrein results in inflammation and thrombosis.
Mechanisms leading to activation of enzymes:-
1. Pancreatic duct obstruction eg by gallstone, leads to interstitial oedema with enzyme-rich
fluid, +/- cytokine-induced increased vascular permeability. Oedema may compromise blood flow.
2. Direct acinar cell injury, eg, trauma,ischaemia,drugs,viruses.
3. Abnormal packaging and transport of intracellular proenzymes. Seen in animal models; may be a factor in alcohol. Alcohol may act by increasing secretion, spasm of sphincter of
Oddi, direct toxic effect.
Clinical features and complications
Clinical features. Severe, constant upper abdominal pain radiating to the back, nausea and vomiting, epigastric tenderness. Shock in the severe form.
The severe form is an acute medical emergency and the differential is that of the “acute abdomen.” 5% mortality in first week.
Laboratory findings. Serum amylase rise in 1st 24 hours. Serum lipase rise in 72 hours.
Hypocalcemia and glycosuria may occur. Complications. ARDS and acute renal failure.
Pseudocysts (lined by granulation tissue).Infection and abscess formation.
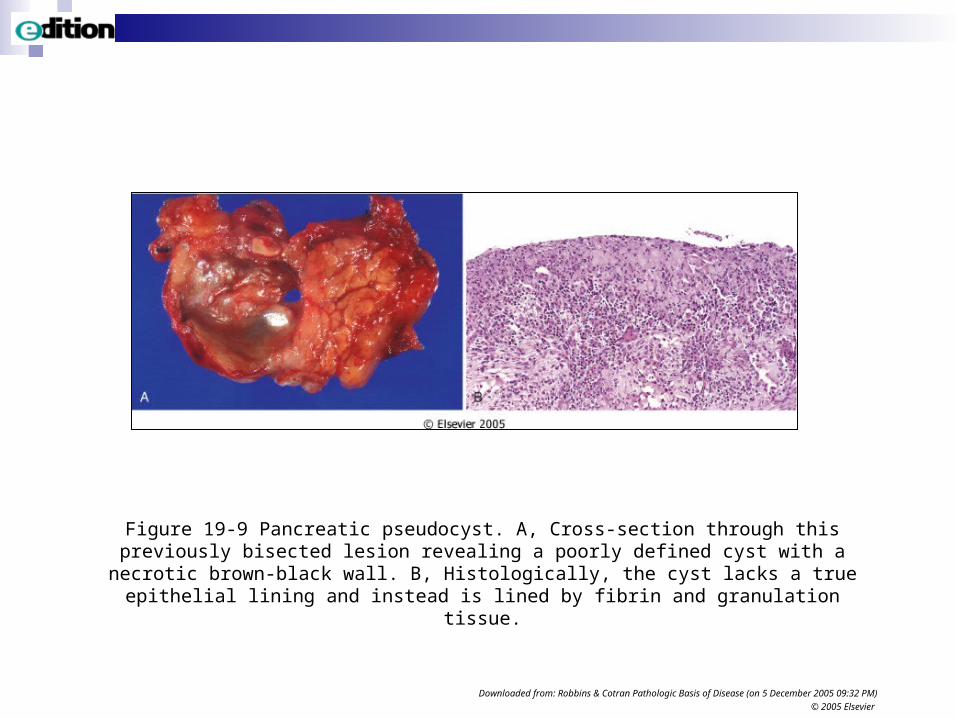
Figure 19-9 Pancreatic pseudocyst. A, Cross-section through this previously bisected lesion revealing a poorly defined cyst with a necrotic brown-black wall. B, Histologically, the cyst lacks a
true epithelial lining and instead is lined by fibrin and granulation tissue.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier
CHRONIC PANCREATITIS
Inflammation and fibrosis with loss of the exocrine pancreas and, in late stages, of the endocrine pancreas.
Usually progressive. May appear to be repeated attacks of “acute” pancreatitis. Irreversible.
Incidence difficult to assess owing to difficulties in diagnosis. Probably 3 per 100,000.
Average age of onset 40yrs. in Western societies. M>F. <20yrs. In the tropics. M=F.
Aetiology
Alcohol. 80% in Western societies. Mainly middle-aged males.
Obstruction, eg pancreas divisum (a congenital anomaly), calculi, stenosis of ampulla of Vater, neoplasms, pseudocyst.
Tropical pancreatitis. Possibly due to protein/calorie malnutrition.
Hereditary pancreatitis due to the germ line mutations seen in some cases of acute pancreatitis.
Idiopathic. Some patients have mutations of the cystic fibrosis transmembrane conductance regulator (CFTR) gene but different to those seen in cystic fibrosis.
Pathogenesis
Unclear but 4 suggested mechanisms. 1. Duct obstruction. Alcohol leads to hypersecretion of protein-
rich fluid -> protein plugs -> calculi. Other factors may cause pancreatic calculi in non-alcoholics.
2. Direct toxic effect of alcohol on acinar cells with accumulation of intracellular lipid, acinar cell loss, fibrosis.
3. Oxidative stress - free radicals due to alcohol. 4. Necrosis/fibrosis as a result of repeated attacks of acute
pancreatitis. Especially thought to be a factor in hereditary forms.
Pancreatic stellate cells are transformed into myofibroblasts and are important in the fibrosis formed in chronic pancreatitis.
Morphology and clinical features
Morphology. Hard gland due to fibrosis; may have dilated ducts and calculi. Microscopically great loss of parenchyma and replacement by fibrosis.
Clinical features. Recurrent abdominal pain becoming constant and severe. Often radiates to back. Serum amylase may be raised. Jaundice if fibrosis affects common bile duct. Malabsorption with steatorrhoea, and weight loss. Diabetes mellitus. Pancreatic pseudocysts in 10%. Pancreatic carcinoma in hereditary forms.
Investigations include imaging and tests of pancreatic function.
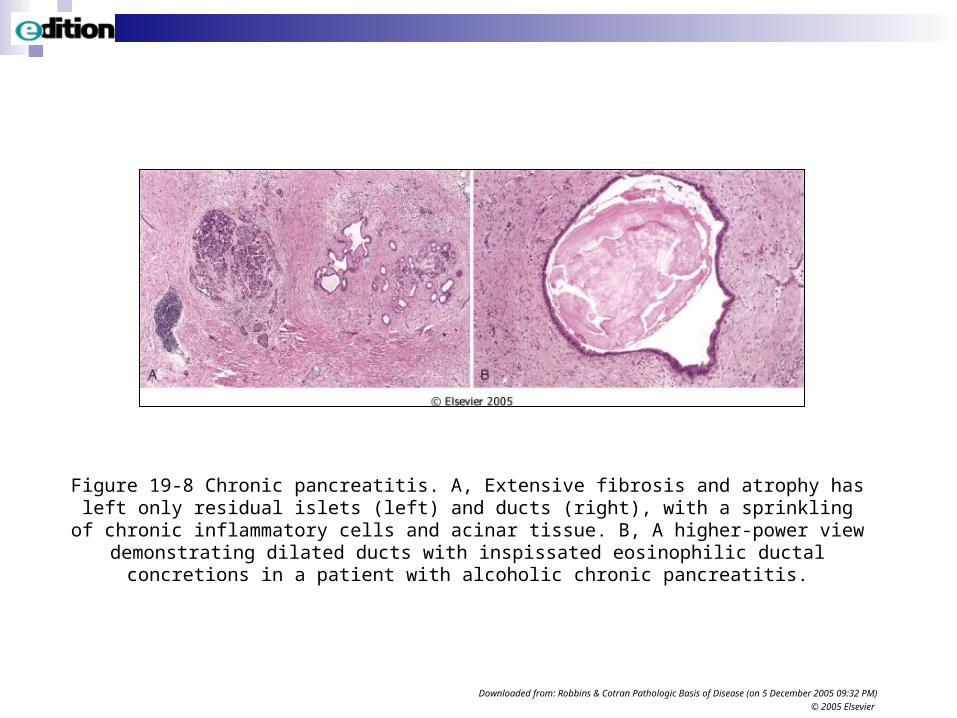
Figure 19-8 Chronic pancreatitis. A, Extensive fibrosis and atrophy has left only residual islets (left) and ducts (right), with a sprinkling of chronic inflammatory cells and acinar tissue. B, A
higher-power view demonstrating dilated ducts with inspissated eosinophilic ductal concretions in a patient with alcoholic chronic pancreatitis.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 09:32 PM)
© 2005 Elsevier
CARCINOMA OF THE PANCREAS Increasing in frequency in
Western countries, eg doubled in the past 40 years in England and Wales.
Incidence 10 per 100,000. 4th most common cause of
death in the USA. Age 50+ M=F or slight male
preponderance.
Aetiology.
Smoking - strong association. High lipid diet - weak
association.
Chronic pancreatitis associated statistically, but may not be the cause, except hereditary form.
Diabetes mellitus associated but probably secondary to pancreatic destruction by tumour.
Precursors
Epithelial precursor lesions show a progression from non-neoplastic changes to non-invasive neoplastic changes to invasive carcinoma.
These are named pancreatic intraepithelial neoplasia (PanIN)Stages 1-3 are described before frank invasion.
Molecular changes parallel the above with early telomere shortening, K-RAS mutations followed by inactivation of p16, followed by inactivation of p53 and SMAD4. Many other less common genetic changes are described.
Predisposing familial syndromes are described.

Morphology
Usually a solid, hard, white tumour. 60% arise in the head. 15% arise in the body. 5% arise in the tail. 20% are diffuse.
Usually an adenocarcinoma arising from ductal epithelium. Typically has much fibrous stroma. Often shows a tendency to peri-neural invasion.
Spread is:- Direct to other adjacent structures. To regional lymph nodes. To liver and lungs.
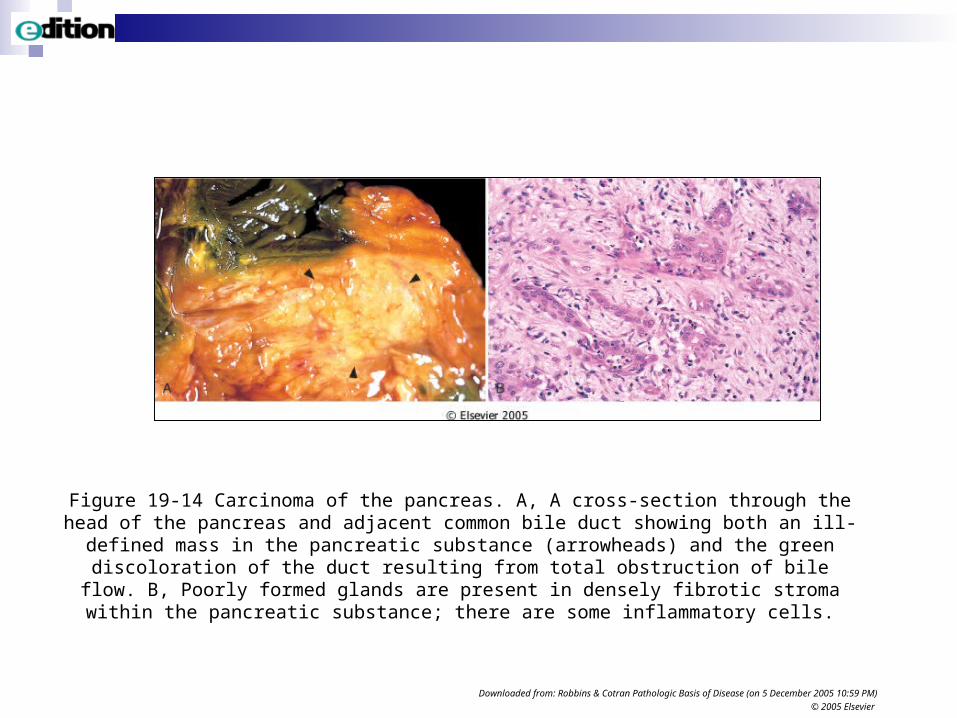
Figure 19-14 Carcinoma of the pancreas. A, A cross-section through the head of the pancreas and adjacent common bile duct showing both an ill-defined mass in the pancreatic substance
(arrowheads) and the green discoloration of the duct resulting from total obstruction of bile flow. B, Poorly formed glands are present in densely fibrotic stroma within the pancreatic substance;
there are some inflammatory cells.
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 5 December 2005 10:59 PM)
© 2005 Elsevier
Clinical features and course
Abdominal pain, often constant, radiating to back, relieved by leaning forward.
Weight loss and later cachexia. Obstructive jaundice if arising in the head and obstructing CBD with
palpable gall bladder (Courvoisier’s sign). Migratory thrombophlebitis is 10% (Trousseau’s sign). CEA and CA19-9 antigen in peripheral blood but not specific.
Average survival from symptom onset to death is 7.5 months. 5 year survival is 1%. The poor prognosis is due to the advanced nature of the tumour and its
unresectability by the time of diagnosis.
Other neoplasms, cysts, congenital anomalies Less than 5% of pancreatic neoplasms are cystic, either serous
cystadenomas or mucinous cystadenomas/cystadenocarcinomas.
Pancreaticoblastoma is a rare childhood neoplasm.
Congenital cysts may be associated with cysts in other organs.
Pancreas divisum is the most common congenital anomaly.Annular pancreas may cause duodenal obstruction. Ectopic pancreatic tissue may occur in the GIT.
The pancreas is one of the most important organs to be involved in cystic fibrosis (mucoviscidosis).
Top Related