







Languages
Pages
Legal

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 1/26
1
CHAPTER 1BACKGROUND
1.1 Background
Dengue virus infection is an acute fever caused by a virus of the genus
flavivirus, family Flaviviridae which has four serotypes are DEN-1, DEN-,
DEN-!, and DEN-", through the intermediary by Aedes aegypti or Aedes
albopictus. #ourth dengue serotypes are in $ndonesia. DEN-! is the
predominant serotype and is associated with severe cases, followed by DEN-.1
%t this time, the number of dengue cases is still high at around 1&-' per
1&&.&&& population. (he age at which most children affected by dengue are
aged "-1& years. (he death rate due to dengue fever from &&1 to &&) is 1**
people. $n $ndonesia reported as many as 11.!!" cases of dengue fever with a
mortality rate of +*+ cases.!
(he clinical spectrum of dengue can be divided
into silent dengue infection, dengue fever, dengue hemorrhagic fever and
dengue shock syndrome.1
1. bective
(his paper is one of the reuirements to fullfil in the senior clinical
assistance programs in /ediatric Department of 0ai %dam alik 2eneral
0ospital, 3niversity of 4umatera 3tara. $n addition, this paper can be used asreference to know and understanding a little about dengue infection.

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 2/26
2
CHAPTER 2
LITERATURE REVIEW
.1. Dengue 5irus $nfection
.1.1 Definition
Dengue 5irus $nfection is a disease that caused by mosuito6s bite, such
as Aedes Aegypty and Aedes Albopictus.1
Dengue hemorrhagic fever 7/hilippine, (hai, or 4ingapore hemorrhagic
fever8 hemorrhagic dengue8 acute infectious thrombocytopenic purpura9 is an
acute and severe, often fatal, febrile disease caused by the dengue viruses, a group of
four antigenically related flaviviruses designated serotypes 1 through ". $t is
characteri:ed by capillary permeability, abnormalities of hemostasis, and in severe
cases, a protein-losing shock syndrome (dengue shoc s!nd"o#e$% which is
thought to have an immunopathologic basis.
.1. Epidemiology
Dengue disease is endemic disease in many countries such as $ndonesia,
yamar, (hailand, (imor ;este, and others. $n $ndonesia, dengue disease is a
contagious disease and a freuent cause of outbreaks. (his disease is second rank
disease of the top ten diseases that hospitali:ed patients in $ndonesia in &&*.
Based on the data, the cases of dengue hemorrhagic fever as much as 11.!!"
with the death as many as +*+ cases.!," 4till high number of deaths due to dengue
fever can not be separated from risk factor of dengue shock syndrome. Based on
the results of research conducted 4ubahagio 7&&*9 that 1)< of patients with
dengue fever will develop into dengue shock syndrome.' eanwhile, according to
research conducted by %nders, et al., that children aged = to 1& years are at risk of
developing into dengue shock syndrome and girls are more likely to suffer from
dengue shock syndrome than boys.=

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 3/26
3
.1.! Etiology
Dengue fever is the cause of dengue virus has four serotypes 7dengue-1,
dengue-, dengue-!, dengue-"9, which included in the %rbovirus group, genus
Flavivirus, family Flaviviridae. %rbovirus is a virus that is transmitted by
arthropods such as mosuitoes.1 Dengue virus entered to the human body through
the bite of aedes aegypti. $n general, these mosuitoes bite during the day 7*>&& to
1&>&& pm9 and afternoon 71=>&& to 1)>&&9. %edes aegypty lives in tropical to
subtropical lowland. %dult mosuitoes are medium-si:ed, dark brown body, and
the body and legs are covered with scales and silvery white stripes.
%edes aegypty likes the cool house, damp, dark, and alighted on clothing or
belongings hanging. % place to live in clear stagnant water such as a bath tub and
water reservoirs. %edes aegypti mosuito lifespan of about to ! weeks, laying
about && to "&& grains, and flew a distance of about 1&& meters.)
Aedes aegypti is a small, dark mosuito with white lyre shaped markings
and banded legs. (hey prefer to bite indoors and primarily bite humans. (hese
mosuitoes can use natural locations or habitats 7for e?ample treeholes and plant
a?ils9 and artificial containers with water to lay their eggs. (hey lay eggs during
the day in water containing organic material 7e.g., decaying leaves, algae, etc.9 in
containers with wide openings and prefer dark-colored containers located in the
shade. %bout three days after feeding on blood, the mosuito lays her eggs inside
a container ust above the water line. Eggs are laid over a period of several days,
are resistant to desiccation and can survive for periods of si? or more months.
@hen rain floods the eggs with water, the larvae hatch. 2enerally larvae feed
upon small auatic organisms, algae and particles of plant and animal material in
water-filled containers. (he entire immature or auatic cycle 7i.e., from egg to
adult9 can occur in as little as )-+ days. (he life span for adult mosuitoes is
around three weeks. Egg production sites are within or in close pro?imity to
households.
Aedes albopictus 74kuse9, also called the A%sian tiger mosuito6, is a
vector for a series of human arboviruses among which flaviviruses 7dengue virus,

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 4/26
4
yellow fever virus, apanese encephalitis virus, and @est Nile virus9 and
togaviruses 7Coss Civer virus and hikungunya virus9. (he species is known to be
an important vector of dengue, second only to Aedes aegypti, and is suspected to
be the only important vector of the hikungunya outbreak on the $ndian $slands
outbreak in &&=. (he %sian tiger mosuito is a highly invasive mosuito species
and is difficult to control. $t is an aggressive day biting mosuito whose bites can
cause dermatological and allergic reactions. $t is considered a container breeder,
preferring to oviposit in small uantities of water such as drums, tyres, buckets,
flower saucers, tarpaulins, and manholes.
.1." lassification
%ccording to the @0 in &11 that the dengue virus infections are
classified as follows> 1

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 5/26
5
/icture 1. lassification of Dengue $nfection
.1.' /athogenesis
/athogenesis of dengue hemorrhagic fever is still debated. Based on
available data, there is strong evidence that the mechanism of imunopatologis role
occurrence of dengue hemorrhagic fever and dengue shock syndrome.
(he immune response that is known to play a role in the pathogenesis of dengue
are>
a9 0umoral response in the form of antibodies that play a role in virus
neutrali:ation process. %ntibodies to dengue virus play a role in virus replication
accelerates in monocytes or macrophages. (his hypothesis is called antibody
dependent enhancement.
b9 ( lymphocytes both (-helper 7D"9 and ( cytoto?ic 7D+9 plays a role in
cellular immune response against dengue virus. (01 differentiation of ( helper
that will produce interferon gamma, $;- and lymphokine, while (h produces
$;-", $;-', $;-= and $;-1&8
c9 onocytes and makrolag role in phagocytosis by opsoni:ation virus
antibodies. 0owever, this causes increased phagocytosis process of viral
replication and secretion of cytokines by macrophages8
d9 $n addition, (he activation of complement by immune comple?es led to
the formation of !a and 'a.
0alstead in 1*)! filed a secondary heterologous infection hypothesis
which states that dengue fever occurs when a person is infected with the dengue
virus with different types. Ce-infection causes anamnestic antibody reaction
resulting in high concentrations of immune comple?es.
;ess and Ennis in 1**" summari:es the opinion 0alstead and other researchers8
states that dengue virus infection causes macrophage activation phagocyte virus-
antibody comple? non neutrali:ation so that the virus replicate in macrophages.
acrophage infection by dengue virus causes the activation of ( helper and
cytoto?ic ( thus produced lymphokines and interferon-gamma. $nterferon gamma
activates monocyte thus secreted a variety of inflammatory mediators such as
7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 6/26
6
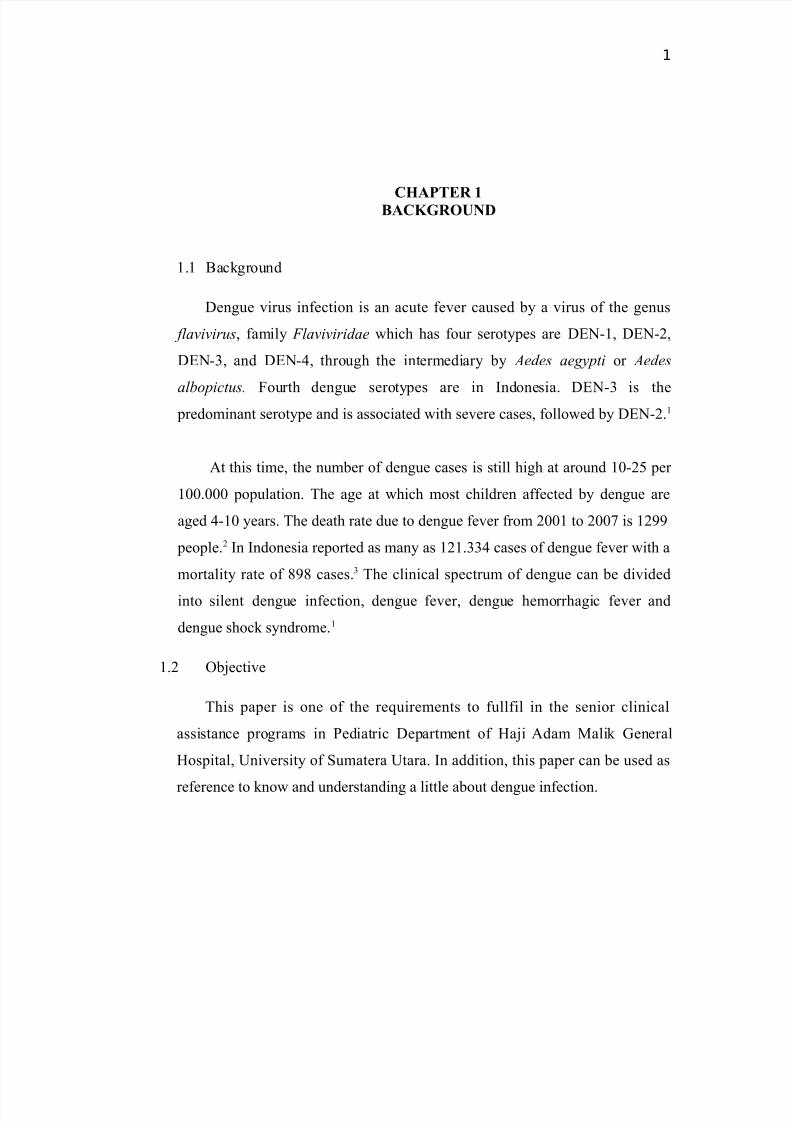
(N#-, $;-1, /%# 7platelet activating factor9, $;-= and histamine that causes
dysfunction of endothelial cells and plasma leakage. $ncreased !a and 'a
occurs through activation of the virus-antibody comple? that also resulted in the
leakage of plasma. (hrombocytopenia in dengue infections occur through the
mechanism of bone marrow suppression and destruction and shortening the life
span of platelets.+
/icture . /athogenesis of D0#
.1.=. (he ourse of Disease
(he course of disease in dengue hemorrhagic fever is divided into !
phases. (here are three phases of dengue hemorrhage fever such as>
1. #ever /hase
/hase fever lasts to ) days with a body temperature of about !* to "&
. $n the acute febrile phase usually accompanied by redness of the face,
erythema of the skin, pain in the whole body, and headache. 4ome patients

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 7/26
7
also complain of difficulty swallowing, pharyngeal pain, conunctival pain,
loss of appetite, nausea, and vomiting. During the initial phase of fever is
difficult to distinguish between dengue fever and dengue hemorrhagic
fever. n dengue fever, once free of fever for " hours without fever,
patients will enter a period of healing. 0owever, in patients with
hemorrhagic fever, after the febrile phase is completed it will go into a
critical phase.
. ritical /hase
Body temperature in the critical phase decreased by about !).' or down
below. (his phase generally occurs in the third to fifth day of fever. $n thecritical phase of increased capillary permeability causing leakage of
plasma. ritical phase lasts for " to "+ hours. $f there is no leakage of
plasma, the patientFs condition will improve but if there is leakage of
plasma, the patientFs condition will deteriorate. onditions of prolonged
plasma leakage and delays will cause shock.
!. Cecovery /hase
/atients who have passed the critical phase, there will be a process of re-
absorption of fluids within to ! days and gradually the patientFs condition
will improve. 0ealing phase lasts between to ) days. 2enerally dengue
fever patients who have successfully passed the critical phase will recover
without complications within " to "+ hours after the shock. (he healing
phase is characteri:ed by the condition of the patient began to improve,
appetite begins to increase, and vital signs were stable. $n this phase of
intravenous fluids is usually discontinued, replaced with nutrition orally.

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 8/26
8
/icture !. /hase of D0#
.1.) Diagnosis
a. Dengue fever 1
$s an acute febrile illness for -) days, characteri:ed by two or more of
the following clinical manifestations>
G 0eadache.
G /ain retro-oebital.
G yalgia H arthralgia.
G 4kin rash.
G Bleeding manifestations 7petechiae or positive bending test9.
G (orniuet test 7I9.

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 9/26
9
b. Dengue 0emorrhagic #ever 1
Based on the 1**) @0 criteria for D0# diagnosis is made when all of
these things below filled >
G #ever lasts -) days, occasionally biphasic
G 0emorrhagic tendencies
G thrombocytopenia 7J1&&,&&& H mm!9
G Evidence of plasma leakage, manifested
by> - Cise in hematocritK &<
- Drop in hematocrit following volume replacement
- 4igns of plasma leakage
/icture ". 2rade of D0#
c. Dengue 4hock 4yndrome1
• %ll four criteria of D0# must be present
• Evidence of circulatory failure
anifested by >
- Capid and weak pulse
- Narrow pulse pressure 7J & mm0g9 or
- 0ypotension for age, and
- old, clammy skin and restlessness

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 10/26
10
/icture '. Diagnosis of D0#
.1.+ Differential Diagnosis
- easles
- $(/
- hikungunya
- 4carlet #ever
.1.* anagement

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 11/26
11
/icture =. anagement of 4uspected Dengue $nfection
7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 12/26
12
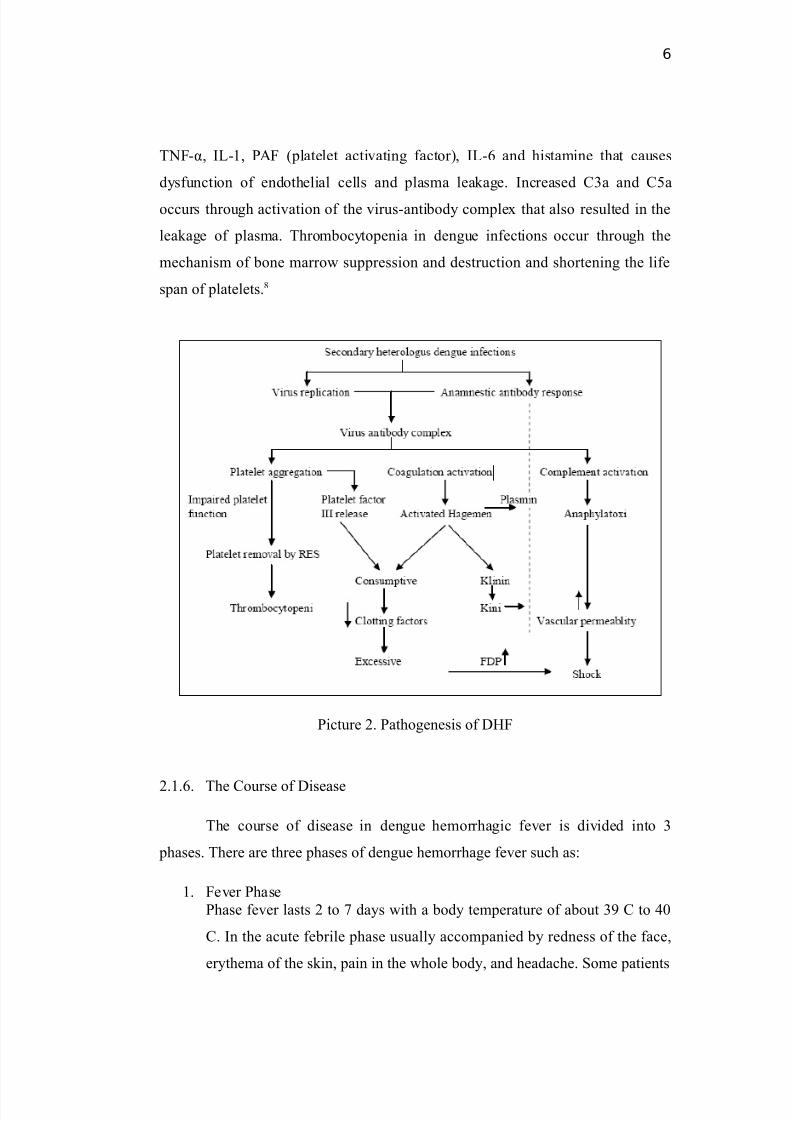
/icture ). anagement of 4uspected Dengue #ever 7$npatient9 or Dengue#ever
7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 13/26

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 14/26
14
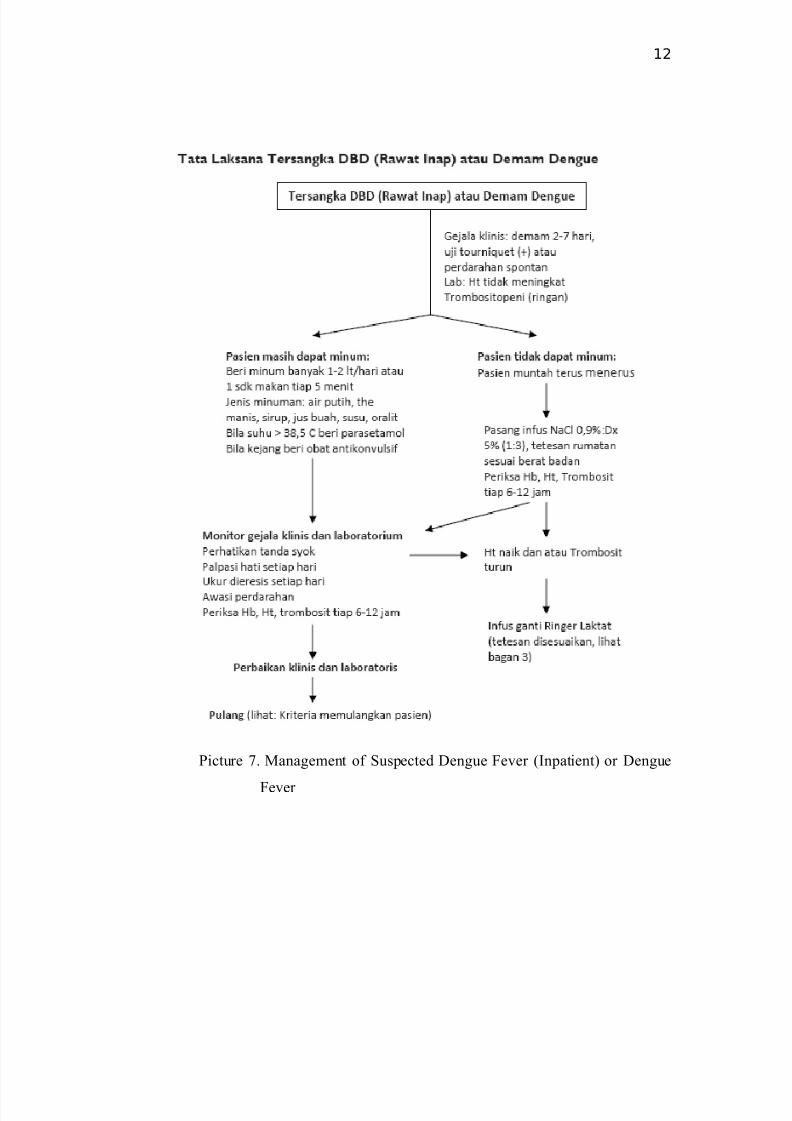
/icture *. anagement of D0# grade $$$ and $5.

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 15/26
15
CHAPTER III
CA&E REPORT
'1 O)*ec+,-e
(he obective of this paper is to report a case of a 1= years old and
months old girl with a diagnosis of Dengue 0emorrhagic #ever.
'2 C.se
% 1= years and months years old boy admitted to emergency room in
0ai %dam alik 2eneral 0ospital edan on = th anuary &1= at 1."& p.m with
the main complain of fever since several days ago.
'' H,s+o"! o/ D,se.se
/atients present with fever e?perienced appro?imately days before
entering %dam alik hospital. #ever with high temperature and goes down with
the consumption of fever medicine. (he patient also complain about headache and
vomiting for the last ! days. 0istory of spontaneous bleeding was not found.
0istory of nausea and vomiting was found since three days ago. 0eadache
encountered since days ago. %bdominal pain and oint pain was found. oughs
and colds was not found. Black colour stool was found. 3rination was within
normal range. 0istory of traveling out of town and to the malaria endemic area
was denied.
H,s+o"! o/ #ed,c.+,on0 -
H,s+o"! o/ /.#,!0 #amily history of the same disease was found.
H,s+o"! o/ ."en+s3 #ed,c.+,on> 3nclear
Ph!s,c. E4.#,n.+,on0
7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 16/26
16
• P"esen+ &+.+us0 ;evel of consciousness> ompos mentis. Body
temperature> !),* L, B@> !' kg, B0> 1=& cm. anemic 7-H-9, ikteric 7-H-9,dyspnea 7-9, cyanosis7-9, edema 7-9.
• Loc.,5ed &+.+us
- 0ead> Eye> eye light reflect IHI, conunctiva palpebral inferior pale -H-,
EarHNoseHouth> within normal range.
- Neck>
ugular 5ein /ressure> CI cm 0o
- (hora?>
4ymetrical fusiformis, Cetractions 7-9, CC> &?HiHregular,
respiratory sound> vesicular, additional sound 7-9, 0C> *& ?Hi,
regular, murmur 7-9.
- %bdomen>
4oepel, /eristaltic 7I9 N, 0epar and ;ien> unpalpable, Epigastric
pain 7I9.
- E?tremities>
/etechial rash is found on the lower of left arm, pulse> *&?Hi,
regular, weak, cold acral, C( J !M, edema pretibial 7-9, blood
pressure> 11&H+& mm0g.
L.)o".+o"! 6,nd,ngs0
=rd an &1'
omplete Blood ount>
(est Cesult 3nit Ceferal
• Eye > light refle? IHI, isochoric pupil, conunctiva palpebra
inferior pale 7-H-9
• Ear > within normal range
• Nose > within normal range
• outh > within normal range

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 17/26
17
0emoglobin 1'.& g< 1!.-1).!
Erythrocyte '.1! 1&=
Hmm!
".&-".+)
;eucocyte .1* 1&!Hmm! ".'-11.&
(hrombocyte 11! 1&!Hmm! 1'&-"'&
0ematocrite ",+& < "!-"*
Eosinophil &.&& < 1-=
Basophil &.&& < &-1
Neutrophil ==.&& < !)-+&
;ymphocyte 1.)& < &-"&
onocyte 1.1& < -+
Neutrophil
absolute
!.*+ 1&!H; .)-=.'
;ymphocyte
absolute
1.!1 1&!H; 1.'-!.)
onocyte absolute &.)! 1&!H; &.-&."
Basophyl absolute &.&1 1&!H; &-&.1
5 )1.'& f; +'-*'
0 '.'& /g +-!
0 !'.)& g< !!-!'
Blood 2lucose *!.&& mgHd; J&&
4odium 1* mEH; 1!'-1''Oalium '.& mEH; !.=-'.'
hloride 1&1 mEH; *=-1&=
D,.gnos,s0 Dengue hemorrhagic fever without shock
The".!0
- $5#D D'< Nal &."'< "& dropsHminute macro
- $n. /aracetamol '&&mgH$5
- B Diet &&&kkal I *&gr protein

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 18/26
18
P"ognos.0
Dubia ad bonam
6oo7 U0
=th an &1= &).&&
& O A P
#ever 7I9 4ensorium> ompos
entis , (> !),+ o, B@> "'
kg, B0> 1=& cm.
0ead> Eye Ceflect IHI,
$sochoric /upil, on.
D0# - $5#D D'<
Nal &."'<
1& dropsHmin
micro
- $n.

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 19/26
19
/alpebral $nferior /ale -H-,
outhHNoseHEar> Normal.
Neck> 5/ CI 0
(hora?> 4ymetris
#usiformis, Cetraction 7-9
0C> +=?Hi, 4ystolic urmur
7-9, CC> "?Hi, Conchi -H-.
%bdomen> 4oepel, Normal
peristaltic, 0epar
unpalpable, ;ien>
unpalpable, Epigastric /ain
7I9.
E?tremities> /ulse> +=?Hi,
Cegular, @eak, @arm
%cral, C( J !M, Edema
/retibial 7-9, B/ > 11&H)&
mm0g.
Cumple leed (est 7I9
paracetamol
'&& mgH +
hoursH
intravenous.
- heck for $g2
anti dengue
- omplete
Blood test
6oo7 U0
=th an &1= 1).&&& O A P
#ever 7I9 4ensorium> ompos
entis , (> !),+ o, B@> "'
kg, B0> 1=& cm.
0ead> Eye Ceflect IHI,
$sochoric /upil, on.
/alpebral $nferior /ale -H-,
outhHNoseHEar> Normal.
D0# - $5#D D'< Nal
&."'< 1&
dropsHmin micro
- $n. paracetamol
'&& mgH + hoursH
intravenous.
- heck for $g2 anti

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 20/26
20
Neck> 5/ CI 0
(hora?> 4ymetris
#usiformis, Cetraction 7-9
0C> *&?Hi, 4ystolic
urmur7-9, CC> ?Hi,
Conchi -H-.
%bdomen> 4oepel, Normal
peristaltic, 0epar
unpalpable, ;ien>
unpalpable, Epigastric /ain
7I9.
E?tremities> /ulse> *&?Hi,
Cegular, %deuate, @arm
acral, C( J !M, Edema
/retibial 7-9, B/ > 11&H)&
mm0g.
Cumple leed (est 7I9
dengue
- omplete blood
test
6oo7 U0
)th an &1= &=.&&
& O A P
#ever 7I9 4ensorium> %lert, (> !*.1 o
,
B@> "' kg, B0> 1=& cm.
0ead> Eye Ceflect IHI,
isochoric pupil, on.
/alpebral $nferior /ale -H-,
NouthHnoseHEar> Normal.
Neck> 5/ CI 0
(hora?> 4ymetris #usiformis,
D0# - $5#D D'<
Nal &."'<
1& dropsHmin
micro
- $n.
paracetamol
'&& mgH +
hoursH

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 21/26
21
Cetraction 7-9 0C> 11&?Hi,
4ystolic urmur 7-9, CC>
"?Hi, Conchi -H-.
%bdomen> 4oepel, Normal
/eristaltic, 0epar unpalpable,
;ien> unpalpable. Epigastric
pain 7-9.
E?tremities> /ulse> 11&?Hi,
regular, %deuate, @arm
%cral, C( J !M, Edema
/retibial 7-9, B/ > 11&H=&
mm0g.
Cumple leed (est 7I9
$g > -
$g2 > I
intravenous.
6oo7 U0
+th an &1= 1=.!&
& O A P
#ever 7-9 4ensorium> , (> !), o,
B@> "' kg, B0> 1=& cm.
0ead> Eye Ceflect IHI,
$sochoric /upil, on.
/alpebral $nferior /ale -H-,
outhHNoseHEar> Normal.
Neck> 5/ CI 0
(hora?> 4ymetris #usiformis,
Cetraction 7-9 0C> *=?Hi,
D0# - $5#D D'<
Nal &."'<
1& dropsHmin
micro
- $n.
paracetamol
'&& mgH +
hoursH
intravenous.
7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 22/26
22
4ystolic urmur 7-9, CC>
+?Hi, Conchi -H-.
%bdomen> 4oepel, Normal
/eristaltic, 0epar unpalpable,
;ien> unpalpable. Epigastric
pain 7-9.
E?tremities> /ulse> 11+?Hi,
regular, %deuate, @arm
%cral, C( J !M, Edema
/retibial 7-9, B/ > 11&H)&
mm0g.
- urola? supp
CHAPTER IV
DI&CU&&ION
ase (heory

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 23/26
23
% 1= years and months years old boy
admitted to emergency room in 0ai
%dam alik 2eneral 0ospital edan on
=th anuary &1= at 1."& p.m with the
main complain of fever since several
days ago and was diagnosed with
Dengeu hemorrhagic fever..
/atients has a history of fever, nausea
and vomiting, headache, abdominal and
oint pain, black colour stool, and
petechie rash.
Based on laboratory result, trombosit was
11!.&&&Hmm!
- %ccording to research that children
aged = to 1& years are at risk of
developing into dengue hemorrhagic
fever and girls are more likely to suffer
from dengue hemorrhagic fever than
boys.
(he clinical manifestation of D0# are>
G #ever lasts -) days with of the
following such as headache, retroorbital
pain, myalgia, athralgia, and rash.
G 0emorrhagic manifestation.
;aboratory criteria of D0# are >
G(hrombocytopenia 7J1&&,&&& H mm!9
G Evidence of plasma leakage,
manifested by >
- Cise in hematocritK &<
- Drop in hematocrit following
volume replacement
- 4igns of plasma leakage
/atient was classified into dengue
hemorrhagic fever as manifested >
- Cumple leed test I
- D0# is classified into grade $, $$, $$$
and $5. D0# is diagnosed with the help
of rumple leed test
/atient was treated with >
- $5#D D'< Nal &."'< 1&
dropsHmin micro
- $n. paracetamol '&& mgH + hoursH
- (he management of dengue
hemorrhagic fever grade $ is >
$5#D D'< Nal &,"'< =-)
mlHkgbwHhour within !-" hours,

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 24/26
24
intravenous.
- onitoring for shock sign
and then evaluation. 7if the vital
sign still abnormally, higher the
fluid to 1&-1' mlHkgbwHhour. $f
the vital sign turn normally,
lower the fluid to ' to !
mlHkgbwHhour and then we6ve to
evalution again9. $n this case the
patient also diagnose with mild-
moderate gastroenteritis, so we
give this patient initial therapy
with $5#D D'< Nal &,"'<
1>tHmin micro
CHAPTER V
&U88AR9
% 1= years and months years old boy admitted to emergency room in
0ai %dam alik 2eneral 0ospital edan on = th anuary &1= at 1."& p.m with
the main complain of fever since several days ago.
/atients present with fever e?perienced appro?imately days before
entering %dam alik hospital. #ever with high temperature and goes down with

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 25/26
25
the consumption of fever medicine. (he patient also complain about headache and
vomiting for the last ! days. 0istory of spontaneous bleeding was not found.
0istory of nausea and vomiting was found since three days ago. 0eadache
encountered since days ago. %bdominal pain and oint pain was found. oughs
and colds was not found. Black colour stool was found. 3rination was within
normal range. 0istory of traveling out of town and to the malaria endemic area
was denied.
/atients was treated with $5#D D'< Nal&,"'< 1>tHmin7mikro9 for
rehydration and was give paracetamol '&&mgH+hoursHoral for the fever.
RE6ERENCE&
1. %ntonius 0, Eva Devita, 4etio 0, Ellen /. &&*. /edoman /elayanan Olinis
$D%$ > $nfeksi 5irus Dengue. $katan Dokter %nak $ndonesia.

7/25/2019 DHF William
http://slidepdf.com/reader/full/dhf-william 26/26
26
. @0. &&*. Dengue guidelines for diagnosis, treatment, prevention, and
control. @orld 0ealth rgani:ation.
!. Depkes C$. &&*. /rofil Oesehatan $ndonesia &&*. Diunduh >
www.depkes.go.id.
". Depkes C$. &&'. /encegahan dan /emberantasan Demam Berdarah di
$ndonesia. akarta > Direktorat enderal /engendalian /enyakit dan Oesehatan
;ingkungan.
'. 4ubahagio. &&*. enentukan #aktor Cesiko Dominan Oeadian Dengue 4yok
4indrome pada /enderita DBD. Diunduh > digilib.bmf.litbang.depkes.go.id.
=. %nders, O.;, et al. &11. Epidemiological factor associated with dengue shock
syndrome and mortality in hospitali:ed dengue patients.
AM.J.Trop.Med.Hyg,84(1).1!"1#4.
). 4aleha 4ungkar. &11. Buku %ar /arasitologi Oedokteran. akarta > #O3$.
+. @ichman, , et al., &1. /athogenesis of Dengue 0emmorhagic #ever. .
(ropical edicine and $nternational 0ealth. 1&-1&+.