





Languages
Pages
Legal


Compartment Syndrome

Introduction
• Relatively common• Commonly missed• Menace of the traditional bone setter• Life and limb-threatening consequences

Scope
• History• Definition and classification• Pathophysiology• Diagnosis• Treatment

History
• Volkmann (1881) – described contracture secondary to muscle necro
Cause ? – decreased arterial flow secondary to tight splints
• Bardenheuer (1911) – First to describe decompression for forearm compartment syndrome
• Griffiths (1940) – described 5 P’s

History
• Rorabeck (1976) – CS produced due to arterial insufficiency or venous obstruction
• Heppenstall (1988), Matava (1994) – described relationships between pressure, duration and muscle cell death

Definitions
Compartment syndrome exists when interstitial tissue pressure within an osteofascial envelope rises to levels that impair cellular function and, if sustained, can lead to irreversible changes in the contents of the compartment
Leversedge et al. JHS Vol 36A March 2011

Pathophysiology
Events at physical level – AV gradient theory (Rowland and Matsen)
Events at Cellular level – Ischemia reperfusion theory

Pathophysiology
Decreased Pa (Hge,
hypotension, elevati
on)
Increased Pv (increa
sed intersti
tial
pressure)
Decrease
d local bloo
d flow
Local Blood flow = Pa - Pv

Pathophysiology
ischemia Muscle death
Replacement by fibrous tissue
Contracture and
strangulation
neuropathy

Ischemia Re-perfusion Theory
Ischemia
Accumulation of intracellular
Calcium, activation of
enzymes, platelet
activation, NO synthesis, Neutrophil activation
Cell death
Microvascular
damage and
edema
Increased interstitial pressure

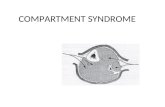
Compartment Syndrome - Causes
Decreased Compartment volume• Tight cast • Lying on limb• Burns eschar• Closure of fascia
Increased Compartment Content• Bleeding• Trauma
• Revascularization• Wringer injuries

Classification (Leversedge et al)
Acute insipient CS
Acute established CS (Reversible)
Late Compartment syndrome
Acute established CS (ir-reversible)
VIC

Diagnosis
• Predominantly clinical• Pain - out of proportion to clinical finding - not relieved by analgesics - worsening on elevation - increasing analgesic requirement

Diagnosis
• Sensory symptoms - type C fibers are most susceptible to
hypoxia - Parasthesia is early sign• Stretch test• Hard feel of compartment• Difficult situations – head injury, Brachial
plexus injury and anaesthetic block

Measurement of Compartment PressuresWhitesides Matsen
Clearance of Xenon – 133 - indicative of muscle circulationGelberman and Steinberg – probe for measuring tissue hardness

Diagnosis - Pitfalls
• Disappearance of pulse – might not happen
• Change of color – superficial veins still patent
• Elevated CPK and Myoglobin – no role• No role for MRI/CT scans

Management
• Removal of tight plasters• Elevate hand to level of heart• Splint – for comfort• Keep patient NBM• Inform OR• Frequent monitoring – clinical/manometer

Management - Medical
• Resucitation• Fluid and electrolyte balance• Monitor Renal function • Look for coagulopathy• Diuresis with Mannitol?

Surgical Treatment - Fasciotomy
• Longitudinal incisions• Wide exposure• Look for subcompartments• Consider epimysiotomy if necessary• Stabilize fractures• Neurolysis• Excision of dead muscle• No primary closure

Treatment

Post-op Managment
• Splint and elevate• Antibiotics• Physiotherapy• Continue monitoring• Plan wound closure as appropriate
Top Related