







Languages
Pages
Legal

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 1/35
The Ins and OutsThe Ins and Outsof of
ColoRectal Cancer ColoRectal Cancer ByBy
Kelly HannKelly Hann

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 2/35
Anatomy Anatomy
The Body¶s Digestive System
± Esophagus, Stomach, Small Intestine &
Large Intestine1st 6 feet = large bowel or colon
Last 6 inches = rectum & anal canal
The anal canal ends at the anus

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 3/35
American Cancer Society

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 4/35
Signs & SymptomsSigns & Symptoms
Change in bowel habits
Blood in Stool
± Bright red
± Very dark red ± Black/Tarry Stool
Diarrhea
Constipation
Does your bowel feel likeit emptied completely?
General abdominal
discomfort
± Gas pains
± Bloating ± Fullness
± Cramps
Weight loss w/ no
explained reason
Constant tiredness
Vomiting (coffee grounds)

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 5/35
Tests that examine«Tests that examine«
Rectum, Rectal Tissue, & BloodRectum, Rectal Tissue, & Blood
Aids in diagnosing & preventing colon cancer Aids in diagnosing & preventing colon cancer
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 6/35
Physical ExamPhysical Exam
General Medical History
± Includes self health habits
± Past self illnesses
± Various treatments used for previous issues
± Family health history
If patient reports problems with respect to signs
and symptoms related to common bowel change
habits« Are symptoms affecting your everyday life?
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 7/35
Fecal occult blood testFecal occult blood test
Check stool for evidence of blood
Method
± Small samples of stool are placed on specialcards and returned to the Dr. or Lab for
testing under a microscope
Potential harms
± False-positive & false negative results
(uncommon«serious

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 8/35
Digital Rectal ExamDigital Rectal Exam
The doctor or nurse inserts a lubricated,
GLOVED finger into the rectum to feel for
lumps or abnormal areas.

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 9/35
Barium EnemaBarium Enema
Barium is a liquid, that contains a silver-
white compound, inserted into the rectum
The barium coats the lower GI tract and aseries of x-rays are taken of the lower GI
tract
AK A = a lower GI series

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 10/35
What does a Barium Enema do?What does a Barium Enema do?
Detects
± Ulcers
± Narrowed areas (strictures) ± Growth of the lining (polyps)
± Small pouches in the wall of the intestine
Diverticula
± Cancer
± abnormalities

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 11/35
How can one prepare for this test?How can one prepare for this test?
Colon must be completely empty
± Prescribed laxatives or enema (pre-exam)
Special Diet to follow (2 days prior) ± Clear liquids
± Tea or coffee without milk or cream
± Any juice without pulp (NO OJ or Tomato)
± Broth
± Carbonated beverages
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 12/35
Types of Barium EnemasTypes of Barium Enemas
Single Column
± Lie on side on Xray table
± Enema tube inserted into rectum
± Barium bag is delivered into colon
± May feel urge to have a bowel movement«.DON¶T
± Though, a small balloon will keep it inside you
± Take long deep breaths through mouth«helps relax
± May be asked to turn & rotate to evenly coat all colon
± Then the radiologist will take a number of X-ray images
from various angles
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 13/35
Air Contrast (Double contrast) Air Contrast (Double contrast)
Similar to single-column
Big difference« Air is inflated with air in
addition to the barium to expand andimprove the quality of the images
Polyps can be seen easier, among other
abnormalities

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 14/35
Post Barium Enema instructionsPost Barium Enema instructions
You will be able to go to the restroomimmediately following the procedure to expellthe remaining barium
Over next few days your stool will be white, gray,or pink
Might be given a cleansing enema, laxatives,and told to drink a lot of liquids
The remaining barium can cause constipation. Refer back to MD if you don¶t return to normal in
3-4 days

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 15/35
ResultsResults
Negative = no
abnormalities are
found
Positive =abnormalities found,
such as polyps.
If positive you maybe scheduled for
further testing.
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 16/35
Pros of Barium EnemaPros of Barium Enema
Pros
± No sedation, complications are slight
(perforation of colorectal wall)
± If 50+ Medicare covers this every four years
for colorectal cancer screening as an
alternative to colonoscopy
± If you are high risk, covered every two years,though colonoscopy is preferred
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 17/35
Cons of Barium EnemaCons of Barium Enema
miss small polyps or sometimes evensmall cancers
Biopsy and polyp removal cannot be doneduring testing
you may need to follow up with acolonoscopy
Preparing for the procedure (emptying thecolon) and the procedure itself can beunpleasant
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 18/35
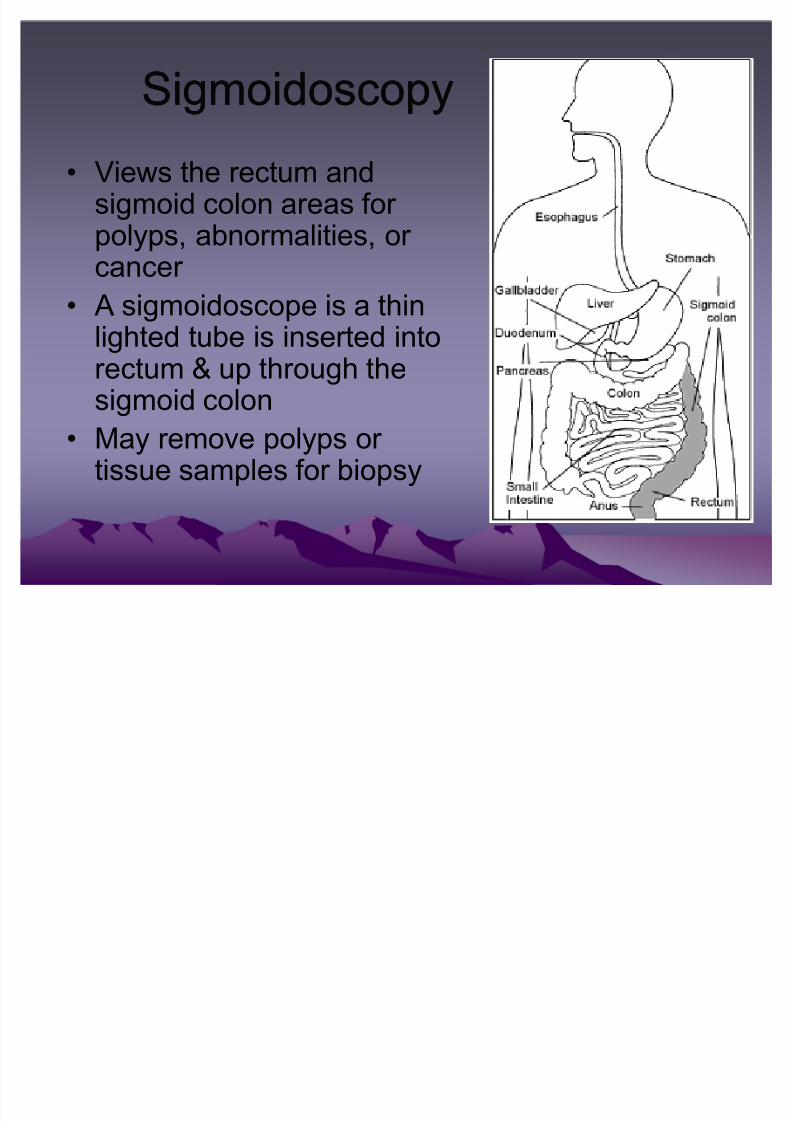
SigmoidoscopySigmoidoscopy
Views the rectum andsigmoid colon areas for polyps, abnormalities, or
cancer A sigmoidoscope is a thin
lighted tube is inserted intorectum & up through thesigmoid colon
May remove polyps or tissue samples for biopsy
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 19/35
Procedure DetectionProcedure Detection
The cause of diarrhea, abdominal pain, or constipation
Detect early signs of cancer in descending(sigmoid) colon and rectum
can see bleeding, inflammation, abnormalgrowths, and ulcers
not sufficient to detect polyps or cancer inthe ascending or transverse colon (two-thirds of the colon).

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 20/35
PreparationPreparation ComplicationsComplications
Liquid diet
Most likely given an
enema pre-procedure
Air is pumped into
colon to help expand
and see more surface
area
Duration is 10-20
minutes
Though very
uncommon
It is likely that
bleeding or apuncture of the colon
could result during
procedure

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 21/35
Polyp«««...RemovalPolyp«««...Removal
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 22/35
ColonoscopyColonoscopy
Procedure to look into entire length of
large intestine (colon) to detect
abnormalities
Preparation, procedure, & results same as
sigmoidoscopy
New virtual colonoscopy as alternative
procedure
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 23/35
Virtual or (CT) ColonographyVirtual or (CT) Colonography
a series of x-rays called computed
tomography to make a series of pictures of
the colon
Computer then puts these pictures
together to create a detailed image that
shows polyps, etc.

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 24/35
Prognosis (chances of recovery)Prognosis (chances of recovery)
Depends on
± Stage : in the inner lining of colon only, wholecolon? Spread to other places in body
± Has it blocked or created a hole in the colon? ± Blood levels of carcinoembryonic antigen
(CE A); a substance in the blood that may beincreased when cancer is present, before
treatment begins. ± Has cancer recurred?
± Patient¶s general health?

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 25/35
Treatment OptionsTreatment Options
Surgery (main treatment)
Radiation Therapy
Chemotherapy Newer targeted therapies
± Monoclonal antibodies
Depending on stage of cancer, it is likelythat 2-3 types of treatment may be utilized
at the same time or one after the other
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 26/35
SurgerySurgery
Removal of cancer and normal area of
colon on either side, as well as nearby
lymph nodes
Then sewn back together
Colostomy (bag to catch the waste kept
outside the body)
If cancer is found early, a colonscope can
be used without cutting the abdomen

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 27/35
Surgery for Rectal Cancer Surgery for Rectal Cancer
Surgery is main treatment, along with a combination of radiation therapy
Polypectomy, local excision, and local transanalresection) can be done with instruments placed into the
anus, Stage I, II, & III rectal cancers, other types of surgerymay be done
A low anterior resection is used for cancers near theupper part of the rectum, close to where it connects withthe colon.
Abdominoperineal resection is done for cancers locatedclose near the lower rectum-anal conjunction. After thissurgery, a colostomy is needed

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 28/35
Pelvic Exenteration:
± the surgeon removes the rectum as well asnearby organs such as the bladder, prostate,
or uterus if the cancer has spread to these
organs. A colostomy is needed after this
operation. If the bladder is removed, aurostomy (opening to collect urine) is needed
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 29/35
Radiation TherapyRadiation Therapy high-energy rays (such as x-rays) to kill or shrink
cancer cells
external radiation
internal or implant radiation; placed directly intotumor
Radiation can also be used to ease symptoms of advanced cancer such as intestinal blockage,bleeding, or pain
Main uses is for those where cancer hadattached to an internal organ or the lining of theabdomen
can be aimed through the anus and reaches therectum without passing through the skin of theabdomen

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 30/35
ChemotherapyChemotherapy
use of anticancer drugs injected into a vein or given by mouth
treatment useful for cancers that have spread todistant organs
increase the survival rate for patients with some
stages of colorectal cancer (will kill normal cellsalso)
Side effects depend on amount, length, & type of drugs given (i.e. diarrhea, nausea, vomiting, loss
of appetite & hair, mouth sores, increasedchance of infections, bruising & bleeding after minor cuts or injuries & overall increased fatigue
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 31/35
Risk FactorsRisk Factors
Age 50 or older
Obesity (fat in waist area increases)
30%-40% of smokers diagnosed with cancer will die
A family history of cancer of the colon or rectum.
A personal history of cancer of the colon, rectum, ovary,endometrium, or breast.
A history of polyps or ulcerative colitis (ulcers in thelining of the large intestine) or Crohn¶s disease.
Certain hereditary conditions, such as familial
adenomatous polyposis and hereditary nonpolyposiscolon cancer (HNPCC; Lynch Syndrome)
Heavy use of Alcohol has been linked to this cancer
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 32/35
Dietary Risk FactorsDietary Risk Factors
eat plenty of fruits, vegetables, and whole grainfoods
to limit high-fat foods (especially from animalsources) and limit excessive alcohol
consumption studies suggest that taking a daily multivitamin
containing folic acid or folate can lower risk
Other studies suggest that getting more calcium
with supplements or low-fat dairy products canhelp
Getting enough exercise is important as well 30min of physical activity on 5+ days per week.

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 33/35
Survival RatesSurvival Rates
9 of 10 people whose cancer is found & treated
at early stage (before spreading) will live at least
5 years
Spread to nearby organs/lymph nodes= 5years ± 66% survival rate
Spread to lungs/liver= 5 year ± 9%
(5 yr is based on percentage of patients thatwere alive 5 yrs after diagnosis. Leaving out
those who died of other causes)
8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 34/35
Closing PointsClosing Points These numbers provide an overall picture, but keep in
mind that every person¶s situation is unique and thestatistics can¶t predict exactly what will happen in your case.
Don¶t ³strain´ yourself«use more fiber in your diet(supplements work well when you can¶t get it through
your food intake ~ just drink lots of water & not within 1hour of laying down)
Eat healthy food when on the run pack your lunch/snacks
Increase your Healthy lifestyle potential
Parents/Grandparents Increase awareness that it is ok to get screened
Mark it on your to do list in 25-30 years as a birthdaypresent to yourself and family.

8/3/2019 Colorectal Cancer Presentation
http://slidepdf.com/reader/full/colorectal-cancer-presentation 35/35
Dedicated toDedicated to
FRANCIS HARRY COMPTON CRICK
1962 Nobel Laureate in Medicine f or their discoveries concerning the molecular structure of nuclear acids and its signi f icance f or inf ormation transf er
in living material.
Background
Born: 1916
Died: 7/2 9 /2004 Died Today of Colon Canc er (88 yrs old) R esidence: Great Britain
Aff iliation: Institute of Molecular Biology, Cambridge
Top Related