





Languages
Pages
Legal

Coagulopathy and Goal Directed Hemostatic Resuscitation in Pediatric
Trauma
Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery
Washington University in St. Louis School of Medicine December 3, 2013
Disclosure
I have no relevant financial or nonfinancial relationships to disclose
Outline
• Acute coagulopathy of trauma • TEG
– Mechanics – Interpretation
• TEG in adults trauma • TEG in pediatric trauma • SLCH
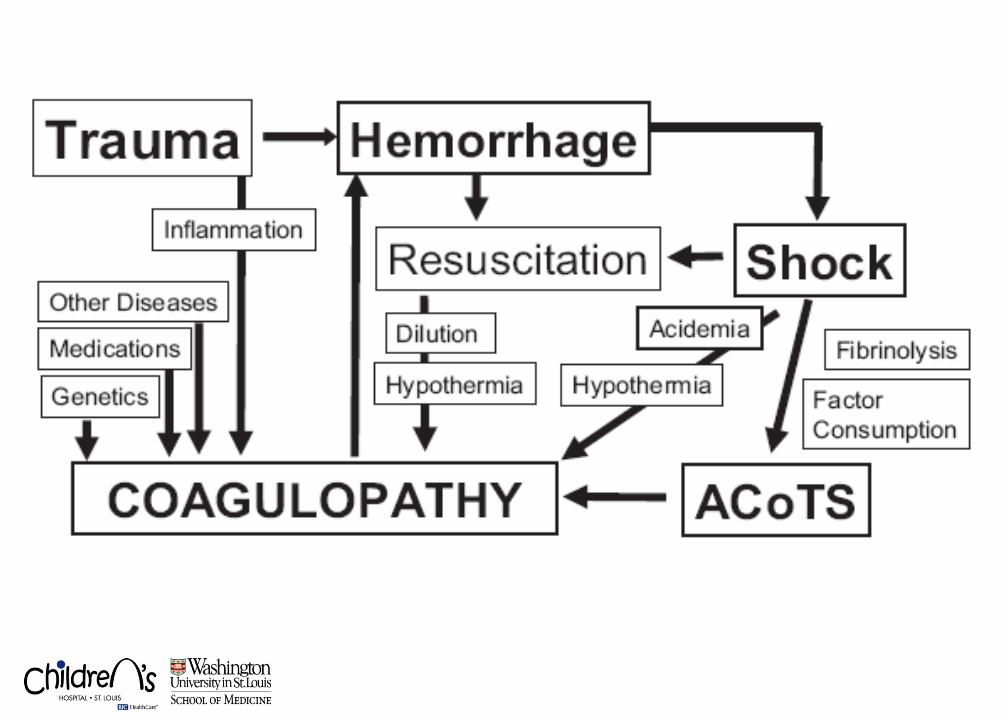
Acute Coagulopathy of Trauma


Acute Coagulopathy of Trauma • Multifactorial coagulopathy associated with severely
injured patients
• Distinct from: – “dilutional coagulopathy” – “transfusion related coagulopathy”
• Related to: – Tissue factor release – Protein C activation – Hypoperfusion – Hyperfibrinolysis
• 3287 patients, 391 patients transfused • Acute coagulopathy (INR > 1.5) on arrival: 38% • Mortality (+) coagulopathy 24% (vs. 4%)
• Retrospective study 1,088 patients • PT, aPTT, thrombin time >1.5 times nL
• On admission, 24.4 % (+) coagulopathic
• Coagulopathy: higher mortality (46% vs. 11%)
• 211 patients receiving MTP or TEP • Prevalence of coagulopathy 70% (INR>1.5)
• Mortality in non-coagulopathic 42% • Mortality in coagulopathic 67%
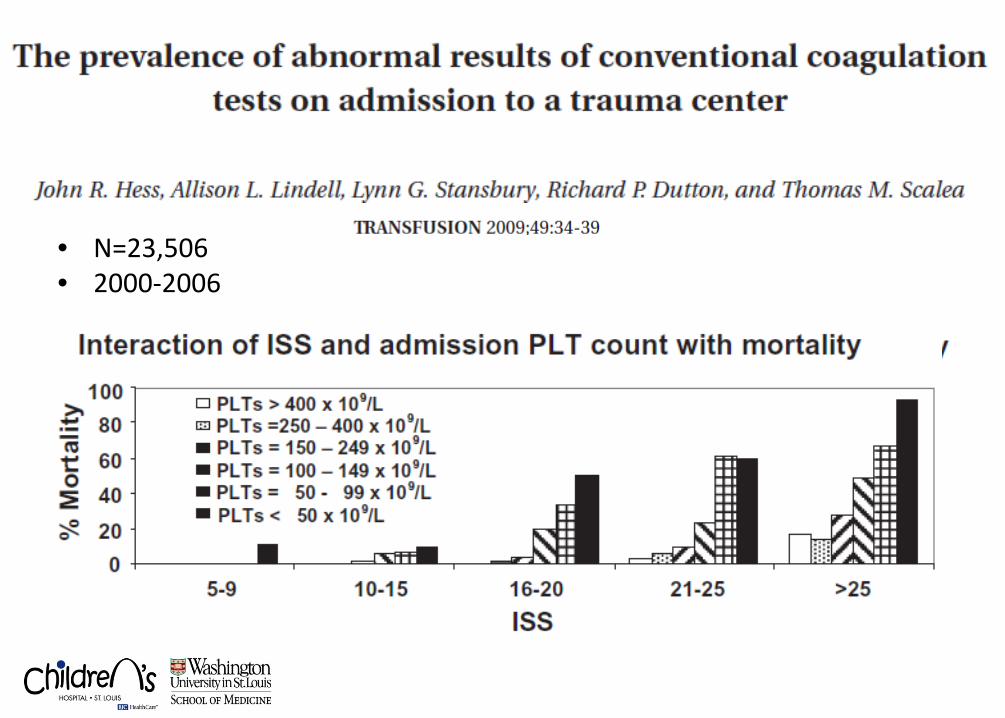
• N=23,506 • 2000-2006
In Children . . .
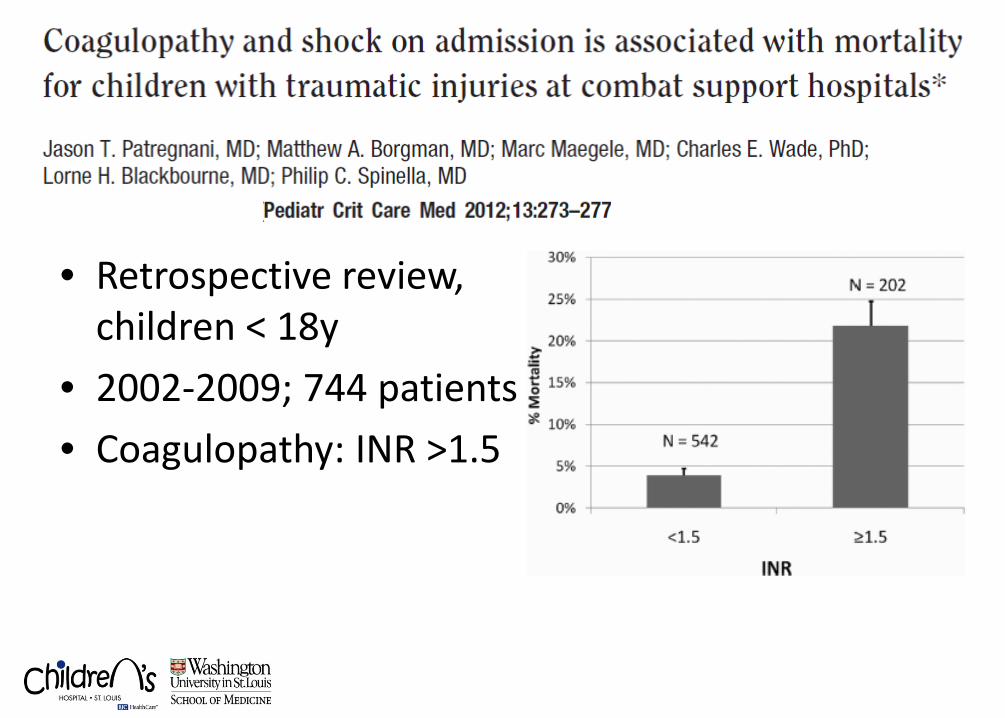
• Retrospective review, children < 18y
• 2002-2009; 744 patients • Coagulopathy: INR >1.5
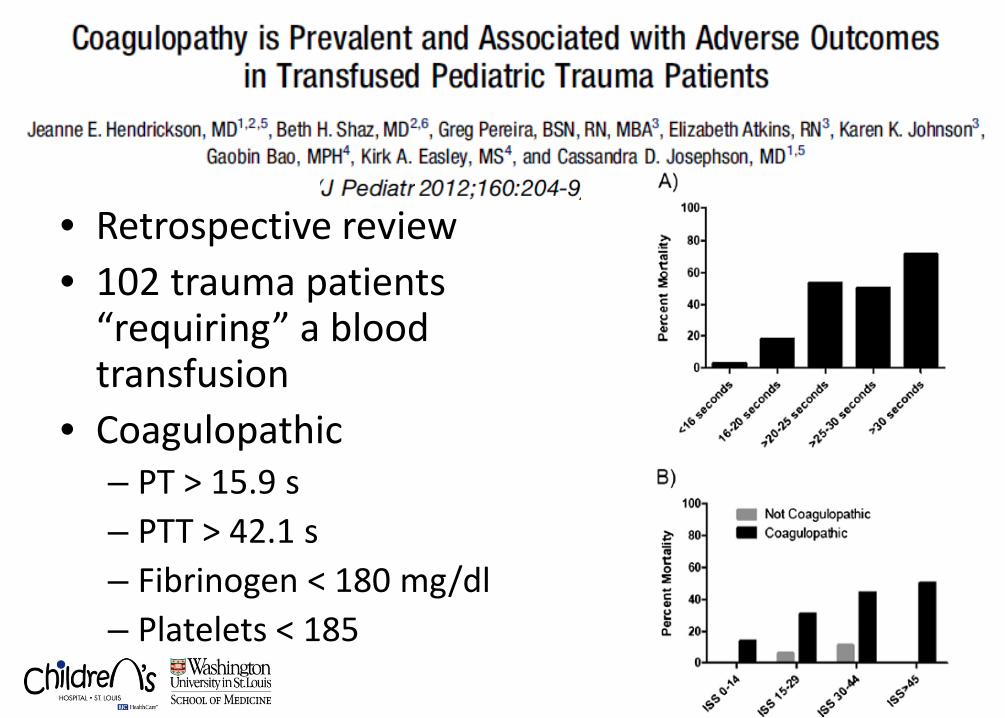
• Retrospective review • 102 trauma patients
“requiring” a blood transfusion
• Coagulopathic – PT > 15.9 s – PTT > 42.1 s – Fibrinogen < 180 mg/dl – Platelets < 185
We therefore conclude . . .
Acute coagulopathy of trauma is real and is BAD
“Goal Directed” Resuscitation • Restore “normal” physiology • Reversal of the “shock” state
• End Organ Perfusion
– Mental status, capillary refill, urine output • Vital signs
– HR, BP, MAP, RR, SaO2 • Laboratory data
– ABG base deficit, lactate • Real-time imaging
– FAST-ECHO, IVC filling
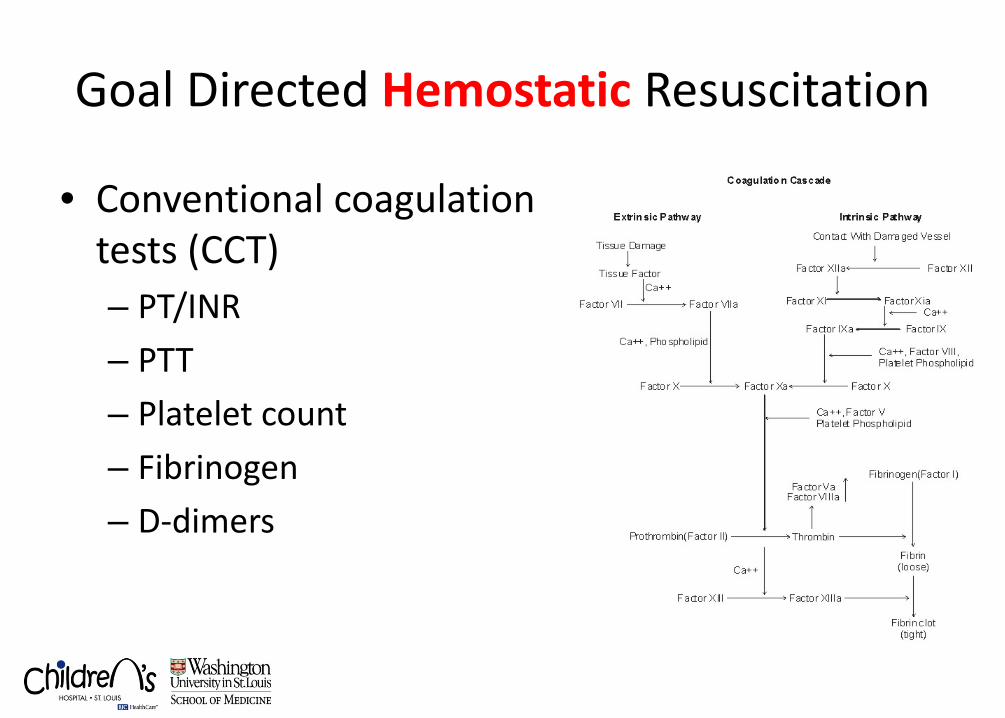
Goal Directed Hemostatic Resuscitation
• Conventional coagulation tests (CCT) – PT/INR – PTT – Platelet count – Fibrinogen – D-dimers
Thrombelastography • TEG
– Assesses global function of clotting proteins, platelets, and the fibrinolytic system
– Viscioelastic mechanical properties of blood – Useful point-of-care assay
• Different devices: TEG™ vs. ROTEM™
– Different names for the parameters
• Multiple flavors of “activating” agents: – Celite – Kaolin – Tissue factor – “Rapid”: Kaolin + tissue factor
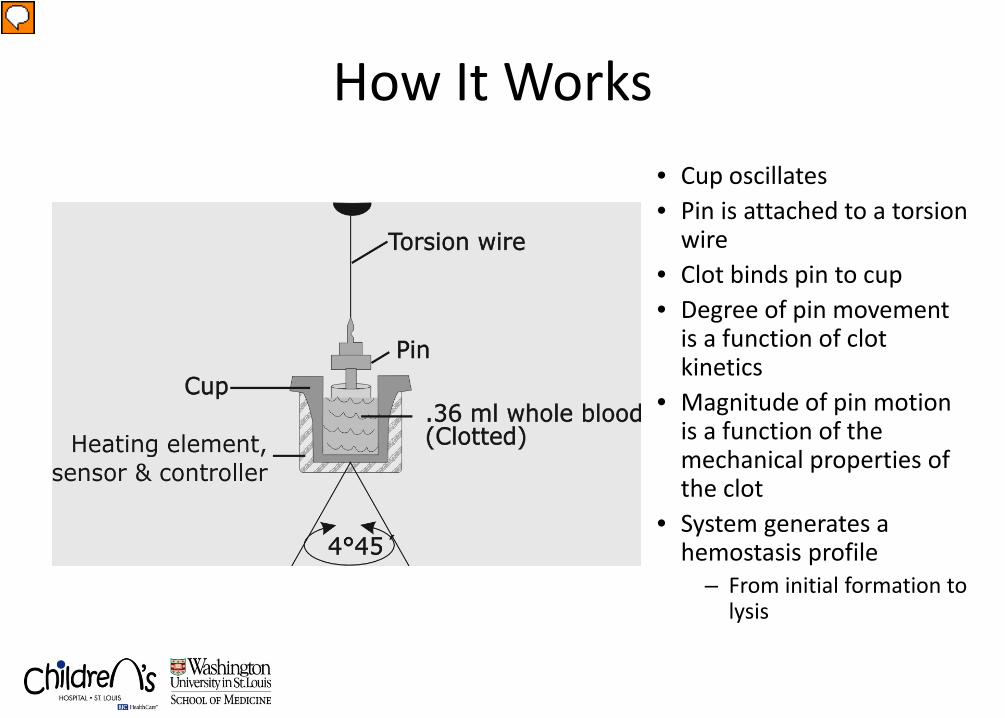
How It Works • Cup oscillates • Pin is attached to a torsion
wire • Clot binds pin to cup • Degree of pin movement
is a function of clot kinetics
• Magnitude of pin motion is a function of the mechanical properties of the clot
• System generates a hemostasis profile
– From initial formation to lysis
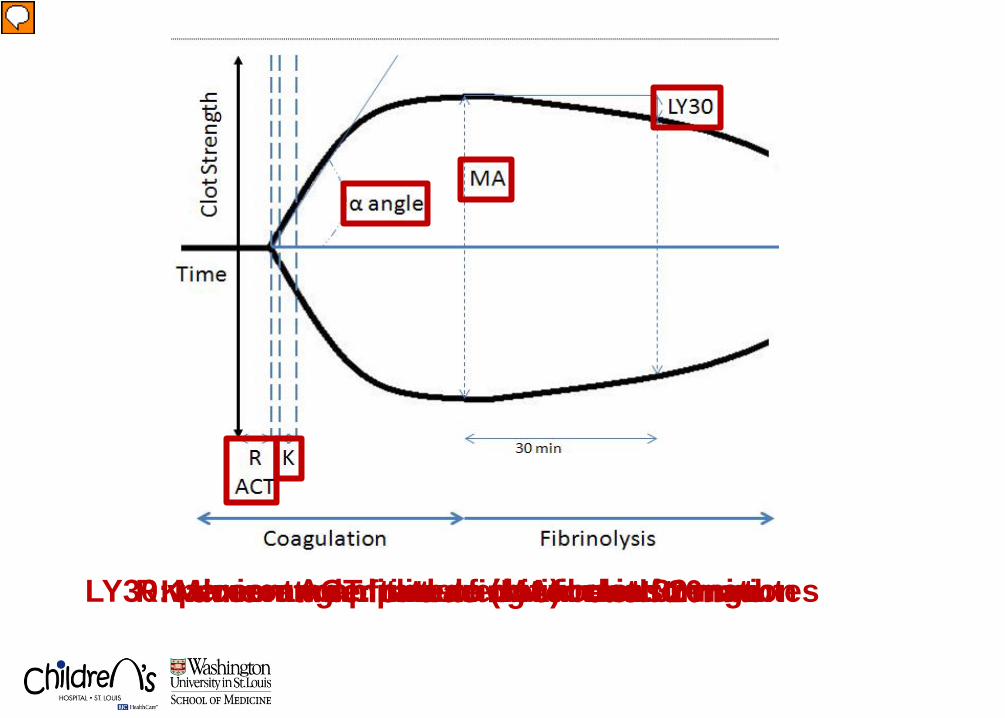
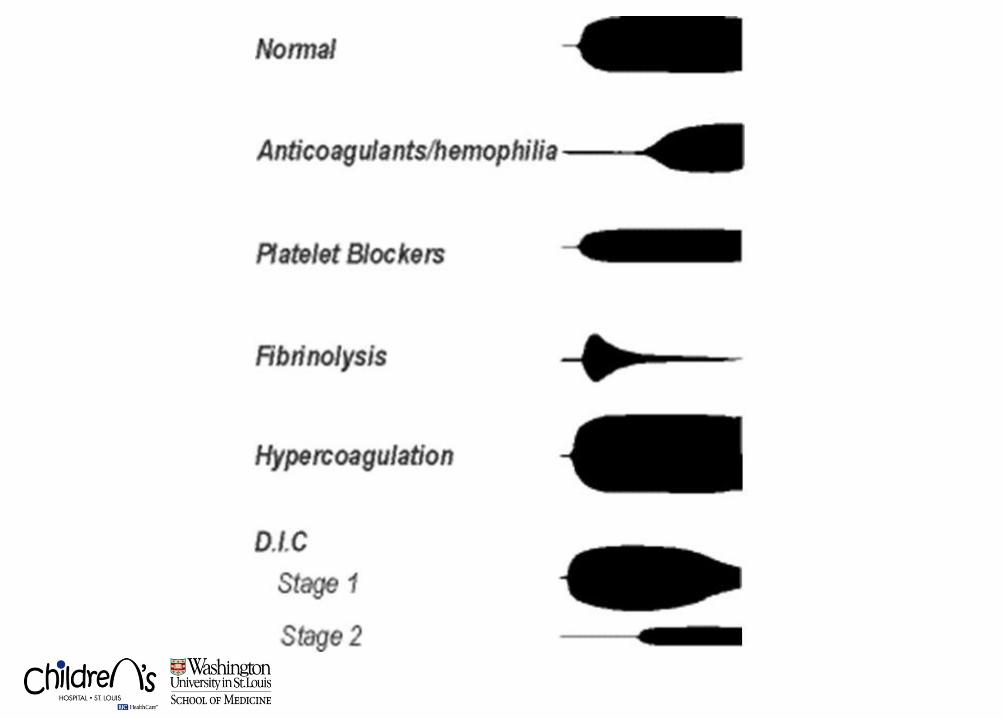
R value or ACT: time to initial clot formation K time – time for tracing to reach 20mm α angle: rate of clot formation Maximum amplitude (MA): clot strength LY30: percent amplitude reduction in 30 minutes
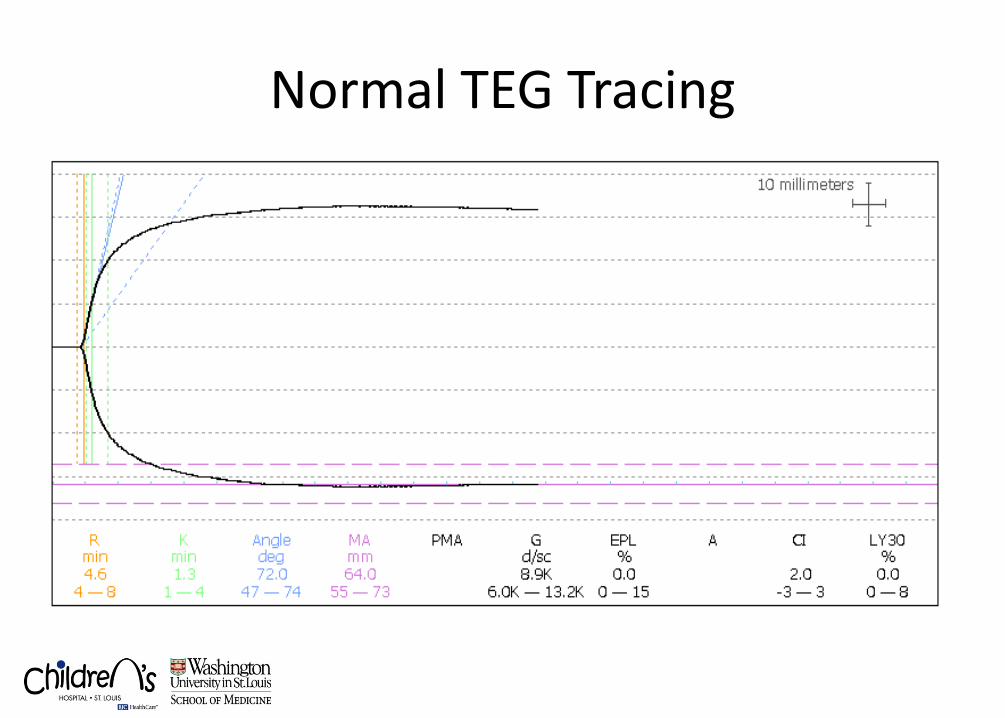
Normal TEG Tracing
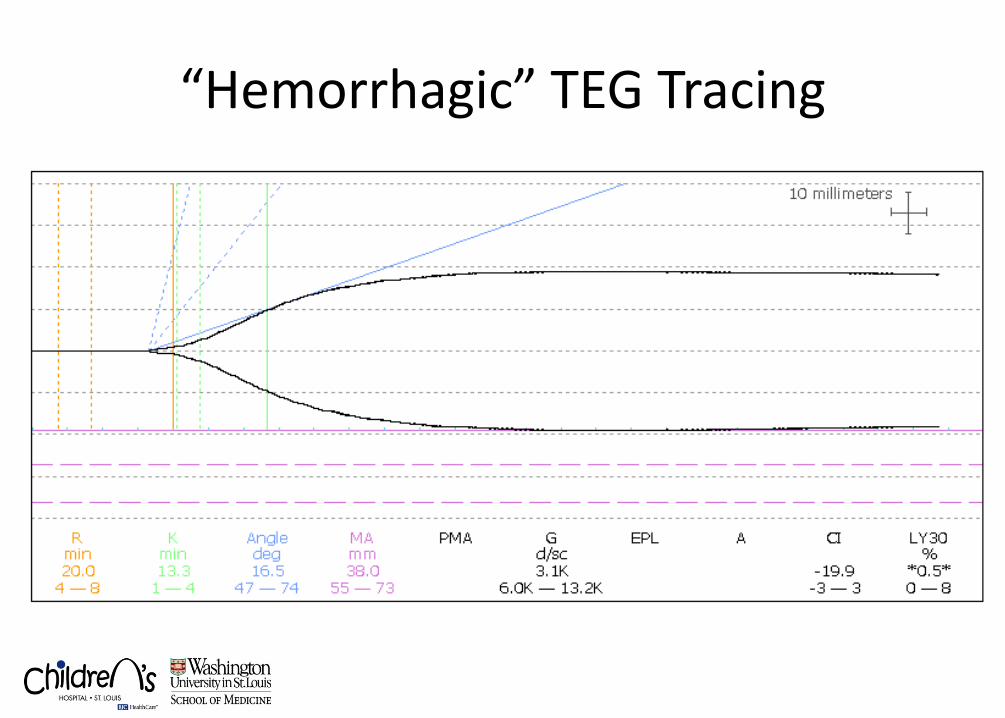
“Hemorrhagic” TEG Tracing
Monitoring Hemostasis
• Need whole blood sample – TEG analysis uses whole blood – CCT and platelet counts use plasma
• Measure interaction of components – TEG analysis reflects interaction – CCT and platelet counts isolate components
• Measure dynamic changes from start to finish of process – TEG analysis reflects dynamic changes – CCT and platelet counts reflect one point in time
TEG in Adult Trauma
• Prospective, observational • N=300 • ATC: PT > 1.2 • Low CA (MA in ROTEM) at 5 min < 35
– Likelihood of PRBC and FFP – Likelihood of MTP
• Prospective, TBI by CT • N= 69; TEG and CCT • Hypocoagulability
– TEG (R<9, α<59, MA<55) – CCT: INR>1.2, PLT<150, PTT>36, fibrinogen<200
• Hypocoagulability as shown by TEG had higher mortality and increased neurosurgical intervention
• Prospective data collection • > 6 units PRBC within 6 hours of admission • Pre-rTEG (N=34) and post-rTEG(N=34)
• Trend towards fewer products in the post-rTEG • Improved “lower” FFP:PRBC in the post-rTEG • Improved mortality 65% to 29%
– Small N, ISS differences
• 20 patients • rTEG, kTEG, CCT • Time to results (MA)
– rTEG: 19.2 ± 3.1 min – kTEG: 29.9 ± 4.3 min – CCT: 34.1 ± 14.5 min
• rTEG is the fastest
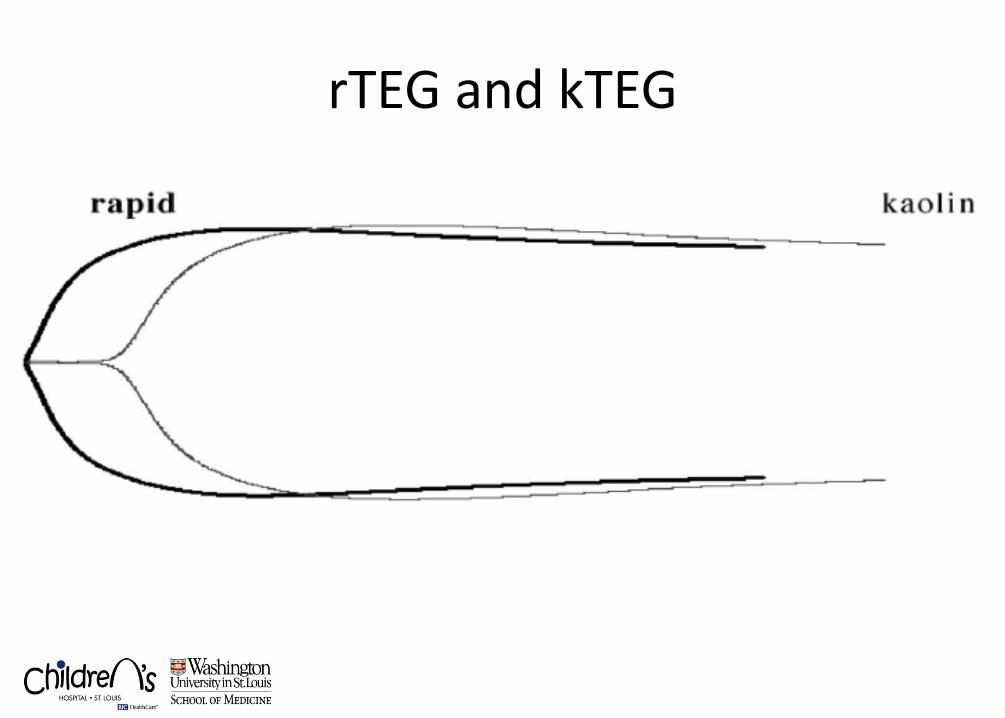
rTEG and kTEG
• Prospective data collection • 10/2009 – 2/2010 • 272 major trauma activations • rTEG: kaolin + tissue factor • CCT: PT, aPTT
• Timing: specimen “clocked-in” to results – Early rTEG values (ACT, K,): 5 min – Late rTEG values (α, MA): 15 min – CCT: 48 min – p < 0.001
• Transfusions – ACT > 128 s (first to result) predicts PRBC, plasma, platelet,
and MTP – ACT < 105 s identifies patients who did not receive a
transfusion
• Prospective, 9/2009-2/2011 • N=1974
• Multiple linear regression controlling for age,
gender, mechanism w-RTS, ISS, and base deficit
• ACT predicted patients with substantial bleeding and RBC transfusion better than PT/PTT or INR (p = 0.03)
• α-angle was superior to fibrinogen for predicting plasma transfusion (p < 0.001)
• mA was superior to platelet count for predicting platelet transfusion (p < 0.001)
Can TEG replace CCTs?
• These correlations improved for transfused, shocked or head injured patients
• The charge for r-TEG ($317) was similar to the five CCTs (>$400)
• Admission conventional coagulation tests can be
replaced with r-TEG
Can TEG replace CCTs?
• TXA: antifibrynolytic agent • Randomized, prospective, blinded, placebo-
controlled in 40 countries, 274 hospitals • Adult trauma pts with “hemorrhage” < 8hrs from
injury w/: SBP < 90, HR > 110 or “at risk” • TXA (N=10060) vs placebo (N=10067) • TXA reduced mortality
TEG in Pediatric Trauma
• 5yM s/p peds v. auto • CHI, pulmonary contusion • Grade IV liver w/ Hepatic artery injury • Damage control laparotomy: packing • Interventional radiology • Serial TEGs, goal directed therapy (w/ factor VII)
rTEG in Pediatric Trauma • Retrospective
• January 1, 2007 – July 31, 2011
• Pediatric “code III” trauma activations
– Age ≤ 14 years • Pediatric level I trauma center • Admission rTEG
Methods • Demographic, clinical, outcome data
– Transfusions (6 hours) – Life saving interventions (6 hours)
• Endotracheal intubation • Bedside surgical procedure (ICPm, CT, CVL) • Emergent surgical procedure
• Statistical analysis – Spearman’s correlation – Multivariate analysis (age, gender, ISS)
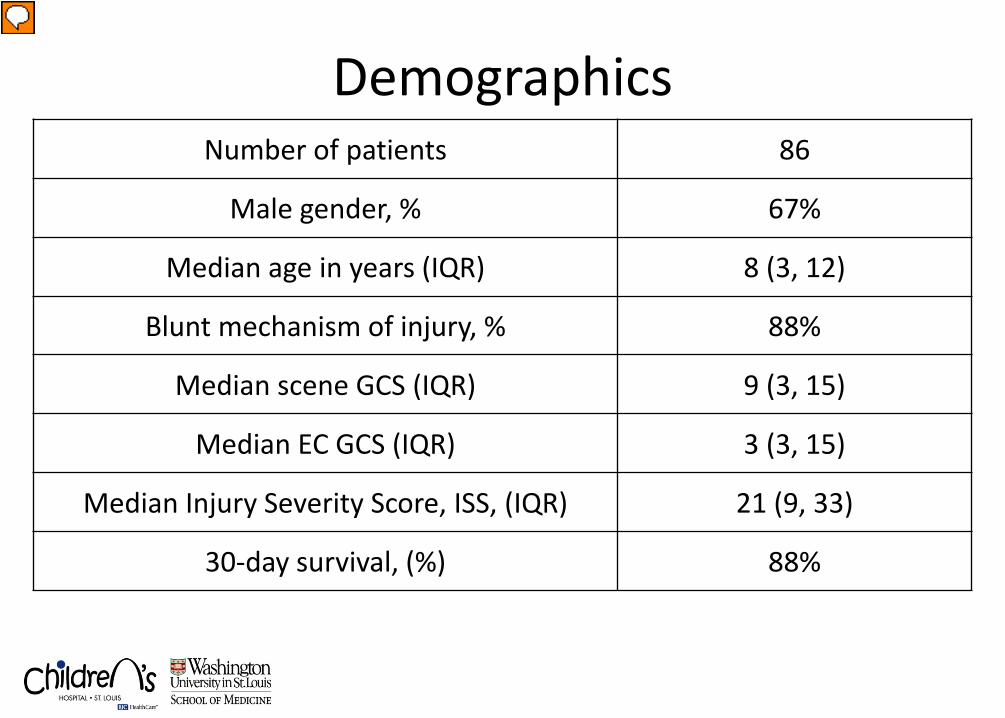
Demographics Number of patients 86
Male gender, % 67%
Median age in years (IQR) 8 (3, 12)
Blunt mechanism of injury, % 88%
Median scene GCS (IQR) 9 (3, 15)
Median EC GCS (IQR) 3 (3, 15)
Median Injury Severity Score, ISS, (IQR) 21 (9, 33)
30-day survival, (%) 88%
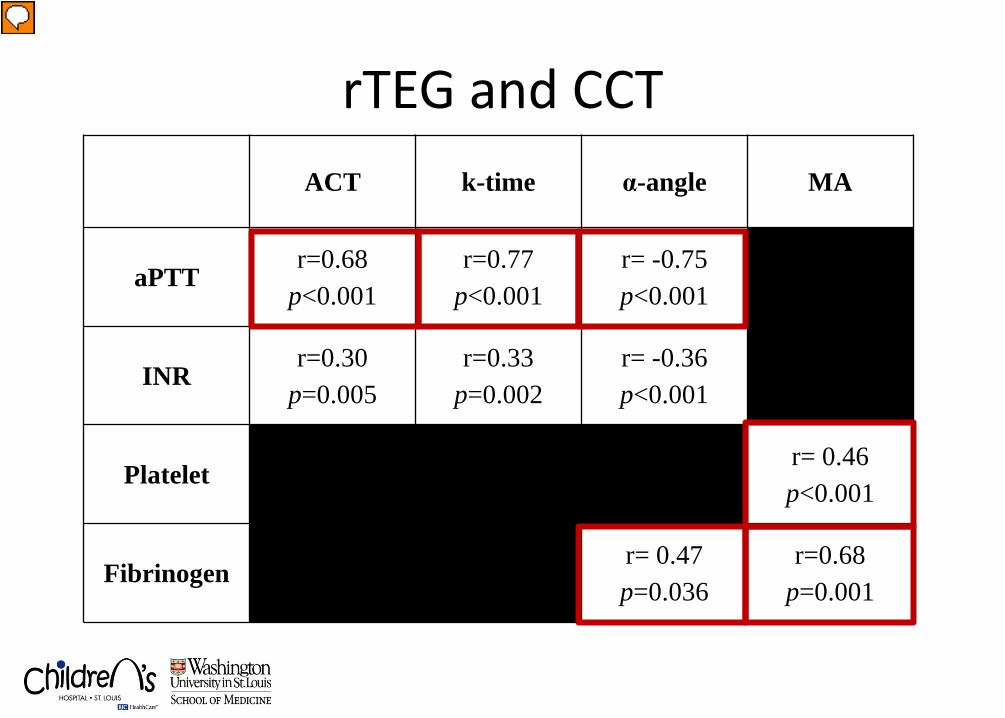
rTEG and CCT ACT k-time α-angle MA
aPTT r=0.68
p<0.001 r=0.77
p<0.001 r= -0.75 p<0.001
INR r=0.30
p=0.005 r=0.33
p=0.002 r= -0.36 p<0.001
Platelet r= 0.46 p<0.001
Fibrinogen r= 0.47 p=0.036
r=0.68 p=0.001
Early Transfusion
• Controlling for age, gender, ISS
• ACT, R, K, α, and MA – “Predict” PRBC and FFP transfusion
Life Saving Interventions
• Only MA predicted life saving interventions – OR 0.84; 95% CI 0.72-0.98; p=0.032
Limitations
• Single center
• Retrospective
• Sample size
Conclusions
• rTEG correlates with conventional coagulation tests
• rTEG predicts transfusion requirements
• rTEG predicts life saving interventions
• “GOAL DIRECTED” HEMOSTATIC RESUSCITATION
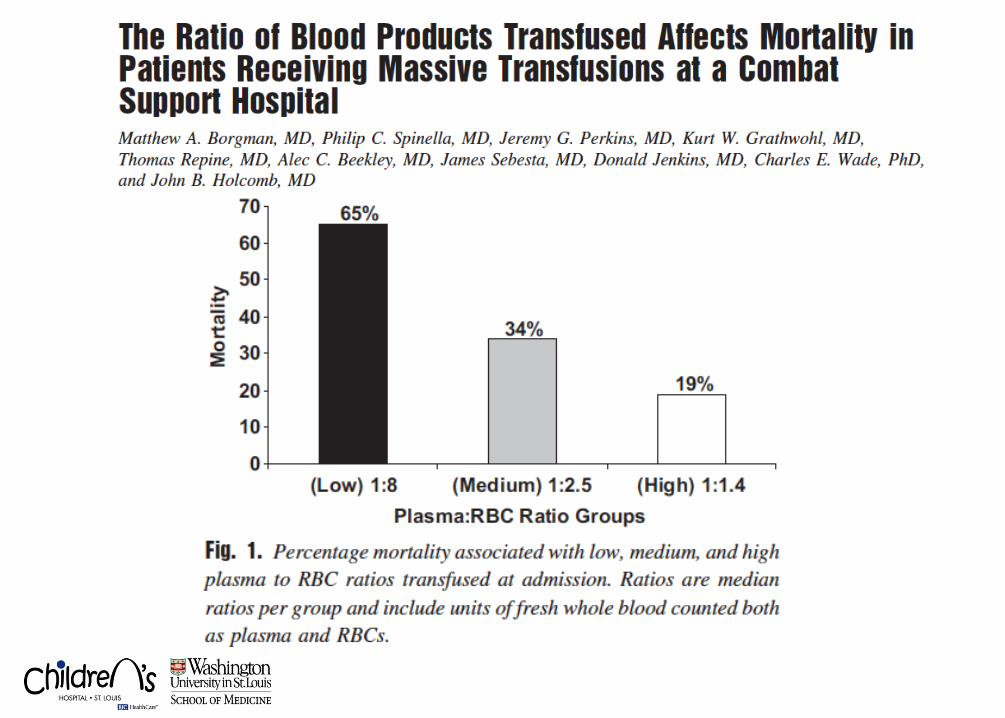
A word (or two) on Massive Transfusion

Here at Children’s . . .
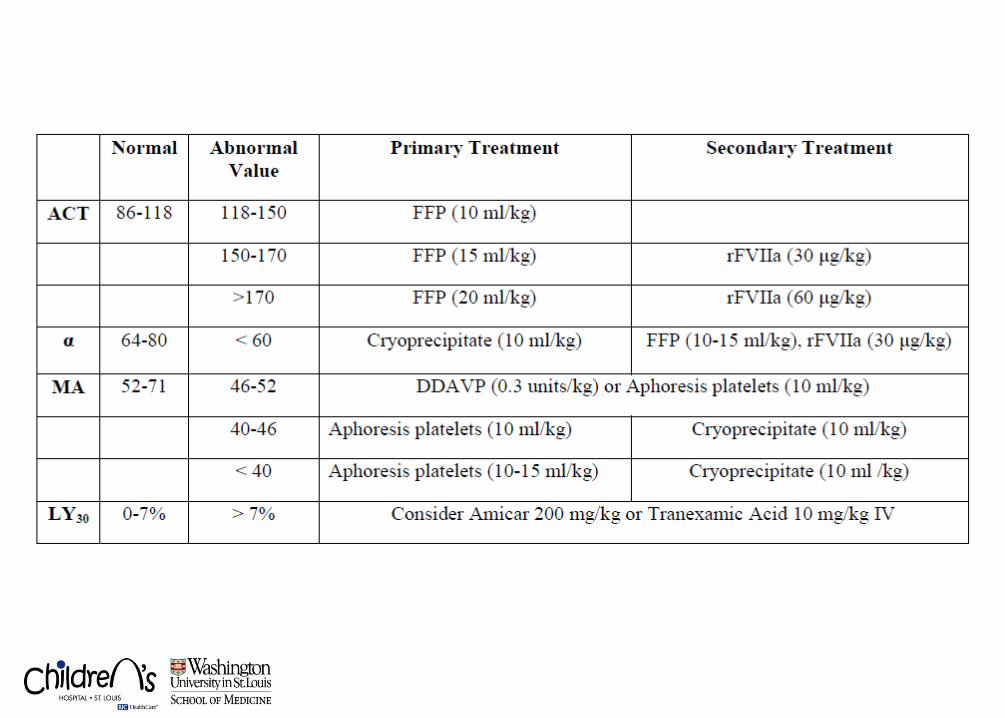
Goal Directed Hemostatic Resuscitation at SLCH
• TEG provides rapid, valuable, “actionable” data on hemostasis and coagulopathy
• The “goal” for goal directed therapy • Massive Transfusion Protocol
• Add TEG to admission labs for patients identified at
risk for bleeding/coagulopathy – GCS/TBI – Penetrating trauma (“t-shirt and boxer shorts”) – Massive transfusion protocol
Thank you
Top Related