








Languages
Pages
Legal


1
Closed loop medication process in a teaching hospital in 9 months
LUIS MARTINEZ ESCOTET, MD
e-huca+ project manager
Hospital Universitario Central de Asturias

Where are we located?
We are at the North of SpainOviedo is Principality of Asturias capital city

HEALTHCARE GEOGRAPHIC DISTRIBUTION
1,075,948 citizens

HEALTHCARE GEOGRAPHIC DISTRIBUTION

HEALTHCARE GEOGRAPHIC DISTRIBUTION

989
2,700 beds
HEALTHCARE GEOGRAPHIC DISTRIBUTION

Hospital Universitario Central de Asturias
(HUCA).
Oviedo, Spain
Tertiary care teaching hospital. 989 beds
7 adult intensive care units (ICU), 1
neonatal ICU, 1 pediatric ICU

GESTION DEL CAMBIO WWW: ayuda de los sistemas de información
WEB 1.0
Data recorder
Not interface
WEB 2.0
P2P
Virtual communities
Information share
WEB 3.0
semantic web
Using metadata and tags
Natural Language
SNOMED y Semantic Search
TIC’S EVOLUTION

• Paper medical records
• Handwritten medication orders
JUNE 2014: hospital move and model change
• Electronic medical records
(EMR)
• Computerized prescriber order
entry (CPOE)
• Clinical decision support
systems (CDSS)
From To

• Illegible handwriting
• Transcription errors
• Lack of traceability
• No access to the full medical history
Advantages & disadvantages
• Real-time access to patient records
• Avoid transcription errors and illegible
issues
• Improve workflow efficiency
• Help prescribers with decision
support systems
• New type of medication errors

11 / XX
GESTION DEL CAMBIO: AJUSTE DE PROCESOS
Adverse events, which represent
between 3% and 5% of all hospital
admissions in the UK, costing the
NHS around 500 million GBP
Hospital errors leading to
preventable adverse events,
typically occur in:
34%4%56%
The cost of care based on memory
Medication management during the
entire cycle
CVLab
Rad
•Computerized
prescriber order
entry (CPOE)
Indications
managemet
Pharmacy
Management
Electronic
medication
administration
In Spain, adverse events accounted for 3.47% of
admissions in large hospitals (ENEA). According to
AHQR (Agency for Healthcare Research and
Quality's) each adverse event linked to medication
costs about € 3,200.
In UE, make a mistake until 60 million in non-electronic
prescriptions per year, (3% of all prescriptions issued)
With a 40% adoption of electronic prescribing, 40% of the errors
could be avoided
British Journal of General Practice.

CPOE+CDSS reduce prescribing errors. However, they have no
effect on medication administration errors. ‘Closed loop’
medication management systems, which combine CPOE+CDSS
with other proven technologies to prevent errors at each step
of the medication pathway, show great promise for preventing
clinical adverse events.
Ranji SR, Rennke S, Wachter RM. Computerised provider order entry combined with clinical
decision support systems to improve medication safety: a narrative review. BMJ Qual Saf
2014;23:773–780.

Closed loop medication process

Pharmacy Inpatient Formulary: 2,070 products
CPOE

2,254 Inpatient Medication Orders (Indications)
CPOE

4,765 Inpatient Medication Order Sentences
CPOE

Search options:
• Drug name
• Brand name
CPOE

Using Tall Man Letters for look-alike drug names to reduce confusion
between similar drug names (following ISMP recommendation)
CPOE

IV Sets: 1,015- Continuous infusion: 752- Intermittent infusion: 263
CPOE

IV sets
• Standardization in critical drugs (amiodarone, dobutamine,…).
• Standardization in IV sets preparation (instructions for nurses).
• Use of low-volume fluids to reduce the % of positive fluid balances.
• Avoid compatibility problems.
CPOE

Medication containing PowerPlans: 362
CPOE

A. Drug powerplans
CPOE

B. Clinical situations powerplans
CPOE

Intravenous fluid therapy powerplans: 27
CPOE

ICU PowerPlans: 77
CPOE

NICU PowerPlans: 69
CPOE

PICU PowerPlans: 29
CPOE
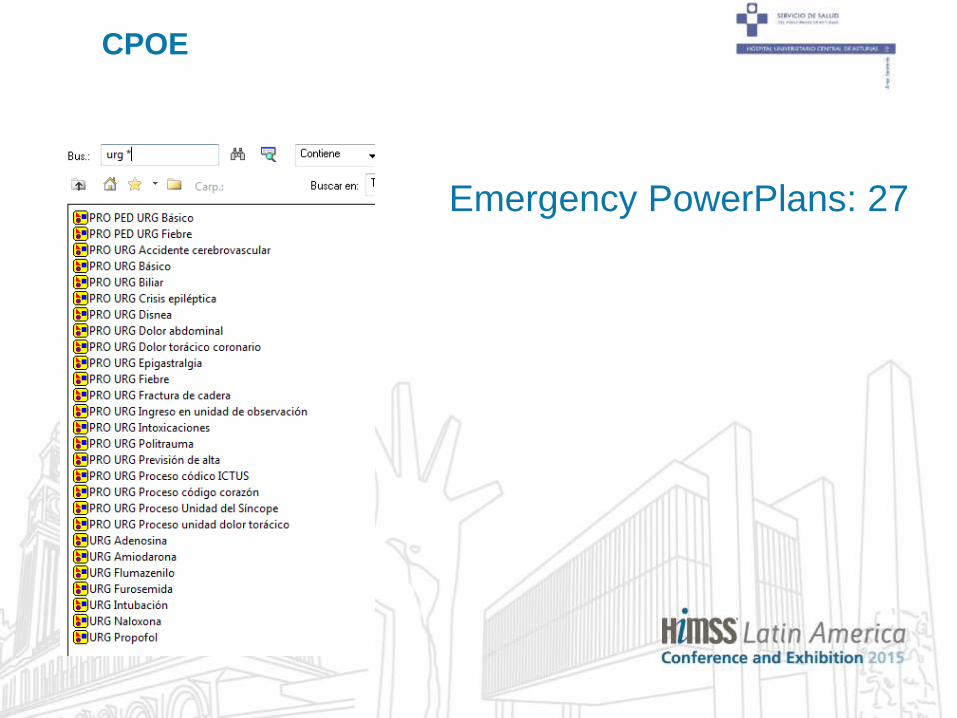
Emergency PowerPlans: 27
CPOE

Anesthesia PowerPlans: 15
CPOE

Cardiology PowerPlans: 23
CPOE

Intoxication management PowerPlans: 13
CPOE & CDSS

Intoxication management PowerPlans
CPOE & CDSS

Therapeutic Interchange Program PowerPlans: 135
Therapeutic alternative for 223 drugs
CPOE & CDSS

Therapeutic Interchange Program PowerPlans
CPOE & CDSS
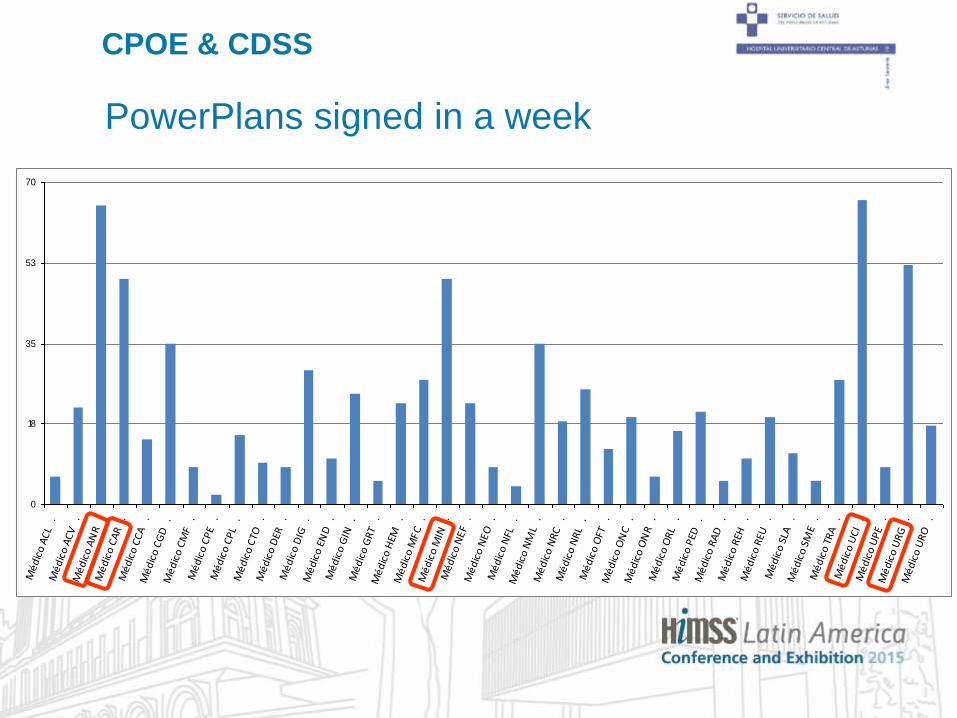
PowerPlans signed in a week
0
18
35
53
70
Mé
dic
o A
CL
.M
éd
ico
AC
V
.M
éd
ico
AN
R
.M
éd
ico
CA
R
.M
éd
ico
CC
A
.M
éd
ico
CG
D
.M
éd
ico
CM
F .
Mé
dic
o C
PE
.M
éd
ico
CP
L .
Mé
dic
o C
TO
.M
éd
ico
DER
.
Mé
dic
o D
IG
.M
éd
ico
EN
D
.M
éd
ico
GIN
.
Mé
dic
o G
RT
.M
éd
ico
HEM
.
Mé
dic
o M
FC
.M
éd
ico
MIN
.
Mé
dic
o N
EF
.M
éd
ico
NE
O
.M
éd
ico
NFL
.
Mé
dic
o N
ML
.M
éd
ico
NR
C
.M
éd
ico
NR
L .
Mé
dic
o O
FT
.M
éd
ico
ON
C .
Mé
dic
o O
NR
.
Mé
dic
o O
RL
.M
éd
ico
PED
.
Mé
dic
o R
AD
.
Mé
dic
o R
EH
.M
éd
ico
REU
.
Mé
dic
o S
LA
.M
éd
ico
SM
E .
Mé
dic
o T
RA
.
Mé
dic
o U
CI
.M
éd
ico
UP
E .
Mé
dic
o U
RG
.
Mé
dic
o U
RO
.
CPOE & CDSS

Indications included in PowerPlans signed in a week
0
250
500
750
1000
Méd
ico
ACL
.M
édic
o AC
V
.M
édic
o AN
R .
Méd
ico
CAR
.M
édic
o CC
A .
Méd
ico
CGD
.
Méd
ico
CMF
.M
édic
o CP
E .
Méd
ico
CPL
.M
édic
o CT
O
.M
édic
o D
ER
.M
édic
o D
IG
.M
édic
o EN
D .
Méd
ico
GIN
.
Méd
ico
GRT
.
Méd
ico
HEM
.
Méd
ico
MFC
.
Méd
ico
MIN
.
Méd
ico
NEF
.
Méd
ico
NEO
.
Méd
ico
NFL
.
Méd
ico
NM
L .
Méd
ico
NRC
.
Méd
ico
NRL
.
Méd
ico
OFT
.
Méd
ico
ON
C .
Méd
ico
ON
R .
Méd
ico
ORL
.
Méd
ico
PED
.
Méd
ico
RAD
.
Méd
ico
REH
.
Méd
ico
REU
.
Méd
ico
SLA
.M
édic
o SM
E .
Méd
ico
TRA
.
Méd
ico
UCI
.
Méd
ico
UPE
.
Méd
ico
URG
.
Méd
ico
URO
.
CPOE & CDSS

Flowsheets and quick indications
CPOE & CDSS

Flowsheets and quick indicationsCPOE & CDSS
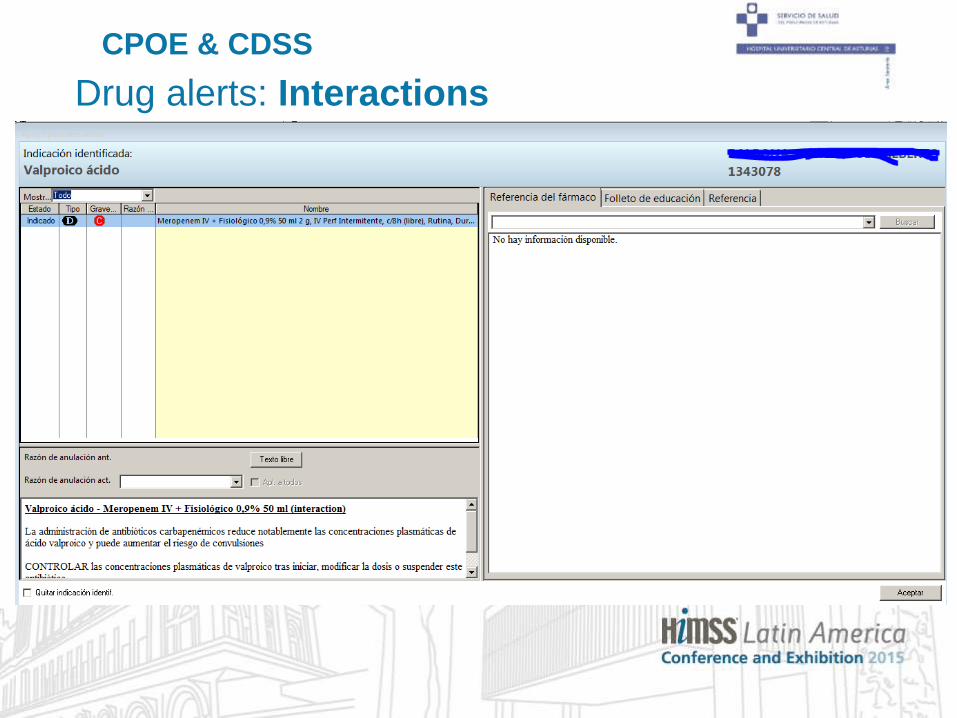
Drug alerts: Interactions
CPOE & CDSS

Drug alerts: Therapeutic Duplications
CPOE & CDSS

Drug alerts: Allergies
CPOE & CDSS

Drug alerts
Fatigue
To avoid alert fatigue:
• Inactivation of non clinically significant drug-drug interactions.
• Daily review of alerts to eliminate non significant ones.
Autovalidation increase
CPOE & CDSS

Other alerts: Dose Range Checking
CPOE & CDSS

Other alerts: using Rules
Intravenous to oral therapy conversion
CPOE & CDSS

Other alerts: using Rules
Intravenous to oral therapy conversion
CPOE & CDSS

Pharmacist Interventions: clinical interventions
CPOE & CDSS

Pharmacist Interventions: reporting Adverse Drug Reactions
CPOE & CDSS

Pharmacist Interventions: compassionate-use
CPOE & CDSS

• Implemented in May 2015
• Developed and used in hematology: conditioning regimens and
GVHD prophylaxis.
• Will be used for Ambulatory Treatment Center indication and
administration: not only chemotherapy.
• Need of onco-hematology treatments standardization.
Oncology CPOE

Oncology CPOE

Oncology CPOE

Oncology CPOE

CERNER integrations at Pharmacy Department
Indication Pharmacist Validation
Dispensing
Inventory management

Safe drug administration: BCMA
Bar-code medication administration
(BCMA)

• Implemented in Child and Adolescent Inpatient
Psychiatric Unit.
• All medications dispensed from Pharmacy
Department with bar-code identification.
• Nurses trained in bar-coding.
• Reduces administration errors.
Safe drug administration: BCMA

HiMSS Analytics Stage 6 - April 2015

Outpatient Pharmacy - Retail
Pharmacy Outpatient Formulary: 432 products

432 Outpatient Medication Prescriptions
Outpatient Pharmacy - Retail

464 Outpatient Medication Prescriptions Sentences
Outpatient Pharmacy - Retail

• Implemented in July 2014.
• 5,000 patients per year (HIV, HCV, HBV, Multiple Esclerosis, Cancer patients).
• Retail integrated with a robotic dispensing system.
Outpatient Pharmacy - Retail


✓ Smart infusion pumps
• Infusion pumps with software that can alert users
to potential errors.
• Library of drugs that provides medication dosing
guidelines, by establishing concentrations, dose
limits, and clinical advisories.
• Indications ready to use the new pumps.

✓ PowerChart Oncology integration with LUG technology
• Drug preparation work sheets on screens
inside biosafety cabinets.
• Voice commands.
• Bar-code technology.
• Computer-assisted gravimetric production
control.
✓ Implement BCMA in the rest of units.
✓ Specific order sentences for weight and age ranges.
✓ Increase dose range checking alerts: new drugs.

✓ Include new alerts, new rules: e.g. antibiotic treatment
duration.
✓ Develop Discern Analytics 2 reports to link indications with
clinical parameters: e.g. erythropoietin and hemoglobin levels.

Conclusions
1. Closed loop medication process improve
patient safety reducing medication errors.
2. Development of the tools we have will lead
our institution to increase patient safety
and reach a high-quality care.

68Thank you for your attention
Top Related