







Languages
Pages
Legal


Challenges of Nocturia in Older People
Dr Chan Ngai Ho Tony
Associate Consultant
Department of Medicine and Geriatrics, Tuen Mun Hospital
Specialist in Geriatric Medicine
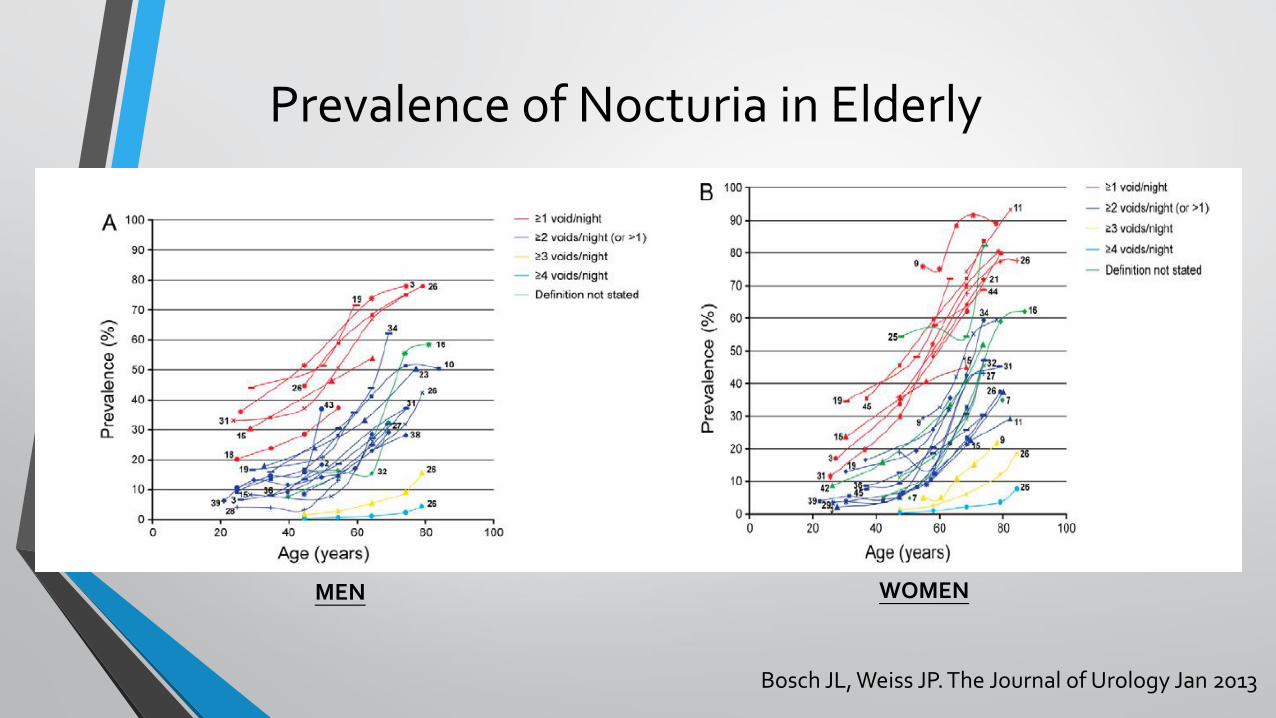
Prevalence of Nocturia in Elderly
MEN WOMEN
Bosch JL, Weiss JP. The Journal of Urology Jan 2013

Prevalence of Nocturia in Elderly
• Telephone survey conducted in HK in 2003
• 22979 subjects
• 10730 (46.7%) reported to have nocturia. The
• 58% of women and 64% of men 51-60 years
• 61% of women and 81% of men over 70 years
Tam PC. The Hong Kong Medical Diary July 2005

Impacts
• Sleep impairment
• ↑ Daytime sleepiness and napping
• Depression
• Fall and fracture
• Carer stress
• Institutionalization
• Death

Age related changes that contribute to nocturia
• ↓ ability to postpone urination
• ↓ bladder compliance
• ↓ functional bladder capacity
• ↓ maximum urinary flow rate
• Detrusor overactivity
• ↑ post-void residual volume
• ↓ nocturnal antidiuretic hormone levels

The challenge of LUTS management in elderly patients
• Managing LUTS in elderly involves balancing the current co-morbidities and concomitant treatments
• Involves multidisciplinary approach
• Choose appropriate and “elder friendly” treatment
Incontinence LUTS

Reasons of Fall in elderly patient with nocturia
• Incontinence -> wet floor
• Urgency -> hurry
• Micturition syncope
• Negative fluid balance in nocturnal polyuria resulted in dizziness/postural hypotension
• Drug induced side effects e.g. delirium, postural dizziness
• Poor sleep
• Reduced mobility/balance
• Reduced dexterity
• Lack of assistance/aids
• Impaired cognition
Comprehensive Geriatric Assessment (CGA)
Multidisciplinary Approach
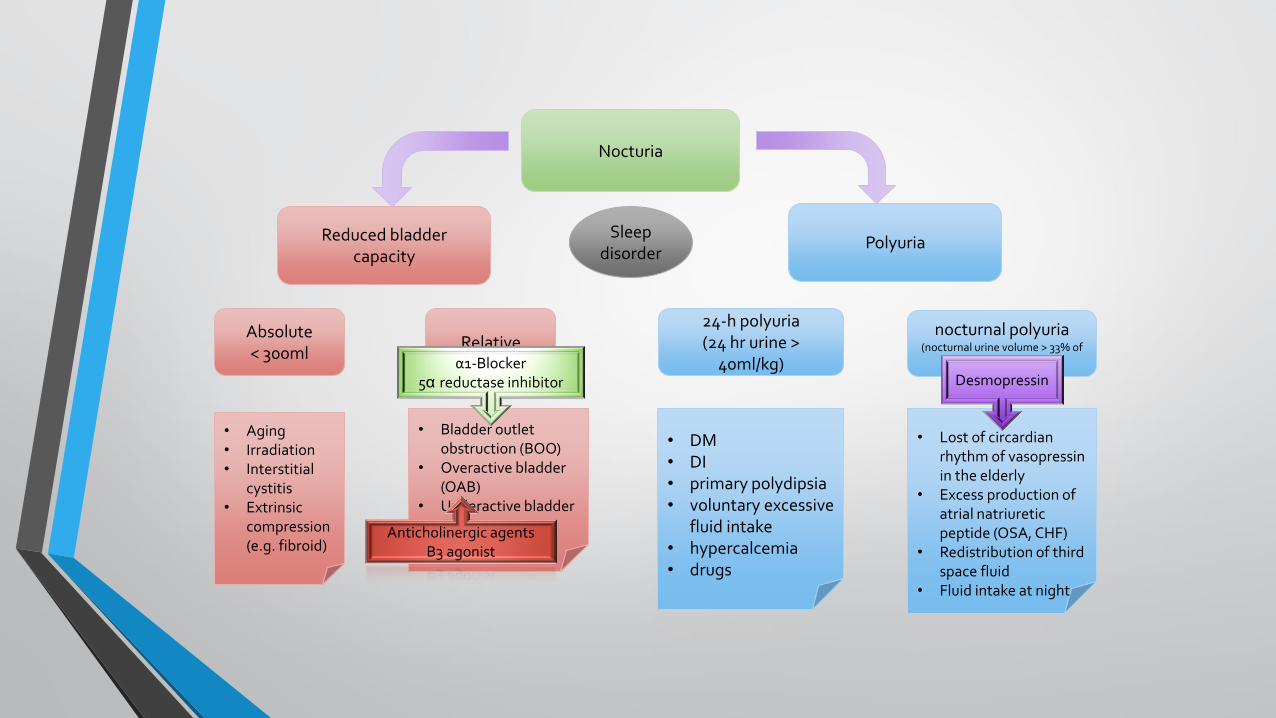
Nocturia
Reduced bladder capacity
Polyuria Sleep
disorder
Absolute < 300ml
Relative
• Aging • Irradiation • Interstitial
cystitis • Extrinsic
compression (e.g. fibroid)
• Bladder outlet obstruction (BOO)
• Overactive bladder (OAB)
• Underactive bladder (UAB)
24-h polyuria (24 hr urine >
40ml/kg)
nocturnal polyuria
(nocturnal urine volume > 33% of total urine volume)
• DM • DI • primary polydipsia • voluntary excessive
fluid intake • hypercalcemia • drugs
• Lost of circardian rhythm of vasopressin in the elderly
• Excess production of atrial natriuretic peptide (OSA, CHF)
• Redistribution of third space fluid
• Fluid intake at night
Desmopressin α1-Blocker
5α reductase inhibitor
Anticholinergic agents Β3 agonist

Frequency-volume chart (bladder diary)
160
150
140 Total urine volume: 1770ml (< 40ml/hr)
Nocturnal urine volume: 620ml (0.35% of total volume)
Max bladder capacity: 320ml
Average voided volume ~150ml
Nocturnal polyuria
Reduced bladder capacity (relative)
M/70 BW 55kg

Continuous Urine Volume Sensor

Treatment
• Non pharmacological treatment
• Treat the concurrent co-morbidities
• Drug review
• Pharmacological treatment

Non pharmacological treatment
• Avoidance of nighttime fluid intake, including alcohol and caffeine
• Afternoon leg elevation -> decrease fluid retention and result in less nighttime urination
• Moderate daytime exercise
• Reducing non-sleep time spent in bed
• Keeping a warm bed to decrease cold-induced diuresis

Concurrent MEDICAL CONDITIONS associated with nocturia
• Stroke
• Dementia
• Parkinsonism
• DM
• CHF
• Obstructive sleep apnoea
• UTI

Medications Influencing Lower urinary tract function
Alcohol Polyuria, frequency, urgency
α-Receptor agonists Urethral constriction and urinary
retention (males)
α-Receptor antagonists Urethral relaxation
ACE inhibitors Cough → SUI
Anticholinergics (antihistamine,
antiparkinsonism agent)
Urinary retention, overflow
incontinence, fecal impaction
Antidepressants, tricyclic Anticholinergic effect,
α-receptor antagonist effect
Medication Class Effect

Medications Influencing Lower urinary tract function (cont)
β-Receptor antagonists Urinary retention
Calcium channel blockers Urinary retention, fecal impaction
Opioids Urinary retention, fecal impaction
Benzodiazepines Sedation, delirium, muscle relaxation
Diuretics Polyuria, frequency, urgency
Cholinesterase inhibitors Urgency, urge incontinence
Neuroleptics Anticholinergic effect, sedation
Medication Class
Effect

Pharmacological treatment
• α1-blocker
• Anticholinergic agents
• β3 agonist
• Desmopressin

α1-Blocker and BPO
• Improve symptoms and increase urinary flow rate by relaxing prostatic and bladder neck smooth muscle through sympathetic activity blockade
α1 receptors ↑ smooth muscle tone and resistance within the gland
α1-blocker
Bladder outlet obstruction

α1-receptor subtypes
Prostate Urethra
Bladder neck
Blood vessels
Bladder
α1A
α1D
α1B
↓ Outflow resistance ↓ Voiding Sx
↓ Bladder overactivity ↓ Storage Sx
↓ Blood pressure Dizziness
Postural hypotension
Blockade
Blockade
Blockade

α1-Blocker
Drug Receptor Selectivity
Non Selective
Prazosin (Minipress) α1A = α1B = α1D
Terazosin (Hytrin) α1B = α1D > α1A
Doxazosin (Cardura) α1A = α1B = α1D
Alfuzosin (Xatral) α1A = α1B = α1D
Selective (α1A)
Tamsulosin (Harnal Ocas) α1A = α1D > α1B
Silodosin α1A > α1D >> α1B
Minimal effect on blood pressure
Minipress
• 1st α1-Blocker • Short acting – requires
dose titration and multiple dosing
• Lack of large randomized controlled trial – not in FDA approval list and guidelines for BPH treatment

Anticholinergic agents
• OAB symptoms relieved by
• inhibition of involuntary bladder contractions
• increased bladder capacity
• Similar efficacy among different anticholinergics
• Less side effects and better tolerability in newer generation (e.g. solifenacin (Vesicare)).
• Treatment can be limited by side effects such as dry eye/mouth, GI effects (e.g, constipation), and CNS effects (e.g. impaired cognition, delirium)
• Contraindications: untreated narrow-angle glaucoma, impaired gastric emptying, hx of urinary retention.

• the first new class of oral therapy for OAB
• Mirabegron (Betmiga)was approved for use in clinical practice in Japan in September 2011
• Approved by FDA in June 2012
• Approved by EMEA in December 2012
• 50mg once daily (25mg once daily in severe renal/moderate liver impairment)
β3-Agonist

Betmiga® (mirabegron) promotes urine storage without affecting bladder voiding
Astellas Pharma Ltd. Betmiga™ (mirabegron) SmPC, January 2013; Takasu T et al. J Pharmacol Exp Ther
2007;321:642-7; Barkin J and Folia C. Can J Urol 2012;19(Suppl 1):49-53; Tyagi P et al. Expert Opin Drug Saf
2011;10:287-94
Activation β3-AR by mirabegron • detrusor relaxation & promotes urine storage
• increased bladder capacity and
• increased duration between voids
Noradrenaline
β3-AR
Acetylcholine
Muscarinic receptors
Mirabegron: • no effect on parasympathetic stimulation of
detrusor contraction and bladder emptying
• may reduce the risk of acute urinary retention compared with AM agents
Betmiga® (mirabegron)
Urine storage Bladder voiding

Mirabegron (BETMIGA)
First selective β3-AR agonist, EMEA approved December, 2012
• EAU guideline urinary incontinence 2018
• 6th International Consultation on Incontinence 2016
Level of evidence Grade of recommendation
β3-AR agonists 1 A
EAU guidelines on urinary incontinence 2018
ICI book 2016, Paul A et al.
Strength rating
β3-AR agonists Strong
If an antimuscarinic treatment proves ineffective, consider dose escalation or offering an alternative antimuscarinic formulation, or mirabegron, or a combination
Strong

Betmiga® - SCORPIO: Most common TEAEs (≥2% in any treatment group)1
• In SCORPIO, rates of drug discontinuation due to TEAEs were low and comparable in the active groups (<5%)1
For the full list of adverse events refer to the SmPC.2
Tolterodine ER 4mg was included as an active control therefore direct statistical comparisons cannot be made between mirabegron and tolterodine ER 4mg.
Table adapted from Khullar et al., 2013.1
Data not shown for the unlicensed 100mg dose of Mirabegron. TEAEs, treatment-emergent adverse events.
1. Khullar V et al. Eur Urol 2013;63(2):283–295.
2. Betmiga Summary of Product Characteristics, December 2012.
Incidence of most common (≥2%) TEAEs1
Adverse events %
Placebo (n=494)
Mirabegron 50mg (n=493)
Tolterodine ER 4mg active control (n=495)
Dry mouth 2.6% 2.8% 10.1%
Constipation 1.4% 1.6% 2.0%
Hypertension 7.7% 5.9% 8.1%
Nasopharyngitis 1.6% 2.8% 2.8%
Headache 2.8% 3.7% 3.6%
Urinary tract infection 1.4% 1.4% 2.0%

Dementia and OAB/Urge incontinence
Dementia
OAB
Cholinesterase inhibitor (CEI)
Anticholinergic

• High quality data to guide the choice of pharmacological agent in those with dementia are lacking.
• Oxybutynin has been shown to have significant adverse cognitive effects.
• Neither age, frailty, nor dementia should be considered a barrier to pharmacological management, but consideration should be given to the total anticholinergic load.
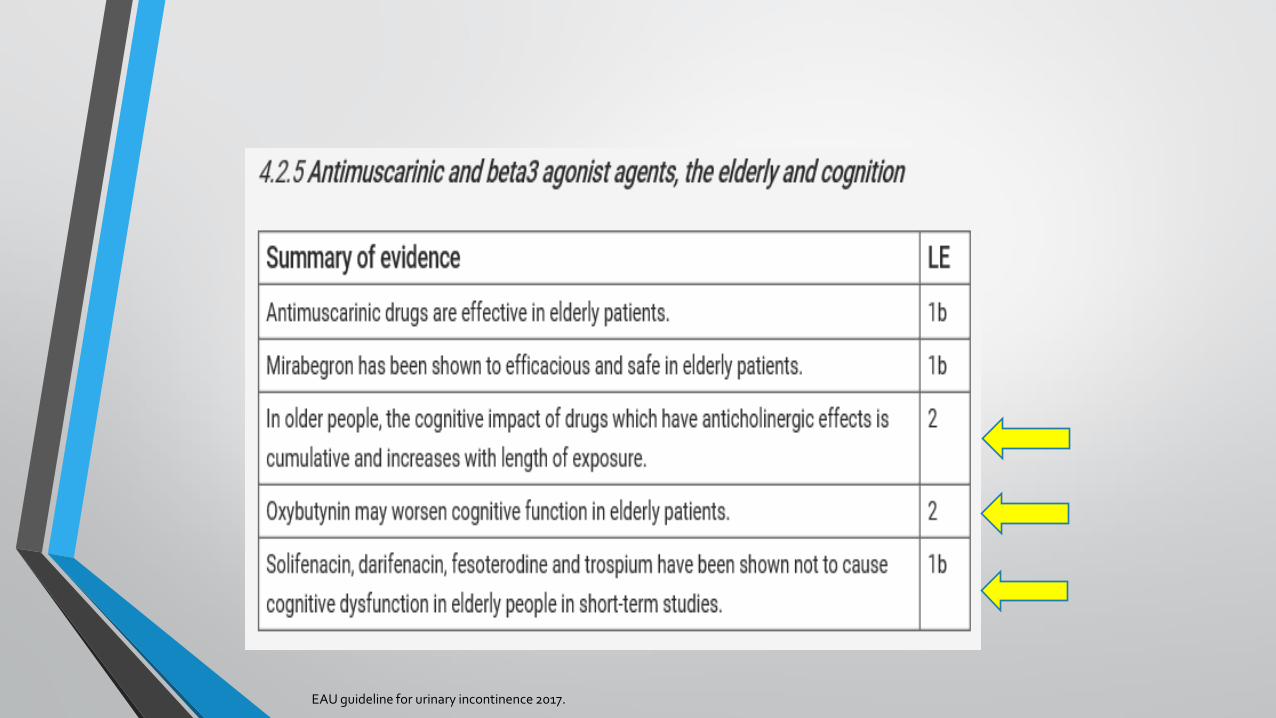
EAU guideline for urinary incontinence 2017.

EAU guideline for urinary incontinence 2017.
EAU – Urinary incontinence guideline

Desmopressin (DDAVP)
• Synthetic analogue of the human hormone vasopressin
• Increases reabsorption of water, concentrating urine and decreasing urine production
• Administered by oral tablets, sublingual route
• Efficacy is well-established in multiple well-designed studies, including several randomised, placebo-controlled trials
• The International Consultation on Incontinence (ICI) (2008) renewed the recommendation for desmopressin as the only treatment for nocturnal polyuria (Grade A, Level 1)

Desmopression (DDAVP) – oral form
• Initiate at low dose (0.1 mg/day – before sleeping)
• Increase dose weekly until maximal efficacy reached
• Maximum recommended dose: 0.2 mg/day
• Patients should avoid drinking fluids 1 hour before and 8 hours after administration
• In patients ≥ 65 years, desmopressin should be avoided if serum sodium concentration below normal
• In patients ≥ 65 years, measure serum sodium at day 3 and 7, and 1 month. If all readings normal, then monitor every 3–6 months

Desmopression (DDAVP)
• Side effects: Fluid retention and hyponatremia
• Contraindications: liver cirrhosis, renal failure, or congestive heart failure
• FDA cautions against its use in patients over 65 years


• Hyponatremia incidence was 4.4% • 2 patients had hyponatremia 120mml/l and 127 mmol/l (aged 73 and 76) • 1 patient had weight gain, aged 73 • All patients recovered by stopping medication.
Desmopressin orally disintegrating tablet (ODT)
• Sublingual use
• 25mcg
• Nocdurna - approved in the EU in May 2016 for the symptomatic treatment of nocturia due to idiopathic nocturnal polyuria in adults.



• a meta-analysis of data from three clinical trials of desmopressin in nocturia
• Patients received placebo or desmopressin orally disintegrating tablet (ODT; 10–100 lg)
• The incidence of serum sodium <130 mmol/L was recorded by age, sex and dose



Take home messages
• The cause of nocturia in older people is multi-factorial.
• Concurrent comorbidities, functional and cognitive problem, polypharmacy, frailty, etc. may predispose and increase the risk of nocturia in older people.
• “Individualized Care”, “Elder-Friendly” and “Multidisciplinary Approach” are essential in treating older people with nocturia.

Thank you
Top Related