


![anti anginal drugs · Microsoft PowerPoint - anti anginal drugs [Compatibility Mode] Author: venkatesan Created Date: 1/27/2020 11:15:06 AM ...](https://static.fdocuments.net/doc/165x107/5f3de8de62847b2a0c1b25eb/anti-anginal-microsoft-powerpoint-anti-anginal-drugs-compatibility-mode-author.jpg)




Languages
Pages
Legal

CALCIUM CHANNEL BLOCKERS
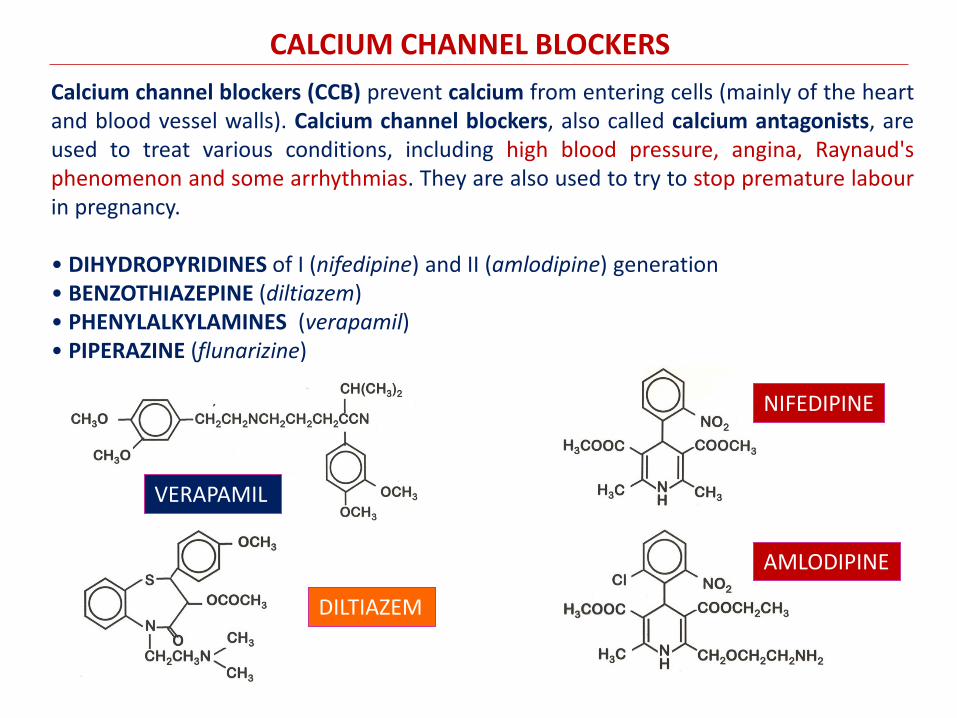
Calcium channel blockers (CCB) prevent calcium from entering cells (mainly of the heart and blood vessel walls). Calcium channel blockers, also called calcium antagonists, are used to treat various conditions, including high blood pressure, angina, Raynaud's phenomenon and some arrhythmias. They are also used to try to stop premature labour in pregnancy. • DIHYDROPYRIDINES of I (nifedipine) and II (amlodipine) generation • BENZOTHIAZEPINE (diltiazem) • PHENYLALKYLAMINES (verapamil) • PIPERAZINE (flunarizine)
VERAPAMIL
NIFEDIPINE
DILTIAZEM
AMLODIPINE

Voltage-operated Ca++ CHANNELS (VOCCs)
TYPE VOLTAGE MOST OFTEN FOUND IN
L-TYPE CALCIUM CHANNEL ("LONG-LASTING" AKA "DHP
RECEPTOR")
HVA (high voltage
activated)
Skeletal muscle, smooth muscle, bone (osteoblasts), ventricular myocytes (responsible for prolonged action potential in cardiac cell; also termed DHP receptors), dendrites and dendritic spines of cortical neurones L-Type channel blockers are used as antihypertensive and antiarrhythmic drugs
P-TYPE CALCIUM CHANNEL ("PURKINJE") /Q-TYPE
CALCIUM CHANNEL
HVA (high voltage
activated)
Purkinje neurons in the cerebellum / Cerebellar granule cells
N-TYPE CALCIUM CHANNEL ("NEURAL"/"NON-L")
HVA (high-voltage-
activated)
Throughout the brain and peripheral nervous system.
R-TYPE CALCIUM CHANNEL ("RESIDUAL")
intermediate-voltage-activated
Cerebellar granule cells, other neurons
T-TYPE CALCIUM CHANNEL ("TRANSIENT")
low-voltage-activated
neurons, cells that have pacemaker activity, bone (osteocytes) T-Type channel blockers are used as antiepileptic and neuropathic painkiller drugs

L-TYPE CALCIUM CHANNEL 1 SUBUNIT
PHENYLALKYLAMINE
BENZOTHIAZEPINE
DIHYDROPYRIDINE
PHENYLALKYILAMINE bind to intracellular IV6 segment.
DIHYDROPYRIDINE bind to extracellular site on III5-III6 loop
BENZOTHIAZEPINE bind in between III and IV transmembrane segment
IMPLICATIONS
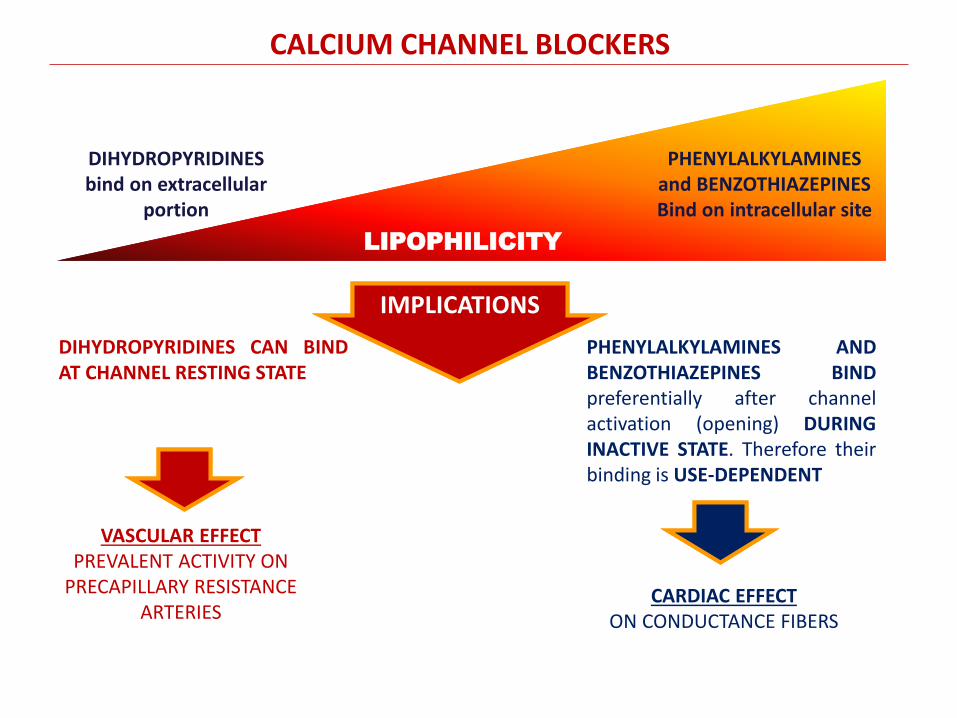
IMPLICATIONS DIHYDROPYRIDINES CAN BIND
AT CHANNEL RESTING STATE PHENYLALKYLAMINES AND BENZOTHIAZEPINES BIND preferentially after channel activation (opening) DURING INACTIVE STATE. Therefore their binding is USE-DEPENDENT
DIHYDROPYRIDINES bind on extracellular
portion
PHENYLALKYLAMINES and BENZOTHIAZEPINES Bind on intracellular site
LIPOPHILICITY
VASCULAR EFFECT PREVALENT ACTIVITY ON
PRECAPILLARY RESISTANCE ARTERIES
CARDIAC EFFECT ON CONDUCTANCE FIBERS
CALCIUM CHANNEL BLOCKERS

• amlodipine (NORVASC, ANTACAL, MONOPINA) 5mg & 10mg
• felodipine (FELODAY, PLENDIL, PREVEX) 5mg & 10mg
• barnidipine (LIBRADIN, OSIPINE, VASEXTEN) 10mg & 20mg
• isradipine (LOMIR SRO, CLIVOTEN, ESRADIN) 5mg
• lacidipine (LACIPIL, LACIREX) 4mg & 6mg
• lercanidipine (ZANEDIP, LERCADIP, CARDIOVASC) 10mg & 20mg
• manidipine (IPERTEN, VASCOMAN) 20mg
• nicardipine (NICARDAL, NIMICOR, PERDIPINA, ecc.) 20mg & 40mg
• nifedipine (ADALAT, NIFEDICOR, generico) 20mg, 30mg, 60mg «CRONO»
• nisoldipine (SYSCOR) 10mg
• nitrendipine (BAYPRESS, DEITEN) 20mg
• dilthiazem (TILDIEM, generic)
• verapamil (ISOPTIN, generic)
• gallopamil (PROCORUM, ALGOCOR) 50mg & 100mg
CALCIUM CHANNEL BLOCKERS - NOMENCLATURE

DOSE NIFEDIPINE VERAPAMIL
Oral Intravenous
Plasma concentrations
Protein binding
Liver metabolism 1° passage
Half-life (t1/2)
10-40 mg 8 h-1 5-15 mg kg-1
10-75 ng ml-1
95
40-60 %
3-5 h
80-160 mg 8 h-1 100-200 mg kg-1
50-250 ng ml-1
90
75-85 %
5-10 h
MAIN PK FEATURES OF CCBs
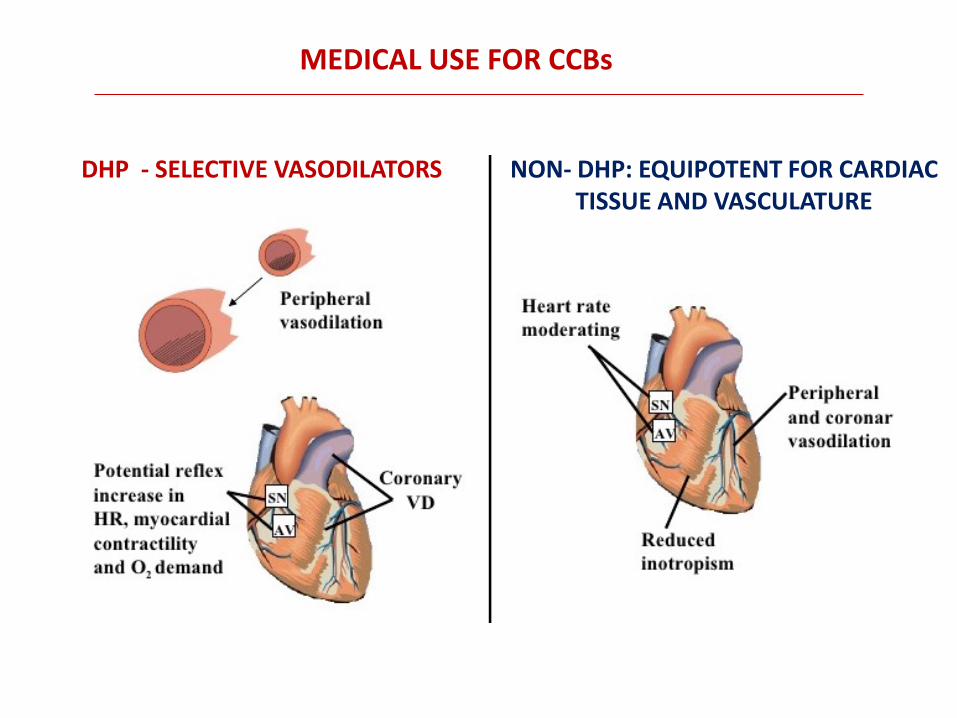
MEDICAL USE FOR CCBs
DHP - SELECTIVE VASODILATORS NON- DHP: EQUIPOTENT FOR CARDIAC TISSUE AND VASCULATURE

• HYPERTENSION
By causing vascular smooth muscle relaxation, CCBs (DHP) decrease systemic vascular resistance, which lowers arterial blood pressure. These drugs primarily affect arterial resistance vessels, with only minimal effects on venous capacitance vessels.
MEDICAL USE FOR CCBs
Reducing peripheral vascular resistance, however, is accompanied by compensatory mechanism increasing heart rate, inotropic stimulation, and renin release. These common effects of DHP, especially at the beginning of treatment, tend to reduce during the first two weeks for baroreceptor adjustments

• ANGINA
The anti-anginal effects of CCBs are derived from their vasodilator and cardiodepressant actions. Systemic vasodilation reduces arterial pressure, which reduces ventricular afterload (wall stress) thereby decreasing oxygen demand.
MEDICAL USE FOR CCBs
The more cardioselective CCBs (verapamil and diltiazem) decrease heart rate and contractility, which leads to a reduction in myocardial oxygen demand, which makes them excellent antianginal drugs. CCBs can also dilate coronary arteries and prevent or reverse coronary vasospasm (as occurs in Printzmetal's variant angina), thereby increasing oxygen supply to the myocardium.
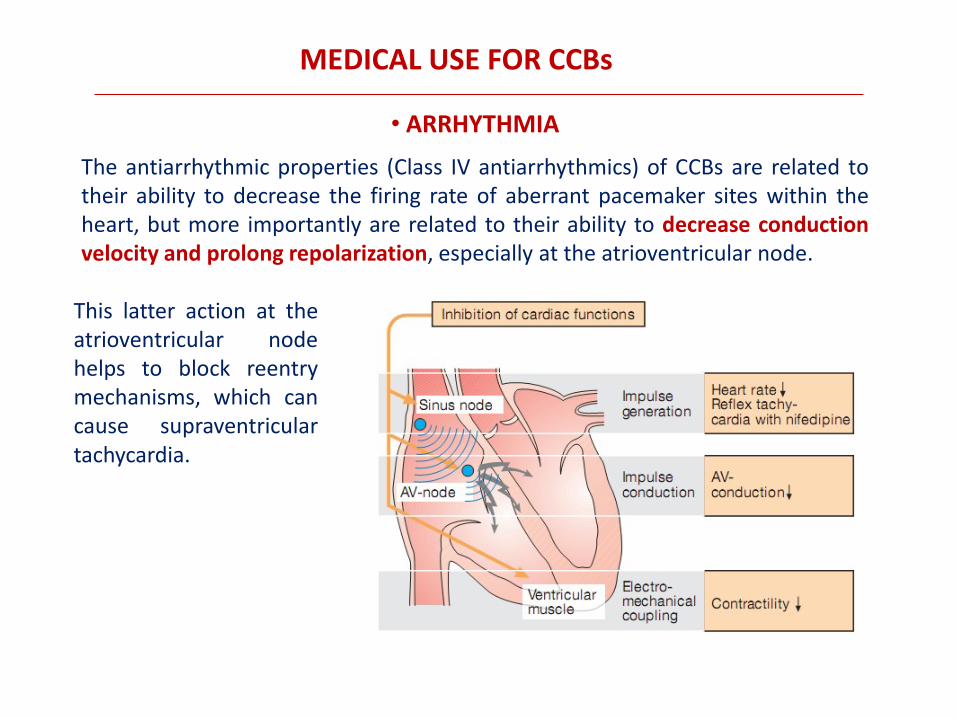
• ARRHYTHMIA
The antiarrhythmic properties (Class IV antiarrhythmics) of CCBs are related to their ability to decrease the firing rate of aberrant pacemaker sites within the heart, but more importantly are related to their ability to decrease conduction velocity and prolong repolarization, especially at the atrioventricular node.
MEDICAL USE FOR CCBs
This latter action at the atrioventricular node helps to block reentry mechanisms, which can cause supraventricular tachycardia.

• CEREBRAL VASOSPASM Some CCBs may be used to treat migraine headaches or vertigo. They may also prevent cerebral ischemic damage from reactive vasospasm after subarachnoid hemorrhage by dilating cerebral vessels and increasing blood flow.
MEDICAL USE FOR CCBs

MOST COMMON SIDE EFFECTS OF CCBS
• DIHYDROPIRYDINE - Nifedipine (18%)
– Distal edema
– Headache
– Vertigo
– Fatigue, dizziness
– Postural hypotension/ reflex tachycardia
– Palpitation
– Aggravamento dell’angina
• PHENYLALKYLAMINE - Verapamil (10%)
– Constipation
– AV Block, bradicardia
– Insufficienza cardiaca
– Vertigo, headache, dizziness
• BENZOTHIAZEPINE - Diltiazem (5%)
– AV Block, bradycardia
– Vertigo, dizziness
– Rashes
– Headache

ATP-sensitive K+-channels OPENERS
These drugs hyperpolarize the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium. With less calcium available to combine with calmodulin, there is less activation of myosin light chain kinase and phosphorylation of myosin light chains. This leads to relaxation and vasodilation. Because small arteries and arterioles normally have a high degree of smooth muscle tone, these drugs are particular effective in dilating these resistance vessels, decreasing systemic vascular resistance, and lowering arterial pressure. The fall in arterial pressure leads to reflex cardiac stimulation (baroreceptor-mediated tachycardia).
DIAZOXIDE MINOXIDIL
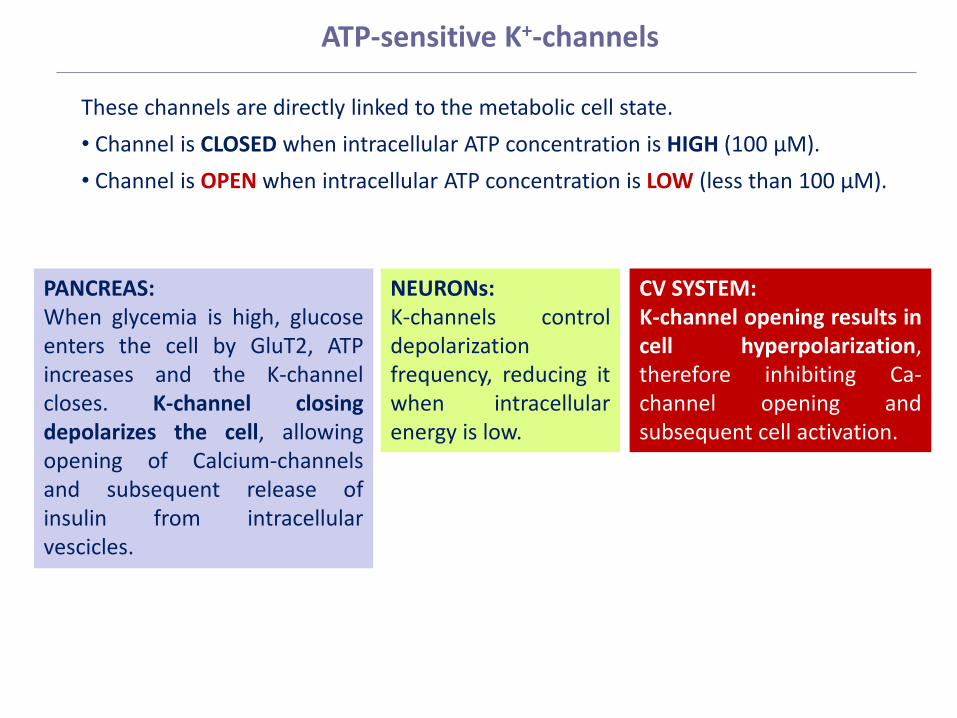
These channels are directly linked to the metabolic cell state.
• Channel is CLOSED when intracellular ATP concentration is HIGH (100 µM).
• Channel is OPEN when intracellular ATP concentration is LOW (less than 100 µM).
NEURONs: K-channels control depolarization frequency, reducing it when intracellular energy is low.
PANCREAS: When glycemia is high, glucose enters the cell by GluT2, ATP increases and the K-channel closes. K-channel closing depolarizes the cell, allowing opening of Calcium-channels and subsequent release of insulin from intracellular vescicles.
CV SYSTEM: K-channel opening results in cell hyperpolarization, therefore inhibiting Ca-channel opening and subsequent cell activation.
ATP-sensitive K+-channels
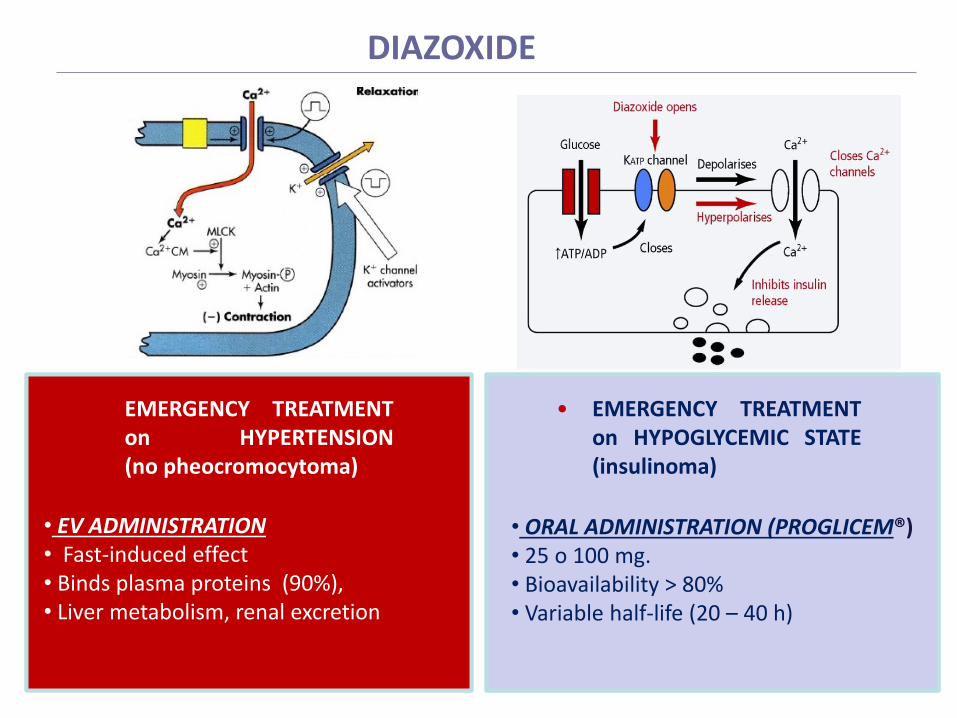
DIAZOXIDE
• EMERGENCY TREATMENT on HYPERTENSION (no pheocromocytoma)
• EV ADMINISTRATION • Fast-induced effect • Binds plasma proteins (90%), • Liver metabolism, renal excretion
• EMERGENCY TREATMENT on HYPOGLYCEMIC STATE (insulinoma)
• ORAL ADMINISTRATION (PROGLICEM®) • 25 o 100 mg. • Bioavailability > 80% • Variable half-life (20 – 40 h)
MINOXIDIL
Common side effects to minoxidil include headaches, flushing and reflex tachycardia. The potent vasodilator actions of minoxidil can lead to fluid retention and edema formation. Reflex cardiac stimulation can precipitate angina in patients with coronary artery disease. Minoxidil produces T wave changes in a high percentage (~60%) of patients under chronic treatment. One of the most noted side effects of minoxidil is hypertrichosis, a thickening and enhanced pigmentation of body hair, and therefore this drug is more commonly used for treating baldness.

ENDOTHELIN-1 RECEPTOR ANTAGONISTS
• Endothelin-1 (ET-1) is produced mainly by vascular endothelial cells and exerts both vasoconstriction and vascular smooth muscle cells proliferation. • ET-1 biological activity depends on activation of ETA and ETB receptor subtypes. • ETA receptors are prevalently expressed on vascular smooth muscle cells, and are particularly important on pulmunar arteries. • ETB receptors sare ubiquitously expressed on endothelial cells and their activation results in increased release of NO and prostacyclin (with subsequent vasodilatant effects). Their role on pulmunary arteries includes also clearing of circulating ET-1.

ENDOTHELIN-1 EFFECTS, RECEPTORS and ANTAGONISTS

Bosentan is a competitive antagonist of ET-A and ET-B receptors, with a slightly higher affinity for ET-A than ET-B. Bosentan is indicated mainly for the treatment of pulmonary hypertension. In Europe, bosentan is also approved for reducing the number of new digital ulcers in patients with systemic sclerosis . Due to potential hepatotoxicity and onset of anemia, bosentan requires a monthly monitoring of liver function and hematocrit. Due to a pharmacokinetic interaction, hormone-based contraception is not possible in women taking bosentan, therefore other highly reliable forms of contraception should be used instead. Bosentan is contraindicated in pregnancy because of its teratogenicity
BOSENTAN
ENDOTHELIN-1 RECEPTOR BLOCKERS
are selective ETA receptor antagonists with similar medical use and comparable side effects (including teratogenicity)
SITAXENTAN, AMBRISENTAN, ATRASENTAN
Top Related