







Languages
Pages
Legal


Breastfeeding, Fertility and the Life-Cycle
Miriam Labbok, MD, MPH, FABMSenior Advisor, Infant and Young Child Feeding and CareUNICEF NYHQ

Areas to be Discussed:1. What is a Life-cycle approach to Health? 2. How does Delaying the First Birth and
Increasing Birth Intervals contribute to Nutrition?
3. How does Breastfeeding contribute to Birth Spacing?
4. How does this effect us today, and what should be considered in terms of policy and programmes?
References: Labbok MH. Effects of Breastfeeding on the Mother. Ped Clin of
North America, 2001 Feb; 48(1)143-5 Optimal Birthspacing Saves Lives
http://www.rhcatalyst.org/site/DocServer/Catalyst_OBSI_Overview_Final.pdf?docID=341

Intergenerational Life-cycle Approach: Programme Entry Points
Adolescent and School Programmes:DELAY OF FIRST BIRTH
EPI, FP, All contacts:AT LEAST 3 YRS. SPACING
WITH EXCLUSIVE BREASTFEEDING, CONTINUED BREASTFEEDINGAND FREQUENT QUALITY CFs
Mother
Child
Birth
ANC: IRON/NUTRITION SAFE DELIVERY
FEEDING SPACING

Intergenerational Life-cycle Approach: Prolonging periods of the lifecycle to allow for improved
outcomes
Child’s Path
Maternal Path
Pregnancy
Complications/Abortion
Puberty
Birth
Paternal Path
Delay First UnionBreastfeedUse Contraception
Unable to prolong, extra intervention necessary
Breastfeeding is the Heartbeat of Intergenerational Health
Logo, Breastfeeding Division, IRH
Survival:Oral Rehydration
Growthand Development
Immunization
Women’s Health, Survival, and Reproductive Readiness
Nutrition
Birth Spacing and Fertility
Reduced Cancersand Chronic Diseases
Breastfeeding supports:

What is the importance of Maternal Nutrition?
Poor nutritional
status
Increased death from bleeding if already anemic
Increased risk of
SGA/LBW
Decreased stores for fetus and for breastfeeding
Reduced Growthand Productivity
Small statureat age of
Reproduction

2. How does Delaying the First Birth and Increasing Birth Intervals
contribute to Nutrition?

0.60
0.80
1.00
1.20
1.40
1.60
<17 18-23 24-29 30-35 36-41 42-47 48-53 54-59 60+
Duration of Preceding Birth Interval (months)
Ad
j. R
elat
ive
Od
ds
Rat
io
Small Size at Birth
Low Birth Weight
Length of the Birth Interval is Correlated with Small Size and Low Weight at Birth, controlled for many variables(Also, Mother’s Age and Nutritional Status, are associated with SGA/LBW)
It is good to be born three years after your sib!
Safest

0.4
0.6
0.8
1.0
1.2
1.4
1.6
<1718
-23
24-2
9
30-3
5
36-4
1
42-4
7
48-5
3
54-5
960
+
Length of Preceding Birth Interval (months)
Ad
j. R
elat
ive
Od
ds
Rat
io
Stunting
Underweight
Length of the Birth Interval is Correlated with Stunting and Underweight, controlled for many variables
It is good to be the youngest child for as long as possible!
Safest


0 20 40 60 80 100
Highest Risk of Under Five Mortality
Higest Risk of Infant Mortality
Highest Risk of Perinatal Mortality
Highest Risk of Maternal Mortality
Lowest Risk of Under 5 Mortality
Lowest Risk of Infant Mortality
Lowest Risk of Perinatal Mortality
Lowest Risk of Perinatal Mortality
Lowest risk of maternal Mortality
Highest Risk of Preterm Birth
Highest Risk of Pre-eclampsia
Highest Risk of Stillbirths
Data from analyses of Shea Rutstein, Agustín Conde-Agudelo, and Fuentes-Afflick and Hessol
Why the New Policy is “At least Three Years Birth Spacing” or “Three to Five Saves Lives”
monthsCurrentNorm
ProposedNorm

Where can we intervene for Maternal Nutrition?
Maintain her body
Develop Stores
Work
Breastfeeding
Fetal/placentalgrowth
FoodNutrients
DELAY!!
Golden Bow Initiative (UNICEF and WABA) Breastfeeding is the Gold Standard for
Resolution of Pregnancy and for Infant Feeding One Loop indicates the Child One Loop indicates the Mother The Knot: Father, Family, and Community,
without whose support, breastfeeding will not succeed.
One streamer for Continued Breastfeeding with Frequent and Quality Complementary Feeding
Second Streamer for the 3-5 Years of Birth Spacing

How does infant feeding contribute to Birth Spacing?
Survival Fertility Delay Método de Lactancia y Amenorrea
(MELA / LAM)

Timing of subsequent pregnancy by month postpartum and by
breastfeeding status
0
10
20
30
40
50
60
70
80
90
0 3 6 9 12 15 18 21 24 27 30 33 36 Months since last birth
% p
reg
nan
t
Non-lactating,non-contracepting -IndiaNon-lactating,non-contracepting -AlaskaLactating, non-contracepting -India
Lactating, non-contracepting -Alaska

Median duration of breastfeeding
and lactational amenorrhea in selected countries
0
5
10
15
20
25
30
35
Bangladesh Sri Lanka Senegal Peru
Breastfeeding AmenorrheaDHS, 1980s

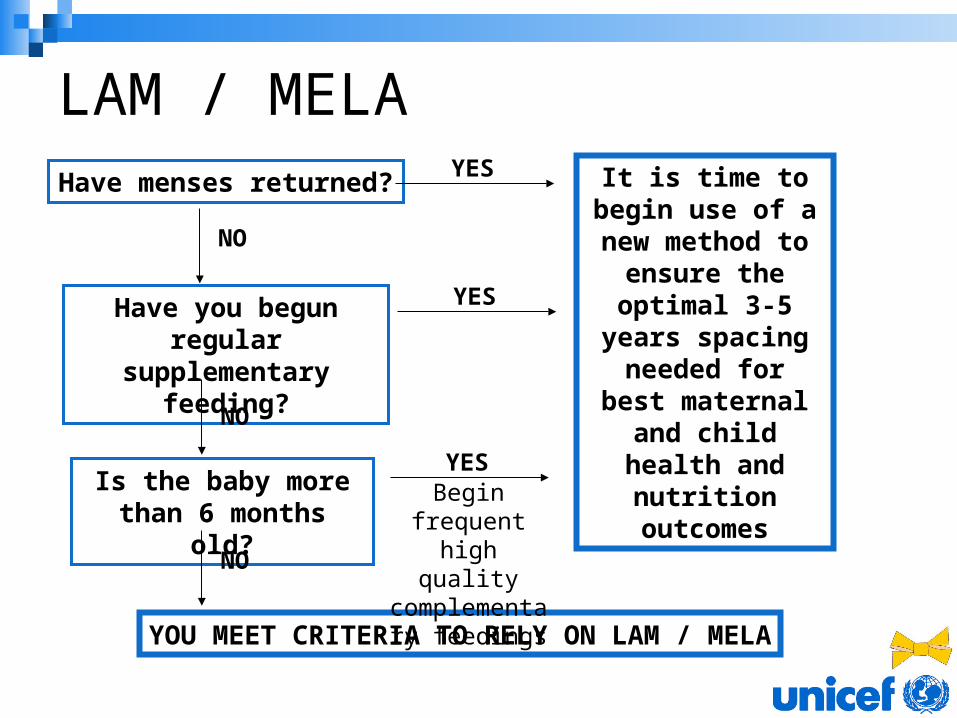
LAM / MELAHave menses returned?
Have you begun regular supplementary
feeding?
Is the baby more than 6 months old?
It is time to begin use of a new
method to ensure the optimal 3-5 years spacing
needed for best maternal and child
health and nutrition
outcomes
YES
YES
YES
NO
NO
NO
YOU MEET CRITERIA TO RELY ON LAM / MELA
Begin frequent high quality
complementary feedings
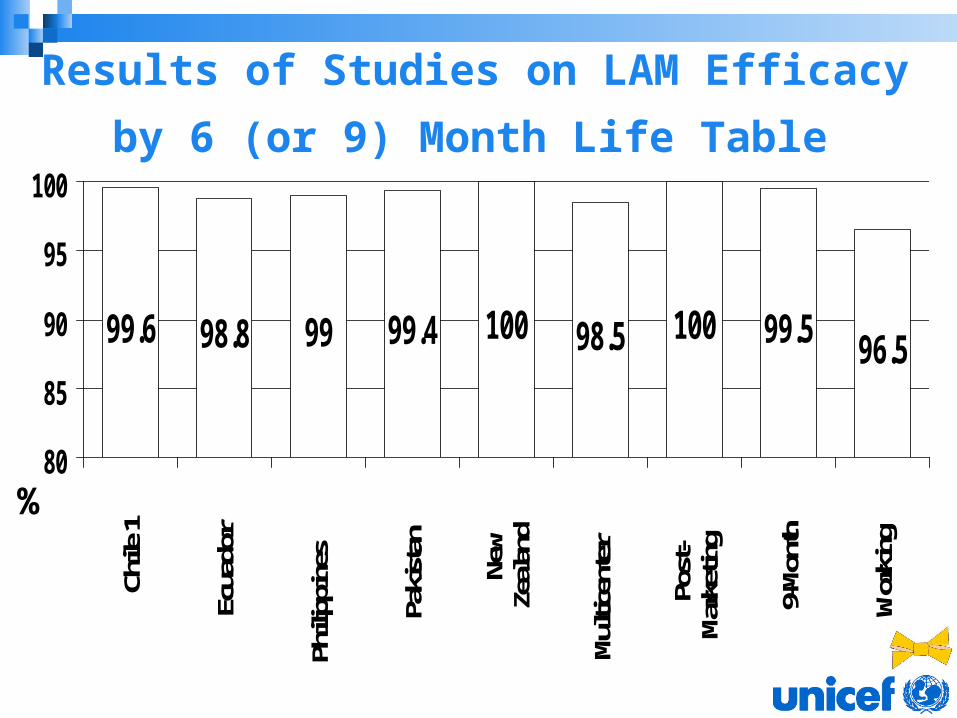
Results of Studies on LAM Efficacy
by 6 (or 9) Month Life Table
99.6 98.8 99 99.4 100 98.5 100 99.5 96.5
80
85
90
95
100
Chile
1
Ecua
dor
Phili
ppin
es
Pakis
tan
New
Zeala
nd
Multi
cent
er
Post
-Ma
rket
ing
9-Mo
nth
Wor
king
%

Return of Menses among Exclusively Breastfeeding Women: Approximate Cumulative Percent by Six-Month Life Table
0
5
10
15
20
25
30
35
40
1 2 3 4 5 6
Control Group
LAM Group

Average Number of Feeds per Day by Month Postpartum
6.5
7
7.5
8
8.5
9
1 2 3 4 5 6 months
LAM group
Control group
*
* * *
*p<0.05

Why does LAM have improved efficacy over lactational amenorrhea?
Slightly, but significantly, shorter intervals Slightly, but significantly, more feeding
episodes per day Greater attention to night feeds Dedication to breastfeeding patterns for
fertility impact
Conclusion: Women who choose LAM will practice closer to optimal breastfeeding behaviors
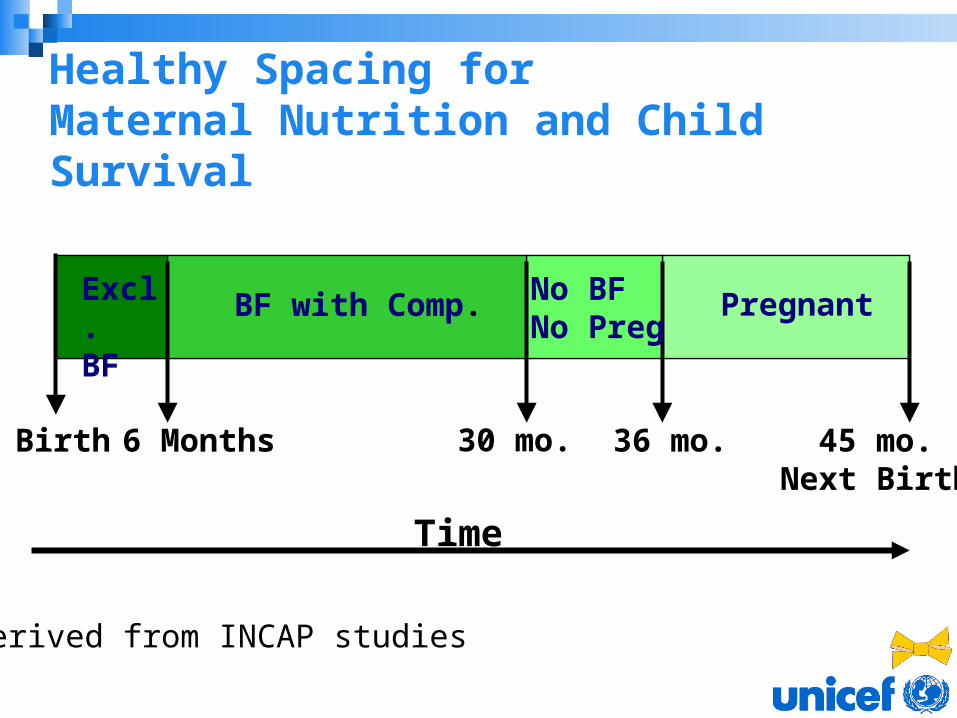
Healthy Spacing for Maternal Nutrition and Child Survival
Birth 6 Months 30 mo. 36 mo. 45 mo.Next Birth
Excl.BF
BF with Comp. No BFNo Preg
Pregnant
Derived from INCAP studies
Time

0
2
4
6
8
Indonesia Pakistan Brazil Peru Burkina Faso Nigeria
If there were no Breastfeeding - additional births (000,000)
Current Births (000,000)
Additional Births If There Were No Breastfeeding...
Becker et al, 1999
Globally, if breastfeeding disappeared, the birth rate Globally, if breastfeeding disappeared, the birth rate would increase immediately and significantlywould increase immediately and significantly

3. How does this effect us today, and what should be considered in
terms of policy and programmes?
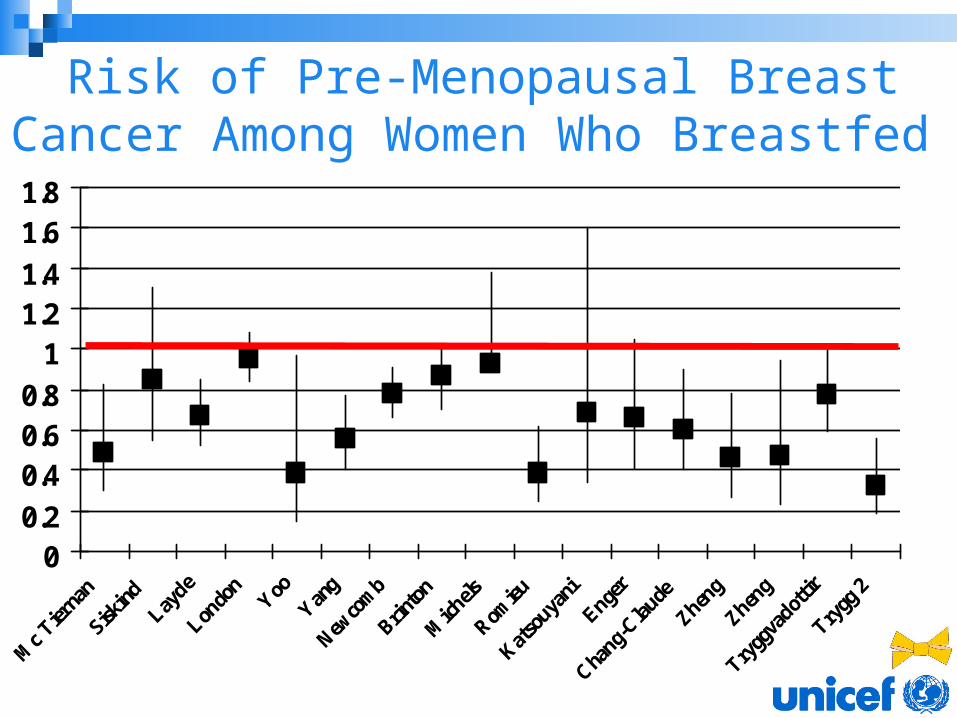
Risk of Pre-Menopausal Breast Cancer Among Women Who Breastfed
00.2
0.40.60.8
11.21.4
1.61.8
?Breastfeeding and Reduced Osteoporosis?
YES: Melton et al, Influence of breastfeeding and other reproductive factors on bone mass later in life. Osteoporos Int 1993 Mar;3(2):76-83
YES: Kreiger N, Kelsey JL, Holford TR, O'Connor T. An epidemiologic study of hip fracture in postmenopausal women. Am J Epidemiol 1982 Jul;116(1):141-8
NONE: Ramalho AC, Lazaretti-Castro M, Hauache O, Vieira JG, Takata E, Cafalli F, Tavares F Sao Paulo Med J 2001 Mar;119(2):48-53 Osteoporotic fractures of proximal femur: clinical and epidemiological features in a population of the city of Sao Paulo.
NONE: Clark P, de la Pena F, Gomez Garcia F, Orozco JA, Tugwell P. Risk factors for osteoporotic hip fractures in Mexicans. Arch Med Res 1998 Autumn;29(3):253-7
HIV Breastfeeding and Maternal Mortality Nduati R, Richardson BA, John G, Mbori-Ngacha D,
Mwatha A, Ndinya-Achola J,Bwayo J, Onyango FE, Kreiss J. Effect of breastfeeding on mortality among HIV-1 infected women: a randomised trial Lancet. 2001
Versus
Coutsoudis A, Coovadia H, Pillay K, Kuhn L. Are HIV-infected women who breastfeed at increased risk of mortality? AIDS 2001 Mar 30;15(5):653-5
WHO Statement, 2003, no reason to change policy that states that pregnancy is not an additional risk

For today’s woman: Delayed first birth and birth spacing allow mothers’ bodies
to mature and achieve better nutritional status. Better maternal nutritional status at conception is
associated with less SGA/LBW and reduced MMR Better maternal nutrient status supports best breastfeeding
practices The longer the baby is the youngest, the longer it will be
breastfed, the more time the mother will have for active feeding, the longer this child will remain the center of family care and benefit in terms of survival, growth and development.
The best birth interval for both maternal and child outcomes is three to five years
Considering all “best choices” results in “best outcomes”
Recognize that our bodies evolved for survival, and if problems arise, they merit consideration from an evolutionary and intergenerational life-cycle perspective.

Thank you!!!
Muchas Gracias!!!
Merci!!!
Cпасибо!!!
Danke!!!
Top Related