







Languages
Pages
Legal

Ersin KÜRŞAT
December 2007

Contents
History Fields of applications Components Polymerisations Clinical case Antibiotics Clinical studies Surgical procedurs
HISTORY
The story of modern cements began with Otto Röhm’s invention in the early 20th century of polymethyl methacrylate (PMMA), a solid material with good biocompatibility.
In the 1960s Sir John Charnley began using bone cement on numerous patients for the fixation of both the femur and acetabulum. Before the end of the decade, Buchholz came up with the idea of adding an antibiotic to the cement to decrease the incidence of infection.
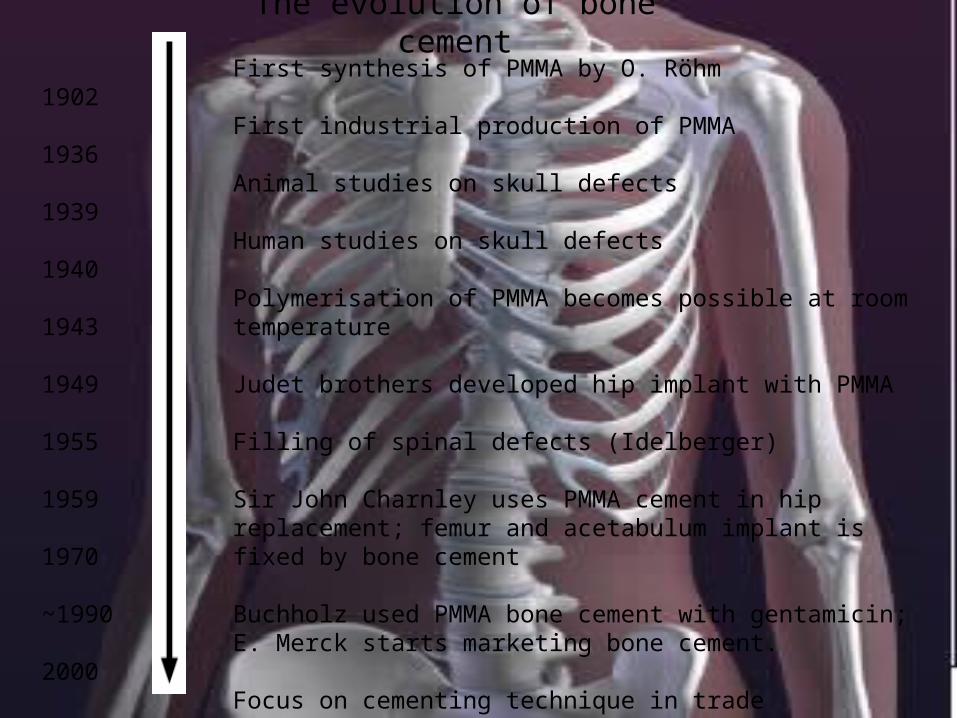
The evolution of bone cement
1902
1936
1939
1940
1943
1949
1955
1959
1970
~1990
2000
First synthesis of PMMA by O. Röhm
First industrial production of PMMA
Animal studies on skull defects
Human studies on skull defects
Polymerisation of PMMA becomes possible at room temperature
Judet brothers developed hip implant with PMMA
Filling of spinal defects (Idelberger)
Sir John Charnley uses PMMA cement in hip replacement; femur and acetabulum implant is fixed by bone cement
Buchholz used PMMA bone cement with gentamicin; E. Merck starts marketing bone cement.
Focus on cementing technique in trade publications
1 million implants fixated with bone cement worldwide
Bone Cement
Bone cements consist of two primary components: a powder consisting of copolymers based on the substance polymethyl methacrylate (PMMA), and a liquid monomer, methylmethacrylate (MMA). These two components are mixed at an approximate ratio of 2:1 to form a polymethyl methacrylate cement.
When the polymer powder and monomer liquid meet, the polymerization process starts. During polymerization of the monomer, the original polymer beads of the powder are bonded into a dough-like mass. The mass hardens approximately 7-15 minutes after the start of mixing, depending on temperature
The polymerisation process can be divided into four different phases: mixing, waiting, application and setting.
Processing times of bone cement
Polymerization depends on a.Room temperature b.Temperature of the bone cement
components c.Prothesis temperature
1. Mixing phase Complete wetting of the powder with liquid ! This produces a homogeneous cement Hand mixing: Risk of air bubbles in the paste
2. Waiting phase Swelling of the paste material Slow polymerisation Increased viscosity, but paste still
sticky
3. Working phase completion of the waiting phase
essential!(ideal working viscosity) application into the femur(for
manual application non-sticky,viscosity not too high))
4.Hardening phase Strength of the cement increases Polymerisation comes to a halt Duration of poşymerisation dependent
on .Room temperature, .Component temperature, .Prothesis temperature .Air humidity
During polymerization, cement properties critical for operating procedures, such as viscosity change, setting time, cement temperature, mechanical strength, shrinkage and residual monomer, are determined. These properties will influence cement handling, penetration and interaction with the prosthesis.
Properties
Viscosity Mixing together the powder and the liquid
components marks the start of the polymerization process.
During the reaction, the cement viscosity increases, slowly at first, then later more rapidly.
Clinical experience has shown that high viscosity cements produce better clinical results, as compared to low viscosity cements.

*Bone cements may be divided into two kinds: low viscosity and high viscosity.
Viscosity affects the following:
Mixing behaviour Penetration into
cancellous bone Resistance
against bleeding Insertion of the
implant
Low viscosity: These cements have a long-lasting liquid, or mixing phase, which makes for a short working phase.4 As a consequence, application of low viscosity cements requires strict adherence to application times.
High viscosity: These cements have a short mixing phase and loose their stickiness quickly. This makes for a longer working phase, giving the surgeon more time for application
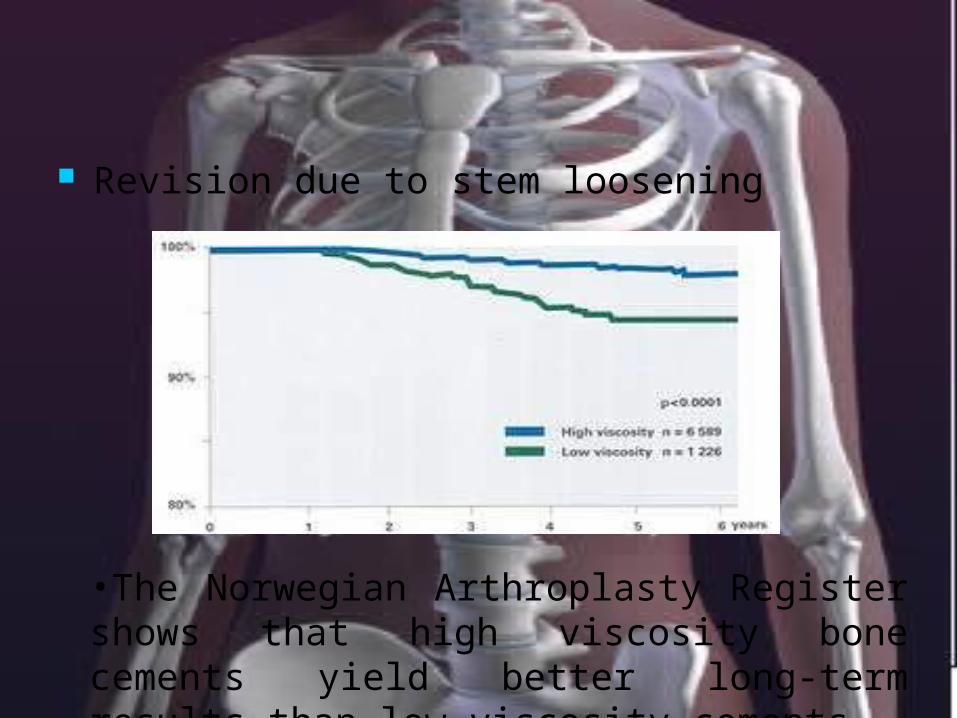
Revision due to stem loosening
•The Norwegian Arthroplasty Register shows that high viscosity bone cements yield better long-term results than low viscosity cements.
Temperature affects mixing time, delivery of the cement, prosthesis insertion, and other aspects of the cementing process. It is therefore very important to control the temperature of the bone cement and the OR.
To achieve optimal cement properties, it is important to adhere to the time schedules indicating the correlation of temperature to handling time. These time schedules are usually included in the instructions for the bone cement.
High viscosity cements are sometimes pre-chilled for use with mixing systems for easier mixing and prolonged working phase. This will also increase the setting time. The relative humidity might also influence the handling properties. That is the reason why the the working time and setting time of the cement might vary in winter and summer.
Temperatures
Mechanical properties
The bone cement is subjected to high mechanical stress in the body. In vivo, the biomechanical situation is rather complex, involving different types of loading (bending, compression, shear), which must be tested. The international standard ISO 5833 describes the methods for determining compressive strength, bending strength and bending modulus.7
As the cemented implant is subjected to not only static load but also dynamically alternating loads, the fatigue properties of the cement affect survival of the implant.
Antibiotic-loaded bone cement
Periprosthetic infection is the most feared complication in total hip and knee replacement. The infection usually leads to a complete failure of the joint replacement, resulting in a long series of operative procedures, great discomfort for the patient and heavy costs.1
Infections occur because of the high affinity of many germs to the surface of implants. Once settled, germs are less sensitive to antibiotics, as they are covered with a “slime” preventing them from attacks from the host defence mechanism. This renders treatment with systemic antibiotics ineffective
A solution to the problem is preventing the settlement of germs. The use of antibiotic-loaded bone cements allows for high local concentrations of antibiotics to be administered to the areas surrounding the implant, protecting the implant from the settling of germs. Moreover, antibiotic levels in the serum are sufficiently low so as to avoid causing side effects.
The addition of antibiotics to bone cement was undertaken at the beginning of the 1970s by Buchholz,2 from the Endo-Klinik in Hamburg. His idea was to add antibiotics to the cement in order to reduce the incidence of infection, which was high at that time. Using gentamicin in combination with PMMA cement, it was found that the combination with gentamicin was stable and offered a suitable spectrum of antibiotic activity.
Attention must be given to reducing the incidence of infection in joint replacement surgery and to fighting infection once it has occurred.
Orthopaedic infections There are numerous reports in the literature
about the incidence of postoperative wound sepsis and the organisms causing this complication. Almost 75% of all bacteria that can be isolated during hip operations are Gram-positive, with staphylococci representing the majority. Among Gram-negative bacteria, E. coli and pseudomonas are most common.3
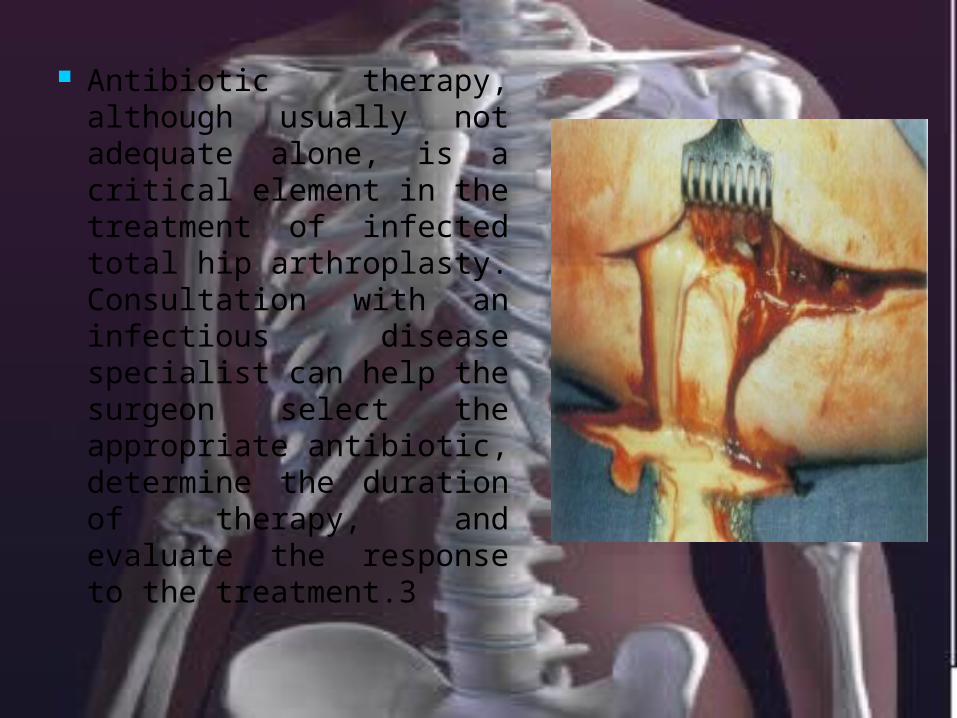
Antibiotic therapy, although usually not adequate alone, is a critical element in the treatment of infected total hip arthroplasty. Consultation with an infectious disease specialist can help the surgeon select the appropriate antibiotic, determine the duration of therapy, and evaluate the response to the treatment.3
Antibiotic therapy, although usually not adequate alone, is a critical element in the treatment of infected total hip arthroplasty. Consultation with an infectious disease specialist can help the surgeon select the appropriate antibiotic, determine the duration of therapy, and evaluate the response to the treatment
Antibiotic-loaded bone cement
Gentamicin is an aminoglycoside antibiotic . It is bactericidal, has a dose-dependent killing curve, remains stable when exposed to heat and is soluble in water. These four characteristics make it especially suited for use in bone cement.
Gentamicin is mixed in bone cement for prophylaxis against infections after arthroplasties. The substance is slowly eluted in the surrounding tissue
Gentamicin loaded bone cement
Clindamycin belongs to the group of lincosamide antibiotics. It is additionally active against some anaerobic germs, such as peptostreptococci, anaerobic germs. This activity makes it a suitable antibiotic in combination with gentamicin, covering most of the germs typically occuring in periprosthetic infection
Gentamicin and clindamycin is a combination known to have a bacterical effect on more than 90% of the bacteria common to infected arthroplasty cases.8

Vacuum Mixing and Delivery
Vacuum mixing, which was adapted from the dental field, was developed for bone cement in the early 1980s. Vacuum mixing has several important purposes:
to enhance cement properties to reduce bone cement porosity and to improve the working environment in the
operating room.
Numerous studies have shown that, compared to hand mixing, vacuum mixing prevents air entrapment in cement, reduces cement porosity, decreases the number of unbounded particles in cement and increases cement’s mechanical strength. Vacuum mixing furthermore reduces monomer evaporation and exposure in the operating room

Mixing as well as collecting cement under vacuum yields a homogenous mix without affecting viscosity or any cement additives such as antibiotics or radio-contrast media.
Delivering cement with a syringe,under ressurization, produces better penetration into the bone bed than delivering cement with the hands.
Bone bed preparation and Pressurization in Total Hip Replacement
Careful preparation of the bone cavity and bone bed with high-pressure pulse lavage and brushing is essential for achieving an effective micro-interlock between the bone and the cement.
Clinical studies have shown that the use of high-pressure pulse lavage reduces the risk of revision due to aseptic loosening.
In the early days syringes and knives were used to clean the bone bed. These tools had the disadvantage of removing healthy tissue along with unhealthy and not sufficiently cleaning the bone bed.
The importance of careful preparation of the bone surfaces, using brushes and pulse lavage to achieve micro-interlock, has been described since the 1970s.
In the 1980´s techniques for pressurization of bone cement were introduced. Proper pressurization is important. The pressure on the cement has to be larger than the blood pressure no to be pushed out of the bone. Pressure should be applied until the viscosity of the bone cement has increased so it is high enough to resist blood pressure.

Reaming The bone cavity should be
shaped to provide an even cement layer between the bone and prosthesis. An even cement layer provides better stress distribution and reduces the risk of cement mantle failure. Size of reaming should be determined at preoperative planning.
It is important to save the transversal ligament in order to optimize pressurization for acetabular cementing.
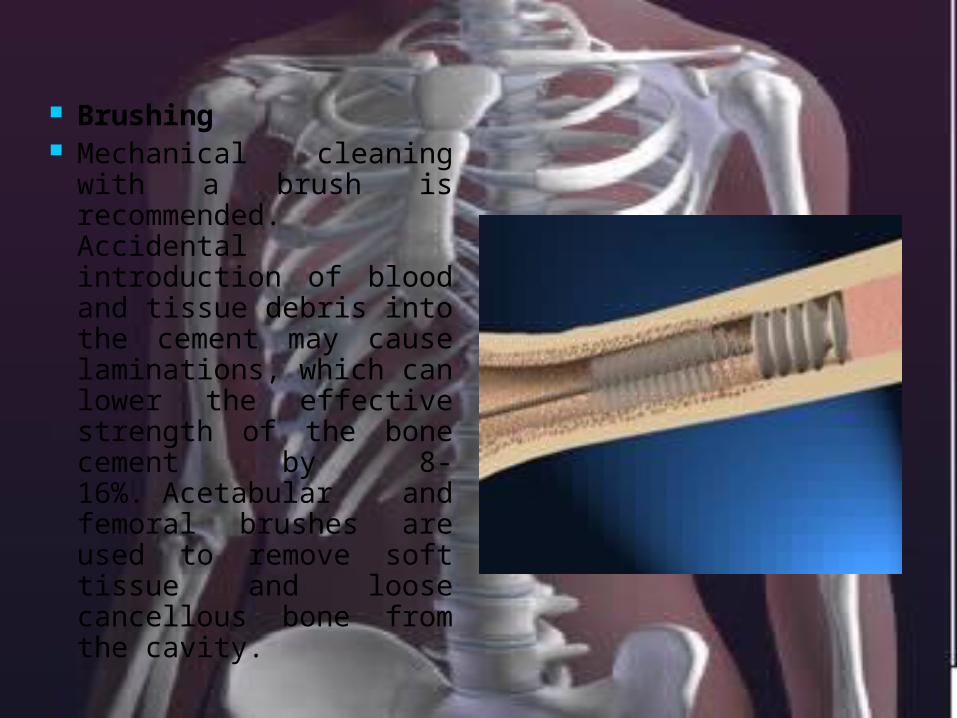
Brushing Mechanical cleaning
with a brush is recommended. Accidental introduction of blood and tissue debris into the cement may cause laminations, which can lower the effective strength of the bone cement by 8-16%. Acetabular and femoral brushes are used to remove soft tissue and loose cancellous bone from the cavity.
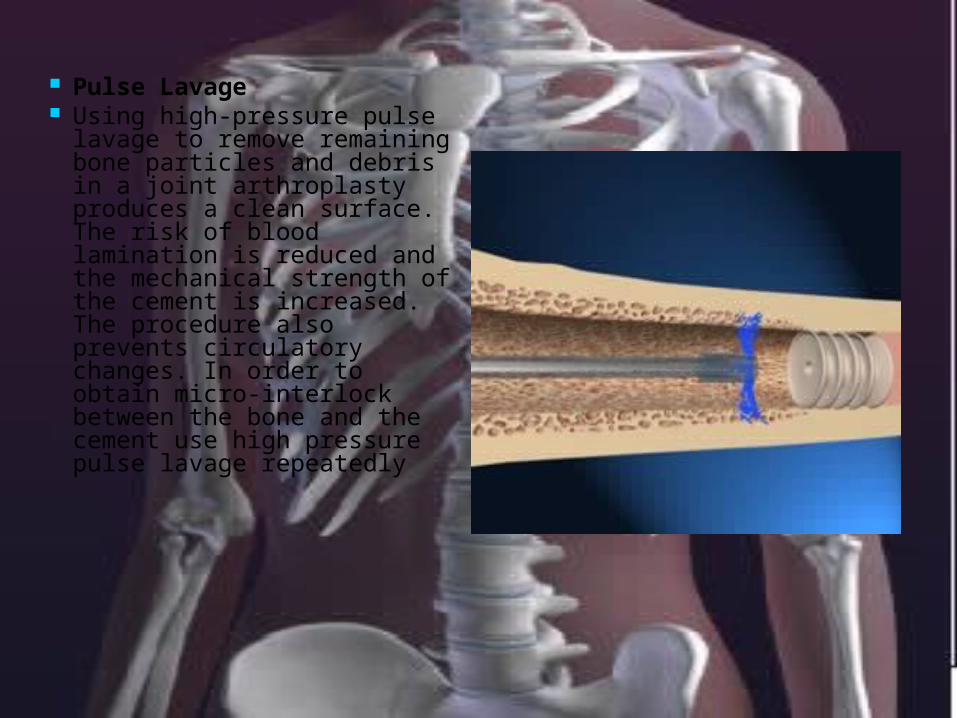
Pulse Lavage Using high-pressure pulse
lavage to remove remaining bone particles and debris in a joint arthroplasty produces a clean surface.The risk of blood lamination is reduced and the mechanical strength of the cement is increased. The procedure also prevents circulatory changes. In order to obtain micro-interlock between the bone and the cement use high pressure pulse lavage repeatedly
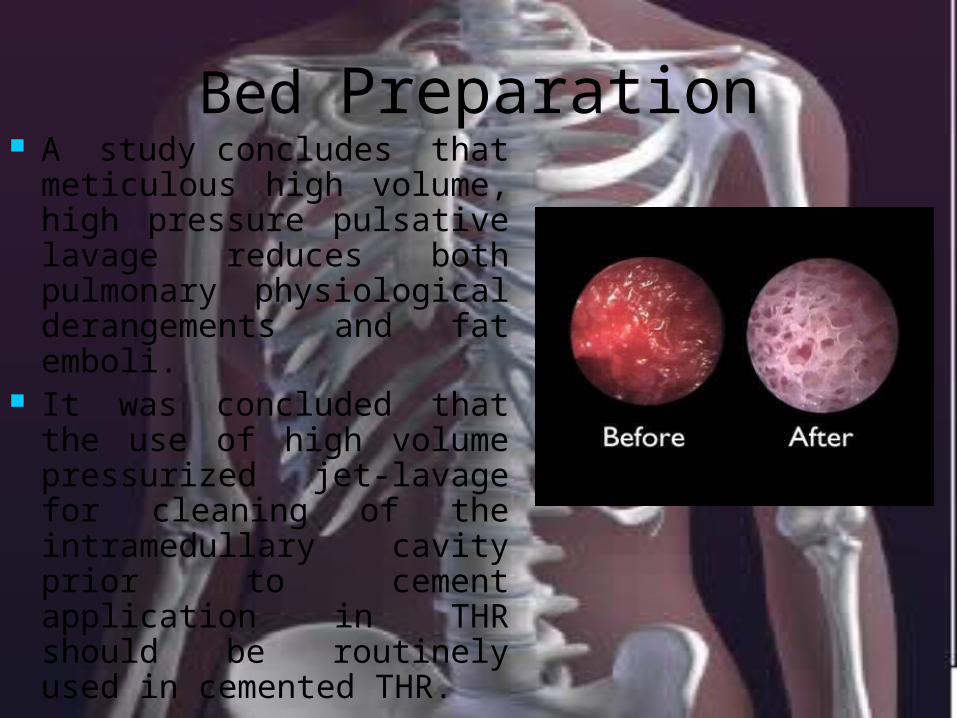
Bed Preparation A study concludes that
meticulous high volume, high pressure pulsative lavage reduces both pulmonary physiological derangements and fat emboli.
It was concluded that the use of high volume pressurized jet-lavage for cleaning of the intramedullary cavity prior to cement application in THR should be routinely used in cemented THR.
Anchorage holes and restrictors
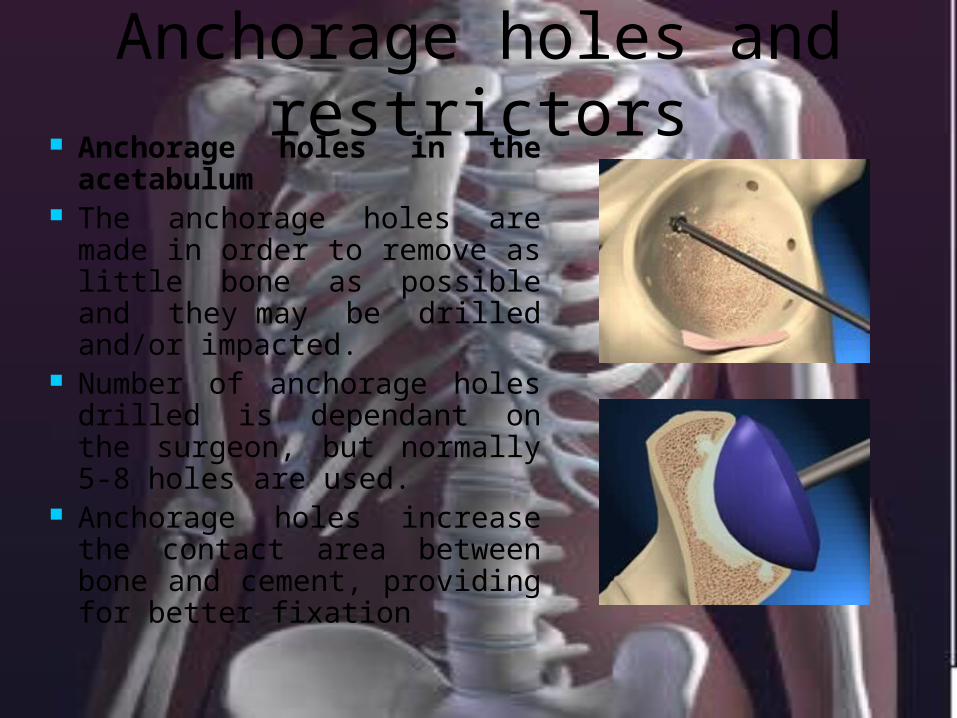
Anchorage holes in the acetabulum
The anchorage holes are made in order to remove as little bone as possible and they may be drilled and/or impacted.
Number of anchorage holes drilled is dependant on the surgeon, but normally 5-8 holes are used.
Anchorage holes increase the contact area between bone and cement, providing for better fixation
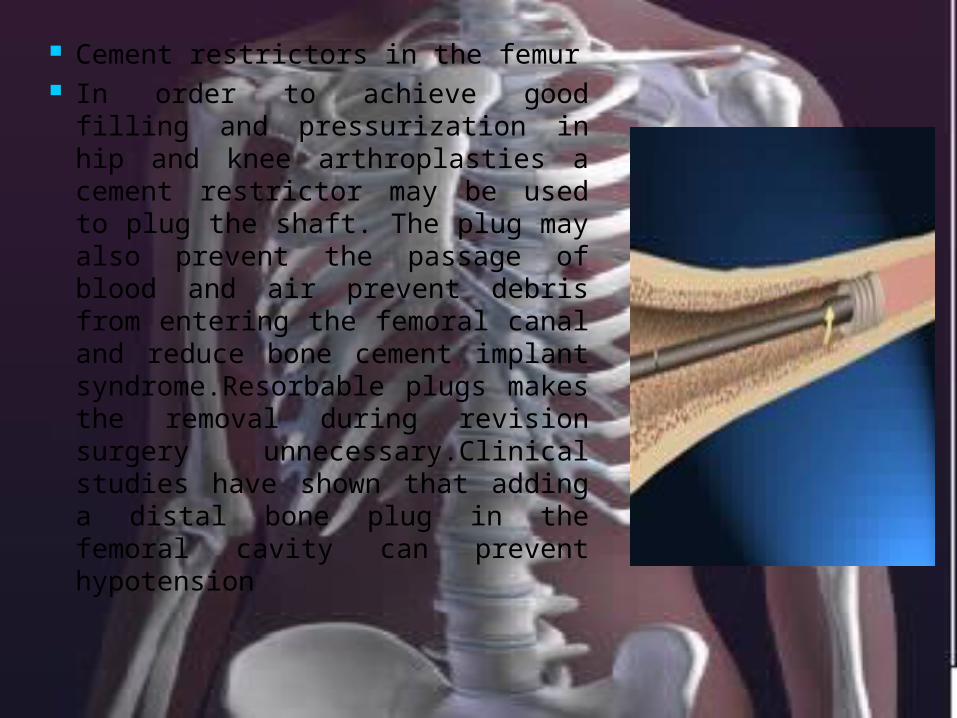
Cement restrictors in the femur In order to achieve good filling
and pressurization in hip and knee arthroplasties a cement restrictor may be used to plug the shaft. The plug may also prevent the passage of blood and air prevent debris from entering the femoral canal and reduce bone cement implant syndrome.Resorbable plugs makes the removal during revision surgery unnecessary.Clinical studies have shown that adding a distal bone plug in the femoral cavity can prevent hypotension


Funcion of bone cement
Fixing the artificial joint Anchoring the implant the bone Connection stabilisation of vertebral
defects Transfering load from the prothesis to
the bone Optimal load distribution Release of antibiotics
All currently available bone cements are base on MethylMethAcrylate (MMA) /
ButhylMethAcrylate / Styrene
All cements consist of two components, i.e. Powder and liquid
Yet there are significant differences in: Specification of monomers and polymers Composition Sterilization method Radiopaque additives Antibiotics and very important Manifacturing
process

Polymerisation Temperature of Bone Cement
Per mole MMA, during the radcal polymerisation of MMA to PMMA, a reaction enthalpy of 57 kj is released.
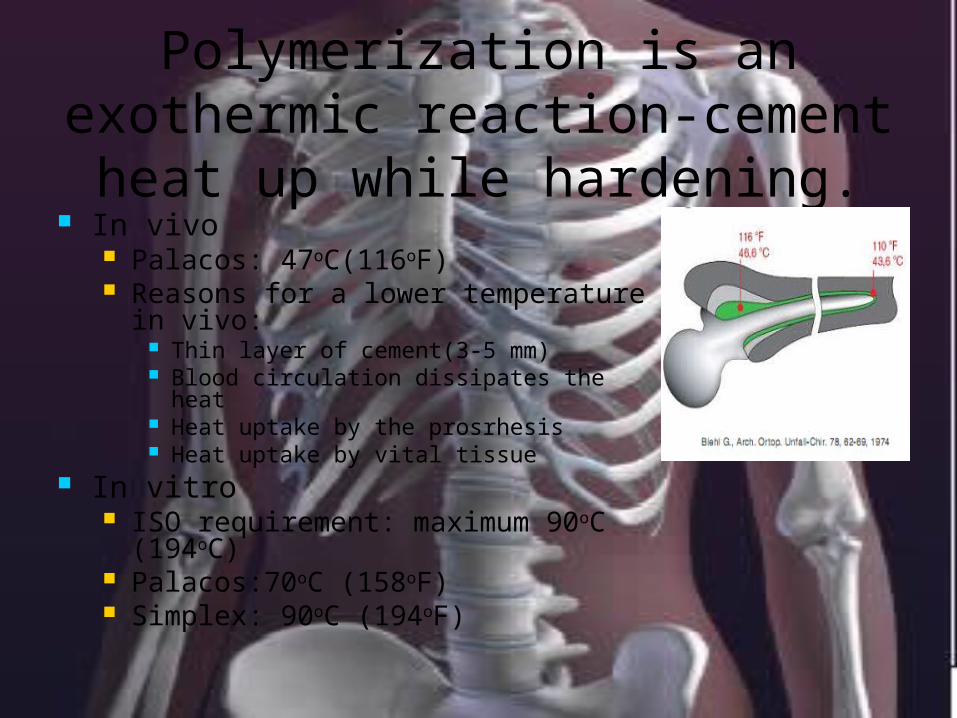
Polymerization is an exothermic reaction-cement
heat up while hardening. In vivo
Palacos: 47oC(116oF) Reasons for a lower temperature
in vivo: Thin layer of cement(3-5 mm) Blood circulation dissipates the heat Heat uptake by the prosrhesis Heat uptake by vital tissue
In vitro ISO requirement: maximum 90oC
(194oC) Palacos:70oC (158oF) Simplex: 90oC (194oF)
Top Related