







Languages
Pages
Legal


Prof. Vladimir BobićMD FRCSEd, Consultant Orthopaedic Knee Surgeon
Chester Knee Clinic at Nuffield Health, The Grosvenor Hospital Chester, United Kingdomwww.kneeclinic.info [email protected] @ChesterKnee
BioPoly®RS Knee System The partial resurfacing implant
1
Relevant Disclosures
1: Royalties received from Schwartz Biomedical3b: Paid Consultant for intellectual property (implant
and instrument design), Schwartz Biomedical
2

Mr Mike McNicholasBSc, MD, FRCSEd(Tr&Orth), FFSEM RSCI
Consultant, University Hospital Aintree, LiverpoolHon Prof, Directorate of Sport, University of Salford
Hon Senior Lecturer, Department of Musculoskeletal Biology, University of Liverpool
BioPoly®RS Knee System
The partial resurfacing implant
Cardiff, 3rd February 2017
3
@BioKneeSociety

Articular Cartilage Repair: Surgical Options
ACI/MACI
BioPoly: Filling the Void?
OATSMicrofracture
Allografts UKR & TKR4
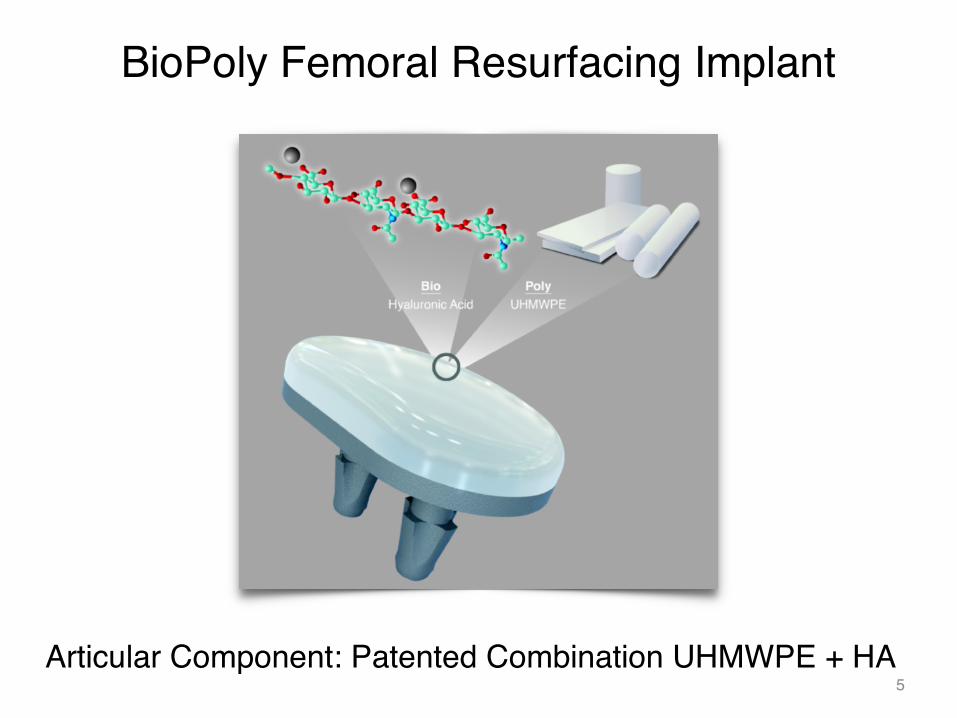
BioPoly Femoral Resurfacing Implant
Articular Component: Patented Combination UHMWPE + HA5
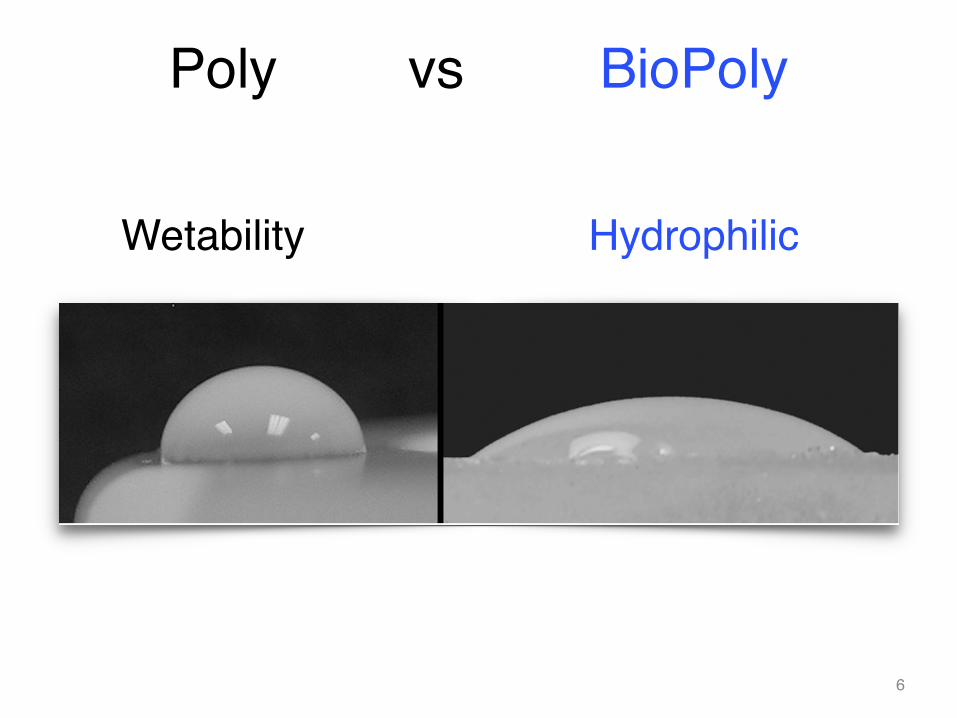
Poly vs BioPoly
Wetability Hydrophilic
6

Self-lubricating material for better wear
7

• BioPoly® Material– “Microcomposite” (UHMWPE and Hyaluronic Acid)– Hydrophilic (water attracting) polymer
• Hyaluronic Acid within BioPoly®– Attracts synovial fluid for lubrication– Allows for articulation with cartilage
• No damage to opposing cartilage surfaces• No damage to implant surface
• Resurfacing Applications
BioPoly® Technology Overview
Hyaluronic Acid
8
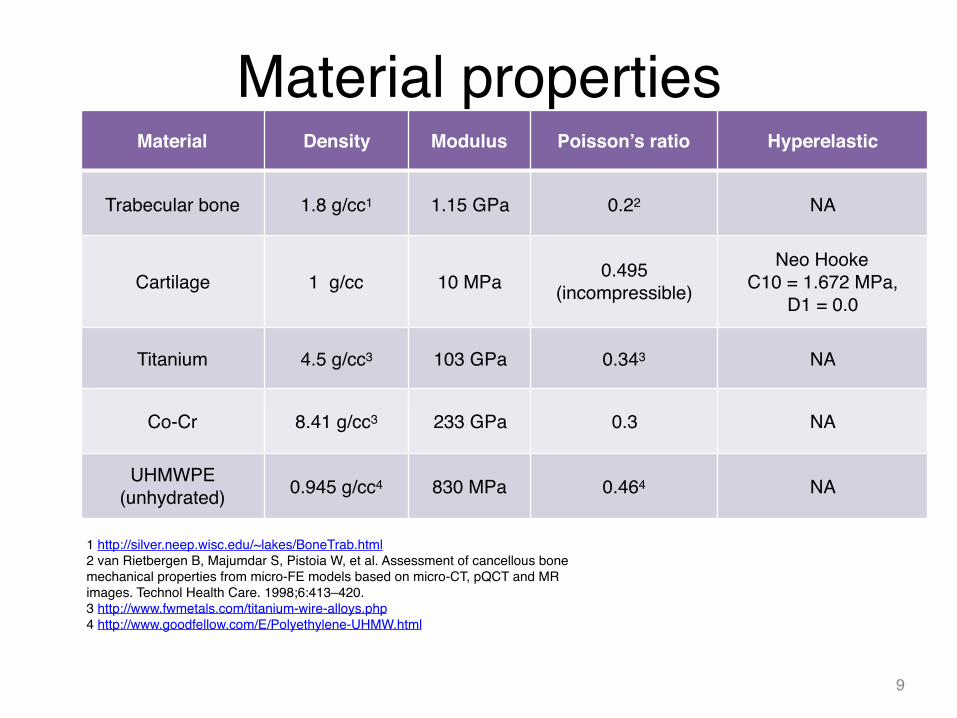
Material properties
9
Material Density Modulus Poisson’s ratio Hyperelastic
Trabecular bone 1.8 g/cc1 1.15 GPa 0.22 NA
Cartilage 1 g/cc 10 MPa 0.495 (incompressible)
Neo HookeC10 = 1.672 MPa,
D1 = 0.0
Titanium 4.5 g/cc3 103 GPa 0.343 NA
Co-Cr 8.41 g/cc3 233 GPa 0.3 NA
UHMWPE (unhydrated) 0.945 g/cc4 830 MPa 0.464 NA
1 http://silver.neep.wisc.edu/~lakes/BoneTrab.html2 van Rietbergen B, Majumdar S, Pistoia W, et al. Assessment of cancellous bone mechanical properties from micro-FE models based on micro-CT, pQCT and MR images. Technol Health Care. 1998;6:413–420.3 http://www.fwmetals.com/titanium-wire-alloys.php4 http://www.goodfellow.com/E/Polyethylene-UHMW.html
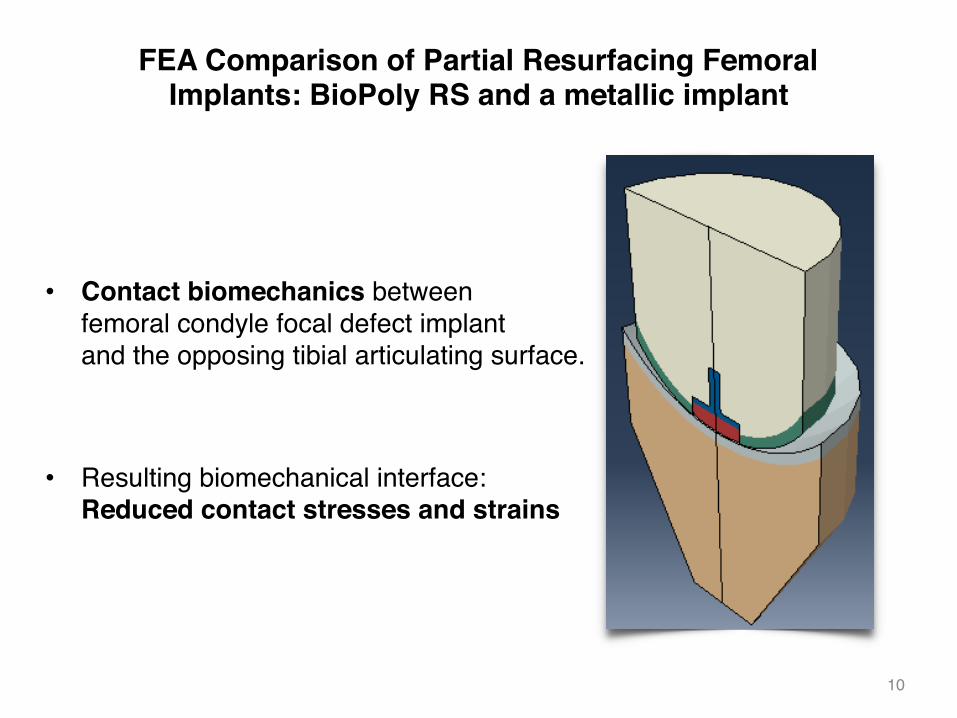
FEA Comparison of Partial Resurfacing Femoral Implants: BioPoly RS and a metallic implant
• Contact biomechanics between femoral condyle focal defect implant and the opposing tibial articulating surface.
• Resulting biomechanical interface: Reduced contact stresses and strains
10
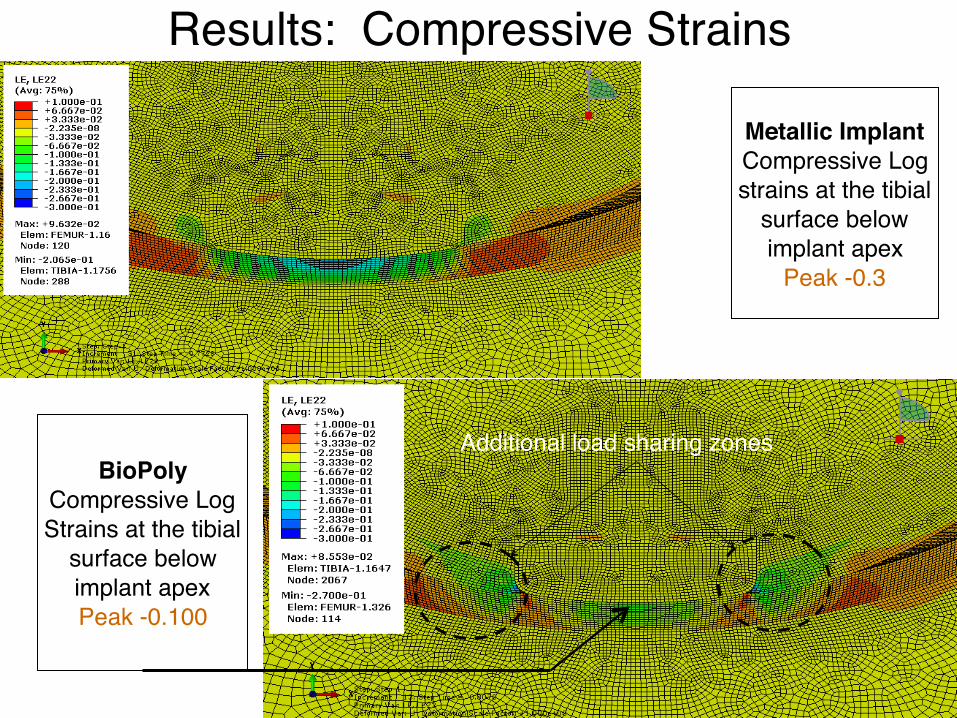
Results: Compressive Strains
11
Metallic Implant Compressive Log strains at the tibial
surface below implant apex
Peak -0.3
BioPoly Compressive Log Strains at the tibial
surface below implant apexPeak -0.100
Additional load sharing zones

BioPoly loading FEA
12
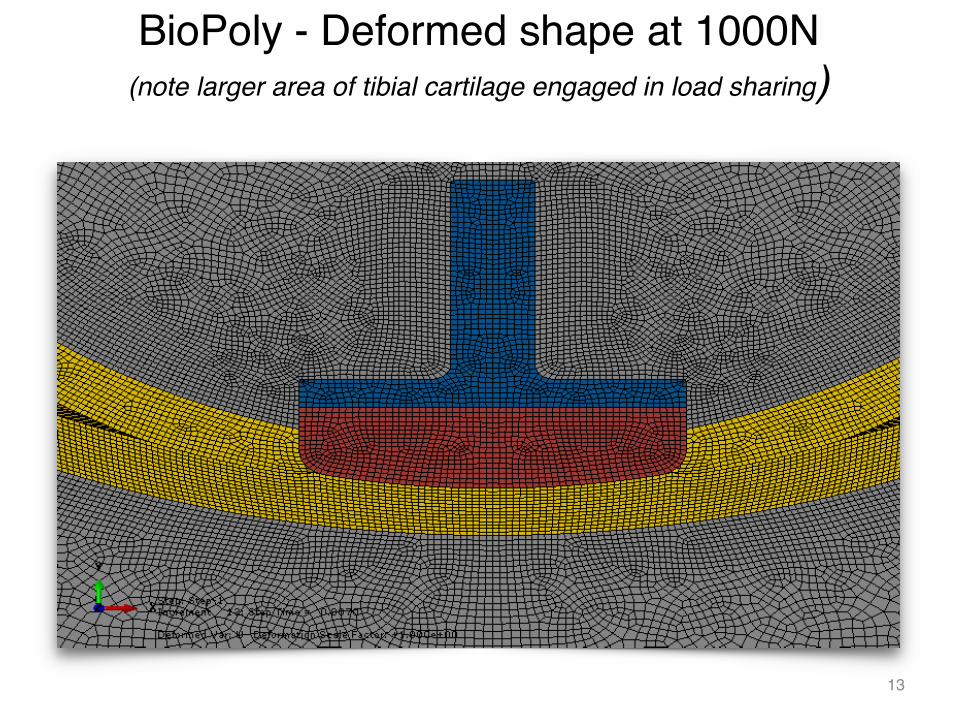
BioPoly - Deformed shape at 1000N (note larger area of tibial cartilage engaged in load sharing)
13

Results in lower opposing cartilage contact pressure (2.5x body weight load)
BioPoly Tibial Cartilage
Contact Pressure
Peak = 3.46 MPa
Active Contact Zone Loaded Area ~ 471
mm2
Metal Implant Tibial Cartilage
Contact Pressure
Peak = 7.24 MPa
Active Contact Zone Loaded Area ~ 314 mm2
14

®Confidential
BioPoly RS Knee and Patella System
• CE Marked• Suitable for cartilage defects in the distal
femur and patella up to 3.1 cm2
• Femoral Condyle and Trochlear Facet Implants
– Ti64 grit blasted stems. Press fit or cemented• Patella implants
– All BioPoly construction for cementation• Simple surgical instrument set and
technique• Existing reimbursement codes
Femoral Condyles and Trochlear Facets
Patella15mm 20mm 15x24mm
15mm/0 15mm/1 20mm/0 20mm/1
15
BioPoly RS Knee Surgical Technique
16

17
The Race-track BioPoly RS Knee Surgical Technique

BioPoly Surgical Technique
18

BioPoly Surgical Technique
19

20
BioPoly RS Knee Surgical Technique

21
BioPoly RS Knee Surgical Technique

22
BioPoly RS Knee Surgical Technique

23
BioPoly RS Knee Surgical Technique

24
BioPoly RS Knee Surgical Technique

25
BioPoly RS Knee Surgical Technique

26
BioPoly RS Knee Surgical Technique

27
BioPoly RS Knee Surgical Technique

28
BioPoly RS Knee Surgical Technique

29
BioPoly RS Knee Surgical Technique

30
BioPoly RS Knee Surgical Technique

31
BioPoly RS Knee Surgical Technique

Race-track BioPoly
32
33

Patellar BioPoly
34
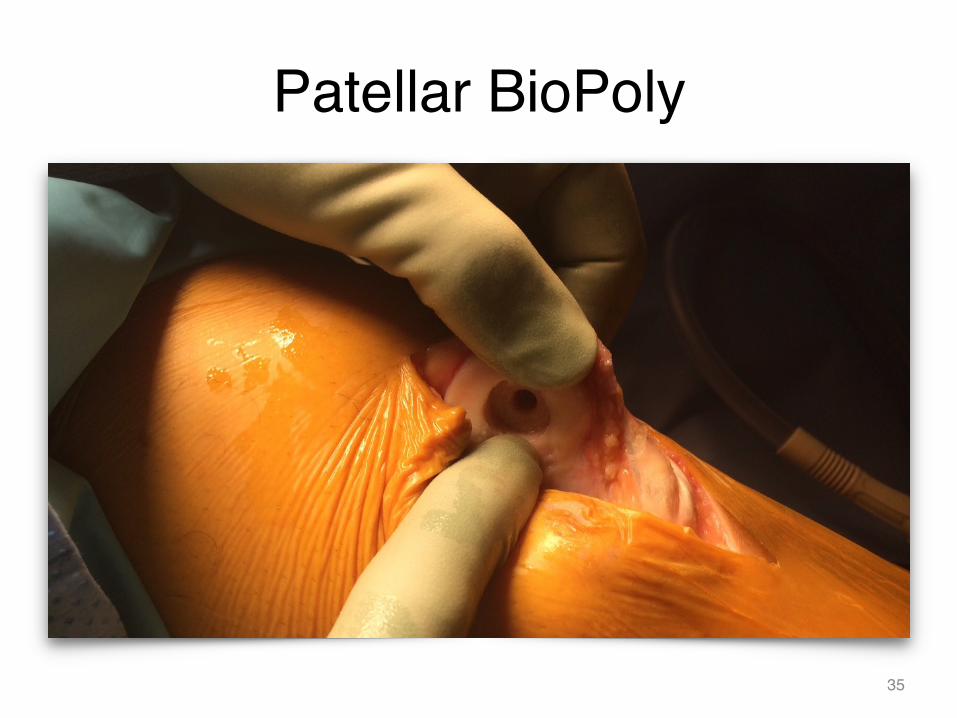
Patellar BioPoly
35

Cemented all BioPoly Implant
36

Current BioPoly® RS Partial Resurfacing3 Families of Products
BioPoly® RS KNEECE Marked
BioPoly® RS PATELLACE Marked
BioPoly® RS SHOULDERCE Marked
Patella HumeralheadDistal Femur
37+ BioPoly® RS Femoral Trochlea and Talar Dome in the pipeline

BioPoly® RS Partial Resurfacing Knee Implantations
5 yrs
600+ cases
38

BioPoly® RS Partial Resurfacing Knee SystemTypical Resurfacing Patient
▪ 21+ year old active adult▪ Knee pain▪ Too young for TKR▪ Often failed Debridement, Microfracture,
OATS or ACI▪ Patients wanting to regain active lifestyle
▪ Focal defects ▪ Femoral condyles
39
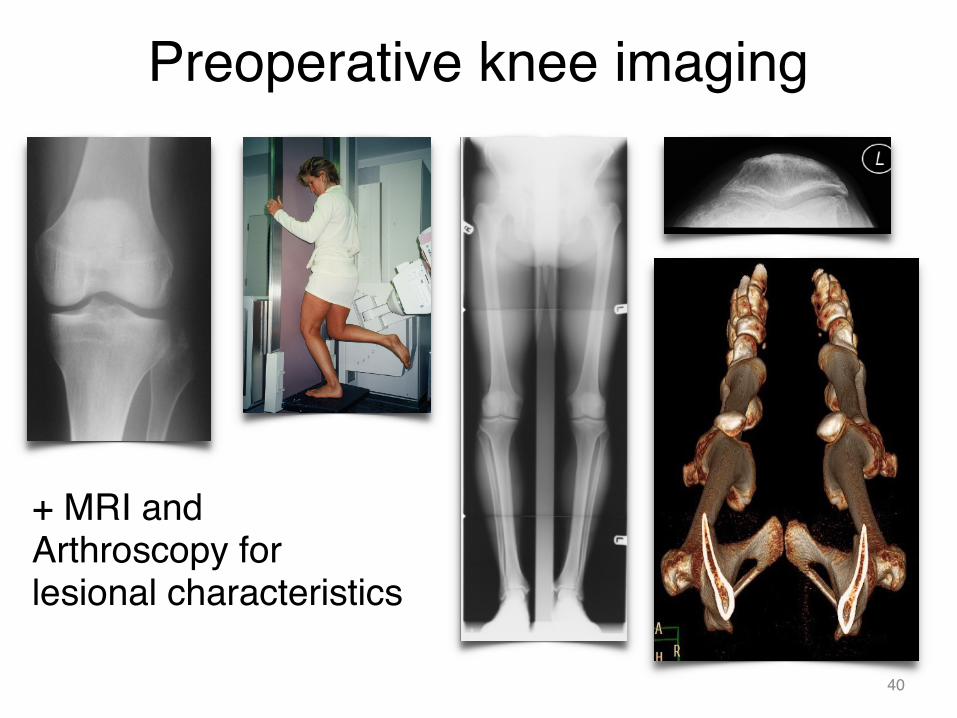
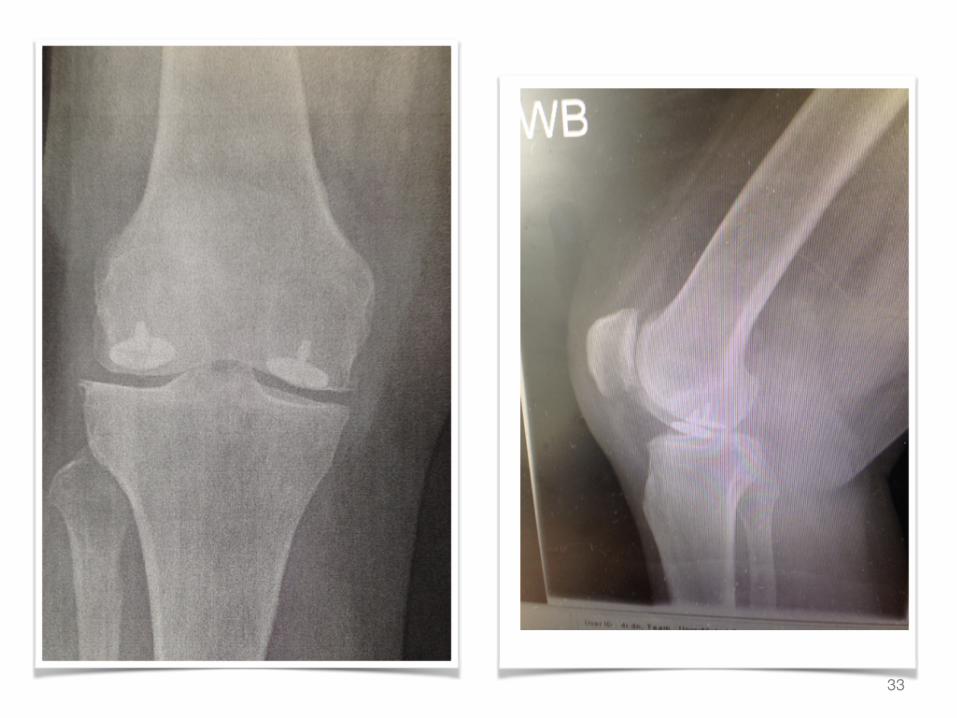
Preoperative knee imaging
+ MRI and Arthroscopy for lesional characteristics
40

Indications : Lesion Characteristics• Medial or Lateral femoral condyle, NOT tibial condyles
• Focal 2cm2 or (2.4 x 1.5) cm2 ≤3.1cm2 (Entire lesion visualized in static knee through static arthroscope)
• ICRS grade 2, 3, or 4
• Contained ICRS 0/1
• Depth from articular surface < 4mm
• Good subchondral bone (MRI)
X41
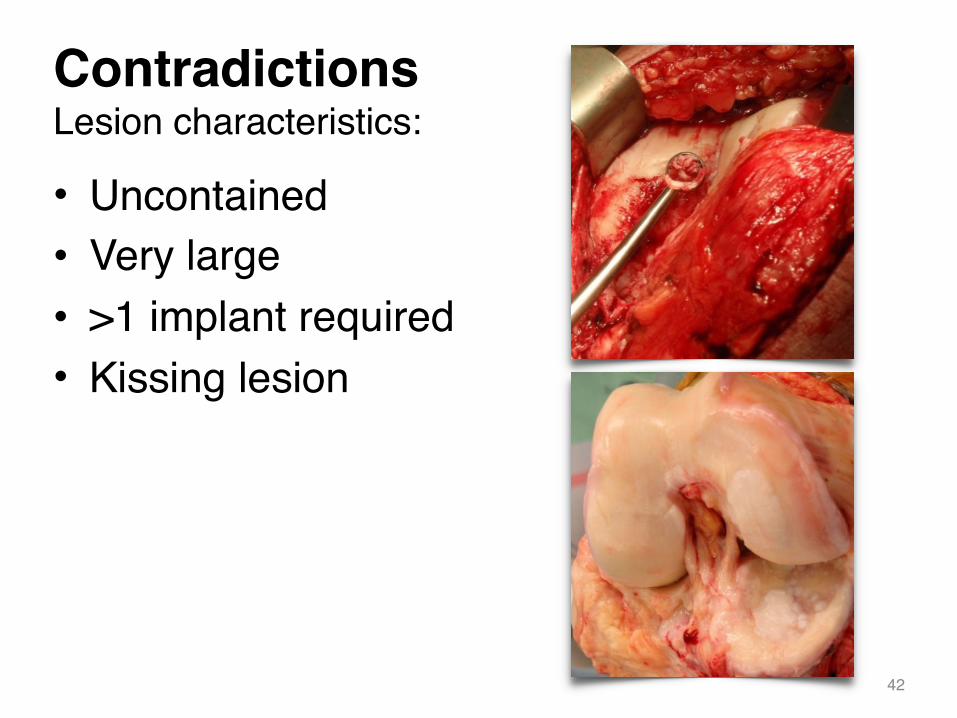
Contradictions Lesion characteristics:
• Uncontained• Very large• >1 implant required• Kissing lesion
42
Contradictions Other joint pathology
• Malalignment
• Laxity
• Major meniscal deficiency
• Subchondral sclerosis
• Advanced degenerative changes43

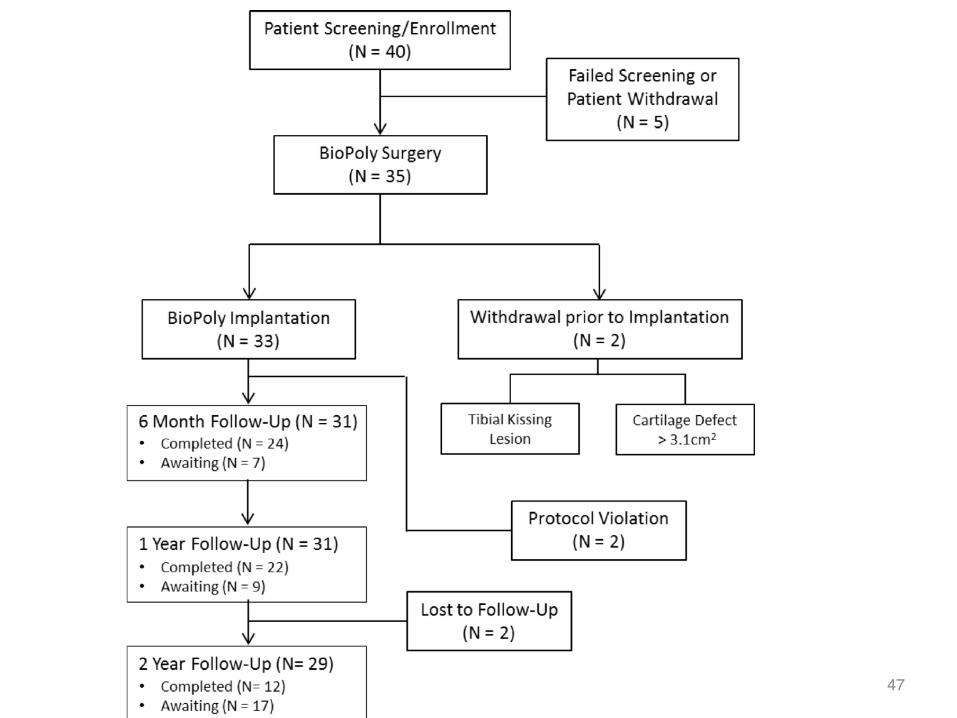
Registry Study: Preliminary Report
44

Study Investigators and Collaborators:Prof Vladimir Bobic - Chester Knee Clinic, Chester, UKProf Mike McNicholas – Aintree, Liverpool, UKMr Dinesh Nathwani - Imperial College, London, UKProf Alister Hart - RNOH Stanmore, London, UKMr Jonathan Miles - RNOH Stanmore, London, UKMatt Hill - Schwartz Biomedical, USAHerb Schwartz - Schwartz Biomedical, USA
45
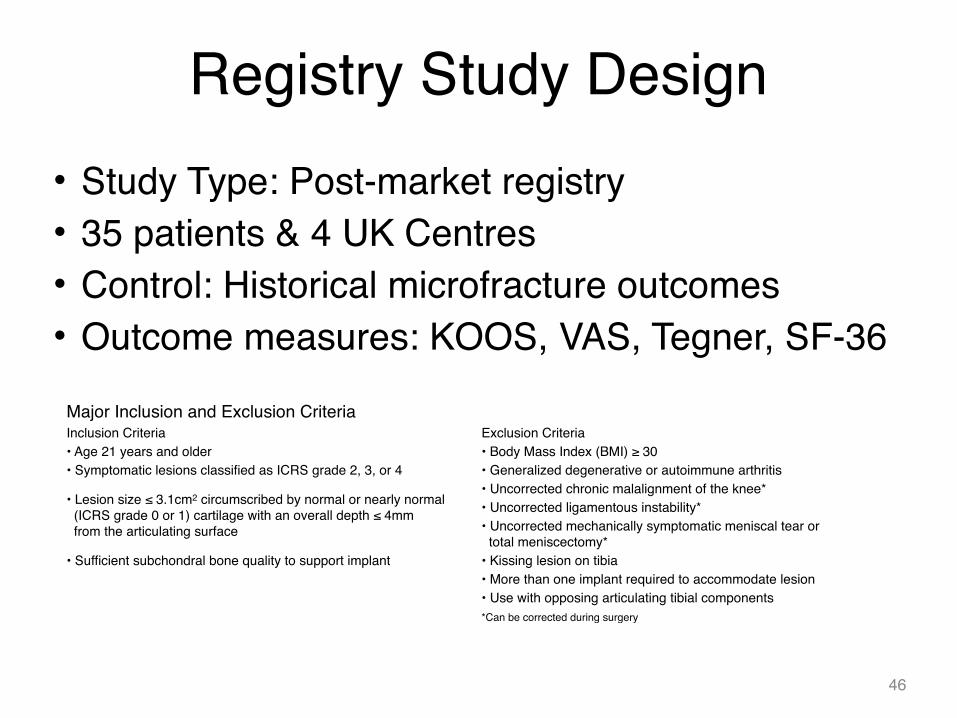
Registry Study Design• Study Type: Post-market registry• 35 patients & 4 UK Centres• Control: Historical microfracture outcomes• Outcome measures: KOOS, VAS, Tegner, SF-36
46
Major Inclusion and Exclusion CriteriaInclusion Criteria Exclusion Criteria• Age 21 years and older • Body Mass Index (BMI) ≥ 30• Symptomatic lesions classified as ICRS grade 2, 3, or 4 • Generalized degenerative or autoimmune arthritis
• Lesion size ≤ 3.1cm2 circumscribed by normal or nearly normal (ICRS grade 0 or 1) cartilage with an overall depth ≤ 4mm from the articulating surface
• Uncorrected chronic malalignment of the knee*• Uncorrected ligamentous instability*• Uncorrected mechanically symptomatic meniscal tear or total meniscectomy*
• Sufficient subchondral bone quality to support implant • Kissing lesion on tibia• More than one implant required to accommodate lesion• Use with opposing articulating tibial components*Can be corrected during surgery
47

Registry Study Results
• Interim results after 2 years indicate:– Significant improvement in
all clinical outcomes– One revision (2.9%) due to
subchondral bone disorder– No differences between
younger and older patients
• Mean Defect size = 2.7cm2
• Over half of patient population (54.3%) failed previous cartilage repair procedures
48
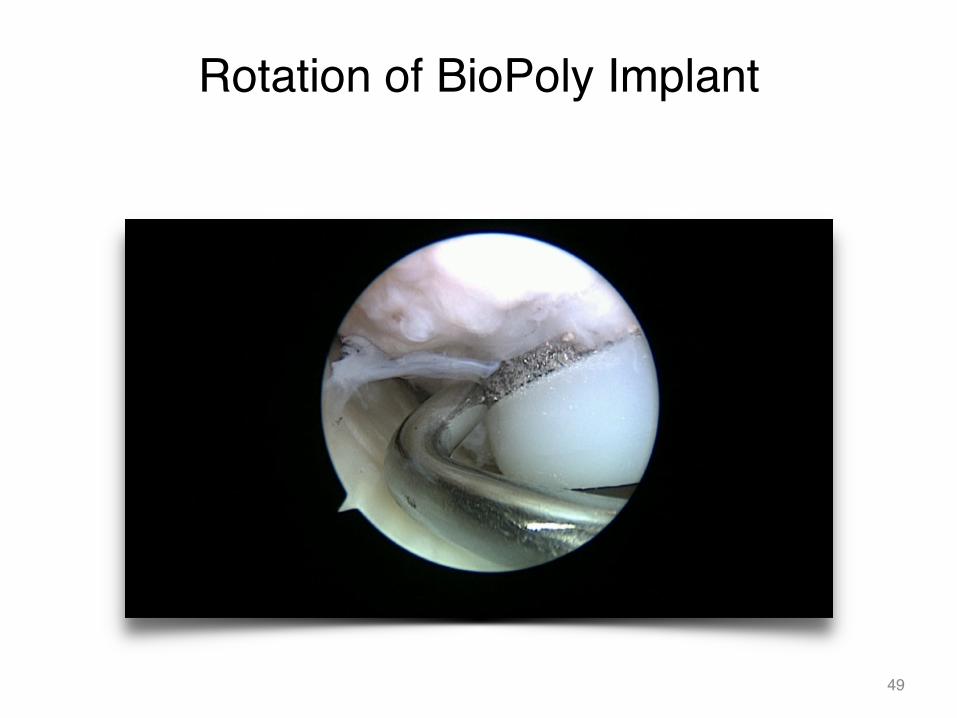
Rotation of BioPoly Implant
49

Failed BioPoly Implant• Why? No structural or technical problems identified. No infection. Patient selection? Surgical technique?• Very difficult to remove! Revised successfully with deep subchondral drilling + ChondroTissue patch.• Possible reasons: inadequate osseous support (previous microfractures + failed MACI = failure of implant
to bone integration)
50
Patient Adverse Events
• 1 Wound infection reported after 1/12– Resolved quickly with medication
• 1 Patient began experiencing pain at 3/12– Arthroscopy revealed implant intact, and loose
cartilage body as source of pain– Removal of loose cartilage body resolved
2symptoms
51

Registry Study Results
• BioPoly compared to historical microfracture outcomes– BioPoly patients on average 7 – 9 years older
• Significantly superior KOOS QoL and Sport after 2 years52

53
Registry Study Results

54

OrthoBiologics vs Metal and Plastic
Hmmm ... not really. Not so soon, but will happen ... 55
Top Related