






Languages
Pages
Legal


8 Biliary Diseases
ANATOMY OF THE EXTRAHEPATIC BILIARY SYSTEM• Anatomy of the biliary system is highly
variable,andthisincludesducts,arteries,veins,andlymphatics.
Common Hepatic Duct• Intrahepatic biliary duct systems converge on
rightandlefthepaticducts.• Right and left hepatic ducts typically form the
commonhepaticduct.• Leftductisusuallylonger.• Junctionoftheductsmaybeintrahepatic(e.g.,
inhepatomegaly).• Accessoryhepaticductscanoccur.• There may be no common hepatic duct
if the cystic duct empties into right and lefthepatic duct junction (bile duct branchvariant).
Gallbladder• NormallyliesbetweenhepaticsegmentsIVand
V, in a ventral fossa between the anatomicalrightandleftlobes
• Ventralsurfacetypicallyliesincontactwiththedescendingpartoftheduodenum.

96 Biliary Diseases
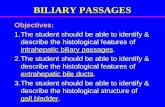
Right and lefthepatic ducts
Commonhepatic duct
(Common)bile duct
Cysticartery
Cystic duct
Gallbladder
Right and lefthepaticarteries
Proper hepaticartery
Commonhepaticartery
Hepatic ductsCystic duct
Right LeftSpiralfold
Smoothpart
Commonhepaticduct
NeckInfundibulum(Hartmann’spouch)
Body
Fundus
Hepatopancreaticampulla (of Vater)
Descending(2nd) part ofduodenum Pancreatic
duct
(Common)bile duct
Viscera: Gallbladder and Extrahepatic Ducts

97 Biliary Diseases
• Peritoneum surrounds fundus and attachesbody and neck to the ventral surface of theliver.
• Hepatic surface of the gallbladder has fibroustissueconnectionstolivercapsule.
• Mucosan Columnarepithelium,nosubmucosan ActivelyabsorbsNa+andwater,concentrating
bile• Smoothmuscleofthefibromuscularlayerispri-
marilyorientedlongitudinally.• Parasympatheticpreganglionicinnervationfrom
left(anterior)vagusfiberscontractsgallbladderandrelaxesbileductsphincter.
• Postganglionic sympathetic fibers from theceliacganglionaredrivenbypreganglionicfibersfromT7-T10spinalsegmentstravelingingreatersplanchnicnerves.
• Visceral afferent fibers (e.g., pain) travel backtoward thoracic spinal ganglia, through theceliac plexus and greater splanchnic nerve,alongsideincomingsympathetics.
Cystic Duct• Proximalportionisconvoluted;spiralfoldkeeps
theductopen.• Distalportionissmooth.• Typical cystic duct joins the common hepatic
ductwellbelow the rightand lefthepaticductjunction.
• Triangle of Calot: classic configuration (shownabove)withcysticductright,commonbileductleft,liverabove,andrighthepaticarterypassingthrough

98 Biliary Diseases
Low unionwith commonhepatic duct
Adherent tocommonhepatic duct
Highunion withcommonhepaticduct
Cystic ductabsent orvery short
Anterior spiraljoining commonhepatic duct onleft side
Posterior spiraljoining commonhepatic duct onleft side
Joiningcommonhepatic duct
Joiningcystic duct
Variations in cystic duct
Accessory (aberrant) hepatic ducts
Joining(common)bile duct
Joininggallbladder Two accessory
hepatic ducts
Variations in Cystic and Hepatic Ducts

99 Biliary Diseases
Cystohepatic Junction• Classicnormal
n High, sub-hepatic origin of the commonhepaticduct
n Joinedinferiorly,atananglefromtheright,bythecysticduct(<3cm)
n Produces the (common) bile duct some dis-tanceabovethedescendingduodenum
• Variationsn Shortorabsentcysticductn Cysticductparalleltohepaticductn Insertionintorighthepaticductn Lowinsertionofcysticduct,crossinganterior
tocommonhepaticduct,insertingbehindtheduodenum
n Low medial insertion of (anterior crossing)cysticductintobileduct
n Lowanterior insertionof(posteriorcrossing)cysticductintobileduct
• Anatomical types of cystohepatic junction:angular,parallel,spiral
Ducts of Luschka• Small biliary ducts that connect directly from
livertothegallbladder• Potential source of leakage following
cholecystectomy
(Common) Bile Duct• Formedbytheunionofhepaticandcysticducts• Portions:supraduodenal,retroduodenal,pancre-
atic,intraduodenal• Bileductsphincter:smoothmusclesurrounding
thedistalendof theduct,partof thecomplexsphincterofOddi

100 Biliary Diseases
Dimensions• 4-8mmdiameternormalundilated• Diametertendstoincreasewithadvancedage.• Heuristic:normalductdiameterinmm=age/10
Hepatopancreatic Ampulla (Vater)• Formedbytheunionofthe(common)bileduct
andthemainpancreaticduct• Ampulla empties posteromedially through the
majorduodenalpapilla(ofVater)intotheretro-peritoneal, descending (second) part of theduodenum.
• Hepatopancreatic sphincter (of Oddi): formedfromacomplexof smoothmuscle surroundingtheterminalpartoftheampullaanditscontrib-utingduct
Bile Secretion• Increased by cholecystokinin (CCK), secretin,
andvagalactivity• Decreased by vasoactive intestinal peptide
(VIP),somatostatin,sympatheticactivity• CCKcausestonicgallbladdercontraction.• Bilemediatesabsorptionoffat-solublevitamins
andexcretionofbilirubinandcholesterol.
VESSELS AND LYMPHATICSArteries• Gallbladderissuppliedbycysticartery,typically
a branch of the right hepatic artery (from thehepatic artery proper, off common hepatic,celiacaxis).
• Source and course of the cystic artery vary widely: this must be carefully determined incholecystectomy.

101 Biliary Diseases
Right hepaticartery
Cystic artery
Cystohepatictriangle(of Calot)
Cystic duct
Commonhepaticduct
(Common)bile duct
Supraduodenalartery
Gastroduodenalartery
Left hepaticartery Common hepatic
artery
Celiac trunk
Biliary System Arteries
• Variants includeorigins fromcommonhepatic,left hepatic, superior mesenteric arteries,passing anterior or posterior to hepatic or bileducts.
• Bile ducts: supplied by branches of posteriorsuperior pancreaticoduodenal, retroduodenal,right,andlefthepaticarteries(celiacaxis)

102 Biliary Diseases
Veins• Cystic veins are variable; veins from the body
typicallypassdirectlyintothelivertodrainintohepaticsinusoids.
• Otherveinsfromtheneckandcysticducttypi-callydraindirectlyintotherightportalvenoussystem, and other veins drain the biliary ductsystem.
Lymphatics• Cysticlymphnodesclusteraroundtheneck.• Cysticlymphaticsalsodrainintohepaticnodes
clusteredaroundtheupperbileduct.• Deeper drainage into celiac nodes around the
arterialtrunk
CLINICAL CORRELATESNormal Bile Production• 500to1000mL/day• Secretin production and meals rich in fats
increasebileproduction.• Bile constituents: electrolytes, bile salts, pro-
teins,cholesterol,fats,andbilepigments• Major salts: cholic, deoxycholic, and chenode-
oxycholic acids; anionic and conjugated withtaurineorglycine
• Contains unesterified cholesterol, lecithin, andfattyacids
• pHof5.6-8.6isnormalrange.n Morealkalineathighersecretionratesn Moreacidicwithproteininmeals
• Cholesterolsolubilityandlackofstoneprecipi-tationdependonabalanceamongcholesterol,bilesalts,andlecithin(inmicelles).

103 Biliary Diseases
Left gastricnodes
Hepaticnodes
Celiac nodes
Pyloricnodes
Cystic node(of Calot)
Pancreatico-duodenalnodes
Hepatic nodesaround bileducts andproper hepaticartery
Lymph Vessels and Nodes of Pancreas

104 Biliary Diseases
• Gallbladderalsosecretesmucus,whichprotectstissuesfromthelyticactionofbile.
Control of Bile Secretion• Bile produced by the liver is shunted to the
gallbladder,withthesphincterofOdditonicallyclosed(betweenmeals).
• Cholecystokininissecretedbyintestinalmucosainresponsetoingestionoffood.
• Gallbladder contracts and pushes bile into theductalsystem.
• Sphincter of Oddi relaxes, and bile is releasedintoduodenum.
Cholelithiasis• Incidence: about 10% of the population, with
mostasymptomatic• Diabetics not at increased risk, though inflam-
matory responses can complicate late-detectedcases,withhigherincidenceofopensurgery
• Onlyabout10%ofbilestonesareradiopaque.• Nonpigmentedstones
n MostcommontypeinU.S.(~75%)n Increasedinsolubilizationofcholesteroln Factors can include cholestasis, increased
H2O reabsorption, Ca2+ nucleation by mucinglycoprotein, and decrease in bile acids andlecithin.
• Pigmentedstonesn Occurrence ~25% in U.S., most common
worldwiden Precipitationofcalciumbilirubinateandinsol-
ublesalts,withsolubilizationofunconjugatedbilirubin

105 Biliary Diseases
Mechanisms of biliary pain
Visceral pain, mediated bysplanchnic nerve, results fromincreased intraluminal pressure and distention caused by suddencalculous obstruction of cystic orcommon duct.
Sites of pain in bilary colic
Sites of pain and hyperesthesiain acute cholecystitis
Patient lies motionlessbecause jarring or respiration increasespain. Nausea is common.
Parietal epigastric or rightupper quadrant pain results fromischemia and inflammation of gall-bladder wall caused by persistentcalculous obstruction of cystic duct.Prostaglandins are released.
Sudden obstruction(biliary colic)
Persistent obstruction(acute cholecystitis)
Calculus in Hartmann’spouch
Edema, ischemia,and transmuralinflammation
Transduodenalview ofbulging of ampulla
Ampullarystone
Calculus in common duct
Cholelithiasis

106 Biliary Diseases
n Black stones may be caused by cirrhosis,hemolyticdisorders,ilealresection,orchronictotalparenteralnutrition(TPN).
n Usuallyfoundonlyinthegallbladder
Diagnostic Procedures• Liverandbiliaryfunctiontests
n Serumalkalinephosphatase:verysensitivetoobstruction; sensitivity increased by isoen-zymedatabloodlevels
n Serumglutamic-oxaloacetictransferase(AST/SGOT)bloodlevels
n Serum glutamate-pyruvate transaminase(ALT/SGPT)bloodlevels
n Lacticaciddehydrogenase(LDH)bloodlevelsn Bloodbilirubinlevels
• Ultrasoundn Often the first test ordered for suspected
biliarytractdiseasen Safe,inexpensiven 95% sensitivity for stones, identifies gallblad-
dermorphologyandmechanicalvs.metabolicsourcesofjaundice
• Endoscopic retrograde cholangiopancreatogra-phy(ERCP)n Catheter from a side-viewing endoscope is
insertedintotheampullaofVater.n Contrastagentisinjected.n Radiographsaretaken.n Devicecanperformsphincterotomyifneeded.n Standing questions: What are indications for
performing an ERCP before a lap chole?Blockedbileduct?May identifyvariantsandreduceinjuries?

107 Biliary Diseases
Cholecystitis• Gallbladderwalldistentionandinflammation• Mostcommoncauseisobstructionofthecystic
ductbyastone.• Classic right upper quadrant pain referred to
rightscapulaandshoulder• Pain mediated by segmental visceral afferent
fibers traveling with the splanchnic nerves (tothoracicspinalsegments)
• Nausea,vomiting,lossofappetite,pain• Symptomsoftenoccurafterfattymeal,withper-
sistentpain.• Murphy’s sign: patient resists deep inspiration
owingtopain,withdeeppalpationofrightupperquadrant
• Ultrasound~95%sensitivityforstones• Risk factors for stones: female, obesity, age
>40y, pregnancy, rapid weight loss, vagotomy,TPN,ilealresection
Cholecystectomy• Laparoscopic cholecystectomy (lap chole)
has been the treatment of choice for manyyears, preferred to formerly traditional opencholecystectomy.
• Complicated laparoscopic case may be con-vertedtoanopencholecystectomy.
• Opencholecystectomyusesconventionalsurgi-cal instrumentswitharightupperquadrantormidlineabdominalincision.
• Lapcholeessentialsn Generalanesthesia,sub-umbilicalincisionfor
CO2(insufflation)trocar

108 Biliary Diseases
n 3trocarsplaced(forlaparoscopeandspecial-izedtools)inrightsubcostalregion
n Retraction of gallbladder, incision of triangleofCalot
n Dissection and ligation of cystic duct andartery
n Dissectionandremovalofgallbladder• Mostcommonbileductinjuriesassociatedwith
laparoscopiccholecystectomyn (Common)bileductmistakenforcysticduct
andtransectedn Variable extent of extrahepatic biliary tree
excisedwithgallbladdern Righthepaticarteryinjuredwithdissection
Gallstone Pancreatitis• Estimated40%ofacutepancreatitiscasesresult
from transient obstruction of pancreatic ductflowbystonesblockingbileductorampullaofVater.
• Mechanismofsuchpancreatitisnotknown• Symptoms: epigastric and radiating back pain,
nausea, vomiting, elevated serum lipase andamylaselevels
• Treatmentcancomplicatethetimingofarelatedcholecystectomy.
• ERCPmaybeneededifanimpactedampullaissuspected.
Carcinoma of the Biliary Tract• Canoccuratanypointalongtheintra-orextra-
hepaticbiliarytreeandgallbladder• Gallbladder carcinoma is the most common
biliary cancer and the fifth most common GIcancer.
Top Related