





Languages
Pages
Legal


WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Biliary and Pancreatic Endoscopy Stones Strictures and IPMN
Sandeep N Patel DO
Director Pancreas Center
University of Texas Health Science Center San Antonio TX USA
Memorial Hermann Gastroentrology amp Hepatology Symposium
February 10 2018
Role of Intraductal Endoscopy Overview
Biliary
bull Stones
bull Indeterminate biliary strictures
Pancreas
bull Stones
bull IPMN
EndoscopicRetrogradeCholangioPancreatography
Diagnosis
Fluoroscopic imaging
Therapy
Sphincterotomy
Stenting
Dilation
Sampling
Intraductal Endoscopy Evolution
Single-Operator technique mother-baby system
2007 1970rsquos
Intraductal Endoscopy Evolution
SpyGlass DS
2015
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Indeterminate biliary strictures and filling defects
Sampling of CBD Strictures ERCP
Yield
ndash brush ~ 30
ndash biopsy ~ 30
bull Serial brushing
bull Dilation and brush
bull Novel brushes
bull ldquoSmashrdquo technique
30-50
Sampling of CBD Strictures Directed biopsies using SpyGlass
bull 56 yo female with recurrent cholangitis
bull Undergoes 3 ERCPrsquos at OSH ndash Filing defect CHDstricture
ndash Brushings biopsies negative for CA
ndash Prematurely occludes stents
bull Referred for management
bull What should we do
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
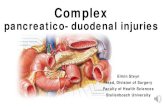
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Role of Intraductal Endoscopy Overview
Biliary
bull Stones
bull Indeterminate biliary strictures
Pancreas
bull Stones
bull IPMN
EndoscopicRetrogradeCholangioPancreatography
Diagnosis
Fluoroscopic imaging
Therapy
Sphincterotomy
Stenting
Dilation
Sampling
Intraductal Endoscopy Evolution
Single-Operator technique mother-baby system
2007 1970rsquos
Intraductal Endoscopy Evolution
SpyGlass DS
2015
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Indeterminate biliary strictures and filling defects
Sampling of CBD Strictures ERCP
Yield
ndash brush ~ 30
ndash biopsy ~ 30
bull Serial brushing
bull Dilation and brush
bull Novel brushes
bull ldquoSmashrdquo technique
30-50
Sampling of CBD Strictures Directed biopsies using SpyGlass
bull 56 yo female with recurrent cholangitis
bull Undergoes 3 ERCPrsquos at OSH ndash Filing defect CHDstricture
ndash Brushings biopsies negative for CA
ndash Prematurely occludes stents
bull Referred for management
bull What should we do
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

EndoscopicRetrogradeCholangioPancreatography
Diagnosis
Fluoroscopic imaging
Therapy
Sphincterotomy
Stenting
Dilation
Sampling
Intraductal Endoscopy Evolution
Single-Operator technique mother-baby system
2007 1970rsquos
Intraductal Endoscopy Evolution
SpyGlass DS
2015
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Indeterminate biliary strictures and filling defects
Sampling of CBD Strictures ERCP
Yield
ndash brush ~ 30
ndash biopsy ~ 30
bull Serial brushing
bull Dilation and brush
bull Novel brushes
bull ldquoSmashrdquo technique
30-50
Sampling of CBD Strictures Directed biopsies using SpyGlass
bull 56 yo female with recurrent cholangitis
bull Undergoes 3 ERCPrsquos at OSH ndash Filing defect CHDstricture
ndash Brushings biopsies negative for CA
ndash Prematurely occludes stents
bull Referred for management
bull What should we do
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Intraductal Endoscopy Evolution
Single-Operator technique mother-baby system
2007 1970rsquos
Intraductal Endoscopy Evolution
SpyGlass DS
2015
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Indeterminate biliary strictures and filling defects
Sampling of CBD Strictures ERCP
Yield
ndash brush ~ 30
ndash biopsy ~ 30
bull Serial brushing
bull Dilation and brush
bull Novel brushes
bull ldquoSmashrdquo technique
30-50
Sampling of CBD Strictures Directed biopsies using SpyGlass
bull 56 yo female with recurrent cholangitis
bull Undergoes 3 ERCPrsquos at OSH ndash Filing defect CHDstricture
ndash Brushings biopsies negative for CA
ndash Prematurely occludes stents
bull Referred for management
bull What should we do
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Intraductal Endoscopy Evolution
SpyGlass DS
2015
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Indeterminate biliary strictures and filling defects
Sampling of CBD Strictures ERCP
Yield
ndash brush ~ 30
ndash biopsy ~ 30
bull Serial brushing
bull Dilation and brush
bull Novel brushes
bull ldquoSmashrdquo technique
30-50
Sampling of CBD Strictures Directed biopsies using SpyGlass
bull 56 yo female with recurrent cholangitis
bull Undergoes 3 ERCPrsquos at OSH ndash Filing defect CHDstricture
ndash Brushings biopsies negative for CA
ndash Prematurely occludes stents
bull Referred for management
bull What should we do
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Indeterminate biliary strictures and filling defects
Sampling of CBD Strictures ERCP
Yield
ndash brush ~ 30
ndash biopsy ~ 30
bull Serial brushing
bull Dilation and brush
bull Novel brushes
bull ldquoSmashrdquo technique
30-50
Sampling of CBD Strictures Directed biopsies using SpyGlass
bull 56 yo female with recurrent cholangitis
bull Undergoes 3 ERCPrsquos at OSH ndash Filing defect CHDstricture
ndash Brushings biopsies negative for CA
ndash Prematurely occludes stents
bull Referred for management
bull What should we do
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Sampling of CBD Strictures ERCP
Yield
ndash brush ~ 30
ndash biopsy ~ 30
bull Serial brushing
bull Dilation and brush
bull Novel brushes
bull ldquoSmashrdquo technique
30-50
Sampling of CBD Strictures Directed biopsies using SpyGlass
bull 56 yo female with recurrent cholangitis
bull Undergoes 3 ERCPrsquos at OSH ndash Filing defect CHDstricture
ndash Brushings biopsies negative for CA
ndash Prematurely occludes stents
bull Referred for management
bull What should we do
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Sampling of CBD Strictures Directed biopsies using SpyGlass
bull 56 yo female with recurrent cholangitis
bull Undergoes 3 ERCPrsquos at OSH ndash Filing defect CHDstricture
ndash Brushings biopsies negative for CA
ndash Prematurely occludes stents
bull Referred for management
bull What should we do
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 1
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Case 2
Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Sampling of CBD Strictures Directed biopsies using Digital SpyGlass
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade Case 3
Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Results from Biopsy of Indeterminate Biliary Strictures ndash Does Direct Visualization Help A Multicenter
Experience
Presented by KF Binmoeller Interventional Endoscopy Services California Pacific Medical Center San Francisco CA
Registry Data tissue acquisition-SpyGlass
Analysis of the data set of indeterminate strictures - intrinsic (intralumenal)
Sensitivity 78 (2127)
Specificity 64 (711)
Positive Predictive Value 95 (2122)
Negative Predictive Value 58 (712)
Analysis of total data set of indeterminate strictures - extrinsic and intrinsic (intralumenal)
Sensitivity 59 (2339)
Specificity 75 (34)
Positive Predictive Value 100 (2323)
Negative Predictive Value 20 (315)
Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Role of single-operator peroral cholangioscopy in the
diagnosis of indeterminate biliary lesions a single-
center prospective study
Ramchandani M Reddy DN Gupta R Lakhtakia S Tandan M Darisetty S
Sekaran A Rao GV
Gastrointest Endosc 2011 Sep74(3)511-9
bull The overall accuracy of SpyGlass visual impression for differentiating malignant from benign ductal lesions was 89 (3236)
bull The accuracy of SpyBite biopsies for differentiating malignant from benign ductal lesions that were inconclusive on ERCP-guided brushing or biopsy was 82 (2733) in an intent-to-treat analysis
Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Can we do even better
bull 58 yo male newly diagnosed PSC
bull Pruritic
bull CA-19 high
bull No dominant strictures
Does he have cancer
Where
Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Sequela
bull Abdomnal pain
bull Jaundice
bull Cholangitis
bull Acute Pancreatitis
ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

ERCP Stone Extraction
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 90
Binmoeller KF Soehendra N et al Endoscopy 1993
ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

ERCP Stone Extraction ldquolimitationsrdquo
Difficult stones
Altered anatomy
Stone(s) above a stricture Intrahepatic stones
Large BD stones (gt2cm)
ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

ERCP Stone Extraction success rate
Techniques Success
Sphincterotomyextraction balloonbasket 80
Mechanical lithotripter 901
1 Binmoeller KF Soehendra N et al Endoscopy 1993
2 Maydeo A Kwek BE et al GIE 2011
EHLLaser ~1002
Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Electrohydrolylic Lithotripsy (EHL)
bull Spark between electrodes at fiber tip
bull Sparks induces a spherical shock wave
bull Shock wave oscillates to fragment the stone
bull Done under direct visualization
Very high energy
Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Author n Clearance Complications
Liguory19 17 94
Bonnel20 50 92 hemobilia = 21
Binmoeller21 65 98 cholangitis = 22
Siegal22 21 86 pancreatitis = 3
Yoshimoto23 31 97 perforation = 3
Adamek24 46 74 hemothorax = 1
Arya25 94 90 bile leak = 1
Piraka18 30 81
Others 138 83
n = 492 89 51492 (10)
Electrohydraulic Lithotripsy for Common Bile Duct Stones
Summary of studies (23) with lt 15 pts
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Light
Amplification by
Stimulated
Emission of
Radiation
Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Various Lasers
bull Several are available
bull Differ in
bull wavelength
bull pulse length
bull pulse energy
Aluminum
Erbium
Holmium Neodymium
Yttrium
Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Why Holmium
bull Wavelength (2120 nm) = water
bull Low pulse length low energy shock wave
Equally effective less traumatic
Vassar et al J Endourol 1999
Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Laser Lithotripsy
bull Pulsed laser causes instantaneous fluid evaporation
bull This induces formation of cavitation bubble
bull Bubble collapse leads to shock wave
ldquo photo-mechanical effectrdquo
bull Bigger the bubble --gt stronger the mechanical effect
HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

HolmiumYAG laser safety data on bile duct epithelium in the porcine model
bull 6 female 50 kg domestic pigs underwent necropsy and the bile ducts
(BD) were explanted
Sandeep Patel Dustin Kiker Joanna Lindsteadt Bryan Hanysak GIE 2009
0
10
20
30
40
50
60
s
8 9 10 12 14 15
W
Median Time to Perforation
Statistically Significant Differences in Time to Perforation
8 W vs 15 W
9 W vs 15 W
10 W vs 15 W
12 W vs 15 W
Pairwise multiple comparison by Dunns Method (Plt005)
Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Refractory Stone Extraction laser lithotripsy
10W with 365 probe
S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

S Patel L Rosenkranz B Hooks P Tarnasky D Fishman I Raijman B Sauer M Kahaleh GIE 2014
Total number of patients 74
Extrahepatic stones 5774 (772)
Intrahepatic stones 874 (103)
Cystic duct stones 474 (54)
Pancreatic stones 574 (68)
Prior failed ERCP attempts micro=14 (1-6)
Sessions needed for ductal clearance micro=12
Patients requiring one session 2331 (742)
Attained ductal clearance
a) biliary
b) pancreatic
67 69 (973) 710 (70)
Procedural time micro=69 min (5-105 min)
Procedural-related complications 374 (41)
74 pts (27 male 47 female mean age of 602 years ranging from 20-96)
underwent holmiumYAG lithotripsy at four participating centers
Holmium-YAG Laser Lithotripsy in the Treatment of Pancreaticobiliary Calculi Utilizing (SpyGlass) A Multi-Center Trial
Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Author n clearance complications
FREDDY
Cho31 52 92 23
Lui32 30 90 7
Kim33 17 88 17
HolmiumYAG
Lee35 10 90 10
Maydeo36 60 100 14
Patel37 69 97 4
Results of Laser Lithotripsy FREDDY and HolmiumYAG
Patel S Rosenkranz L ERCP for stone burden in the bile and pancreatic ducts Clin of North A merica 2012
Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Refractory Stone Extraction laser lithotripsy
12W with 550 probe
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Approach to pancreatic diseases
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Treatment of Pancreatic Stones
pancreatoscopy
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Management of pancreatic duct stones
ESWL
lithotripsy
pancreatoscopy
EHL Laser
Conventional ERCP
therapies
HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

HolmiumYAG for PD stones
Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Shah R Attwell A Raijman I Kahaleh M Fukami N Patel S [abstract] Presented DDW 2012
Per Oral Pancreatoscopy with Intraductal Holmium Laser
Lithotripsy for Treatment of Main Pancreatic Duct Calculi A
Multi-Center US Experience
N=28 (male 12 female 16 = 57yo)
Technical Success 97
Complete Stone Clearance 86
Median sessions 1 (range 1-6)
Clinical improvement 97
Complications 4
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Evaluation of intraductal papillary
mucinous neoplasm
pancreatoscopy
First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

First described in 1982
Proliferation of mucus-producing ductal
epithelial cells
Precancerous lesion
Rate of progression to carcinoma slow
features
Patulous ampullary orifice
Dilated pancreatic duct
Mucus secretion
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Main duct disease Side branch IPMN Combined disease
Intraductal Papillary Mucinous Neoplasm (IPMN) background
Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Management of IPMN Sendai Consensus Guidelines
bull Main Duct IPMN
bull PD gt 10mm
bull Intramural nodules
bull Thickened walls
bull Suspicious or positive cytology
bull Symptomatic
Surgery
Tanaka M et al Pancreatology 201212 198
Sensitivity = 100 Specificity = 25-30
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
ndash Tissue sampling
bull Mucinous vs non-mucinous
bull malignant vs non-malignant
EUS-FNA
Cytology yield = 40-50
Fluid analysis
CEA K-ras LOH MUC 245AC GNAS
Grutzmann R et al Oncologist 2010151294
miRNA
Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Evaluation of Intraductal Papillary Mucinous Neoplasm (IPMN)
Current limitations
Pre-operative planning
bull Whipple
bull Distal pancreatectomy
bull Total pancreatectomy
What is the extent of disease
Is there multi-centric disease (~20)
Hidetoshi et al Cancer 1072567
Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Intraductal Papillary Mucinous Neoplasm (IPMN)
Diagnosis
Treatment
How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

How well does pancreatoscopy dx pancreatic cancers
K Yamao et al Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases Gastrointest Endosc 57 (2003)
115 patients undergoing pancreatoscopy
35 pts with adenocarcinoma 60 pts with IPMN
95 63
Fish-egg
Elevated lesions
Friable mucosa
Papillary projections
Tumor vessels
Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Diagnostic Yield of Pancreatoscopy for IPMN
Author n Sens Specificity
Hara 60 66 87 Tetsuya et al 24 100 100 Yamao et al 60 95 100 Patel et al 32 92 100
Pancreatoscopy
Pancreatoscopy + biopsy
1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

1 Yelamali N Reddy et al Surg Endosc (2012) 263682ndash3685
2 Muira T et al Dig Endosc 201022119
3 Itoi T et al Gastrointest Endosc 200766793
Pancreatoscopy with narrow-band imaging
Enhancement of mucosal vascular pattern Vascular patterns and protrusions are detected more clearly than with white light
White light (400-700nm) vs Blue (415 nm) and Green (540 nm) light
bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

bull Almost all biliary stones can be managed endoscopically
bull Now improved biliary imaging available to all with complimentary modalities coming
Intraductal Endoscopy for Biliary Disease conclusion
Stones and strictures
Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

Intraductal Endoscopy for Pancreatic Disease conclusion
IPMN and Pancreatic duct stones
bull Pancreatoscopy improves diagnostic yield in IPMN
bull Pancreatoscopy may be a useful modality in guiding surgical resection for MD-IPMN
bull Pancreatoscopy with EHLLaser is an effective modality for removal of pancreatic duct stones
WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you

WE MAKE LIVES BETTER
UTHSC SAN ANTONIO
trade
Thank you
Top Related