






Languages
Pages
Legal



CASE PRESENTATION
BY : DR MUHAMMAD UMAR NISARPGT (SURGERY)

PATIENT: XYZ AGE: 50YRS GENDER: FEMALE RESIDENCE: sarghoda D.O.A: 27-07-2015
05/01/2023 3
PATIENT PROFILE :

known diabetic – 16 years
Off and on Pain in RHC – 03 years Off and on nausea/ vomiting - 03 years
05/01/2023 4
Presenting complaints:

PAST HX: C section – 1 year back
SYSTEMIC HX: FAMILY HX: NAD PERSONAL HX:

50 years Old lady lying comfortabely in bed well oriented in time place and person.
B.P : 130/80 mmHg Pulse : 82/min Temp : Afebrile R.R : 19/min
Examination

Pallor : absent Cyanosis : absent Jaundice : absent Thyroid : not enlarge Edema : absent Lymph node : not palpable

Chest: CNS CVS
Abdomen:◦ Soft ◦ Non tender ◦ No visceromegaly◦ BS present
Examination
NAD

Labs Blood CP :
◦ Hb = 11.6 mg/dl , ◦ WBC,s = 6.21 X 109/l ◦ Platelets = 177x 109 /l
RFTs = WNL LFTs = WNL BSR= 16.1mmol/l
Urine RE= Normal
05/01/2023 9

Ultrasound Abdomen Chest XRAY
CholelithiasisNormal study

Open cholecystectomy was done on 29-07-2015
Abdomen was opened via right upper transverse incision
Per op findings were thick walled gall bladder and omental adhesions
Cystic artery ligated Cystic duct tied Gall bladder was removed Homeostasis secured, abdomen closed
Surgery

Patient was stable vitally Abdomen was soft and there was
tenderness at wound site Patient was discharged 2 days after surgery
Post op

Patient presented again in emergency on 5th Aug 2015 with C/O ◦ Pain RHC ◦ Abdominal distention◦ Nausea and anorexia ◦ Yellowish discoloration of sclera◦ Clay colored stool and dark color urine
GPE:◦ Anemia : present◦ Jaundice : present

Abdomen◦ Rt upper transverse scar of cholecystectomy◦ Distended ◦ Tender◦ Guarding ◦ BS +ve

Blood CP : ◦ Hb = 8.6 g/dl , ◦ WBC,s = 16.21 X 109/l ◦ Platelets = 442x 109 /l
RFTs = ◦ Urea: 18.4mmol/l◦ Creat: 314 mmol/l
LFTs = ◦ Bili: 55 umol/l
BSR= 252 mg/dl
Coagulation profile: WNL
Serum Amylase: WNL
labs

Abdomen was opened via previous scar. Suction of almost 2L of bile was done. Per op findings were transected CBD at
cystic duct level with proximal stump of about 3-4cm from confluence and distal stump was approx 2-3 cm.
Peritoneal cavity washed with 8L of fluid. CBD stent placed inside the CBD and end to
end anastomosis done with vicryl 6/0. Drains placed in RHC and in Pelvis. Abdomen closed ASD done
Re-exploration

Kept in ICU for 2 days and in ward for 8 days with daily output in RHC drain of 500-800ml
Thus the patient is considered to be managed on the lines of controlled biliary fistula
Discharged on 12th POD with RHC drain in place
Advised follow up after 2 weeks First post op visit:
◦ Daily output in drain= 400-600ml◦ Abd: soft, non tender◦ LFTs: bili- 26 umol/l◦ Coag : WNL
Post op

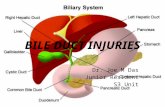
IATROGENIC BILE DUCT INJURIES

Bile duct injuries represent a complex clinical scenario seen with increased frequency owing to ◦aberrant anatomy◦more lap cholecystectomies being performed
Incidence : ◦0.1-0.2 % in open cholecystectomy◦0.4-0.6 % in lap cholecystectomy

HISTORY

Earliest known gall stones - Priestess of Arnan (1085-945 BC) – Egyptian
The first clinical description of gallstone disease - Gordon Taylor, in his description of the symptoms manifested by Alexander the Great in 323 BC

John Stough Bobbs - first elective cholecystostomy in Indianapolis for hydrops of the gallbladder
In 1878 Kocher drained an empyema of gallbladder.

Ludwig George Courvoisier (1843-1918).◦Law (Statistical
article on the pathology and surgery of the biliary system)
◦First choledocholithotomy

First open cholecystectomy
•Dr Carl Johann August Langenbuch (German surgeon)
•July 15, 1882, at Lazarus
Krankenhaus in Berlin

Hans Kehr – invented a T tube
First laparoscopic cholecystectomy
Erich Mühe in Germany in 1985

REVIEW ON SURGICAL ANATOMY


The cranial segments : cystic artery and the hepatic arteries, especially the right (R) hepatic artery.
The caudal segment:pancreaticoduodenal artery through the retroduodenal artery.
The middle segment :is vascularized by an axial network of a varying number of arterial anastomoses between the cranial and caudal supplies.
Blood supply of CBD

60% by the distal vessels
38% by the cranial ones
2% by a nonaxial supply from common hepatic artery
This arterial pattern predisposes the supraduodenal segment of the common bile duct to ischemic damage and resulting
in strictures.
CBD blood supply

space bordered by:
◦ Cystic duct inferiorly,
◦ Common hepatic
artery medially
◦ Superior border of the cystic artery
Calot’s triangle(Cystohepatic triangle)

Variations in cystic duct


Iatrogenic injury Cholecystectomy Gastrectomy Pancreatectomy ERCP
Trauma
Bile Duct Injuries (BDI)

Inflammation in the porta,Variable biliary anatomy, Inappropriate exposure,Aggressive attempts at hemostasis,Surgeon inexperience. 97% due to visual misperception, only 3% accounts for
technical skills and knowledge.
Risk factors

Misperception .. With sufficient cephalad retraction of the gall
bladder fundus ,the cystic duct overlies the common hepatc duct running in a parrellel path. without inferolateral traction of the gallbladder infundibulum to dossociate this structures, the dissection of apparent cystic duct may actually include CBD…

Acute inflammation and scarring of the triangle of calot.
Acute cholecystitis. Acute pancreatitis. Chronic cholecystitis. Mirizzi syndrome Perforated duodenal ulcer.
Complicated pathology

Cephalad and lateral retraction of gall bladder is necessary to expose the structures.
Cautious retraction in case of acute inflammation or gangrenous gall bladder.
Avoid application of clips too close to the cystic duct CBD junction.
Technical errors

Avoid strenous dissection too close to the CBD.
Blind application of clips to achieve hemostasis.
Willingness to convert to open technique.
Early in the surgeons learning curve.

Use of electrocautery Avoided near the CBD Bipolar cautery is better. Avoid usage near metallic clips Low intensity for short duration
Thermal and laser injuries

CLASSIFICATION

Era of Open Chole
Based upon level of biliary strictures with respect to hepatic bifurcation
Type 1-5.
Helps surgeon choose appropriate site for repair
Bismuth classification (1982)


A drawback of the Bismuth classification is that patients with limited strictures, isolated right hepatic duct strictures, or cystic duct leaks cannot be classified

Strasberg classification is able to classify all types of injury and is used extensively in describing bile duct injuries associated with laparoscopic cholecystectomy

BL from minor duct◦ Cystic duct leak◦ Liver bed leak◦Accessory duct leak
Communication between liver and duodenum via major ducts unaffected
Type A

Occlusion of the part of biliary tree
Usually due to Rt abberant duct ligature
May be segmental,sectorial, main RHD
Type B

Transection of aberrant right hepatic ducts
Similar to B but…
Presents and treated differently from B
Type C

Lateral injury to main extrahepatic bile ducts
Similar to A◦Bile collection
Dissimilar to A◦Location on the main biliary tree
◦Consequences more severe RHD, CHD, CBD may be involved
Type D

E: injury to main duct (Bismuth) E1: Transection >2cm from confluence
E2: Transection <2cm from confluence
E3: Transection in hilum E4: Seperation of major ducts in hilum
E5: Type C plus injury in hilum
Type E

McMahon
Amsterdam Academic Medical Center's classification (1996)
Neuhaus' classification (2000)
Csendes' classification (2001)
CUHK (Chinese University of Hong Kong), 2007
Other classifications

What are the clinical features ?

The common clinical symptoms are jaundice, fever, chills, and epigastric pain.
divided into two groups.
patients with bile leaks, If the subhepatic region is not drained, subhepatic bile collection (biloma) or abscess develops. ◦ fever, abdominal pain and other signs of sepsis
occur. ◦ Generally, jaundice is not observed in these
patients because cholestasis does not appear.
patients with biliary strictures, jaundice is the commonest clinical symptom caused by cholestasis .

Is it possible to detect these injuries intra operatively?

Fletcher et al. in 1999 found that intraoperative cholangiography had a protective effect for complications of cholecystectomy in a retrospective study of 19,000 cholecystectomies.
Routine intraoperative cholangiography

Cholangiogram abnormalities:◦Failure to opacify the proximal hepatic ducts◦Narrowing of the CBD at the site of cholangiogram catheter insertion
Bile drainage:◦Drainage of bile from any location other than a lacerated gallbladder
◦Bile draining from a tubular structure
Intraoperative clues to a bile duct injury

Clipped duct is not fully encompassed by a standard clip (9mm)
Presence of another unexpected ductal structure
A large artery (RHA) behind the duct
Extra lymphatic &vascular structure seen
Proximal hepatic ducts fail to opacify on IOC
Suspect CBD, not cystic duct, if..

◦Second cystic artery, this may be the right hepatic artery
◦Lymphatics surrounding the duct or more tissue around the cystic duct than is usually encountered, this indicates that the dissection is in the porta
◦Fibrous tissue in the gallbladder bed, indicates transection of the proximal hepatic ducts
Anomalous anatomy:

How to prevent?

Proper selection of cases
In LC of obese patients, place the optical port little higher up from the umbilicus to avoid the tangential view of the Calot’s triangle.
Always dissect to the right of the line joining the right free margin of lesser omentum to cystic node.

While dissecting the Calot’s triangle stay close to the GB.
It is advised that Calot’s triangle is dissected in such a way that the retro-infundibular window is opened first and then the window between the cystic artery and duct is opened. Visualisation of the double window is called “Critical view of Strasberg”.

The technique of “critical view of safety” of Strasberg
Calot’s triangle is completely unfolded by mobilizing the gallbladder neck from the gallbladder bed of the liver before transecting the cystic artery and duct

Vessels pulsating before clipping should be considered as hepatic artery until proved otherwise.
While dissecting GB from the liver bed stay close to the GB and avoid any injury to abnormally superficial right anterior sectoral duct.

Once the Calot’s triangle is fully dissected and cystic artery has been clipped and cut, GB is left attached medially to only one structure, CD.
If the plane between the liver and GB is absent, it might be better to leave a part of posterior GB wall adhered to the liver bed and cauterise its mucosa

The cystic duct and the GB neck and infundibulum together looks like Lord Ganesha’s trunk and head (or elephant’s trunk and head) respectively and so also called as Lord Ganesha’s sign.

In case of excessive bleeding during the lap surgery:
Have a low threshold for conversion.
If there is continuous ooze from the inflammed surface, liberal irrigation and aspiration should be used.
If there is sudden arterial spurt, compress the area temporary with small gauge or atraumatic grasper. Irrigate / aspirate and clean the operative field. Effectively control the bleeding vessel with left hand grasper, identify the vessel and arrest bleeding with clips or bipolar electrocautery.

MANAGEMENT

HOW ESSENTIAL IS TO TREAT BILE DUCT INJURIES?

Most bile duct injuries or strictures occur as a result of cholecystectomy for symptomatic gallstone disease.
The majority of these patients are young (40–50 years), female, have a long life expectancy, and are in the most productive years of their life.

Biliary strictures may result in significant morbidity and mortality secondary to complications such as biliary cirrhosis , cholangitis, portal hypertension.
Because of this, it is essential that these patients have prompt recognition of their problem and a reliable treatment with a long-term success rate.

WHAT ARE THE FACTORS ONE SHOULD CONSIDER BEFORE
TREATING BILE DUCT INJURIES?

1.Timing of diagnosis ◦ Intra-operative◦ Early post-op ◦ Late post-op
2.Extent and level of injury
3.Patient presentation
4.Hospital setup

WHAT ARE THE TREATMENT OPTIONS AVAILABLE ?

1) Surgical Management 2) Interventional Radiologic Techniques 3) Endoscopic Techniques Most of these injuries and strictures are best
repaired surgically. SURGERY - GOLD STANDARD

A multidisciplinary approach The team consisting of experienced
interventional radiologists, endoscopists, and surgeons, coordinated by an experienced hepatobiliary surgeon

PRE-OPERATIVE MANAGEMENT

Early post-op period Sepsis /SIRS Treat with –Broad spectrum antibiotics -Percutaneous biliary drainage - Percutaneous/operative
drainage of bilomas
No hurry for surgical repair ◦ Friable tissue ◦ Retraction of small ducts

Next step- Pre-op cholangiography (to define anatomy)
Control bile leak with percutaneous stents
Delayed surgical repair

Late post-op period Strictures Cholangitis Treat with- Broad spectrum antibiotics
Urgent cholangiography
Biliary decompression Transhepatic biliary drainage Endoscopic drainage + stent
Surgical repair

If patient presents only with jaundice & no cholangitis
ERC / PTC - to define anatomy
In these cases biliary decompression has not been demonstrated to improve outcome
Surgical repair

Sahajpal et el retrospective medical record review of 69
patients who underwent repair after LC-BDIs
BDIs were classified into 3 groups based on timing of repair from time of injury.◦ Immediate repair (0-72 hours of LC)◦ Intermediate (between72 hours and 6weeks after
LC)◦ Late (after 6weeks)
Patients who underwent repairs in the intermediate period were at a significantly higher risk of developing biliary stricture
Literature review…

De Reuver et al investigated the influence of timing of repair on outcome
3 groups of patients were defined.◦ Acute repair: Within 6 weeks ◦ Delayed repair: After 6 weeks ◦ Late Repair:
Repair in the acute phase after injury is associated with long term stricture formation.
Cont’d….

INTRA OPERATIVE MANAGEMENT

Intra-operatively, any suspicious biliary injury
1) Intra-op cholangiography +/- Careful dissection 2) Lap to open conversion is often
necessary
Isolated, small, non–cautery-based partial lateral bile duct injury Placement of a T tube

Injury involves <50% of the circumference of the bile duct wall
Primary closure over a T-tube

More extensive biliary injury Significant thermal damage owing to
cautery-based trauma Injury involving >50% of the circumference
of the bile duct wall
End-to-side choledochojejunostomy with a Roux-en-Y loop of jejunum should be performed

MANAGEMENT OF HEPATIC DUCT INJURIES

Major bile duct injuries, including transections of the common common hepatic duct, can be repaired.
Isolated hepatic ducts smaller than 3 mm or those draining a single hepatic segment can be safely ligated.
Ducts larger than 3 mm are more likely to drain several segments or an entire lobe and need to be reimplanted.

TECHNICAL ASPECTS OF SURGICAL REPAIR

The choice and technique of repair correlates with the success rate.
End-to-end anastomosis- The common duct (or common hepatic duct) has been divided and there is sufficient length to perform an end-to-end anastomosis without tension

Unsuccessful :1.When repaired at the initial open cholecystectomy
The reasons for the high failure rate of end-
to-end biliary anastomoses relate to ischemia and tension.

Roux-en-Y hepaticojejunostomy
Has the best success rate for the repair of a transection injury of CBD/CHD

Certain technical factors for a successful hepaticojejunostomy are
• Preoperative eradication of intra-abdominal infection
• Viable ductal tissue (excise damaged ductal tissue)
• Single-layer mucosa-to-mucosa anastomosis
• Fine, monofilament, absorbable suture• Alleviate tension on the anastomoses

Stenting
Stenting is useful, however, when very small ducts are repaired
For other injuries stenting may not be required.

OVERVIEW

Suspected CBD injury during lap-cholecystectomy
Intra-op cholangiogram
Partial injury(<30%) Primary repair over T-tube
Extensive injury(>30%) Roux en Y choledochojejunostomy
Complete transection Roux en Y.
Injury to isolated hepatic duct
>3mm Reimplantation or reconstruction by Roux en Y hepaticojejunostomy
<3mm Ligate

Role of Interventional Radiology

Interventional radiologic techniques are useful in patients with bile duct injuries, leaks, or postoperative strictures.

These techniques allow
1)Percutaneous drainage of abdominal fluid collections
2)Preoperative identification of the ductal anatomy through percutaneous transhepatic cholangiography
3)Stricture dilation with or without placement of palliative stents for bile drainage in the patient whose overall physiologic status precludes a major operation.

◦Intrahepatic ductal disease
◦ERCP is not possible
◦Adjunct to operative repair in order to assist with identification of the proximal biliary tree for reconstruction and for the dilation of anastomotic strictures
Percutaneous transhepatic biliary dilatation

ROLE OF ENDOSCOPIC DILATATION IN BILIARY
STRICTURES

Adjunctive option in patents with a dominant extrahepatic stricture causing clinical symptoms.
Requires multiple sessions of dilations
Nonischemic strictures (anastomotic strictures) respond best.

Metalic stents are more durable than plastic stents
Endoscopic dilation also has a low mortality rate, but it has a significant morbidity rate.

Complications following endoscopic biliary interventions:◦Hemobilia◦Bile leak◦Pancreatitis◦Cholangitis ◦Re-stricture

POST-REPAIR COMPLICATIONS

1. Cholangitis2. Pancreatitis3. Stent occlusion4. Stent migration5. Ductal perforation6. Restricturing7. Biliary fistula8. Hemobilia

Surg Clin N Am 90 (2010) 787-802 Surg Clin N Am 88 (2008) 1329-1343 Schwartz's Principles of Surgery, 9e Sabiston Textbook of Surgery, 17e Bailay and love 26th e Ajay K. Sahajpal et al. Arch Surg.
2010;145(8):757-763. de Reuver et al. Ann Surg. 2007;245(5):763-
770.
References

THANK YOU
Top Related