







Languages
Pages
Legal


AuthorsInstitutions

Background
Rib fractures are the most common thoracic injury
Rib fractures are associated with an increase in hospital morbidity and mortality
Pulmonary function can be compromised
Pain control is critical in decreasing the pulmonary complications
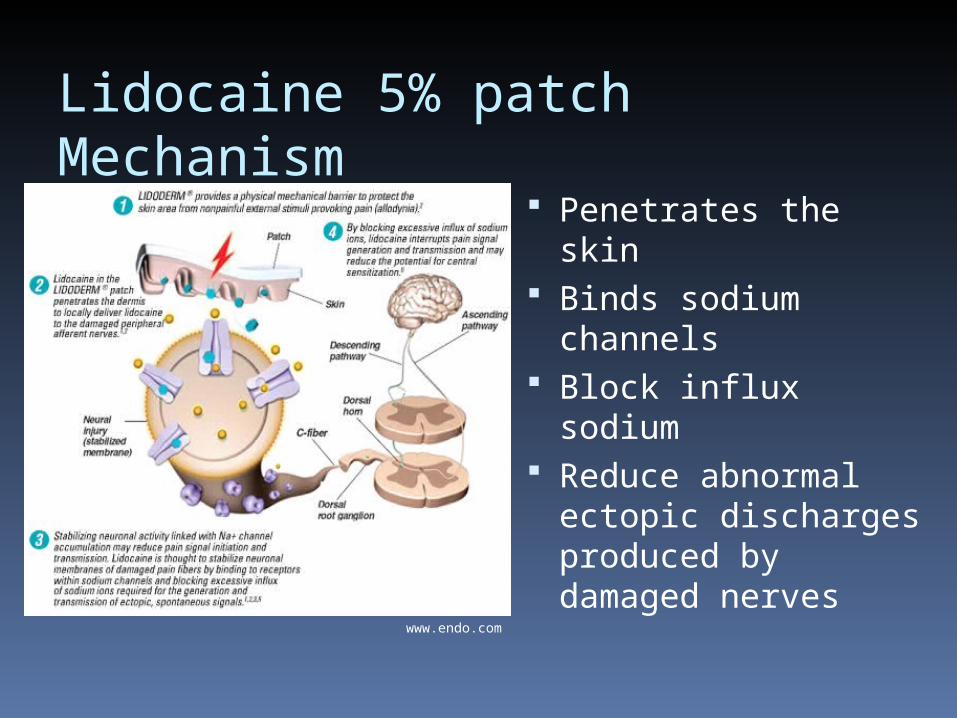
Lidocaine 5% patch Mechanism
Penetrates the skin Binds sodium
channels Block influx
sodium Reduce abnormal
ectopic discharges produced by damaged nerves
www.endo.com
Lidocaine Patch Use
FDA Approval: Post herpetic neuralgia
Other Studies: Back pain Headache Postoperative pain after lap ventral
hernia repair Trauma patients with rib fractures
Hypothesis
The lidocaine patch would reduce the amount of narcotic pain medication used by hospitalized traumatically injured patients with rib fractures.
Study Design
Randomized, double blinded placebo controlled Level I evidence
Setting Spectrum Health – Butterworth Hospital Jan 2007 – Aug 2008

Intervention
Randomized trauma patients with rib fractures to receive either Lidocaine or placebo patch
Data collected for 72 hoursAge
Sex
Injury Severity Score
History of asthma/COPD
Mechanism of injury
Number of rib fractures
Chest tube placement
History of tobacco use and current use

Patch Specifics
10 x 14 cm 5% lidocaine applied to non-woven
polyester felt backing 700 mg lidocaine, 3 + 2% absorbed Mean blood concentration 0.13
µg/mL (1/10 of the therapeutic concentration for arrhythmias)

Outcome Variable Assessment 10 point pain scale administered by
nursing Pain assessments were conducted per
hospital protocol (each shift and prior to administering pain medication)
IV and PO narcotic pain medications were analyzed independently
Incidence of pulmonary complications Length of stay
Patients
Inclusion Criteria Trauma patients with rib fracture on
CT/Xray Age > 18 years of age
Exclusion Criteria Inability to communicate a pain score Inability to use an incentive spirometer History lidocaine allergy Open wounds at the site of patch
application
Primary Outcome
Decrease narcotic use when use lidocaine patch after trauma injury with rib fracture

p = 0.88
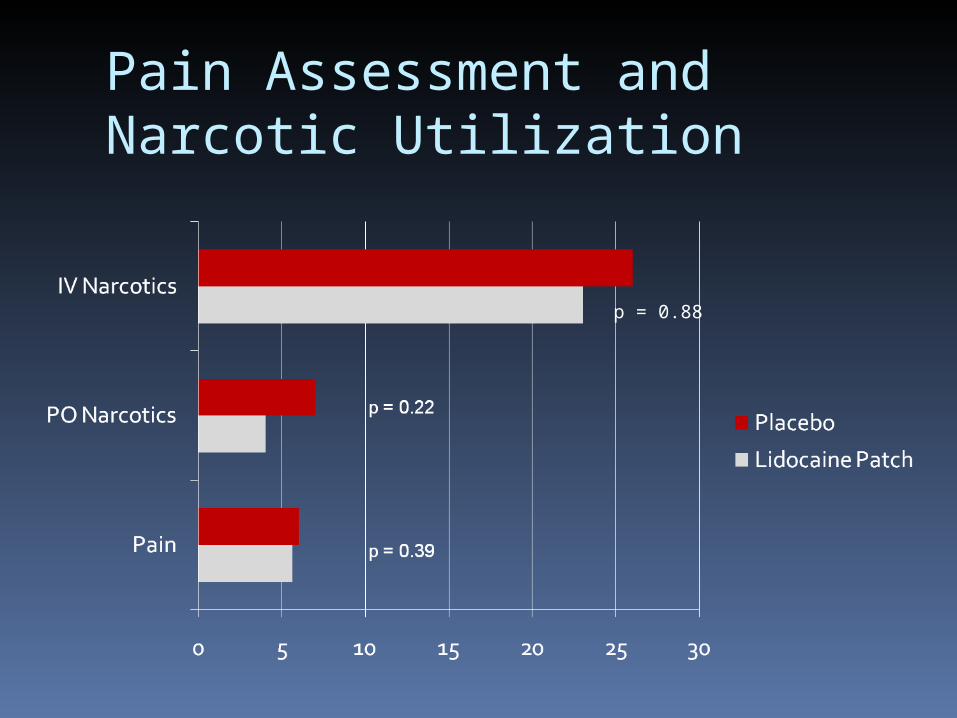
Pain Assessment and Narcotic Utilization
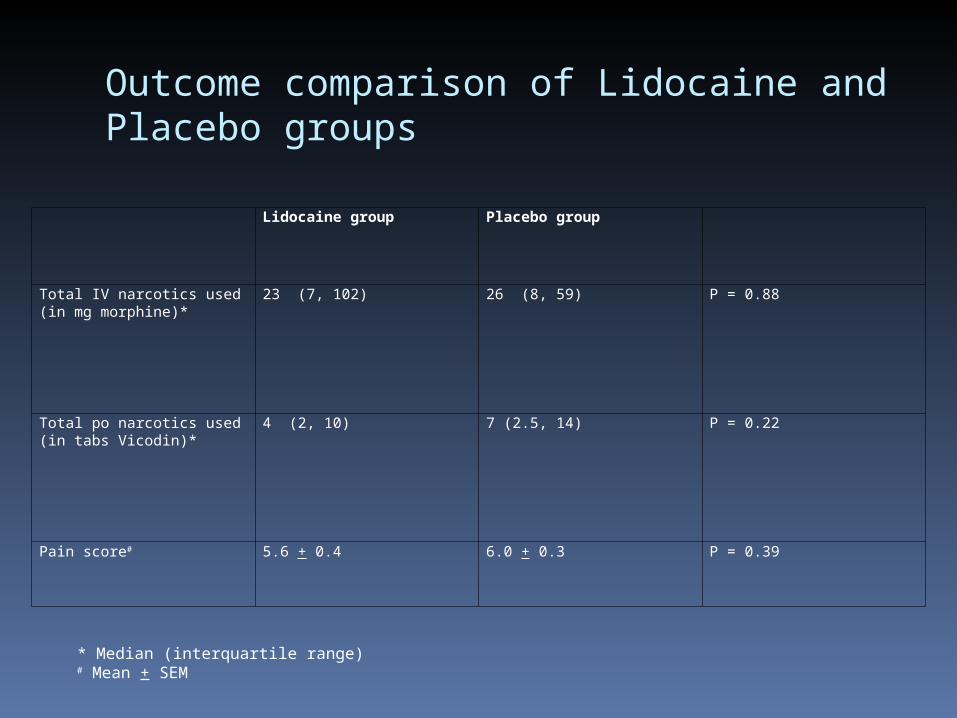
Outcome comparison of Lidocaine and Placebo groups
Lidocaine group Placebo group
Total IV narcotics used (in mg morphine)*
23 (7, 102) 26 (8, 59) P = 0.88
Total po narcotics used (in tabs Vicodin)*
4 (2, 10) 7 (2.5, 14) P = 0.22
Pain score# 5.6 + 0.4 6.0 + 0.3 P = 0.39
* Median (interquartile range)# Mean + SEM
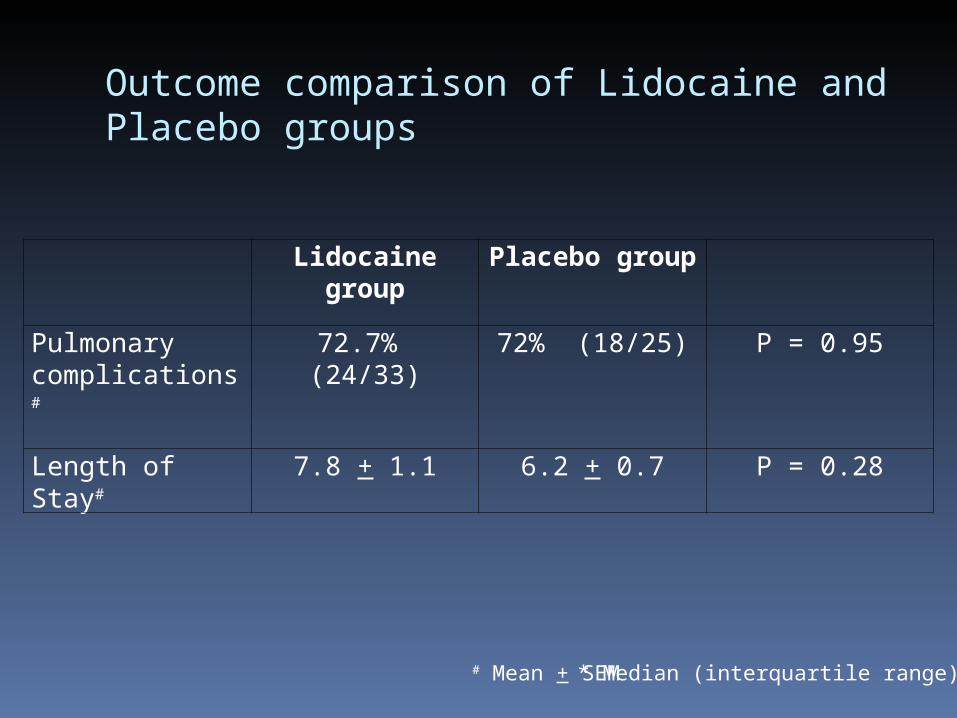
Outcome comparison of Lidocaine and Placebo groups
Lidocaine group Placebo group
Pulmonary complications#
72.7% (24/33) 72% (18/25) P = 0.95
Length of Stay# 7.8 + 1.1 6.2 + 0.7 P = 0.28
# Mean + SEM
* Median (interquartile range)
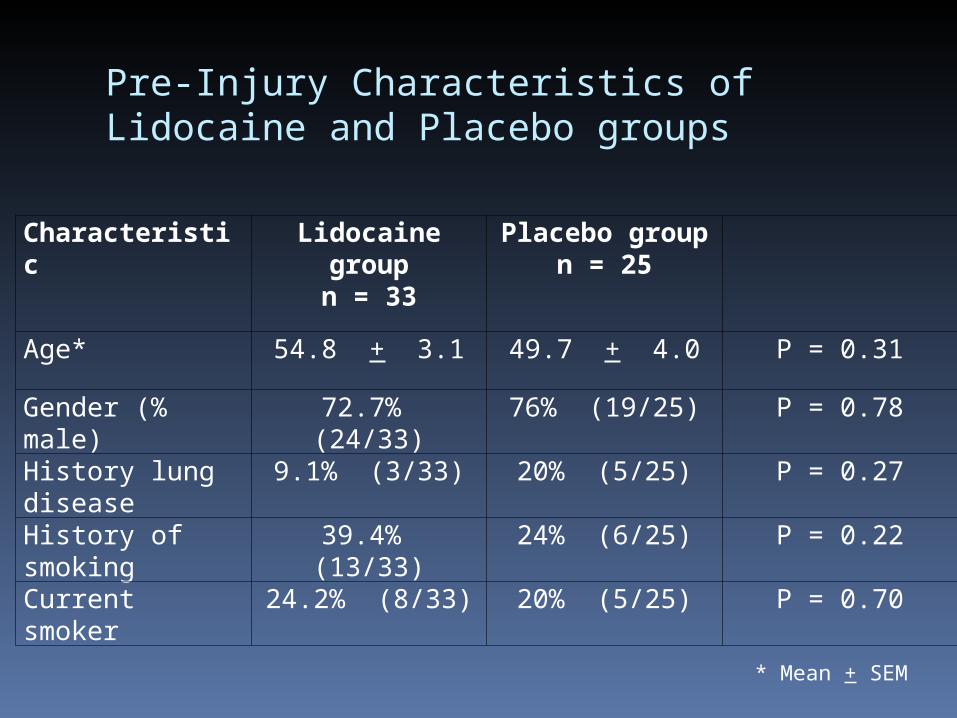
Pre-Injury Characteristics of Lidocaine and Placebo groups
Characteristic Lidocaine groupn = 33
Placebo groupn = 25
Age* 54.8 + 3.1 49.7 + 4.0 P = 0.31
Gender (% male) 72.7% (24/33) 76% (19/25) P = 0.78
History lung disease 9.1% (3/33) 20% (5/25) P = 0.27
History of smoking 39.4% (13/33) 24% (6/25) P = 0.22
Current smoker 24.2% (8/33) 20% (5/25) P = 0.70
* Mean + SEM

Mechanism of Injury
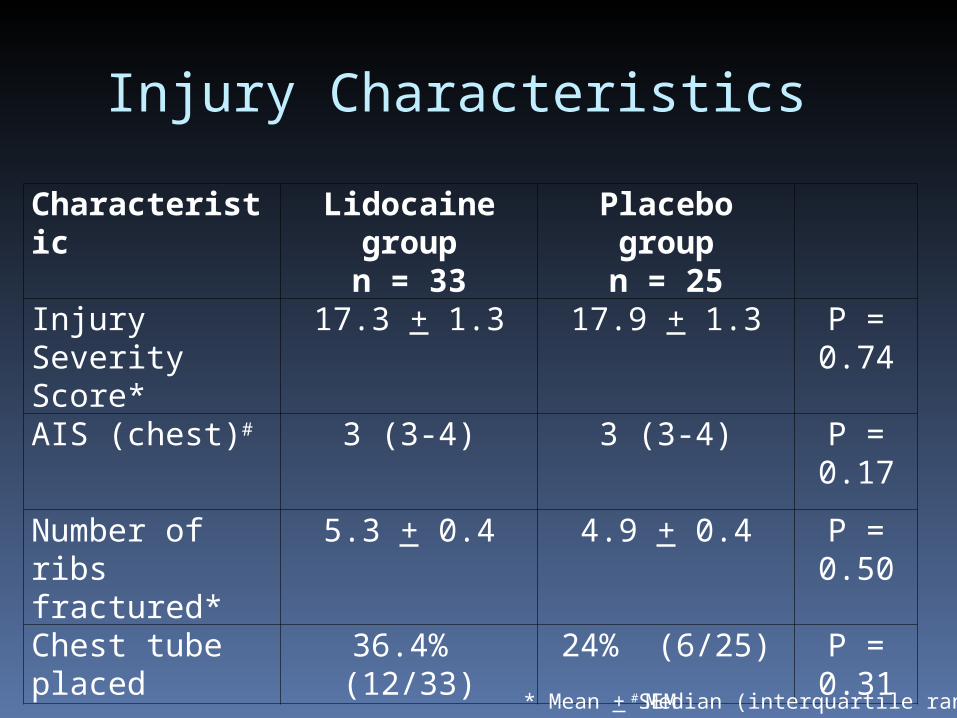
Injury Characteristics
Characteristic Lidocaine groupn = 33
Placebo groupn = 25
Injury Severity Score*
17.3 + 1.3 17.9 + 1.3 P = 0.74
AIS (chest)# 3 (3-4) 3 (3-4) P = 0.17
Number of ribs fractured*
5.3 + 0.4 4.9 + 0.4 P = 0.50
Chest tube placed 36.4% (12/33) 24% (6/25) P = 0.31
* Mean + SEM# Median (interquartile range)
Lidocaine Patch in Trauma Patients
Zink et al. Oregon Health & Science University. Presented at EAST. January 2009 Retrospective 29 patients each group Lidocaine 5% patch patients had
decreased pain scores, but no difference in narcotic use
Conclusion: Further prospective studies needed

Conclusions
Lidocaine patches do not decrease narcotic pain medication use in hospitalized trauma patients with rib fractures
No difference in pain scores pulmonary complications length of stay
Should not be routinely used in multi-system trauma patients with rib fractures
Top Related