



![ASCO Numatics Company product presentation - · PDF file[File Name or Event] Emerson Confidential 27-Jun-01, Slide 1 ASCO Numatics Company product presentation A marine paper can set](https://static.fdocuments.net/doc/165x107/5a7703df7f8b9aea3e8db31b/asco-numatics-company-product-presentation-emerson-a-file-name-or-event.jpg)



Languages
Pages
Legal


ASCO 2015 Investor EventMay 31, 2015

Forward Looking Statements and Adjusted Financial Information
This presentation contains forward-looking statements, which are generally statements that are nothistorical facts. Forward-looking statements can be identified by the words “expects,” “anticipates,”“believes,” “intends,” “estimates,” “plans,” “will,” “outlook” and similar expressions. Forward-looking, , , p , , p gstatements are based on management’s current plans, estimates, assumptions and projections, andspeak only as of the date they are made. We undertake no obligation to update any forward-lookingstatement in light of new information or future events, except as otherwise required by law. Forward-looking statements involve inherent risks and uncertainties, most of which are difficult to predict andare generally beyond our control Actual results or outcomes may differ materially from those impliedare generally beyond our control. Actual results or outcomes may differ materially from those impliedby the forward-looking statements as a result of the impact of a number of factors, many of whichare discussed in more detail in our Annual Report on Form 10-K and our other reports filed with theSecurities and Exchange Commission.
In addition to unaudited financial information prepared in accordance with U.S. GAAP, thispresentation also contains adjusted financial measures that we believe provide investors andmanagement with supplemental information relating to operating performance and trends thatfacilitate comparisons between periods and with respect to projected information. These adjustedmeasures are non-GAAP and should be considered in addition to but not as a substitute for themeasures are non GAAP and should be considered in addition to, but not as a substitute for, theinformation prepared in accordance with U.S. GAAP. We typically exclude certain GAAP items thatmanagement does not believe affect our basic operations and that do not meet the GAAP definitionof unusual or non-recurring items. Other companies may define these measures in different ways.Further information relevant to the interpretation of adjusted financial measures, and reconciliations
f th dj t d fi i l t th t bl GAAP b f d
2
of these adjusted financial measures to the most comparable GAAP measures, may be found onCelgene’s website at www.Celgene.com in the “Investor Relations” section.

Jackie Fouse, PhDPresident, Global Hematology & Oncology

Agenda
Welcome/ Introduction Jackie Fouse, PhD
Clinical Update Jay Backstrom, MD
Celgene and Immuno-Oncology Rob Hershberg, MD PhD
W U J ki F PhDWrap-Up Jackie Fouse, PhD
Q&A
4

ASCO 2015: Presentations Across Our Portfolio
TOPIC ABX LEN POM AZA CC 486 Durvalumab Other TotalTOPIC ABX LEN POM AZA CC-486 Durvalumab (MEDI4736)
Other Total
Breast Cancer 8 8
Lung Cancer 2 2
Pancreatic Cancer 7 1 1 9
MM 11 3 3 17MM 11 3 3 17
Myeloid Disease 2 1 1 1 5
Lymphoma 9 9
Other 6 2 1 2 11
TOTAL 23 22 3 2 3 1 7 61
5
Abstract count includes all studies with a Celgene product
5

Jay Backstrom, MD SVP, Global Hematology & Oncology Clinical R&D

Agenda
Advancing ABRAXANE®1 Advancing ABRAXANE®1 Advancing ABRAXANE®1 Advancing ABRAXANE®1
Ongoing Progress in Myeloma2 Ongoing Progress in Myeloma2
Expanding into Lymphoma3 Expanding into Lymphoma3
7

Agenda
Advancing ABRAXANE®1 Advancing ABRAXANE®1 Advancing ABRAXANE®1 Advancing ABRAXANE®1
Ongoing Progress in Myeloma2 Ongoing Progress in Myeloma2
Expanding into Lymphoma3 Expanding into Lymphoma3
8

Treatments in Pancreatic Cancer
AdjuvantAdjuvant
Neoadjuvant/ Borderline
Neoadjuvant/ Borderline Gemcitabine monotherapyGemcitabine monotherapy
Gemcitabine monotherapyGemcitabine monotherapyAdjuvant(~10K pts)Adjuvant(~10K pts)
Borderline Resectable (~2K pts)
Borderline Resectable (~2K pts)
Locally Advanced(~17K pts)
Locally Advanced(~17K pts)
Gemcitabine monotherapyGemcitabine monotherapy
ChemotherapyChemotherapy
1st Line Metastatic(~64K pts)
1st Line Metastatic(~64K pts)
(~17K pts)(~17K pts)
ABRAXANE®/GemcitabineABRAXANE®/Gemcitabine
2nd Line Metastatic(~26K pts)
2nd Line Metastatic(~26K pts) ChemotherapyChemotherapy
9
Footnote: Patient numbers are estimates of annual treated patients in US and EU G5
9

Clinical Development in Pancreatic Cancer
AdjuvantAdjuvantAdjuvant Adjuvant
Neoadjuvant/ Borderline
Neoadjuvant/ Borderline
Adjuvant(~10K pts)Adjuvant(~10K pts)
Multiple Investigator
Registration StudyAPACT
Registration StudyAPACT
Borderline Resectable (~2K pts)
Borderline Resectable (~2K pts)
Locally Advanced(~17K pts)
Locally Advanced(~17K pts)
Neoadjuvant studies
Locally advanced LAPACT
Locally advanced LAPACT
1st Line Metastatic(~64K pts)
1st Line Metastatic(~64K pts)
(~17K pts)(~17K pts)
Elevated BilirubinElevated Bilirubin
LAPACTLAPACT
>50 AG + novel therapy ongoing
2nd Line Metastatic(~26K pts)
2nd Line Metastatic(~26K pts)
10
Footnote: Patient numbers are estimates of annual treated patients in US and EU G5Celgene-sponsored trials IITs or Cooperative Group trials
10

Pancreatic Cancer Abstracts of Interest at ASCO 2015
Author Abstract Title
Hidalgo #4118 A Phase Ib Study of the Anti-Cancer Stem Cell Agent Demcizumab and Gemcitabine +/- Paclitaxel Protein Bound Particles in Pts with Pancreatic Cancer Poster, Monday
Hingorani #4006 High Response Rate and PFS with PEGPH20 Added to nab-P lit l/G it bi i St IV P i l U t t d P tiPaclitaxel/Gemcitabine in Stage IV Previously Untreated PancreaticCancer Patients with High-HA Tumors: Interim Results of a Randomized Phase II StudyOral, Sunday, 10am
O'Reilly #4114 Safety Pharmacokinetics Pharmacodynamics and Antitumor Activity ofO Reilly #4114 Safety, Pharmacokinetics, Pharmacodynamics, and Antitumor Activity ofNecuparanib Combined with nab-Paclitaxel and Gemcitabine in Patientswith Metastatic Pancreatic Cancer: Phase 1 ResultsPoster, Monday
11

Pancreatic Cancer Abstracts of Interest at ASCO 2015
Author Abstract Title
Hidalgo #4118 A Phase Ib Study of the Anti-Cancer Stem Cell Agent Demcizumab and Gemcitabine +/- Paclitaxel Protein Bound Particles in Pts with Pancreatic Cancer Poster, Monday
Hingorani #4006 High Response Rate and PFS with PEGPH20 Added to nab-P lit l/G it bi i St IV P i l U t t d P ti
Demcizumab (OncoMed)
Ongoing phase 1b dose escalationPaclitaxel/Gemcitabine in Stage IV Previously Untreated PancreaticCancer Patients with High-HA Tumors: Interim Results of a Randomized Phase II StudyOral, Sunday, 10am
O'Reilly #4114 Safety Pharmacokinetics Pharmacodynamics and Antitumor Activity of
• Ongoing phase 1b dose escalation• Cohorts 4, 5 & 6 received truncated demcizumab(2.5, 3.5 or 5 mg/kg every 2 wks through Day 70) and ABRAXANE® 125 mg/m2 + gemcitabine 1000 mg/m23 of 4 wksO Reilly #4114 Safety, Pharmacokinetics, Pharmacodynamics, and Antitumor Activity of
Necuparanib Combined with nab-Paclitaxel and Gemcitabine in Patientswith Metastatic Pancreatic Cancer: Phase 1 ResultsPoster, Monday
ABRAXANE 125 mg/m2 + gemcitabine 1000 mg/m23 of 4 wks
• Treatment was generally well-tolerated with mainly GI and fatigue AEsfatigue AEs• Encouraging clinical activity was observed• Updated data on tolerability and efficacy to be presented
12

Pancreatic Cancer Abstracts of Interest at ASCO 2015
Author Abstract Title
Hidalgo #4118 A Phase Ib Study of the Anti-Cancer Stem Cell Agent Demcizumab and Gemcitabine +/- Paclitaxel Protein Bound Particles in Pts with Pancreatic Cancer Poster, Monday
Hingorani #4006 High Response Rate and PFS with PEGPH20 Added to nab-P lit l/G it bi i St IV P i l U t t d P ti
ABRAXANE®/gemcitabine emerging as standard-Paclitaxel/Gemcitabine in Stage IV Previously Untreated PancreaticCancer Patients with High-HA Tumors: Interim Results of a Randomized Phase II StudyOral, Sunday, 10am
O'Reilly #4114 Safety Pharmacokinetics Pharmacodynamics and Antitumor Activity of
g g gof-care in 1st line metastatic pancreatic cancer
ABRAXANE®/gemcitabine is the research platform O Reilly #4114 Safety, Pharmacokinetics, Pharmacodynamics, and Antitumor Activity of
Necuparanib Combined with nab-Paclitaxel and Gemcitabine in Patientswith Metastatic Pancreatic Cancer: Phase 1 ResultsPoster, Monday
for multiple combinations with novel therapies
13

Treatments in Non-Small Cell Lung Cancer
Metastatic NSCLC (Stage IIIB/IV)Metastatic NSCLC (Stage IIIB/IV)
Non-Squamous (70-75%)Non-Squamous (70-75%) Squamous (25-30%)Squamous (25-30%)
EGFR/ALK+ EGFR/ALK+ PDL1Ineligible
PDL1IneligiblePDL1 High PDL1 High PDL1 Low PDL1 Low PDL1
Ineligible PDL1
Ineligible PDL1 High PDL1 High PDL1 Low PDL1 Low
1st-Line (~290K pts)1st-Line
(~290K pts)ABRAXANE®/carboplatinABRAXANE®/carboplatin
gggg
ChemoChemoTKITKIMaint(~100K pts)
Maint(~100K pts)
Chemo or TKIChemo or TKI
2nd-Line(~140K pts)2nd-Line
(~140K pts)TKI orChemoTKI orChemo Chemo or TKIChemo or TKI
14
Footnote: Patient numbers are estimates of annual treated patients in US and EU G5Source: NCCN Guidelines
14

Ongoing ABRAXANE® NSCLC Trials
Metastatic NSCLC (Stage IIIB/IV)Metastatic NSCLC (Stage IIIB/IV)
Non-Squamous (70-75%)Non-Squamous (70-75%) Squamous (25-30%)Squamous (25-30%)Non-Squamous (70-75%)Non-Squamous (70-75%) Squamous (25-30%)Squamous (25-30%)
EGFR/ALK+ EGFR/ALK+ PDL1Ineligible
PDL1IneligiblePDL1 High PDL1 High PDL1 Low PDL1 Low PDL1
Ineligible PDL1
Ineligible PDL1 High PDL1 High PDL1 Low PDL1 Low
1st Line(~290K pts)
1st Line(~290K pts)
ABRAXANE®
/carbo/MPDL ABRAXANE®
/carbo/MPDL Abound.70+Abound.70+ ABRAXANE®
/carbo/MPDL ABRAXANE®
/carbo/MPDL
TKITKI Abound.PS2Abound.PS2 Abound.PS2Abound.PS2
Abound.sqm
Abound.sqm
Maint (~100K pts)
Maint (~100K pts)
CheckpointCheckpoint Chemo or TKI
Chemo or TKI
Chemo or TKI
Chemo or TKI CheckpointCheckpoint Chemo
or TKIChemo or TKI
2nd Line (~140K pts)2nd Line
(~140K pts)
Chemo or TKI or checkpoint
combo
Chemo or TKI or checkpoint
combo
Chemo or TKI
Chemo or TKI
Chemo/checkpoint or I/O combo or chemo
Chemo/checkpoint or I/O combo or chemo Abound.2LAbound.2L Chemo/checkpoint or I/O
combo of chemoChemo/checkpoint or I/O
combo of chemo
15
Footnote: Patient numbers are estimates of annual treated patients in US and EU G5; Source: NCCN Guidelines
Celgene-sponsored trials Non Celgene-sponsored trials

NSCLC Cancer Abstracts of Interest at ASCO 2015
Author Abstract Title
Kotasek #8045 A Phase 1b Study of the Anti-Cancer Stem Cell Agent Demcizumab, Pemetrexed and Carboplatin in Pts with 1st Line Non-Squamous NSCLCPoster, Monday
Liu #8030 Safety and Efficacy of MPDL3280A (anti-PDL1) in Combination with Platinum-based Doublet Chemotherapy in Patients with Advanced Non-S ll C ll L CSmall Cell Lung Cancer Poster, Monday
16

NSCLC Cancer Abstracts of Interest at ASCO 2015
Author Abstract Title
Kotasek #8045 A Phase 1b Study of the Anti-Cancer Stem Cell Agent Demcizumab, DemcizumabPemetrexed and Carboplatin in Pts with 1st Line Non-Squamous NSCLCPoster, Monday
Liu #8030 Safety and Efficacy of MPDL3280A (anti-PDL1) in Combination with Platinum-based Doublet Chemotherapy in Patients with Advanced Non-S ll C ll L C
Demcizumab• 1 of 33 (3%) evaluable pts had a RECIST CR, 15
(45%) had a PR and 13 had SD• Potential for explore demcizumab in combination in
Small Cell Lung Cancer Poster, Monday
1st-line non-squamous NSCLC
ABRAXANE® + Atezolizumab• 2 Complete Responses and 6 Partial Responses in2 Complete Responses and 6 Partial Responses in
advanced NSCLC
Phase III trials in 1st-line NSCLC ( )(squamous and non-squamous) with ABRAXANE®/carbo +/- atezolizumab enrolling
17

Treatments in Breast Cancer
HER2+(25%)
HER2+(25%)
HER2-(75%)HER2-(75%)
Neoadjuvant/Neoadjuvant/
HR-(15%)HR-
(15%)HR+
(60%)HR+
(60%)
Neoadjuvant/Adjuvant(~250K pts)
Neoadjuvant/Adjuvant(~250K pts)
Pre-ChemoMetastaticPre-ChemoMetastatic
Trastuzumab + AC + Taxane
Trastuzumab + AC + Taxane
Not ApplicableNot Applicable
AC + TaxaneAC + Taxane
Not ApplicableNot Applicable
Taxane/C or AC to hormonal therapyTaxane/C or AC to hormonal therapy
Hormonal therapy +/- mTOR Hormonal therapy +/- mTOR
1st-Line Metastatic1st-Line
Metastatic
Metastatic(~115K pts)Metastatic(~115K pts)
Trastuzumab + Pertuzumab +
Trastuzumab + Pertuzumab +
Not ApplicableNot Applicable
ABRAXANE®ABRAXANE®
Not ApplicableNot Applicable
Hormonal therapy / Capecitabine
Hormonal therapy / Capecitabine
pyor CDK
pyor CDK
(~105K pts)(~105K pts)
2nd-Line Metastatic(~75K pts)
2nd-Line Metastatic(~75K pts)
TaxaneTaxane CapecitabineCapecitabine
ABRAXANE®ABRAXANE®
18
Footnote: Patient numbers are estimates of annual treated patients in US and EU G5; AC: Anthracycline/cyclophosphamide

Ongoing ABRAXANE® Breast Cancer Trials
HER2+(25%)
HER2+(25%)
HER2-(75%)HER2-(75%)
Neoadjuvant/Neoadjuvant/
HR-(15%)HR-
(15%)HR+
(60%)HR+
(60%)
GEPARSEPTONeoadjuvant/Adjuvant(~250K pts)
Neoadjuvant/Adjuvant(~250K pts)
Pre-ChemoMetastaticPre-ChemoMetastatic
GEPARSEPTO
Not ApplicableNot Applicable
ETNA
Not ApplicableNot Applicable
ADAPT
Hormonal therapy +/- mTOR Hormonal therapy +/- mTOR
1st-Line Metastatic1st-Line
Metastatic
Metastatic(~115K pts)Metastatic(~115K pts)
Trastuzumab + Pertuzumab +
Trastuzumab + Pertuzumab +
Not ApplicableNot Applicable
ABRAXANE® +/-MPDL3280A
Not ApplicableNot Applicable
Hormonal therapy / Capecitabine
Hormonal therapy / Capecitabine
pyor CDK
pyor CDK
(~105K pts) (~105K pts)
2nd-Line Metastatic(~75K pts)
2nd-Line Metastatic(~75K pts)
TaxaneTaxane CapecitabineCapecitabine tnAcitytnAcity
19
Footnote: Patient numbers are estimates of annual treated patients in US and EU G5; AC: Anthracycline/cyclophosphamide
Celgene-sponsored trials IITs or Collaborator Trials

Breast Cancer Abstracts of Interest at ASCO 2015
Author Abstract Title
Gluz #1032 Efficacy of 12 Weeks Neoadjuvant nab-Paclitaxel Combined with Carboplatinum vs. Gemcitabine in Triple-Negative Breast Cancer: WSG-ADAPT TN Randomized Phase II TrialPoster, Saturday
20

Breast Cancer Abstracts of Interest at ASCO 2015
Author Abstract Title
Gluz #1032 Efficacy of 12 Weeks Neoadjuvant nab-Paclitaxel Combined with Carboplatinum vs. Gemcitabine in Triple-Negative Breast Cancer: WSG-ADAPT TN Randomized Phase II TrialPoster, Saturday
ADAPTpCR was in 36% of patients overall; 25% with ABRAXANE®/gem and 49.2% with ABRAXANE®/carbo( 0 006)(p = 0.006)
Updates to GEPARSEPTO and ETNA expected over the next 12 months
Phase III trial in 1st-line TNBC with ABRAXANE®+/-atezolizumab to begin enrollment soon
21

Agenda
Advancing ABRAXANE®1 Advancing ABRAXANE®1 Advancing ABRAXANE®1 Advancing ABRAXANE®1
Ongoing Progress in Myeloma2 Ongoing Progress in Myeloma2
Expanding into Lymphoma3 Expanding into Lymphoma3
22

MM-020: Updated Overall Survival Descriptive Analysis (Rd vs MPT in Newly-Diagnosed Multiple Myeloma)
1Rd
Updated OS per Health Authority request45.5 months median follow-up
(78% of final OS events)
0.8
bilit
y
Rd
MPT
( )
0.4
0.6
rviv
al P
roba
b
0.2
Surv
Study arm Hazard ratioRd vs MPT 0.74 (0.61, 0.89)
Study arm Median OSRd 58.9 mo
MPT 48.5 mo0
0 6 12 18 24 30 36 42 48 54 60 66 72Time, mo
Rd 535 488 457 433 403 366 337 246 156 74 13 0MPT 547 484 448 418 375 347 310 230 130 58 10 0MPT 547 484 448 418 375 347 310 230 130 58 10 0
MPT = melphalan, prednisone, thalidomide; OS = overall survival; Rd = lenalidomide plus low-dose dexamethasone.Hazard ratio is based on stratified Cox-PH model and p value is based on stratified log-rank test.23

MMMM--003: Overall 003: Overall Survival Survival ––ITT Population with POMALYSTITT Population with POMALYST®®/IMNOVID/IMNOVID®®
Median follow-up 10 months
CI, confidence interval; HiDEX, high-dose dexamethasone; HR, hazard ratio; ITT, intent to treat; LoDEX, low-dose dexamethasone; OS, overall survival; POM, pomalidomide.San Miguel J., et al. Lancet Oncol. 2013. DOI: 10.1016/S1470-2045(13)70380-2.
24

MM Abstracts of Interest at ASCO 2015
Author Abstract Title
Holstein #8523 Updated Analysis of CALGB/ECOG/BMT CTN 100104: Lenalidomide vs. Placebo Maintenance Therapy after Single Autologous Stem Cell Transplant for Multiple MyelomaPoster, Sunday
Dimopoulos #8525 Effect of Carfilzomib, Lenalidomide, and Dexamethasone vs L lid id d D th i P ti t ith R l d M lti lLenalidomide and Dexamethasone in Patients with Relapsed Multiple Myeloma by Line of Therapy: Secondary Analysis from an Interim Analysis of the Phase III Study ASPIRE (NCT01080391)Poster, Sunday
Lonial #8508 ELOQUENT 2: A Phase III Randomized Open Label Study ofLonial #8508 ELOQUENT-2: A Phase III, Randomized, Open-Label Study of Lenalidomide/Dexamethasone with/without Elotuzumab in Patients with Relapsed/Refractory Multiple Myeloma Oral, Tuesday 9:45am
Zimmerman #8510 Phase II MMRC Trial of Extended Treatment with CarfilzomibZimmerman #8510 Phase II MMRC Trial of Extended Treatment with Carfilzomib, Lenalidomide, and Dexamethasone plus Autologous Stem Cell Transplantation in Newly Diagnosed Multiple MyelomaOral, Tuesday 10:33am
25

CALGB 100104: REVLIMID® Improved TTP and OS
Median: 53 vs 26 mosHazard ratio 0.54 (p<0.001)
Median: NR vs 76 mosHazard ratio 0.60Hazard ratio 0.60(p=0.001)
Intent-to-treat analysis, data cut-off Nov 2014
26

Research in Multiple Myeloma with Rd Backbone
• ASPIRE (KRd vs RD in RRMM)
Median PFS for pts receiving 1 prior line was 29.6 mos for KRd vs17.6 mos for Rd (hazard ratio [HR]: 0.694; P= .0083). Median PFS for pts ≥ 2 prior lines was 25.8 mos for KRd vs 16.7 mos for Rd (HR: 0.688; P= .0017)
• ELOQUENT-2 (Erd vs RD in RRMM)
Median PFS: ERd 19.4 mos vs. Rd 14.9 mos (HR [95% CI] 0.70 [0.57, 0.85]; p = 0.0004). ORR 79% ERd vs. 66% Rd
• MMRC (KRd + ASCT) in NDMM
Post-Induction Post-Transplant Post-Consolidation
Post-KRdConsolidation
≥ PR% 98 100 100 100≥ VGPR% 78 97 100 100≥ nCR% 14 44 91 100
27
sCR% 10 25 70 86

Agenda
Advancing ABRAXANE®1 Advancing ABRAXANE®1 Advancing ABRAXANE®1 Advancing ABRAXANE®1
Ongoing Progress in Myeloma2 Ongoing Progress in Myeloma2
Expanding into Lymphoma3 Expanding into Lymphoma3
28

REVLIMID® Clinical Plan in Lymphoma Addresses Unmet Need
2nd Relapse 1st Relapse 1L MaintenanceInduction/1L
GCB LRGCB LR patients CD20patients CD20 CHOPCHOP ASCT li ibl ASCTASCT li ibl ASCTHighHigh--risk patients risk patients (Lenalidomide, (Lenalidomide,
BTKi?) BTKi?) REMARCREMARC
NonNon--GCB patientsGCB patientsCD20CD20--CHOPCHOPRR22--CHOPCHOPD
LBC
L GCB LR GCB LR patients CD20patients CD20--CHOPCHOP
GCB HR GCB HR patients CD20patients CD20--CHOPCHOP R(CD20)R(CD20)--ChemoChemo//nnew ew comboscombosASCT ineligible: ASCT ineligible:
R(CD20)R(CD20)--ChemoChemo//new new comboscombos
ASCT eligible: ASCTASCT eligible: ASCT
CD20CD20--nonnon--ChemoChemoCDCD--20 20 ChemoChemo
AUGMENTAUGMENTTMTM
MAGNIFYMAGNIFYTMTM
CD20CD20--nonnon--ChemoChemoIndo
lent RELEVANCERELEVANCE®® (FL)(FL)
CDCD--20 Chemo20 Chemo
CD20 or CD20CD20 or CD20--Combos (R2, BTK) Combos (R2, BTK)
(maint.)(maint.)RIT (consolid.)RIT (consolid.)
Vaccines Vaccines –– TBDTBD
RELEVANCERELEVANCE®® (FL)(FL)
MC
L RR--Chemo Chemo ±± novel agents novel agents (e.g. i(e.g. ibrutinibbrutinib))
MCLMCL--001001MCLMCL--002002
MCL NetworkMCL NetworkRR22
PTC
L RoRo--CHOPCHOPRoRo--CHOPCHOP ISTODAXISTODAX®®ISTODAXISTODAX®®
CHOPCHOP F l tF l t
29
REVLIMID®Existing therapy
P CHOPCHOPOtherOther ChemoChemo
ISTODAX®
FolotynFolotynChemosChemos

Follicular Lymphoma Is a Hematologic Malignancy With a Protracted Disease Course
Availability of novel treatment options and introduction of rituximab maintenance have improved overall survival relative to historical controls
30
Tan D, et al. Blood. 2007;110:Abstract 3428.
Years10 20 30 40

Follicular Lymphoma Analysis of Surrogacy Hypothesis (FLASH): Meta-Analysis Aims to Identify a Surrogate Endpoint for PFS
CTI
VES
CTI
VES • Establish a novel surrogate efficacy endpoint for PFS in first-line
follicular lymphoma to be used for regulatory decision making• Establish a novel surrogate efficacy endpoint for PFS in first-line
follicular lymphoma to be used for regulatory decision making
OB
JEC
OB
JEC
• Reduce duration of clinical trials to expedite patient access to effective new therapies
• Reduce duration of clinical trials to expedite patient access to effective new therapies
RO
AC
HR
OA
CH • Independently conducted by Mayo Clinic Biostatistics Group (US) in
collaboration with cooperative groups from across the world
• Support from Celgene and Roche
• Independently conducted by Mayo Clinic Biostatistics Group (US) in collaboration with cooperative groups from across the world
• Support from Celgene and Roche
APP
APP
Support from Celgene and Roche
• Followed guidelines and considerations from the FDA
Support from Celgene and Roche
• Followed guidelines and considerations from the FDA
THO
DO
LGY
THO
DO
LGY • A thorough review of all studies conducted in front-line FL was
performed and initially identified > 300 studies of published data
• Patient-level data was obtained from studies that met prespecified selection criteria and where available to perform a meta analysis
• A thorough review of all studies conducted in front-line FL was performed and initially identified > 300 studies of published data
• Patient-level data was obtained from studies that met prespecified selection criteria and where available to perform a meta analysis
31
MET
MET selection criteria and where available to perform a meta-analysis
designed to identify and qualify a surrogate endpointselection criteria and where available to perform a meta-analysis designed to identify and qualify a surrogate endpoint

Lymphoma Abstracts of Interest at ASCO 2015
Author Abstract Title
Sargent #8504 Evaluation of Complete Response Rate at 30 Months as a Surrogate for Progression-Free Survival in First-Line Follicular Lymphoma Studies: Results from the Prospectively Specified Follicular Lymphoma Analysis of Surrogacy Hypothesis (FLASH) Analysis with Individual Patient Data of 3,837 PatientsOral Monday 10:57amOral, Monday, 10:57am
32

Lymphoma Abstracts of Interest at ASCO 2015
Author Abstract Title
Sargent #8504 Evaluation of Complete Response Rate at 30 Months as a Surrogate for Progression-Free Survival in First-Line Follicular Lymphoma Studies: Results from the Prospectively Specified Follicular Lymphoma Analysis of Surrogacy Hypothesis (FLASH) Analysis with Individual Patient Data of 3,837 PatientsOral Monday 10:57am
FLASH Analysis
Trial type Trials, N (pts) R2 WLS (95% CI)a R2 Copula (95% CI)aOral, Monday, 10:57amy ( ) ( ) ( )
Overall 13 (3,837) 0.88 (0.77-0.96) 0.86 (0.72-1.00)Rituximabincluded
9 (2,851) 0.85 (0.62-0.97) 0.80 (0.56-1.00)
No rituximab 4 (986) 0.91 (0.05-1.00) 0.96 (0.90-1.00)Induction 8 (2,207) 0.89 (0.75-0.98) 0.89 (0.74-1.00)Maintenance 5 (1 630) 0 93 (0 84 1 00) 0 89 (0 71 1 00)Maintenance 5 (1,630) 0.93 (0.84-1.00) 0.89 (0.71-1.00)
a R2 values range from 0 (no association) to 1 (perfect prediction)
33
g ( ) (p p )
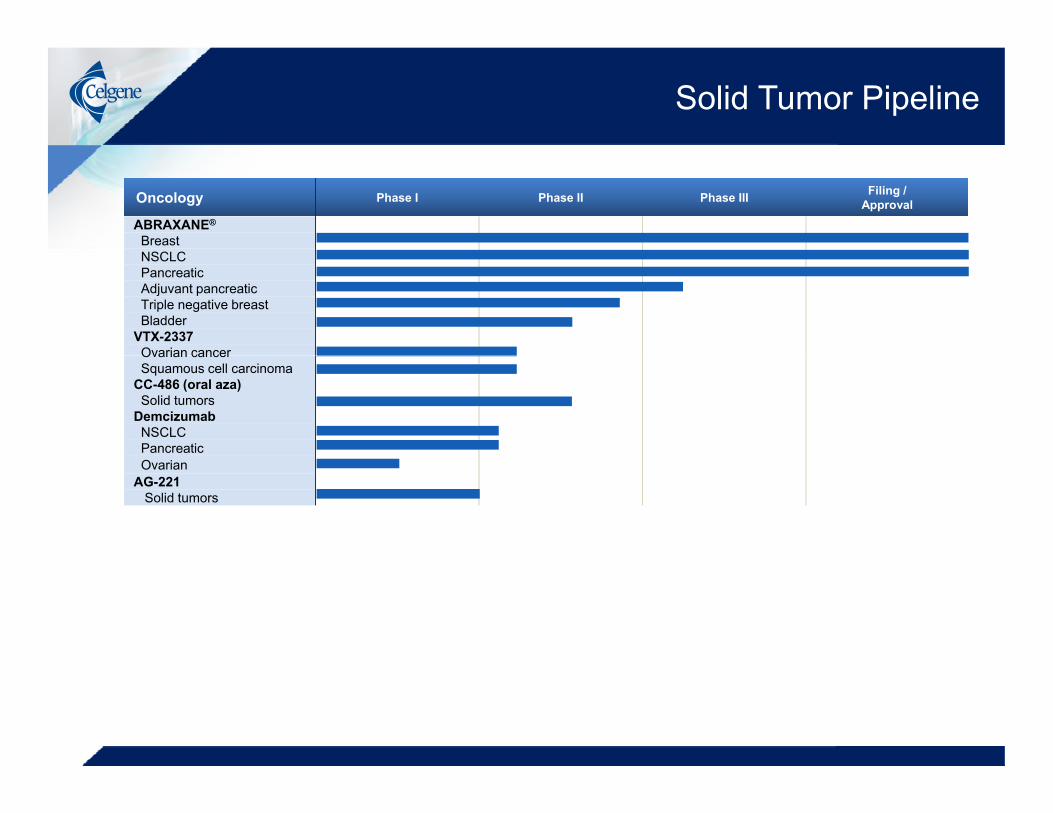
Solid Tumor Pipeline
Oncology Phase I Phase II Phase III Filing /Approval
ABRAXANE®
BreastNSCLCNSCLCPancreaticAdjuvant pancreaticTriple negative breastBladder
VTX-2337Ovarian cancerOvarian cancerSquamous cell carcinoma
CC-486 (oral aza)Solid tumors
DemcizumabNSCLCPancreaticOvarian
AG-221Solid tumors

Solid Tumor Pipeline
Oncology Phase I Phase II Phase III Filing /Approval
ABRAXANE®
BreastNSCLCNSCLCPancreaticAdjuvant pancreaticTriple negative breastBladder
VTX-2337Ovarian cancer
Advancing Oncology Portfolio
ABRAXANE® t bli h d i h d t t t i l di t t tiOvarian cancerSquamous cell carcinoma
CC-486 (oral aza)Solid tumors
DemcizumabNSCLCPancreatic
• ABRAXANE® established in hard to treat cancers including metastatic pancreatic, lung and metastatic breast
• Expected data read outs over the next 12 monthsOvarian
AG-221Solid tumors
Expected data read outs over the next 12 months • ABRAXANE®/gemcitabine in combination with demcizumab in pancreatic cancer (phase II)• Updated data from GEPARSEPTO in neoadjuvant breast cancer
Demci mab in combination ith carbo/pemetre ed in NSCLC• Demcizumab in combination with carbo/pemetrexed in NSCLC• Motolimod (VTX-2337) in ovarian and head and neck cancers (phase II)

Hematology Pipeline
Hematology Phase I Phase II Phase III Filing /Approval
REVLIMID®
MMMDS deletion 5qMDS non-deletion 5qCLLT-Cell leukemiaNHL - MCLNHL - DLBCLNHL - FLNHL iNHLNHL - iNHL
VIDAZA®
MDSAML
ISTODAX®
CTCL, PTCLPOMALYST®/IMNOVID®
MMCC-486 (oral aza)MDSAML
Sotatercept (ACE-011)MDSDi d bl kf iDiamond blackfan anemiabeta-thalassemiaLuspatercept (ACE-536)MDSbeta-thalassemia
AG-221Heme malignancies
36
Heme malignancies

Hematology Pipeline
Hematology Phase I Phase II Phase III Filing /Approval
REVLIMID®
MMMDS deletion 5qMDS non-deletion 5qCLLT-Cell leukemiaNHL - MCLNHL - DLBCLNHL - FLNHL iNHL
Advancing the Hematology Portfolio
REVLIMID® and POMALYST®/IMNOVID® backbone in MM • Advance REVLIMID® as maintenance treatment post ASCTNHL - iNHL
VIDAZA®
MDSAML
ISTODAX®
CTCL, PTCLPOMALYST®/IMNOVID®
• Advance REVLIMID® as maintenance treatment post ASCT
Continuing in Lymphoma• Data on CC-122 phase II in 2016
MMCC-486 (oral aza)MDSAML
Sotatercept (ACE-011)MDSDi d bl kf i
• Data for RELEVANCE®, REMARC and AUGMENTTM expected beginning in 2017
Advancing AG-221 and luspatercept into phase III programsDiamond blackfan anemiabeta-thalassemiaLuspatercept (ACE-536)MDSbeta-thalassemia
AG-221Heme malignancies
Advancing AG-221 and luspatercept into phase III programs
Initiate “Immuno-Hematology” programs with durvalumab
37
Heme malignancies

Robert Hershberg, MD PhDSVP, Immuno-Oncology

Celgene’s Immuno-Oncology Portfolio Addresses Multiple Aspects of the Anti-Tumor Immune Response
39

Celgene’s Immuno-Oncology Portfolio Addresses Multiple Aspects of the Anti-Tumor Immune Response
Durvalumab (MEDI4736)IMiDs®
VTX 2337IMiDs® VTX-2337CAR-TSutro 2.0
ABRAXANE®
CC-486
IMiDs®Anti-CD47VTX-2337NK cells (CCT)
VTX-2337
IMiDs®
40

PD-1/PD-L1 Targeting Agents are Dominant Assets in the I/O Landscape
• Unprecedented value expected in multiple oncology indications
• Nivolumab (BMS) and Pembrolizumab (Merck) approved
• Atezolizumab (MPDL3280A) (Roche) and durvalumab (AZ) likely to be approved in next 24 months
• Avelumab (Pfizer) in clinical development
• Impressive data across multiple tumor types, and intense competition are solidifying the position of this target and these drugs with patientsare solidifying the position of this target and these drugs with patients and physicians
4141

Emerging Themes and Key Questions with Checkpoint Inhibitors
• Most patients don’t respond to these agents in isolation, instead requiring combination therapy.
What are the most important combination agents that will be used in the near and mid-term?
• PD-1 and/or PD-L1 expression alone are inadequate to predict p q presponse
What characteristics define responsive patients and how will this inform optimal combination and innovation in the space?p p
• Multiple molecules beyond PD-1 and CTLA-4 control T-cell checkpoints
Whi h f th t l ill lif i diWhich of these controls will amplify responses in non-responding patients?
4242

ABRAXANEABRAXANE®® Delivers Activity without CorticosteroidsDelivers Activity without Corticosteroids
® Cremophor is a registered trademark of BASF.® nab is a registered trademark of Celgene Corporation.
References: Gardner et al. Clin Cancer Res. 2008;14(13):4200-4205.Desai et al. Clin Cancer Res. 2006;12:1317-1324.
43

REVLIMID® is an Immunomodulatory Drug
DC, dendritic cell; NK, natural killer.
44
Citations in appendix

IMiDs® and PD-1/PD-L1 Inhibitors May Have Complementary and Synergistic Effects
Effect IMiDs® PD-1 / PD-L1 axis blockade1. Recruitment/↑ number Expansion of T cells, CTLs, NK cells and1. Recruitment/↑ number
of immune cellsExpansion of T cells, CTLs, NK cells and NKT cells
2. Induction/ priming of ↑ Response to vaccines ↑ response to vaccines2. Induction/ priming of T cells/ immune response
↑ Response to vaccines↑ DC antigen presentation/T cell priming↑ Antibody priming
↑ response to vaccines↑ T cell priming
3. T cell polarisation ↑ Th1 polarization/cytokines ↑ Th1 polarization/cytokines
4. Effector cell function ↑ CTL activity↑ Th cell activity↑ NKT cell activity↑ NK cell activity↑ NK cell tumor killing/ADCC
Re-activation of CTL and Th cell activityRe-activation of NK cell activityEnhanced B-cell antibody production
5. PD1/PD-L1 axis activity
↓ PD-1 expression on T-cells↓ PD-1 expression on MM cells
Reversal of PD-1–induced T cell anergyReactivation of CTL and Th cell activityRe-activation of NK cell activity
45

Cereblon Modulates Immune Response
THALOMID® REVLIMID® POMALYST®/IMNOVID®
CC-122 CC-220 Future
CEREBLON
Substrates(Common, Unique, Partially shared)
REVLIMID® modulates T cell biology (T cell synapse, IL-2 d ti ) d NK bi l i IKAROS d AILOS2 production) and NK biology via IKAROS and AILOS regulation
Novel CELMoDs™ are being developed with potent,
46
g p p ,directed immunomodulatory properties

Combining Epigenetic Modulation and Checkpoint Blockade
Hypothesis:Hypothesis: • Azacitidine hypomethylates/
reactivates genes necessary for recognition of tumor cells by immune
CC-486
g yeffectors
– PD-L1 expression– Tumor antigen expression– HLA Class 1 expression– Type-1 Interferon expression
• Blockade of PD-1 pathway in bi ti ith CC 486Anti PD1
X
combination with CC-486 may improve anti-tumor activity
Anti-PD1
4747
Celgene’s Campaign in Immuno-Oncology
Complementarity
Conviction
CommitmentCommitment
48

Advancing Checkpoint Combinations with Celgene Assets
Atezolizumab - Roche• Two randomized pivotal studies with ABRAXANE® in combination in NSCLC enrolling• Phase III trial with ABRAXANE® in 1st-line metastatic triple negative breast cancer to begin enrollment soon
Nivolumab – Bristol-Myers Squibb • Phase I trial with ABRAXANE® in multiple solid tumors
Pembrolizumab - Merck• Phase I/II trials with REVLIMID® or POMALYST®/IMNOVID® in RRMM enrolling• Phase I/II trial with ABRAXANE® in NSCLC to begin enrollment soon• Trials with CC-486 in NSCLC and ovarian cancer planned
49

Emerging Data Suggest that PD-1/PD-L1 Pathway is Important in Hematologic Malignancies
Multiple Myeloma
• In vitro and in vivo experiments show significant up-regulation of PD-L1 in ndMM and rrMM patients1
Myeloid
• Increasing evidence for the importance of immunotherapeutic approaches in AML and MDS2-8AML and MDS
– Allogeneic transplant as curative approach in AML and high-risk MDS patients– Increased PD-L1 expression on AML and MDS cells in patients post-treatment with HMA– Increased PD-L1 expression on AML stem cells and in residual disease (MRD+)
1. Gorgun GT et al. Clin CancerRes 2015 [Epub ahead of print]2. Kondo A, et al. Blood. 2010;116(7):1124-1131.
3. Tamura H. J Nippon Med Sch. 2010;77(1):45-47 [abstract].
50
pp ( ) [ ]4. Zhang L, et al. Blood. 2009;114(8):1545-1552.
5. Krönig H, et al. Eur J Haematol. 2013;92:195-203. 6. Zhou Q, et al. Blood. 2010;116(14):2484-2493.
7. Yang H, et al. Leukemia. 2013. [Epub ahead of print].8. Yang H, et al. Blood. 2013;122(21):2767 [abstract].
50

Emerging Data Suggest that PD-1/PD-L1 Pathway is Important in Hematologic Malignancies
Lymphomas
• Impressive single agent response data with anti-PD1 antibodies in Hodgkin Lymphoma
– 9p amplification in Reed-Sternberg cell includes PD-L1/PD-L2 locus1
I i id f li ti f i th ti h• Increasing evidence for application of immunotherapeutic approaches in lymphomas
– Allogeneic transplant as curative approach in indolent lymphoma– Increased PD-1 expression on tumor infiltrating T-lymphocyes post treatment
with R22,3
– Early clinical data with PD-1 in DLBCL, PD-1 plus rituximab in FL suggest clinical activity4
1 Yamamoto et al Blood 2008; 111; 3220
51
1. Yamamoto et al. Blood. 2008; 111; 32202. Myklebust JH et al. Blood. 2013; 121:1367
3. Fowler et al., Lancet Oncology, 20154. Westin JR et al. Lancet Oncol. 2014;15:69-77
51
Celgene Poised for “Immuno-Hematology” Leadership
• Recently announced collaboration with AstraZeneca/MedImmune for durvalumab
• Celgene will lead clinical development of combination trials in hematologic indications
• Celgene will be working closely with MedImmune on translational aspects of studies and will have
t b d biliti d d t iaccess to broad capabilities and data in emerging I/O space
Celgene has competitive advantage in hematology• I/O backbone therapies across hematology: Rd, Pd, R²• Scientific/Clinical expertise in indications that will be the focus for checkpoint inhibitor development in hematology: MM NHL MDS/AML
52
checkpoint inhibitor development in hematology: MM, NHL, MDS/AML• Existing hematology commercial infrastructure

Anticipated Clinical Development Strategy for Durvalumab: Combinations in Hematology
Combinations with
First Wave
Multiple Myeloma REVLIMID® and POMALYST® /
IMNOVID®
Non-Hodgkin Lymphoma
CLL
Combinations with IMiDs®, mAbs and targeted therapiesCLL
MDS/AML
targeted therapies
Combinations withMDS/AML Combinations with CC-486 and VIDAZA®
5353

Anticipated Clinical Development Strategy for Durvalumab: Combinations in Hematology
Combinations with Combinations with
First Wave Second Wave
Multiple Myeloma REVLIMID® and POMALYST® /
IMNOVID®
Combinations with pipeline assets and
novel therapies
Non-Hodgkin Lymphoma
CLL
Combinations with IMiDs®, mAbs and targeted therapies
Combinations with pipeline assets and
novel therapiesCLL
MDS/AML
targeted therapies
Combinations with
novel therapies
Combinations with i li t dMDS/AML Combinations with
CC-486 and VIDAZA® pipeline assets and novel therapies
5454

The Complexity of the Tumor Microenvironment
55
W Fridman et al. Nature Rev Can 12, 298-306 (2012) doi:10.1038/nrc3245
55

Additional I/O Assets at Celgene
• Anti-CD47 (CC-90002) monoclonal antibody– First-in-class molecule targeting novel macrophage biology in cancer
Advanced to Phase 1 in multiple tumor types– Advanced to Phase 1 in multiple tumor types
• Toll-like receptor 8 agonist (motolimod, VentiRx)– First-in-class small molecule stimulator of Innate Immunity (macrophages, NK)– 2 large randomized Phase II studies (ovarian, head/neck) to read out in 2016
• Novel IMiDs®/CELMoDs™ (CC-122)– Existing clinical assets are immunomodulatory, stimulate T cells and NK cells– CRBN biology leading to novel immunomodulators
• SUTRO/Novel Biologics– Collaborative and internal efforts leading to 2nd generation, novel checkpoint
inhibitors (“bi-specifics” and other approaches)
• InfrastructureInfrastructure– I/O TCoE operational in Seattle– Focus on translational and computational aspects of I/O to enable current and
next generation products
56

Dedicated to Immuno-Oncology;Pioneering “Immuno-Hematology”
Existing assets are mechanistically unique andExisting assets are mechanistically unique and complementary to checkpoint inhibitors
ABRAXANE®, REVLIMID®, CC-486
Aggressively pursuing a broad development Aggressively pursuing a broad development program with durvalumab in multipleprogram with durvalumab in multipleprogram with durvalumab in multiple program with durvalumab in multiple
hematological malignancies in collaboration hematological malignancies in collaboration with AZ/MEDIwith AZ/MEDI
Emerging assets extend and complement Emerging assets extend and complement
57
beyond current Tbeyond current T--cell checkpoint inhibitorscell checkpoint inhibitors

Jackie Fouse, PhDPresident, Global Hematology & Oncology

On-Track to Deliver 2020 Hematology and OncologyTargets
>$17B
15%CAGR
$7.45B
2014 2017E 2020E
59
Hematology Oncology

New ABRAXANE® Opportunities Accelerate Momentum Through 2020
Expected Growth OpportunitiesExpected Growth Opportunities>$2 2
Sales ($B)>$2.2Growth from Existing Portfolio:
• Market share and geographic expansion of ABRAXANE® in NSCLC and metastatic pancreatic cancer 14%
CAGR $1.917%CAGRpancreatic cancer
New Indications & Opportunities:• ABRAXANE® late stage trials in:
• Adjuvant pancreatic cancer
CAGR $1.9CAGR
$0.85Adjuvant pancreatic cancer
• Additional segments of NSCLC
• Triple negative breast cancer
• Neoadjuvant breast cancer
2014 2017E 2020E
j
60
ABRAXANE® Label Expansions; New Opportunities

Market Share in “MPACT Population” Patients Approaching 50%
60%Pancreatic 1st line Stage IV Regimen ShareDE NOVO METASTATIC “MPACT Population”
49.5%
40%
50%
33.1%
20%
30%
13.8%
1.7%1.8%
0%
10%
Abraxane gemcitabine** FOLFIRINOX 5FU + other all otherAbraxane gemcitabine FOLFIRINOX 5FU other all other
61
Source: IntrinsiQ Report: Diag Combo LOT Stage Monthly_pancreatic (exocrine) carcinoma; Apr R3M pre-projected patients: 116; projected patients: 2928
**Gemcitabine includes monotherapy and combination other than with ABRAXANE®

Market Share in Squamous 1st-Line NSCLC Stable
50%mNSCLC Squamous 1st line Molecule Share
40%
16.9%20%
30%
6 9%
0%
10%
0%
paclitaxel gemcitabine Abraxane docetaxelb i b l ti ib i b i l b
Source: IntrinsiQ Report: Diag Drug Met Status Pathology 3MRA (Progression Line)_lung cancer (non-small cell); Apr R3M pre-projected patients: 146; projected patients: 3669
62
bevacizumab erlotinib ramucirumab nivolumab
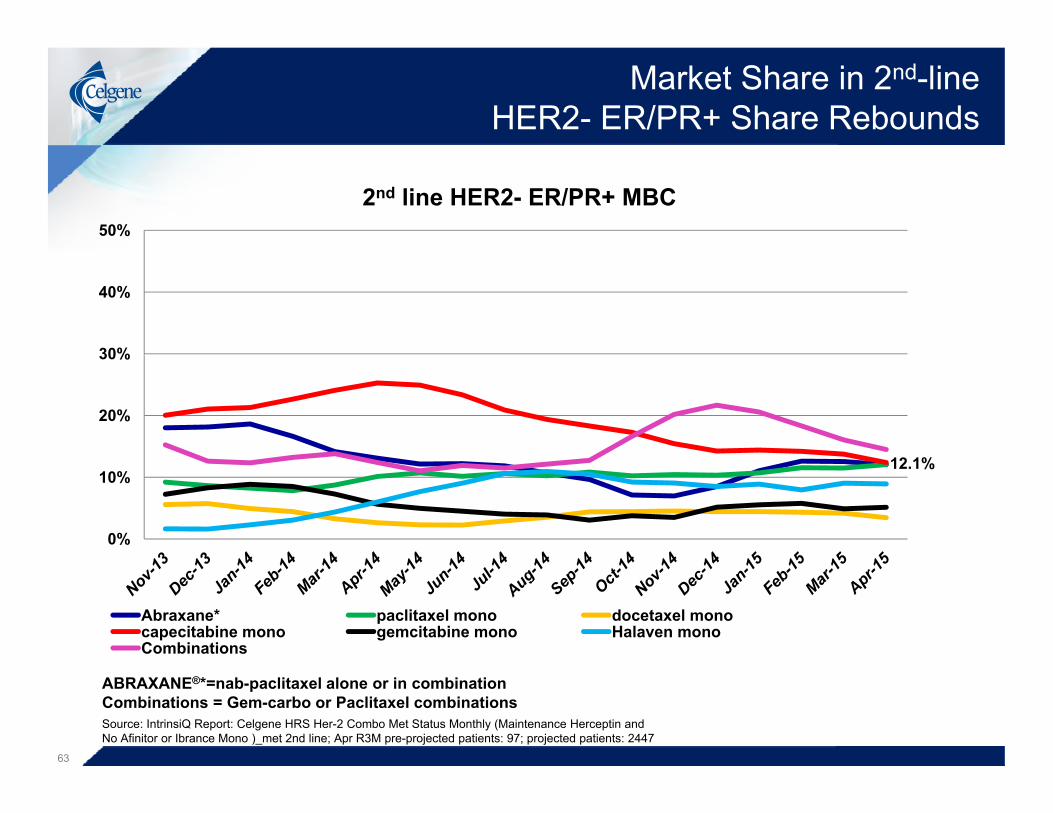
Market Share in 2nd-line HER2- ER/PR+ Share Rebounds
50%
2nd line HER2- ER/PR+ MBC
30%
40%
12 1%
20%
30%
12.1%
0%
10%
Abraxane* paclitaxel mono docetaxel monocapecitabine mono gemcitabine mono Halaven monoCombinations
Source: IntrinsiQ Report: Celgene HRS Her-2 Combo Met Status Monthly (Maintenance Herceptin and No Afinitor or Ibrance Mono )_met 2nd line; Apr R3M pre-projected patients: 97; projected patients: 2447
ABRAXANE®*=nab-paclitaxel alone or in combinationCombinations = Gem-carbo or Paclitaxel combinations
63

New Opportunity with Emerging Data in Triple Negative mBC
50%
Triple Negative mBC All Lines Share
30%
40%
20%
30%
7.4%
0%
10%
capecitabine mono paclitaxel mono carboplatin - gemcitabinegemcitabine mono Abraxane* docetaxel mono
64
Halaven mono taxane combo
Source: IntrinsiQ Report: Celgene HRS Her-2 Combo Met Status Monthly (Maintenance Herceptin and No Afinitor or Ibrance Mono ); Apr R3M pre-projected patients: 184; projected patients: 4638
ABRAXANE®*=nab-paclitaxel alone or in combination
64

Additional Oncology Opportunities Accelerate Momentum Through 2020
Expected Growth OpportunitiesExpected Growth Opportunities>$2 2
Sales ($B)Oncology Upside Potential Through 2020Oncology Upside Potential Through 2020>$2.2
Growth from Existing Portfolio• Market share and geographic expansion of
ABRAXANE® in NSCLC and metastatic pancreatic cancer
14%CAGR $1.917%CAGR
ABRAXANE® in anti-PD-1 / anti-PD-L1 combinationspancreatic cancer
New Indications & Opportunities:• ABRAXANE® late stage trials in:
• Adjuvant pancreatic cancer
CAGR $1.9CAGR
Demcizumab approval in non-small cell lung and pancreatic cancers
$0.85• Adjuvant pancreatic cancer
• Triple negative breast cancer
• Neoadjuvant breast cancer
Additional segments of NSCLC
VTX-2337 approval in ovarian and SCCHN
2014 2017E 2020E
• Additional segments of NSCLCCC-486 approval in solid tumors
65
ABRAXANE® Label Expansions; New Opportunities

New Hematology Opportunities Expected to Accelerate Growth Through 2020
Expected Growth OpportunitiesExpected Growth Opportunities Sales ($B)
12%14%
Growth from Existing Portfolio:• REVLIMID® approved for NDMM in U.S. and
Europe• Duration and market share gains for
>$14.8
$13 012%CAGR 14%CAGR
Duration and market share gains for REVLIMID® and POMALYST®/IMNOVID®
New Indications & Opportunities:• REVLIMID® in novel combos in myeloma $6 6
$13.0
y• REVLIMID® for NHL
New Product Introductions:• CC-486 (oral azacitidine) in MDS and AML
$6.6
2014 2017E 2020E
• Luspatercept in beta-thalassemia• AG-221 in IDH2 mutant AML
66
Existing Products
Label Expansions; New Products

Additional Hematology Opportunities Accelerate Momentum Through 2020
Expected Growth OpportunitiesExpected Growth Opportunities Sales ($B)Hematology Upside Potential Through 2020Hematology Upside Potential Through 2020
12%14%
Growth from Existing Portfolio• REVLIMID® approvals for NDMM in U.S.
and Europe• Duration and market share gains for
>$14.8
$13 0
• Full impact of REVLIMID® and POMALYST®/IMNOVID® treatment duration
• REVLIMID® for non-del 5q in Europe 12%CAGR 14%CAGR
Duration and market share gains for REVLIMID® and POMALYST®
New Indications & Opportunities:• REVLIMID® in novel combos in myeloma $6 6
$13.0• REVLIMID® for maintenance in CLL
• Broader and earlier adoption of REVLIMID® in lymphomasy
• REVLIMID® for NHL
New Product Introductions:• CC-486 (oral azacitidine) in MDS and AML
$6.6• Approval for luspatercept in MDS
• Earlier than expected approval for AG-221 in R/R AML (IDH2 mutations)
2014 2017E 2020E
• Sotatercept or Luspatercept in beta-thalassemia
• AG-221 (IDH2 mutant AML)
in R/R AML (IDH2 mutations)
• Approval for AG-120 in R/R AML (IDH1 mutations)
• Approval for CC-122 in DLBCL, CLL or MM
67
Existing Products
Label Expansions; New Products
pp ,

Additional Hematology Opportunities Accelerate Momentum Through 2020
Expected Growth OpportunitiesExpected Growth Opportunities Sales ($B)Hematology Upside Potential Through 2020Hematology Upside Potential Through 2020
12%14%
Growth from Existing Portfolio• REVLIMID® approvals for NDMM in U.S.
and Europe• Duration and market share gains for
>$14.8
$13 0
• Full impact of REVLIMID® and POMALYST®/IMNOVID® treatment duration
• REVLIMID® for non-del 5q in Europe 12%CAGR 14%CAGR
Duration and market share gains for REVLIMID® and POMALYST®
New Indications & Opportunities:• REVLIMID® in novel combos in myeloma $6 6
$13.0• REVLIMID® for maintenance in CLL
• Broader and earlier adoption of REVLIMID® in lymphomasFirst approval y• REVLIMID® for NHL
New Product Introductions:• CC-486 (oral azacitidine) in MDS and AML
$6.6• Approval for luspatercept in MDS
• Earlier than expected approval for AG-221 in R/R AML (IDH2 mutations)
ppfor durvalumab
possible by 2020
2014 2017E 2020E
• Sotatercept or Luspatercept in beta-thalassemia
• AG-221 (IDH2 mutant AML)
in R/R AML (IDH2 mutations)
• Approval for AG-120 in R/R AML (IDH1 mutations)
• Approval for CC-122 in DLBCL, CLL or MM
68
Existing Products
Label Expansions; New Products
pp ,

Generating Strong Franchise Momentum
Key Drivers for 2020 Targets in PlaceKey Drivers for 2020 Targets in Place
MidMid-- to Lateto Late--Stage Pipeline AdvancingStage Pipeline AdvancingLeading to Data Readouts in 2016Leading to Data Readouts in 2016
Investing in Next Generation Drugs toInvesting in Next Generation Drugs toSustain High Growth Beyond 2020Sustain High Growth Beyond 2020
69
g yg y

Questions & Answers
Moderator: Peter KelloggggEVP and CFO
Panelists: Jackie Fouse, PhDPresident, Global Hematology & Oncology
Jay Backstrom, MDSVP, Global Hematology & Oncology Clinical R&D
Rob Hershberg, MD PhDRob Hershberg, MD PhDSVP, Immuno-Oncology
70

ASCO 2015 Investor EventMay 31, 2015

Reconciliation Tables
013 6,36
2.3
131.
6 6,49
3.9
340.
4 2,22
6.2
1,68
4.5
262.
8 17
1.1
4,68
5.0
1,80
8.9
22.0
(91.
6) (7
3.9)
1,66
5.4
215.
5 1,44
9.9
1.75
1.
68
827.
7 86
0.6
une
18,
-one
Ende
d
2014
20
7,56
3.8
6
$
106.
6
7,67
0.4
6
385.
9
2,43
0.6
2
2,
027.
9
1
258.
3
48.7
5,15
1.4
4
2,51
9.0
1
28.2
(176
.1)
(4
3.7)
2,32
7.4
1
327.
5
1,99
9.9
1
$
2.49
$
2.39
$
802.
7
836.
0
te o
f inc
orpo
ratio
n on
Ju
on a
nd e
ffec
t a tw
o-fo
r-an
d pe
r sha
re a
mou
nts
Twel
ve-M
onth
Per
iods
ED
ecem
ber 3
1,
arie
sf I
ncom
e
$
$
$
$
ties
y am
ende
d its
cer
tific
at
5.0
milli
on to
1.1
50 b
illio
Acc
ordi
ngly
, all
shar
e a
ock
split
.
T
tion
and
Subs
idia
ted
Stat
emen
ts o
fna
udite
d)ce
pt p
er s
hare
dat
a)
ing
amor
tizat
ion
ofss
ets)
t stra
tive
ntan
gibl
e as
sets
s, ne
tns
es
com
e, n
et
net es hare
:(1)
1) ts &
mar
keta
ble
secu
rit
gs quity
r app
rova
l, th
e C
ompa
nynu
mbe
r of
com
mon
sto
ck fr
om 5
75an
ding
com
mon
sto
ck. A
ect t
he im
pact
of t
he s
to
Cel
gene
Cor
pora
ten
sed
Con
solid
at (Un
(In m
illio
ns, e
xc
t pro
duct
sal
eshe
r rev
enue
Tota
l rev
enue
st o
f goo
ds s
old
(exc
ludi
acqu
ired
inta
ngib
le a
sse
arch
and
dev
elop
men
tlin
g, g
ener
al a
nd a
dmin
ism
ortiz
atio
n of
acq
uire
d in
quisi
tion
rela
ted
char
ges
Tota
l cos
ts a
nd e
xpen
erat
ing
inco
me
eres
t and
inve
stm
ent i
ncer
est (
expe
nse)
her i
ncom
e (e
xpen
se),
n
ome
befo
re in
com
e ta
xe
ome
tax
prov
ision
t inc
ome
t inc
ome
per c
omm
on s
hB
asic
Dilu
ted
ight
ed a
vera
ge s
hare
s:(
Bas
icD
ilute
d
lanc
e sh
eet i
tem
s:C
ash,
cas
h eq
uiva
len t
Tota
l ass
ets
Shor
t-ter
m b
orro
win
gLo
ng-te
rm d
ebt
Tota
l sto
ckho
lder
s' eq
Follo
win
g st
ockh
olde
r20
14, t
o in
crea
se th
e n
auth
orize
d sh
ares
of c
stoc
k sp
lit o
f its
out
sta
pres
ente
d he
rein
refleC
Con
de
72
Net
Oth
Cos
Res
Selli
Am
Acq
Ope
Inte
Inte
Oth
Inco
Inco
Net
Net
Wei
Bal (1)

Reconciliation Tables
8.4
for t
helv
e-m
onth
ility-
wei
ghte
d
.
9.9
8.5
4.7
5.8
- 2.6
- 2.8
1.1
0.0
2.3)
3.1
.10
.98
Dec
embe
r 31,
201
4 an
d $9
8to
talin
g $4
47.6
for t
he tw
e31
, 201
3.
hang
es in
est
imat
ed p
roba
bil
gani
zatio
n.es
ter P
harm
aceu
tical
s, In
cla
).uc
este
r, A
brax
is, A
vila
and
se
o ed
2014
2013
1,99
9.9
1,44
9$
26.2
18
196.
5
144
45
3.6
57
5
129.
2
-
224.
9
162
25
.0
-
258.
3
262
48.7
171
-
8 0
(263
.7)
(3
0 2
3,
098.
6
2,
563
$
3.86
3 .$
3.71
2.$
thre
e-m
onth
per
iod
ende
d D
sed
com
pens
atio
n ex
pens
e h
perio
d en
ded
Dec
embe
r 3lla
bora
tion
arra
ngem
ents
.t r
ecor
ded
as a
resu
lt of
ch
tribu
tions
to a
non
-pro
fit o
rgof
Pha
rmio
n C
orp.
, Glo
uce
omic
s R
esea
rch,
Inc.
(Avi
ld
to th
e ac
quisi
tions
of G
lou
S. G
AAP,
this
pre
ss r
elea
sve
stor
s an
d m
anag
emen
t d
tren
ds th
at fa
cilit
ate
tion.
The
se a
djus
ted
tion
to, b
ut n
ot a
s a
AP. W
e ty
pica
lly e
xclu
de
ic o
pera
tions
and
that
do
er c
ompa
nies
may
def
ine
wel
ve-M
onth
Per
iods
End
eD
ecem
ber 3
1,
ries
t Inc
ome
$
on
(1)
(1)
(2)
(3)
(1)
(4)
ts(5
)
nsid
erat
ion
(6)
(7)
(8)
$
$
$
nse
tota
ling
$128
.4 fo
r the
th1,
201
3. E
xclu
de s
hare
-bas
325.
8 fo
r the
twel
ve-m
onth
earc
h an
d de
velo
pmen
t col
men
t (IP
R&
D) i
mpa
irmen
t
tion
to m
ake
mat
chin
g co
ntr
acqu
ired
in th
e ac
quisi
tions
A
brax
is) a
nd C
elge
ne A
vilo
ngen
t con
sider
atio
n re
late
d
ed in
acc
orda
nce
with
U.S
hat w
e be
lieve
pro
vide
inv
pera
ting
perf
orm
ance
and
ect t
o pr
ojec
ted
info
rmat
uld
be c
onsi
dere
d in
add
itac
cord
ance
with
U.S
. GAA
not b
elie
ve a
ffec
t our
bas
ino
n-re
curr
ing
item
s. O
thT w
ratio
n an
d Su
bsid
iar
AA
P to
Adj
uste
d N
et, e
xcep
t per
sha
re d
ata)
P ustm
ents
:s
sold
(exc
ludi
ng a
mor
tizat
ioin
tang
ible
ass
ets)
:ed
com
pens
atio
n ex
pens
e
d de
velo
pmen
t:ed
com
pens
atio
n ex
pens
eol
labo
ratio
n ex
pens
em
pairm
ent
al a
nd a
dmin
istra
tive:
ed c
ompe
nsat
ion
expe
nse
of c
ontin
gent
obl
igat
ion
of a
cqui
red
inta
ngib
le a
sset
elat
ed c
harg
es, n
et:
fair
valu
e of
con
tinge
nt c
on
(exp
ense
), ne
tng
ass
et im
pairm
ent
x ad
just
men
tste
d
mm
on s
hare
- A
djus
ted
tmen
ts:
base
d co
mpe
nsat
ion
expe
npe
riod
ende
d D
ecem
ber 3
1D
ecem
ber 3
1, 2
014
and
$3nt
pay
men
t exp
ense
for r
ese
cess
rese
arch
and
dev
elop
mla
ted
to C
C-2
92.
men
t of a
con
tinge
nt o
blig
atiza
tion
of in
tang
ible
ass
ets
aA
brax
is B
ioSc
ienc
e In
c. (A
es in
the
fair
valu
e of
con
tin
ncia
l inf
orm
atio
n pr
epar
est
ed fi
nanc
ial m
easu
res
thin
form
atio
n re
latin
g to
op
en p
erio
ds a
nd w
ith r
esp
are
non-
GAA
P an
d sh
o unf
orm
atio
n pr
epar
ed in
as
that
man
agem
ent d
oes
nde
finiti
on o
f unu
sual
or
diff
eren
t way
s.
Cel
gene
Cor
por
Rec
onci
liatio
n of
GA
(In m
illio
ns,
73
Net
inco
me
- GA
AP
Bef
ore
tax
adju
Cos
t of g
oods
o
f acq
uire
d i
Shar
e-ba
se
Res
earc
h an
d
Sh
are-
base
Upf
ront
co
IPR
&D
im
Sel
ling,
gen
era
Shar
e-ba
se
Se
ttlem
ent
Am
ortiz
atio
n o
Acq
uisit
ion
re
C
hang
e in
f
Oth
er in
com
e
Non
-ope
rati n
Net
inco
me
tax
Net
inco
me
- A
djus
Net
inco
me
per c
omB
asic
Dilu
ted
Expl
anat
ion
of a
djus
t(1
)Ex
clud
e sh
are-
th
ree-
mon
th p
pe
riod
ende
d (2
)Ex
clud
e up
fron
(3)
Excl
ude
in-p
roc
cas
h flo
ws
rel
(4)
Excl
ude
settl
em(5
)Ex
clud
e am
orti
(G
louc
este
r),
(6)
Excl
ude
chan
ge
In a
dditi
on to
fina
nal
so c
onta
ins
adju
sw
ith s
uppl
emen
tal i
com
pari
sons
bet
we
finan
cial
mea
sure
s su
bstit
ute
for,
the
ince
rtai
n G
AAP
item
sno
t mee
t the
GAA
P th
ese
mea
sure
s in
dR

Appendix

Citations for REVLIMID® Mechanism of Action
1. Reddy N, Hernandez-Ilizaliturri FJ, Deeb G, et al. Immunomodulatory drugs stimulate natural killer-cell function, alter cytokine production by dendritic cells, and inhibit angiogenesis enhancing the anti-tumor activity of rituximab in vivo. Br J Haematol. 2007;140:36-45.
2. Schafer PH, Gandhi AK, Loveland MA, et al. Enhancement of cytokine production and AP-1 transcriptional activity in T cells by thalidomide-related immunomodulatory drugs. J Pharm Exp Ther. 2003;3051222-1232.
3. Haslett PA, Hanekom WA, Muller G, Kaplan G. Thalidomide and a thalidomide analogue drug costimulate virus-specific CD8+ T cells in vitro. J Infect Dis. 2003;187:946-955.
4. Chang DH, Liu N, Klimek V, et al. Enhancement of ligand-dependent activation of human natural killer T cells by lenalidomide: therapeutic implications. Blood. 2006;108:618-621.
5. Davies FE, Raje N, Hideshima T, et al. Thalidomide and immunomodulatory derivatives augment natural killer cell cytotoxicity in multiple myeloma. Blood. 2001;98:210-216.
6. Tai YT, Li XF, Catley L, et al. Immunomodulatory drug lenalidomide (CC-5013, IMiD3) augments anti-CD40 SGN-40-induced cytotoxicity in human multiple myeloma: clinical implications. Cancer Res. 2005;65:11712-11720.
7. Wu L, Adams M, Carter T, et al. Lenalidomide enhances natural killer cell and monocyte-mediated antibody-dependent cellular cytotoxicity of rituximab-treated CD20+ tumor cells. Clin Cancer Res. 2008;14:4650-4657.
8. Baz R, Dimopoulos M, Richardson P, et al. Lenalidomide-based therapy leads to improvement of humoral immunity in relapsed or refractory multiple myeloma patients who respond to the therapy. Haematologica. 2009;94:159[Abstract 0395].
9. Noonan KA, Ferguson A, Emerling L, et al. Lenalidomide augments immune responses to Prevnar® vaccination in relapsed myeloma patients: implications for cancer and infectious vaccines. Blood (ASH Annual Meeting Abstracts). p y p p ( g )2009;114:739-740[Abstract 1864].
75

Lymphoma Prevalence
Disease overview
DLBCL (aggressive) Diffuse large B-cell lymphoma 300K
PREVALENCETYPE
FL (indolent) Follicular lymphoma 190K
MCL (aggressive) Mantle cell lymphoma 30KB cell MCL (aggressive) Mantle cell lymphoma 30K
Other indolent lymphomas Marginal zone, WM etc. 210KNHL
B-cell
Other aggressiveNHL Burkitt etc. 155K
CTCL (indolent) Cutaneous T-cell lymphoma 10KC C ( do e t) Cuta eous ce y p o a 0
PTCL (aggressive) Peripheral T-cell lymphoma 35K
T t l P l 930K
T-cell
76
Notes: 10-Year Prevalence across US, EU5, and Japan (2015)Source: Kantar Health
Total Prevalence 930K

Celgene Pipeline
77
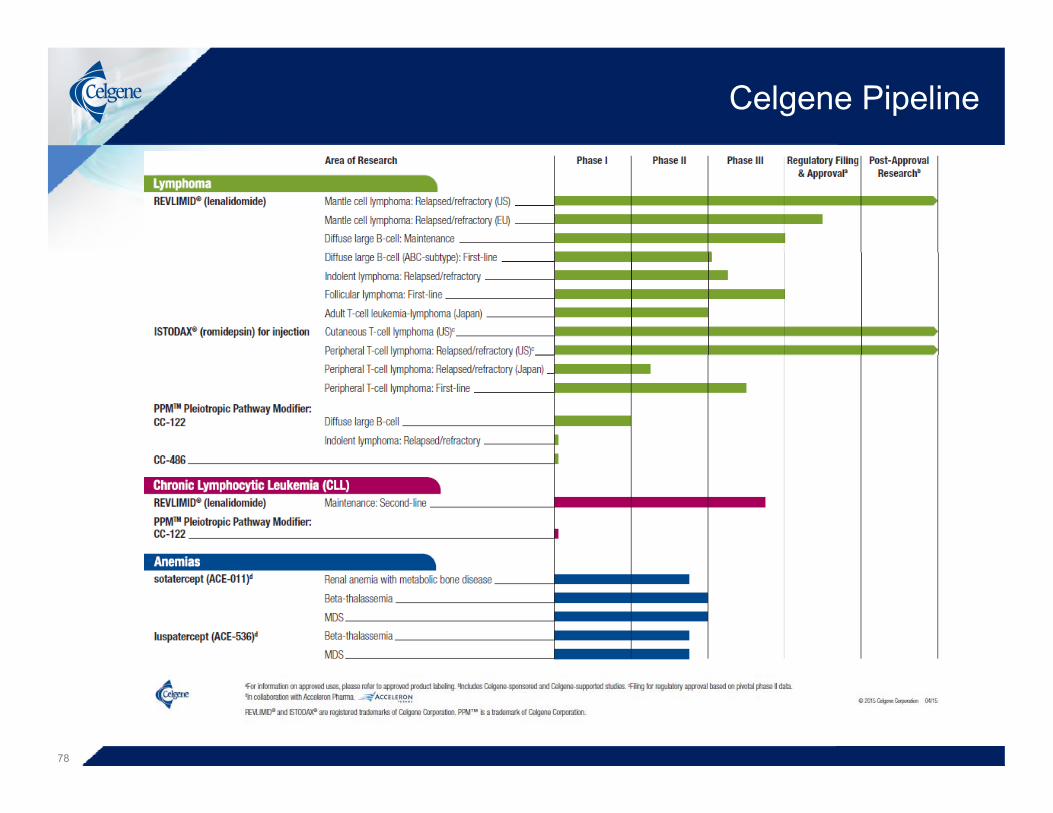
Celgene Pipeline
78

Celgene Pipeline
79

Celgene Pipeline
80

Celgene-Sponsored Trials in Presentation
Patient Population Adjuvant Therapy in Surgically Resected Pancreatic Cancer
Locally Advanced Pancreatic Cancer
T i l NPANC-003
Trial NameAPACT
PANC-007
Phase III II
Target Enrollment 800 110Target Enrollment 800 110
DesignArm A: ABRAXANE® (125 mg/m2) / Gemcitabine (1000 mg/m2) D 1, 8 and 15 for 6 28-day cyclesA B G it bi (1000 / 2) D 1 8 d
ABRAXANE® (125 mg/m2) D 1,8 and 15 / Gemcitabine (1000 mg/m2) D 1, 8, and 15 for 6
28-day cyclesSubjects who complete 6 cycles w/o PD or
unacceptable toxicities can:gArm B: Gemcitabine (1000 mg/m2) D 1, 8 and
15 for 6 28-day cycles. Continue on therapyGo on to chemoradiation
Go on to surgical intervention
Primary Endpoint Disease Free Survival Time to Treatment FailurePrimary Endpoint Disease Free Survival Time to Treatment Failure
Status Trial enrolling Trial enrolling
81

Celgene-Sponsored Trials in Presentation
Patient PopulationPts with Advanced Pancreatic Cancer Who Have Cholestatic
Hyperbilirubenemia
Trial Name PANC-004
Phase I
Target Enrollment 60
Design
ABRAXANE® at 3 different doses (75, 100 and 125 mg/m2) on D 1, 8, and 15 / Gemcitabine at 3different doses (600, 800 and 1000 mg/m2) on D
1, 8 and 15 for a 28-day cycleDesign Subject with three different levels of bilirubin are
evaluatedBilirubin level > 1.5 x ULN to 2 x ULN, > 2 x ULN
to 3 x ULN and > 3 x ULN to 5 x ULN
MTD, Pharmacokinetics, Apparent volume of distribution at the steady state and Apparent total
Primary Endpointdistribution at the steady state and Apparent total
body clearance
St t T i l lliStatus Trial enrolling
82

Celgene-Sponsored Trials in Presentation
Patient Population
Advanced NSCL Cancer in the Elderly
First Line NSCLC Subjects With ECOG
PS2Second Line Advanced Nonsquamous NSCLC
NSCL 005 NSCL 004Trial Name
NSCL-005Abound.70+
NSCL-004Abound.PS2
Abound.2L
Phase IV II II
Target 284 50 160Target Enrollment 284 50 160
Arm A: ABRAXANE® (100 mg/m2) D 1, 8, and 15 / Carboplatin (AUC=6 mg*min/mL) D 1 of a 21-day cycle
ABRAXANE® (100 mg/m2) D 1 and 8 / Carboplatin (AUD=5
Arm A: ABRAXANE® (100 mg/m2) D 8 and 15 / CC-486
(200 mg) daily D 1-4 for a 21-day cycle
Designmg min/mL) D 1 of a 21 day cycle
Arm A: ABRAXANE® (100 mg/m2) D 1, 8, and 15 / Carboplatin (AUC=6 mg*min/mL) D 1 of a 28-day cycle
and 8 / Carboplatin (AUD=5 mg*min/mL) D 1 of a 21-day
cycle
y yArm B ABRAXANE® (100
mg/m2) D 1 and 8 for a 21-day cycle
Primary Endpoint
Percentage of participants who will experience either peripheral
neuropathy or myelosuppressionSafety Progression Free Survival
Status Trial Enrolling Trial Enrolling Trial EnrollingStatus Trial Enrolling Trial Enrolling Trial Enrolling
83

Celgene-Sponsored Trials in Presentation
Patient Population First Line Stage IIIB / IV Squamous NSCLC
Trial NameNSCL-003
Abound sqmAbound.sqm
Phase III
Target Enrollment 260
Design
Arm A: Induction – ABRAXANE® (100 mg/m2) D 1, 8 and 15 / Carboplatin (6 mg/min/ml) D 1 of a 21-day cycle; Maintenance – ABRAXANE® (100 mg/m) D
1 and 8 of a 21-day cycle or Best supportive careArm B: Induction – ABRAXANE® (100 mg/m2) D 1, 8 and 15 / Carboplatin (6
mg/min/ml) D 1 of a 21-day cycle; Maintenance – Best supportive careg ) y y ; pp
Primary Endpoint Progression Free Survival
Status Trial enrolling
84
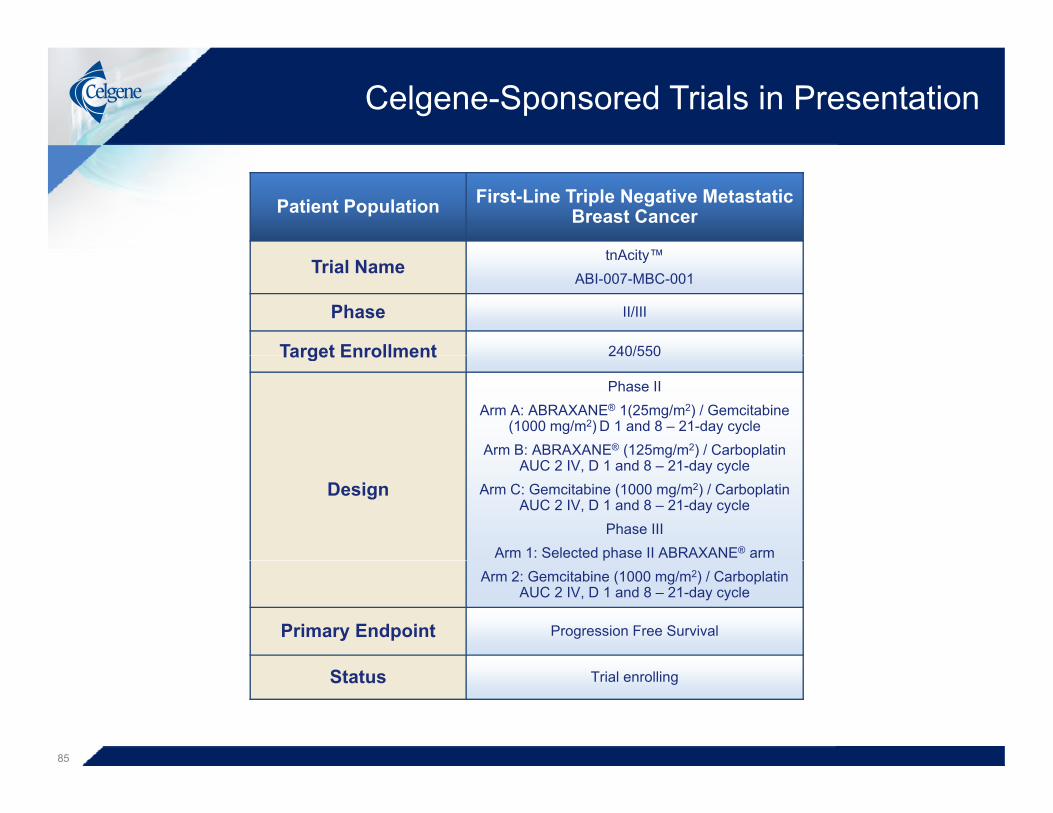
Celgene-Sponsored Trials in Presentation
Patient Population First-Line Triple Negative Metastatic Breast Cancer
tnAcity™Trial Name
tnAcity™ABI-007-MBC-001
Phase II/III
Target Enrollment 240/550Target Enrollment 240/550
Phase IIArm A: ABRAXANE® 1(25mg/m2) / Gemcitabine
(1000 mg/m2) D 1 and 8 – 21-day cycleArm B: ABRAXANE® (125mg/m2) / Carboplatin
DesignAUC 2 IV, D 1 and 8 – 21-day cycle
Arm C: Gemcitabine (1000 mg/m2) / Carboplatin AUC 2 IV, D 1 and 8 – 21-day cycle
Phase IIIArm 1: Selected phase II ABRAXANE® armp
Arm 2: Gemcitabine (1000 mg/m2) / Carboplatin AUC 2 IV, D 1 and 8 – 21-day cycle
Primary Endpoint Progression Free Survival
Status Trial enrolling
85
Top Related