







Languages
Pages
Legal

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 1/36
MUCOSAL VACCINE FOR
TUMOR THERAPY
Aliasgar Shahiwala, PhD
8th
International Symposium, Controlled Release Society-India Chapter

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 2/36
Mucosal system• Covers aerodigestive and urogenital as well as the
eye conjunctiva and the inner ear and the ducts of allendocrine glands are endowed with powerful
mechanical and chemical cleansing mechanismsthat degrade and repel most foreign matter.
• Contributes almost 80% of all immunocytes,accumulated in, or in transit between, various
mucosa-associated lymphoid organ system.• Comprised of anatomical defined lymphoid
microcompartments such as the Peyer patches, the
mesenteric lymph nodes, the appendix and solitaryfollicles in intestine, and the tonsils and adenoids atthe entrance of the aerodigestive tract, which serveas the principal mucosal inductive sites where
immune responses are initiated.

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 3/36

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 4/36

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 5/36
VaccinesLive attenuated pathogens•may induce cell mediated immunity, can cause disease in immuno-suppressedindividuals
•Some pathogens are difficult or impossible to grow in culture (e.g. HCV)
Whole inactivated organisms
Inactivated toxins
•generally proven ineffective at inducing cell mediated immunity which isnecessary for most difficult pathogens, which often establish chronicinfections (e.g., HIV, HCV, TB and Malaria).
•Many traditional inactivated vaccines (e.g. Bordetella pertussis) also containscomponents that can cause undesirable side effects and safety issues.
New Approaches
•Recombinant protein subunits
•synthetic peptides
•protein polysaccharide conjugates•plasmid DNA
These new approaches may offer important safety advantages, a general problem isthat the vaccines alone are poorly immunogenic. Therefore, there is an urgent need for
the development of potent and safe adjuvants and delivery systems that can be usedwith new generation vaccines, including DNA vaccines.

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 6/36
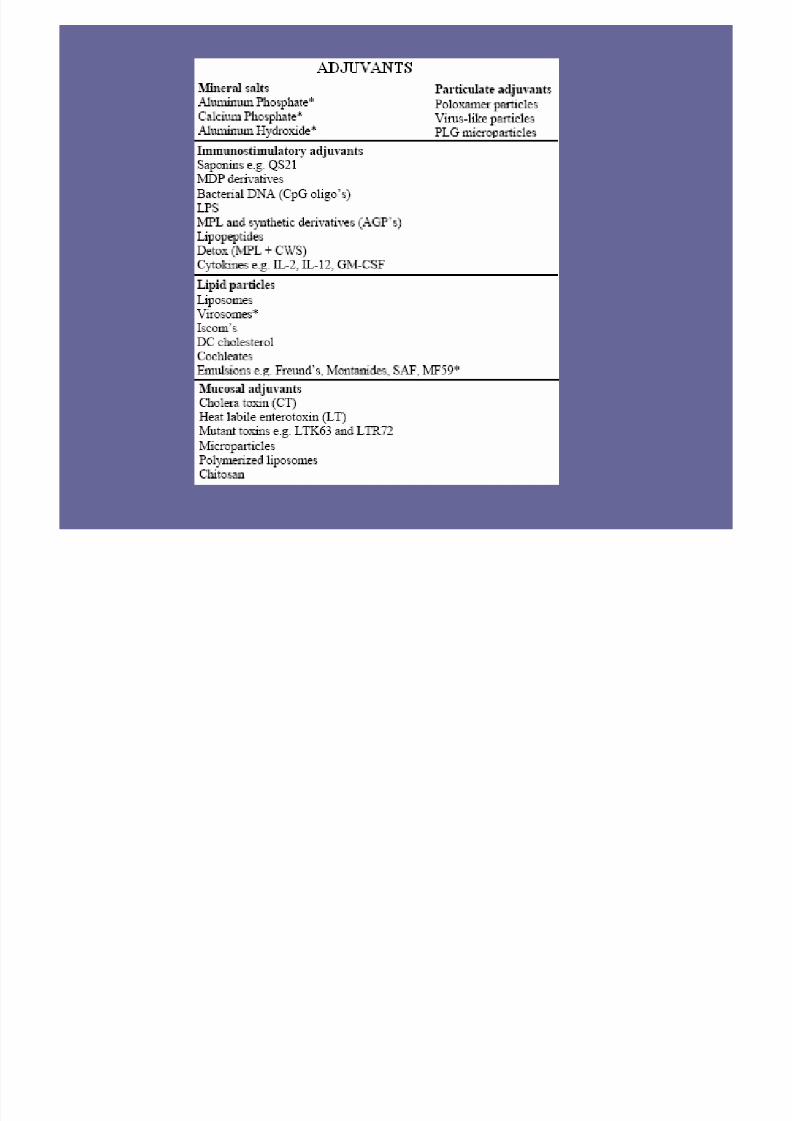
Adjuvants
Advantages Can increase the immunogenicity of weak antigens,
Enhance the speed and duration of the immune response,
Stimulate cell mediated immunity (CMI),
Promote the induction of mucosal immunity,
Enhance immune responses in immunologically immature, or senescent individuals, Decrease the dose of antigen in the vaccine and reduce costs,
Help to overcome antigen competition in combination vaccines.
Mechanisms of action
• For most of the adjuvants still remains only partially understood• Enhances delivery of the antigen to the lymph node
• Increase cellular infiltration into the injection site, so that more cells are present to takeup antigen (the principal mode of action of a range of particulate adjuvants, or antigendelivery systems e.g. microparticles, emulsions, liposomes, etc., may be to promote
uptake of the antigen by APC at the injection site.• In addition, some of these delivery systems may also be capable of moving away fromthe injection site in lymph and may deliver antigen directly to the lymph node.
• Particulate adjuvants (e.g. emulsions, microparticles, iscoms, liposomes, virosomes andvirus-like particles) have comparable dimensions to the pathogens which the immunesystem evolved to combat. Therefore, these particulates are normally taken up efficiently
by phagocytic cells of the innate immune system and function mainly to deliverassociated antigen into these key cells.
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 7/36

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 8/36

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 9/36
Approved Nanocarrier based vaccine
• EMULSIONSSqualene o/w emulsion based Influenza
vaccines approved in Italy in 1997, and for
several additional countries through mutualrecognition in 2000.
• LIPOSOMES
Liposomal vaccines based on viral membrane
proteins (virosomes) without additional
immunostimulators, have been extensively
evaluated in the clinic and are approved as
products in Europe for hepatitis A and influenza.
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 10/36
MUCOSAL VACCINATION FOR
TUMOR THERAPY
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 11/36
MULTIPLE EMULSIONS
W/O/W multiple emulsions are small (nanometer sized)
aqueous droplets entrapped within a larger oil droplets,
which are again stabilized and dispersed in a continuousaqueous phase.
• Taste masking
• Enzyme immobilization
• Sorbent for treatment of drug overdose
• Enhances enteral or dermal absorption
• Vaccine adjuvants
• Can encapsulate several active agents in a singleformulation and sequestering the different agents in
selective compartments for enhanced stability

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 12/36
Composition of an optimized W/O/W emulsion formulation
2 mLSaline
0.25%Tween® 80
2 mLW/O Emulsion
W/O/W Emulsion
0.8 mLSaline20%Span
®
80
1 mLSqualene Oil
W/O Emulsion
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 13/36
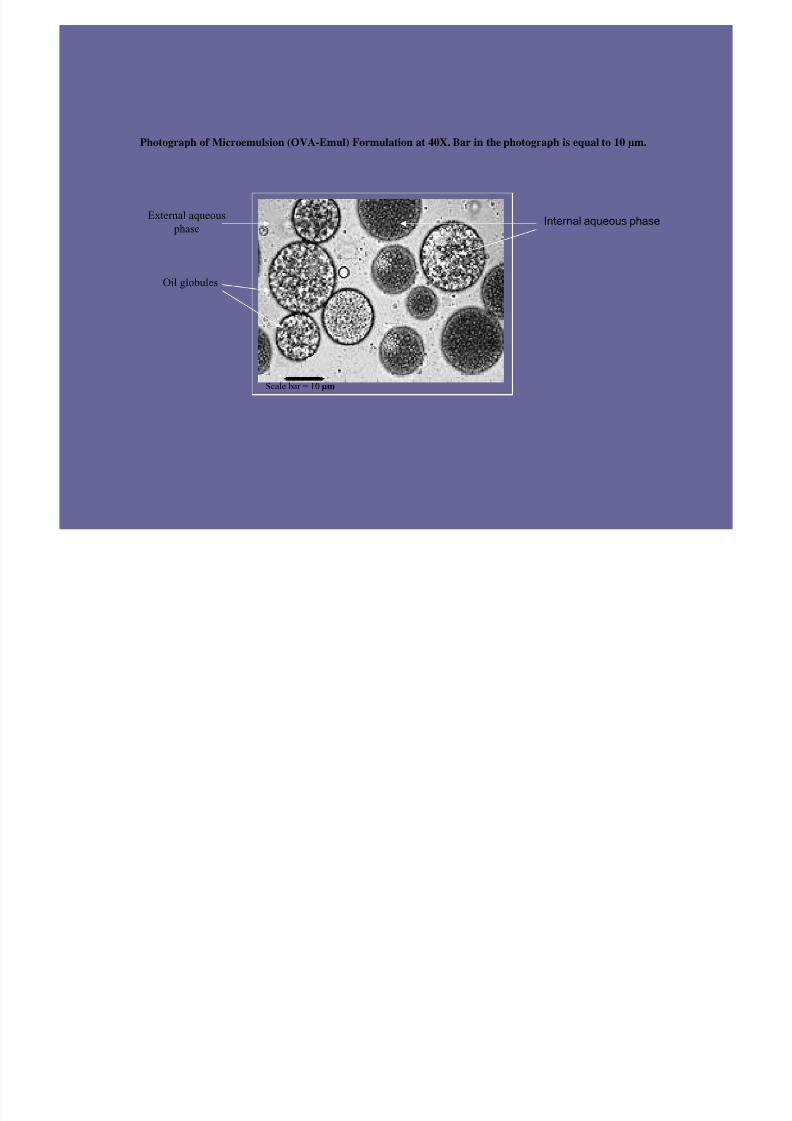
Photograph of Microemulsion (OVA-Emul) Formulation at 40X. Bar in the photograph is equal to 10 µm.
Internal aqueous phase
Oil globules
External aqueous
phase
Scale bar = 10 µm
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 14/36
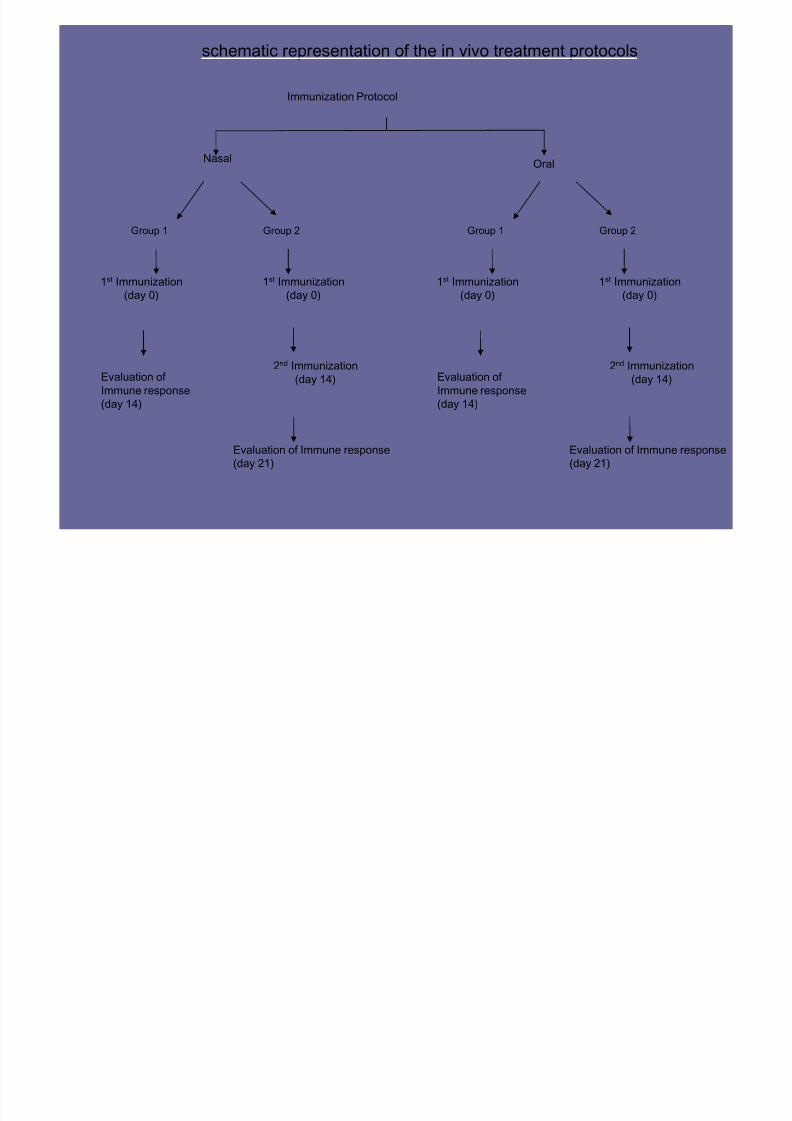
schematic representation of the in vivo treatment protocols
Immunization Protocol
NasalOral
Group 1 Group 2
1st Immunization
(day 0)
2nd Immunization
(day 14)
1st Immunization
(day 0)
Evaluation of
Immune response(day 14)
Evaluation of Immune response
(day 21)
Group 1 Group 2
1st Immunization
(day 0)
2nd Immunization
(day 14)
1st Immunization
(day 0)
Evaluation of
Immune response(day 14)
Evaluation of Immune response
(day 21)

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 15/36
0
5
10
15
20
25
30
35
OVA Saline OVA-Emul OVA-Emul-Chi
OVA Formulati on (100 mcg dose)
O V A - S p e c i f i c A n t i b o d y
I g G ( m c g / m L )
1st Immunization 2nd Immunization
OVA Specific IgG Response following Nasal and Oral Administration of Different Formulations. a and b showing OVA Specific IgG
Response following nasal and oral administration of different formulations respectively.
0
20
40
60
80
100
OVA Saline OVA-Emul OVA-Emul-Chi
OVA Formulation (100 mcg dose)
O V A - S p e c i f i c A n t i b o d y
I g G ( m c g / m L )
1st Immunization 2nd Immunization
a
b
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 16/36
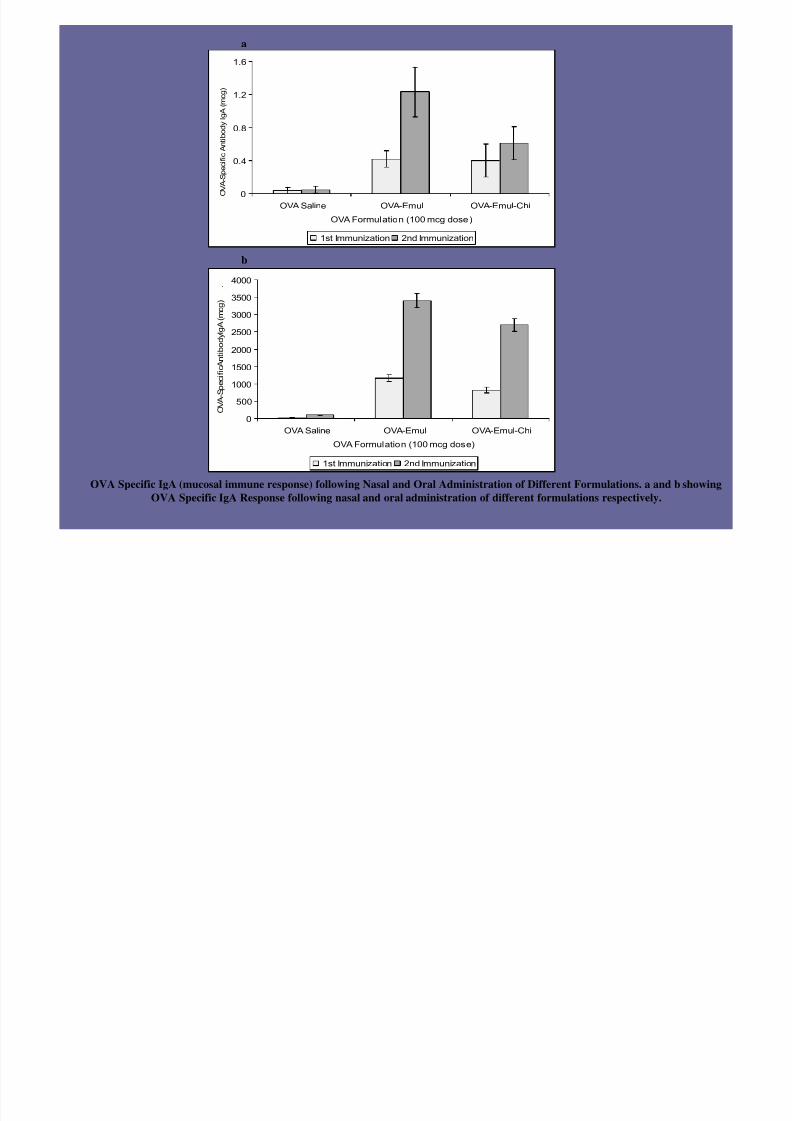
OVA Specific IgA (mucosal immune response) following Nasal and Oral Administration of Different Formulations. a and b showing
OVA Specific IgA Response following nasal and oral administration of different formulations respectively.
a
b
0
500
1000
1500
2000
2500
3000
3500
4000
OVA Saline OVA-Emul OVA-Emul-Chi
OVA Formulation (100 mcg dose)
O V A - S
p e c i f i c A n t i b o d y I g A ( m c g )
.
1st Immunization 2nd Immunization
0
0.4
0.8
1.2
1.6
OVA Saline OVA-Emul OVA-Emul-Chi
OVA Formulation (100 mcg dose)
O V A - S p e c i f i c A n t i b o d y I g A ( m
c g )
1st Immunization 2nd Immunization

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 17/36
• Melanoma is a malignant tumor of melanocytes that often starts
from harmless-looking moles. Once the tumor has started to
metastasize, the prognosis is generally poor. The metastases may
spread to any organ. Despite intensive research and numeroustherapeutic approaches, no satisfactory treatment is available today.
The first treatment of choice is, whenever possible, surgical removal
of the tumor.
• Active vaccination strategies represent a relatively new disciplinein the management of melanoma . Based on evidence that the immune
system plays a natural role in melanoma regression, there is well-
founded hope that the power of the immune system could be
enhanced by the use of melanoma vaccines. The key to an effective
tumor vaccine lies in the abili ty to overcome self-tolerance and to
specifically activate tumor-specific killer cells (i.e. cytotoxic T cells).
Melanoma
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 18/36
• Recent advances in the molecular identification of melanoma
specific antigens have given a significant boost to the study of
novel cancer vaccines.
• Glycoprotein GP100 is an antigen expressed in most humanmelanoma cells and can also be recognized by immune cells
including melanoma-derived tumor-infiltrating lymphocytes.
• Adoptive transfer of autologous, GP100-reactive, tumor-
infiltrating lymphocytes into melanoma patients, along with IL-2treatment, has been associated with tumor regression in some
patients.
• The antigen has been shown to be highly immunogenic and an
important target for active-specific immunotherapy in humans.
Gp100
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 19/36
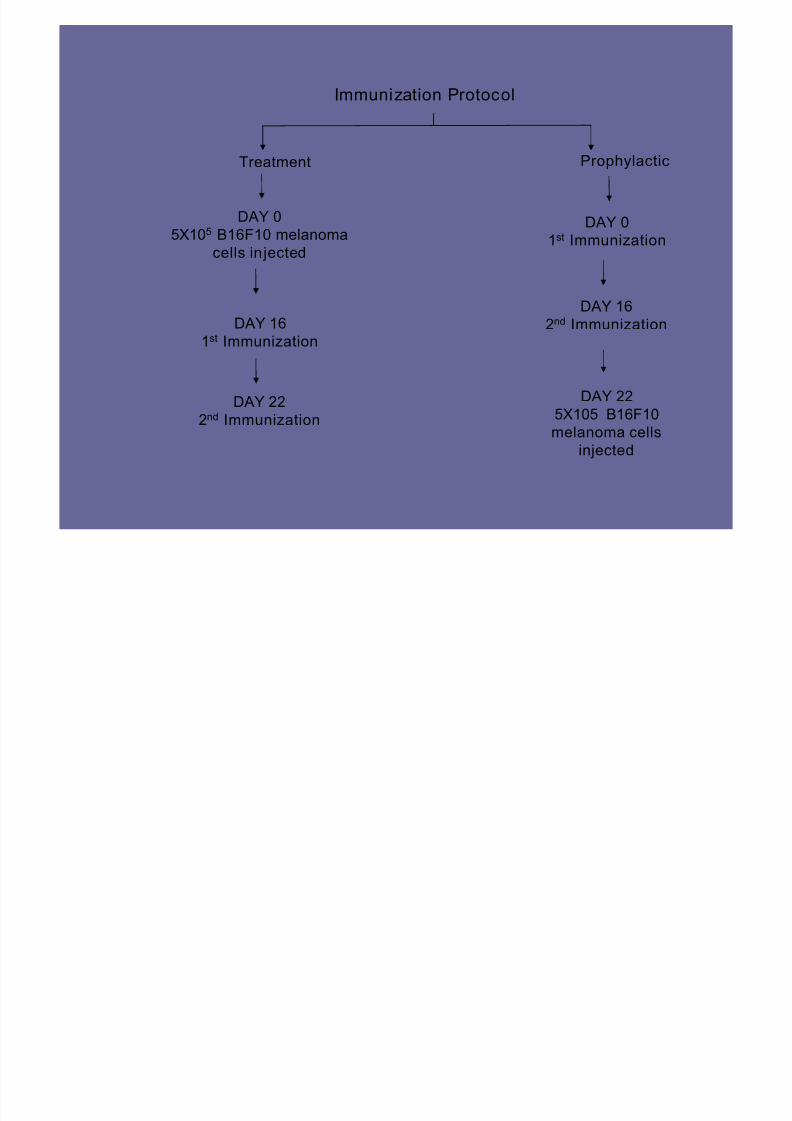
Immunization Protocol
Treatment Prophylactic
DAY 0
5X105 B16F10 melanoma
cells injected
DAY 22
2nd Immunization
DAY 16
1st Immunization
DAY 0
1st Immunization
DAY 225X105 B16F10
melanoma cells
injected
DAY 16
2nd Immunization
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 20/36
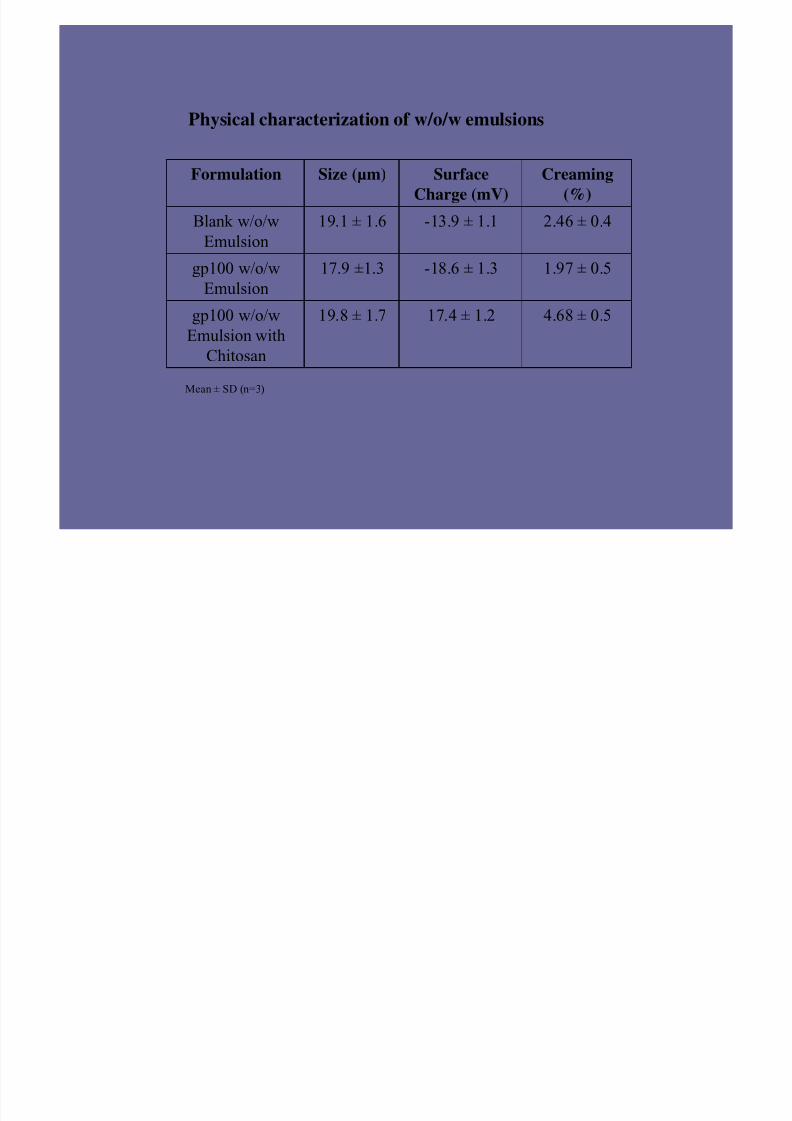
Physical characterization of w/o/w emulsions
4.68 ± 0.517.4 ± 1.219.8 ± 1.7gp100 w/o/w
Emulsion with
Chitosan
1.97 ± 0.5-18.6 ± 1.317.9 ±1.3gp100 w/o/w
Emulsion
2.46 ± 0.4-13.9 ± 1.119.1 ± 1.6Blank w/o/w
Emulsion
Creaming
(%)
Surface
Charge (mV)
Size (µm)Formulation
Mean ± SD (n=3)

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 21/36
0
1000
2000
3000
4000
5000
6000
12 14 16 18 20 22 24 26 28 30Days
T u m o
r v o l u m e ( m m 3
)
Control GP100 solution GP100-Emul-Chi GP100-Emul
1st dose
2nd dose
Change in tumor volume as a function of time: Treatment
Group
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 22/36
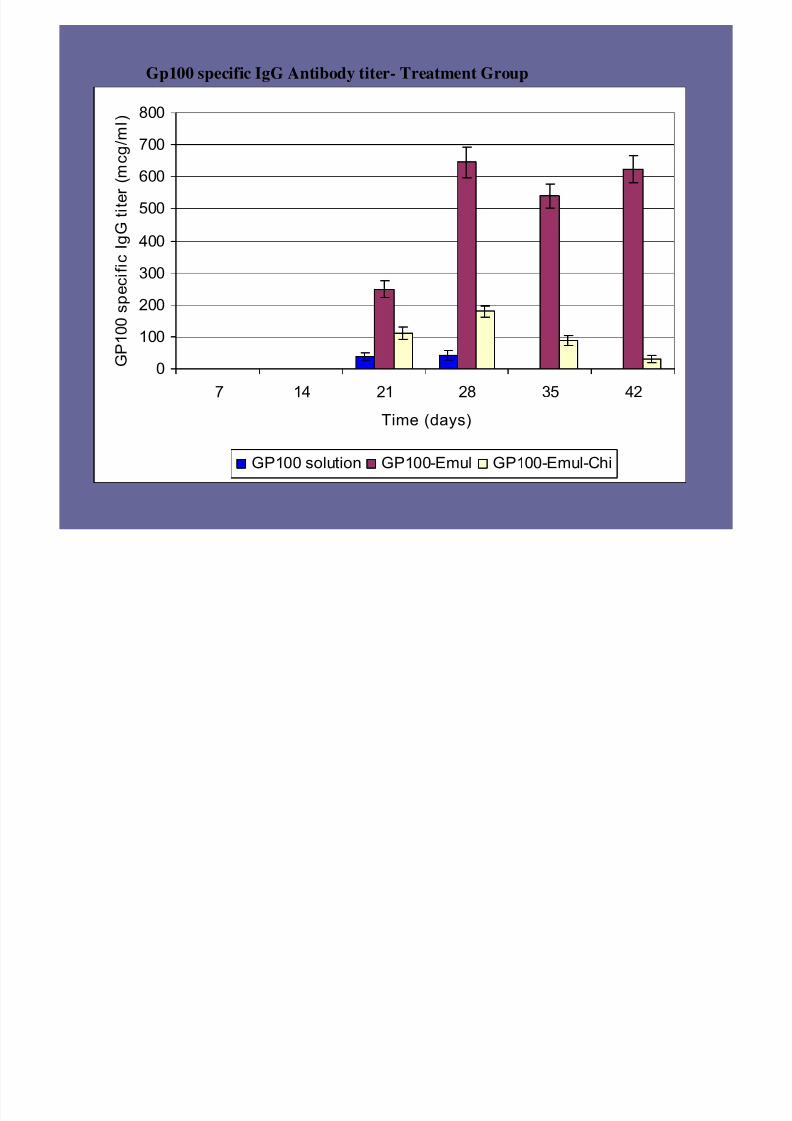
Gp100 specific IgG Antibody titer- Treatment Group
0
100
200
300
400
500
600
700
800
7 14 21 28 35 42
Time (days)
G P 1 0 0 s p e c i f i c I g G t i t e
r ( m c g / m l )
GP100 solution GP100-Emul GP100-Emul-Chi

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 23/36
Gp100 specific IgG Antibody titer- Prophylactic Group
0
100
200
300
400
500
600
700
7 14 21 28 35 42Time (days)
G P 1 0 0 s p
e c i f i c I g G t i t e
r ( m c g / m l )
GP100 solution GP100-Emul GP100-Emul-Chi
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 24/36
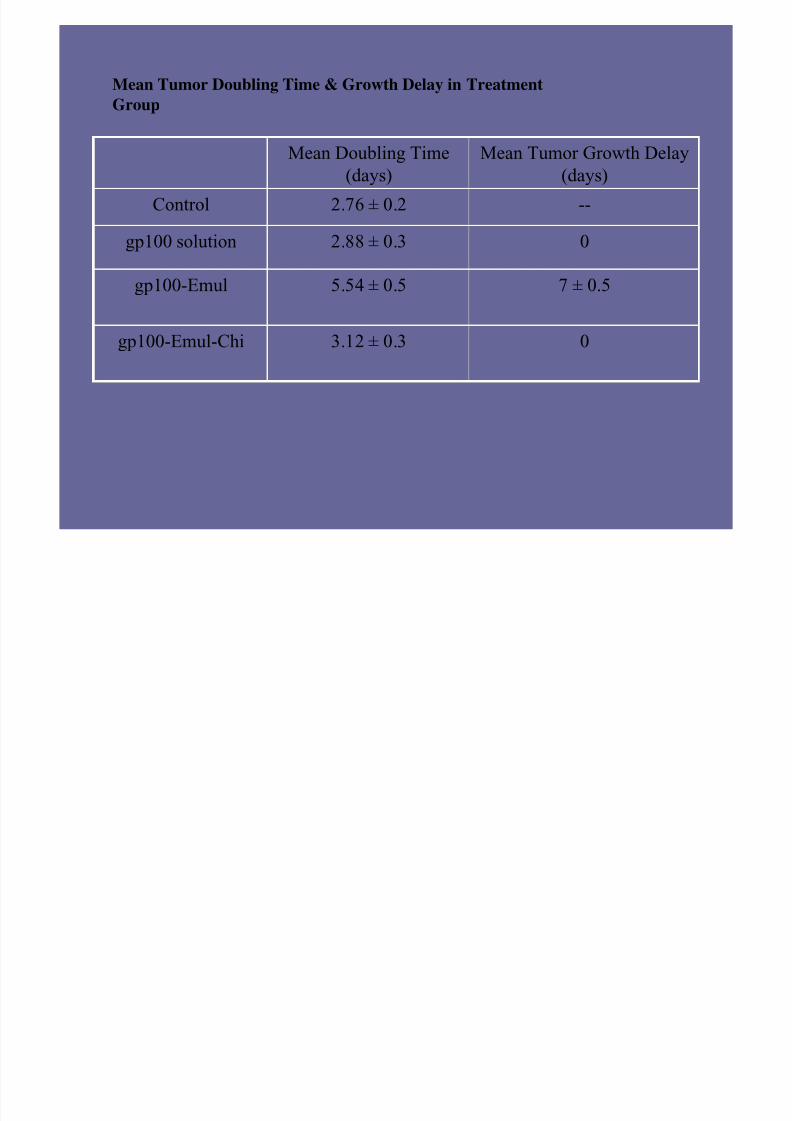
Mean Tumor Doubling Time & Growth Delay in Treatment
Group
03.12 ± 0.3gp100-Emul-Chi
7 ± 0.55.54 ± 0.5gp100-Emul
02.88 ± 0.3gp100 solution
--2.76 ± 0.2Control
Mean Tumor Growth Delay
(days)
Mean Doubling Time
(days)
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 25/36
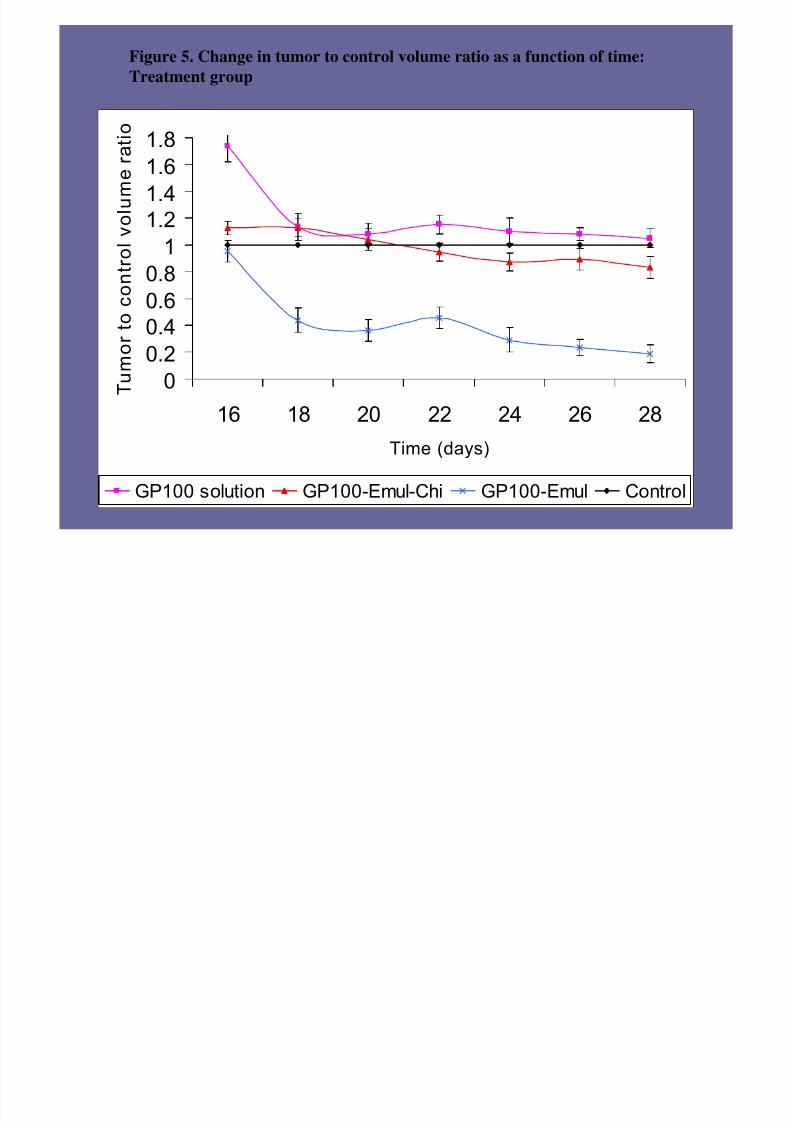
Figure 5. Change in tumor to control volume ratio as a function of time:
Treatment group
0
0.2
0.40.6
0.8
1
1.21.4
1.6
1.8
16 18 20 22 24 26 28
Time (days)
T u m o r t o c o n t r o l v o l u m e r a t i o
GP100 solution GP100-Emul-Chi GP100-Emul Control

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 26/36
The weights of the excised tumor mass-Treatment Group
0
0.5
1
1.52
2.5
3
3.5
4
4.5
Control gp100 solution gp100-Emul-Chi gp100-Emul
T u m o r W e i g h t ( g )
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 27/36
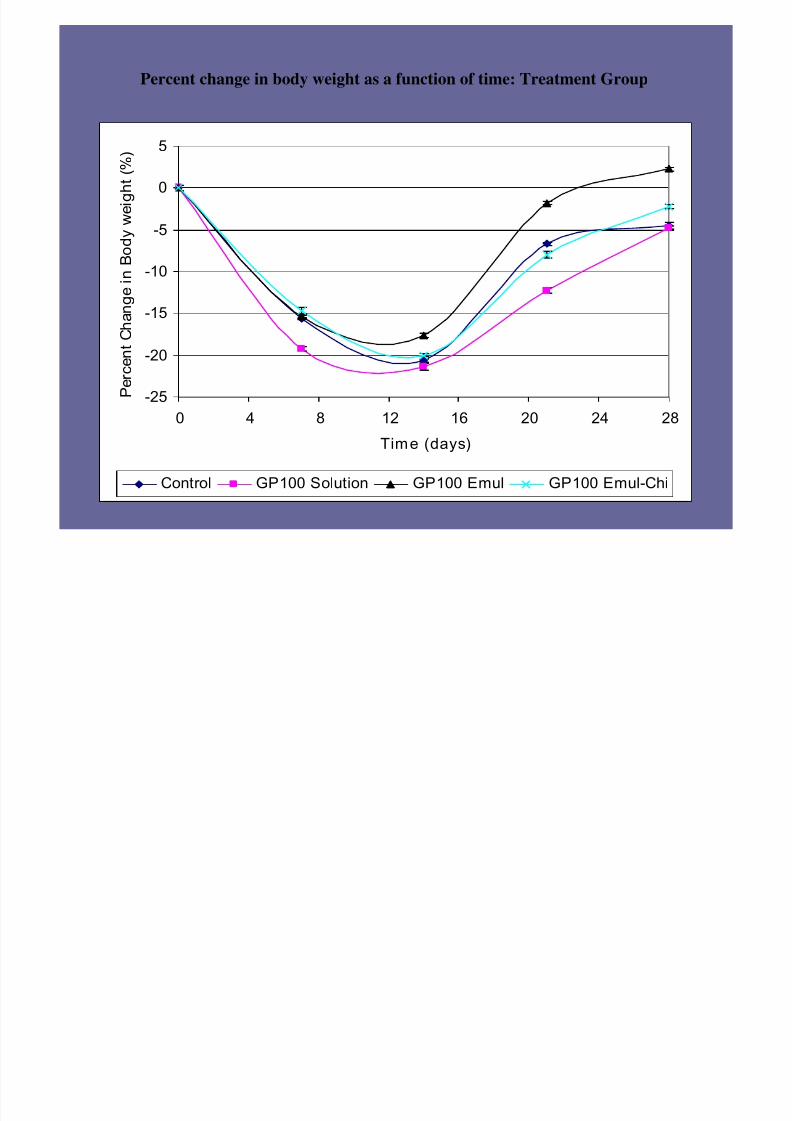
Percent change in body weight as a function of time: Treatment Group
-25
-20
-15
-10
-5
0
5
0 4 8 12 16 20 24 28
Time (days)
P
e r c e n t C h a n g e i n B o d y w e i g
h t ( % )
Control GP100 Solution GP100 Emul GP100 Emul-Chi
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 28/36
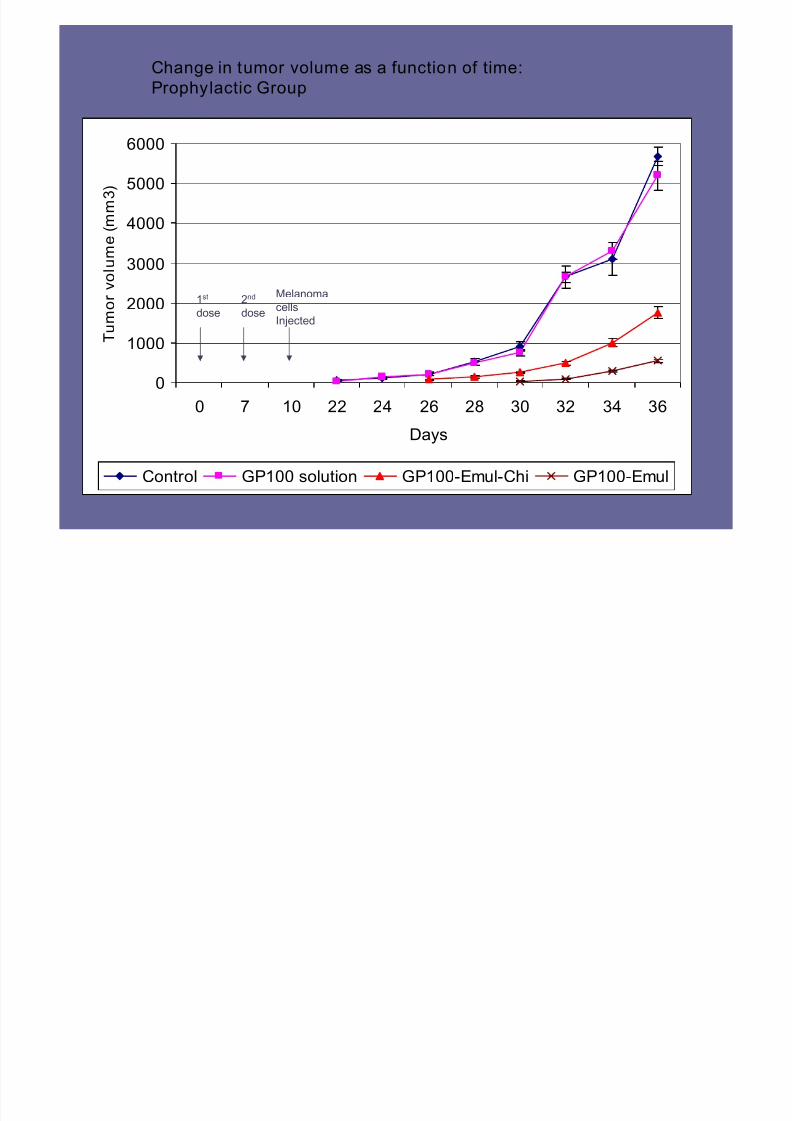
0
1000
2000
3000
4000
5000
6000
0 7 10 22 24 26 28 30 32 34 36
Days
T u m o r
v o l u m e ( m m 3 )
Control GP100 solution GP100-Emul-Chi GP100-Emul
1st
dose2nd
doseMelanomacells
Injected
Change in tumor volume as a function of time:
Prophylactic Group

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 29/36
Mean Tumor Growth Delay in Prophylactic Group
4 ± 0.5Gp100-Emul-Chi
8 ± 0.5Gp100-Emul
0gp100 solution
0Control
Mean Tumor Growth Delay
(days)
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 30/36
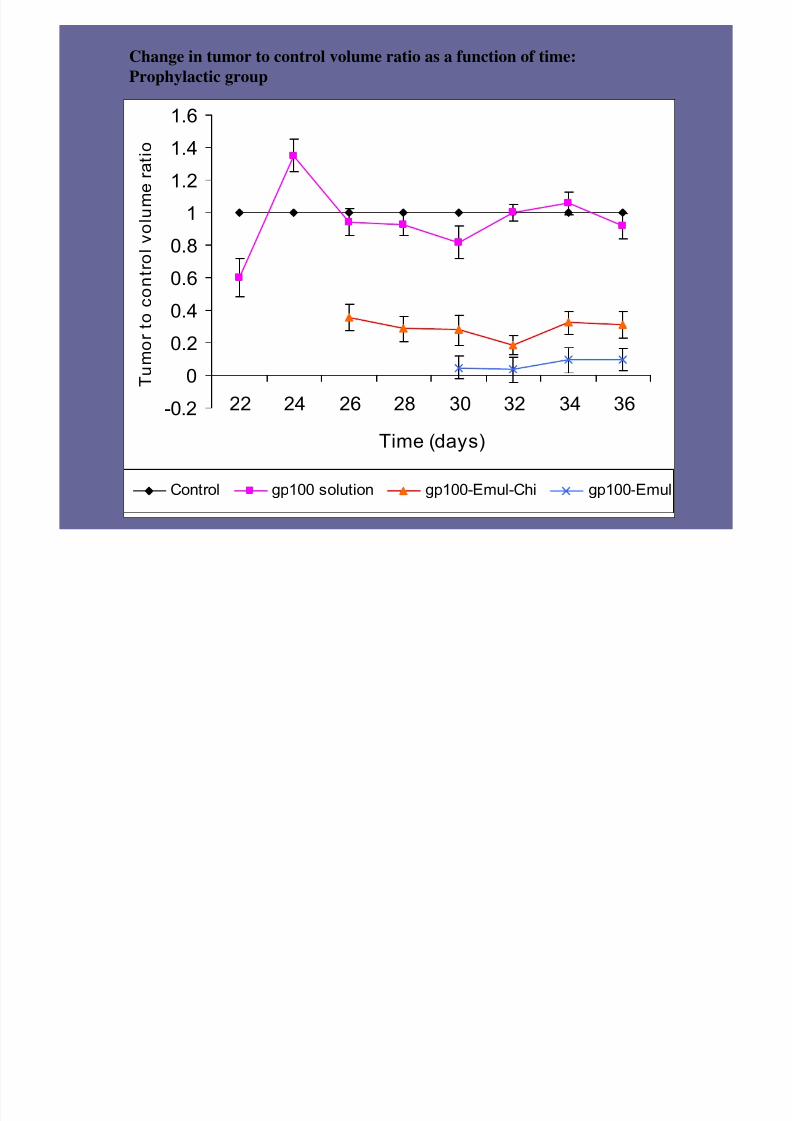
Change in tumor to control volume ratio as a function of time:
Prophylactic group
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
22 24 26 28 30 32 34 36
Time (days)
T u m o r t o c o n t r o l v o l u m
e r a t i o
Control gp100 solution gp100-Emul-Chi gp100-Emul
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 31/36
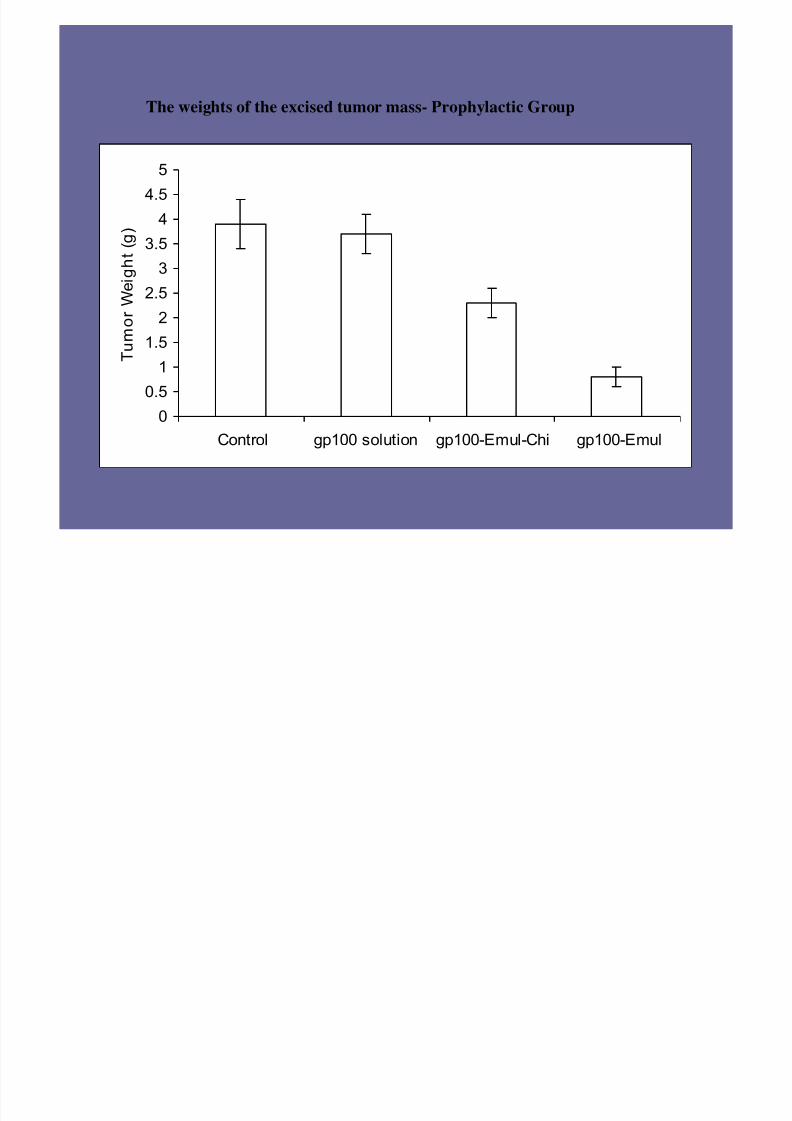
The weights of the excised tumor mass- Prophylactic Group
00.5
1
1.5
22.5
3
3.5
44.5
5
Control gp100 solution gp100-Emul-Chi gp100-Emul
T u m o r W
e i g h t ( g )
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 32/36
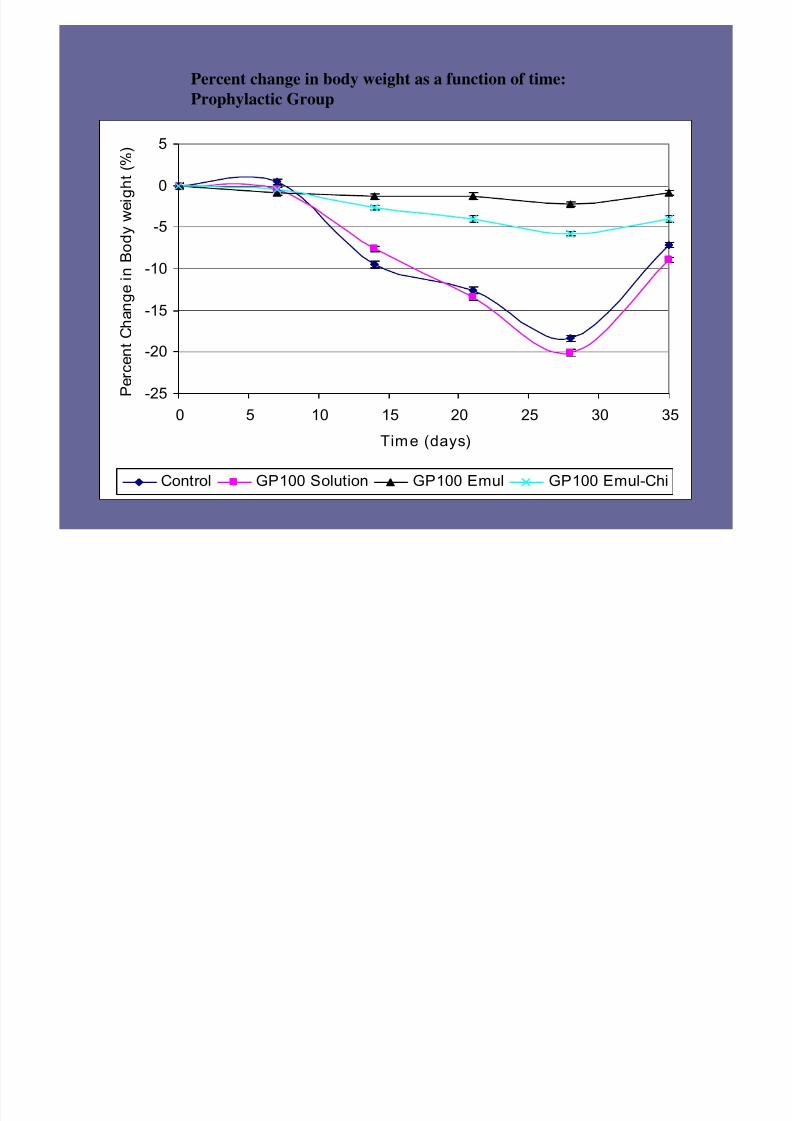
Percent change in body weight as a function of time:
Prophylactic Group
-25
-20
-15
-10
-5
0
5
0 5 10 15 20 25 30 35
Time (days)
P e r c e n t C h a n g
e i n B o d y w e i
g h t ( % )
Control GP100 Solution GP100 Emul GP100 Emul-Chi
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 33/36
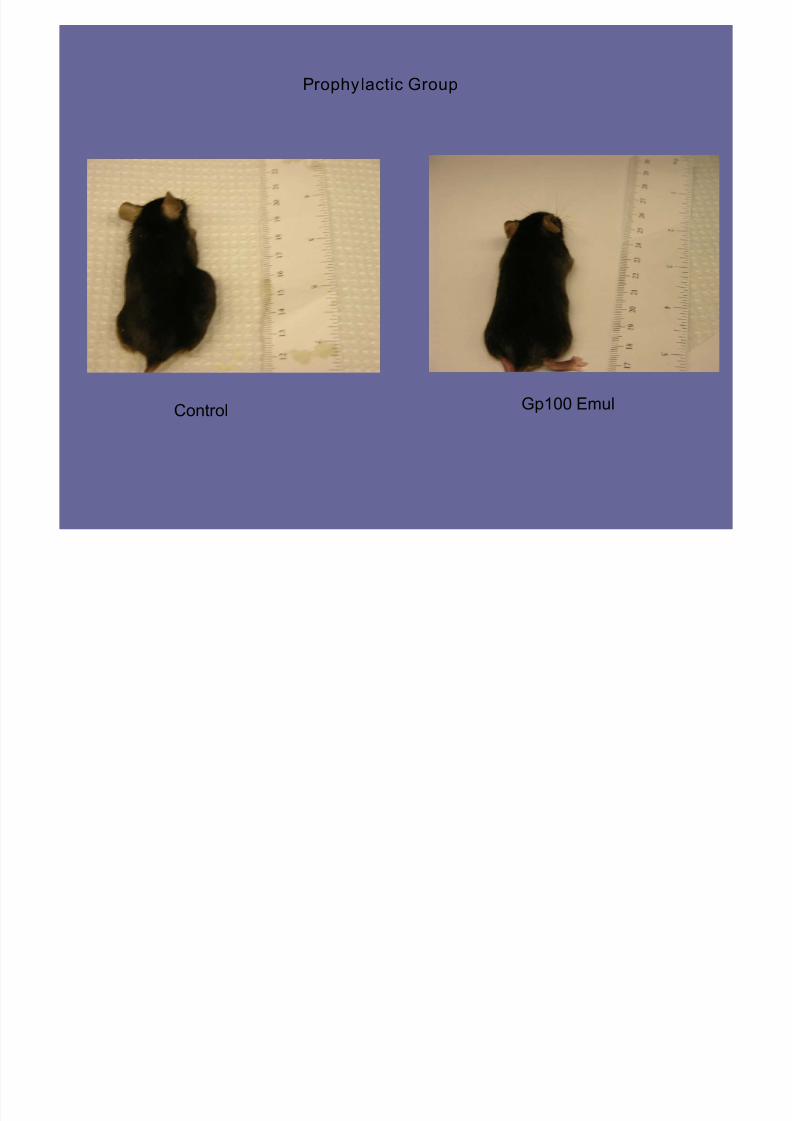
Control Gp100 Emul
Prophylactic Group

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 34/36
Excised Tumors-Prophylactic Group
Control Gp100 Solution
Gp100 Emul-Chi Gp100 Emul
7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 35/36
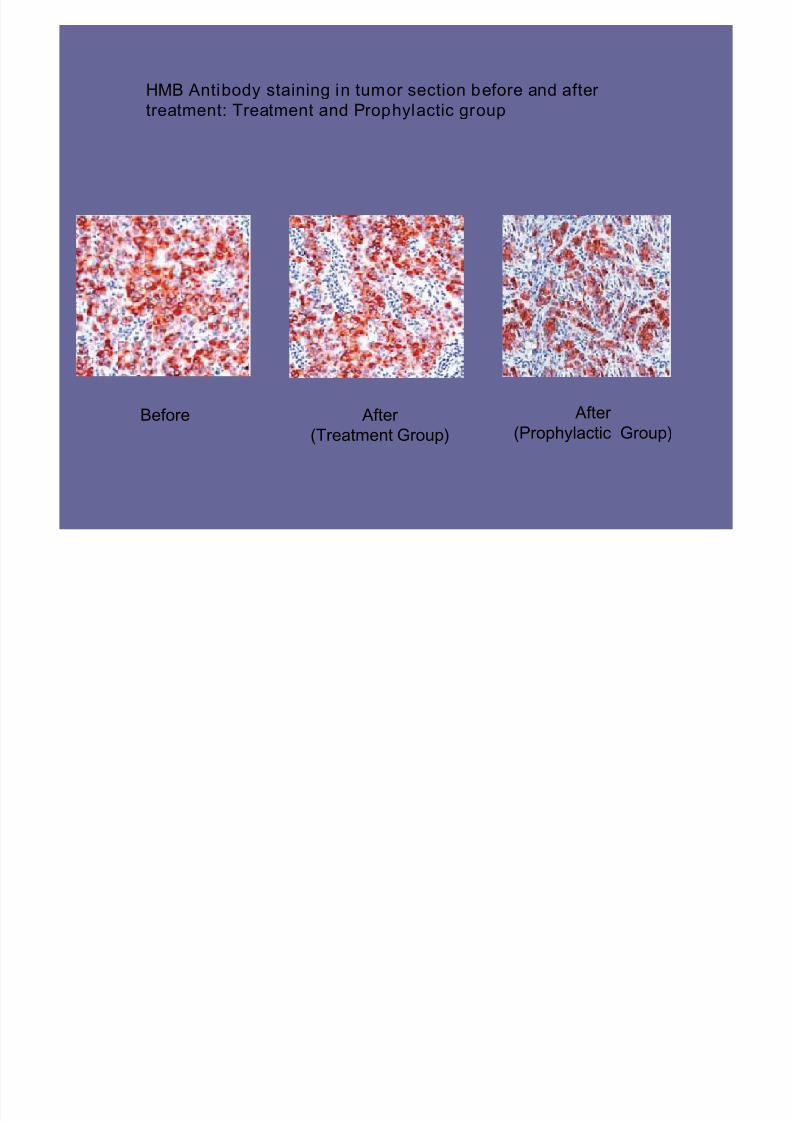
Before After
(Treatment Group)
HMB Antibody staining in tumor section before and after
treatment: Treatment and Prophylactic group
After
(Prophylactic Group)

7/23/2019 Aliasgar Shahiwala
http://slidepdf.com/reader/full/aliasgar-shahiwala 36/36
Thank you
Top Related