





Languages
Pages
Legal


Affymetrix Resequencing Arrays
Matthew SmithTrainee Presentation
West Midlands Regional Genetics Laboratory

Introduction• Autosomal recessive disorders are a major cause of infant morbidity
and mortality • Significantly higher in WM than rest of country (Bundy report, 1990)• Clinical phenotypes can be caused by mutations in one of several
genes or different mutated genes can cause very similar clinical phenotype
• Genes are analysed sequentially until a mutation is identified – Time consuming– Expensive– Medical management in absence of key information
Solution
• Screening all the genes at once– Next generation sequencing– Resequencing Arrays
• Offer rapid small scale diagnosis • Influence clinical management and prognosis

Resequencing Arrays
• 300kb sequence in 48hours• Sequences both forward and reverse strands simultaneously• Sequencing for “less than a penny a base”• Overall 1/6 the cost of conventional sequencing
• Amplify target of interest• Fragment DNA• Label DNA• Wash over Array• DNA hybridises to probe with
complementary sequence• Signal amplification• Signal Intensity determines identity
of base
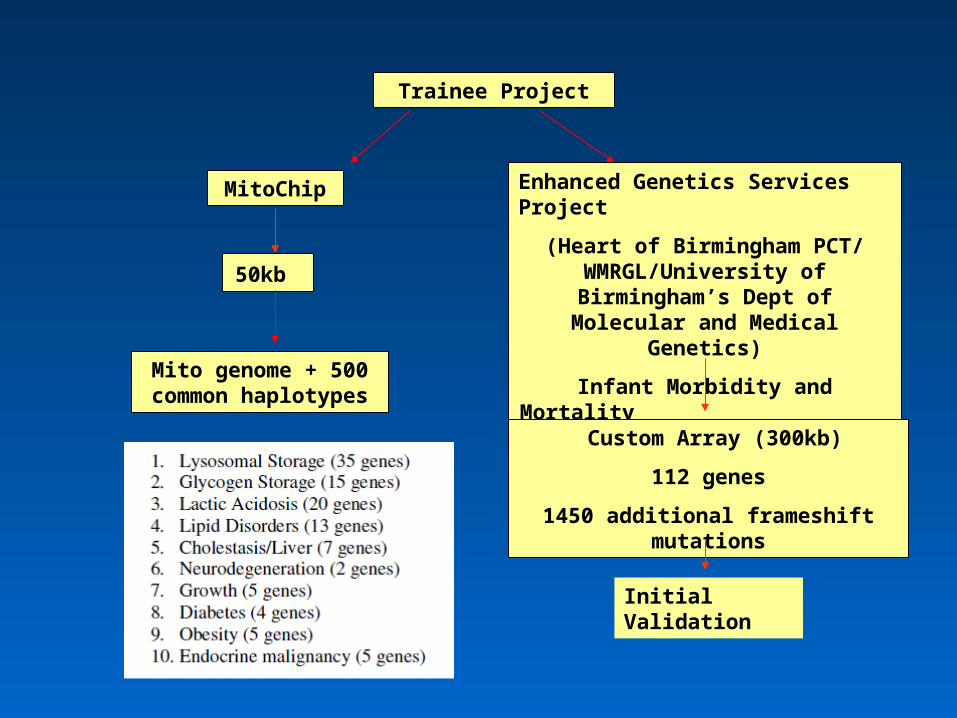
Trainee Project
MitoChip Enhanced Genetics Services Project
(Heart of Birmingham PCT/ WMRGL/University of Birmingham’s
Dept of Molecular and Medical Genetics)
Infant Morbidity and Mortality
50kb
Mito genome + 500 common haplotypes
Custom Array (300kb)
112 genes
1450 additional frameshift mutations
Initial Validation

Custom Array Design Exonic Tiling
Mutation Tiling
1231 Exons
1450 frameshift mutations
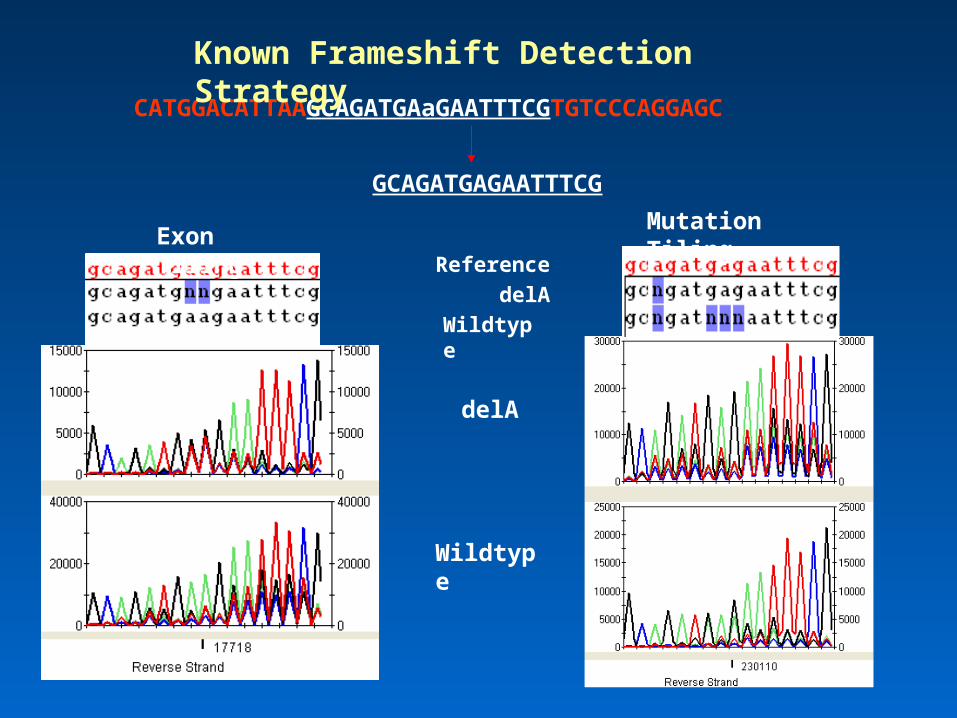
CATGGACATTAAGCAGATGAaGAATTTCGTGTCCCAGGAGC
GCAGATGAGAATTTCG
delA
Wildtype
Exon TilingMutation Tiling
delA
Wildtype
Reference
Known Frameshift Detection Strategy

Initial Validation
• Validation of a subset of genes
– SDHB, SDHC, SDHD, VHL partial coverage of RET
– PLA2G6
• Developed LPCRs
• Single exons from 26 patients comprising 27 nonsynonymous pathogenic mutations were interrogated on the array
• 27/27 mutations were detected.
• Sequenced 24988 bases• Call rate over 90% and a 99.8%
concordance with capillary sequencing
• No cross hybridisation
GeneArray Sequencing
Capillary Sequencing

Current Technical Limitations
• Reduced ability to detect insertions and deletion mutations
– Inclusion of probes complementary to known insertions or deletions– Possible to design array to detect these sorts of mutations– 10kb target
• 1-5bp deletions – 100,000 probes• 1-5bp insertions – 27,000,000 probes
– Advances in software and improvements in the GSeq algorithm– SeqC from JSI medical claims to detect insertions and deletions
• No Calls
– GSeq analysis is based on a learning algorithm– When it can not assign a genotype it assigns a no call– Majority of No calls are due to strings of C’s (60%) and can be called
uni-directionally.– Comparison of unique no calls could be indication of frameshift
mutation

Project outcomes
• Gained valuable expertise in the design and development of resequencing array technology
• Highlighted areas of development to make it suitable for diagnostics
Continuation of project
– Enhanced Genetics Service Project (Heart of Birmingham/WMRGL)– Major initiative to reduce childhood morbidity and mortality
• Carrier testing• Prenatal diagnosis
– 20 highest priority autosomal recessive conditions (clinical study)– Continue evaluation of resequencing methodology for diagnostic
use– Development of methods for unknown frameshift detection
(bioinformatics)– Evaluation of Array design

Conclusions
• Bridges the gap between current sequencing technology and next generation technology
• Potentially a powerful method for complex disease screening• Resequencing offers a targeted approach to mutation detection
– Rapid– Acute medical management
• Future Array designs• Smaller capacity array with a smaller number of genes• Modifier genes
Next Generation Sequencing
Huge Impact in Research Labs Impact on diagnostic Service
Full use of capacity
IT issues Gene Targeting

Acknowledgments
University Dept of Medical and Molecular Genetics
• Paul Gissen
• Chris Bruce
• Fatimah Rahman
WMRGL
• Fiona MacDonald
• Jennie Bell
• Dominic McMullan
Top Related