






Languages
Pages
Legal

Scenario
A 72-year-old woman presents to the emergency room after 2 episodes ofcoffee-ground emesis and a 1-day history of melena. She has no othergastrointestinal (GI) symptoms.
She complains of dizziness when standing, but denies shortness of breathand chest pain. She has a history of hypertension, diabetes, and coronaryartery disease. Three weeks ago, she sustained a myocardial infarction andhad 3 stents placed. She takes insulin, metformin, metoprolol, aspirin, andclopidogrel. Her heart rate is 98,blood pressure is 135/80
The physical examination is unremarkable except for melenic stool on rectalexamination. Relevant laboratory values include a hemoglobin level of 8.1,platelet count of 215, blood urea nitrogen level of 38, creatinine level of 1.2,and a normal INR.
Acute GI Bleeding
Romeo Mathew
MSc Nursing 2nd year
Manipal College of nursing, Manipal
Outline
1. Meaning
2. Etiology
3. Diagnostic History
4. Physical Examination
5. Interpretation of Findings
6. Pathophysiology with symptoms
7. Diagnosis
8. Treatment
9. Nursing Management
10. Risk Stratification
Meaning
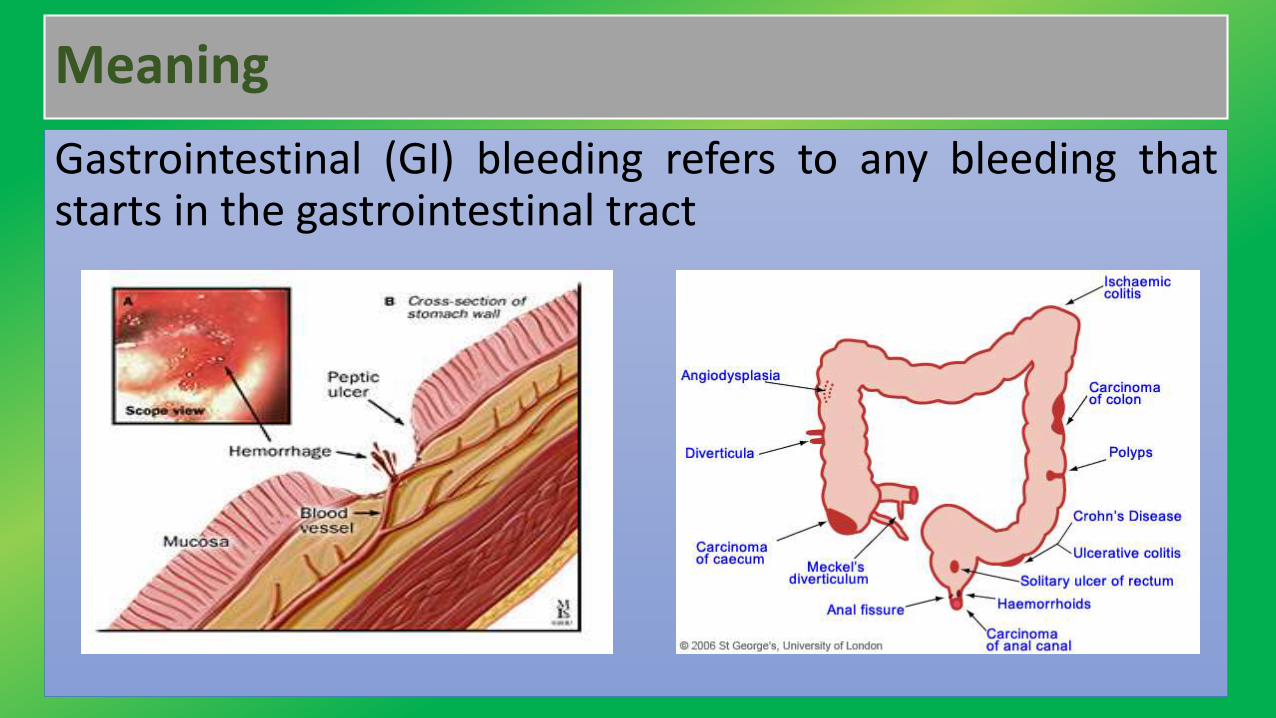
Gastrointestinal (GI) bleeding refers to any bleeding thatstarts in the gastrointestinal tract
Meaning
Bleeding may come from any site along the GI tract, but is oftendivided into:
• Upper GI bleeding: The upper GI tract includes the esophagus(the tube from the mouth to the stomach), stomach, and firstpart of the small intestine.
• Lower GI bleeding: The lower GI tract includes much of the smallintestine, large intestine or bowels, rectum, and anus.
Etiology
GI bleeding may be due to conditions including:
•Anal fissure
•Hemorrhoids
•Cancer of the colon
•Cancer of the small intestine
•Cancer of the stomach
• Intestinal polyps (a pre-cancerous condition)
Upper GI tract disorders
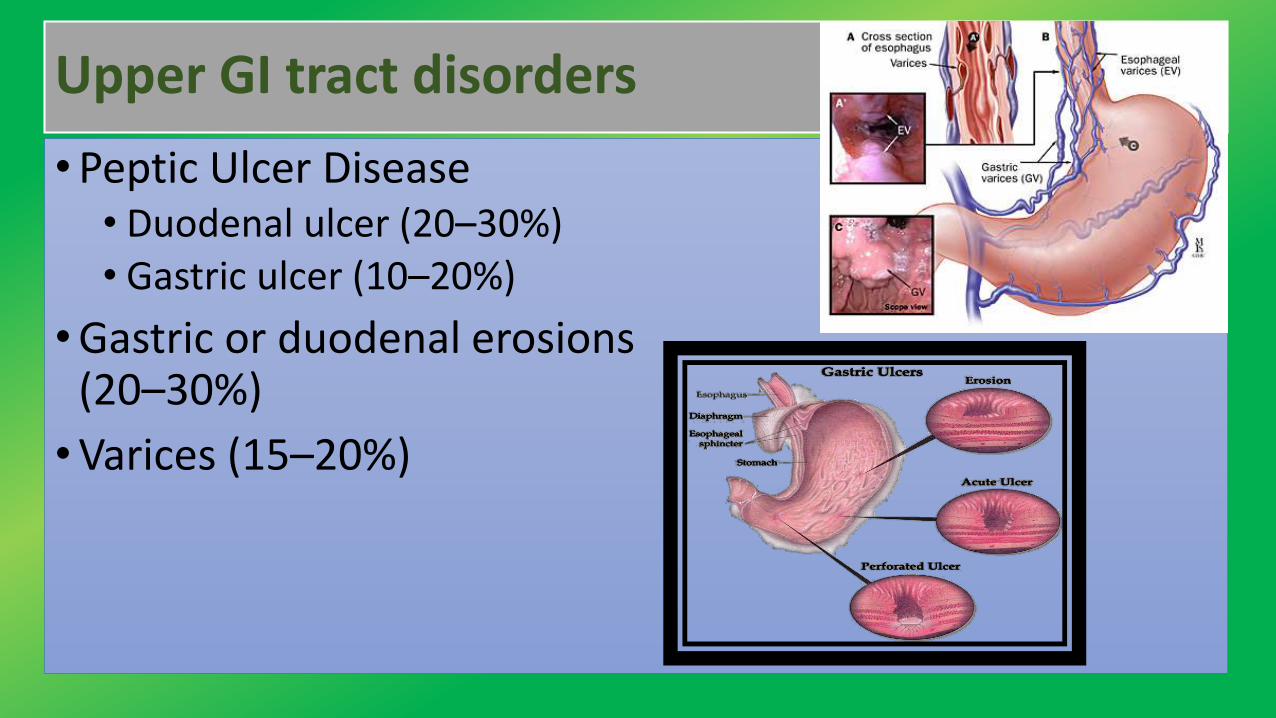
•Peptic Ulcer Disease• Duodenal ulcer (20–30%)• Gastric ulcer (10–20%)
•Gastric or duodenal erosions (20–30%)
•Varices (15–20%)
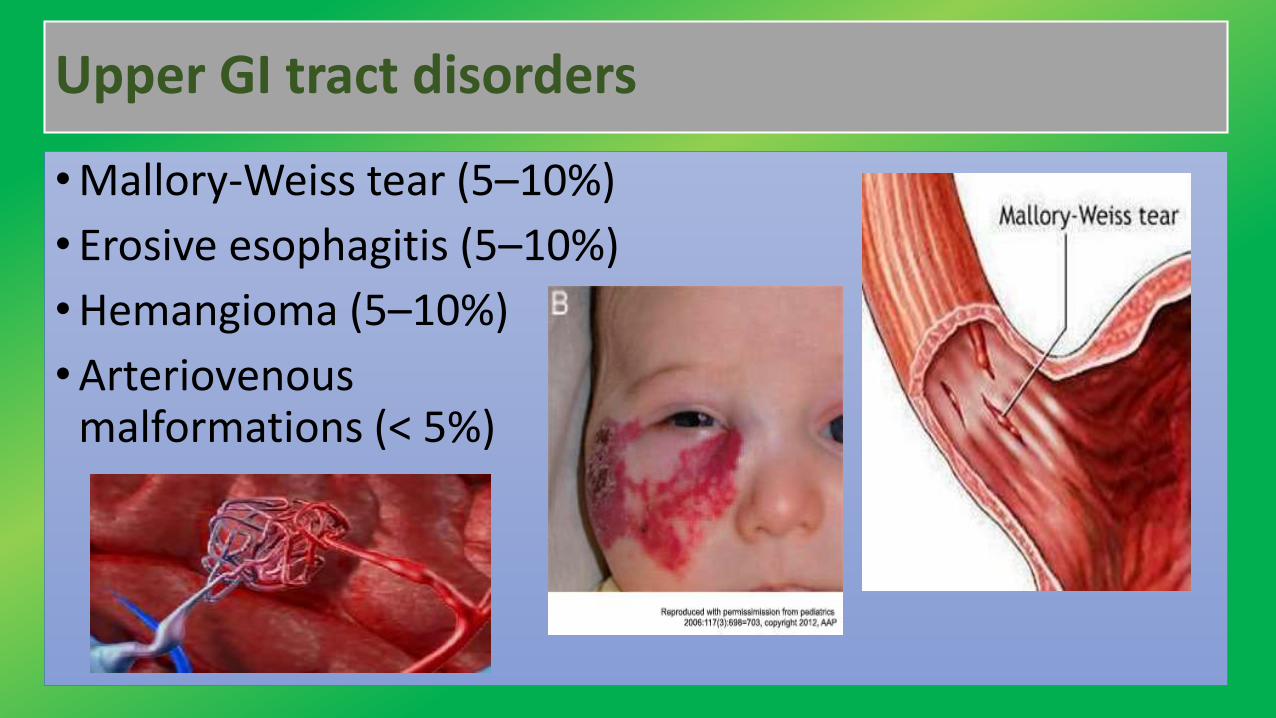
Upper GI tract disorders
•Mallory-Weiss tear (5–10%)
• Erosive esophagitis (5–10%)
•Hemangioma (5–10%)
•Arteriovenous malformations (< 5%)
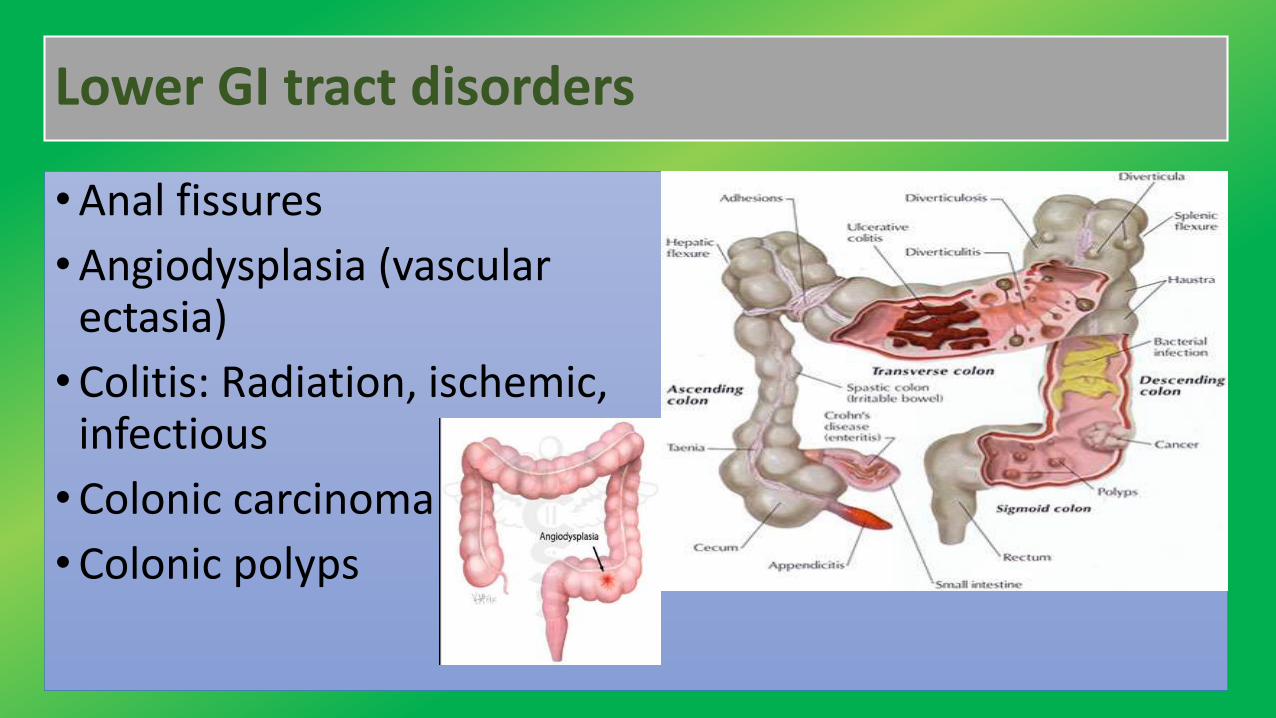
Lower GI tract disorders
•Anal fissures
•Angiodysplasia (vascular ectasia)
•Colitis: Radiation, ischemic, infectious
•Colonic carcinoma
•Colonic polyps
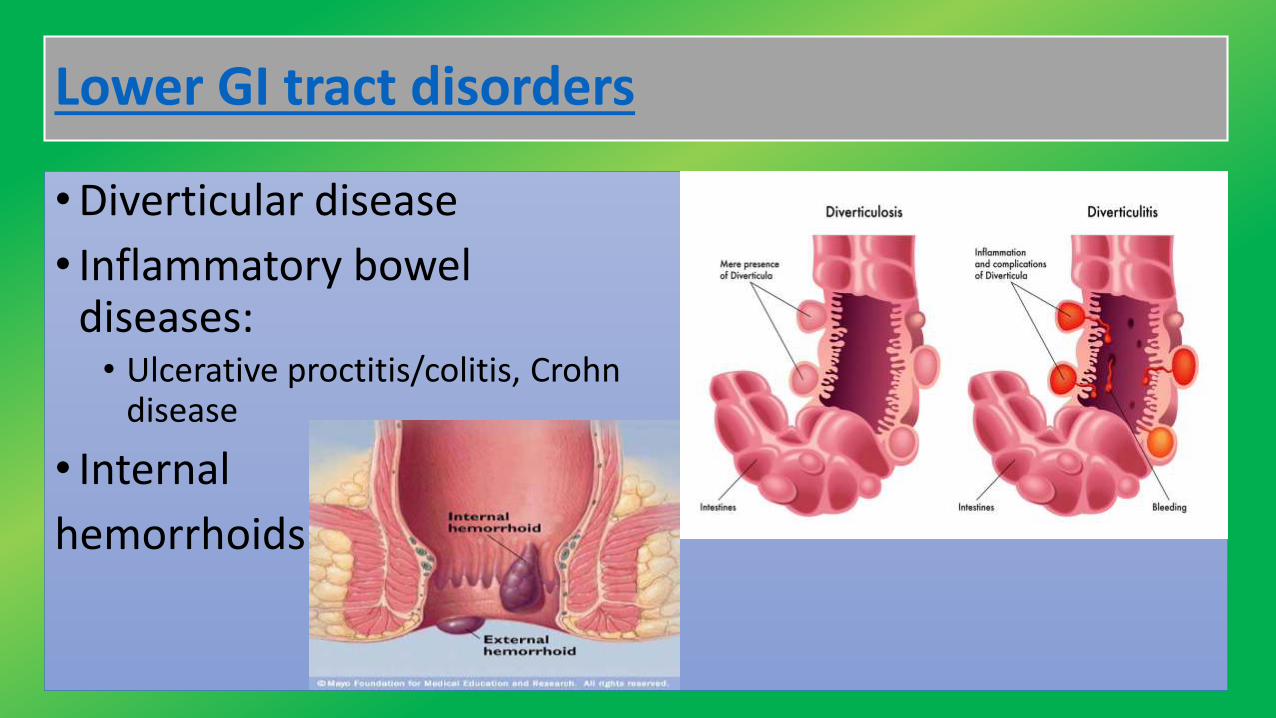
Lower GI tract disorders
•Diverticular disease
• Inflammatory bowel diseases:• Ulcerative proctitis/colitis, Crohn
disease
• Internal
hemorrhoids
Diagnostic History
• History of present illness should attempt to ascertain quantityand frequency of blood passage
• Quantity can be difficult to assess because even small amounts (5to 10 mL) of blood turn water in a toilet bowl an opaque red, andmodest amounts of vomited blood appear huge to an anxiouspatient
• Patients with hematemesis should be asked whether blood waspassed with initial vomiting or only after an initial (or several)non-bloody emesis.
• Patients with rectal bleeding : whether pure blood was
passed/was mixed with stool, pus, or mucus; or whether blood
simply coated the stool. Those with bloody diarrhea should be
asked about travel or other possible exposure to GI pathogens
• Past medical history : previous GI bleeding (diagnosed or
undiagnosed); known inflammatory bowel disease, bleeding
diatheses, and liver disease; and use of any drugs that increase
the likelihood of bleeding or chronic liver disease (eg, alcohol).

Medication history
•A thorough medication history should be obtained, withparticular attention paid to drugs that predispose topeptic ulcer formation, such as aspirin and othernonsteroidal anti-inflammatory drugs (NSAIDs)
•Promote bleeding, such as antiplatelet agents(eg:Clopidogrel) and anticoagulants
•May alter the clinical presentation, such as bismuth andiron, which can turn the stool black
Physical examination
•General examination focuses on vital signs and other
indicators of shock or hypovolemia (eg:Tachycardia,
tachypnea, pallor, diaphoresis, oliguria, confusion) and
anemia (eg:pallor, diaphoresis)
•Patients with lesser degrees of bleeding may simply have
mild tachycardia (heart rate > 100)
• Orthostatic changes in pulse (a change of > 10 beats/min) or BP
(a drop of ≥ 10 mm Hg) often develop after acute loss of ≥ 2
units of blood
• A digital rectal examination is necessary to search for stool
color, masses, and fissures.
• Anoscopy is done to diagnose hemorrhoids.
• Chemical testing of a stool specimen for occult blood completes
the examination if gross blood is not present
Red flags
Several findings suggest hypovolemia or hemorrhagic shock:
• Syncope
•Hypotension
•Pallor
•Diaphoresis
• Tachycardia
Interpretation of findings
• The history and physical examination suggest a diagnosis in about50% of patients, but findings are rarely diagnostic andconfirmatory testing is required.
• Epigastric abdominal discomfort relieved by food or antacids• peptic ulcer disease
• Weight loss and anorexia, with or without a change in stool• GI cancer
• History of cirrhosis or chronic hepatitis :• esophageal varices.
• Dysphagia suggests• esophageal cancer or stricture
• A history of bleeding(eg:purpura,ecchymosis, hematuria)• Bleeding diathesis (eg, hemophilia, hepatic failure)
• Bloody diarrhea, fever, and abdominal pain• Ischemic colitis, inflammatory bowel disease (eg:ulcerative colitis, Crohn disease) or an
infectious colitis(eg:Shigella,Salmonella, Campylobacter,amebiasis)
• Hematochezia• diverticulosis or angiodysplasia
• Fresh blood only on toilet paper or the surface of formed stools• Internal hemorrhoids or fissures, whereas blood mixed with the stool indicates a more
proximal source
• Occult blood in the stool• First sign of colon cancer or a polyp, particularly in patients > 45 yr.
•Vomiting and retching before the onset of bleeding• Mallory-Weiss tear of the esophagus
• Spider angiomas, hepatosplenomegaly, or ascites withchronic liver disease• possible esophageal varices.
•Arteriovenous malformations, especially of the mucousmembranes• Hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome)
•Cutaneous nail bed and GI telangiectasia may indicate• systemic sclerosis or mixed connective tissue disease
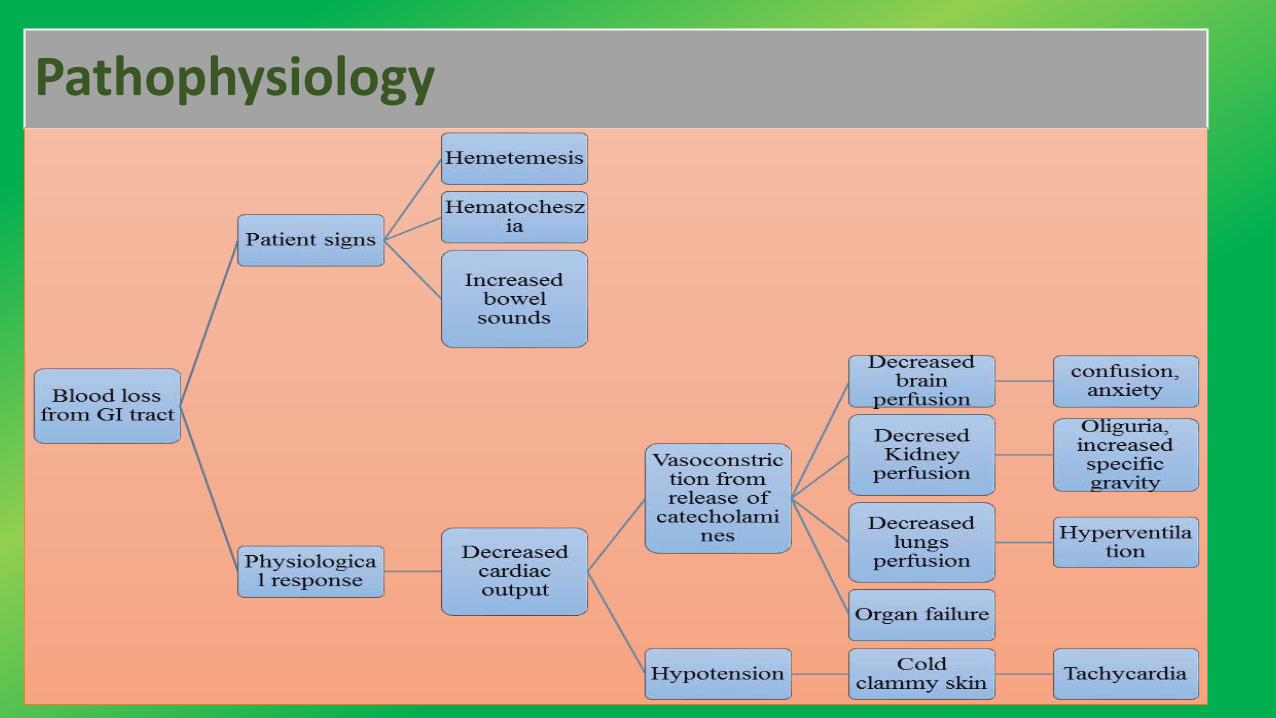
Pathophysiology
Diagnosis
• Abdominal X-ray, CT scan, MRI
• Angiography
• Bleeding scan (tagged red blood cell scan)
• Capsule endoscopy (camera pill that is swallowed to look at the small intestine)
• Colonoscopy
• CBC, clotting tests, platelet count, and other laboratory tests
• Enteroscopy
• Sigmoidoscopy
•CBC, coagulation profile
•NGT
•Upper endoscopy for suspected upper GI bleeding
•Colonoscopy for lower GI bleeding (unless clearly caused
by hemorrhoids)
•Upper endoscopy (examination of the esophagus,stomach, and duodenum) should be done for upper GIbleeding. Because endoscopy may be therapeutic as wellas diagnostic, it should be done rapidly for significantbleeding but may be deferred for 24 h if bleeding stops oris minimal.
•Angiography is useful in the diagnosis of upper GI bleedingand permits certain therapeutic maneuvers(eg:embolization, vasoconstrictor infusion).
• Flexible sigmoidoscopy and anoscopy may be all that is
required acutely for patients with symptoms typical of
hemorrhoidal bleeding.
•All other patients with hematochezia should have
colonoscopy, which can be done electively after routine
preparation unless there is significant ongoing bleeding.
Treatment
Airway
•A major cause of morbidity and mortality in patients withactive upper GI bleeding is aspiration of blood withsubsequent respiratory compromise.
• To prevent these problems, endotracheal intubationshould be considered in patients who have inadequate gagreflexes or are obtunded or unconscious—particularly ifthey will be undergoing upper endoscopy.
•Hemostasis : GI bleeding stops spontaneously in about80% of patients. The remaining patients require some typeof intervention. Early intervention to control bleeding isimportant to minimize mortality, particularly in elderlypatients
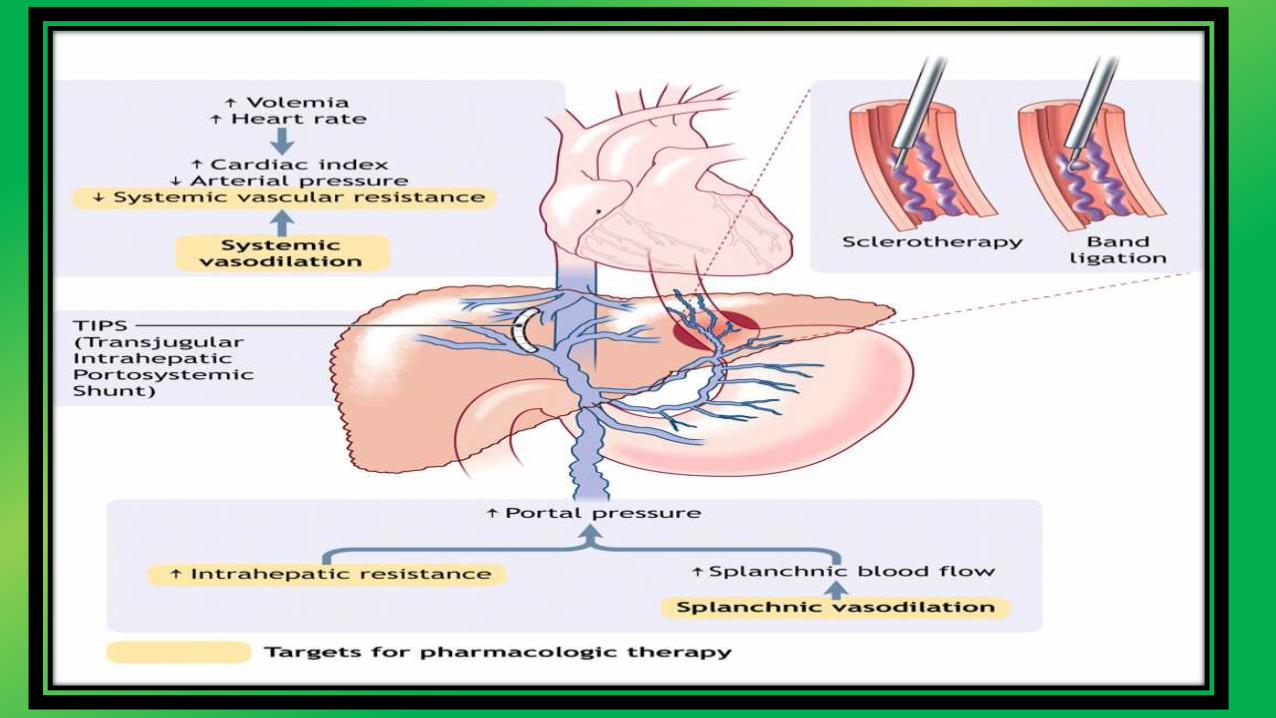
•Active variceal bleeding can be treated with endoscopicbanding, injection sclerotherapy, or a transjugularintrahepatic portosystemic shunting (TIPS) procedure
Treatment
Severe, ongoing lower GI bleeding caused by diverticula or
angiomas can sometimes be controlled colonoscopically by
electrocautery, coagulation with a heater probe, or injection with
dilute epinephrine.
Polyps can be removed by snare or cautery. If these methods are
ineffective or unfeasible, angiography with embolization
or vasopressin infusion may be successful
Treatment : Geriatrics care
• In the elderly, hemorrhoids and colorectal cancer are themost common causes of minor bleeding. Peptic ulcer,diverticular disease, and angiodysplasia are the mostcommon causes of major bleeding. Variceal bleeding isless common than in younger patients.
•Massive GI bleeding is tolerated poorly by elderly patients.Diagnosis must be made quickly, and treatment must bestarted sooner than in younger patients, who can bettertolerate repeated episodes of bleeding
GENERAL MANAGEMENT
• Triage — All patients with hemodynamic instability or
active bleeding should be admitted to an intensive care
unit for resuscitation and close observation with
monitoring
•Other patients can be admitted to a regular medical ward

General support
• Supplemental oxygen by nasal cannula
•Nothing by mouth
•PIVC(16G/18G) or a central venous line should be inserted
•Placement of a pulmonary artery catheter
• Elective endotracheal intubation in patients with ongoinghematemesis or altered respiratory or mental status mayfacilitate endoscopy and decrease the risk of aspiration.
Treatment- Fluid resuscitation
• Adequate resuscitation and stabilization is essential
• Patients with active bleeding should receive intravenous fluids(eg, 500 mL of NS or RL over 30 minutes) while being cross-matched for blood transfusion. Patients at risk of fluid overloadmay require intensive monitoring with a pulmonary arterycatheter.
• If the blood pressure fails to respond to initial resuscitationefforts, the rate of fluid administration should be increased.
Treatment: Blood transfusion
• The decision to initiate blood transfusions must beindividualized
• The approach is to initiate blood transfusions if thehemoglobin is <7 g/dL (70 g/L) for most patients (includingthose with stable coronary artery disease), with a goal ofmaintaining the hemoglobin at a level ≥7 g/dL (70 g/L)
•We do not have an age cutoff for determining whichpatients should have a goal hemoglobin of ≥9 g/dL (90g/L), and instead base the decision on the patient'scomorbid conditions
•Avoid over transfusion in patients with suspected variceal
bleeding, as it can precipitate worsening of the bleeding .
Transfusing patients with suspected variceal bleeding to a
hemoglobin >10 g/dL (100 g/L) should be avoided
•A randomized trial suggests that using a lower hemoglobin
threshold for initiating transfusion improves outcomes.
Treatment: Medications
Acid suppression —Proton pump inhibitor (PPI)
• The patients with acute upper GI bleeding shall be startedempirically on an intravenous (IV) PPI (eg, omeprazole 40mg IV twice daily).
• It can be started at presentation and continued untilconfirmation of the cause of bleeding
Prokinetics — Both erythromycin and metoclopramide
• To improve gastric visualization at the time of endoscopyby clearing the stomach of blood, clots, and food residue.
• Erythromycin, a macrolide antibiotic, facilitates themotility of the gastric antrum and duodenum by acting asa motilin receptor agonist.
•3 mg/kg IV over 20 to 30 minutes, 30 to 90 minutes priorto endoscopy
Treatment: Medications
• Somatostatin and its analogs — Somatostatin, or itsanalog octreotide, is used in the treatment of varicealbleeding and may also reduce the risk of bleeding due tonon-variceal causes.
• In patients with suspected variceal bleeding, octreotide isgiven as an intravenous bolus of 20 to 50 mcg, followed bya continuous infusion at a rate of 25 to 50 mcg per hour
Treatment: Medications
Antibiotics for patients with cirrhosis : Bacterial infections
are present in up to 20 % of patients with cirrhosis who are
hospitalized with gastrointestinal bleeding; up to an
additional 50 % develop an infection while hospitalized.
Such patients have increased mortality.
Treatment: Medications
Tranexamic acid : an anti-fibrinolytic agent that has been
studied in patients with upper GI bleeding.
•A meta-analysis that included eight randomized trials of
tranexamic acid in patients with upper GI bleeding found a
benefit with regard to mortality but not with regard to
bleeding, surgery, or transfusion requirements.
Treatment: Medications
Surgical Interventions
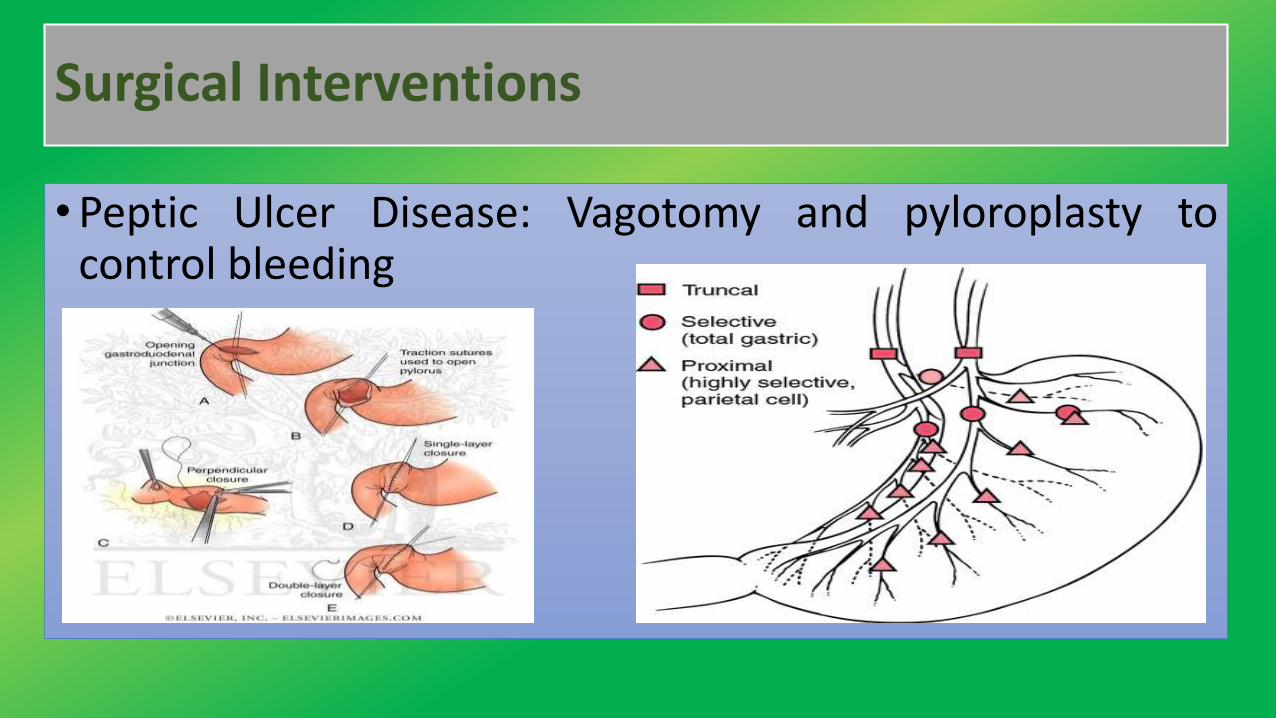
•Peptic Ulcer Disease: Vagotomy and pyloroplasty tocontrol bleeding
Surgical Interventions :
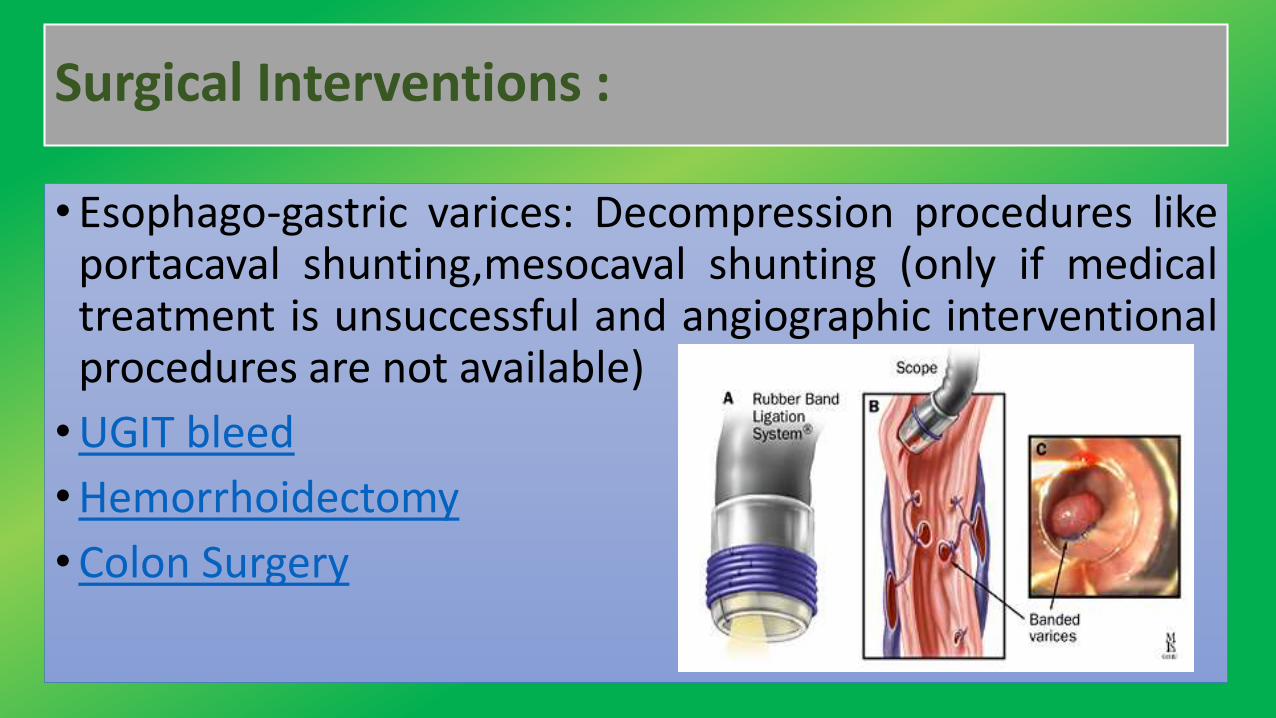
• Esophago-gastric varices: Decompression procedures likeportacaval shunting,mesocaval shunting (only if medicaltreatment is unsuccessful and angiographic interventionalprocedures are not available)
•UGIT bleed
•Hemorrhoidectomy
•Colon Surgery
Nursing Management
All critically ill patients should be considered at risk forstress ulcers and therefore GI hemorrhage. Maintaininggastric fluid pH 3.5-4.5 is a goal of prophylactic therapy.
The major nursing interventions are
•Administering volume replacement
•Controlling the bleeding
•Maintaining surveillance for complications
• Educating the family and patient
RISK STRATIFICATION
Endoscopic, clinical, and laboratory features may be useful for riskstratification of patients who present with acute upper GI bleeding.
Factors associated with re-bleeding identified in a meta-analysisincluded:
• Hemodynamic instability (systolic blood pressure less than 100mmHg, heart rate greater than 100 beats per minute)
• Hemoglobin less than 10 g/L
• Active bleeding at the time of endoscopy
• Large ulcer size (greater than 1 to 3 cm in various studies)
• Ulcer location
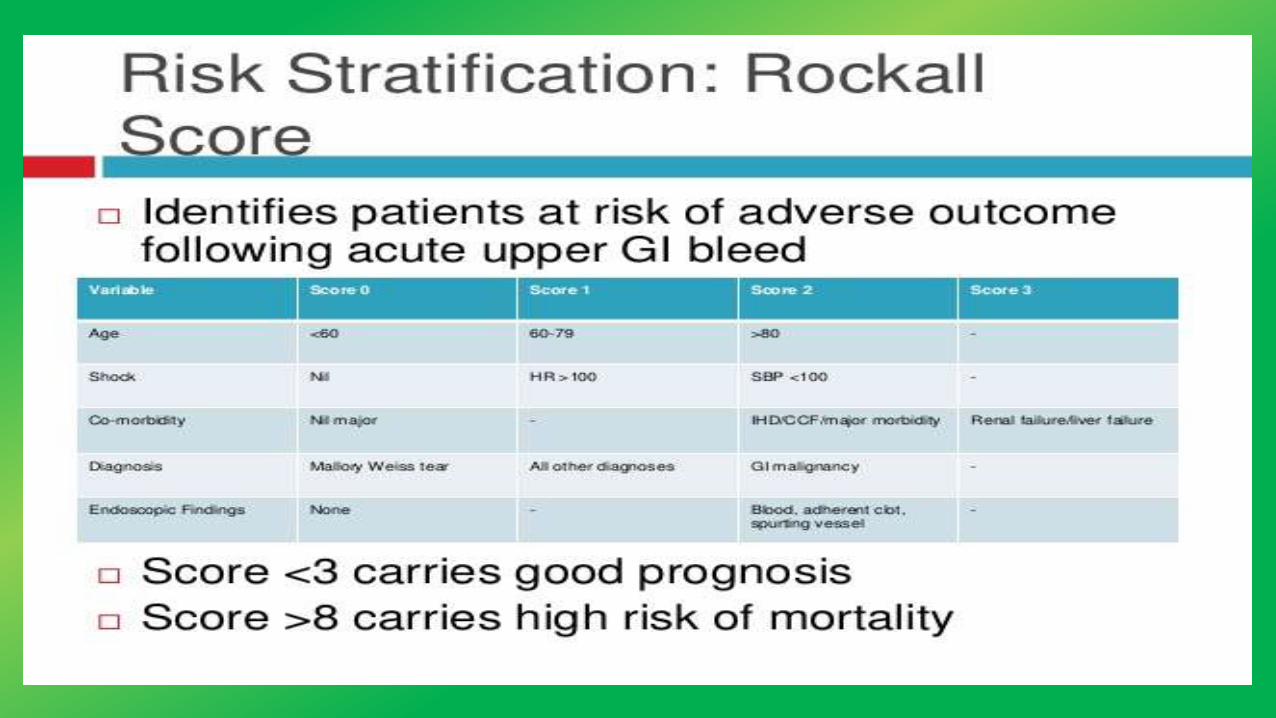
Risk scores
Two commonly cited scoring systems are the Rockall scoreand the Blatchford score:
The Rockall score is based upon age, the presence of shock,comorbidity, diagnosis, and endoscopic stigmata of recenthemorrhage
Glasgow Blatchford score
The score is based upon the BUN, hemoglobin, systolicblood pressure, pulse, and the presence of melena,syncope, hepatic disease, and/or cardiac failure
The score ranges from zero to 23 and the risk of requiringendoscopic intervention increases with increasing score.
One meta-analysis found that a Blatchford score of zero wasassociated with a low likelihood of the need for urgentendoscopic intervention
Nursing Diagnoses
•Deficient fluid volume related absolute loss through bleeding
•Decreased cardiac output due to alterations in preload
• Imbalanced nutritional status less than body requirement related to lack of exogenous nutrients
•Risk for infection related to bleeding
•Compromised family coping related to critically ill family member
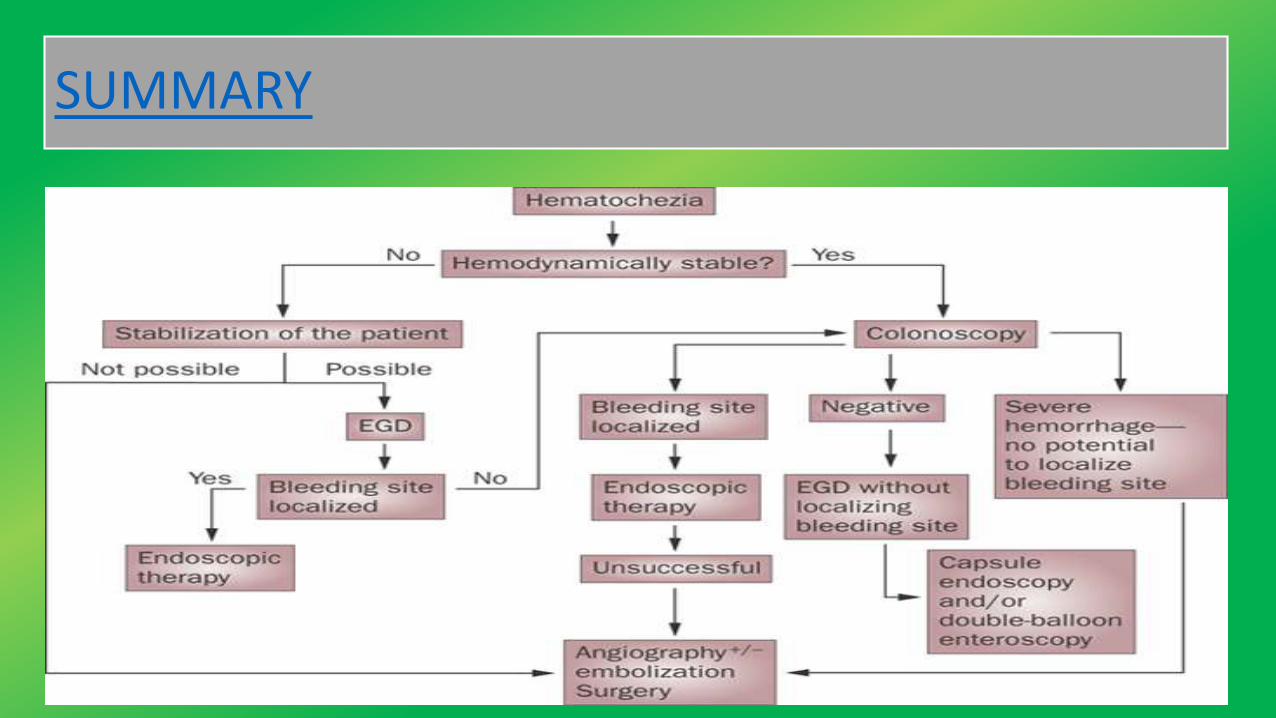
SUMMARY
Journal
• A Meta-analysis of Randomized Controlled Trials was done onadministration of Erythromycin before Endoscopy in UpperGastrointestinal Bleeding. Six studies (N = 558) met the inclusioncriteria. Erythromycin infusion before endoscopy in UGIBdemonstrated a statistically significant improvement invisualization of the gastric mucosa compared with noerythromycin. In addition, erythromycin infusion beforeendoscopy resulted in a statistically significant decrease in theneed for a second endoscopy, and the duration of hospitalstay.(Saudi journal of gastroenterology,2013)
REFERENCES
• Black, J.M. & Hawks, J.H. (2009). Medical Surgical Nursing: Clinical Management for Positive Outcomes. 8th ed. : Elsevier
• Ignatavicius, D.D. and Workman, M.L. (2003). Medical Surgical Nursing: Patient Centered Collaborative Care. 7th ed. : Elsevier
• Linda D. Urden.Kathleen M. Stacy.Mary E. Lough. Critical Care Nursing: Diagnosis and Management, Thelans Critical Care Nursing Diagnosis. 7th Edition
• Jarvis,C. (2008). Physical Examination and Health Assessment. 5th ed. : Saunder, an imprint of Elsevier Inc.
• Lewis, S.L et. al., (2009). Medical Surgical Nursing: Assessment and Management of Clinical Problems. 7th ed. : Mosby Elsevier
• Barkun A, Bardou M, Marshall JK.(2013). Nonvariceal Upper GI Bleeding Consensus Conference Group. Consensus recommendations for managing patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med
• Laine L, Jensen DM.(2012) Management of patients with ulcer bleeding. Ameriacan J Gastroenterology; 107:345.
• Srygley FD, Gerardo CJ, Tran T, Fisher DA. Does this patient have a severe upper gastrointestinal bleed? JAMA 2012; 307:1072.
• Cappell MS, Friedel D. Initial management of acute upper gastrointestinal bleeding: from initial evaluation up to gastrointestinal endoscopy. Med Clin North Am 2008; 92:491.
• https://www.nlm.nih.gov/medlineplus/ency/article/003133.htm
• http://www.nature.com/ajg/journal/v98/n7/abs/ajg2003350a.html
• http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3793471/
SUMMARY AND RECOMMENDATIONS
●Obscure bleeding is defined as bleeding from the gastrointestinal tract that persists or recurs without an obvious etiology after upper endoscopy and colonoscopy.Obscure bleeding may be occult or overt. (See 'Introduction' above.)
●The approach to the evaluation of patients with obscure gastrointestinal bleeding depends on whether the bleeding is occult or overt, if the patient has signs ofsevere bleeding, and if the patient is healthy enough to undergo an aggressive endoscopic evaluation (algorithm 1). The evaluation typically starts with wirelessvideo capsule endoscopy, though angiography or even intraoperative enteroscopy may be indicated for patients with signs of severe bleeding (eg, hypotension,tachycardia, or orthostatic hypotension). (See 'General diagnostic approach' above.)
●In patients without an obvious source of bleeding on capsule endoscopy, the decision to pursue further testing should consider the rate of blood loss and thepresence of comorbidities. In patients with significant comorbid illnesses with slow rates of blood loss, it may be reasonable to stop the evaluation and treat withiron repletion and/or transfusions as needed. Aggressive evaluation is generally warranted in patients younger than 50 years old. The next step, if additional testing isbeing pursued, is typically deep small bowel enteroscopy, though push enteroscopy is an alternative if deep small bowel enteroscopy is not available. (See'Enteroscopy' above.)
●Among patients with occult bleeding, the first test obtained is usually wireless video capsule endoscopy. If the capsule endoscopy is negative, patients are managedexpectantly, with no additional workup if the bleeding does not continue or recur. If the bleeding continues or recurs, the next step is to repeat an upper endoscopy,colonoscopy, and/or capsule endoscopy. The choice of test will depend on the quality of the prior examinations and the suspected site of bleeding (upper, mid, orlower gastrointestinal tract). A side-viewing endoscope may be of value in examining the medial aspect of the second part of the duodenum and periampullary area.(See 'Repeat upper endoscopy and colonoscopy' above.)
If no source is identified, the next step is typically deep small bowel enteroscopy, though push enteroscopy is an alternative if deep small bowel enteroscopy is notavailable. If the bleeding continues, additional testing may include a Meckel's scan or laparoscopy with intraoperative enteroscopy. We typically perform a Meckel'sscan for patients who are under the age of 50 years old (though bleeding from a Meckel's diverticulum may occur at any age). For patients with significant ongoingbleeding (eg, bleeding that is requiring blood transfusions), we will proceed with computed tomographic enterography, and if needed, intraoperative enteroscopy,provided the patient is a good surgical candidate. (See 'Enteroscopy' above and 'Radiographic imaging' above.)
●For patients with overt bleeding, the first question is whether the patient has severe bleeding (bleeding associated with signs such as of hypotension, tachycardia,or orthostatic hypotension).
If severe bleeding is present, the first step in the evaluation is angiography. If angiography is negative, we proceed with deep small bowel enteroscopy or, if there ismassive, ongoing bleeding, intraoperative enteroscopy. (See 'Angiography' above and 'Deep small bowel enteroscopy' above and 'Intraoperative enteroscopy' above.)
For patients who do not have severe bleeding, the first step is capsule endoscopy. If that is negative, repeating an upper endoscopy, colonoscopy, and/or capsuleendoscopy is typically the next step (again based on the suspected site of bleeding). A side-viewing endoscope may be of value in examining the medial aspect of thesecond part of the duodenum and periampullary area. (See 'Wireless video capsule endoscopy' above.)
Deep small bowel enteroscopy is the next step if a source is still not identified. Push enteroscopy is an alternative if deep small bowel enteroscopy is not available orfor patients at risk for an aortoenteric fistula (eg, patients with a prior aortic aneurysm repair). As with occult bleeding, further diagnostic testing for ongoingbleeding may include a Meckel's scan or laparoscopy with intraoperative enteroscopy. (See 'Enteroscopy' above and 'Radiographic imaging' above.)
Top Related