




Languages
Pages
Legal


Acute Acute cholecystitischolecystitis
Sergey Usov M.D.Sergey Usov M.D.

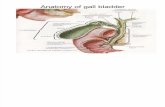
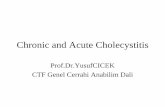
GallbladderGallbladder anatomyanatomy

GallbladderGallbladderanatomyanatomy

Acute cholecystitisAcute cholecystitis
Definition: Definition:
Acute cholecystitis is an Acute cholecystitis is an inflammation of a gall-inflammation of a gall-bladder. bladder.

Etiology and pathogenesis.Etiology and pathogenesis.
• In etiology of cholecystitis major In etiology of cholecystitis major factors are the following: cholelithiasis, factors are the following: cholelithiasis, infection. Problems with bile passage infection. Problems with bile passage through the cystic duct from through the cystic duct from gallbladder to the common bile duct gallbladder to the common bile duct due to stenosis or obstruction of cystic due to stenosis or obstruction of cystic duct with inflammation process around duct with inflammation process around a cervix of the gallbladder there are. a cervix of the gallbladder there are.

Causes of cholecystitisCauses of cholecystitis
All reasons of acute cholecystitis All reasons of acute cholecystitis causes are divided in two groups: causes are divided in two groups:
• cholecystitis with formation of cholecystitis with formation of calculi (gall stones) calculi (gall stones) - 80%.- 80%.
• Non calculi cholecystitis – Non calculi cholecystitis – 20%.20%.

What is that? It might be What is that? It might be pineapplepineapple??

What is that? It might be precious What is that? It might be precious stone?stone?

What is that? It might be What is that? It might be jewel?jewel?

No! This is a gall-stone.No! This is a gall-stone.

No! This is a gall-stoneNo! This is a gall-stone

No! This is a gall-stone No! This is a gall-stone againagainNo! This is a gall-stone No! This is a gall-stone againagainNo! This is a gall-stone No! This is a gall-stone againagain

Causes of cholecystitisCauses of cholecystitis
Non calculi cholecystitis is Non calculi cholecystitis is conditioned: conditioned:
•by gram-positive and gram-by gram-positive and gram-negative infections negative infections - 10%. - 10%.
•or blood supply disturbance of or blood supply disturbance of the wall gallbladder – 5%.the wall gallbladder – 5%.

Other causes of cholecystitisOther causes of cholecystitis
microbes: Cmicrobes: Colibacillus, Proteus, olibacillus, Proteus, Staphylococcus, Enterococcus Staphylococcus, Enterococcus and mixed form bacteria. and mixed form bacteria.
It is particular form of acute It is particular form of acute cholecystitis (5%) due to: cholecystitis (5%) due to:
acute pancreatitis acute pancreatitis (pancreatogenic) (pancreatogenic)
or parasitogenic diseases. or parasitogenic diseases.

PathomorphologyPathomorphology of acute of acute cholecystitischolecystitis
The wall of gall-bladder is The wall of gall-bladder is thickened, edematous, and thickened, edematous, and hyperemic with stratification of hyperemic with stratification of fibrin and the gall bladder fills fibrin and the gall bladder fills with puswith pus

PathomorphologyPathomorphology of of cholecystitischolecystitis
The catarrhal acute cholecystitis The catarrhal acute cholecystitis develops to phlegmonous and develops to phlegmonous and suppuration inflammation.suppuration inflammation.
Progress of inflammation process Progress of inflammation process can lead to gangrene of the gall can lead to gangrene of the gall bladder. bladder.

Gangrenous cholecystitisGangrenous cholecystitis

Necrosis of the gall bladder. Necrosis of the gall bladder.

Classification:Classification:
• A. acute calculi cholecystitis (with A. acute calculi cholecystitis (with presence gall stones)presence gall stones)
• B. acute non - calculi cholecystitis B. acute non - calculi cholecystitis (without gall stones)(without gall stones)
• 1. Catarrhal1. Catarrhal
• 2. Phlegmonous2. Phlegmonous
• 3. Gangrenous3. Gangrenous
• 4. Perforated4. Perforated

Complication:Complication:
• peritonitis (local, widespread, general)peritonitis (local, widespread, general)
• cholangitis (inflammation process into cholangitis (inflammation process into the bile duct)the bile duct)
• empyema of gall bladderempyema of gall bladder
• abscess around the gall bladderabscess around the gall bladder
• hydrops of gall bladderhydrops of gall bladder
• mechanical jaundice mechanical jaundice
• hepatitis or hepato-renal insufficiencyhepatitis or hepato-renal insufficiency

Clinical management:Clinical management:
Acute cholecystitis usually Acute cholecystitis usually begins after violation of a begins after violation of a diet: intake of spice or fried diet: intake of spice or fried food, plenty fatty eating. food, plenty fatty eating.

Pain syndromePain syndrome. .
• Main symptom of acute Main symptom of acute cholecystitis is severe pain in right cholecystitis is severe pain in right hypochondrium and epigastric area hypochondrium and epigastric area with radiation to right half of the with radiation to right half of the chest and right shoulder. When a chest and right shoulder. When a hypertension in a gall bladder and hypertension in a gall bladder and bile ducts progresses the pain bile ducts progresses the pain syndrome is strongly expressed and syndrome is strongly expressed and becomes attack-like in character, becomes attack-like in character, but this clinical phenomenon is but this clinical phenomenon is named as biliary colic. named as biliary colic.

Dyspepsia syndromeDyspepsia syndrome ::
• Frequent symptoms which Frequent symptoms which disturb a patient are nausea disturb a patient are nausea and repeated vomiting with and repeated vomiting with bile. Later feeling of fullness bile. Later feeling of fullness of abdomen, delay of of abdomen, delay of emptying bowel and gases emptying bowel and gases are often followed. are often followed.

Objective examinationObjective examination
•A doctor can observe slight A doctor can observe slight icterus skin or sclera during icterus skin or sclera during examination in many patients. examination in many patients. Tongue is whites-grey in Tongue is whites-grey in colour. Patients complain of a colour. Patients complain of a dryness of mouth. In difficult dryness of mouth. In difficult cases the tongue is usually cases the tongue is usually dry, assessed white dry, assessed white stratification with yellow spot. stratification with yellow spot.

Objective examinationObjective examination
• Increase of body’s temperature Increase of body’s temperature (to 37,5 C) in brief period is (to 37,5 C) in brief period is insignificant in catarrhal insignificant in catarrhal cholecystitis and with destructive cholecystitis and with destructive forms the temperature could be forms the temperature could be higher (38C). The fever in the higher (38C). The fever in the range of 37,7-38,8 is marked range of 37,7-38,8 is marked inflammation and toxemia. inflammation and toxemia. Tachycardia testifies the degree Tachycardia testifies the degree of intoxication.of intoxication.

Objective examinationObjective examination
• The upper part of abdomen is strongly The upper part of abdomen is strongly tense and often palpable mass tense and often palpable mass develops in the hypochondrium region develops in the hypochondrium region or projection of the gall bladder. By or projection of the gall bladder. By superficial and deep palpation right superficial and deep palpation right hypochondrium area a tenderness of hypochondrium area a tenderness of the abdominal wall, increased size of the abdominal wall, increased size of gall bladder are exposed. An inflamed gall bladder are exposed. An inflamed gall bladder wrapped in inflammatory gall bladder wrapped in inflammatory adhesions with adjacent organs, adhesions with adjacent organs, especially the omentum. especially the omentum.

The following symptoms are The following symptoms are diagnosed in acute diagnosed in acute
cholecystitis:cholecystitis:• Murphy’s sign is a delay of breathing Murphy’s sign is a delay of breathing
during palpation of gall bladder on during palpation of gall bladder on inspiration.inspiration.
• Kehr’s sign is increase of pain Kehr’s sign is increase of pain with pressure on the area of gall with pressure on the area of gall bladder, especially on deep bladder, especially on deep palpation.palpation.
• Ortner’s sign is tenderness on Ortner’s sign is tenderness on light percussion at right costal light percussion at right costal margin by edge of the hand. margin by edge of the hand.

Diagnostic program:Diagnostic program:
• Laboratory analysisLaboratory analysis. Leukocytes from 10.0/L . Leukocytes from 10.0/L and more, shift of leukocyte formula to the and more, shift of leukocyte formula to the left, lymphopenia and increased ESR.left, lymphopenia and increased ESR.
• SonographicSonographic examination of gall bladder can examination of gall bladder can reveal the increase in its sizes, bulge of reveal the increase in its sizes, bulge of walls, development of perivesical abscesses, walls, development of perivesical abscesses, presence or absence of bile sludge and presence or absence of bile sludge and stones. stones.
• X-rayX-ray examination with observe of abdominal examination with observe of abdominal cavity organs can identify free gas in cavity organs can identify free gas in abdominal cavity and X-ray photography-abdominal cavity and X-ray photography-positive of the gall stones. positive of the gall stones.

CholecystographyCholecystography

Cholecystography with Cholecystography with contrast agentcontrast agent

CT investigationCT investigation

UltrasonographyUltrasonography

UltrasonographyUltrasonography

UltrasonographyUltrasonography

UltrasonographyUltrasonography

CholangiographyCholangiography

Differential diagnosis Differential diagnosis
• TThesehese should be suspected whenever should be suspected whenever the acute pain the acute pain at at right upper right upper quadrantquadrant of abdomen is appeared of abdomen is appeared. . – Perforated peptic ulcer Perforated peptic ulcer
- - Acute amoebic liver Acute amoebic liver abscessabscess – Acute pancreatitis Acute pancreatitis – Acute intestinal obstruction Acute intestinal obstruction – Renal colic Renal colic – Acute retrocolic appendicitis Acute retrocolic appendicitis – Myocardial infarctionMyocardial infarction– Basal pneumoniaBasal pneumonia

TreatmentTreatment
• For most patients the definitive For most patients the definitive treatment is surgical removal of the treatment is surgical removal of the gallbladder. Supportive measures are gallbladder. Supportive measures are basbased in the meantime to prepare the ed in the meantime to prepare the patient for surgery. Thepatient for surgery. The ininfusionfusion of of fluid fluid and and antibioticsantibiotics should be given should be given. . Antibiotic regimens usually consist of a Antibiotic regimens usually consist of a broad spectrum antibiotic such as a broad spectrum antibiotic such as a cephalosporin (e.g.cephalosporin (e.g.ceftriaxoneceftriaxone) and an ) and an antibacterial with good coverage antibacterial with good coverage against against anaerobicanaerobic bacteriabacteria, such as , such as metronidazolemetronidazole. .

The surgeryThe surgery
• Gallbladder removal, Gallbladder removal, cholecystectomycholecystectomy, can be , can be accomplished via open surgery or a accomplished via open surgery or a laparoscopiclaparoscopic procedure. Laparoscopic procedure. Laparoscopic procedures haprocedures hass less less morbiditymorbidity and a and a shorter recovery shorter recovery periodperiod. Open . Open procedures are usually done if procedures are usually done if complications have developed or the complications have developed or the patient has had prior surgery to the patient has had prior surgery to the area, making laparoscopic surgery area, making laparoscopic surgery technically difficult. Open procedure technically difficult. Open procedure may also be done if the surgeon may also be done if the surgeon could could meet with meet with a a difficult clinical casesdifficult clinical cases. .

Consequently, LConsequently, Laparoscopic aparoscopic cholecystectomy is the cholecystectomy is the Gold standardGold standard for the gall for the gall bladder bladder planed planed surgery. surgery.
• Film 5 min.Film 5 min.

UrgentUrgent operations need the operations need the open surgical approach and open surgical approach and handmade a gall bladder handmade a gall bladder surgery. surgery.
• Film 10 min.Film 10 min.

CCholecystostomyholecystostomy
• In cases of severe inflammation, In cases of severe inflammation, shock, or if the patient has higher shock, or if the patient has higher risk for general anesthesia risk for general anesthesia (required for (required for cholecystectomycholecystectomy), ), the managing physician the managing physician shouldshould ttake ake a a percutaneouspercutaneous drainage drainage catheter into the gallbladder catheter into the gallbladder ('percutaneous cholecystostomy ('percutaneous cholecystostomy tube') and treat the patient with tube') and treat the patient with antibiotics until the acute antibiotics until the acute inflammation resolves. inflammation resolves.

CCholecystostomyholecystostomy

The surgeryThe surgery
•Open procedures are usually Open procedures are usually done if complications have done if complications have developed or the patient has developed or the patient has had prior surgery to the area, had prior surgery to the area, making laparoscopic surgery making laparoscopic surgery technically difficult technically difficult
• Film 5 min.Film 5 min.

Complications Complications aaffter ter cholecystectomy cholecystectomy
• bile leak ("biloma") bile leak ("biloma") • bile duct injury Open and laparoscopic surgeries bile duct injury Open and laparoscopic surgeries
have essentially equal rate of injuries, but the recent have essentially equal rate of injuries, but the recent trend is towards fewer injuries with laparoscopy. It trend is towards fewer injuries with laparoscopy. It may be that the open cases often result because the may be that the open cases often result because the gallbladder is too difficult or risky to remove with gallbladder is too difficult or risky to remove with laparoscopy) laparoscopy)
• Intraabdominal Intraabdominal abscess abscess • wound infection wound infection • bleeding (liver surface and cystic artery are most bleeding (liver surface and cystic artery are most
common sites) common sites) • hernia hernia • deepdeep veinvein thrombosisthrombosis//pulmonarypulmonary embolismembolism
(unusual- risk can be decreased through use of (unusual- risk can be decreased through use of sequential compression devices on legs during sequential compression devices on legs during surgery) surgery)

Thank you!Thank you!
Sergey Usov M.D.Sergey Usov M.D.
Top Related