






Languages
Pages
Legal

For queries on the status of this document contact [email protected] or telephone 029 2031 5512
Status Note amended March 2013
A guide to the decontamination of reusable surgical instruments
2003
STATUS IN WALES
APPLIES
A guide to the decontamination of
reusable surgical instruments

© Crown copyright 2003
A guide to the decontamination of
reusable surgical instruments
1.0 INTRODUCTION page 7
AimScopeAudienceStructureDecontamination life-cycleBasic requirements for decontaminationTracking and traceability of surgical
instrumentsInfection control policiesDecontamination training
2.0 TRANSPORTATION OFCONTAMINATED SURGICALINSTRUMENTS ANDASSOCIATED EQUIPMENT
page 11
3.0 ACQUISITION page 13
PurchasingLoan of surgical instruments andequipment
4.0 CLEANING page 15
First use of surgical instrumentsPre-treatment of surgical instrumentsDisassembly of instrumentsAutomated cleaningProcedure for manual cleaning
5.0 DISINFECTION page 21
6.0 INSPECTION AND FUNCTIONTESTING
page 23
Inspection of surgical instrumentsFunction testingRepairs
7.0 PACKAGING page 25
General requirementsLabelling of sterile surgical instruments
8.0 STERILIZATION page 27
Porous-load sterilizersBowl and instrument sterilizersBenchtop sterilizers
9.0 TRANSPORTATION OFDECONTAMINATED SURGICALINSTRUMENTS ANDASSOCIATED EQUIPMENT
page 33
10.0 STORAGE OF STERILEPRODUCTS page 35
11.0 USE OF SURGICALINSTRUMENTS ANDASSOCIATED EQUIPMENT
page 37
5
Contents
APPENDIX 1 – Processing of flexibleendoscopes
page 39APPENDIX 2 – References page 41APPENDIX 3 – Glossary page 45
Acknowledgements page 48
6
AIM
The aim of this guide is to provideinformation on the decontamination ofsurgical instruments. It can be applied toany healthcare setting where reusablesurgical instruments are reprocessed.
SCOPE
This guide covers the broader issuesrelating to the reprocessing of re-usablesurgical instruments (for example trays),and is intended for people working inmulti-disciplinary healthcare fields whoare involved in any aspect of themanagement of surgical instruments andequipment. This may involve the actualcleaning and sterilization of surgicalinstruments and equipment, or theirtransportation, storage and use.
AUDIENCE
It is written for a wide audience, andwhilst reflecting the basic principles ofdecontamination, it should not be usedas a replacement for legislativedocuments or detailed guidanceissued by the Department of Healthand other recognised bodies.
Since the National DecontaminationInitiative began in 1999, NHS Estateshave issued a number of CD-ROMs tothe NHS, which have containeddecontamination guidance documentsrelating to decontamination standardsand their application. The latest edition
was issued in July 2003. References toguidance contained on the CD-ROM aregiven throughout this guide to allow formore detailed information to be obtainedby the reader as required. A fulldescription of these references is listed inAppendix 2. These documents can alsobe accessed through the NHS Estateswebsite.
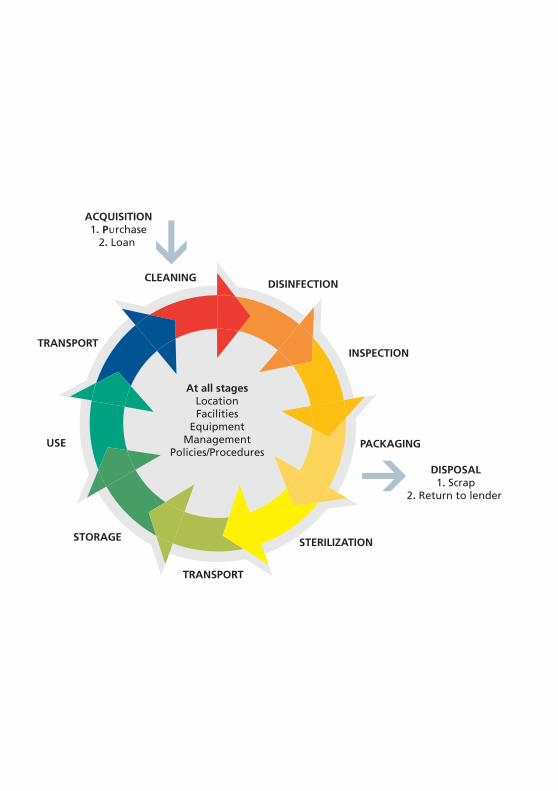
STRUCTURE
The guide is divided into specific sectionsfor ease of reference following the orderof the “decontamination life-cycle” shownin Figure 1. This allows healthcareworkers involved in particular areas ofdecontamination to focus directly onthose topics that are of interest to them.
DECONTAMINATION LIFE CYCLE
The decontamination life cycle modelhighlights the extent to whichdecontamination affects the whole of anorganisation and not just those areasprocessing equipment.
Traditionally, decontamination has beenthe responsibility of the departmentalheads of specialist units, for examplesterile services, endoscopy units, theatresuites etc. Management arrangementswithin organisations often divided thesefunctions and made it difficult for a totallyco-ordinated approach to the applicationof decontamination standards andpractices to be achieved. However,regardless of the location, the same
7
1.0 Introduction
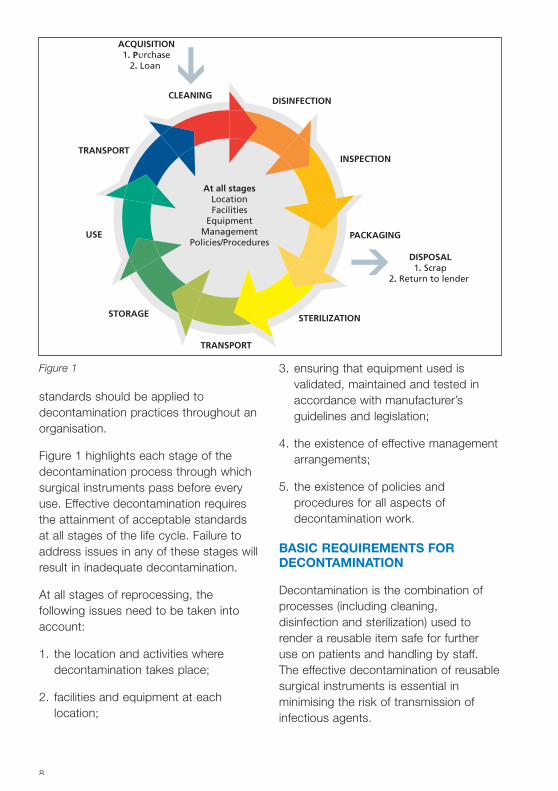
standards should be applied todecontamination practices throughout anorganisation.
Figure 1 highlights each stage of thedecontamination process through whichsurgical instruments pass before everyuse. Effective decontamination requiresthe attainment of acceptable standardsat all stages of the life cycle. Failure toaddress issues in any of these stages willresult in inadequate decontamination.
At all stages of reprocessing, thefollowing issues need to be taken intoaccount:
1. the location and activities wheredecontamination takes place;
2. facilities and equipment at eachlocation;
3. ensuring that equipment used isvalidated, maintained and tested inaccordance with manufacturer’sguidelines and legislation;
4. the existence of effective managementarrangements;
5. the existence of policies andprocedures for all aspects ofdecontamination work.
BASIC REQUIREMENTS FORDECONTAMINATION
Decontamination is the combination ofprocesses (including cleaning,disinfection and sterilization) used torender a reusable item safe for furtheruse on patients and handling by staff.The effective decontamination of reusablesurgical instruments is essential inminimising the risk of transmission ofinfectious agents.
8
Figure 1
In maintaining and developingorganisation-wide decontaminationstandards and practices, the followingshould be included:
• an effective management controlsystem must be in place to cover allaspects of the decontamination life-cycle;
• every organisation should have anominated lead with responsibility fordecontamination, either at directorlevel or someone who has linemanagement responsibility to a seniorresponsible person at that level;
• documented robust andcomprehensive policies andprocedures to ensure thatdecontamination processes areundertaken in a controlled manner toprotect the health and safety ofpatients and staff;
• a procurement policy which ensuresthat all purchased instruments arecompatible with decontaminationprocesses available within theorganisation;
• manual cleaning of devices to berestricted to those items deemedincompatible with automatedprocesses;
• reprocessing of surgical instruments tobe undertaken in dedicated facilitiesand outside the clinical/patientenvironment, preferably in centralfacilities;
• equipment used to decontaminatesurgical instruments and associatedequipment must be fit for purpose,validated and tested in accordancewith current recommendations;
• organisations should have systems inplace to trace instrument sets andendoscopes through decontaminationprocesses and to the patient (seebelow; see also HSC 2000/032 andHSC 1999/178);
• a documented training scheme mustbe in operation with individual trainingrecords for all personnel, includingmanagement involved indecontamination activities.
TRACKING AND TRACEABILITY OFSURGICAL INSTRUMENTS
It is important to be able to traceproducts through the decontaminationprocesses to which they have beensubjected and also to the patient onwhom they have been used. The abilityto track and trace surgical instrumentsand equipment through thedecontamination life-cycle enablescorrective action to be taken whennecessary. For example, in the unlikelyevent of a sterilization cycle failure,products can then be recalled.
HSC 2000/032 states:
“It is important that systems are inplace to allow sets of surgicalinstruments to be tracked throughdecontamination processes in order toensure that the processes have beencarried out effectively. Systems shouldalso be implemented to enable theidentification of patients on whom theinstrument sets have been used. Thisis important so that the relevantpatients can be identified in the eventof exposure to potential risk, and isrelevant to both the primary andsecondary care sectors. Thisrequirement for traceability of
9
instrument is in addition to themeasures for identification andtracking of flexible endoscopes set outin Health Service Circular 1999/178.”
Records should be maintained for all thesets cleaned, identifying:
• the cleaning and sterilization methodused;
• the name of the person undertakingthe decontamination; and
• details of the actual item beingprocessed.
This information is required so thatinstrument sets can be traced, ifrequired, in the event of a failure in thedecontamination cycle or for infectioncontrol reasons.
Records relating to decontaminationprocesses should be maintained by theorganisation for a minimum of 11 yearsor in accordance with local data policies.
INFECTION CONTROL POLICIES
All organisations must have an infectioncontrol policy that contains:
• advice on decontamination andstorage of surgical instruments;
• local policies on recommendeddisinfectants, their application, use,storage and disposal;
• protocols for the cleaning anddisinfection of surgical instrumentswhere instruments have to beprocessed in a local setting;
• protocols for the use of personalprotective equipment (PPE);
• risk assessments for procedures usedin the reprocessing of surgicalinstruments;
• spillage procedures;
• management and treatment of needle-stick/sharps injuries.
This policy should be written incollaboration with the infection controlteam.
Controls Assurance standards exist forthe related issues of decontamination,the management of surgical instrumentsand associated equipment, and infectioncontrol. Organisations are legally requiredto undertake assessments and completetheir returns as part of their riskmanagement system.
DECONTAMINATION TRAINING
Members of staff undertakingdecontamination must be competent,properly trained and supervised. Anational training scheme is currentlybeing devised and will describe basictraining for staff involved in all aspects ofthe decontamination of surgicalinstruments.
Individual training records, detailing anindividual’s core competencies and anytraining received, must be maintainedand updated regularly. Line managers areresponsible for maintaining theserecords.
In the primary care setting, whoeverowns or manages the practice isresponsible for ensuring that systems arein place for ongoing staff training.
10
All used surgical instruments present arisk of infection. To minimise this risk, theinstruments must be placed in closed,secure containers and transported to thedecontamination area as soon aspossible following use.
Transport containers must protect boththe product during transit and thehandler from inadvertent contaminationand therefore must be:
• leak-proof;
• easy to clean;
• rigid, to contain instruments,preventing them becoming a sharpshazard to anyone handling the goodsand to protect them against accidentaldamage;
• capable of being closed securely;
• lockable, where appropriate, toprevent tampering;
• clearly labelled to identify the user andthe contents;
• robust enough to prevent instrumentsbeing damaged in transit.
Where decontamination takes place inthe clinical setting, the above principles
can be modified to suit localcircumstances. However, the methodsused must ensure that the product andhandler are protected at all times. It isrecommended that wherevercontaminated items are transported, riskassessments should be undertakenrelating to the safe movement of thedevice. Staff handling contaminatedinstruments and equipment must wearPPE in accordance with local policy andbe vaccinated against hepatitis B.Without exception after each use,transport containers must be cleaned,disinfected and dried, or discarded (asappropriate), using agreed methods.
Where contaminated instruments areto be transported outside of thehealthcare premises onto a publichighway, those responsible for suchtransportation must refer to therequirements of the Carriage ofDangerous Goods by Road Act 1992and the Health and Safety at Worketc Act 1974. It is essential to use amethod of transportation thatensures the segregation ofcontaminated product fromclean/sterile instruments.
11
2.0 Transportation of contaminated surgicalinstruments and associated equipment

PURCHASING
Organisations must have a clearly statedpolicy outlining how the purchasing ofmedical devices will be managed. Thisshould include a consultation process to ensure that all those involved in thepurchase, decontamination, and use ofthe device are given the opportunity todiscuss the suitability of an instrument orpiece of equipment before a purchase ismade. See the Microbiology AdvisoryCommittee manual (MAC manual) andMDA DB 9801.
Lack of consultation has often resulted indevices being purchased which cannotbe adequately decontaminated, as they are subsequently found to beincompatible with the decontaminationprocesses available within anorganisation. For example, devicesmanufactured outside the UK may requireprocesses that are not routinely availablewithin the UK, such as those that requiresterilization temperatures other than thestandard 121°C and 134°C cycles (seeMDA SN 2001 (28)).
To help organisations in purchasingdecisions, the NHS Purchasing andSupply Agency (PASA) has establishedframework agreements for purchasing anumber of medical products and devices,for example washer-disinfectors, surgicalinstruments etc. Details are available fromthe PASA catalogue and their website.
Best practice suggests that automatedwashing processes are the preferredoption. Therefore, devices that can bemechanically cleaned and thermallydisinfected should be purchasedwhenever possible. Some devices are,however, incompatible with automatedwashing processes and arerecommended for manual cleaning by themanufacturer.
When considering the purchase ofinstruments, the following issues shouldbe taken into account:
• Does the instrument have lumens/canthe device be easily cleaned? If not, isthere an alternative reusable devicewhich is easier to clean, or is a single-use device available as an alternative?
• Does the instrument need dismantlingbefore cleaning? Are instructionsprovided by the manufacturerdescribing how this can be done?
• Does the instrument have electricalcomponents? If yes, does theorganisation have the capability toclean and sterilize them in the mannerdescribed by the manufacturer?
• Does the instrument have a limitedlife? Is this specified by themanufacturer?
• What method of cleaning does themanufacturer recommend and is thisprocess available within theorganisation?
13
3.0 Acquisition
• What cleaning agents arerecommended and does this complywith local infection control policies,COSHH and health and safetyrequirements?
• If the instrument needs to besterilized, is the preferred method ofsteam sterilization (134°C for aminimum of three minutes)recommended? If another method ofsterilization is recommended, is thisavailable within the organisation?
• If the product is heat- or pressure-sensitive, what alternative means ofsterilization is recommended? Is thisprocess available within theorganisation?
• Has a risk assessment beenundertaken to determine whether asingle-use or a reusable product ismore appropriate for thecircumstances?
Manufacturers of re-usable surgicalinstruments are required to supplyinformation on the appropriatedecontamination process to allow reuse,including cleaning, disinfection and whereappropriate the method of sterilization(Consumer Protection Act 1997; MedicalDevices Regulations 2002).
LOAN SURGICAL INSTRUMENTSAND EQUIPMENT
It may sometimes be necessary toborrow equipment from anotherorganisation or manufacturer: forexample, for a trial, to treat a patientwhere equipment is not routinely availableor where workload dictates thatadditional equipment is required on atemporary basis. All surgical instrumentsand equipment entering the organisation,regardless of the source, should becleaned and sterilized before and afteruse in accordance with manufacturers’instructions (see MDA SN 2000 (18)).
If staff are unfamiliar with on-loanequipment or newly purchased devices, itis essential to arrange training from thesupplier/manufacturer to ensureequipment is decontaminated properlyand to minimise the potential for damage.Items requiring disassembly duringprocessing must be dismantled inaccordance with manufacturers’instructions.
Device loans should be so arranged togive adequate time for learning about theequipment and for decontamination ofthe device before it is required for use ona patient.
14
Effective cleaning of instruments (medicaldevices) before sterilization is of theutmost importance to reduce the risk oftransmission of infectious agents. This may be achieved in a number ofways. Whenever possible, cleaningshould be undertaken using anautomated and validated process inpreference to manual cleaning. Manualcleaning should be considered onlywhere manufacturer’s instructions specifythat the device is not compatible withautomated processes. Where manualcleaning is undertaken, it should becarried out in accordance with the‘Protocol for the local decontamination ofsurgical instruments’ issued by NHSEstates.
Research suggests that instrumentscleaned as soon as possible after use aremore easily cleaned than those left for anumber of hours before reprocessing.Where instruments have to betransported from the point of use to theprocessing centre, collections should bemade at frequent intervals throughout theday to ensure processing takes place assoon as possible after use.
It should be noted that certain solutions,in particular blood, saline and iodine, arecorrosive to stainless steel instrumentsand will cause pitting and then rusting ifallowed to remain on instruments for anylength of time.
FIRST USE OF SURGICALINSTRUMENTS
Many reusable items are manufactured inuncontrolled environments and some arehandled extensively during this process.In addition, many manufacturers leaveanti-corrosive agents such as oil andgrease on the surface and in the joints ofthe item for protection during transit.New items should be cleaned andsterilized before being put into use.Manufacturer’s instructions should befollowed, where available.
PRE-TREATMENT OF SURGICALINSTRUMENTS
Under normal circumstances it shouldnot be necessary to pre-treat surgicalinstruments at the point of use beforebeing sent to the central processing unit(sterile services department).
Gross contamination may makedecontamination more difficult if notremoved immediately. In suchcircumstances it is suggested thatinstruments should be cleaned as soonas possible after use.
All staff undertaking pre-treatmentcleaning of instruments should ensuretheir own safety by wearing appropriatePPE and carry out a risk assessment forthe procedures being employed.
15
4.0 Cleaning
DISASSEMBLY OF INSTRUMENTS
Equipment consisting of more than onecomponent must be dismantled so thateach part can be adequately cleaned.Advice on the methods for disassemblyof surgical instruments should be soughtfrom manufacturers. Training should beupdated to take into account any newinstruments introduced into theorganisation to ensure that theequipment is dismantled and thatadequate cleaning and sterilization takesplace. Personal training records shouldreflect the range of devices upon whichan individual has been trained and iscompetent to decontaminate.
AUTOMATED CLEANING
Washer-disinfectors
All washer-disinfectors used fordecontamination should be purchasedagainst the Model EngineeringSpecification C30 and be capable ofbeing validated in accordance with HTM2030.
There are a number of different models ofwasher-disinfector that meet currentstandards. The size, model and type tobe chosen should be considered againstworkload and throughput requirements,together with the availability of space.
Washer-disinfector logbooks and recordsshould be kept by the designated “user”as defined in HTM 2030. Records shouldinclude a description of any loadsprocessed, cycle parameters, productrelease together with details of routinetesting and maintenance of theequipment used.
Each stage of the decontaminationprocess should contribute to thereduction of bio-burden on the devicebeing reprocessed. The recognisedstages of the washing process mayinclude a cool pre-wash (below 35ºC toprevent protein coagulation), main wash,rinse, thermal disinfection and post-disinfection rinse (where appropriate). Theuse of ultrasonic cleaners may beconsidered to assist the process (seenext section).
Ultrasonic cleaners
Ultrasonic cleaners may be of the stand-alone ultrasonic bath type or may bewasher-disinfectors of Type 1 (singlechamber) or Type 2 (multi-chamber).
Many Type 1 washer-disinfectors do notincorporate a disinfection stage and areintended for use as a pre-cleaningprocess before final cleaning anddisinfection in a washer-disinfector forsurgical instruments.
Cleaning in the primary care setting isusually undertaken in a stand-alone bathfilled with potable water (drinking quality)and a measured amount of detergent, asper manufacturer’s instructions.Instruments are placed in a basket andinto the water where the ultrasonic actionwill remove gross soiling. This method ofcleaning should be seen as a first-stagecleaning process, which would normallybe followed by cleaning in a washer-disinfector or, where this is unavailable, athorough rinse before sterilization.
Where such cleaners are used, theequipment manufacturer’s operatinginstructions must be adhered to and staffgiven adequate training in the use of themachine. Ultrasonic cleaning should be
16
used only if recommended by theinstrument/device manufacturer.
Ultrasonic action is generated bytransducers that agitate the water bycreating bubbles. The bubbles implodeand dislodge dirt from the surface andjoints of surgical instruments.
Ultrasonic action helps to thoroughlyclean devices with joints or multiplecomponents that are difficult to cleanmanually.
Ultrasonic cleaners are notrecommended for cleaning certain items,in particular rubber products which willabsorb the ultrasonic waves and reducethe efficacy of the cleaning process.
Directions for use of ultrasoniccleaners
Staff must wear PPE at all times whilehandling contaminated instruments andworking with the ultrasonic cleaner.
1. Fill the tank with potable water(drinking quality) to the manufacturer’sdesignated level. This ensures that thedevice being cleaned is notcontaminated by water impurities.
2. De-gas the water as recommended bythe machine manufacturer.
3. Add detergent, ensuring themanufacturer’s recommendations arefollowed. It is advisable to use asuitable enzymatic detergent that iseffective at low temperatures.
4. If the tank has a heater, set thetemperature control to be comparablewith the detergent manufacturer’srecommendations.
5. When the specified temperature hasbeen reached, place theopened/dismantled instruments intothe basket.
6. Place the basket of instruments intothe tank. Never put instrumentsdirectly onto the base of an ultrasonicwasher.
7. Set the timer control to the timespecified by the machinemanufacturer.
8. After the cycle has been completed,remove the basket from the tank andrinse the items with clean, potablewater – unless the machine has anautomatic rinse stage, or the load is tobe transferred directly into a washer-disinfector for further processing.
9. Drain and dry the items using a non-linting cloth or mechanical dryingsystem.
10. Record the instrument(s) that hasbeen processed, including themethod and solutions used anddetails of the staff member whocompleted the procedure.
11. After use, the ultrasonic washershould be drained, cleaned, dried,covered and left dry and empty untilrequired for further use, as per themanufacturer’s instructions.
Testing of ultrasonic cleaners
In accordance with guidance contained inHTM 2030, a qualified “test person”should regularly maintain and testultrasonic cleaners. The testrequirements and the role of the testperson can be found in HTM 2030. It isrecommended that a soil test and a
17
residual protein test should be performedas part of the weekly tests to establishthe efficacy of the washer’s cleaningprocess.
The following simple test may beundertaken to establish that there isultrasonic action in the tank. It shouldnot, however, replace the detailed testsspecified in HTM 2030:
1. Clamp the edge of a piece ofaluminium foil (approximately 5 cm2) ina pair of metal forceps.
2. Hold in the centre of the bath forapproximately three minutes.
3. Remove, dry and inspect thealuminium foil for changes.
4. File the strips of foil as a record of thetest having been undertaken, togetherwith all relevant test details, that ismachine number, date, test result(pass/fail), name of operator etc.
(Note: Do not put hands into the tank ofan ultrasonic cleaner while the machine isin use.)
Effective ultrasonic action will serrate theedge and pit/perforate the centre of thefoil. However, if the aluminium foil iswithdrawn without any noticeable changeto its condition, this may indicate that themachine is not functioning properly andthe manufacturer/supplier should beconsulted. It should be noted howeverthat the strength of the ultrasonic waveswill vary throughout the tank.
(Note: the appropriateness of this testwill depend on the frequency at whichthe ultrasonic cleaner operates. Consultthe equipment manufacturer for furtherinformation.)
Points for consideration
Contamination of instruments can occurwhen the water in the ultrasonic bath isnot changed regularly: if grosscontamination is present on the surfaceof the water, debris can be depositedonto instruments when they are lifted outof the bath. Therefore, it is recommendedthat the tank be emptied regularly – as aminimum, every four hours, or when thewater is visibly soiled.
PROCEDURE FOR MANUALCLEANING
Manual cleaning would normally becarried out using either immersion ornon-immersion methods depending onthe construction of the device.
Immersion method
To minimise the risk to personnelundertaking manual cleaning, splashingand the creation of spray must beavoided at all times. Staff carrying outmanual cleaning should wear PPE at alltimes.
1. Fill sink 1 (not a hand basin or otherclean receptacle) with potable water toa predetermined level at the specifiedtemperature and with the appropriatedetergent. Sink 1 must be solelydedicated for the cleaning ofinstruments, and not for any otherpurpose.
2. Detergents used must be specificallydesigned to clean surgicalinstruments: washing-up liquid shouldnot be used. Detergent dilution andwater temperature should be inaccordance with the manufacturer’sinstructions and local policy.Consideration should be given to the
18
use of an enzymatic detergent tofacilitate the cleaning of surgicalinstruments with channels or complexparts.
3. Dismantle or open the instrument tobe cleaned and fully immerse in thesolution to displace trapped air and, inthe case of hollow instruments, toensure penetration of channels.
4. Brush, wipe, agitate, irrigate, jet-washor hand-spray the item to dislodgeand remove all visible dirt, taking careto ensure the item remains under thesurface of the water at all times toprevent the creation of aerosol (spray).Brushes should be made from nylonbristles and should be cleaned andsterilized daily, or preferably, should besingle-use only.
5. If high-pressure-jet guns are used forcannulated instruments, they shouldbe connected to the cold-water supplyonly. The gun is connected to theinstrument and held under waterduring the irrigation process.
6. Remove the device from sink 1 anddrain any excess cleaning solutionbefore placing in sink 2 for rinsing.
7. Change the rinse-water after everybatch of instruments or when itbecomes visibly soiled or cloudy.
8. Rinse the item thoroughly with cleanpotable water using the water-jet gunwhen necessary (see point 5).
9. Remove and drain the item, and thendry using the preferred method: for
example, by using a clean, non-lintingcloth or by mechanical drying. Analcohol wipe can be used to facilitatethe drying process.
10. Cleaning materials should be safelydisposed of in accordance with localwaste policy.
11. Record the device that has beenprocessed including the method andsolutions used and details of thestaff member who completed theprocedure.
Non-immersion method
This method is appropriate for itemswhose working components will becomecompromised by soaking, for exampledental drills, power tools or electronicequipment.
Cleaning information about the methodsto be used for specific devices must besought from individual devicemanufacturers.
Devices should be:
1. cleaned using a non-linting cloth,impregnated with the appropriatedetergent solution, followed by aclean, damp, non-linting cloth; andthen
2. dried using another clean, non-lintingcloth.
Alcohol-impregnated wipes may be usedfollowing a manual cleaning process.
19

Disinfection is defined as a process usedto reduce the number of viable micro-organisms in a load, but which may notnecessarily inactivate some viruses andbacterial spores. Disinfection in theclinical setting may be achieved by anumber of methods, the two mostcommon being moist heat and liquidchemicals.
Moist heat is the method of first choiceas it is easily controlled, leaves no toxicresidues and is relatively safe to thoseinvolved in the process. Disinfection canbe achieved by washing or rinsingdevices in water at between 73°C and90°C. Most of the washers manufacturedfor the reprocessing of surgicalinstruments incorporate a disinfectionstage.
Devices that cannot withstand relativelyhigh temperatures required fordisinfection by moist heat may bedisinfected using chemicals. Receptaclesused for chemical disinfectant solutionsmust be cleaned and steam-sterilizedbefore being used. Care must be takento ensure that the device is scrupulouslyclean, that the correct chemicalconcentration is used and that the deviceis properly submerged to ensure contactwith all parts.
It is important to note that whenpreparing chemical disinfectants, staffinvolved must wear the appropriate PPE.The room used for chemical disinfectionmust be well-ventilated or contain an
appropriate Class 1 exhaust-protectivecabinet or equivalent. COSHHassessments must be consultedregarding the toxicity of the substance(s)used. Staff should be aware that certainsubstances may require personalmonitoring and/or monitoring byoccupational health services as part ofhealth and safety requirements.
In the case of devices with lumens, itmay be necessary to agitate the device inthe disinfectant to dislodge any airtrapped inside. Disinfectants will beeffective only if the solution reaches allsurfaces of the device to be disinfectedand appropriate exposure timesrecommended by the disinfectantmanufacturer are adhered to.
If the device is for immediate use afterdisinfection, staff must use an aseptictechnique when removing it from thechemical solution. Then, the device mustbe thoroughly rinsed in sterile water andcarefully dried using a sterile, non-lintingcloth. The manufacturer’s recommendedmethod(s) and the compatibility of thedevice with the chosen process will alsobe important considerations.
If the device is to be stored before beingused, it can be removed from the liquid,rinsed in sterile water, dried with a non-linting cloth and stored in a secure area.Where a sterile product is required, itshould be processed immediately beforebeing used and not stored before use.
21
5.0 Disinfection
The inspection, maintenance or testing ofdevices must be carried out by suitablytrained staff in accordance with themanufacturer’s instructions and localpolicy. Where practical, the inspectionand function-testing of surgicalinstruments should not be carried out bythe same staff responsible for cleaningthe devices. These staff members have aresponsibility for ensuring the item isthoroughly cleaned and fit for reuse.Records should be kept of all inspectionand testing work undertaken.
INSPECTION OF SURGICALINSTRUMENTS
The importance of inspecting eachinstrument cannot be over-emphasised.A visual check for cleanliness anddryness should be made for all itemswashed as part of the decontaminationprocess. All non-conforming product –that is, dirty, wet or stained – should berejected and returned to the wash areafor manual cleaning, followed by anautomated wash process (where thisprocess is available and the device iscompatible) before continuing through topackaging and sterilization.
The condition of the instrument has asignificant effect on how adequately itcan be cleaned. Instruments that aresubjected to rough handling (despitebeing made of stainless steel!) willdevelop scratches and roughenedsurfaces, which will harbour dirt.
Instruments that have an outer insulationcoating, for example diathermy forcepsetc, require close inspection to ensurethat the insulation remains intact.Damaged surfaces not only will allow dirtand bacteria to collect, but can also bepotentially dangerous for both staff andpatients.
FUNCTION-TESTING
As part of the decontamination process,all instruments should be subject tofunction-testing following the cleaningprocess to ensure that they will performthe tasks for which they are designed. Itis difficult to test surgical instruments tomimic their actual use; however, somebasic tests can be undertaken to ensurethat:
• there is free movement of all parts andthat joints do not stick;
• the edges of clamping instrumentsmeet with no overlap and that teethmesh together;
• scissor edges meet to the tip andmove freely across each other with nooverlap or burrs (rough edges);
• all screws on jointed instruments aretight and have not become lose duringthe cleaning process.
Occasional use of a lubricant may berequired where hinged instruments arefound to be stiff. A non-oil-based
23
6.0 Inspection and function testing
lubricant should be used to avoid itinterfering (that is, preventing the steamcoming into contact with the instrumentsurface) with the sterilization process.
In preparing instruments for wrappingand sterilization, it is essential that allsurfaces are presented to the sterilizationmedia (that is, steam or chemical) andthat, where devices can be taken apart,they are sterilized in this state whereverpracticable. For instruments withratchets, to ensure steam can penetrateto all surfaces, they should be closed onthe first ratchet only.
It is vital to have a procedure wherebythe users of surgical instruments willinform those responsible for reprocessingabout defects and the need to haveitems repaired and/or replaced. In thecase of instrument sets, the contentssheet may be used to indicate faultyinstruments but the actual item must beidentified in case there are a number ofsimilar devices on the same set.
REPAIRS
Instruments may become damagedduring use or suffer from general wearand tear over their life span. Instrumentsbecome damaged for a number of
reasons, but typically throughinappropriate use, poor handling orcontact with corrosive substances. Thedamage to instruments may take theform of physical damage, for examplewhen an item is dropped or as a result ofa reaction to contact with corrosiveagents during use, for example iodine orsaline solutions used in operatingtheatres. Typical damage includesrusting, pitting or general surfacecorrosion.
If devices are found to be faulty ordamaged during inspection and function-testing, or if users identify that they arefaulty, they should be taken out of useand either repaired or replaced.Instruments for repair should be returnedto either the manufacturer or a reputablerepair company. They should bedecontaminated in accordance withMHRA DB 2003 (05) and beaccompanied by a DecontaminationCertificate (a sample of which can befound in the MHRA device bulletin; seethe MHRA web-site). Where instrumentsare taken out of use, which are part ofinstrument “sets”, the set should beremoved from use until the repair can beundertaken and the instrument returnedto the set.
24
It is not always necessary for instrumentsto be wrapped before being sterilized.Indeed, when certain types of sterilizersare used, for example non–vacuumbenchtop or bowl and instrumentsterilizers, packaging is notrecommended. (Items sterilized in a non-vacuum benchtop sterilizer must not bepackaged because this may impede thepenetration of steam to all surfaces of theinstrument and prevent sterilization takingplace).
Where packaging is recommended, forexample in porous-load and vacuumbenchtop sterilizers, materials should beused which comply with appropriatepackaging standards for sterilization asdetailed in the BS EN 868 series. Thepackaging materials must be compatiblewith the sterilization process and may beof either a rigid or flexible material.
The reasons for packaging instrumentsare:
• containment of the product throughthe different stages of thedecontamination process;
• to allow sterilization to take place;
• to protect the product duringsterilization and transportation fromdeterioration and damage;
• to maintain sterility to the point of use;
• to prevent contamination of theproduct following decontamination.
Packaging of products after thesterilization process is not recommended.
There are a variety of packaging materialsavailable for individual surgicalinstruments. The choice of type and sizewill depend on the item to be packaged.Peel-apart pouches or plain paper bagsare often used for single instruments orsmall loads, that is bags with a see-through front and paper backing.
• Sealing peel-apart pouches isessential to ensure that the productremains sterile after autoclaving. Inself-sealing pouches, adhesive ismanufactured into the open end of thebag or plain top and either a heat-sealing machine or autoclave tape isthen required to create a seal.
• Paper bags can either be plain top(which requires autoclave tape forsealing) or have a heat-seal top (whichrequires a crimping and sealingmachine).
Other forms of packaging suitable forlarger devices or multiple items includemetal or plastic containers, metal trays ofvarying dimensions, sterilization paper,plain and crêpe, and many moredepending upon the chosen method ofsterilization.
25
7.0 Packaging
LABELLING OF STERILE SURGICALINSTRUMENTS
Sterile surgical instruments should belabelled in accordance with therequirements of BS EN 980 – ‘Graphicalsymbols for use in the labelling ofmedical devices’.
In addition to the above symbols, thefollowing information should be availablefor the device being processed:
1. Name of device/pack.
2. Name of the manufacturer, that is“reprocessor”.
3. The date of manufacture/sterilization.
4. Date of expiry (where appropriate).
5. The method of sterilization used, forexample steam, ethylene oxide etc.(This may already be obvious by thesterilization indicator panel on thepackaging material).
6. Cycle number/machine number of thesterilizer used.
26
Saturated steam under pressuredelivered at the highest temperaturecompatible with the product is thepreferred method for the sterilization ofmost instruments (devices) used in theclinical setting. To facilitate sterilization,load items must first be thoroughlycleaned and disinfected.
There are a number of different types ofsterilizer used within the healthcaresetting:
• Porous-load sterilizers. These aresteam autoclaves with an active air-removal stage designed to processwrapped goods or lumened devices.They are produced in various sizesranging from portable benchtopdesign to large capacity (commonly0.6 m3/21 ft3) machines and areusually located in sterile servicesdepartments (SSDs).
• Bowl and instrument sterilizers.These machines often have largecapacity and may be found inoperating theatres. They have cycleparameters similar to those of porous-load sterilizers but without an activeair-removal stage or drying cycle,therefore prohibiting packaged loadsfrom being sterilized. Their use islimited to sterilizing items which aresolid and not hollow or cannulated.
• Benchtop steam sterilizers. Thereare several types available. The twomost common types are:
– non-vacuum: commonly usedfor surgical instruments that areunwrapped, not hollow and donot have lumens;
– vacuum: can be used forwrapped and hollow/lumeninstruments.
POROUS-LOAD STERILIZERS
These machines are more commonlyknown as autoclaves, and use vacuumassistance to remove air from thechamber at relatively high temperatures.They are designed to process porousloads such as wrapped items (that istextiles, dressings, surgical instrumentsetc) which may be either solid or hollowand items with lumens.
The typical stages to a porous-loadsterilizer cycle include:
• air evacuation;
• sterilizing;
• post-vacuum or drying stage.
Where surgical instruments areprocessed, specific time–temperaturerelationships exist for the standardoperating cycle:
134°C plus 3 minus 0 for a holdingtime of 3 to 3.5 minutes.
HTM 2010 defines the responsibilities ofthe operator and users of these
27
8.0 Sterilization
machines and provides information onhow these sterilizers should be used,tested and maintained.
BOWL AND INSTRUMENTSTERILIZERS
These sterilizers are similar in design andoperate in a similar way to porous-loadsterilizers, but without an active dryingcycle or air removal. They must not beused for wrapped items or those whichare hollow or have lumens. Machineslocated in operating theatres aregradually being phased out as thedecontamination of surgical instrumentsis transferred to central processing units,that is SSDs.
BENCHTOP STERILIZERS
Benchtop sterilizers must be operated toensure that:
• they are compliant with safetyrequirements;
• they are installed, validated andmaintained appropriately (HTM 2010;MDA DB 9804 and MDA DB 2002(06));
• they are operated in accordance withthe equipment manufacturer’sinstructions.
Users should be aware of the cautionarynotes relating to the improper use ofsmall benchtop sterilizers. These include:
• Wrap instruments only where this isrecommended by the manufacturerand where the sterilizer is vacuum-assisted. The sterilizer must bevalidated for the intended load.
• Rigid endoscopes cannot beprocessed in benchtop sterilizersunless designated as autoclavable bythe manufacturer and the process hasbeen validated for the instrument (seethe Medical Devices Directive, Annex1, ER 13.6(h)).
• Hollow or lumen instruments are notsuitable for sterilization in non-vacuumsterilizers.
All steam sterilizers are subject to thePressure Systems Safety Regulations2000 and must be examined periodicallyby a Competent Person (PressureVessels).
Use and testing of benchtopsterilizers
To ensure the safety of this device, thefollowing points must be adhered to:
1. Each sterilizer will have a reservoirchamber from which the water isdelivered for steam generation; thismust be filled daily using sterile waterfor irrigation BP. At the end of the dayor following final use, the chambershould be drained (only when thewater has cooled), cleaned, dried,covered with a lid and left empty forfuture use (see HTM 2031).
2. Testing is an integral part of ensuring abenchtop sterilizer consistentlyperforms to operating parameters setduring the machine’s commissioning.Failure to carry out routine periodictests and maintenance tasks couldcompromise safety and have legal andinsurance-related implications for theuser or owner of the sterilizer.
28

3. A schedule for periodic testing shouldtherefore be planned and performed inaccordance with documentedprocedures (see HTMs 2010 and2031; and MDA DB 2002 (06)). Theschedule should provide details ofdaily, quarterly and yearly testing.Each sterilizer should have a logbook(file) in which details of the followingare recorded:
– maintenance;
– validation;
– faults;
– modifications;
– routine tests.
HSC 1999/053 provides guidance on thelength of time for which records shouldbe retained.
Details of each load processed shouldalso be retained in this logbook.Examples of logbook pages can befound in the Annex of MDA DB 2002(06).
Daily testing and housekeeping tasks
Some benchtop sterilizers require awarm-up cycle before instruments can beprocessed. The manufacturer’sinstruction manual should be consultedto find out whether this is the case.
The daily tests should be performed bythe operator or user and consist of:
• a steam penetration test (vacuumbenchtop sterilizers only);
• an automatic control test (all benchtopsterilizers).
The tests may be carried out at the sametime.
Sterilizers must not be used until thedaily tests and housekeeping taskshave been carried out, and theresults found to be satisfactory.
Before carrying out the daily tests, theuser should:
• clean the rubber door seal with aclean, damp, non-linting cloth;
• check the chamber and shelves forcleanliness and debris;
• fill the reservoir with sterile water forirrigation BP;
• turn the power source on;
• record these tasks with the date andsignature of the operator in thelogbook.
If the sterilizer fails to meet any of thetest requirements, it should be withdrawnfrom service and advice should besought from the manufacturer and/ormaintenance contractor (for example, theestates department).
A schedule of weekly, quarterly andannual tests may be found in MDA DB2002 (06) or MDA DB 9804.
Steam penetration test procedure
• Place the Bowie–Dick type test pack(conforming to BS EN 867:2001)within the chamber in a positionrecommended by the manufacturer.This will ensure that the test presentsthe machine with the greatestchallenge from which to remove airfrom the load.
29
• Select a standard cycle or the cyclespecified by the sterilizer manufacturer.(The test should always be performedusing the same cycle).
• At the end of the test, remove the testsheet from the middle of the pack andcompare the results with themanufacturer’s test sheet.
• The test is satisfactory if the indicatorshows a uniform colour change.
• The test results PASS/FAIL should berecorded in the sterilizer logbook.
• The test result indicator paper shouldbe marked with the result, date andcycle number and kept within thelogbook for reference. (It should bestored according to the manufacturer’srecommendations).
• If the sterilizer is fitted with a chartrecorder, the test cycle print-outshould also be retained within thelogbook.
If the test result is unsatisfactory, themachine should be taken out of use andthe fault investigated (this may requiretesting by a designated Test Person).
Automatic control test
Daily tests are referred to as automaticcontrol tests. Details of how to undertakethese tests can be found in themanufacturer’s user manual. For accuratemonitoring of the cycle parameters, astopwatch is recommended for accuratetimings. (An automatic control test is notrequired if the sterilizer is equipped with arecorder that provides a permanentrecord (print-out) of the temperature,pressure and elapsed time during allstages of the sterilization cycle/s in use.)
Use of chemical process indicators
Chemical process indicators are amechanism by which sterilizer loads canbe identified as having passed through aprocess. The chemical indicator reactswhen exposed to steam anddemonstrates a change in character,usually colour. These chemical indicatorscan take the form of an autoclave tape,test tubes containing chemical indicatoror sterilization packaging/bags. In allthese cases, the chemical indicators willchange colour when subjected to heat.
• Indicators must be stored inconditions that will not adversely affectthe performance of the chemicals.
• Store in accordance withmanufacturer’s instructions.
• Do not use indicators beyond theexpiry date stated by themanufacturer.
• Chemical process indicators should beused and read in conjunction withsterilizer-process print-outs or asterilization cycle’s parameters.
Microbiological testing of steam sterilizersis not recommended.
Processed devices for immediate use
Non-vacuum benchtop steam sterilizersare designed to process items forimmediate use within a clinicalenvironment.
Upon completion of the sterilizationcycle, if the machine does not have avacuum cycle, steam is condensed withinthe sterilizer’s chamber, resulting in a wetload. Partial drying does occur by naturalevaporation after the load is removedfrom the chamber, but once the door to
30
the sterilizer chamber has been opened,the load is compromised andsubsequently exposed torecontamination. Benchtop sterilizersused to sterilize unwrapped items shouldtherefore only be used to sterilize loadsfor immediate use.
It is not recommended that loads arepackaged after sterilization.
(Note: where sterilized items are notrequired for immediate use, they shouldbe dried using a clean, non-linting clothbefore storage in clean, closed, securedcontainers until required. Such containersshould be regularly cleaned andsterilized. Should unwrapped items needto be sterile at the point of use, the itemsshould be resterilized immediately beforebeing used.)
Vacuum benchtop steam sterilizers
Steam sterilization requires direct contactbetween dry saturated steam and allsurfaces of the load at a specifiedtemperature and pressure for a definedperiod of time. To enable sterilizing
conditions to be achieved, load itemsmust, therefore, be cleaned thoroughlyand air removed effectively from thesterilizing chamber and the load. Effectiveair removal is essential to enable steamto penetrate wrapped devices and thosewith lumens. This can be achieved only ifthe sterilizer is equipped with an activeair-removal system, as are vacuumbenchtop sterilizers. They can processporous loads (Type B cycle) or types ofdevices specified by the sterilizermanufacturer (Type S cycle).
The drying stage must reduce themoisture content of packages andporous materials to a level that will notpermit bacterial recontamination.
Because vacuum benchtop steamsterilizers are more complex than theirnon-vacuum counterparts, they requiremore rigorous testing to demonstratethat they function correctly. Therefore,owners/users of benchtop sterilizersshould ensure that the sterilizer is subjectto a planned and documented scheduleof preventative maintenance.
31
Central decontamination facilities areoften located away from clinical areasand may be some distance from thepoint of use. It is therefore recommendedthat processed goods are stored inclinical areas ready for use. The methodof transport used to transfer surgicalinstruments and equipment is determinedby:
• the type of product being moved;
• the distance between thedecontamination centre and the pointof use;
• whether deliveries are being made tointernal or external users.
Transit containers must:
• protect the instruments andequipment;
• prevent inadvertent contaminationduring transportation; and
• prevent contamination of staff etcwhen transporting used instrumentsfor reprocessing.
They should have the followingcharacteristics:
• be waterproof;
• be easy to clean (ideally suitable fordecontamination in an automatedwasher-disinfector);
• be rigid in order to protect instrumentsfrom damage;
• be capable of being closed securely;
• be fitted with a tamper-proof seal;
• be constructed in such a way so as toprevent damage to the products beingtransported;
• be clearly labelled to identify thedelivery address.
33
9.0 Transportation of decontaminatedsurgical instruments and associatedequipment
Following the decontamination of surgicalinstruments and other medical devicesand accessories, it is important to ensurethat the storage conditions maintain thepacks in the condition in which they arerequired for use. As a general rule, thiswould involve maintaining the sterility ofwrapped products but may also includethose packs which have been processedand which are not required in a sterilestate at the point of use, that isdisinfected.
Sterile products are usually stored at thepoint of use, for example wards, clinics,departments and operating theatres.However, regardless of the location, thestorage area should be dedicated for thepurpose and not used for other activities,for example patient treatment areas.
• The storage area should beappropriately designed to preventdamage to packs and to allow for thestrict rotation of stocks.
• Shelving should be easily cleaned andallow the free movement of air aroundthe stored product.
• Products must be stored above floorlevel away from direct sunlight andwater in a secure, dry and coolenvironment.
Inadequate control of these areas mayhave an adverse effect on the integrity of
the sterile product and subsequentlyrender it unsterile and unsuitable for use.
Rough handling of sterile products candamage both the product and thewrapping and may render the productunsterile. Do not pack products tightlytogether on shelves, in draws or incontainers as this may also damage thepackaging (see MDA SN 1999 (32)).Products found to be damaged or wetshould be returned for reprocessing.
Before being used, the sterile productshould be checked to ensure that:
• the packaging is intact;
• the sterilization indicator confirms thepack has been subjected to anappropriate sterilization process; and
• the product is still within the expirydate.
As a “rule of thumb”, product which hasremained unused for more than sixmonths should be deemed to be aproduct of over-stocking and anassessment undertaken as to its futureneed.
There are occasions where devices mustform part of emergency stocks and as aresult may not be used within this timeframe. Procedures should be put in placeto ensure that these products are subjectto a reprocessing regime over time.
35
10.0 Storage of sterile products
It is the responsibility of the “user”, that isnursing staff etc, to ensure that theequipment they intend using is “fit forpurpose”. By this, it is meant that theproduct has been subjected to anappropriately validated process and thatevery reasonable precaution has beentaken to ensure that the sterile condition(or otherwise) of the product has beenmaintained up to the point of use.
Responsibility for ensuring that safe andeffective decontamination of devices hastaken place will fall to a number ofhealthcare workers depending on thesetting in which they work.
• In hospitals, it is often the sterileservices technician or nursing auxiliarywhere decontamination takes place inthe clinical setting.
• In a primary care setting, it may be thepractice nurse or dental technicianwho undertakes reprocessing.
Each will have his/her own responsibilityfor elements of the decontamination
process. In some circumstances, thetransportation of devices may be theresponsibility of the person who has alsodecontaminated the product; in others, itmay be a different person or department,for example portering staff or other third-party.
Thus, for the product to reach the pointof use safely and in good condition, allthose involved in the different elements ofthe decontamination life-cycle must beappropriately trained and aware of theirresponsibilities in providing a productwhich is fit for purpose.
Users have a responsibility to notify thoseproviding a decontamination service ofany service problems, either aboutavailability of devices or about thedevices themselves. This may includesurgical instruments which require repairor sharpening or about late deliverieswhich may have affected patienttreatments.
37
11.0 Use of surgical instruments andassociated equipment
The environment in which flexibleendoscopes are processed should be ofthe same high standards as those forother surgical instruments, dedicated forthe purpose and separated fromtreatment areas.
In accordance with manufacturer’srecommendations, the channels offlexible endoscopes should be flushedimmediately after use and then manuallycleaned before the automated cleaningprocess. Cleaning brushes should be ofthe single-use type.
Flexible endoscope accessories shouldbe processed in accordance withmanufacturer’s instructions and identifiedso as to allow tracking/tracing throughthe decontamination process of theflexible endoscope and the patient onwhom it is used.
An automated endoscope reprocessorwith an integrated cleaning and drying
system is the preferred option forreprocessing flexible endoscopes(HTM 2030).
Flexible endoscopes should be stored byhanging in a dedicated cupboard wherethey can be protected against damageand potential recontamination.
Where endoscopes have been cleanedand stored but are required to be used ina high-level disinfection state, thedisinfection process must be repeated foreach device immediately before use.
Detailed guidelines for the cleaning andhigh-level disinfection of endoscopyequipment can be found in MDA DB2002 (05).
It is vital that the outer covering of theendoscope be tested before use for thesafety of patient and staff. This is knownas “leak testing” (see MDA DB 2002(05)).
39
Appendix 1 – Processing of flexibleendoscopes
ACTS AND REGULATIONS(GENERAL)
(The) Carriage of Dangerous Goods byRoad Act 1992, HMSO.
Consumer Protection Act 1998 (ProductLiability), HMSO.
(The) Control of Substances Hazardousto Health (COSHH) Regulations 2002,HMSO.
Health & Safety at Work etc Act 1974,HMSO.
(The) Management of Health & Safety atWork Regulations 1999, HMSO.
Medical Devices Regulations 2002,HMSO.
Personal Protective Equipment at WorkRegulations 1992, HMSO.
MEDICAL DEVICES
HSC 2000/032: Decontamination ofmedical devices, Department of Health,2000.
MDA DB 9801: Medical device andequipment management for hospital andcommunity-based organisations, MedicalDevices Agency, 1998.
MDA SN 1999 (32): Storage of sterilemedical devices, Medical DevicesAgency, 1999.
MDA SN 2000 (18): Handling of surgical:instruments on loan from anotherorganisation, Medical Devices Agency,2000.
Medical Devices Directive 93/42 EC, EUCouncil Directive, 1995.
MHRA DB 2003 (05): Management ofmedical devices prior to inspection,service & repair, Medicines andHealthcare Products Regulatory Agency,2003.
PROCESSING
BS EN 867:2001 Non-biological systemsfor use in sterilizers, British StandardsInstitution, 2001.
BS EN 868: Packaging materials andsystems for medical devices which are tobe sterilized, British Standards Institution,1997-2000.
BS EN 980:1997 Graphical symbols foruse in the labelling of medical devices,British Standards Institution, 1997.
MDA DB 2000 (04): Single-use medicaldevices – implications and consequencesof re-use, Medical Devices Agency, 2000.
MDA SN 2001 (28): Compatibility ofmedical devices and reprocessing unitswith decontamination agents, MedicalDevices Agency, 2001.
41
Appendix 2 – References
MDA DB 2002 (05): Decontamination ofendoscopes, Medical Devices Agency,2002.
Protocol for the local decontamination ofsurgical instruments, NHS Estates,HMSO, 2001.
Sterilization, disinfection and cleaning ofmedical equipment: guidance ondecontamination from the MicrobiologyAdvisory Committee to the Department ofHealth Medical Devices Agency (MDA)1996, 1999, 2000, 2002, ISBN1 85839518 6 (MAC Manual), Medical DevicesAgency, 1993-2002.
DECONTAMINATION PROCESSINGAND EQUIPMENT
C30 – Model Engineering Specificationfor Washer-disinfectors for surgicalinstruments, NHS Estates, The StationeryOffice, 2001.
HTM 2010: Sterilization, NHS Estates,HMSO, 1994-1997.
HTM 2030: Washer-disinfectors, NHSEstates, HMSO, 1997.
HTM 2031: Clean steam for sterilization,NHS Estates, HMSO, 1997.
MDA DB 9804: The validation andperiodic testing of benchtop vacuumsteam sterilizers, Medical DevicesAgency, 1998.
MDA DB 2002 (06): Benchtop steamsterilizers – guidance on purchase,operation and maintenance, MedicalDevices Agency, 2001.
(The) Pressure Systems SafetyRegulations 2000, HMSO, 2000.
INFECTION CONTROL/RISKMANAGEMENT
Advisory Committee on DangerousPathogens Spongiform EncephalopathyAdvisory Committee (SEAC):Transmissible spongiformencephalopathy agents: safe workingand the prevention of infection,Department of Health, 2001.
Controls Assurance Standard: InfectionControl, Rev(03), Department of Health,2002.
Controls Assurance Standard: MedicalDevices Management, Rev(03),Department of Health, 2002.
Controls Assurance Standard:Decontamination of reusable medicaldevices, Rev(02), Department of Health,2002.
HSC 1999/053: Preservation, retentionand destruction of records. Departmentof Health, 1999.
HSC 1999/178: Variant Creutzfeld-JakobDisease: Minimising the risk oftransmission, Department of Health,1999.
HSC 1999/179 – Controls Assurance inInfection Control – Decontamination ofMedical Devices, Department of Health,1999.
USEFUL WEBSITE ADDRESSES
Institute Of Sterile Services Management– http://www.issm.org.uk
Medicines and Healthcare productsRegulatory Agency (MHRA) – (formerlythe Medical Devices Agency)http://www.mhra.gov.uk
42

NHS Estates –http://www.decontamination.nhsestates.gov.uk
NHS Purchasing and Supplies Agency –http://www.pasa.doh.gov.uk
43
AerosolDispersion of solid or liquid particles in agas.
Automatic control testA test designed to show that theoperating cycle – as evidenced by thevalues of the cycle variables indicatedand recorded by the instruments fitted tothe sterilizer – functions correctly.
Benchtop sterilizerApparatus designed to achievesterilization, which requires no permanentconnections or installation.
Bio-burdenThe population of viable infectious agentscontaminating a medical device.
Bowie–Dick testTest designed to indicate that thesterilizer is capable of removing air andnon-condensable gases from a load.
Central decontaminationWhen reprocessing occurs in a centraldecontamination unit, for example asterile services department (SSD).
Chemical indicatorA device designed to show, usually by achange of colour, whether specifiedvalues of one or more cycle variableshave been attained.
Clinical area/settingAny medical and surgical ward,department or patient treatment area.
DecontaminationA process which removes or destroyscontamination and thereby preventsinfectious agents or other contaminantsreaching a susceptible site in sufficientquantities to initiate infection or any otherharmful response. Differing levels ofdecontamination are available. They are:cleaning followed by high leveldisinfection; or cleaning followed bysterilization, depending on the procedureand chemicals used.
DisinfectionA process used to reduce the number ofviable micro-organisms in a load butwhich may not necessarily inactivatesome viruses and bacterial spores.
DisinfectorAn apparatus designed to achievedisinfection.
FaultThe recognition by the automaticcontroller that the pre-set cycle variablesfor the operating cycle have not beenattained, and that sterilization ordisinfection has been jeopardised.
Holding time The period during which the temperaturein all parts of the chamber, load and anycoolant fluid is held within the sterilizationtemperature band. It follows immediatelyafter the equilibration time.
45
Appendix 3 – Glossary
Load Collectively, all the goods, equipment andmaterials that are put into a sterilizer ordisinfector at any one time for thepurpose of processing it by an operatingcycle.
Load items One of several discrete containers, packsor other items that together constitute aload.
Local decontaminationWhen instruments are reprocessed withinthe department where they are used.
Medical device Any instrument, apparatus, appliance,material or other article, whether usedalone or in combination, including thesoftware necessary for its properapplication intended by the manufacturer,to be used for human beings for thepurpose of: diagnosis, prevention,monitoring, treatment or alleviation ofdisease; diagnosis, monitoring,treatment, alleviation of or compensationfor an injury or handicap; investigation,replacement or modification of theanatomy or of a physiological process;and control of conception: and whichdoes not achieve its principal intendedaction in or on the human body bypharmacological, immunological ormetabolic means, but which may beassisted in its function by such means(source: EU Council Directive93/42/EEC).
Operating cycle The set of stages of the sterilization ordisinfection process carried out insequence and regulated by the automaticcontroller. It is synonymous with theterms sterilization cycle for sterilizers anddisinfection cycle for disinfectors.
Periodic tests A series of tests carried out at specifiedintervals, for example daily, weekly,monthly, quarterly or annually.
Porous-load sterilizer A clinical sterilizer designed to process,by exposure to high-temperature steamunder pressure, porous items such astowels, gowns and dressings, and alsomedical devices that are wrapped inporous materials such as paper orfabrics.
Potable waterWater of suitable quality for drinking,cooking or food production.
Reusable deviceA medical device which can bereprocessed for repeated episodes ofuse.
Single useA medical device that is intended to beused on an individual patient during asingle procedure and then discarded. It isnot intended to be reprocessed and usedon another patient.
Sterile Condition of a load item that is free fromviable micro-organisms. BS EN 556-1:2001 details the requirements for amedical device to be designated assterile.
Sterilization cycleAutomatic sequence of operating stagesperformed in a sterilizer for the purposeof sterilization.
Sterilization process The complete set of procedures requiredfor sterilization of a load, including theoperating cycle and any treatment of theload before or after the operating cycle.
46
Sterilization temperature Minimum temperature of the sterilizationtemperature band.
Sterilization temperature bands The range of temperatures that mayprevail throughout the load during theholding time. These temperatures areexpressed as a minimum acceptable (thesterilization temperature) and a maximumallowable, and are stated to the nearestdegree Celsius.
Sterilizer An apparatus designed to achievesterilization.
Type B (sterilization cycle)Intended to process porous loads e.g.wrapped instruments and fabrics.
Type S (sterilization cycle)Designed to process air-retentive loadse.g. tubular devices, as specified by thesterilizer manufacturer.
Validation A documented procedure for obtaining,recording and interpreting data requiredto show that a sterilization process wouldconsistently comply with predeterminedspecifications.
Washer-disinfectorAutomated machine intended to cleanand disinfect medical devices. Alsoknown as an automated endoscopereprocessor when dedicated toendoscope decontamination.
47
Our thanks to the following people for their contribution to the writing of this guide:
Mrs G. Sills – Chairman of International Federation for Sterile Supply's
Miss K. Woodhead – Past Chair of National Association of Theatre Nurses
Mrs P. Oliver – Past Director of Education Institute of Sterile Services Managers
Miss S. Meredith – Director of Education Institute of Sterile Services Managers
Mrs A. Fuller – Control of Infection Nurses Association
Mrs L. Davies – Senior Consultant for Decontamination
Mrs S. Morgan – Chairman of Infection Control Nurses Association
48
Acknowledgements
Top Related