




Languages
Pages
Legal

8/2/2019 235 Sen Banjo
1/25
1
INFLUENCE OF SOCIO-ECONOMIC FACTORS ON NUTRITIONAL STATUS
OF CHILDREN IN A RURAL COMMUNITY OF OSUN STATE, NIGERIA
*Senbanjo IO (FWACP), **Adeodu OO (FWACP), ***Adejuyigbe EA (FMCPaed)
* Senior registrar, Department of Paediatrics & Child Health, Obafemi Awolowo
University Teaching Hospitals Complex, Ile-Ife, Osun State, Nigeria.
** Associate professor, Department of Paediatrics & Child Health, Obafemi Awolowo
University Teaching Hospitals Complex, Ile-Ife, Osun State, Nigeria.
*** Senior lecturer, Department of Paediatrics & Child Health, Obafemi Awolowo
University Teaching Hospitals Complex, Ile-Ife, Osun State, Nigeria
8/2/2019 235 Sen Banjo
2/25
2
ABSTRACT
Protein energy malnutrition (PEM) remains a major public health problem in
Nigeria to such extent that it is the second most common cause of childhood morbidity
and mortality. This was a questionnaire-based, cross sectional survey which relied on
anthropometry to assess the nutritional status of children aged one year to five years. It
was conducted using the multistage cluster sampling technique in Ifewara, a rural
community in Osun State, about 200 kilometers from Lagos, Nigeria in order to
determine the prevalence and types of malnutrition and the associated socio-economic
determinants in the population. A total of 420 children were recruited from 344
households.
By the modified Wellcome Classification, the prevalence of PEM was 20.5 percent, and
using the World Health Organization/ National Centre for Health Statistics (WHO/
NCHS) cut off points, the prevalence rates of underweight, wasting and stunting were
23.1 percent, 9 percent and 26.7 percent respectively. One hundred and twelve (26.7
percent) children had borderline malnutrition. However, severe forms of PEM were not
common. Only 4 (1 percent) children had marasmus while there were no cases of
kwashiorkor or marasmic-kwashiorkor. Of the 348 mothers, 336 (96.6 %) had secondary
education at best while 12 (3.4 %) had post secondary. The prevalence rate of
underweight children was three times as high in the former as in the later group. Also,
children of mothers who were not educated beyond secondary school level had one and a
half to two times the prevalence rate of stunting. On the other hand, children of mothers
with post secondary education were apparently more often affected by wasting than those
with less educated mothers. However, no statistically significant difference was found in
8/2/2019 235 Sen Banjo
3/25
3
all these comparisons (2
= 2.38, p = 0.667; 2
= 1.9, p = 0.754 and2
= 2.38, p = 0.666
respectively). Of the 344 fathers, 25 (7.3 %) were educated beyond secondary school
level. The others (92.7 %) had at least secondary school education at best. There was a
subtle inverse relationship between fathers educational qualification and prevalence of
underweight but the differences were not statistically significant (p = 0.568). There was
no consistent trend in the pattern of wasting or stunting with respect to paternal
educational level. Low maternal income and overcrowding were associated with higher
prevalence of wasting (2
= 4.63, p = 0.031 and 2
= 4.79, p = 0.029 respectively). No
association was found between the source of drinking water or social class and
malnutrition.
It is concluded from this study that PEM is a major childhood public health hazard in
Ifewara and the local government authorities need to plan and implement effective child
health promotion. However, the prevalence of PEM in Ifewara is low when compared
with reports from other parts of Nigeria and this has been ascribed to the availability of
social amenities and access to basic medical careprovided by a comprehensive health
centre and a Non Governmental Organization. To this end, it is recommended that
governments should support and collaborate with Non Governmental Agencies in the
provision of health care needs to the people. Empowerment of mothers with the aim of
augmenting family income and parental education on the need to limit family size may
also be key measures in reducing the incidence and expectedly mitigate the effect of PEM
among the children of this rural community.
8/2/2019 235 Sen Banjo
4/25
4
INTRODUCTION
Malnutrition has for a long time been recognized as a consequence ofpoverty
since most of the worlds malnourished children live in the developing nations of Asia,
Africa and Latin America where those mostly affected are from low income families.1It
is conceivable that most of the resources of these developing countries are spent servicing
external debts at the expense of health and other social welfare services. The heavy
depletion of state funds by corrupt political leaders as well as the ravaging effects of wars
and strife result in economic instability and low purchasing power of the currencies.2
This
translates to low standard of living of the people.2
Therefore, this study, aimed at determining the current nutritional status of under-
five children in a rural Nigerian community and the socio economic determinants can be
used to canvass for nutrition surveillance and appropriate nutritional intervention
programme particularly in a times of depressed economy.
8/2/2019 235 Sen Banjo
5/25
5
SUBJECTS AND METHODS
The study was carried out in Ifewara, a rural community located in Atakunmosa
West Local Government Area, of Osun State, south-western Nigeria. Ifewara with the
estimated population of 3, 927 and household count of 1,849 is located 18 kilometers
from Osu, the headquarters of the local government area, 36 kilometers from Osogbo, the
capital of Osun State and 200 kilomaters from Lagos, a former federal capital city.3, 4
The multistage cluster and random sampling techniques were used to select
households and subjects. All under-five children in the entire households of the selected
houses were studied. For the purpose of this study, the housing system was classified into
flats or self contained apartments and individual rooms. A flat/self contained apartment
refers to residence whereby a family is able to carry out some of its major functions
without sharing with another family while individual room refers to sleeping room.
In each household, information was obtained on demographic, socio-economic and
environmental characteristics and the families were assigned a socio-economic class
using the method recommended by Oyedeji.5
The anthropometric parameters of every
child were recorded and each child was clinically examined for gross evidences of
malnutrition. Standardization checks on the tools for anthropometric measurements were
done periodically. Children with evidences of chronic diseases were excluded.
Malnutrition was diagnosed clinically using the modified Wellcome System of
Classification.6
The National Centre for Health Statistics/World Health Organization
(NCHS/WHO) guidelines and cut off points7, 8, 9, 10
were also used to determine the
degree of stunting, underweight and wasting. Underweight, wasting and stunting were
8/2/2019 235 Sen Banjo
6/25
6
diagnosed when the Weight-for-Age (WA), Weight-for-Height (WH) and Height-for-Age
(HA) were equal to minus two Standard Deviation (-2 SD) or below the mean of this
reference international standards respectively.7
Using the Mid Arm Circumference
(MAC), the subjects with values less than 12.5cm, between 12.5cm and 13.5cm and
above 13.5cm were deemed to have severe malnutrition, borderline malnutrition and
normal nutritional status respectively as suggested by Shakir.10
Data analysis was done using the Epi info 2002 and the SPSS for windows version 11
softwares.11, 12 Personal and family data were separately analyzed to avoid data
duplication. Proportions and rates were compared using the Pearson Chi squared (2
) test.
p values less than 0.05 were accepted as statistically significant.
8/2/2019 235 Sen Banjo
7/25
7
RESULTS
Demography
A total of 420 children were studied from 344 households consisting of 348
mothers and 344 fathers. The mean age of the study population was 35.4 + 14 months.
There were 218 (51.9 %) females and 202 (48.1 %) males giving a female: male ratio of
1.1: 1. The means ( SD) of the weight-for-age Z-scores (WAZ), height-for-age Z-scores
(HAZ) and weight-for-height Z-scores (WHZ) were -1.25 + 1.36, - 1.30 + 1.30 and
0.402 + 1.12 respectively. The prevalence of underweight, wasting and stunting are 23.1
%, 9.0 % and 26.7 % respectively (Table II).
Socioeconomic Characteristics of Parents and Nutritional Status
Tables III and IV shows the level of education of the parents in relation to the
nutritional status of their children. Of the 348 mothers, 336 (96.6 %) had secondary
education at best while 12 (3.4 %) had post secondary education. Underweight and
stunting were more common among the former than the latter while wasting was found
more among the latter. These differences, however, lack statistical significance.
Of the 344 fathers, 319 (92.7%) had at most secondary education while 25 (7.3
%) were educated beyond secondary school level. There was no consistent trend in the
pattern of wasting or stunting with respect to paternal educational level but there was a
non- significant relationship between fathers educational qualification and prevalence of
underweight.
The earning power of fathers and mothers are as shown in Tables V and VI. One
hundred and ninety-nine (57.8 %) fathers earned more than ten thousand naira per month
compared to 178 (51.1 %) mothers. The nutritional status of children of fathers that
8/2/2019 235 Sen Banjo
8/25
8
earned more than ten thousand naira per month and those that earned less than ten
thousand naira per month was similar. While underweight and stunting were common in
both groups of mothers, wasting was more significantly associated with mothers who
earn less than ten thousand naira. (2= 4.63, p = 0.031).
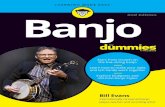
None of the children studied belonged to the social class I. In classes II, III, IV and
V were 3 (0.87 %), 86 (25 %), 245 (71.2 %) and 10 (2.91 %) children respectively. There
was no significant relationship between the prevalence of underweight (p = 0.826),
wasting (p = 0.537) and stunting (0.484) and the social classes to which the parents
belonged (Figure 1).
Housing and Nutritional Status
Fourteen (4.1 %) households occupied flats and self contained apartments, 35 (10.2 %)
lived in houses with at least 4 rooms, 38 (11 %) lived in houses with 3 rooms, 154 (44.8
%) occupied 2 rooms and 103 (29.9 %) families occupied only one room each (Table
VII). The nutritional status as measured by the degree of underweight, wasting and
stunting showed a correlation with the types of houses occupied although without
statistical significant. Underweight (2
= 5.93, p = 0.313), wasting (2
= 3.57, p = 0.614)
and stunting (2
= 4.78, p = 0.443). Two hundred and fifty-three (73.5 %) children lived
in rooms with less than four people while 91 (26.5 %) lived in rooms with more than 4
people (Table VIII). There was a significantly higher prevalence of wasting among
children with more than four occupants per room (2
= 4.79, p = 0.029). The prevalence
rates of underweight and stunting were comparable in the two groups ((2
= 0.76, p =
0.385 and 2= 0.027, p = 0.868 respectively).
8/2/2019 235 Sen Banjo
9/25
9
Source of Drinking Water and Nutritional Status
The major sources of water supply were stream 256 (74.4 %), well 55 (16 %) and
rain water 11(3.2 %). Twenty-two (6.4 %) households used packaged water either in
satchets or bottles. None of the households used pipe borne water (Table IX). There was
no significant relationship between the prevalence of underweight (p = 0.568), wasting (p
= 0.575 and stunting (p = 0.37) and their sources of water supply.
8/2/2019 235 Sen Banjo
10/25
10
DISCUSSION
Most of the parents in this rural Nigerian community had at least primary education
in contrast to the literacy level of 56 % and 72 % reported in 2000 for female and male
Nigerians respectively.7
There exist a direct relationship between educational
qualification of mothers and the nutritional status of their wards similar to previous
reports13-15
It is expected that the more educated a mother is, the more likely she is to be
receptive to developmental initiatives such as the Childhood Survival Strategies. This has
the resultant effect of improved family nutrition and less risk of childhood malnutrition.
16
The majority of the mothers in Ifewara were traders while the fathers were mainly
farmers. This is as expected of a rural Nigerian community. Therefore, the lack of
relationship between parental occupation and the nutritional status of children may be
attributed to the fact that most of families belonged to about the same socioeconomic
class.
Although many factors are involved in the development of PEM, it is believed that
poverty at the family level is the principal cause of childhood malnutrition. The average
monthly income of fathers in this study is higher than the national minimum monthly
payable wage of ten thousand naira (about seventy dollars). The empirical position is that
a womans earnings will more likely be spent on family feeding than the husbands
income. This is contrary to the belief that the earning power of father rather than that of
the mother determines the finances of the family and is directly related to the nutritional
status of children.17
The implication of this finding is that if empowered economically,
8/2/2019 235 Sen Banjo
11/25
11
women could supplement the finances of the households and help in reducing the
prevalence of PEM.
The provision of adequate and proper housing is essential for the normal growth
and development of a child. In Nigeria, the population growth rate is very high (2.88%)
compared with that of the developed world where population growth rate is almost static
at 0.6%.18
The high population growth rate leads to overcrowding if adequate number of
housing is not provided for the citizens. The consequence of overcrowding is the spread
of diseases like Acute Respiratory Infection (ARI) and diarrhoea which are known causes
of malnutrition. The lack of any relationship between the type of housing and the
prevalence of malnutrition in this study may reflect the generally poor construction
standard of most of the houses since the socioeconomic status of the families is not
significantly different. However, the association of wasting with the number of occupants
of a room is similar to the finding in Lagos where it was ascribed to rapid urbanization.13
Malnutrition may also be associated with overcrowding not just because of the
transmission of infections but also because food sharing may be unfavorable to the
younger ones.
The provision of adequate, safe and clean water is a component of Primary Health
Care. Today, only a few Nigerians have access to this. In rural Nigeria, only 49 % of the
population use improved quality potable water compared with 78 % for the urban.18
The
situation is not different in Ifewara where the major source of drinkable water is the
stream as the entire community has no pipe borne water supply. The apparent lack of
association between source of water and poor childhood nutrition in this study may be
ascribed to the probability that the children in this community have developed antibodies
8/2/2019 235 Sen Banjo
12/25
12
to the various organisms contaminating the water they consume thereby leading to
reduction in their susceptibility to water borne diseases like diarrhoea which could
predispose to malnutrition.
The findings in this study have confirmed many issues about the risk factors for
childhood malnutrition which have been known for decades. It is remarkable that almost
halfway into the 21st
century, the same factors still abound. This calls the impact of the
various intervention programmes used in this wise in the past to question and demands a
reverberated approach. Women empowerment promises improved family finances, better
food security and better childhood nutrition. This is worth trying in the developing world.
8/2/2019 235 Sen Banjo
13/25
13
REFERENCES
1. UNICEF. Malnutrition: causes, consequences and solution. The state of the worldschildren 1998.
2. Osibogun A. The epidemiology of undernutrition. In: Osibogun A (Ed) Ahandbook of public health nutrition for developing countries Miral press first
edition, 1998: 13-30.
3. Microsoft Encarta Reference Library Software. Microsoft Corporation, 2002.4.
National Population Commission. Final result of 1991 population census of Nigeria.
5. Oyedeji GA. Socioeconomic and cultural background of hospitalized children inIlesa. Nig J Paediatr 1985; 12 (4): 111 117.
6. Hendrickse RG. Protein energy malnutrition. In: Hendrickse RG, Barr DGD,Mathews TS (Eds.) Paediatrics in the tropics. Blackwell scientific publications first
edition, 1991: 119-131.
7. UNICEF. The state of the world children 2003.8. Binns CW. Assessment of growth and nutritional status. J Food Nutr. 1985;
42(3):119-125.
9. WHO. Use and interpretation of anthropometric indicators of nutritional status.Bull World Health Organ.1986; 64: 929-941.
10.World Health Organisation (1998). Management of severe malnutrition; a manualfor physician and other senior health workers.
11.WHO/Centers for Disease Control and Prevention. Epi Info 2002.12.SPSS for windows. Release 11.0.0 SPSS Inc Standard Version 2001.
8/2/2019 235 Sen Banjo
14/25
14
13.Abidoye RO, Ihebuzor NN. Assessment of nutritional status using anthropometricmethods on 1-4 year old children in an urban ghetto in Lagos, Nigeria. Nutr Health
2001; 15(1): 29-39.
14.Abidoye RO, Sikabofori. A study of the prevalence of protein energy malnutritionamong 0-5 years in rural Benue state, Nigeria. Nutr Health 2000; 13(4):235-47.
15.Esimai OA, Ojofeitimi EO, Oyebowale OM. Sociocultural practices influencingunder five nutritional status in an urban community in Osun State, Nigeria. Nutr
Health 2001; 15(1): 41-46.
16.UNICEF. Female education. The state of the world children 2000.
17.Ighogboja SI. Some factors contributing to protein energy malnutrition in themiddle belt of Nigeria. East Afr Med J 1992; 69(10): 566-71.
18.Rao S, Kanade AN. Prolonged breast feeding and malnutrition among rural Indianchildren below 3 years of age. Eur J Clin Nutr. 1992; 46 (3): 187 195.
8/2/2019 235 Sen Banjo
15/25
15
TABLES
Table I: Epidemiological features of the 420 children study.
Parameters No of children Percentage
1. Age (months)
12-23 105 25
24-35 94 22.4
36-47 120 28.6
48-60 101 24
2. Sex
Male 202 48.1
Female 218 51.9
3. Religion
Christianity 290 84.3
Islam 54 15.7
4. Ethnic groups
Yoruba 289 84
Non-Yoruba 55 16
8/2/2019 235 Sen Banjo
16/25
16
Table II: Nutritional status of the study population using the Weight-for-Age Z-
score (WAZ), Height-for-age Z- scores (HAZ) and Weight-for-Height Z-
score
Nutritional status WAZ HAZ WHZ
Normal (> - 2.00 SD) 323 (76.9) 308 (73.3) 382 (91.0)
Malnourished (- 2.00 to - 2.99 SD) 65 (15.5) 78 (18.6) 29 (6.9)
Severely Malnourished (-3.00 SD and above) 32 (7.6) 34 (8.1) 9 (2.1)
Total 420 (100.0) 420(100.0) 420(100.0)
Key: Figures in parenthesis are percentages of the total in the respective column.
8/2/2019 235 Sen Banjo
17/25
17
Table III: Nutritional status in relation to level of education of mothers.
Nutritional status
Educational status> - 2 SD - 2 SD and below
Total
No formal education
WAZ
WHZ
HAZ
20 (74.1)
24 (88.9)
19 (70.4)
7 (25.9)
3 (11.1)
8 (28.6)
27 (100)
Primary
WAZ
WHZ
HAZ
96 (75.6)
113 (89)
97 (76.4)
31 (24.4)
14 (11)
30 (23.6)
127 (100)
Secondary
WAZ
WHZ
HAZ
138 (75.8)
168 (92.3)
129 (70.9)
44 (24.2)
14 (7.7)
53 (29.1)
182 (100)
Post Secondary
WAZ
WHZ
HAZ
11 (91.7)
10 ( 83.3)
10 (83.3)
1 (8.3)
2 (16.7)
2 (16.7)
12 (100)
Key: Figures in parenthesis are percentages of the total in the respective row.
WAZ - 2
= 2.38, (df) = 3, p = 0.667.
WHZ - 2
= 2.38, (df) = 3, p = 0.666.
HAZ - 2
= 1.9, (df) = 3, p = 0.754.
8/2/2019 235 Sen Banjo
18/25
18
Table IV: Nutritional status in relation to level of education of fathersNutritional status
Educational status> - 2 SD - 2 SD and below
Total
No formal education
WAZ
WHZ
HAZ
19 (70.4)
23 (85.2)
21 (77.8)
8 (29.6)
4 (14.8)
6 (22.2)
27 (100)
Primary
WAZ
WHZ
HAZ
63 (73.3)
79 (91.9)
57 (66.3)
23 (26.7)
7 (8.1)
29 (33.7)
86 (100)
Secondary
WAZ
WHZ
HAZ
158 (76.7)
186 (90.3)
154 (74.8)
48 (23.3)
20 (9.7)
52 (21.2)
206 (100)
Post Secondary
WAZ
WHZ
HAZ
21 (84)
23 (92)
19 (76)
4 (16)
2 (8.0)
6 (24.0)
25 (100)
Key: Figures in parenthesis are percentages of the total in the respective row.
WAZ - 2
= 2.94, (df) = 3, p = 0.568.
WHZ - 2
= 1.88, (df) = 3, p = 0.757.
HAZ - 2
= 2.87, (df) = 3, p = 0.579.
8/2/2019 235 Sen Banjo
19/25
19
Table V: Nutritional status in relation to fathers monthly income.
Nutritional status
Monthly income (Naira)> - 2 SD - 2 SD and below
Total
< Ten thousand
WAZ
WHZ
HAZ
110 (75.9)
127 (87.6)
108 (74.5)
35 (24.1)
18 (12.4)
37 (25.5)
145 (100)
> Ten thousand
WAZ
WHZ
HAZ
151 (75.9)
184 (92.5)
143 (71.9)
48 (24.1)
15 (7.5)
56 (28.1)
199 (100)
Key: Figures in parenthesis are percentages of the total in the respective row.
WAZ - 2
= 0.0, (df) = 1, p = 0.997.
WHZ - 2
= 2.3, (df) = 1, p = 0.129.
HAZ - 2 = 0.29, (df) = 1, p = 0.589.
8/2/2019 235 Sen Banjo
20/25
20
Table VI: Nutritional status in relation to mothers monthly income.
Nutritional status
Monthly income (Naira)> - 2 SD - 2 SD and below
Total
< Ten thousand
WAZ
WHZ
HAZ
128 (75.3)
148 (87.1)
128 (75.3)
42 (24.7)
22 (12.9)
42 (24.7)
170 (100)
> Ten thousand
WAZ
WHZ
HAZ
137 (77)
167 (93.8)
127 (71.3)
41 (23.0)
11 (6.2)
51 (28.7)
178 (100)
Key: Figures in parenthesis are percentages of the total in the respective row.
WAZ - 2
= 0.13. (df) = 1, p = 0.714.
WHZ - 2
= 4.63, (df) = 1, p = 0.031.
HAZ - 2
= 0.69, (df) = 1, p = 0.406.
8/2/2019 235 Sen Banjo
21/25
21
Table VII: Nutritional status in relation to type of house
Type of House
Nutritional status
> - 2 SD -2 SD and below Total
One room
Underweight
Wasting
Stunting
73 (70.9)
92 (89.3)
71 (68.9)
30 (29.1)
11 (10.7)
32 (31.1)
103(100)
2 rooms
Underweight
Wasting
Stunting
115 (74.7)
131 (189)
111 (72.1)
39 (25.3)
17 (11)
43 (27.9)
154 (100)
3 rooms
Underweight
Wasting
Stunting
> 4 rooms
Underweight
Wasting
Stunting
Flat
Underweight
Wasting
Stunting
32 (84.2)
35 (92.1)
28 (73.7)
29 (82.9)
33 (94.3)
28 (80)
12 (85.7)
14 (100)
13 (92.9)
6 (15.8)
3 (7.9)
10 26.3)
6 (17.1)
2 (5.7)
7 (20)
2 (14.3)
- (0)
1 (7.1)
38(100)
35 (100)
14 (100)
Key: Figures in parenthesis are percentages of the total in the respective row.WAZ -
2= 5.93, (df) = 4, p = 0.313.
WHZ - 2= 3.57, (df) = 4, p = 0.614.
HAZ - 2= 4.78, (df) = 4, p = 0.443.
8/2/2019 235 Sen Banjo
22/25
22
Table VIII: Nutritional status and number of persons living in a room
Number of person Nutritional status
> - 2 SD -2 SD and below Total
Less than 4
Underweight
Wasting
Stunting
195 (77.1)
234 (92.5)
184 (72.71)
58(22.9)
19 (7.5)
69 (27.3)
253 (100)
More than 4
Underweight
Wasting
Stunting
66 (72.5)
77 (84F.6)
67 (73.6)
25 (27.5)
14 (15.4)
24(26.4)
91 (100)
Key: Figures in parenthesis are percentages of the total in the respective row.
WAZ - 2
= 0.76, (df) = 1, p = 0.385
WHZ - 2
= 4.79, (df) = 1, p = 0.029
HAZ - 2
= 0.027, (df) = 1, p = 0.868.
8/2/2019 235 Sen Banjo
23/25
23
Table IX: Nutrition status in relation to source of drinking water.
Nutritional status
Source of Water > - 2 SD -2 SD and below Total
Well
WAZ
WHZ
HAZ
43 (78.2)
48 (87.3)
43 (78.2)
12 (21.8)
7 (12.7)
12 (21.8)
55 (100)
Rain Water
WAZ
WHZ
HAZ
10 (90.9)
11 (100)
9 (81.8)
1 (9.1)
- (0.0)
2 (18.2)
11 (100)
Stream
WAZ
WHZ
HAZ
192 (75)
231 (90.2)
180 (70.3)
64 (25.0)
25 (9.8)
76 (29.7)
256 (100)
Others
WAZ
WHZ
HAZ
16 (72.7)
21 (95.5)
19 (84.4)
6 (27.3)
1 (4.5)
3 (13.6)
22 (100)
Key: Figures in parenthesis are percentages of the total in the respective row.
WAZ - 2
= 2.94, (df) = 4, p = 0.568.
WHZ - 2
= 3.26, (df) = 4, p = 0.575.
HAZ - 2
= 4.28, (df) = 4, p = 0.37.
8/2/2019 235 Sen Banjo
24/25
24
0
5
10
15
20
25
1 2 3 4 5
Social class
Prevalence(%)
Underweight Wasting Stunting
Figure 1: Nutritional status of Children in relation to social class of parents.
8/2/2019 235 Sen Banjo
25/25
25
Correspondence to:
Dr. Senbanjo I.O,
Department of Paediatrics & Child Health,
Obafemi Awolowo University Teaching Hospitals Complex,
Ile-Ife, Osun State,Nigeria.
E-mail: [email protected]
Top Related