






Languages
Pages
Legal


201PR Natio
14 NRACT
onal Reg
NATITICE
gistry o
IONE AN
f EMTs
NAL NAL
s
EMLYS
MS IS

2014 National EMS Practice Analysis National Registry of Emergency Medical Technicians (NREMT®)
Mission Statement To serve as the National EMS Certification organization by providing a valid, uniform process to assess the knowledge and skills required for competent practice by EMS professionals throughout their careers and by maintaining a registry of certification status. Copyright ©2015 by the National Registry of Emergency Medical Technicians (NREMT®), Rocco V. Morando Building, 6610 Busch Blvd, Columbus, Ohio 43229 COPYRIGHT WARNING: All rights reserved. This document is protected by Copyright laws of the United States of America. This document may not be used, reproduced or disseminated to any third party without written permission from NREMT. Violators will be subject to prosecution and other actions. NREMR®, NREMT®, NRAEMT® and NRP® are registered trademarks of NREMT. Address inquires in writing to NREMT Research Department, 6610 Busch Blvd, Columbus, Ohio 43229. Suggested Citation: National Registry of Emergency Medical Technicians (2015). 2014 National EMS Practice Analysis. Columbus, Ohio. Printed in the United States of America. ISBN: 978-0-9962885-0-7

Table of Contents
EXECUTIVE SUMMARY ............................................................................................................ 1 Data Collection......................................................................................................................................... 3 Data Analysis ............................................................................................................................................ 3 Representativeness of the Sample ............................................................................................................. 3 Test Plan Development ............................................................................................................................. 3
BACKGROUND OF STUDY ........................................................................................................ 5
METHODOLOGY ......................................................................................................................... 6 Study Population....................................................................................................................................... 6 Population Setting .................................................................................................................................... 6 Study Design ............................................................................................................................................. 7 Survey Development ................................................................................................................................. 7 Sampling Plan ........................................................................................................................................ 10 Data Collection....................................................................................................................................... 10 Data Analysis .......................................................................................................................................... 11
RESULTS ..................................................................................................................................... 11 Representativeness of the Sample ........................................................................................................... 11 Test Plan Development ........................................................................................................................... 12
Appendix A ................................................................................................................................... 13
Appendix B ................................................................................................................................... 14
Appendix C ................................................................................................................................... 26
Appendix D ................................................................................................................................... 28
©2015 by the National Registry of EMTs Page 1
EXECUTIVE SUMMARY The mission of the National Registry of Emergency Medical Technicians (NREMT) is to serve as the National EMS Certification organization by providing a valid, uniform process to assess the knowledge and skills required for competent practice by EMS professionals throughout their careers and by maintaining a registry of certification status. To help ensure a legally defensible and psychometrically sound credentialing process, it is necessary to understand current practice in the out-of-hospital setting. Thus, the primary objective of the 2014 National EMS Practice Analysis was to identify the frequency, potential of harm, and impact of tasks performed by cohorts of nationally representative Emergency Medical Responders, Emergency Medical Technicians, Advanced Emergency Medical Technicians and Paramedics. The results of the current study will inform the examination blueprint and item development for each of the NREMT certification examinations. Methodology Population setting The practice of out-of-hospital care involves applying and adapting concepts of emergency medicine to unique, unpredictable, dynamic, and potentially hazardous field environments. Therefore, to be a competent EMS practitioner, one must demonstrate competence in both patient care and operational knowledge and skills. Further, EMS providers are confronted with patients of all types and ages, some frequently and others infrequently; some critical and others not so critical. Importance, therefore, must account for both variables as some situations are frequent but not terribly critical (e.g., flu-like symptoms), while others are infrequent but very critical (e.g., pediatric respiratory arrest). Study design The National EMS Practice Analysis is a cross-sectional analysis of a stratified sample of randomly selected, nationally certified EMS professionals who are currently providing out-of-hospital care at all certified provider levels. The American Institutes for Research Institutional Review Board approved this study. Survey development The NREMT convened a committee of national subject matter EMS experts. Members of the Practice Analysis Committee are active in EMS as managers, physicians, educators, supervisors, and state-level regulators. All possess expertise and a different perspective on the street level practice of EMS at the four (4) levels of National EMS Certification.
©2015 by the National Registry of EMTs Page 2
Using previous practice analysis survey instruments as a conceptual and theoretical framework, the Committee updated the tasks that would cover the breadth of patient conditions (including the assessment and management of those patients), operational tasks, and intervention skills (including assessment tasks, medication administration, and patient care tasks) that are currently within the domain of EMS practice. The task list ultimately serves as the basis for cataloging content developed and delivered via the NREMT cognitive examinations. The list was intended to include the EMS tasks performed by Emergency Medical Responder, Emergency Medical Technician, Advanced Emergency Medical Technician and Paramedic levels. By modifying previous survey items, the Committee identified thirty-three (33) adult and thirty-three (33) pediatric patient presentations that all EMS providers must assess and manage. Further, nine (9) categories of EMS Operations Tasks were identified. A total of seventy-five (75) tasks were included in each survey at all levels. Due to the variations in scopes of practice between the four (4) levels, the Committee developed separate task lists for assessment, patient care, medication administration, operations, and items related to community EMS for each provider level. Data related to the assessment, patient care, medication administration, operations, and community EMS tasks were collected for research purposes and are not intended to influence the NREMT cognitive test plan. After completion of task lists for each of the respective national EMS provider levels, the Committee deliberated on the dimensions necessary to determine the importance of a task. The Committee determined that importance would be a function of both the frequency that a task is performed and the criticality of the task. Data for ten (10) demographic and work-life characteristics were also collected. These data would enable to the Committee to determine if any response bias or under/over-representation of any provider characteristics exists in the respondents. It also enabled the Committee to determine if the sample was representative of all nationally certified EMS professionals. Following Committee development of the surveys, the draft survey instruments were cognitively tested. Drafts were administered to individuals ensuring geographic, ethnic, gender, and provider-level diversity. A standard debriefing protocol was followed. Sampling plan The population of interest for this study consisted of non-military, nationally certified EMS professionals at all levels of National EMS Certification. At the time of data collection, there were approximately 202,898 civilian nationally certified EMS professionals. The proportion of minorities who held National EMS Certification had not changed appreciably since 2009. Sampling was conducted using a random selection method stratified by minority status for all four (4) levels of certification. In an effort to achieve sufficient minority representation, the same oversampling strategy was employed for the 2014 sample that was used successfully in the 2009 practice analysis. Further, to determine reasonable estimates at a 95% confidence level and an acceptable 5% margin of error for categorical data, power calculations were performed.

©2015 by the National Registry of EMTs Page 3
Data Collection To incentivize individuals to participate, each randomly selected EMS provider was mailed a hand-signed letter explaining the study and its importance as well as a decal of their respective certification level. Individuals then received an email two (2) weeks later that highlighted the importance of the practice analysis and provided an individual’s URL link to the electronic survey. Those individuals who did not respond received a reminder e-mail stressing the importance of the study each week for a total of three weeks. Each electronic survey had a unique identifier that linked the results to an individual. The logs were kept confidential from the Committee and were only used to send reminder emails to those who had not participated. No specific individual responses were identified.
Data Analysis One of the major goals of the practice analysis is to determine the relative importance of job-related activities performed by EMS providers. The Practice Analysis Committee determined that the importance of each task performed by EMS professionals is a function of the frequency that a task is performed and the potential of harm related to that task. Using an additive model for combining scales, a Weighted Importance Score (WIS) formula consisting of 1/3 weight calculated for frequency and 2/3 weight calculated for potential for harm was utilized for each task.
Results
Representativeness of the Sample The Practice Analysis Committee reviewed the demographics of individuals who responded to the practice analysis survey. These data were compared to population data from the NREMT database and other research initiatives. The Committee determined that the responses in the present study were representative of the population of all levels of nationally certified EMS providers throughout the nation).
Test Plan Development The goal of the practice analysis is to determine the relative proportions for each of these relationships on each level of the NREMT examination based on the importance of tasks. To determine the balance of the exam, a relative weight for each domain was determined. The proportion of the examination related to patient care and operations was determined in evaluating the WIS of all patient care tasks as well as the EMS operations section. Responses for adult and pediatric patient care tasks were combined in each of the patient care content areas to determine the final representative proportion for each section in the final test plan (Appendix C).

©2015 by the National Registry of EMTs Page 4
Based on the examination lengths recommended by the NREMT Standards and Examination Committee and approved by the NREMT Board of Directors, the number of items for each section was determined by relative weight of the section, multiplied by the range of the total number of exam items in the currently approved examinations.
Following the Practice Analysis Committee’s review of data, outcome and drafted test plans, the NREMT Board of Directors adopted the four (4) test plans at the November 2014 Board of Directors meeting for implementation on September 1, 2015 (Appendix D).

©2015 by the National Registry of EMTs Page 5
BACKGROUND OF STUDY The goal of licensure and certification is to assure the public that individuals who work in a particular profession have met certain standards and are qualified to engage in practice (American Educational Research Association, American Psychological Association, and National Council on Measurement in Education, 1999). To meet this goal, the requirements for certification and licensure must be based on the ability to practice safely and effectively (Kane, 1982). The practice analysis is a component for developing a legally defensible and psychometrically sound credentialing process. The primary purpose of a practice analysis is to develop a clear and accurate picture of the current practice of a job or profession, in this case the provision of emergency medical care in the out-of-hospital environment. The results of the practice analysis are used throughout the entire National Registry of Emergency Medical Technicians (NREMT) examination development process, which helps to ensure a connection between the examination content and actual practice. The practice analysis helps to answer the questions, “What are the most important aspects of practice?” and “What constitutes safe and effective care?” It also enables the NREMT to develop examinations that reflect contemporary, real-life practice of out-of-hospital emergency medicine. As the nation’s EMS certification agency, the NREMT is obligated to develop certification materials that reflect entry-level competency for safe and effective practice of out-of-hospital providers. The National EMS Education Standards and the National EMS Practice Analysis help to determine the distribution of test material. Numerous sources are utilized to determine the depth and breadth of content contained in the national EMS Certification materials, including, but not limited to: the National EMS Education Standards, the National EMS Practice Analysis, the most current American Heart Association guidelines, recommendations from the Centers for Disease Control and Prevention on Trauma Triage, organizational position statements, current peer-reviewed literature, content of EMS textbooks, and the judgments of panels of experts periodically convened by the NREMT that represent the diversity of the national EMS community. The NREMT conducted its first practice analysis in 1994 and at five-year intervals thereafter (1994, 1999, 2004, 2009). The primary objective of this study, the 2014 National EMS Practice Analysis, was to identify the frequency, potential of harm, and impact of tasks performed by cohorts of nationally representative Emergency Medical Responders, Emergency Medical Technicians, Advanced Emergency Medical Technicians and Paramedics. The results of the current study will inform the examination blueprint and item development for each of the NREMT certification examinations.
©2015 by the National Registry of EMTs Page 6
METHODOLOGY
Study Population At the time of the present study, there were four (4) nationally defined levels of EMS providers based on the National EMS Scope of Practice and the National EMS Education Standards and Instructional Guidelines published in 2009 (Table 1). Table 1. Nationally Defined Levels of EMS Providers
National Certification Level Basis Emergency Medical Responder National EMS Scope of Practice Model Emergency Medical Technician National EMS Scope of Practice ModelAdvanced Emergency Medical Technician National EMS Scope of Practice ModelParamedic National EMS Scope of Practice Model
Population Setting The practice of out-of-hospital care involves applying and adapting concepts of emergency medicine to unique, unpredictable, dynamic, and potentially hazardous field environments. Therefore, to be a competent EMS practitioner, one must demonstrate competence in both patient care and operational knowledge and skills. EMS professionals encounter patients of all types and ages. Hence, patient care competence is the combined ability to apply an understanding of the pathophysiology of a patient’s presentation to the appropriate assessment and correct management of any patient, regardless of presenting complaint or age. While not all patients are easily categorized, there has been a natural tendency in EMS education to broadly divide patient presentations into four areas: 1) Airway, Respiration & Ventilation, 2) Cardiology & Resuscitation, 3) Trauma, and 4) Medical/Obstetrics/Gynecology. Historically, pediatrics has been considered a separate category, however, the EMS for Children National Resource Center has emphasized that most problems which occur in adults can also occur in pediatric patients. While modification of the approach may be necessary due to age considerations, pediatric content should be fully integrated into EMS education and practice rather than being treated as a separate aspect of EMS practice. Competence in patient care can be represented as demonstrating knowledge and skills in the four patient presentation categories for patients of all ages. EMS providers are confronted with a variety of patient types, some frequently and others infrequently; some critical and others not so critical.1 Importance, therefore, must account for both variables as some situations are frequent but not terribly critical (e.g., flu-like symptoms), while others are infrequent but very critical (e.g., pediatric respiratory arrest). 1 In defining criticality, we have chosen to analyze “Potential for harm.” We recognize that to the patient and his/her family, all situations are critical and it is not our intent to trivialize any patient complaint.
©2015 by the National Registry of EMTs Page 7
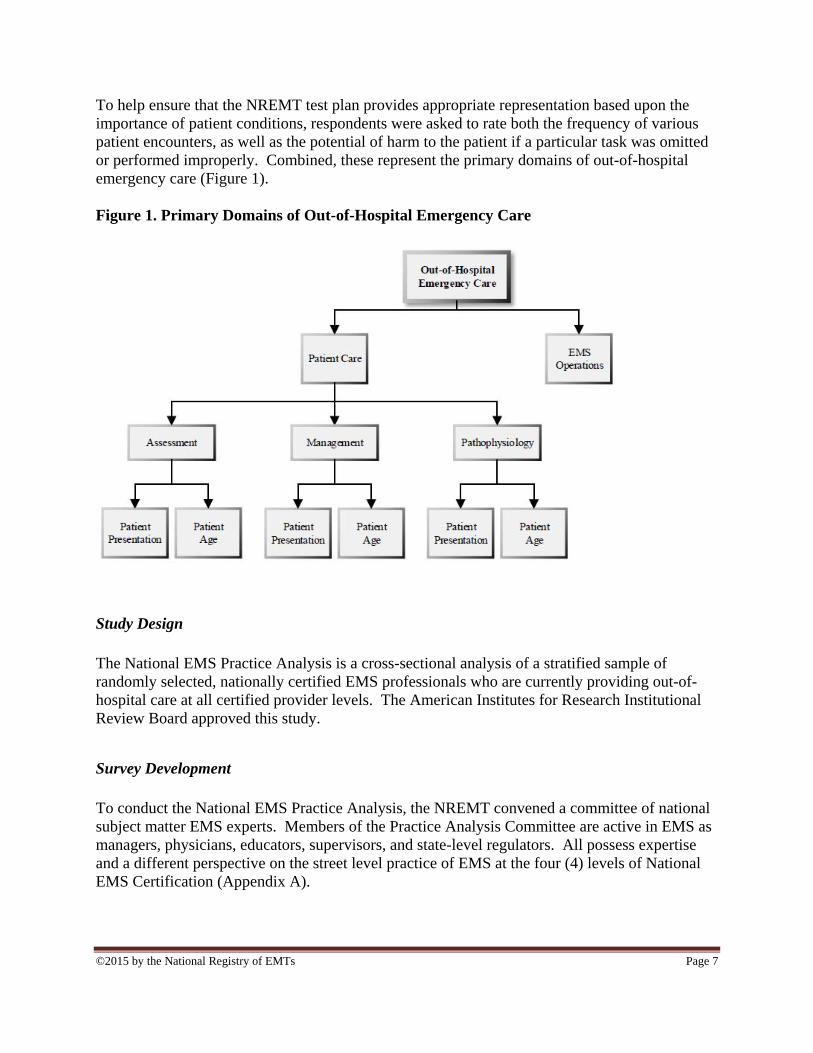
To help ensure that the NREMT test plan provides appropriate representation based upon the importance of patient conditions, respondents were asked to rate both the frequency of various patient encounters, as well as the potential of harm to the patient if a particular task was omitted or performed improperly. Combined, these represent the primary domains of out-of-hospital emergency care (Figure 1). Figure 1. Primary Domains of Out-of-Hospital Emergency Care
Study Design The National EMS Practice Analysis is a cross-sectional analysis of a stratified sample of randomly selected, nationally certified EMS professionals who are currently providing out-of-hospital care at all certified provider levels. The American Institutes for Research Institutional Review Board approved this study.
Survey Development To conduct the National EMS Practice Analysis, the NREMT convened a committee of national subject matter EMS experts. Members of the Practice Analysis Committee are active in EMS as managers, physicians, educators, supervisors, and state-level regulators. All possess expertise and a different perspective on the street level practice of EMS at the four (4) levels of National EMS Certification (Appendix A).
©2015 by the National Registry of EMTs Page 8
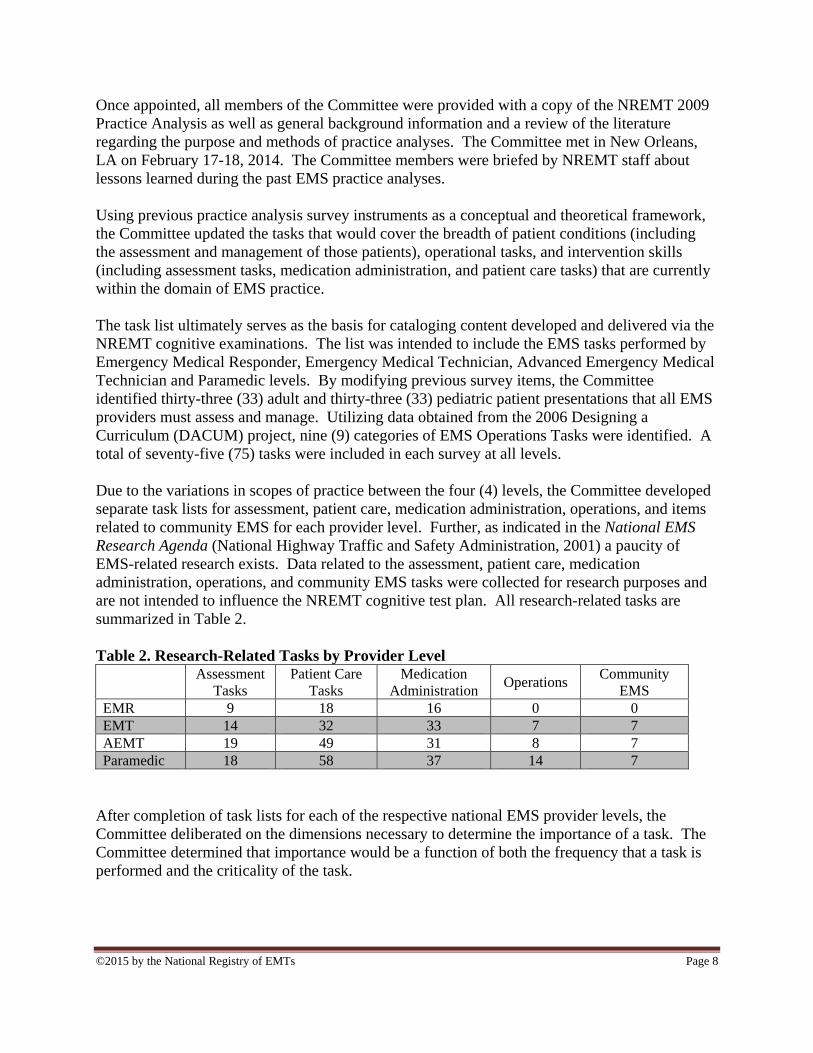
Once appointed, all members of the Committee were provided with a copy of the NREMT 2009 Practice Analysis as well as general background information and a review of the literature regarding the purpose and methods of practice analyses. The Committee met in New Orleans, LA on February 17-18, 2014. The Committee members were briefed by NREMT staff about lessons learned during the past EMS practice analyses. Using previous practice analysis survey instruments as a conceptual and theoretical framework, the Committee updated the tasks that would cover the breadth of patient conditions (including the assessment and management of those patients), operational tasks, and intervention skills (including assessment tasks, medication administration, and patient care tasks) that are currently within the domain of EMS practice. The task list ultimately serves as the basis for cataloging content developed and delivered via the NREMT cognitive examinations. The list was intended to include the EMS tasks performed by Emergency Medical Responder, Emergency Medical Technician, Advanced Emergency Medical Technician and Paramedic levels. By modifying previous survey items, the Committee identified thirty-three (33) adult and thirty-three (33) pediatric patient presentations that all EMS providers must assess and manage. Utilizing data obtained from the 2006 Designing a Curriculum (DACUM) project, nine (9) categories of EMS Operations Tasks were identified. A total of seventy-five (75) tasks were included in each survey at all levels. Due to the variations in scopes of practice between the four (4) levels, the Committee developed separate task lists for assessment, patient care, medication administration, operations, and items related to community EMS for each provider level. Further, as indicated in the National EMS Research Agenda (National Highway Traffic and Safety Administration, 2001) a paucity of EMS-related research exists. Data related to the assessment, patient care, medication administration, operations, and community EMS tasks were collected for research purposes and are not intended to influence the NREMT cognitive test plan. All research-related tasks are summarized in Table 2. Table 2. Research-Related Tasks by Provider Level Assessment
Tasks Patient Care
Tasks Medication
Administration Operations
Community EMS
EMR 9 18 16 0 0 EMT 14 32 33 7 7 AEMT 19 49 31 8 7 Paramedic 18 58 37 14 7
After completion of task lists for each of the respective national EMS provider levels, the Committee deliberated on the dimensions necessary to determine the importance of a task. The Committee determined that importance would be a function of both the frequency that a task is performed and the criticality of the task.
©2015 by the National Registry of EMTs Page 9
Based on survey methodology and EMS subject matter expertise, it was determined that each respondent would be asked, “How often do you encounter a patient with this condition?” with the following response categories in order to determine frequency:
Never Once per year or less Between once per year and once per month Between once per week and once per month More than once per week
The criticality for patient presentation types and assessment tasks was assessed by asking the respondents, “What is the potential for harm to the patient if you do not provide proper care?” using the following response categories:
Little to no potential for harm Moderate potential for harm Significant potential for harm Extreme potential for harm
The criticality of EMS Operations tasks was determined by a slight modification of the leading question, “What is the potential for harm to you, your partner, the patient, or bystanders if you omit or improperly perform each of the following?” utilizing the following response categories:
Little to no potential for harm Moderate potential for harm Significant potential for harm Extreme potential for harm
For assessment tasks, patient care tasks, routes of medication administration, medication administration tasks and community EMS tasks, an “I am not authorized to perform this task” option was added to the frequency response options. The potential for harm category was replaced by an assessment of the “impact” that interventions have on patient outcome. Specifically, participants were asked to respond to the question, “If you performed this task properly, what effect would it have on the patient while under your care?” with the following response options:
Worsen No impact Prevent deterioration Improvement Life-saving
©2015 by the National Registry of EMTs Page 10
Data for ten (10) demographic and work-life characteristics were also collected. These data would enable to the Committee to determine if any response bias or under/over-representation of any provider characteristics exists in the respondents. It also enabled the Committee to determine if the sample was representative of all nationally certified EMS professionals. Following Committee development of the surveys, the draft survey instruments were cognitively tested. Drafts were administered to individuals ensuring geographic, ethnic, gender, and provider-level diversity. A standard debriefing protocol was followed. Following revisions based on the results of the cognitive debriefing, all Committee members approved the final drafts for the four (4) surveys.
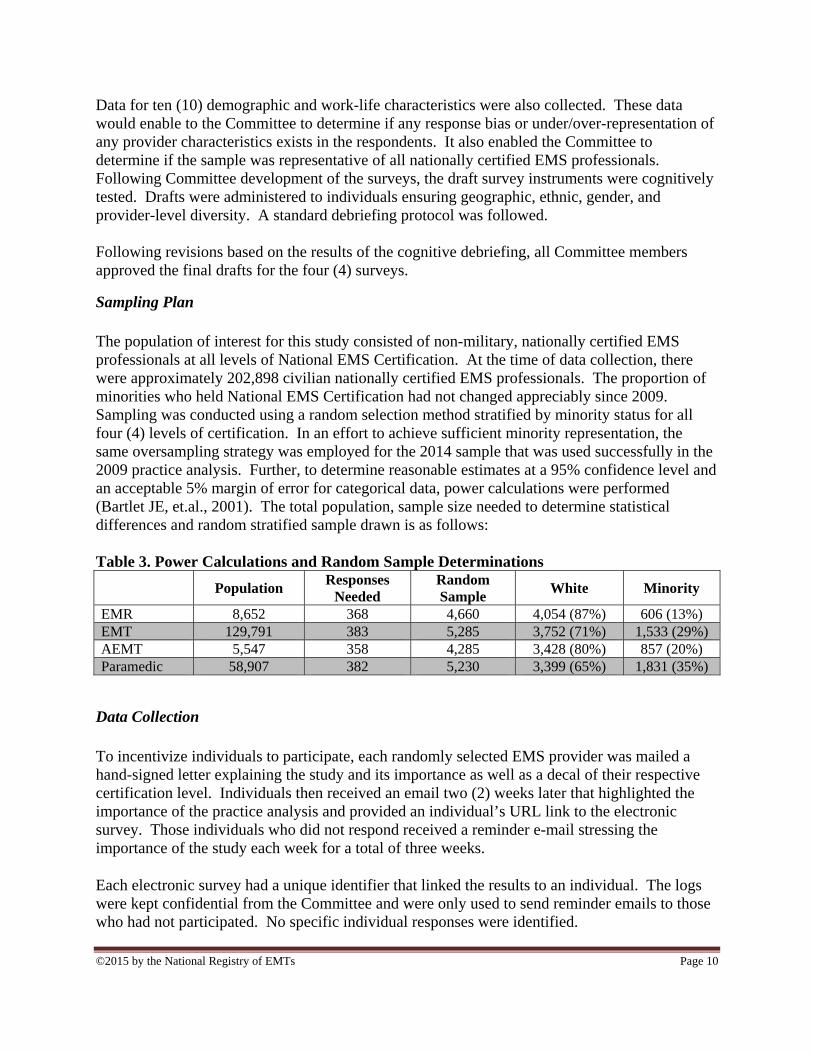
Sampling Plan The population of interest for this study consisted of non-military, nationally certified EMS professionals at all levels of National EMS Certification. At the time of data collection, there were approximately 202,898 civilian nationally certified EMS professionals. The proportion of minorities who held National EMS Certification had not changed appreciably since 2009. Sampling was conducted using a random selection method stratified by minority status for all four (4) levels of certification. In an effort to achieve sufficient minority representation, the same oversampling strategy was employed for the 2014 sample that was used successfully in the 2009 practice analysis. Further, to determine reasonable estimates at a 95% confidence level and an acceptable 5% margin of error for categorical data, power calculations were performed (Bartlet JE, et.al., 2001). The total population, sample size needed to determine statistical differences and random stratified sample drawn is as follows: Table 3. Power Calculations and Random Sample Determinations
Population Responses
Needed Random Sample
White Minority
EMR 8,652 368 4,660 4,054 (87%) 606 (13%) EMT 129,791 383 5,285 3,752 (71%) 1,533 (29%) AEMT 5,547 358 4,285 3,428 (80%) 857 (20%) Paramedic 58,907 382 5,230 3,399 (65%) 1,831 (35%)
Data Collection To incentivize individuals to participate, each randomly selected EMS provider was mailed a hand-signed letter explaining the study and its importance as well as a decal of their respective certification level. Individuals then received an email two (2) weeks later that highlighted the importance of the practice analysis and provided an individual’s URL link to the electronic survey. Those individuals who did not respond received a reminder e-mail stressing the importance of the study each week for a total of three weeks. Each electronic survey had a unique identifier that linked the results to an individual. The logs were kept confidential from the Committee and were only used to send reminder emails to those who had not participated. No specific individual responses were identified.

©2015 by the National Registry of EMTs Page 11
Because of the electronic nature of the study, double answers on items were not possible. All data were entered into a Microsoft Excel (Microsoft Corp., Redmond, WA) database and analyzed in Stata IC 12 (College Station, TX).
Data Analysis One of the major goals of the practice analysis is to determine the relative importance of job-related activities performed by EMS providers. The Practice Analysis Committee determined that the importance of each task performed by EMS professionals is a function of the frequency that a task is performed and the potential of harm related to that task. Using an additive model for combining scales (Sanchez & Levine, 1989), a Weighted Importance Score (WIS) formula consisting of 1/3 weight calculated for frequency and 2/3 weight calculated for potential for harm was utilized for each task.
WIS = 1/3(frequency) + 2/3(potential for harm)
The frequency score for each task ranged from 1 to 5. The potential for harm for each task ranged from 1 to 4. Since we are interested in a provider’s rating of the potential for harm of a task based on personal experience, we excluded any ranking of potential harm if the individual respondent had never performed a particular task as had been done in our previous practice analyses. Thus, a WIS (ranging from 1.0 to 4.33) was calculated for each task.
RESULTS The questionnaire response rates can be found in Table 4. Table 4. Provider Level Questionnaire Response Rates Certification Level Complete Surveys1 Partial Surveys2 Response Rate EMR 614 252 13.8% (19.5%) EMT 468 303 9.1% (15.0%) AEMT 605 355 14.5% (23.0%) Paramedic 818 431 16.2% (24.7%)
1. Individuals who completed the survey and clicked “submit” at the end. 2. Individuals who began the survey but stopped during it/did not click “submit” at the end
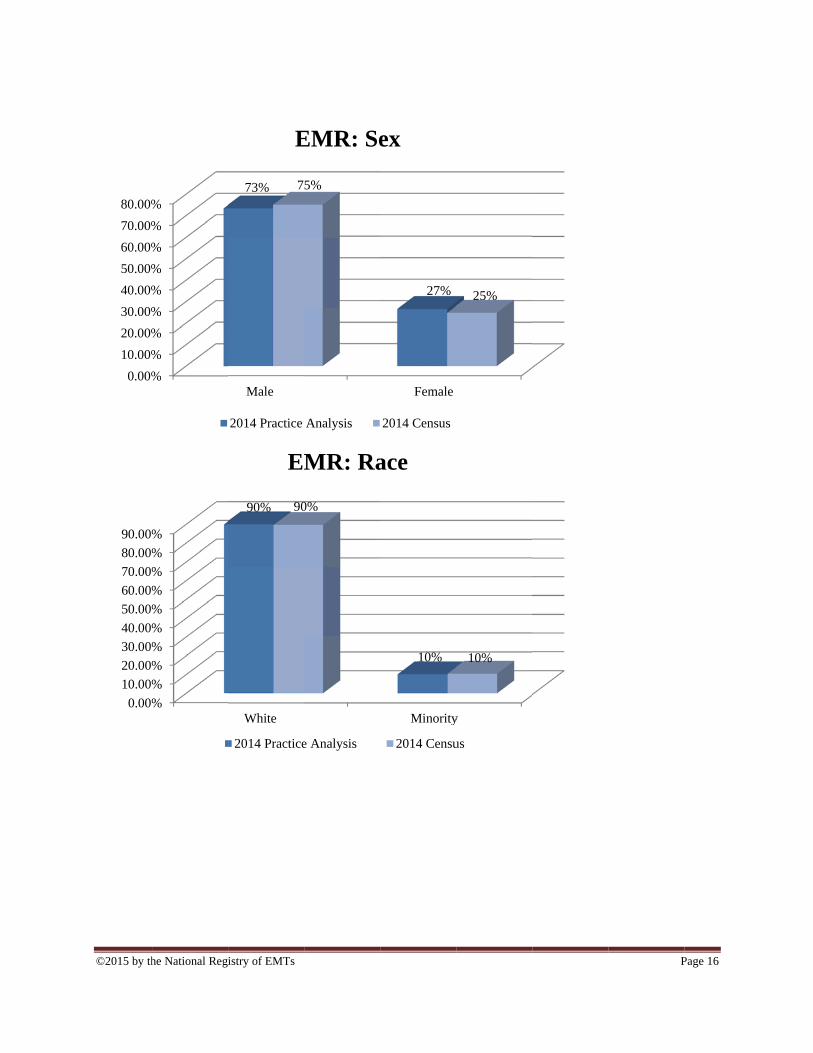
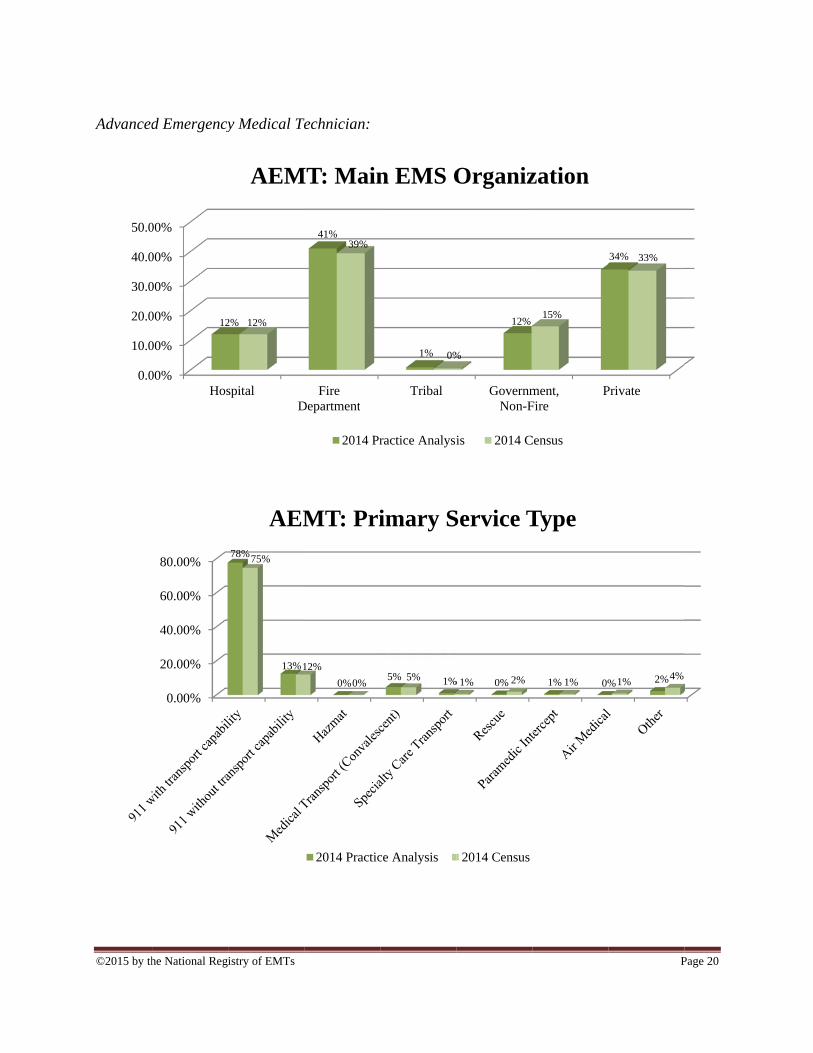
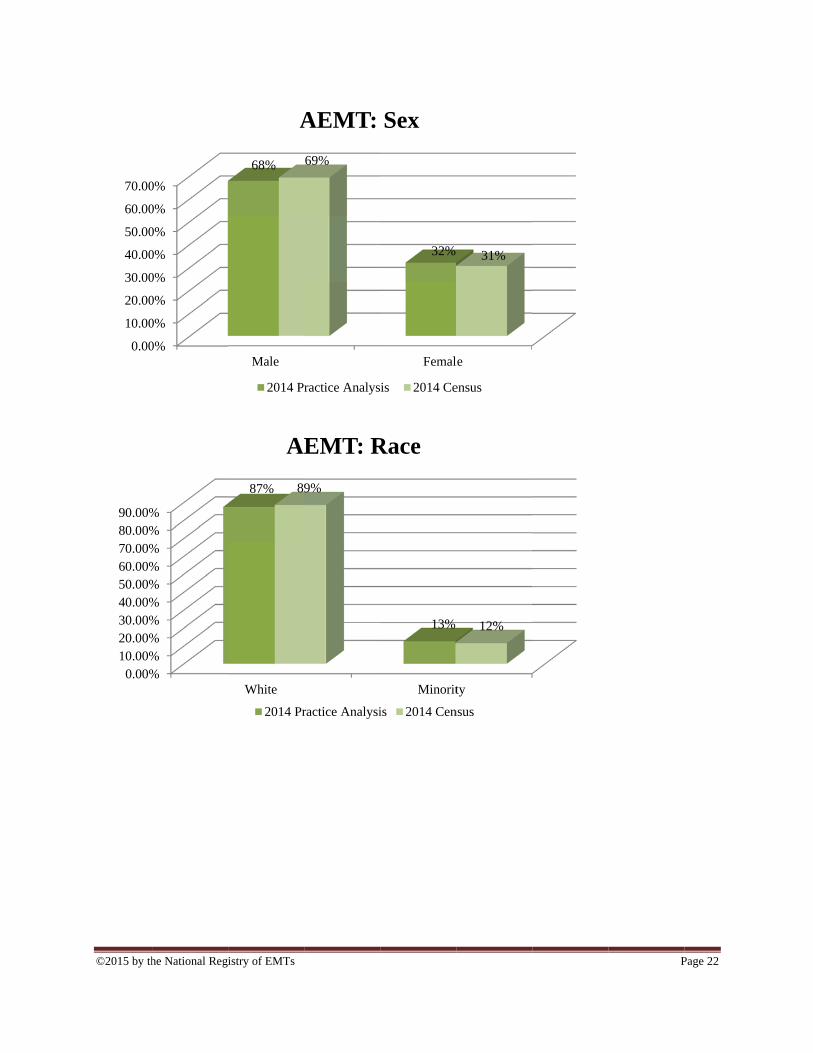
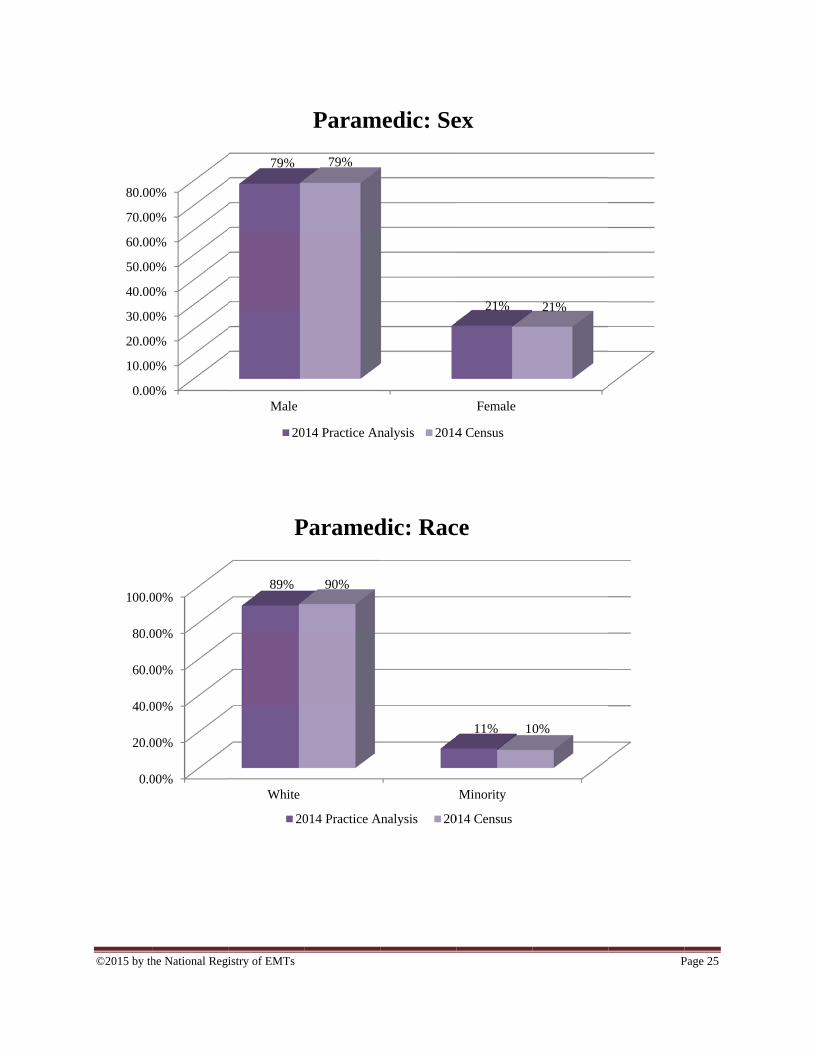
Representativeness of the Sample The Practice Analysis Committee reviewed the demographics of individuals who responded to the practice analysis survey. These data were compared to population data from the NREMT database and other research initiatives. The Committee determined that the responses in the present study were representative of the population of all levels of nationally certified EMS providers throughout the nation (Appendix B).
©2015 by the National Registry of EMTs Page 12
Test Plan Development The Committee analyzed the content domain of the National EMS Education Standards, job descriptions, and patient illnesses and injuries based upon their observation and experience as experts in the field. The Committee recommended that the test plan be developed along a number of dimensions:
Patient Care vs. EMS Operations
Adult vs. Pediatrics
Airway, Respiration & Ventilation vs. Cardiology & Resuscitation vs. Trauma vs. Medical/Obstetrics/Gynecology
Assessment/Pathophysiology vs. Management
The goal of the practice analysis is to determine the relative proportions for each of these relationships on each level of the NREMT examination based on the importance of tasks. To determine the balance of the exam, a relative weight for each domain was determined. The proportion of the examination related to patient care and operations was determined in evaluating the WIS of all patient care tasks as well as the EMS operations section. Responses for adult and pediatric patient care tasks were combined in each of the patient care content areas to determine the final representative proportion for each section in the final test plan (Appendix C). Since pediatric presentations occur throughout all content areas, the proportion of the patient care exam content related to adult and pediatric patients was further determined by comparing it to historical data from EMS systems and other published data citing the proportion of pediatric EMS responses and Committee recommendations. A policy recommendation that 15% of all patient care content areas reflect pediatric content and the remaining 85% contain adult and geriatric content was upheld as in our previous practice analyses. Based on the examination lengths recommended by the NREMT Standards and Examination Committee and approved by the NREMT Board of Directors, the number of items for each section was determined by relative weight of the section, multiplied by the range of the total number of exam items in the currently approved examinations. Following the Practice Analysis Committee’s review of data, outcome and drafted test plans, the NREMT Board of Directors adopted the four (4) test plans at the November 2014 Board of Directors meeting for implementation on September 1, 2015 (Appendix D).
©2015 by the National Registry of EMTs Page 13
Appendix A 2014 Practice Analysis Committee
Chairman: David Persse, MD City of Houston Public Health Authority & EMS Director Houston, Texas Severo Rodriguez, MS, NRP, LP, AEMCA Executive Director National Registry of EMTs Columbus, Ohio Scott Gilmore, M.D., EMT-P, FACEPAssistant Professor of Emergency MedicineProgram Director, EMS FellowshipDivision of Emergency MedicineWashington University School of MedicineMedical Director Saint Louis Fire DepartmentSaint Louis, Missouri William F. Niemeck, NRP City of New Orleans EMS Education Coordinator New Orleans, Louisiana Paul Patrick, M.Ed. NASEMSO President 2014-2016 Deputy Division Director Utah Department of Health Family Health and Preparedness Salt Lake City, Utah
Dee Dee Hillary, LP EMS Captain Lancaster Fire Department Lancaster, Texas Jason Preston, NREMT-P Clinical Education Services Manager American Medical Response Nashua, New Hampshire Rob Wagoner, BSAS, NRP Senior Director National Registry of EMTs Columbus, Ohio Gabe Romero MBA, NRP Director of Examinations National Registry of EMTs Columbus, Ohio Melissa Bentley MS, NRP Director of Research National Registry of EMTs Columbus, Ohio Remle Crowe BS, NREMT EMS Research Fellow National Registry of EMTs Columbus, Ohio

©2015 by th
Emergen
1
2
3
4
5
6
7
he National Reg
ncy Medical R
0.00%
0.00%
0.00%
0.00%
0.00%
0.00%
0.00%
0.00%
H
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
2
istry of EMTs
Responders
Hospital F
4% 3%
EM
25%
55%
25%
E
ApResponde
Fire Departmen
61% 64%
MR: Main
2014 Practic
%
1%
55%
1%
EMR: Pr
2014 P
ppendix B ent Demogra
nt Triba
1%
%
n EMS O
e Analysis
0%% 1%
rimary S
ractice Analys
aphics
al GovNo
0%
Organiz
2014 C
0%
8%
0%
Service
sis 20
vernment,on-Fire
10% 10%
zation
Census
%
1%
9%
1
Type
14 Census
P
Private
20% 23%
0%% 1%
Page 14
%
8% 8%

©2015 by th
0.00
10.00
20.00
30.00
40.00
0.00
10.00
20.00
30.00
40.00
50.00
he National Reg
0%
0%
0%
0%
0%
0
13% 14
0%
0%
0%
0%
0%
0% 47%4
istry of EMTs
1 call
26%
4%
31%
E
34%
43%
26%
2-4 calls 5-9
36% 37%
EMR: W
2014 Pr
9%
%
12%
EMR:
2014 Pra
9 calls 10-cal
15%
5%
12%
Weekly C
ractice Analysi
4%7%
Commu
actice Analysis
19lls
20-29calls
%
2%4% 2
Call Volu
is 2014 Cen
2% 4%
unity Si
2014 Ce
30-39calls
1%2%
1%
ume
nsus
2% 2%
ize
ensus
P
40-49calls mo
0% 0%
2% 2%3%
Page 15
50 orore calls
1% 0%
% 3%
©2015 by th
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
he National Reg
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
istry of EMTs
Male
73% 7
E
2014 Practice
White
90% 90
EM
2014 Practice
5%
EMR: Se
Analysis
0%
MR: Ra
e Analysis
Female
27%
ex
2014 Census
Minority
10%
ace
2014 Censu
25%
y
10%
us
PPage 16

©2015 by th
Emergen
0.0
10.0
20.0
30.0
40.0
50.0
he National Reg
ncy Medical
00%
00%
00%
00%
00%
00%
Ho
1
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00% 5
istry of EMTs
Technician:
ospital Fi
1% 11%
EM
57%
23%
53%
2
EM
ire Department
44% 43%
MT: Mai
2014 Pract
0%
2%
1%
MT: Prim
2014 Practic
t Triba
0%
%
in EMS
tice Analysis
7%1%
7%
mary Se
e Analysis
al GovN
1%
Organi
2014 Census
2%1% 3%
ervice Ty
2014 Censu
vernment,Non-Fire
12% 11%
ization
s
1% 1%1%
Type
us
P
Private
33%35
%
9%
1%
10%
Page 17
5%
%

©2015 by th
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
0.0
5.0
10.0
15.0
20.0
25.0
30.0
he National Reg
%
%
%
%
%
%
%
0
9%
12%
0%
0%
0%
0%
0%
0%
0% 25%
2
istry of EMTs
1 call 2-
12%% 13%
E
28%
22%
28%
-4 calls 5-9 c
23%
15%
25%
EMT: W
2014 Practic
15%
%
16%
EMT: C
2014 Prac
calls 10-19calls
%17%
16% 16
Weekly C
ce Analysis
8% 8%
Commu
ctice Analysis
20-29calls
12%
6%
9%
Call Volu
2014 Cen
10%
2
8%
unity Siz
2014 Cen
30-39calls
4c
6%
5%
ume
nsus
2%
10
4%
ze
nsus
P
0-49calls
50 omorcall
1%
6%
2%
0%
2%
10%
Page 18
orres
%
3%
4%

©2015 by th
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
0.00
20.00
40.00
60.00
80.00
100.00
he National Reg
%
%
%
%
%
%
%
%
0%
0%
0%
0%
0%
0%
istry of EMTs
Male
66% 6
2014 P
White
87%84
EM
2014 Pra
69%
EMT: S
Practice Analys
4%
MT: Ra
actice Analysis
Femal
34%
Sex
sis 2014 Cen
Minority
13%
ace
s 2014 Cen
le
31%
nsus
16%
nsus
P
Page 19
©2015 by th
Advanced
0.0
10.0
20.0
30.0
40.0
50.0
he National Reg
d Emergency
00%
00%
00%
00%
00%
00%
Hos
12
0.00%
20.00%
40.00%
60.00%
80.00%
istry of EMTs
y Medical Te
spitalD
2% 12%
AEM
78%
13%
75%
1
AEM
Technician:
FireDepartment
41%39%
MT: Main
2014 Pr
0%
12%
0%
MT: Pri
2014 Practic
Tribal
1% 0%
n EMS O
ractice Analysi
5% 1%5%
imary S
ce Analysis
GovernmNon-F
12%
%
Organiz
is 2014 C
% 0%1% 2%
Service T
2014 Census
ment,Fire
P
15%
zation
Census
1% 0%1%
Type
P
Private
34% 33%
% 2%1% 4%
Page 20

©2015 by th
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
0.00
10.00
20.00
30.00
40.00
he National Reg
%
%
%
%
%
%
%
0
2%3%
0%
0%
0%
0%
0%
15%
2
istry of EMTs
1 call 2-
5%
8%
AE
39%
28%
35
-4 calls 5-9 c
19%20%
27%
EMT: W
2014 Prac
18%
%
15%
AEMT:
2014 Practi
alls 10-19calls
%
22%22%
18%
Weekly C
ctice Analysis
7% 7%
: Comm
ice Analysis
20-29calls
16%%
11%
Call Volu
2014 Cen
9%
26%
munity Si
2014 Censu
30-39calls
40ca
8%
3
7%
ume
nsus
2%7%
3%
ize
us
P
-49alls
50 ormorecalls
%
6%
2%3
%3%4%
Page 21
3%
2%
©2015 by th
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%90.00%
he National Reg
0%
0%
0%
0%
0%
0%
0%
0%
%%%%%%%%%%
istry of EMTs
Male
68%
A
2014 P
White
87% 8
A
2014 Pr
69%
AEMT:
ractice Analys
9%
EMT: R
ractice Analysi
Femal
32%
Sex
is 2014 Ce
Minorit
13%
Race
is 2014 Cen
le
31%
ensus
ty
12%
nsus
P
Page 22

©2015 by th
Paramed
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
he National Reg
dic:
00%
00%
00%
00%
00%
00%
00%
00%
00%
Hos
17
0.00%
20.00%
40.00%
60.00%
80.00%
istry of EMTs
pitalDe
7% 16%
Param
73%
8%
75%
8
Param
Fireepartment
36% 37%
medic: M
2014 Prac
0%8%
0%
medic: Pr
2014 Practice
Tribal
0% 0%
Main EM
ctice Analysis
4% 3%3%
rimary S
Analysis
GovernmeNon-Fir
17%
MS Agen
2014 Censu
0%3% 1%
Service
2014 Census
ent,re
Priv
30
16%
ncy
us
2% 5%2% 5
Type
P
vate
0% 30%
4%5% 4%
Page 23

©2015 by th
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
0.00
5.00
10.00
15.00
20.00
25.00
30.00
he National Reg
%
%
%
%
%
%
%
0
4%
6%
0%
0%
0%
0%
0%
0%
0%
6%
15%
istry of EMTs
1 call 2
1%2%
24%
%
29%
Par
2-4 calls 5-9
9%
15%
11%
Parame
2014
23%
20%
ramedic
2014 Practice
calls 10-19calls
%
28%
17%
2
edic: Ca
Practice Analy
12%10%
c: Comm
e Analysis
9 20-29calls
20%
28%
19%
all Volum
ysis 2014
15%
3%
8%
munity S
2014 Census
30-39calls
4
11%
%
9%
me
Census
%
12%
5%
Size
s
P
40-49calls
50 mocal
4%
9
3%
5%
8%6%
Page 24
ororells
%
4%
%
©2015 by th
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
0.0
20.0
40.0
60.0
80.0
100.0
he National Reg
0%
0%
0%
0%
0%
0%
0%
0%
0%
00%
00%
00%
00%
00%
00%
istry of EMTs
Male
79%
20
White
89%
P
20
79%
Param
014 Practice An
90%
Paramed
014 Practice A
medic: Se
nalysis 2014
dic: Rac
Analysis 20
Female
21%
ex
4 Census
Minority
11% 10
ce
014 Census
21%
0%
P
Page 25

©2015 by the National Registry of EMTs Page 26
Appendix C 2014 Practice Analysis Test Plan: Sections with Tasks
AIRWAY, RESPIRATION & VENTILATION (7 Tasks) (includes assessment, pathophysiology and management)
1. Airway Management 2. Ventilation 3. Respiratory Distress 4. Respiratory Failure 5. Respiratory Arrest 6. Upper Airway Respiratory Emergencies 7. Lower Airway Respiratory Emergencies
CARDIOLOGY & RESUSCITATION (6 Tasks) (includes assessment, pathophysiology and management)
1. Chest Discomfort 2. Cardiac Rhythm Disturbance 3. Cardiac Arrest 4. Stroke-like Symptoms 5. Post-resuscitation Care 6. Hypotension/Hypertension from a Non-traumatic Cause
TRAUMA (7 Tasks) (includes assessment, pathophysiology and management)
1. Bleeding 2. Chest Trauma 3. Abdominal/Genitourinary Trauma 4. Orthopedic Trauma 5. Soft Tissue 6. Head/Neck/Face/Spine Trauma 7. Multisystem Trauma

©2015 by the National Registry of EMTs Page 27
Appendix C (continued) 2014 Practice Analysis Test Plan: Sections with Tasks
MEDICAL, OBSTETRICS AND GYNECOLOGY (12 Tasks)
(includes assessment, pathophysiology and management) 1. Neurological Emergencies 2. Abdominal Disorders 3. Immunological Emergencies 4. Infectious Disease 5. Endocrine Emergencies 6. Psychiatric Emergencies 7. Toxicological Emergencies 8. Hematological Emergencies 9. Genitourinary/Renal Emergencies 10. Gynecological Emergencies 11. Obstetrical Emergencies 12. Special Healthcare Needs
EMS OPERATIONS (9 Tasks) (includes assessment, pathophysiology and management)
1. Maintain Vehicle and Equipment Readiness 2. Operate Emergency Vehicles 3. Provide Scene Leadership 4. Resolve an Emergency Incident 5. Provide Emotional Support 6. Maintain Medical/Legal Standards 7. Maintain Community Relations 8. Provide Administrative Support 9. Enhance Professional Development
©2015 by the National Registry of EMTs Page 28
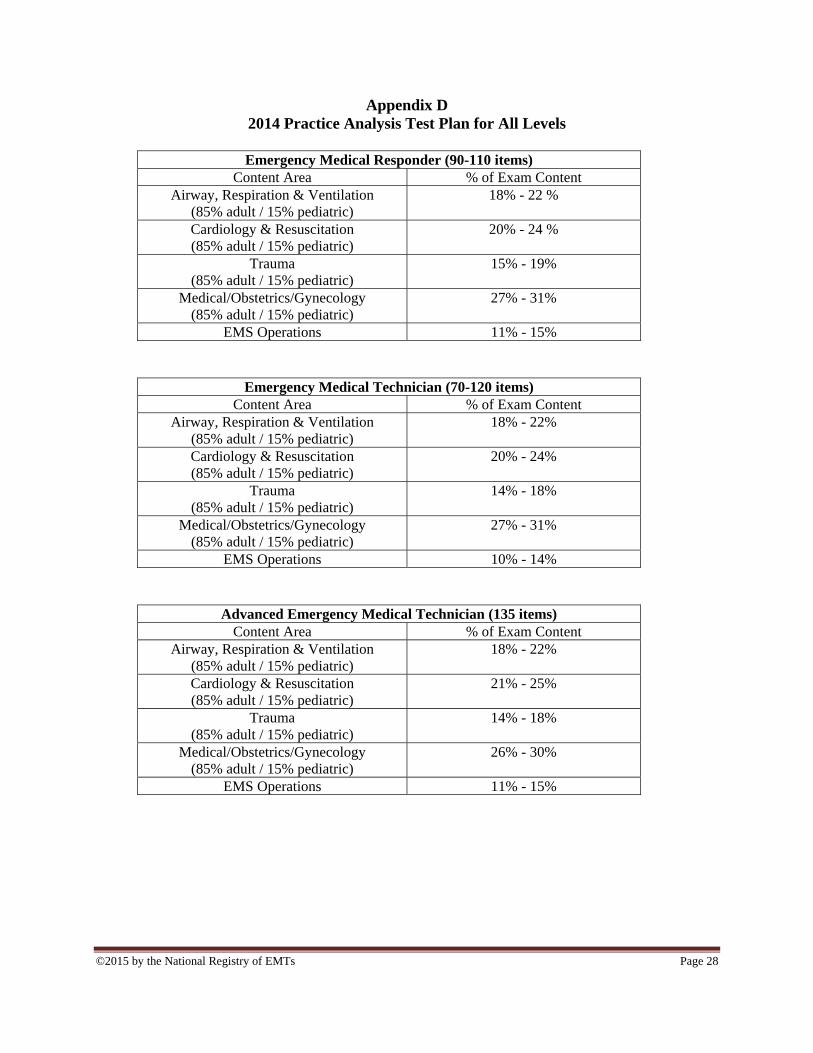
Appendix D 2014 Practice Analysis Test Plan for All Levels
Emergency Medical Responder (90-110 items)
Content Area % of Exam Content Airway, Respiration & Ventilation
(85% adult / 15% pediatric) 18% - 22 %
Cardiology & Resuscitation (85% adult / 15% pediatric)
20% - 24 %
Trauma (85% adult / 15% pediatric)
15% - 19%
Medical/Obstetrics/Gynecology (85% adult / 15% pediatric)
27% - 31%
EMS Operations 11% - 15%
Emergency Medical Technician (70-120 items) Content Area % of Exam Content
Airway, Respiration & Ventilation (85% adult / 15% pediatric)
18% - 22%
Cardiology & Resuscitation (85% adult / 15% pediatric)
20% - 24%
Trauma (85% adult / 15% pediatric)
14% - 18%
Medical/Obstetrics/Gynecology (85% adult / 15% pediatric)
27% - 31%
EMS Operations 10% - 14%
Advanced Emergency Medical Technician (135 items) Content Area % of Exam Content
Airway, Respiration & Ventilation (85% adult / 15% pediatric)
18% - 22%
Cardiology & Resuscitation (85% adult / 15% pediatric)
21% - 25%
Trauma (85% adult / 15% pediatric)
14% - 18%
Medical/Obstetrics/Gynecology (85% adult / 15% pediatric)
26% - 30%
EMS Operations 11% - 15%

©2015 by the National Registry of EMTs Page 29
Appendix D (continued) 2014 Practice Analysis Test Plan for All Levels
Paramedic (80-150 items) Content Area % of Exam Content
Airway, Respiration & Ventilation (85% adult / 15% pediatric)
18% - 22%
Cardiology & Resuscitation (85% adult / 15% pediatric)
22% - 26%
Trauma (85% adult / 15% pediatric)
13% - 17%
Medical/Obstetrics/Gynecology (85% adult / 15% pediatric)
25% - 29%
EMS Operations 10% - 14%
Top Related
