







Languages
Pages
Legal

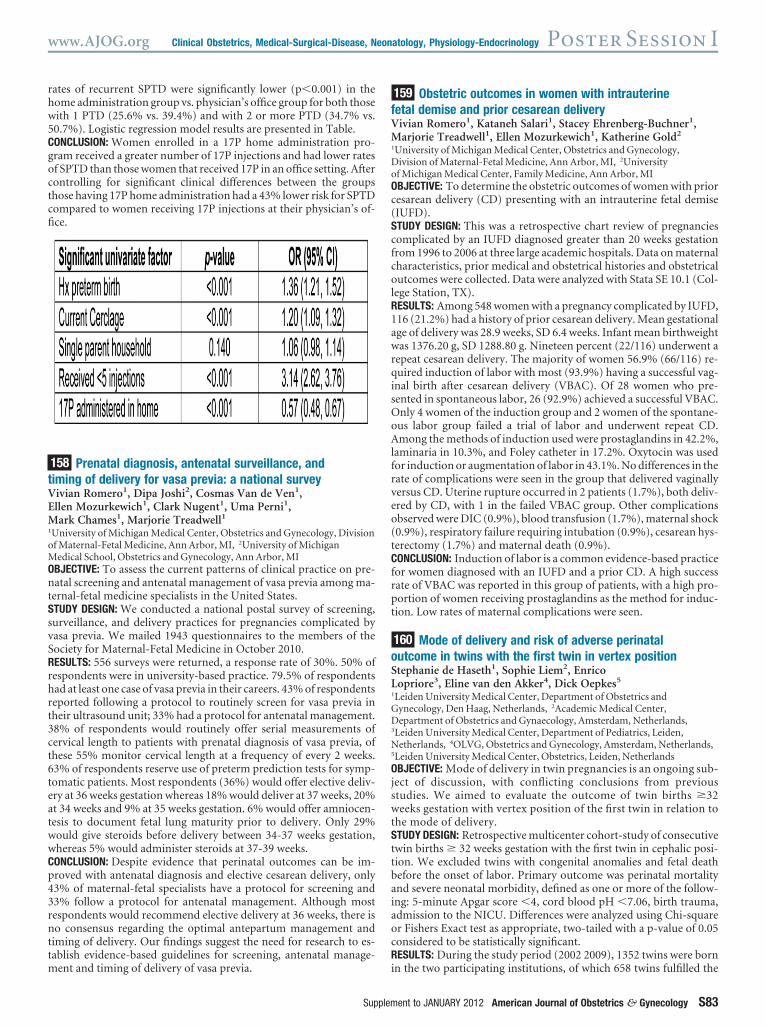
rates of recurrent SPTD were significantly lower (p�0.001) in thehome administration group vs. physician’s office group for both thosewith 1 PTD (25.6% vs. 39.4%) and with 2 or more PTD (34.7% vs.50.7%). Logistic regression model results are presented in Table.CONCLUSION: Women enrolled in a 17P home administration pro-gram received a greater number of 17P injections and had lower ratesof SPTD than those women that received 17P in an office setting. Aftercontrolling for significant clinical differences between the groupsthose having 17P home administration had a 43% lower risk for SPTDcompared to women receiving 17P injections at their physician’s of-fice.
158 Prenatal diagnosis, antenatal surveillance, andtiming of delivery for vasa previa: a national surveyVivian Romero1, Dipa Joshi2, Cosmas Van de Ven1,Ellen Mozurkewich1, Clark Nugent1, Uma Perni1,Mark Chames1, Marjorie Treadwell11University of Michigan Medical Center, Obstetrics and Gynecology, Divisionof Maternal-Fetal Medicine, Ann Arbor, MI, 2University of MichiganMedical School, Obstetrics and Gynecology, Ann Arbor, MIOBJECTIVE: To assess the current patterns of clinical practice on pre-natal screening and antenatal management of vasa previa among ma-ternal-fetal medicine specialists in the United States.STUDY DESIGN: We conducted a national postal survey of screening,surveillance, and delivery practices for pregnancies complicated byvasa previa. We mailed 1943 questionnaires to the members of theSociety for Maternal-Fetal Medicine in October 2010.RESULTS: 556 surveys were returned, a response rate of 30%. 50% ofrespondents were in university-based practice. 79.5% of respondentshad at least one case of vasa previa in their careers. 43% of respondentsreported following a protocol to routinely screen for vasa previa intheir ultrasound unit; 33% had a protocol for antenatal management.38% of respondents would routinely offer serial measurements ofcervical length to patients with prenatal diagnosis of vasa previa, ofthese 55% monitor cervical length at a frequency of every 2 weeks.63% of respondents reserve use of preterm prediction tests for symp-tomatic patients. Most respondents (36%) would offer elective deliv-ery at 36 weeks gestation whereas 18% would deliver at 37 weeks, 20%at 34 weeks and 9% at 35 weeks gestation. 6% would offer amniocen-tesis to document fetal lung maturity prior to delivery. Only 29%would give steroids before delivery between 34-37 weeks gestation,whereas 5% would administer steroids at 37-39 weeks.CONCLUSION: Despite evidence that perinatal outcomes can be im-proved with antenatal diagnosis and elective cesarean delivery, only43% of maternal-fetal specialists have a protocol for screening and33% follow a protocol for antenatal management. Although mostrespondents would recommend elective delivery at 36 weeks, there isno consensus regarding the optimal antepartum management andtiming of delivery. Our findings suggest the need for research to es-tablish evidence-based guidelines for screening, antenatal manage-ment and timing of delivery of vasa previa.
159 Obstetric outcomes in women with intrauterinefetal demise and prior cesarean deliveryVivian Romero1, Kataneh Salari1, Stacey Ehrenberg-Buchner1,Marjorie Treadwell1, Ellen Mozurkewich1, Katherine Gold2
1University of Michigan Medical Center, Obstetrics and Gynecology,Division of Maternal-Fetal Medicine, Ann Arbor, MI, 2Universityof Michigan Medical Center, Family Medicine, Ann Arbor, MIOBJECTIVE: To determine the obstetric outcomes of women with priorcesarean delivery (CD) presenting with an intrauterine fetal demise(IUFD).STUDY DESIGN: This was a retrospective chart review of pregnanciescomplicated by an IUFD diagnosed greater than 20 weeks gestationfrom 1996 to 2006 at three large academic hospitals. Data on maternalcharacteristics, prior medical and obstetrical histories and obstetricaloutcomes were collected. Data were analyzed with Stata SE 10.1 (Col-lege Station, TX).RESULTS: Among 548 women with a pregnancy complicated by IUFD,116 (21.2%) had a history of prior cesarean delivery. Mean gestationalage of delivery was 28.9 weeks, SD 6.4 weeks. Infant mean birthweightwas 1376.20 g, SD 1288.80 g. Nineteen percent (22/116) underwent arepeat cesarean delivery. The majority of women 56.9% (66/116) re-quired induction of labor with most (93.9%) having a successful vag-inal birth after cesarean delivery (VBAC). Of 28 women who pre-sented in spontaneous labor, 26 (92.9%) achieved a successful VBAC.Only 4 women of the induction group and 2 women of the spontane-ous labor group failed a trial of labor and underwent repeat CD.Among the methods of induction used were prostaglandins in 42.2%,laminaria in 10.3%, and Foley catheter in 17.2%. Oxytocin was usedfor induction or augmentation of labor in 43.1%. No differences in therate of complications were seen in the group that delivered vaginallyversus CD. Uterine rupture occurred in 2 patients (1.7%), both deliv-ered by CD, with 1 in the failed VBAC group. Other complicationsobserved were DIC (0.9%), blood transfusion (1.7%), maternal shock(0.9%), respiratory failure requiring intubation (0.9%), cesarean hys-terectomy (1.7%) and maternal death (0.9%).CONCLUSION: Induction of labor is a common evidence-based practicefor women diagnosed with an IUFD and a prior CD. A high successrate of VBAC was reported in this group of patients, with a high pro-portion of women receiving prostaglandins as the method for induc-tion. Low rates of maternal complications were seen.
160 Mode of delivery and risk of adverse perinataloutcome in twins with the first twin in vertex positionStephanie de Haseth1, Sophie Liem2, EnricoLopriore3, Eline van den Akker4, Dick Oepkes5
1Leiden University Medical Center, Department of Obstetrics andGynecology, Den Haag, Netherlands, 2Academic Medical Center,Department of Obstetrics and Gynaecology, Amsterdam, Netherlands,3Leiden University Medical Center, Department of Pediatrics, Leiden,Netherlands, 4OLVG, Obstetrics and Gynecology, Amsterdam, Netherlands,5Leiden University Medical Center, Obstetrics, Leiden, NetherlandsOBJECTIVE: Mode of delivery in twin pregnancies is an ongoing sub-ject of discussion, with conflicting conclusions from previousstudies. We aimed to evaluate the outcome of twin births �32weeks gestation with vertex position of the first twin in relation tothe mode of delivery.STUDY DESIGN: Retrospective multicenter cohort-study of consecutivetwin births � 32 weeks gestation with the first twin in cephalic posi-tion. We excluded twins with congenital anomalies and fetal deathbefore the onset of labor. Primary outcome was perinatal mortalityand severe neonatal morbidity, defined as one or more of the follow-ing: 5-minute Apgar score �4, cord blood pH �7.06, birth trauma,admission to the NICU. Differences were analyzed using Chi-squareor Fishers Exact test as appropriate, two-tailed with a p-value of 0.05considered to be statistically significant.RESULTS: During the study period (2002 2009), 1352 twins were bornin the two participating institutions, of which 658 twins fulfilled the
www.AJOG.org Clinical Obstetrics, Medical-Surgical-Disease, Neonatology, Physiology-Endocrinology Poster Session I
Supplement to JANUARY 2012 American Journal of Obstetrics & Gynecology S83
Top Related