







Languages
Pages
Legal

113 SECTION Q – CLAIMS MANAGEMENT

114 Q.1

Part Two: Technical Proposal
Section Q: Claims Management
Section Q: Claims Management (Section §17 of RFP)
Q.1 Describe the capabilities of your claims management systems as it relates to each of the requirements as specified in Electronic Claims Management Functionality Section and the Adherence to Key Claims Management Standards Section. In your response explain whether and how your systems meet (or exceed) each of these requirements. Cite at least three examples from similar contracts.
For over 25 years, Aetna Better Health®’s affiliates have used their expansive expertise in the development and implementation of an IT infrastructure to improve the accessibility and quality of healthcare services for its covered populations, while controlling the program’s rate of cost increase. We benefit, in this endeavor, from the strategic alignment of IT resources with Aetna Medicaid, an Aetna Company (Aetna Medicaid). For example, while Aetna Better Health benefits – on one hand – from the backing of Aetna Medicaid’s considerable resources in hardware and network infrastructure support, we also count ourselves fortunate – on the other – for the unwavering support of Aetna Medicaid’s expertise in application support and configuration management. When combined, these systems bring Aetna Better Health every advantage one could expect from an IT infrastructure that is reliable, flexible, expandable, and designed to interface seamlessly with other systems. In this section, the systems and applications that support the major functional areas of Aetna Better Health are detailed, starting with the guiding principles that form the foundation of our IT infrastructure:
• Privacy and Security: To secure members’ Protected Health Information (PHI), a layered approach to security includes clearly delineated policies and procedures, employee training, comprehensive communications, hardening of physical systems, adherence to federal laws such as HIPAA and Louisiana specific requirements that are more stringent.
• Business Integration: Aetna Better Health’s IT systems have the ability to integrate and map data from disparate systems, inside and outside the company, and to utilize data mining tools to analyze and report Key Performance Indicators (KPI) to improve the quality of services.
• People: Aetna Better Health shares with Aetna Medicaid the mission of providing “value, integrity and compassion in healthcare management” through recruiting and retaining the most skilled and experienced IT personnel available and continuously training them on the most up-to-date technologies.
• Business Continuity: Even the best applications and systems are ineffectual if they are not available. To address this, Aetna Better Health has built redundancy into the IT infrastructure, communication services and environmental support systems. We have a 99.9% system availability record for our computer systems and applications.
• Scalability: Aetna Better Health will meet DHH’s changing needs by managing the network infrastructure, load-balancing server clusters and communications systems with the ability to grow rapidly without sacrificing availability.
This IT system will support our expansion from GSA A –to GSA B – to GSA C. The depth, reliability, scalability and flexibility of our IT system mean that Aetna Better Health will be able to accept and manage additional membership and providers without interruption or disruption to
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
1

Part Two: Technical Proposal
Section Q: Claims Management
our current members and providers. The Aetna Better Health management team and Aetna Medicaid IT team will work together to see that that our expansion activities are seamless and in accordance with our history of excellence in working with Medicaid programs across the nation.
Provider Payment Support Aetna Better Health and our affiliates paid 17,761,200 claims nationwide during calendar year 2010. This volume is possible because of our efficient systems, tools and processes.
Aetna Better Health offers our network providers a choice between receiving payment via Electronic Fund Transfer (EFT) or physical checks. The payment method is set to physical check by default, but any network provider wishing to activate EFT need only do the following:
• A network provider submits an EFT enrollment form to Aetna Better Health, indicating the desired bank routing and account numbers
• That information is then loaded into QNXT™, Aetna Better Health’s claims payment system, designating that applicant as an EFT network provider
• A test document, called a prenote, is then sent to the network provider’s bank to see that the routing and account numbers are accurate and functioning properly
• Upon notification of a successful test transaction, the network provider’s account is configured accordingly and EFT enabled
• When the network provider has a payment generated during the check run process, the payment is included in a secure electronic file that is then “held” for submission to the various banks and clearing houses for processing
• Upon approval of the check run by Aetna Better Health, physical checks are released for printing and mailing, while the EFT file is released to the designated financial institutions for processing
• Network providers receiving EFT receive a hard copy remittance via mail detailing the claims processed in a particular payment run, as well as a paper copy of what would have been a check indicating the EFT Check # and total dollars, thereby allowing them to post the payment accordingly
Any network provider wishing to discontinue EFT payments and return to payment by physical check need only contact the health plan in writing and claims personnel will discontinue EFT functionality on the indicated accounts accordingly.
Claims Adjudication At the heart of Aetna Better Health’s claims adjudication process lies QNXT™, a client/server based managed care information system with unmatched claims processing capabilities. Operating in a Microsoft Windows NT™ and SQL Server environment, this rules-based system – with its graphical user interface and relational database – allows users immediate access to real-time claims information. Since QNXT™ is based on a common operating system and database platform, a multitude of tools can be used to display, print and analyze information. Moreover, this information can be presented in both textual and graphical formats to enhance readability and review. The following paragraphs detail Aetna Better Health’s claims adjudication processes, our claims inventory and workflow management practices and the monitoring tools and audit trails in place to provide for the timely, accurate adjudication of claims.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
2

Part Two: Technical Proposal
Section Q: Claims Management
Manual and Automated Claims Processing Functions Electronic Claims Acquisition (Electronic Data Interface) To assist us in processing and paying claims efficiently, accurately and timely; and to best leverage QNXT™’s automated claims processing capabilities, Aetna Better Health encourages network providers to submit claims electronically. To facilitate electronic claims submission, we have developed business relationships with ten major clearinghouses, including Gateway EDI, Emdeon and SSI, among others. We receive EDI claims directly from these clearinghouses, process them through pre-import edits to see to the validity of the data, HIPAA compliance and member enrollment and then upload them into QNXT™ each business day. Within 24 hours of file receipt, we provide production reports and control totals to all trading partners to validate successful transactions and identify errors for correction and resubmission. Our Arizona affiliate, Mercy Care Plan (MCP) has received (from February 2010 and February 2011) 70.4 percent of total claims submissions via EDI. At the same time MCP’s EFT transactions rose to over 65 percent and that exceeded the minimum standard for Medicaid health plans in the state.
Manual Claims Acquisition (Paper) Network providers unable to submit claims via EDI can submit paper claims to Aetna Better Health’s designated post office box. Each business day, our imaging contractor, FutureVision, retrieves, opens and sorts the mail using our pre-defined criteria for either imaging and scanning or distribution directly to Aetna Better Health. FutureVision assigns each claim a unique reference number based on the date received and use it to track the claim throughout the entire adjudication process. FutureVision then converts the imaged data into an EDI ready format within 24 to 48 hours of receipt and forwards it to Aetna Better Health. Each business day, Aetna Better Health’s claims processing personnel upload that data into QNXT™ via EDI processing, where it is accessible to users with approved, secure access to claims information.
Importantly, FutureVision is unable to scan certain documents, including non-claim submissions (e.g., returned member/network provider mail, explanations of benefits, checks, medical records documentation) and certain paper claims (e.g., illegible claims or poor quality printed claims). FutureVision forwards these documents to Aetna Better Health’s Claims Administration Department, where they are sorted and distributed to the appropriate department(s). When claims-related, each document is immediately assigned a unique reference number, scanned, indexed for ready retrieval and keyed into QNXT™. Upon successful validation within both Aetna Better Health’s imaging system and QNXT™, the hard copy is shredded and disposed of in accordance with policy.
Claims Adjudication Processes Auto Adjudication Aetna Better Health’s IT Department runs batch processes on a daily basis against a comprehensive set of edits that we individually configure based on contractual and regulatory requirements. In 2010, our Arizona affiliate, Mercy Care Plan, auto adjudicated over 75 percent of claims without manual intervention. This rules-based system [QNXT™] allows for setting multiple edits to test claim validity and to determine if claims are paid or denied appropriately. These edits include, but are not limited to:
• Member eligibility
• Covered/non-covered services
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
3
Part Two: Technical Proposal
Section Q: Claims Management
• Required documentation
• Services within the scope of the network provider’s practice
• Duplication of services
• Prior authorization
• Invalid procedure codes
• Services in excess of benefit limitations
• Services in excess of lifetime benefits
Based on these and other system edits, claims are systematically processed to either a pay, deny or pend status. Those marked “pay” or “deny” are processed in the course of Aetna Better Health’s weekly financial cycle, wherein we generate, print and mail payments and corresponding remittance advices to the submitting provider(s), including the minimum required data elements and HIPAA compliant remit comments. Remittance data is also available via AboveHealth®, Aetna Better Health’s secure provider Web portal and, by request, in HIPAA 835 format. In some instances, we also provide electronic remittance advices to providers that include all fields required for compliance with the HIPAA 835 format.
Ideally, all claims are “clean claims” and can be processed without the need for additional investigation or information from the service provider or third party. In those instances when a claim cannot be adjudicated as a result of insufficient information, the claim is marked “deny,” and returned to the submitting provider with an appropriate remit comment. When the claim is resubmitted with the required information, the original claim is then adjusted for payment per our adjudication rules.
Manual Adjudication of Pended Claims Aetna Better Health assigns a “pend” status to any claim requiring internal attention, such as provider verification, authorization, medical review and/or COB. These pended claims are sent to the appropriate department for research and resolution. For example, should a claim require review for outlier consideration, claims analysts will send the claim to the Medical Management Department, which will then make a determination as to whether the claim will be paid or denied. Once a determination is made, the claim is then sent back to Claims Administration for processing. Should a pended claim assigned to a department other than Claims remain unresolved beyond the required timeframe, the Claims Supervisor will contact the respective department to determine the cause.
In some instances, as in the case of a claim with an Explanation of Benefits attached, pended claims become the responsibility of our own claims analysts, who then manually adjudicate them using a comprehensive set of documented desktop procedures. Regardless of the department assigned, tracking tools and reports provide Claims Supervisors the means to monitor and control the process.
Claims Inventory and Workflow Management Aetna Better Health is committed to achieving the highest level of timeliness in the claims adjudication and payment process. This is accomplished through focused claims inventory and workflow management practices, data monitoring and analysis and management oversight.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
4

Part Two: Technical Proposal
Section Q: Claims Management
As mentioned above, we utilize a suite of tools, scheduled and ad hoc reports to monitor claim receipts, automated claims processing, manual claims adjudication and check and remittance advice production/distribution on a daily, weekly and monthly basis to provide timely claim payment. These tools and reports include, but are not limited to:
• Pended Claims Tool and Reports – Claims and other departments use the pended claims tool to track and manage claims that edit out of the auto adjudication process for manual review. Populated hourly, the tool presents claims counts and billed dollars by pend reason and claim age, with drill down capabilities to detailed information on each claim. The tool can sort and filter the data by claim age, claim type, claim form, network provider, and contract. Additionally, daily reports of pended claims inventory are generated for managerial or historical review.
• Unfinished Claims Tool and Reports – Claims and other departments use the unfinished claims tool to track and manage all claims that are in process, whether a system batch process or pended for manual review and adjudication. Populated hourly, the tool presents claims counts by process status and claim age, with drill down capabilities to detailed information on each claim. Reports can sort and filter by claim age, claim type, claim form, network provider, and contract. Additionally, daily reports of pended claims inventory are generated for managerial or historical review.
• Claims Payment Processing Reports – Finance and Information Technology Departments generate and monitor several process control reports to achieve timely and accurate network provider check and remittance advice production and distribution, whether by mail or electronic funds transfer/electronic remittance advice file. The reports reconcile, through each major process step, the claim counts and amounts from claims waiting payment to payment and remittance advice distribution.
• Claims Awaiting Payment Forecast – The Claims Department uses the claims awaiting payment forecast report to predict claims payment turnaround times based on current inventory and future check dates, initiating additional actions as necessary to achieve our claim payment timeliness regulatory requirements.
Monitored daily, Aetna Better Health’s Claims Management uses these and other tools and reports to proactively manage the claim workflow and our comprehensively trained personnel to achieve our claims timeliness requirements. If our reports reflect a less than favorable trend, such as during a period of unusual high claim receipts, Claims and other departments work aggressively to address our inventories. We immediately develop and implement action plans, which may include one or more of the following: staff overtime, workload balancing with other Aetna Better Health Medicaid managed care plans and Aetna Medicaid operations personnel, temporary personnel, or increase utilization of overflow vendors to assist with the reduction of claim inventories. Additionally, if claim receipt trends and forecasts indicate, Aetna Better Health’s Claims Department will hire and train additional claims personnel in anticipation of increased claim receipts.
On a daily, weekly and monthly basis, we utilize a suite of tools, scheduled and ad hoc reports, claims processing and results data and claims payment feedback from network providers to further support timely claim payment. These tools and reports include, but are not limited to:
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
5

Part Two: Technical Proposal
Section Q: Claims Management
• Deny Analysis – The Claims Department uses the deny claims analysis tool to evaluate all deny status claims that are currently awaiting payment, identifying and investigating abnormal denial patterns. The tool presents claims counts for all claims in a deny status by network provider and denial reason, with drill down capabilities to detailed information on each claim.
• Denial Diagnostics – Claims and other departments use the denied claims analysis tool to evaluate denied claims, trending and evaluating the claims with their corresponding denial reason, investigating abnormal fluctuations or high levels of denied claims. The tool presents denied claims counts and billed amounts with denial reasons by network provider, contract and QNXT™ adjudication edit, with drill down capabilities to detailed information on each claim.
• Network Provider Inquiry Tracking – Claims and other departments use the network provider inquiry tracking tool to monitor, manage, and trend network providers claim inquiries, requests and complaints. The tool presents network provider call counts by network provider, reason, and age, with drill down capabilities to detailed information regarding the call and, when provided, the claim number.
Aetna Better Health’s Claims Department and other departments use these tools and reports to proactively manage and to improve our claims payments. If our reports indicate a claims payment issue, our Claims Department investigates and corrects the claim payment, either prior to the initial payment or post-payment. If the issue requires a systemic solution beyond the immediate actions of the Claims Department, an interim solution permitting claims payment is implemented whenever possible until the systemic issue is resolved.
Claims Adjudication Audit and Quality Review: Aetna Better Health adheres to the following standards with regard to claims accuracy:
• Procedural: 95 percent accuracy (determined by the number of claims processed correctly divided by the total number of claims)
• Payment: 98 percent accuracy (determined by the total number of claims paid without dollar errors divided by the total number of claims paid)
• Financial: 99 percent accuracy (determined by total claim dollars paid correctly divided by the total paid claim dollars)
To support these high standards, a random two percent of all adjudicated claims are reviewed on a daily basis. The Quality Review (QR) Unit within the Claims Department conducts all claim audits, using desktop procedures (desktop procedures are detailed instructions for the claims analyst) as their guide.
To further minimize the impact of inaccurate data, daily focused audits are conducted on all claims with billed charges equal to or greater than $50,000. Non-finalized claims with errors are pended for correction prior to the finance payment process. Finalized claim with identified errors are adjusted retrospectively.
New claims analysts have an increased amount of claim audits conducted over the course of their first month following training, starting at 100 percent and decreasing to the standard two percent if they meet the claims accuracy standards defined above.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
6
Part Two: Technical Proposal
Section Q: Claims Management
Aetna Better Health performs internal reviews of check payments on a weekly basis. A statistically valid sample of claims are selected and reviewed against the applicable network provider contract. In addition, Aetna Better Health performs a review of all high dollar claims and performs an audit for appropriate billing prior to the payment of the claims.
Overpayment and Underpayment of Claims Overpayment and underpayment of claims is identified through QNXT™ system edits; audit activities; and information received from network providers and members. When an overpaid/underpaid claim is identified, the claim is reversed or, reversed and reprocessed. The reversed or reprocessed claim is listed on the network provider’s remittance advice with a remark indicating that the claim (and the check) has been adjusted and the reason for the adjustment. Recouped amounts, if necessary, are credited to the specific claim in the network provider’s claim history; underpaid amounts are reimbursed to the network provider either via check or future remittance advice.
Remediation Process for Manual Adjudication Any claims analyst that fails to meet any of the accuracy levels (payment, procedural or financial) for a given month, receives a documented verbal coaching from the Supervisor. The employee is informed that their quality percentage has dropped below the acceptable rate and is given one month to show improvement. At the end of the month following notification, if there is no noticeable improvement, the employee is provided with a written quality improvement plan. This process can involve additional training and increased audit activity to see that the claims analyst is meeting the required accuracy standards. Failure of any claims analyst to improve substandard accuracy results in further disciplinary action, up to termination.
Remediation Process for Auto Adjudication System Issue Identification Forms (IIF) are submitted to the Business Application Management (BAM) Department for investigation of any suspected system issue. This department conducts a root cause analysis by performing the necessary research, validating the contract or source document against the current system configuration. If a setup issue is discovered, corrections are made and any incorrectly processed claims are identified via a query and forwarded back to the Claims Department for adjustment activities. If appropriate, BAM Department leadership will provide staff coaching and additional training, update the BAM training program, improve configuration methodologies and testing procedures and/or submit product enhancement requests to the TriZetto Group, designer of the QNXT™ application platform.
Management Oversight Aetna Better Health senior leadership reviews claim performance, on a regular basis, addressing any outstanding claim issues or trends as needed. This monitoring includes a weekly CFO review of claims awaiting payment and a monthly CEO review of the claims key indicator reports. Additionally, our operations management team meets weekly. This cross functional team includes Representatives from several disciplines, including network provider services, network provider information management, information technology, finance, claims, business application management and medical management. This meeting includes a standing agenda item for the review of claims inventories, claim payment forecasts, and action planning, when necessary, to achieve timely payment of claims. We have reviewed the claims timeliness standards for DHH and anticipate no problem meeting these requirements.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
7

Part Two: Technical Proposal
Section Q: Claims Management
Claims Performance Measures Aetna Better Health does not differentiate between in-network and out-of-network providers with regard to timeliness of claims payment requirements, holding us to the same performance standards for both. In- and out-of-network providers alike, we measure several claim key indicators, reporting our performance to DHH as required. This key indicator, as well as our respective performance with regard to each over the past 12 months has been stellar.
This outstanding performance speaks to the excellent service which DHH and Aetna Better Health members receive from Aetna Better Health and our operations personnel.
Related Claims Processing and Management Information System Functions Aetna Better Health maintains claims processing activities that include the application of comprehensive clinical and data related edits supporting the efficient, effective adjudication of claims. QNXT™, our core claims adjudication application, has data related edits configured within its software and is supplemented by two clinical claims editing solutions. The first of the two clinical claims editing solutions, iHealth Technologies’ (iHT) Integrated Claims Management Services (ICM Services), applies select payment policies from one of the industry’s most comprehensive correct coding and medical policy content libraries. The second, McKesson’s ClaimCheck®, expands upon those capabilities by enabling our claims management team to define and combine specific claims data criteria, such as provider or diagnosis, to set up unique edits that deliver enhanced auditing power.
The three applications utilize historic and “new day” claims information to detect questionable billing practices, such as new patient billing codes submitted by the same provider for the same member within a six month period. These applications also assist in identifying fraudulent and abusive billing patterns by generating reports that indicate trending and outliers of provider billing behavior. Inbound claims are initially checked for items such as member eligibility, covered services, excessive or unusual services for gender or age (e.g. “medically unlikely”), duplication of services, prior authorization, invalid procedure codes, and duplicate claims. Claims billed in excess of $50,000 are automatically pended for review, as are any requiring additional documentation (e.g. medical records) in order to determine the appropriateness of the service provided. Professional claims that reach an adjudicated status of “Pay” are automatically reviewed against nationally recognized standards such as the Correct Coding Initiative (CCI), medical policy requirements [e.g., American Medical Association (AMA)], and maximum unit requirements supplied by DHH, with recommendations applied during an automatic re-adjudication process. Other methodologies utilized throughout the auto-adjudication process include, but are not limited to, Multiple Surgical Reductions and Global Day E & M Bundling.
QNXT™ Data Edits QNXT™ has over 400 business rules that Aetna Better Health configures to support enforcement of our claims Policies and Procedures (P&Ps). The application of specific conditions, restrictions, and validation criteria promote the accuracy of claim processing against DHH standards. The edits can result in claims pending or denying depending on the editing logic. For example, if the member is not eligible on the date of service, QNXT™will automatically deny the claim. In the event that the category of service of the provider of record does not match the procedure code billed the claim will pend for manual review to validate accuracy of provider set-up.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
8

Part Two: Technical Proposal
Section Q: Claims Management
Examples of data edits specific to QNXT™ include the following:
Benefits Package Variations QNXT™ automatically analyzes CPT, REV, and HCPC codes to determine whether specific services are covered under the contract or benefit rules. If services are not covered, the system will automatically deny the respective claim line. The claim line will deny with the appropriate HIPAA remittance remark on the EOB.
Data Accuracy QNXT™ is continually updated based on the most current code sets available (HCPCS, REV, CPT codes) by year. As new codes are added, terminated, or changed, we update the codes in QNXT™ so the system is always in compliance with HIPAA standards. If a network provider bills a code that has been terminated, QNXT™ will deny the claim line and advise the provider the code is invalid via remittance advice.
Adherence to Prior Authorization Requirements QNXT™ is configured to enforce the supporting documentation requirements of certain services. In addition, QNXT™ has the ability to configure Prior Authorization (PA) by code, provider type, and place of service. QNXT™ is configured to automatically identify certain types of authorizations for medical director review. Claim edit rules are set to validate the claim against the network provider, member, dates of service, services rendered, and units authorized.
Provider Qualifications QNXT™ provider files are configured by specialty and category of service. This allows for the enforcement of categories of service and provider type on claims validation. Certain procedures can only be performed by select network provider types. For example, QNXT™ will not permit the processing of a claim for in-office heart surgery by a podiatrist. iHealth lends additional support in this regard, reviewing any claim line set to “Pay” for billing appropriateness by specialty. QNXT™ checks other provider-specific items as well, verifying, for example, that each provider has obtained the requisite National Provider Identifier (NPI) or its equivalent and included the identifier on all claims submissions.
Member Eligibility and Enrollment QNXT™ validates the date of service against the member’s enrollment segment to determine if the member was eligible on the date of service. If the member was not eligible on the date of service, the system will automatically deny the claim using the appropriate HIPAA approved remittance comment.
Duplicate Billing Logic QNXT™ uses a robust set of edits to determine duplication of services. Examples are same member, same date, same network provider, same service, or any combination of these criteria. In addition, claim lines set to “Pay” are subjected to iHealth’s duplicate logic. This logic protects against Aetna Better Health paying for services rendered by the same physician or other physicians within the same provider group
ClaimCheck® Edits ClaimCheck® is a comprehensive code auditing solution that supports QNXT™ by applying expert industry edits from a provider recognized knowledge base to analyze claims for accuracy
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
9

Part Two: Technical Proposal
Section Q: Claims Management
and consistency with Aetna Better Health’s P&Ps. ClaimCheck® clinical editing software identifies coding errors in the following categories:
• Procedure unbundling
• Mutually exclusive procedures
• Incidental procedures
• Medical visits, same date of service
• Bilateral and duplicate procedures
• Pre and Post-operative care
• Assistant Surgeon
• Modifier Auditing
• Medically Unlikely
Aetna Better Health offers network providers access to Clear Claim Connection®, a provider reference tool that helps providers optimize their claims submission accuracy. Currently there are 2300 provider groups registered to use this web-based tool that providers can use to understand Aetna Better Health’s clinical editing logic. This allows them to better understand the rules and clinical rationale affecting adjudication. Providers access Clear Claim Connection® through Aetna Better Health’s web portal via secure login. Various coding combinations can then be entered to determine why, for example, a particular coding combination resulted in a denial. The provider may also review coding combinations prior to claim submission, to determine if applicable auditing rules and clinical rationale will deny the claim before it is submitted.
iHealth Edits iHealth clinically edits claims to assist Aetna Better Health to promote the proper and fair payment of professional DME and outpatient claims.
Coding Accuracy If the services are up-coded, or unbundled, iHealth will alert the Claims Department to deny the claim line along with the specific clinical editing policy justification for the denial. The claim line will deny with the appropriate HIPAA remittance remark on the Explanation of Benefits (EOB).
Duplicate Billing Logic In addition, claim lines set to “Pay” are subjected to iHealth’s duplicate logic. This logic protects against Aetna Better Health paying for services rendered by the same physician or other physicians within the same provider group
Durable Medical Equipment (DME) Editing iHealth Technologies’ (iHT) performs edits related to select DME payment policies that align with ALTCS covered service policies. These DME edits include but are not limited to; DME rentals, oxygen and oxygen systems, hospital beds and accessories, external infusion pumps and anatomic/functional modifiers required for DME services.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
10

Part Two: Technical Proposal
Section Q: Claims Management
Procedure Code Guidelines - iHealth Aetna Better Health follows the AMA CPT-4 Book and CMS HCPCS Book, which both provide instructions regarding code usage. iHT has developed these guidelines into edits. For example, if a vaccine administration code is billed without the correct vaccine/toxoid codes, Aetna Better Health would then deny the code as inappropriate coding based on industry standards. According to the AMA CPT Book, this vaccination must be reported in addition to the vaccine and toxoid code(s).
Procedure Code Definition Policies - iHealth iHT supports correct coding based on the definition or nature of a procedure code or combination of procedure codes. These editing policies will either bundle or re-code procedures based on the appropriateness of the code selection. For example, if a provider attempts to unbundle procedures, iHT will apply editing logic that will bundle all of the procedures billed into the most appropriate code. For example, if a provider bills an office visit and also bills separately for heart monitoring with a stethoscope at the same visit, iHT will rebundle the service into the appropriate E&M or office code.
Fraud & Abuse Aetna Better Health’s Fraud and Abuse Department, under the direction of the VP of Health Plan Operations, utilizes claims payment tracking and trending reports, claims edits, audits and provider billing patterns as indicators of potential fraud and abuse. The Fraud and Abuse Department uses this information to detect aberrant provider billing behavior, prompting additional analysis and investigation. Aetna Better Health fraud and abuse personnel work in conjunction with Aetna Better Health’s Provider Services and Compliance Departments to address the questionable behavior(s) through provider education and outreach. If Aetna Better Health becomes aware that an incident of potential/suspected fraud and abuse has occurred, internal P&Ps mandate that we report the incident to DHH within 10 business days of discovery by completing and submitting the confidential DHH Referral for Preliminary Investigation form.
Claims Education Aetna Better Health’s Provider Claims Educator works to educate contracted and non-contracted providers on appropriate claims submission requirements, coding updates and available resources, such as provider manuals, websites, fee schedules, etc. In addition, the Provider Claims Educator will participate in any DHH workgroup tasked with developing uniform guidelines for standardizing hospital outpatient and outpatient provider claim requirements, sharing information with providers accordingly.
Claims Editing Results In calendar year 2010, due to our robust and comprehensive claims editing programs, Aetna Better Health cost avoided/recovered in excess of seventeen million dollars related to the ALTCS program.
Use of iHealth Technologies to Detect Questionable Billing Practices QNXT™ is supplemented by an Integrated Claims Management Services (ICM Services) powered by iHealth Technologies (iHT). This software is seamless to the network provider and allows consistent and accurate administration of claims adjudication policies. Professional claims that reach an adjudicated status of “pay” are automatically reviewed against nationally
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
11

Part Two: Technical Proposal
Section Q: Claims Management
recognized standards such as the Correct Coding Initiative (CCI) and recommendations applied during an automatic re-adjudication process.
The QNXT™ and Integrated Claims Management applications utilize historical claims information to detect and correct questionable billing practices and assist in identifying fraudulent and abusive patterns. Professional claims that reach an adjudicated status of “pay” receive a Correct Coding Initiative (CCI) control edit. These edits include, but are not limited to:
Member Eligibility The QNXT™ adjudication system validates the date of service against the member’s enrollment segment to determine if the member was eligible on the date of service. If the member was not eligible on the date of service, the system will automatically deny the claim using the appropriate HIPAA approved remittance comment.
Covered/Non-Covered Services The QNXT™ system automatically determines if specific services using the CPT, REV or HCPC codes are covered under the contract or benefit rules of the DHH plan. If services are not covered, the system will automatically deny that claim line. If the services are up-coded, or unbundled, iHealth will send a recommendation back to deny the claim line along with the specific reason why. The claim line will deny with the appropriate HIPAA remittance remark on the EOB.
Required Documentation The QNXT™ system is configured, for certain services, to require additional documentation before the claim can be adjudicated. For example, a signed consent form is required documentation for sterilization procedures.
Services within the Scope of the Network Provider’s Practice The QNXT™ system is configured by specialty to allow certain procedures to only be performed by selected network provider types. For example, the system does not permit a claim for heart surgery performed in-office by a podiatrist to be processed. In addition to the QNXT™ system, iHealth also reviews claim lines which are set to pay for network provider billing appropriateness by specialty.
Duplication of Services The QNXT™ system has a very robust set of edits to determine duplication of services. Examples are same member, same date, same network provider, same service or any combination of these criteria. In addition, claim lines set to pay will go through the iHealth duplicate logic which will review services rendered by any other physician within the group affiliation for duplicate billings.
Prior Authorization The QNXT™ system has a separate configuration for prior authorization (PA) templates and associated service groups for PA. This allows for flexibility when creating authorizations, which can be accomplished at the code level if needed. The system is organized to automatically identify certain types of authorizations for medical director review. Claim edit rules are set to validate the claim against the network provider, member, dates of service, services rendered and units authorized.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
12

Part Two: Technical Proposal
Section Q: Claims Management
Invalid Procedure Codes QNXT™ reference files are configured by year and procedure code. As new codes are added, terminated or changed, we update the codes in the system so that the system is always in compliance with HIPAA standards. If a network provider bills a code that has terminated, the system will deny the claim line and advise the network provider the code is invalid.
Liability Management Practices Aetna Better Health utilizes generally accepted actuarial practices to estimate its unpaid claim liability. Each month, a query is run to extract paid claims by month of service, month of payment, and category of expense. The paid claims extract is reconciled against the check register and is compared to the previous month's extract to validate the data. Then, for each category a completion factor is calculated for each month of service and is applied to the claims paid to date to develop the estimate of ultimate incurred claims for that month. Results are then aggregated across all months of service and all categories of expense. Adjustments for any known liabilities are added as appropriate (for example, a long hospital stay that is known but for which a bill has not yet been received). A margin is added, and the final result is the estimate of Incurred But Not Paid Claims.
Estimated liabilities for Received But Unadjudicated Claims are determined by applying historical factors to the billed charges for these claims. If the estimated liability is high enough to warrant an adjustment to the unpaid claim liability, such an adjustment is made. Incurred But Not Reported Claims are simply the difference between Incurred But Not Paid Claims and Received But Unadjudicated Claims.
Aetna Better Health’s corporate valuation actuary makes an independent estimate of Incurred But Not Paid Claims each month. This estimate is compared to Aetna Better Health's estimate, and consensus is reached on the appropriate value to use.
Retrieval and Integration of Enrollment/Eligibility Data: Aetna Better Health has over 10 years’ experience successfully managing plan membership, as well as a comprehensive system in place that enables us to efficiently resolve discrepancies in membership data. The purpose of reconciling the member file is to maintain correct member eligibility information at all times and pay only for services provided to eligible members. With the eligibility file kept current, capitated network providers are neither overpaid nor underpaid and the eligibility information transferred to subcontractors is correct. Maintaining accurate membership files allows Aetna Better Health to easily reconcile monthly premium payments from the State to the information in QNXT™. It is important that all eligibility segments be recorded in QNXT™ correctly so that medical services are paid only when appropriate.
QNXT™, Aetna Better Health’s client/server-based managed care information system, serves as the backbone of our ECM functionality. QNXT™ is used to synthesize the online, phone-based, EFT and ACH capabilities that provide our network providers a comprehensive, cohesive and automated means of claims submission, monitoring and payment. We focus here on those services made available to our network providers by our Claims Inquiry Claims Research (CICR) Line and AboveHealth®, Aetna Better Health’s HIPAA-compliant secure Web portal for providers.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
13

Part Two: Technical Proposal
Section Q: Claims Management
Aetna Better Health’s Claims Department maintains a Claims Inquiry Claims Research (CICR) Line, a toll-free number that network providers are free to call between the hours of 6:00 a.m. and 5:00 p.m. to speak with claims research line personnel.
CICR Representatives are specifically designated to answer provider phone inquiries regarding claims status, track those inquiries within QNXT™’s Call Tracking functionality and provide status and/or process adjustments to previously processed claims accordingly. If a single inquiry results in more than three adjustments, the issue is call tracked, by way of QNXT™, to a research and adjustment analyst for processing so that CICR Representatives can remain available to answer provider calls. For every non-status call (requires further action/research) received, a call tracking issue must be opened.
Whenever possible, CICR Representatives resolve provider inquiries in the course of a call. However, in those rare instances when this is not possible, the issue is resolved within seven calendar days. CICR Representatives and Supervisors monitor Call Tracking reports daily to maintain resolution time standards.
With regard to online claims status capabilities, AboveHealth® supports communication between Aetna Better Health and our network providers in a multitude of ways, among them extensive online support of the claim status function. As the screenshots that follow demonstrate, network providers can, at any time, login to AboveHealth®, navigate to the Claim Status Search page, search on multiple criteria, then view and print their search results.
AboveHealth® Network Provider Claim Status Search Page
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
14

Part Two: Technical Proposal
Section Q: Claims Management
Claims Status Search Results (by Network Provider)
Claims Detail
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
15

Part Two: Technical Proposal
Section Q: Claims Management
Claims Status Detail Report (Printable)
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
16

Part Two: Technical Proposal
Section Q: Claims Management
Provider Training and Education For those network providers wishing to take advantage of AboveHealth®’s online claims status inquiry capabilities, Aetna Better Health offers a variety of training opportunities, including, but not limited to the following:
• Orientation sessions
• Distribution of written materials through mailings and on our Website
• Training during scheduled site visits
• Regularly scheduled provider training forums and meetings
• In-person training sessions at provider offices.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
17

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
De
lawar
e Fl
orid
a Ma
rylan
d Re
quire
men
t Me
ets o
r Exc
eeds
Req
uire
men
t Ex
plan
atio
n
17 C
laim
s Man
agem
ent
17.1
Elec
troni
c Clai
ms M
gmt F
unct
iona
lity
17.1.
1 The
Coo
rdina
ted C
are N
etwor
k (CC
N) sh
all
annu
ally c
omply
with
DHH
’s El
ectro
nic C
laims
Da
ta Int
erch
ange
polic
ies fo
r cer
tifica
tion o
f ele
ctron
ically
subm
itted c
laims
.
Meets
Me
ets
Meets
Tw
o app
licati
ons p
rovid
e for
Aetn
a Bett
er H
ealth
’s co
ntinu
ed
comp
lianc
e with
contr
actin
g stat
es’ E
lectro
nic C
laims
Data
Int
erch
ange
polic
ies fo
r cer
tifica
tion o
f elec
tronic
ally s
ubmi
tted
claim
s: 1)
Micr
osoft
BizT
alk w
ith H
IPAA
Acc
elera
tor™
is a
data
trans
forma
tion a
pplic
ation
that
trans
lates
data
to an
d fro
m the
full
spec
trum
of HI
PAA
trans
actio
ns se
ts in
a high
ly cu
stomi
zable
, fle
xible,
and r
obus
t ser
ver-b
ased
envir
onme
nt. 2)
Was
hingto
n Pu
blish
ing C
ompa
ny (W
PC) I
mplem
entat
ion G
uide s
chem
as fo
r ea
ch H
IPAA
ANS
I X12
tran
sacti
on ar
e emb
edde
d dire
ctly w
ithin
the ap
plica
tion e
ngine
, inclu
ding a
facil
ity to
upda
te the
se
sche
mas a
utoma
ticall
y as t
he tr
ansa
ction
sets
are u
pdate
d ove
r tim
e. Ad
dition
ally,
Fore
sight’
s HIP
AA V
alida
tor™
, InSt
ream
™, is
a ful
ly fun
ction
al HI
PAA
editin
g and
valid
ation
appli
catio
n. It v
alida
tes
HIPA
A tra
nsac
tions
thro
ugh a
ll sev
en le
vels
of ed
its as
defin
ed
by th
e Wor
kgro
up fo
r Elec
tronic
Data
Inter
chan
ge an
d Stra
tegic
Natio
nal Im
pleme
ntatio
n Pro
cess
(WED
I/SNI
P), h
as al
l stan
dard
HI
PAA
code
sets
embe
dded
, and
supp
orts
custo
m, tr
ading
-pa
rtner
-spec
ific co
mpan
ion gu
ides a
nd va
lidati
on re
quire
ments
. Ae
tna B
etter
Hea
lth fo
llows
the S
trateg
ic Na
tiona
l Imple
menta
tion
Proje
ct (S
NIP)
reco
mmen
datio
ns fo
r tes
ting c
reate
d by t
he
Wor
kgro
up fo
r Elec
tronic
Data
Inter
chan
ge (W
EDI),
furth
er
prom
oting
syste
m co
mplia
nce w
ith fe
dera
l IT m
anda
tes.
17.1.
2 To t
he ex
tent th
at the
CCN
comp
ensa
tes
prov
iders
on a
fee-fo
r-ser
vice o
r othe
r bas
is re
quirin
g the
subm
ission
of cl
aims a
s a co
nditio
n of
Meets
Me
ets
Meets
QN
XT™
, Aetn
a Bett
er H
ealth
's co
re tr
ansa
ction
proc
essin
g sy
stem,
comp
rises
28 in
tegra
ted m
odule
s tha
t main
tain t
he
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
18

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
paym
ent, t
he C
CN sh
all pr
oces
s the
prov
ider’s
cla
ims f
or co
vere
d ser
vices
prov
ided t
o mem
bers,
co
nsist
ent w
ith ap
plica
ble C
CN po
licies
and
proc
edur
es an
d the
term
s of th
e Con
tract
and t
he
Syste
ms G
uide,
includ
ing, b
ut no
t limi
ted to
, time
ly fili
ng, a
nd co
mplia
nce w
ith al
l app
licab
le sta
te an
d fed
eral
laws,
rules
and r
egula
tions
.
follow
ing:
● Cl
aims d
ata, in
cludin
g ass
ociat
ed ad
judica
tion,
COB
and
TPL p
roce
sses
●
Demo
grap
hic, e
ligibi
lity an
d enr
ollme
nt da
ta, in
cludin
g prio
r co
vera
ge
● Pr
ovide
r con
tract
confi
gura
tion,
includ
ing ne
twor
k and
se
rvice
s ●
EDI p
roce
sses
●
QM/U
M inc
luding
, but
not li
mited
to P
rior A
uthor
izatio
ns an
d co
ncur
rent
revie
ws
Unde
r the
dire
ction
of th
e Dire
ctor o
f Bus
iness
App
licati
on
Mana
geme
nt (B
AM),
Aetna
Bett
er H
ealth
's BA
M De
partm
ent is
re
spon
sible
for:
● De
signin
g and
docu
menti
ng th
e ove
rall c
onfig
urati
on an
d ru
les ne
eded
for t
he Q
NXT™
build
. ●
Load
ing th
e rule
s and
requ
ireme
nts of
any n
ew he
alth p
lan,
prod
uct o
r bus
iness
func
tion i
nto Q
NXT™
, inclu
ding e
ligibi
lity
file la
yout,
prov
ider c
ontra
cts, fe
e sch
edule
s and
mem
ber
bene
fits an
d prio
r auth
oriza
tion r
equir
emen
ts. T
his w
ill all
ow
for th
e cap
ture,
proc
essin
g and
stor
age o
f all d
ata el
emen
ts re
quire
d by D
HH fo
r enc
ounte
r data
subm
ission
as st
ipulat
ed
in thi
s Sec
tion o
f the R
FP an
d the
Sys
tems G
uide.
● Va
lidati
ng th
e ove
rall q
uality
, time
lines
s and
accu
racy
of th
e QN
XT™
buil
d. ●
Partic
ipatin
g in t
he cl
aims p
roce
ssing
syste
m un
it tes
ting w
ith
our O
pera
tions
Pro
cess
and K
nowl
edge
Man
agem
ent
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
19

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
(OPK
M) D
epar
tmen
t and
wor
king t
o res
olve a
ny is
sues
. ●
Partic
ipatin
g in e
nd to
end t
estin
g with
end u
sers;
reso
lving
an
y iss
ues d
uring
imple
menta
tions
and m
ajor s
ystem
up
grad
es.
QNXT
™, in
conju
nctio
n with
the d
ocum
ent s
cann
ing an
d OCR
fun
ction
ality
affor
ded b
y Futu
reVi
sion,
our d
ocum
ent
mana
geme
nt so
lution
vend
or, p
rovid
es fo
r the
subm
ission
and
proc
essin
g of n
on-e
lectro
nic an
d elec
tronic
claim
s by c
ontra
cted
prov
iders.
QN
XT's™
inter
faces
with
Abo
veHe
atlh,
our s
ecur
e web
porta
l, in
addit
ion to
our A
vaya
phon
e sys
tem, p
ermi
t pro
vider
s on-
line a
nd
phon
e-ba
sed a
cces
s to c
laim
proc
essin
g stat
us in
forma
tion.
17.1.
3 The
CCN
shall
main
tain a
n elec
tronic
cla
ims m
anag
emen
t sys
tem th
at wi
ll: Me
ets
Meets
Me
ets
See b
elow:
17.1.
3.1 U
nique
ly ide
ntify
the at
tendin
g and
billin
g pr
ovide
r of e
ach s
ervic
e; Me
ets
Meets
Me
ets
QNXT
™, A
etna B
etter
Hea
lth’s
claim
s pro
cess
ing sy
stem,
utiliz
es
prov
ider s
electi
on lo
gic pr
ovidi
ng fo
r the
uniqu
e ide
ntific
ation
of
the at
tendin
g and
billin
g pro
vider
for e
ach s
ervic
e.
17.1.
3.2 Id
entify
the d
ate of
rece
ipt of
the c
laim
(the d
ate th
e CCN
rece
ives t
he cl
aim an
d en
coun
ter in
forma
tion)
;
Exce
eds
Exce
eds
Exce
eds
QNXT
’s™ c
ore f
uncti
onali
ty re
cord
s the
date
any c
laim
or
enco
unter
infor
matio
n is r
eceiv
ed.
17.1.
3.3 Id
entify
real-
time a
ccur
ate hi
story
with
dates
of ad
judica
tion r
esult
s of e
ach c
laim
such
as
paid,
denie
d, su
spen
ded,
appe
aled,
etc., a
nd
follow
up in
forma
tion o
n app
eals;
Exce
eds
Exce
eds
Exce
eds
Data
histor
y is n
ot pu
rged
in su
ppor
t of r
etriev
al/re
view
of ac
cura
te an
d com
preh
ensiv
e clai
m his
tory p
rofile
s, e.g
. hist
orica
l da
ta of
paid,
denie
d, an
d sus
pend
ed cl
aims.
(Note
that
appe
aled
claim
data
is no
t stor
ed in
the c
laim’
s sys
tem an
d ins
tead i
s sto
red i
n the
appe
als da
tabas
e). T
he ge
nera
l and
admi
nistra
tive
datab
ase t
rack
s clai
m his
tory a
nd re
lated
adjud
icatio
n res
ults,
thus p
rovid
ing an
adde
d mec
hanis
m for
claim
s hist
ory r
eview
. If
claim
is ad
justed
as th
e res
ult of
an ap
peal,
the a
djustm
ent is
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
20

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
docu
mente
d in t
he C
laims
proc
essin
g sys
tem, a
nd th
at his
tory i
s ma
intain
ed an
d retr
ievab
le.
17.1.
3.4 Id
entify
the d
ate of
paym
ent, t
he da
te &
numb
er of
the c
heck
or ot
her f
orm
of pa
ymen
t su
ch as
elec
tronic
fund
s tra
nsfer
(EFT
);
Exce
eds
Exce
eds
Exce
eds
The c
laims
syste
m is
capa
ble of
trac
king a
nd m
aintai
ning e
ach o
f the
se el
emen
ts, an
d inc
ludes
the a
bility
for p
erso
nnel
to qu
ery
the da
tabas
e for
thes
e spe
cific
eleme
nts.
17.1.
3.5 Id
entify
all d
ata el
emen
ts as
requ
ired b
y DH
H for
enco
unter
data
subm
ission
as st
ipulat
ed
in thi
s Sec
tion o
f the R
FP an
d the
Sys
tems G
uide;
and
Meets
Me
ets
Meets
Ou
r pro
priet
ary E
ncou
nter M
anag
emen
t Sys
tem (E
MS) p
rovid
es
for th
e acc
urate
, time
ly an
d com
plete
subm
ission
of en
coun
ter
data
–inclu
ding a
ll bille
d, pa
id an
d den
ied un
its an
d cha
rges
, as
well a
s the
Nati
onal
Prov
ider I
denti
fier (
NPI)
– to D
HH in
HIP
AA
comp
liant
837(
I/P) f
orma
t. Dev
elope
d with
the f
uncti
onali
ty to
mana
ge en
coun
ter da
ta ac
ross
the e
ncou
nter s
ubmi
ssion
co
ntinu
um –
includ
ing pr
epar
ation
, rev
iew, v
erific
ation
, ce
rtifica
tion,
subm
ission
, and
repo
rting –
the s
ystem
cons
olida
tes
requ
ired c
laims
data
from
multip
le so
urce
s (e.g
. QNX
T™ an
d our
de
legate
d visi
on se
rvice
s pro
vider
) for
all s
ervic
es (in
cludin
g tho
se in
the p
rior p
eriod
) for
whic
h Aetn
a Bett
er H
ealth
incu
rred a
fin
ancia
l liab
ility,
as w
ell as
claim
s for
servi
ces e
ligibl
e for
pr
oces
sing w
here
no fin
ancia
l liab
ility w
as in
curre
d. Co
mpre
hens
ive, c
oord
inated
edits
and w
orkfl
ow m
anag
emen
t too
ls ide
ntify
and a
ddre
ss po
tentia
l data
issu
es at
the e
arlie
st op
portu
nity.
EMS
is co
nfigu
red t
o extr
act th
e clai
m va
lues
nece
ssar
y to p
opula
te a v
alid a
nd ac
cura
te en
coun
ter. T
his
proc
ess w
ill be
deve
loped
using
DHH
’s sp
ecific
codin
g ins
tructi
ons a
nd te
sted f
or ac
cura
cy an
d com
pleten
ess.
Our
enco
unter
syste
m is
custo
m bu
ilt for
the r
equir
emen
ts of
each
sta
te. W
e con
sisten
tly co
llabo
rate
with
the M
edica
id ag
encie
s tha
t con
tract
with
us to
prov
ide m
anag
ed ca
re se
rvice
s. A
s an
exam
ple, th
is co
llabo
ratio
n, ou
r affil
iate i
n Ariz
ona,
Mercy
Car
e Pl
an, w
orkin
g with
the S
tate’s
Med
icaid
agen
cy’s
enco
unter
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
21

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
proc
essin
g unit
, con
tribute
d to t
he su
cces
sful a
ccep
tance
of ov
er
99 pe
rcent
of all
subm
itted e
ncou
nters
in ca
lenda
r yea
r 201
0.
17.1.
3.6 A
llow
subm
ission
of no
n-ele
ctron
ic an
d ele
ctron
ic cla
ims b
y con
tracte
d pro
vider
s. Ex
ceed
s Ex
ceed
s Ex
ceed
s
17.1.
4 The
CCN
shall
see t
hat a
n elec
tronic
claim
s ma
nage
ment
(ECM
) cap
abilit
y tha
t acc
epts
and
proc
esse
s clai
ms su
bmitte
d elec
tronic
ally i
s in
place
.
Meets
Me
ets
Meets
Aetna
Bett
er H
ealth
’s cla
ims m
anag
emen
t sys
tem, Q
NXT™
, pr
ovide
s for
the s
ubmi
ssion
and p
roce
ssing
of el
ectro
nic cl
aims
by co
ntrac
ted pr
ovide
rs via
mult
iple c
learin
ghou
ses.
Prov
iders
may a
lso su
bmit p
aper
claim
s to p
lan-sp
ecific
post
office
boxe
s ad
jacen
t to F
uture
Visio
n, Ae
tna B
etter
Hea
lth’s
docu
ment
imag
ing ve
ndor
, pro
viding
for t
heir p
romp
t con
versi
on to
ele
ctron
ic for
mat a
nd up
load t
o QNX
T™, s
hould
any s
uppo
rting
docu
menta
tion b
e atta
ched
(e.g.
EOB
), the
ir sec
ure d
elive
ry to
the ap
prop
riate
Aetna
Bett
er H
ealth
depa
rtmen
t.
17.1.
5 The
CCN
shall
see t
hat th
e ECM
syste
m fun
ction
s in a
ccor
danc
e with
infor
matio
n exc
hang
e an
d data
man
agem
ent r
equir
emen
ts as
spec
ified
in thi
s Sec
tion o
f the R
FP an
d the
Sys
tems G
uide.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth is
able
to co
mply
with
the in
forma
tion
exch
ange
and d
ata m
anag
emen
t req
uirem
ents
spec
ified i
n this
RF
P an
d the
Sys
tems G
uide.
17.1.
6 The
CCN
shall
see t
hat, a
s par
t of th
e ECM
fun
ction
, it ca
n pro
vide o
n-lin
e and
phon
e-ba
sed
capa
bilitie
s to o
btain
proc
essin
g stat
us in
forma
tion.
Meets
Me
ets
Meets
On
line c
apab
ilities
will
be pr
ovide
d via
Abov
eHea
lth® .
Abov
eHea
lth® i
s a se
cure
HIP
AA-co
mplia
nt we
b por
tal fo
r Aetn
a Be
tter H
ealth
’s me
mber
s and
prov
iders.
Des
igned
to fo
ster o
pen
comm
unica
tion a
nd fa
cilita
te ac
cess
to a
varie
ty of
data
in a
multit
ude o
f way
s, thi
s sec
ure,
ASP-
base
d app
licati
on
sync
hron
izes d
ata on
a da
ily ba
sis w
ith Q
NXT™
thro
ugh d
ata
extra
ct an
d loa
d pro
cess
es, a
llowi
ng pr
ovide
rs to
chec
k elig
ibility
sta
tus, r
eview
bene
fits, e
ncou
nters
and p
rior a
uthor
izatio
n stat
us,
and s
end s
ecur
e ema
ils to
Aetn
a Bett
er H
ealth
.. Ph
one-
base
d ca
pabil
ities f
or cl
aim st
atus a
nd ot
her p
roce
ssing
infor
matio
n will
be av
ailab
le via
our C
ICR.
CIC
R pe
rsonn
el wi
ll be a
vaila
ble fr
om
7 am
to 7 p
m, C
entra
l Tim
e, Mo
nday
thro
ugh F
riday
for p
rovid
er
inquir
ies.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
22

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.1.
7 The
CCN
shall
supp
ort a
n auto
mated
cle
aring
hous
e (AC
H) m
echa
nism
that a
llows
pr
ovide
rs to
requ
est a
nd re
ceive
elec
tronic
fund
s tra
nsfer
(EFT
) of c
laims
paym
ents.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth af
fords
prov
iders
the op
portu
nity t
o rec
eive
paym
ent v
ia dir
ect d
epos
it, or
elec
tronic
fund
tran
sfer (
EFT)
. The
pr
oces
s is a
s foll
ows:
1)
Prov
iders
comp
lete a
n EFT
enro
llmen
t form
(ava
ilable
on
line)
, pro
viding
their
bank
routi
ng an
d acc
ount
numb
ers.
The c
omple
ted fr
om is
faxe
d to o
ur E
DI D
epar
tmen
t. 2)
Ae
tna B
etter
Hea
lth pe
rsonn
el en
ter ea
ch pr
ovide
r’s ro
uting
an
d acc
ount
infor
matio
n into
QNX
T™ an
d des
ignate
them
as
an E
FT pr
ovide
r. 3)
A
test d
ocum
ent c
alled
a “p
re-n
ote” is
sent
to the
prov
ider’s
ba
nk to
see t
hat th
e rou
ting n
umbe
r and
acco
unt n
umbe
r are
ac
cura
te an
d fun
ction
prop
erly.
4)
Up
on ap
prov
al of
the “p
re-n
ote” b
y the
prov
ider’s
bank
, EFT
ca
pabil
ities a
re en
abled
with
in the
resp
ectiv
e Aetn
a Bett
er
Healt
h acc
ounts
. 5)
As
prov
ider p
ayme
nts ar
e gen
erate
d dur
ing th
e che
ck ru
n pr
oces
s, pa
ymen
t infor
matio
n is c
ompil
ed w
ithin
a file
and
queu
ed fo
r sch
edule
d dist
ributi
on to
the a
ssoc
iated
bank
s an
d Auto
mated
Clea
ring H
ouse
s (AC
Hs) f
or pr
oces
sing.
Upon
appr
oval
of the
chec
k run
by th
e hea
lth pl
an, c
heck
s ar
e rele
ased
for p
rintin
g and
ing an
d the
EFT
file i
s re
lease
d to t
he re
spec
tive f
inanc
ial in
stitut
ions.
6)
Prov
iders
rece
ive a
hard
copy
remi
ttanc
e in t
he m
ail de
tailin
g the
claim
s pro
cess
ed in
a pa
rticula
r pay
ment
cycle
and a
pa
per c
opy o
f wha
t wou
ld ha
ve be
en a
chec
k ind
icatin
g the
EF
T ch
eck n
umbe
r and
total
dolla
rs, th
ereb
y allo
wing
them
to
post
paym
ents
appr
opria
tely.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
23

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
Any p
rovid
er ca
n cho
ose t
o stop
EFT
paym
ents
at an
y tim
e and
re
turn t
o pay
ment
by ph
ysica
l che
ck by
conta
cting
the h
ealth
plan
in
writin
g.
17.1.
8 The
CCN
shall
not d
erive
finan
cial g
ain fr
om
a pro
vider
’s us
e of e
lectro
nic cl
aims f
iling
functi
onali
ty an
d/or s
ervic
es of
fered
by th
e CCN
or
a thir
d par
ty. H
owev
er, th
is pr
ovisi
on sh
all no
t be
cons
trued
to im
ply th
at pr
ovide
rs ma
y not
be
resp
onsib
le for
paym
ent o
f app
licab
le tra
nsac
tion
fees a
nd/or
char
ges.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth ac
know
ledge
s and
will
comp
ly. It
has n
ever
be
en A
etna B
etter
Hea
lth’s
busin
ess p
racti
ce to
asse
ss a
fee fo
r su
ch se
rvice
s and
we a
re co
nfide
nt tha
t futur
e bus
iness
prac
tices
wi
ll con
tinue
to su
ppor
t our
prov
iders
in the
ir ado
ption
of E
DI
capa
bilitie
s.
17.1.
9 The
CCN
shall
requ
ire th
at the
ir pro
vider
s co
mply
at all
times
with
stan
dard
ized b
illing
form
s an
d for
mats,
and a
ll futu
re up
dates
for
Profe
ssion
al cla
ims (
CMS
1500
) and
Insti
tution
al cla
ims (
UB 04
).
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth's
Claim
s Edu
cator
prov
ides i
n-ne
twor
k and
ou
t-of-n
etwor
k pro
vider
s (i.e
., pro
fessio
nal a
nd in
stitut
ional)
in-
depth
educ
ation
rega
rding
appr
opria
te cla
ims s
ubmi
ssion
re
quire
ments
, cod
ing up
dates
, elec
tronic
claim
s tra
nsac
tions
and
electr
onic
fund t
rans
fer, a
nd av
ailab
le he
alth p
lan re
sour
ces s
uch
as pr
ovide
r man
uals,
web
sites
, fee s
ched
ules,
and s
o for
th.
Prov
ider c
ontra
cts, in
conju
nctio
n with
initia
l and
ongo
ing pr
ovide
r ed
ucati
on an
d tra
ining
relat
ed to
claim
s req
uirem
ents,
supp
ort
prov
iders'
comp
lianc
e with
rega
rd to
claim
s sub
miss
ion
requ
ireme
nts. P
repr
oces
sing e
dits e
nforce
this
requ
ireme
nt an
d de
ny an
y clai
m su
bmitte
d in a
nons
tanda
rd fo
rmat.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
24

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.1.
10 T
he C
CN m
ust c
omply
with
requ
ireme
nts
of Se
ction
6507
of th
e Pati
ent P
rotec
tion a
nd
Affor
dable
Car
e Act
of 20
10, r
egar
ding “
Mand
atory
State
Use
of N
ation
al Co
rrect
Codin
g Init
iative
s,”
includ
ing al
l app
licab
le ru
les, r
egula
tions
, and
me
thodo
logies
imple
mente
d as a
resu
lt of th
is ini
tiativ
e.
Meets
Me
ets
Meets
QN
XT's™
data
relat
ed ed
its ar
e sup
pleme
nted b
y two
clini
cal
claim
s edit
ing so
lution
s. Th
e firs
t, iHe
alth,
appli
es se
lect p
ayme
nt po
licies
from
one o
f the i
ndus
try’s
most
comp
rehe
nsive
corre
ct co
ding a
nd M
edica
l Poli
cy co
ntent
libra
ries.
The s
econ
d, Mc
Kess
on’s
Claim
Chec
k®, e
xpan
ds up
on th
ose c
apab
ilities
by
enab
ling o
ur cl
aims m
anag
emen
t team
to de
fine a
nd co
mbine
sp
ecific
claim
s data
crite
ria, s
uch a
s pro
vider
or di
agno
sis, to
set
up un
ique e
dits t
hat d
elive
r enh
ance
d aud
iting p
ower
. Pr
ofess
ional
claim
s (CM
S 15
00s)
that r
each
an ad
judica
ted
status
of “P
ay” a
re au
tomati
cally
revie
wed a
gains
t nati
onall
y re
cogn
ized s
tanda
rds s
uch N
ation
al Co
rrect
Codin
g Init
iative
(N
CCI),
med
ical p
olicy
requ
ireme
nts [e
.g., A
meric
an M
edica
l As
socia
tion (
AMA)
], and
can m
eet m
axim
um un
it req
uirem
ents
supp
lied b
y DHH
, with
reco
mmen
datio
ns ap
plied
durin
g an
autom
atic r
e-ad
judica
tion p
roce
ss.
The u
se of
thes
e two
syste
ms co
mbine
d, alo
ng w
ith su
ppor
tive
modu
les an
d stat
ed re
sour
ces,
prov
ide fo
r com
plian
ce w
ith C
CI
rules
, reg
ulatio
ns an
d rela
ted m
ethod
ologie
s.
17.1.
11 T
he C
CN ag
rees
that
at su
ch tim
e tha
t DH
H pr
esen
ts re
comm
enda
tions
conc
ernin
g cla
ims b
illing
and p
roce
ssing
that
are c
onsis
tent
with
indus
try no
rms,
the C
CN sh
all co
mply
with
said
reco
mmen
datio
ns w
ithin
ninety
(90)
calen
dar
days
from
notic
e by D
HH.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth ac
know
ledge
s and
will
comp
ly.
17.1.
12 T
he C
CN sh
all ha
ve pr
oced
ures
appr
oved
by
DHH
, ava
ilable
to pr
ovide
rs in
writte
n and
web
for
m for
the a
ccep
tance
of cl
aim su
bmiss
ions
which
inclu
de:
Meets
Me
ets
Meets
Th
e clea
n date
(actu
al re
ceipt
date)
of no
n-ele
ctron
ic cla
ims
(pap
er) is
deriv
ed fr
om F
uture
Visio
n, Ae
tna B
etter
Hea
lth's
docu
ment
imag
ing ve
ndor
. This
date
is a t
rue r
epre
senta
tion o
f wh
en th
e clai
ms w
ere a
ctuall
y rec
eived
and p
roce
ssed
by th
e im
age v
endo
r and
is em
bedd
ed w
ithin
the da
ta file
of th
e clai
ms
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
25

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.1.
12.1
The p
roce
ss fo
r doc
umen
ting t
he da
te of
actua
l rece
ipt of
non-
electr
onic
claim
s and
date
and t
ime o
f elec
tronic
claim
s;
Meets
Me
ets
Meets
17.1.
12.2
The p
roce
ss fo
r rev
iewing
claim
s for
ac
cura
cy an
d acc
eptab
ility;
Meets
Me
ets
Meets
17.1.
12.3
The p
roce
ss fo
r pre
venti
on of
loss
of
such
claim
s, an
d Me
ets
Meets
Me
ets
17.1.
12.4
The p
roce
ss fo
r rev
iewing
claim
s for
de
termi
natio
n as t
o whe
ther c
laims
are a
ccep
ted
as cl
ean c
laims
.
Meets
Me
ets
Meets
trans
mitte
d to u
s by o
ur im
age v
ende
r. Th
is da
te wi
ll also
ma
tches
Alch
emy (
our c
laim
imag
e retr
ieval
appli
catio
n) cl
aim
numb
er (J
ulian
date)
that
is sta
mped
on th
e ima
ges o
f the e
ach
claim
. Th
e ima
ge ve
ndor
scan
s (via
OCR
tech
nolog
y) the
claim
and
assig
ns a
Docu
ment
Contr
ol Nu
mber
(DCN
) to e
ach c
laim
for
track
ing an
d rec
oncil
iation
purp
oses
. The
se im
age f
iles a
re
forwa
rded
to ou
r IT
Oper
ation
s Dep
artm
ent, u
pload
ed to
Alch
emy
and l
inked
to th
e ass
ociat
ed el
ectro
nic cl
aim vi
a DCN
. FV
Tech
pick
s up c
laims
from
the d
esign
ated P
O Bo
x in t
he
morn
ing, s
cans
and u
pload
s the
imag
es, a
nd w
ithin
24 to
26
hour
s of th
eir pi
ck up
time a
t the U
nited
Stat
es P
ostal
Ser
vice,
the im
ages
are s
ent to
Aetn
a Bett
er H
ealth
, with
an im
age f
ile
simult
aneo
usly
loade
d into
Alch
emy.
ED
I clai
ms ar
e typ
ically
rece
ived f
rom
multip
le Cl
earin
ghou
ses,
with
each
Clea
ringh
ouse
boun
d by t
heir s
pecif
ic co
ntrac
tual
agre
emen
t with
a Pr
ovide
r. O
nce E
DI cl
aims a
re re
ceive
d, the
y ar
e pro
cess
ed vi
a Ins
tream
and L
evel
1 & 2
HIPA
A ed
its ar
e ap
plied
. Reje
cts ar
e the
n sub
mitte
d to A
etna E
DI G
atewa
y whic
h cre
ates t
he 27
7 for
the C
learin
ghou
se. I
t is th
e Clea
ringh
ouse
' ag
reem
ent w
ith th
e Pro
vider
that
deter
mine
s data
elem
ents
of re
jects.
Cl
aims t
hat a
re ac
cepte
d are
mas
s adju
dicate
d and
plac
ed in
a Pa
y, De
ny or
Pen
d stat
us. P
end &
Den
y stat
us w
ould
indica
te an
un
clean
claim
.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
26

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.1.
13 T
he C
CN sh
all ha
ve a
proc
edur
e app
rove
d by
DHH
avail
able
to pr
ovide
rs in
writte
n and
web
for
m for
notify
ing pr
ovide
rs of
batch
rejec
tions
. The
re
port,
at a
minim
um, s
hould
conta
in the
follo
wing
inf
orma
tion:
Meets
Me
ets
Meets
17.1.
13.1
Date
batch
was
rece
ived b
y the
CCN
; Me
ets
Meets
Me
ets
17.1.
13.2
Date
of re
jectio
n rep
ort;
Meets
Me
ets
Meets
17
.1.13
.3 Na
me or
iden
tifica
tion n
umbe
r of C
CN
issuin
g batc
h reje
ction
repo
rt;
Meets
Me
ets
Meets
17.1.
13.4
Batch
subm
itters
name
or id
entifi
catio
n nu
mber
; and
Me
ets
Meets
Me
ets
17.1.
13.5
Reas
on ba
tch is
rejec
ted.
Meets
Me
ets
Meets
Batch
rejec
tions
occu
r at th
e Clea
ringh
ouse
and d
ata el
emen
ts co
ntaine
d in t
he re
ports
are d
eterm
ined b
y the
Clea
ringh
ouse
s co
ntrac
tual a
gree
ment.
If a
batch
is re
ceive
d by A
etna B
etter
He
alth's
Clai
ms D
epar
tmen
t and
rejec
ted he
re, w
e sub
mit a
re
port
to the
Aetn
a EDI
Gate
way w
hich i
n tur
n cre
ates t
he 27
7 for
the
Clea
ringh
ouse
. Aga
in, it
is the
Clea
ringh
ouse
's ag
reem
ent
with
the P
rovid
er th
at de
termi
nes d
ata el
emen
ts of
rejec
ts.
17.1.
14 T
he C
CN sh
all as
sume
all c
osts
asso
ciated
with
claim
proc
essin
g, inc
luding
the
cost
of re
proc
essin
g/res
ubmi
ssion
, due
to
proc
essin
g erro
rs ca
used
by th
e CCN
or to
the
desig
n of s
ystem
s with
in the
CCN
’s sp
an of
co
ntrol.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth ac
know
ledge
s and
will
comp
ly.
17.1.
15 T
he C
CN sh
all no
t emp
loy of
f-sys
tem or
gr
oss a
djustm
ents
when
proc
essin
g cor
recti
on to
pa
ymen
t erro
r, un
less i
t req
uests
and r
eceiv
es
prior
writt
en au
thoriz
ation
from
DHH
.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth ac
know
ledge
s and
will
comp
ly.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
27

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.1.
16 F
or pu
rpos
es of
netw
ork m
anag
emen
t, the
CC
N sh
all no
tify al
l con
tracte
d pro
vider
s to f
ile
claim
s ass
ociat
ed w
ith co
vere
d ser
vices
dire
ctly
with
the C
CN, o
r its c
ontra
ctors,
on be
half o
f Lo
uisian
a Med
icaid
memb
ers.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth's
Claim
s Edu
cator
prov
ides i
n-ne
twor
k and
ou
t-of-n
etwor
k pro
vider
s (i.e
., pro
fessio
nal a
nd in
stitut
ional)
in-
depth
educ
ation
rega
rding
appr
opria
te cla
ims s
ubmi
ssion
re
quire
ments
. Lan
guag
e with
in ou
r pro
vider
contr
acts
instru
cts
prov
iders
to file
all c
laims
dire
ctly w
ith A
etna B
etter
Hea
lth. C
laim
subm
ission
instr
uctio
ns ar
e also
inclu
ded i
n the
Pro
vider
Ha
ndbo
ok, th
e pro
vider
page
s of o
ur w
ebsit
e and
claim
s rela
ted
news
letter
s and
bulle
tins.
The r
equir
emen
t is re
itera
ted du
ring
prov
iders'
initia
l orie
ntatio
n and
ongo
ing ed
ucati
on by
Pro
vider
Se
rvice
Rep
rese
ntativ
es.
17.1.
17 A
t a m
inimu
m, th
e CCN
shall
run o
ne (1
) pr
ovide
r pay
ment
cycle
per w
eek,
on th
e sam
e day
ea
ch w
eek,
as de
termi
ned b
y the
CCN
and
appr
oved
by D
HH.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth ru
ns on
e (1)
prov
ider p
ayme
nt cy
cle pe
r we
ek.
17.2
Claim
s Pro
cess
ing
Meth
odol
ogy R
equi
rem
ents
Th
e CCN
shall
per
form
syst
em ed
its, in
cludi
ng, b
ut n
ot lim
ited
to:
17.2.
1 Con
firming
eligi
bility
on ea
ch m
embe
r as
claim
s are
subm
itted o
n the
basis
of th
e elig
ibility
inf
orma
tion p
rovid
ed by
DHH
and t
he E
nroll
ment
Brok
er th
at ap
plies
to th
e per
iod du
ring w
hich t
he
char
ges w
ere i
ncur
red;
Meets
Me
ets
Meets
Inb
ound
claim
s are
uploa
ded t
o QNX
T™, o
ur cl
aims p
roce
ssing
sy
stem,
whe
re th
ey ar
e sub
jected
to m
ultipl
e hea
der a
nd lin
e ite
m ed
its. A
mong
thes
e are
edits
that
comp
are s
ervic
e data
to
eligib
ility i
nform
ation
prov
ided b
y DHH
and t
he E
nroll
ment
Brok
er
in or
der t
o con
firm m
embe
rs' el
igibil
ity du
ring t
he pe
riod t
o whic
h ch
arge
s wer
e inc
urre
d.
17.2.
2 A re
view
of the
entire
claim
with
in fiv
e (5)
wo
rking
days
of re
ceipt
of an
elec
tronic
claim
, to
deter
mine
that
the cl
aim is
not a
clea
n clai
m an
d iss
ue an
exce
ption
repo
rt to
the pr
ovide
r indic
ating
all
defec
ts or
reas
ons k
nown
at th
at tim
e tha
t the
claim
is no
t a cl
ean c
laim.
The
exce
ption
repo
rt sh
all co
ntain
at a m
inimu
m the
follo
wing
Meets
Me
ets
Meets
Le
vel I
and I
I edit
s occ
ur at
the c
learin
ghou
se an
d han
dled w
ithin
5 wor
king d
ays.
The
clea
ringh
ouse
bear
s res
pons
ibility
for
prov
iding
exce
ption
repo
rts to
the p
rovid
ers.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
28

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
infor
matio
n:
17.2.
2.1 M
embe
r nam
e; Me
ets
Meets
Me
ets
17.2.
2.2 P
rovid
er cl
aim nu
mber
, pati
ent a
ccou
nt nu
mber
, or u
nique
mem
ber id
entifi
catio
n num
ber;
Meets
Me
ets
Meets
17.2.
2.3 D
ate of
servi
ce;
Meets
Me
ets
Meets
17
.2.2.4
Tota
l bille
d cha
rges
; Me
ets
Meets
Me
ets
17.2.
2.5 C
CN’s
name
; and
Me
ets
Meets
Me
ets
17.2.
2.6 T
he da
te the
repo
rt wa
s gen
erate
d. Me
ets
Meets
Me
ets
17.2.
3 Med
ical n
eces
sity;
Meets
Me
ets
Meets
Cl
inica
l edit
s are
capa
ble of
verify
ing w
hen a
proc
edur
e is f
or
certa
in ge
nder
or an
age,
e.g.,
the cl
aim ed
its w
ill be
able
to de
tect if
preg
nanc
y-rela
ted se
rvice
s are
inad
verte
ntly b
eing
assig
ned t
o a m
ale m
embe
r. Re
fer to
17.2.
4 app
lies e
dits
acco
rding
ly.
17.2.
4 Prio
r App
rova
l – T
he sy
stem
shall
de
termi
ne w
hethe
r a co
vere
d ser
vice r
equir
ed pr
ior
appr
oval
and i
f so,
wheth
er th
e CCN
gran
ted su
ch
appr
oval;
Meets
Me
ets
Meets
17.2.
5 Dup
licate
Clai
ms –
The s
ystem
shall
in an
au
tomate
d man
ner,
flag a
claim
as be
ing ex
actly
the
same
as a
prev
iously
subm
itted c
laim
or a
poss
ible d
uplic
ate an
d eith
er de
ny or
pend
the
claim
as ne
eded
;
Meets
Me
ets
Meets
Aetna
Bett
er H
ealth
's Bu
sines
s App
licati
on M
anag
emen
t (BA
M)
Depa
rtmen
t is re
spon
sible
for th
e acc
urate
and e
fficien
t co
nfigu
ratio
n of fu
nctio
nal b
usine
ss re
quire
ments
and r
ules w
ithin
QNXT
™ n
eces
sary
for ad
minis
trativ
e ser
vices
to oc
cur.
This
inc
ludes
mee
ting c
laims
proc
essin
g stan
dard
s and
auto-
adjud
icatio
n tar
gets.
The
objec
tives
of th
e buil
d are
to:
● An
alyze
busin
ess r
equir
emen
ts to
desig
n and
confi
gure
an
optim
al an
d effic
ient s
ystem
build
that
will m
inimi
ze th
e nee
d for
man
ual p
roce
ssing
.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
29

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.2.
6 Cov
ered
Ser
vices
- Se
e tha
t the s
ystem
ve
rify th
at a s
ervic
e is a
cove
red s
ervic
e and
is
eligib
le for
paym
ent;
Meets
Me
ets
Meets
17.2.
7 Pro
vider
Vali
datio
n - S
ee th
at the
syste
m sh
all ap
prov
e for
paym
ent o
nly th
ose c
laims
re
ceive
d fro
m pr
ovide
rs eli
gible
to re
nder
servi
ce
for w
hich t
he cl
aim w
as su
bmitte
d;
Meets
Me
ets
Meets
17.2.
8 Qua
ntity
of Se
rvice
- Se
e tha
t the s
ystem
sh
all ev
aluate
claim
s for
servi
ces p
rovid
ed to
me
mber
s to s
ee th
at an
y app
licab
le be
nefit
limits
ar
e app
lied;
Meets
Me
ets
Meets
17.2.
9 Per
form
syste
m ed
its fo
r vali
d date
s of
servi
ce, a
nd as
sure
that
dates
of se
rvice
s are
valid
da
tes su
ch as
not in
the f
uture
or ou
tside
of a
memb
er’s
Medic
aid el
igibil
ity sp
an;
Meets
Me
ets
Meets
● Lo
ad th
e rule
s and
requ
ireme
nts of
a ne
w he
alth p
lan,
prod
uct o
r bus
iness
func
tion i
n the
claim
s pro
cess
ing
syste
m, in
cludin
g elig
ibility
file l
ayou
t, pro
vider
contr
acts,
fee
sche
dules
and m
embe
r ben
efits
and p
rior a
uthor
izatio
n re
quire
ments
. ●
Comp
lete c
onfig
urati
on do
cume
ntatio
n whil
e ente
ring t
he
build
infor
matio
n. ●
Audit
and v
alida
te the
build
base
d on t
he ru
les an
d re
quire
ments
state
d by t
he he
alth p
lan an
d the
im
pleme
ntatio
n tea
m.
● Jo
intly
perfo
rm un
it tes
ting w
ith th
e Ope
ratio
ns P
roce
ss
Know
ledge
Man
agem
ent (
OPKM
) Tes
ting t
eam
to va
lidate
tha
t the s
ystem
is op
erati
onal
and m
eets
busin
ess
requ
ireme
nts.
● Pa
rticipa
te in
end-
to-en
d tes
ting w
ith al
l impa
cted
depa
rtmen
ts to
see t
hat th
e sys
tem is
oper
ating
as ex
pecte
d.
17.2.
10 P
erfor
m po
st-pa
ymen
t rev
iew on
a sa
mple
of cla
ims t
o see
that
servi
ces p
rovid
ed w
ere
medic
ally n
eces
sary;
and
Meets
Me
ets
Meets
17.2.
11 H
ave a
staff
of qu
alifie
d, me
dicall
y tra
ined
and a
ppro
priat
ely lic
ense
d per
sonn
el, co
nsist
ent
with
NCQA
accre
ditati
on st
anda
rds,
whos
e prim
ary
dutie
s are
to as
sist in
evalu
ating
claim
s for
med
ical
nece
ssity
.
Meets
Me
ets
Meets
Aetna
Bett
er H
ealth
main
tains
an in
depe
nden
t (i.e
. doe
s not
repo
rt to
claim
s lea
dersh
ip) po
st-pa
ymen
t Aud
it Dep
artm
ent
resp
onsib
le for
draw
ing st
ratifi
ed ra
ndom
samp
les an
d co
nduc
ting f
ocus
ed au
dits o
f paid
and d
enied
claim
s. Th
e pu
rpos
e of th
ese a
ctivit
ies is
to au
dit co
mplia
nce o
f clai
ms
adjud
icatio
n with
DHH
regu
lator
y req
uirem
ents
and p
rovid
er
contr
acts.
Aud
it find
ings a
re sh
ared
with
Clai
ms m
anag
emen
t for
root
caus
e ana
lysis
and c
orre
ctive
actio
n.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
30

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.3
Expl
anat
ion
of B
enef
its (E
OBs)
17
.3.1 T
he C
CN sh
all w
ithin
forty-
five (
45) d
ays o
f pa
ymen
t of c
laims
, pro
vide i
ndivi
dual
notic
es to
a sa
mple
grou
p of th
e mem
bers
who r
eceiv
ed
servi
ces.
The r
equir
ed no
tice m
ust s
pecif
y:
17.3.
1.1.1
The s
ervic
e fur
nishe
d;
17.3.
1.1.2
The n
ame o
f the p
rovid
er fu
rnish
ing th
e se
rvice
;
17.3.
1.1.3
The d
ate on
whic
h the
servi
ce w
as
furnis
hed;
and
17.3.
1.1.4
The a
moun
t of th
e pay
ment
made
for
the se
rvice
.
17.3.
2 The
CCN
shall
also
:
17.3.
2.1 In
clude
in th
e sam
ple, c
laims
for s
ervic
es
with
hard
bene
fit lim
its, d
enied
claim
s with
mem
ber
resp
onsib
ility,
and p
aid cl
aims (
exclu
ding a
ncilla
ry an
d ane
sthes
ia se
rvice
s).
17.3.
2.2 S
tratify
paid
claim
s sam
ple to
see t
hat a
ll pr
ovide
r typ
es (o
r spe
cialtie
s) ar
e rep
rese
nted i
n the
pool
of ge
nera
ted E
OBs.
To th
e exte
nt tha
t the
CCN
cons
iders
a par
ticula
r spe
cialty
(or p
rovid
er)
to wa
rrant
close
r scru
tiny,
the C
CN m
ay ov
er
samp
le the
grou
p. Th
e paid
claim
s sam
ple sh
ould
be a
minim
um of
two h
undr
ed (2
00) t
o two
hu
ndre
d-fift
y (25
0) cl
aims p
er ye
ar.
See e
xplan
ation
Ae
tna B
etter
Hea
lth ac
know
ledge
s and
will
comp
ly. A
ll elem
ents
requ
ired i
n the
Exp
lanati
on of
Ben
efits
will b
e inc
luded
in th
e EO
B pr
ovide
d to C
CN m
embe
rs. A
s new
EOB
requ
ireme
nts an
d ele
ments
are u
pdate
d, Ae
tna B
etter
Hea
lth w
ill co
mply
and a
s su
ch, m
ake n
eces
sary
modif
icatio
ns to
exist
ing E
OB re
porte
d fie
lds as
requ
ired.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
31

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.3.
3 The
CCN
shall
trac
k any
comp
laints
re
ceive
d fro
m me
mber
s and
reso
lve th
e co
mplai
nts ac
cord
ing to
its es
tablis
hed p
olicie
s an
d pro
cedu
res.
The r
esolu
tion m
ay be
mem
ber
educ
ation
, pro
vider
educ
ation
, or r
eferra
l to D
HH.
The C
CN sh
all us
e the
feed
back
rece
ived t
o mo
dify o
r enh
ance
the E
OB sa
mplin
g me
thodo
logy.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth m
aintai
ns an
inter
nal, p
ropr
ietar
y app
licati
on
that s
uppo
rts th
e Grie
vanc
e and
App
eals
proc
ess b
y tra
cking
me
mber
and p
rovid
er is
sues
from
ince
ption
to re
solut
ion. T
his
affor
ds us
the m
eans
to ad
dres
s not
only
issue
s affe
cting
ind
ividu
al me
mber
and p
rovid
er sa
tisfac
tion,
but p
otenti
al tre
nds
in the
deliv
ery s
ystem
as a
whole
, per
mittin
g hea
lth pl
an
perso
nnel
to tak
e pro
mpt, c
orre
ctive
step
s to m
inimi
zing r
isks t
o pe
rform
ance
stan
dard
s. F
eedb
ack r
eceiv
ed du
ring t
his pr
oces
s or
feed
back
rece
ived t
hrou
gh ot
her m
eans
, will
be sh
ared
with
the
appr
opria
te pe
rsonn
el wi
thin t
he C
laims
unit f
or fu
ture
hand
ling a
nd m
odific
ation
s in c
once
rt wi
th the
IT D
epar
tmen
t. Ae
tna B
etter
Hea
lth w
ill us
e the
feed
back
rece
ived v
ia the
me
mber
comp
liant
syste
m to
impr
ove o
ur E
OB sa
mplin
g me
thodo
logy.
Resu
lts of
mem
ber f
eedb
ack w
ill be
revie
wed b
y ou
r Ser
vice I
mpro
veme
nt Co
mmitte
e (SI
C) an
d res
ults f
orwa
rded
to
QM/U
M Co
mmitte
e for
revie
w an
d rec
omme
ndati
ons
deve
loped
.
17.4
Rem
ittan
ce A
dvice
s In
conj
unct
ion
with
its p
aym
ent c
ycles
, the
CCN
shall
pro
vide:
17
.4.1 E
ach r
emitta
nce a
dvice
gene
rated
by th
e CC
N to
a pro
vider
shall
, if kn
own a
t that
time,
clear
ly ide
ntify
for ea
ch cl
aim, th
e foll
owing
inf
orma
tion:
Meets
Me
ets
Meets
17.4.
1.1 T
he na
me of
the m
embe
r; Me
ets
Meets
Me
ets
17.4.
1.2 U
nique
mem
ber id
entifi
catio
n num
ber;
Meets
Me
ets
Meets
17.4.
1.3 P
atien
t clai
m nu
mber
or pa
tient
acco
unt
numb
er;
Meets
Me
ets
Meets
QNXT
™, A
etna B
etter
Hea
lth's
core
tran
sacti
on pr
oces
sing
syste
m, ge
nera
tes pa
per R
emitta
nce A
dvice
s (RA
s) for
our
prov
iders.
In ad
dition
, pro
vider
s tak
ing ad
vanta
ge of
our
Elec
tronic
Fun
d Tra
nsfer
(EFT
) cap
abilit
y hav
e the
optio
n of
rece
iving
Elec
tronic
Rem
ittanc
e Adv
ices (
ERAs
). Bu
sines
s Ap
plica
tion M
anag
emen
t (BA
M) pe
rsonn
el co
nfigu
re Q
NXT™
to
gene
rate
RAs f
orma
tted s
uch t
hat r
equir
ed da
ta ele
ments
are
read
ily id
entifi
able.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
32

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.4.
1.4 D
ate of
servi
ce;
Meets
Me
ets
Meets
17
.4.1.5
Tota
l pro
vider
char
ges;
Meets
Me
ets
Meets
17.4.
1.6 M
embe
r liab
ility,
spec
ifying
any c
o-ins
uran
ce, d
educ
tible,
co-p
ayme
nt, or
non-
cove
red
amou
nt;
Meets
Me
ets
Meets
17.4.
1.7 A
moun
t paid
by th
e CCN
; Me
ets
Meets
Me
ets
17.4.
1.8 A
moun
t den
ied an
d the
reas
on fo
r den
ial;
and
Meets
Me
ets
Meets
The f
ollow
ing st
ateme
nt sh
all be
inclu
ded o
n eac
h re
mitta
nce a
dvice
sent
to pr
ovide
rs: “I
unde
rstan
d tha
t pay
ment
and s
atisfa
ction
of th
is cla
im w
ill be
fro
m fed
eral
and s
tate f
unds
, and
that
any f
alse
claim
s, sta
temen
ts, do
cume
nts, o
r con
cealm
ent o
f a m
ateria
l fact,
may
be pr
osec
uted u
nder
ap
plica
ble fe
dera
l and
/or st
ate la
ws.”
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth’s
exist
ing re
mitta
nce a
dvice
can b
e co
nfigu
red t
o mee
t this
requ
ireme
nt.
17.5
Adhe
renc
e to
Key C
laim
s Man
agem
ent S
tand
ards
17.5.
1 Pro
mpt
Pay
men
t to
Prov
ider
s 17
.5.1.1
The
CCN
shall
see t
hat n
inety
perce
nt (9
0%) o
f all c
lean c
laims
for p
ayme
nt of
servi
ces
deliv
ered
to a
memb
er ar
e paid
by th
e CCN
to th
e pr
ovide
r with
in fift
een (
15) b
usine
ss da
ys of
the
rece
ipt of
such
claim
s.
See e
xplan
ation
17.5.
1.2 T
he C
CN sh
all pr
oces
s and
, if
appr
opria
te, pa
y with
in thi
rty (3
0) ca
lenda
r day
s, nin
ety-n
ine pe
rcent
(99%
) of a
ll clea
n clai
ms to
pr
ovide
rs for
cove
red s
ervic
es de
liver
ed to
a
See e
xplan
ation
Aetna
Bett
er H
ealth
pres
ently
man
ages
its cl
aims p
ayme
nt pr
oces
s suc
h tha
t Stat
e man
dated
paym
ent ti
mefra
mes a
re ei
ther
met o
r exc
eede
d by t
he C
laim’
s Unit
. For
exam
ple, in
Flor
ida,
Aetna
Bett
er H
ealth
man
ages
the c
laim
proc
ess s
uch t
hat th
e en
tire cl
aims p
roce
ss is
comp
leted
with
12 da
ys on
aver
age,
with
an ad
ded 7
days
tagg
ed on
to th
e pro
cess
to ac
coun
t for c
heck
iss
uanc
e pur
pose
s, so
that
the to
tal tim
e to p
roce
ss, o
n ave
rage
is
20 bu
sines
s day
s (the
requ
ireme
nt is
20 da
ys),
thus t
he cl
aim
paym
ent ti
me ex
ceed
s the
man
dator
y tim
efram
e in F
lorida
. Ae
tna B
etter
Hea
lth an
ticipa
tes al
so ex
ceed
ing th
e exp
ectat
ions
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
33
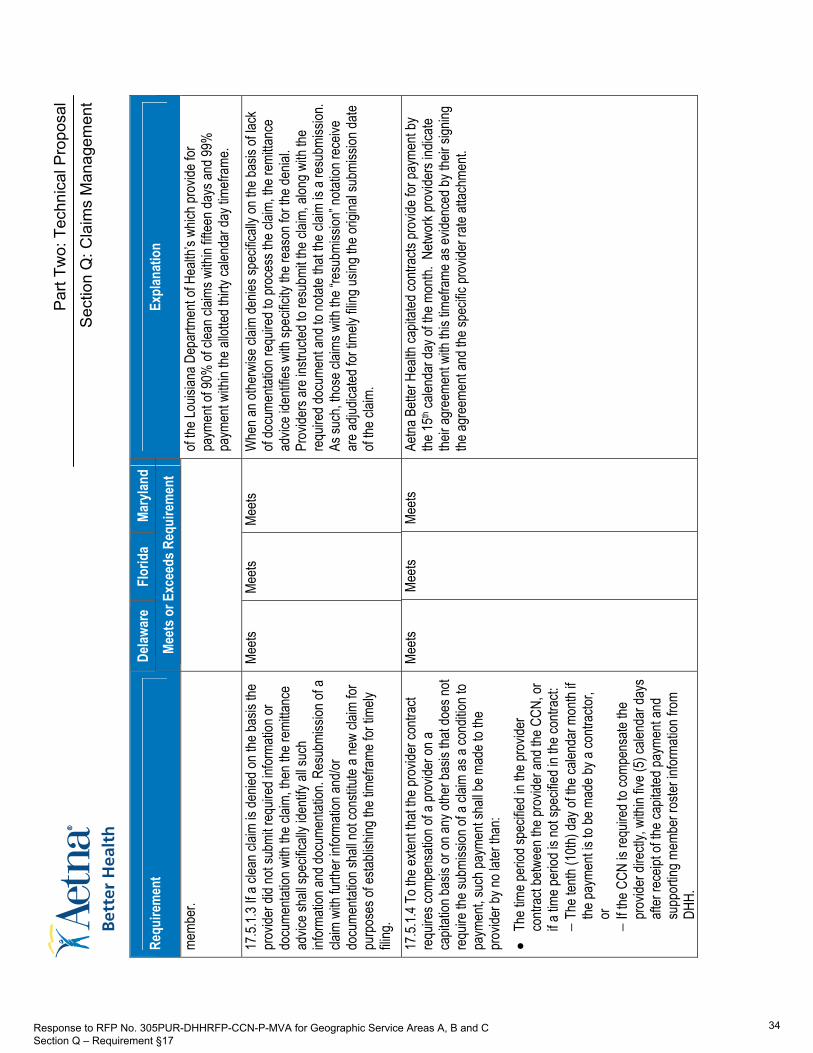
Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
memb
er.
of the
Louis
iana D
epar
tmen
t of H
ealth
’s wh
ich pr
ovide
for
paym
ent o
f 90%
of cl
ean c
laims
with
in fift
een d
ays a
nd 99
%
paym
ent w
ithin
the al
lotted
thirty
calen
dar d
ay tim
efram
e.
17.5.
1.3 If
a clea
n clai
m is
denie
d on t
he ba
sis th
e pr
ovide
r did
not s
ubmi
t req
uired
infor
matio
n or
docu
menta
tion w
ith th
e clai
m, th
en th
e rem
ittanc
e ad
vice s
hall s
pecif
ically
iden
tify al
l suc
h inf
orma
tion a
nd do
cume
ntatio
n. Re
subm
ission
of a
claim
with
furth
er in
forma
tion a
nd/or
do
cume
ntatio
n sha
ll not
cons
titute
a new
claim
for
purp
oses
of es
tablis
hing t
he tim
efram
e for
timely
fili
ng.
Meets
Me
ets
Meets
W
hen a
n othe
rwise
claim
denie
s spe
cifica
lly on
the b
asis
of lac
k of
docu
menta
tion r
equir
ed to
proc
ess t
he cl
aim, th
e rem
ittanc
e ad
vice i
denti
fies w
ith sp
ecific
ity th
e rea
son f
or th
e den
ial.
Prov
iders
are i
nstru
cted t
o res
ubmi
t the c
laim,
alon
g with
the
requ
ired d
ocum
ent a
nd to
notat
e tha
t the c
laim
is a r
esub
miss
ion.
As su
ch, th
ose c
laims
with
the “
resu
bmiss
ion” n
otatio
n rec
eive
are a
djudic
ated f
or tim
ely fil
ing us
ing th
e orig
inal s
ubmi
ssion
date
of the
claim
.
17.5.
1.4 T
o the
exten
t that
the pr
ovide
r con
tract
requ
ires c
ompe
nsati
on of
a pr
ovide
r on a
ca
pitati
on ba
sis or
on an
y othe
r bas
is tha
t doe
s not
requ
ire th
e sub
miss
ion of
a cla
im as
a co
nditio
n to
paym
ent, s
uch p
ayme
nt sh
all be
mad
e to t
he
prov
ider b
y no l
ater t
han:
● Th
e tim
e per
iod sp
ecifie
d in t
he pr
ovide
r co
ntrac
t betw
een t
he pr
ovide
r and
the C
CN, o
r if a
time p
eriod
is no
t spe
cified
in th
e con
tract:
−
The t
enth
(10th
) day
of th
e cale
ndar
mon
th if
the pa
ymen
t is to
be m
ade b
y a co
ntrac
tor,
or
− If t
he C
CN is
requ
ired t
o com
pens
ate th
e pr
ovide
r dire
ctly,
withi
n five
(5) c
alend
ar da
ys
after
rece
ipt of
the c
apita
ted pa
ymen
t and
su
ppor
ting m
embe
r ros
ter in
forma
tion f
rom
DHH.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth ca
pitate
d con
tracts
prov
ide fo
r pay
ment
by
the 15
th cale
ndar
day o
f the m
onth.
Netw
ork p
rovid
ers i
ndica
te the
ir agr
eeme
nt wi
th thi
s tim
efram
e as e
viden
ced b
y the
ir sign
ing
the ag
reem
ent a
nd th
e spe
cific
prov
ider r
ate at
tachm
ent.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
34

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.5.
1.5 T
he C
CN sh
all no
t den
y pro
vider
claim
s on
the b
asis
of un
timely
filing
in si
tuatio
ns
rega
rding
coor
dinati
on of
servi
ces o
r sub
roga
tion,
in wh
ich ca
se th
e pro
vider
is pu
rsuing
paym
ent
from
a thir
d par
ty. In
situa
tions
of th
ird pa
rty
bene
fits, th
e tim
efram
es fo
r filin
g a cl
aim sh
all
begin
on th
e date
that
the th
ird pa
rty co
mplet
es
reso
lution
of th
e clai
m.
Meets
Me
ets
Meets
Ae
tna B
etter
Hea
lth ac
know
ledge
s and
will
comp
ly. A
etna B
etter
He
alth a
ckno
wled
ges D
HH’s
timely
failin
g rela
ted to
subr
ogate
d or
COB
claim
s and
will
comp
ly wi
th sa
id re
quire
ments
. It is
Ae
tna B
etter
Hea
lth’s
stand
ard o
pera
ting p
roce
dure
to ac
cept
claim
s tha
t are
with
in the
statu
torily
allot
ted tim
ely fil
ing lim
its,
and t
hose
timefr
ames
and o
ther c
onsid
erati
ons a
pplic
able
to su
brog
ated c
laims
or co
ordin
ation
of be
nefits
17.5.
1.6 T
he C
CN sh
all no
t pay
any c
laim
subm
itted b
y a pr
ovide
r who
is ex
clude
d fro
m pa
rticipa
tion i
n Med
icare
, Med
icaid,
or C
HIP
prog
ram
pursu
ant to
Sec
tion 1
128 o
r 115
6 of th
e So
cial S
ecur
ity A
ct or
is ot
herw
ise no
t in go
od
stand
ing w
ith D
HH.
Meets
Me
ets
Meets
As
part
of ou
r cre
denti
aling
proc
ess,
Aetna
Bett
er H
ealth
quer
ies
the lis
ting o
f exc
luded
indiv
iduals
, pur
suan
t to th
e req
uirem
ents
of se
ction
1128
or 11
56 of
the S
ocial
Sec
urity
Act,
and s
ees t
hat
those
prov
iders
treati
ng m
embe
rs co
vere
d und
er th
e agr
eeme
nt be
twee
n Aetn
a Bett
er H
ealth
and t
he D
HH, a
re in
good
stan
ding
with
DHH
prior
to co
mplet
ing th
e con
tracti
ng an
d cre
denti
aling
pr
oces
s. A
t rec
rede
ntiali
ng, th
e pro
cedu
res a
re fo
llowe
d to m
ake
certa
in go
od st
andin
g with
DHH
and l
ack o
f exc
lusion
or
restr
iction
for p
artic
ipatio
n in a
Med
icaid,
Med
icare
or ot
her
gove
rnme
nt he
althc
are p
rogr
am. A
etna B
etter
Hea
lth, th
roug
h its
vend
or P
DS, a
lso co
nduc
ts qu
eries
of no
n-ne
twor
k pro
vider
s, on
a p
eriod
ic an
d ran
dom
basis
, to su
pplem
ent it
s exis
ting q
uery
proc
esse
s rela
ted to
the c
ontra
cted n
etwor
k.
17.5.
2 Clai
ms D
isput
e Man
agem
ent
17.5.
2.1 T
he C
CN sh
all ha
ve an
inter
nal c
laims
dis
pute
proc
edur
e tha
t sha
ll be s
ubmi
tted t
o DHH
wi
thin t
hirty
(30)
days
of th
e date
the C
ontra
ct is
signe
d by t
he C
CN, w
hich w
ill be
revie
wed a
nd
appr
oved
by D
HH.
Meets
Me
ets
Meets
17.5.
2.2 T
he C
CN sh
all co
ntrac
t with
inde
pend
ent
revie
wers
to re
view
dispu
ted cl
aims.
Meets
Me
ets
Meets
Aetna
Bett
er H
ealth
’s Cl
aims A
dmini
strati
on D
epar
tmen
t emp
loys
full-ti
me cl
aims i
nquir
y and
Res
earch
Rep
rese
ntativ
es to
resp
ond
to pr
ovide
r que
stion
s, sta
tus in
quirie
s and
claim
s pay
ment
dispu
tes vi
a the
claim
s inq
uiry l
ine fr
om 8:
00 a.
m. to
5:00
p.m.
, Mo
nday
thro
ugh F
riday
. An a
utoma
ted te
lepho
ne sy
stem
allow
s ca
llers
to sp
eak d
irectl
y with
a Re
pres
entat
ive or
leav
e a de
tailed
me
ssag
e reg
ardin
g the
ir inq
uiry.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
35

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.5.
2.3 T
he C
CN sh
all sy
stema
ticall
y cap
ture t
he
status
and r
esolu
tion o
f all c
laim
dispu
tes as
well
as
all a
ssoc
iated
docu
menta
tion.
Meets
Me
ets
Meets
W
hene
ver p
ossib
le, th
e pro
vider
inqu
iry w
ill be
reso
lved w
hile t
he
prov
ider is
on th
e pho
ne. I
f the p
rovid
er’s
inquir
y can
not b
e re
solve
d whil
e the
prov
ider is
on th
e pho
ne an
d the
prov
ider’s
inq
uiry r
equir
es ad
dition
al re
sear
ch to
reac
h res
olutio
n, the
n a
call t
rack
ing ca
se w
ill be
open
for t
he pr
ovide
r’s is
sue.
It is
the
depa
rtmen
t’s go
al to
rese
arch
and r
espo
nd to
the p
rovid
er’s
issue
s with
in fiv
e to t
en bu
sines
s day
s. W
hen i
t is no
t pos
sible
to re
solve
the i
ssue
with
in thi
s tim
e fra
me, th
en th
e iss
ue w
ill be
call
track
ed to
the a
ppro
priat
e dep
artm
ent, a
nd th
erea
fter f
ollow
ed by
an
inde
pend
ent r
eview
er. C
laim
dispu
tes m
ay es
calat
e, at
the
requ
est o
f the p
rovid
er, to
the G
rieva
nce a
nd A
ppea
ls pr
oces
s.
As su
ch tim
e, es
tablis
hed G
rieva
nce a
nd A
ppea
ls pr
oced
ures
are
follow
ed an
d app
lied t
o the
prov
ider’s
claim
disp
ute.
Aetna
Bett
er H
ealth
ackn
owled
ges a
nd w
ill co
mply
with
the
requ
ireme
nt to
subm
it its
spec
ific cl
aims d
ispute
polic
ies to
the
DHH
withi
n 30 d
ays o
f con
tract
awar
d. Cl
aim di
spute
data
is ca
pture
d by A
etna B
etter
Hea
lth in
its
syste
ms an
d fur
ther d
ocum
ented
thro
ugh t
he G
rieva
nce a
nd
Appe
als pr
oces
s, as
appli
cable
.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
36

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
17.5.
3 Clai
ms P
aym
ent A
ccur
acy R
epor
t 17
.5.3.1
On a
mon
thly b
asis,
the C
CN sh
all su
bmit
a clai
ms pa
ymen
t acc
urac
y per
centa
ge re
port
to DH
H. T
he re
port
shall
be ba
sed o
n an a
udit
cond
ucted
by th
e CCN
. The
audit
shall
be
cond
ucted
by an
entity
or pe
rsonn
el ind
epen
dent
of cla
ims m
anag
emen
t as s
pecif
ied in
this
Secti
on
of the
RFP
, and
shall
utiliz
e a ra
ndom
ly se
lected
sa
mple
of all
proc
esse
d and
paid
claim
s upo
n ini
tial s
ubmi
ssion
in ea
ch m
onth.
A m
inimu
m sa
mple
cons
isting
of tw
o hun
dred
(200
) to t
wo
hund
red-
fifty (
250)
claim
s per
year
, bas
ed on
fin
ancia
l stra
tifica
tion,
shall
be se
lected
from
the
entire
popu
lation
of el
ectro
nic an
d pap
er cl
aims
proc
esse
d or p
aid up
on in
itial s
ubmi
ssion
.
Exce
eds
Exce
eds
Exce
eds
Aetna
Bett
er H
ealth
main
tains
a Cl
aims Q
uality
Rev
iew T
eam
to mo
nitor
quali
ty sta
ndar
ds fo
r all c
laims
proc
esse
s. Un
der t
he
direc
tion o
f the d
irecto
r of O
pera
tions
Pro
cess
and K
nowl
edge
Ma
nage
ment
(OPK
M), Q
uality
Rev
iew A
nalys
ts co
nduc
t ran
dom
and f
ocus
ed re
views
of pr
oces
sed c
laims
for p
ayme
nt, fin
ancia
l an
d pro
cedu
ral a
ccur
acy a
nd pr
ovide
r inqu
iry ca
lls, w
hich f
ocus
on
both
accu
racy
and c
ustom
er se
rvice
skills
. Per
forma
nce i
s me
asur
ed ag
ainst
estab
lishe
d dep
artm
ent g
uideli
nes.
More
over
, the C
laims
Qua
lity R
eview
Tea
m ful
ly au
dits t
he w
ork
of all
new
claim
s ana
lysts
for at
leas
t one
mon
th su
bseq
uent
to the
ir orie
ntatio
n and
train
ing. T
he au
dit st
arts
at 10
0 per
cent
of the
ir wor
k pro
duct
and d
ecre
ases
to a
stand
ard t
wo pe
rcent
by
the fif
th we
ek, p
rovid
ed th
e new
claim
s ana
lyst c
ontin
ues t
o mee
t cla
ims a
ccur
acy s
tanda
rds.
Finall
y, we
revie
w 16
prov
ider c
alls
per C
laims
Inqu
iry R
epre
senta
tive p
er m
onth,
asse
ssing
the
quali
ty of
servi
ce in
terac
tion a
nd ac
cura
cy of
infor
matio
n pr
ovide
d. Ind
ividu
al qu
ality
repo
rts ar
e pre
sente
d to t
he
Repr
esen
tative
and t
heir S
uper
visor
for c
orre
ctive
actio
n (e.g
., liv
e call
mon
itorin
g) if
appr
opria
te.
Quali
ty Re
view
Analy
sts co
nduc
t a se
ries o
f pre
-pay
ment
audit
s inc
luding
:
1)
A on
e per
cent
rand
om sa
mple
of sy
stem-
adjud
icated
cla
ims,
2)
A
two p
erce
nt ra
ndom
samp
le of
all an
alyst-
adjud
icated
cla
ims,
3)
A
daily
rand
om sa
mple
of bil
led cl
aims u
p to $
49,99
9.99,
and
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
37

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
4)
100 p
erce
nt of
all cl
aims w
ith bi
lled c
harg
es ov
er $5
0,000
. W
e will
have
one f
ull tim
e Aud
itor a
ssign
ed an
d we w
ill pu
ll a to
tal
of 4 a
udits
per m
onth;
two U
B (fa
cility
) file
s and
two 1
500
(phy
sician
) file
s bas
ed on
a tw
o wee
k paid
date/
chec
k cyc
le. O
ur
samp
le siz
e is 9
5/2/2
(95%
confi
denc
e; the
erro
r rate
is 2%
; with
a d
esire
d pre
cision
of +
/- 2%
) whic
h is a
n ave
rage
of 18
0+ cl
aims
revie
wed e
ach w
eek.
Eac
h file
prov
ides A
etna B
etter
Hea
lth w
ith
Paym
ent a
nd F
inanc
ial A
ccur
acy f
inding
s for
the p
eriod
audit
ed
and e
ach f
ile is
distr
ibuted
for r
eview
and r
espo
nse t
o all
appli
cable
depa
rtmen
ts.
17.5.
3.2 T
he m
inimu
m att
ribute
s to b
e tes
ted fo
r ea
ch cl
aim se
lected
shall
inclu
de:
● Cl
aim da
ta co
rrectl
y ente
red i
nto th
e clai
ms
proc
essin
g sys
tem;
● Cl
aim is
asso
ciated
with
the c
orre
ct pr
ovide
r; ●
Prop
er au
thoriz
ation
was
obtai
ned f
or th
e se
rvice
; ●
Memb
er el
igibil
ity at
proc
essin
g date
corre
ctly
appli
ed;
● Al
lowed
paym
ent a
moun
t agr
ees w
ith
contr
acted
rate;
●
Dupli
cate
paym
ent o
f the s
ame c
laim
has n
ot oc
curre
d; ●
Denia
l reas
on ap
plied
appr
opria
tely;
● Co
-pay
ment
appli
catio
n con
sider
ed an
d
Exce
eds
Exce
eds
Exce
eds
Post-
paym
ent a
udits
revie
w, at
a mi
nimum
, inclu
de au
dit fo
r the
att
ribute
s list
ed in
requ
ireme
nt 17
.5.3.2
., and
also
prov
ide fo
r re
view
of:
● Va
lid C
oding
, e.g.
prop
er us
e of c
odes
and m
odifie
r cod
es;
● Me
mber
eligi
bility
; ●
Data
entry
into
the sy
stems
is ac
cura
te;
● Tim
ely F
iling;
● Cl
aim is
asso
ciated
with
the c
orre
ct tre
ating
prov
ider;
● Pr
ior A
uthor
izatio
n req
uirem
ents;
●
Denia
l reas
ons a
pplie
d cor
rectl
y; ●
Bene
fit ap
plica
tion (
includ
ing lim
itatio
ns an
d exc
lusion
s);
● Co
ordin
ation
of B
enefi
ts ap
plica
tion;
●
Claim
s hist
ory r
eview
for d
uplic
ate cl
aim;
● Ma
nual
Prici
ng ap
plica
tion;
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
38

Par
t Tw
o: T
echn
ical
Pro
posa
l
Sec
tion
Q: C
laim
s M
anag
emen
t
Delaw
are
Flor
ida
Mary
land
Requ
irem
ent
Meet
s or E
xcee
ds R
equi
rem
ent
Expl
anat
ion
appli
ed, if
appli
cable
; ●
Effec
t of m
odifie
r cod
es co
rrectl
y app
lied;
and
● Pr
oper
codin
g.
● Co
ntrac
ted P
rovid
er an
d Spe
cial P
rovid
er ag
reem
ents,
such
as
one-
time c
ase a
gree
ments
and f
or bo
th en
surin
g pay
ment
amou
nt ag
rees
with
contr
acted
rate;
●
Modif
ier D
iscou
nts; a
nd
● Cl
aims b
undli
ng/un
bund
ling.
17.5.
3.3 T
he re
sults
of te
sting
at a
minim
um
shou
ld be
docu
mente
d to i
nclud
e: ●
Resu
lts fo
r eac
h attr
ibute
tested
for e
ach c
laim
selec
ted;
● Am
ount
of ov
erpa
ymen
t or u
nder
paym
ent fo
r ea
ch cl
aim pr
oces
sed o
r paid
in er
ror;
● Ex
plana
tion o
f the e
rrone
ous p
roce
ssing
for
each
claim
proc
esse
d or p
aid in
erro
r; ●
Dete
rmina
tion i
f the e
rror is
the r
esult
of a
keyin
g erro
r or t
he re
sult o
f erro
r in th
e co
nfigu
ratio
n or t
able
maint
enan
ce of
the
claim
s pro
cess
ing sy
stem;
and
● Cl
aims p
roce
ssed
or pa
id in
erro
r hav
e bee
n co
rrecte
d.
Exce
eds
Exce
eds
Exce
eds
Audit
docu
menta
tion c
ompr
ises,
at a m
inimu
m, do
cume
ntatio
n of
findin
gs by
attrib
ute, th
e amo
unt o
f the a
ssoc
iated
un
der/o
verp
ayme
nt, th
e roo
t cau
se an
d res
olutio
n stat
us. A
udit
files r
emain
'ope
n' un
til all
iden
tified
issu
es ha
ve be
en re
solve
d an
d cor
recti
ons/a
djustm
ents
imple
mente
d acc
ordin
gly.
17.5.
3.4 If
the C
CN co
ntrac
ted fo
r the
prov
ision
of
any c
over
ed se
rvice
s, an
d the
CCN
’s co
ntrac
tor is
re
spon
sible
for pr
oces
sing c
laims
, then
the C
CN
shall
subm
it a cl
aims p
ayme
nt ac
cura
cy
perce
ntage
repo
rt for
the c
laims
proc
esse
d by t
he
contr
actor
.
Exce
eds
Exce
eds
Exce
eds
Deleg
ated v
endo
rs ar
e req
uired
to m
atch A
etna B
etter
Hea
lth’s
Claim
s aud
iting p
roce
dure
s. T
o mon
itor c
ompli
ance
with
this
contr
actua
l requ
ireme
nt, A
etna B
etter
Hea
lth co
nduc
ts a s
emi-
annu
al an
d ann
ual e
valua
tion o
f dele
gated
vend
or cl
aims
audit
ing pr
oces
ses,
and w
e will
includ
e a re
view
of DH
H sp
ecific
au
dit re
quire
ments
as pa
rt of
our d
elega
tion o
versi
ght p
roce
ss.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
39

115 Q.2

Part Two: Technical Proposal
Section Q: Claims Management
Q.2 Describe your methodology for ensuring that claims payment accuracy standards will be achieved per, Adherence to Key Claims Management Standards Section. At a minimum address the following in your response:
● The process for auditing a sample of claims as described in Key Claims Management Standards Section;
● The sampling methodology itself;
● Documentation of the results of these audits; and
● The processes for implementing any necessary corrective actions resulting from an audit.
Methodology for Claims Payment Accuracy Standards Claims Accuracy Standards Introduction Aetna Better Health takes pride in our claims performance, nationally – for all Aetna Better Health affiliates, we adjudicate over 80 percent of clean claims within 10 days of receipt and over 95 percent within 30 days of receipt. We also continuously evaluate methods to improve our payment processes and streamline payment. Our processing goal is to adjudicate 90 percent of all Louisiana clean claims within 15 business days of receipt and 99 percent within 30 business days of receipt. When a claim reaches either a pay, deny or reverse status, it is ready for final processing. We process claims in a pay status through weekly finance payment runs.
Our claims processing system determines the timeliness of claims adjudication. We use the claim’s receipt/clean date to calculate the submission window. Discounts are calculated at the time of the check run based on the receipt date of the claim. Within 48 hours of receiving a “pay status” claim, Aetna’s Automated Business Fulfillment (ABF) generates, prints and mails payments and corresponding remittance advice to providers, including the minimum required information elements as well as HIPAA compliant remit comments. We also provide electronic remittance advices to providers that include all fields required for compliance with the HIPAA 835 format.
For those clean claims which are denied due to lack of required or additional information necessary to review the claim, then the remittance advice will indicate the denial reason, with specificity, so that the provider is able to take the necessary action in support of claim resubmission. Additionally, Aetna Better Health providers are instructed to indicate that a claim is a “resubmission” and as such, allows the provider claim to be adjudicated using the same timely filing date as the original claim.
Key Claims Management Standards 1) Requirement - On a monthly basis, the Coordinated Care Network (CCN) shall submit a
claims payment accuracy percentage report to DHH. The report shall be based on an audit conducted by the CCN. The audit shall be conducted by an entity or staff independent of claims management as specified in this Section of the RFP, and shall utilize a randomly selected sample of all processed and paid claims upon initial submission in each month. A minimum sample consisting of two hundred (200) to two hundred-fifty (250) claims per year,
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
40

Part Two: Technical Proposal
Section Q: Claims Management
based on financial stratification, shall be selected from the entire population of electronic and paper claims processed or paid upon initial submission.
Response: Aetna Better Health's Claims Audit Department conducts an average of 48 post-payment audits a year; performing approximately two CMS1500 and two UB04 audits each month, thus exceeding the DHH’s requirements. Auditors review on average 187 Paid/Denied claims per health plan per week, depending on claim volume. The unit operates independent of our Claims Department and bears responsibility for submission of the monthly Claims Accuracy Percentage Report to DHH.
2) Requirement - The CCN shall process and, if appropriate, pay within thirty (30) calendar days, ninety-nine percent (99%) of all clean claims to providers for covered services delivered to a member.
Response: Aetna Better Health presently manages its claims payment process such that State mandated payment timeframes are either met or exceeded by the Claim’s Unit. For example, in Florida, Aetna Better Health manages the claim process such that the entire claims process is completed with 12 days on average, with an added 7 days tagged on to the process to account for check issuance purposes, so that the total time to process, on average is 20 business days (the requirement is 20 days), thus the claim payment time exceeds the mandatory timeframe in Florida. Aetna Better Health anticipates also exceeding the requirements of the Louisiana DHH, which provide for payment of 90% of clean claims within fifteen days and 99% payment within the allotted thirty calendar day timeframe.
3) Requirement - If a clean claim is denied on the basis the provider did not submit required information or documentation with the claim, and then the remittance advice shall specifically identify all such information and documentation. Resubmission of a claim with further information and/or documentation shall not constitute a new claim for purposes of establishing the timeframe for timely filing.
Response: When an otherwise clean claim denies specifically on the basis of lack of documentation required to process the claim, the remittance advice identifies with specificity the reason for the denial. Providers are instructed to resubmit the claim, along with the required document and to notate that the claim is a resubmission. As such, those claims with the “resubmission” notation receive are adjudicated for timely filing using the original submission date of the claim.
4) Requirement - To the extent that the provider contract requires compensation of a provider on a capitation basis or on any other basis that does not require the submission of a claim as a condition to payment, such payment shall be made to the provider by no later than:
The time period specified in the provider contract between the provider and the CCN, or if a time period is not specified in the contract:
- The tenth (10th) day of the calendar month if the payment is to be made by a contractor, or
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
41

Part Two: Technical Proposal
Section Q: Claims Management
- If the CCN is required to compensate the provider directly, within five (5) calendar days after receipt of the capitated payment and supporting member roster information from DHH.
Response: Aetna Better Health capitated contracts provide for payment by the 15th calendar day of the month. Network providers indicate their agreement with this timeframe as evidenced by their signing the agreement and the specific provider rate attachment.
5) The CCN shall not deny provider claims on the basis of untimely filing in situations regarding coordination of services or subrogation, in which case the provider is pursuing payment from a third party. In situations of third party benefits, the timeframes for filing a claim shall begin on the date that the third party completes resolution of the claim.
Response: Aetna Better Health acknowledges DHH’s timely failing related to subrogated or COB claims and will comply with said requirements. It is Aetna Better Health’s standard operating procedure to accept claims that are within the statutorily allotted timely filing limits, and those timeframes and other considerations applicable to subrogated claims or coordination of benefits.
6) Requirement - The CCN shall not pay any claim submitted by a provider who is excluded from participation in Medicare, Medicaid, or CHIP program pursuant to Section 1128 or 1156 of the Social Security Act or is otherwise not in good standing with DHH.
Response: As part of our credentialing process, Aetna Better Health queries the listing of excluded individuals, pursuant to the requirements of section 1128 or 1156 of the Social Security Act, and sees that, through the same process, those providers treating members covered under the agreement between Aetna Better Health and the DHH, are in good standing with DHH prior to completing the contracting and credentialing process. At re-credentialing, the procedures are followed to make certain good standing with DHH and lack of exclusion or restriction for participation in a Medicaid, Medicare or other government healthcare program. Aetna Better Health, through its vendor PDS, also conducts queries of non-network providers, on a periodic and random basis, to supplement its existing query processes related to the contracted network.
7) Requirement - Post-payment audits review, at a minimum,
• Results for each attribute tested for each claim selected;
• Amount of overpayment or underpayment for each claim processed or paid in error;
• Explanation of the erroneous processing for each claim processed or paid in error;
• Determination if the error is the result of a keying error or the result of error in the configuration or table maintenance of the claims processing system; and
• Claims processed or paid in error have been corrected.
Response: Aetna Better Health’s auditing processes exceed the DHH’s mandated audit elements and also include documentation of findings by attribute, the amount of
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
42

Part Two: Technical Proposal
Section Q: Claims Management
the associated under/overpayment, the root cause and resolution status. Audit files remain 'open' until all identified issues have been resolved and corrections/adjustments implemented accordingly.
8) Requirement: If the CCN contracted for the provision of any covered services, and the CCN’s contractor is responsible for processing claims, then the CCN shall submit a claims payment accuracy percentage report for the claims processed by the contractor.
Response: Delegated vendors are required to match Aetna Better Health’s Claims auditing procedures. To monitor compliance with this contractual requirement, Aetna Better Health conducts a semi-annual and annual evaluation of delegated vendor claims auditing processes, and we will include a review of DHH specific audit requirements as part of our delegation oversight process.
Claims Auditing Process Aetna Better Health maintains a Claims Quality Review Team to monitor quality standards for all claims processes. Under the direction of the director of Operations Process and Knowledge Management (OPKM), Quality Review Analysts conduct random and focused reviews of processed claims for payment, financial and procedural accuracy and provider inquiry calls, which focus on both accuracy and customer service skills. Performance is measured against established department guidelines.
Moreover, the Claims Quality Review Team fully audits the work of all new claims analysts for at least one month subsequent to their orientation and training. The audit starts at 100 percent of their work product and decreases to a standard two percent by the fifth week, provided the new claims analyst continues to meet claims accuracy standards. Finally, we review 16 provider calls per Claims Inquiry Representative per month, assessing the quality of service interaction and accuracy of information provided. Individual quality reports are presented to the Representative and their Supervisor for corrective action (e.g., live call monitoring) if appropriate.
Quality Review Analysts conduct a series of pre-payment audits including:
1) A one percent random sample of system-adjudicated claims,
2) A two percent random sample of all analyst-adjudicated claims,
3) A daily random sample of billed claims up to $49,999.99, and
4) 100 percent of all claims with billed charges over $50,000.
Aetna Better Health will have one full-time auditor assigned and we will pull a total of four audits per month: two UB (facility) files and two 1500 (physician) files based on a two week paid date/check cycle. Our sample size is 95/2/2 (95% confidence; the error rate is 2%; with a desired precision of +/- 2%) which is an average of 180+ claims reviewed each week. Each file provides Aetna Better Health with Payment and Financial Accuracy findings for the period audited and each file is distributed for review and response to all applicable departments. Below is a summary of the claim audit process utilized by an auditor:
Random Statistically Valid (RSV) process: Standard audit sample sizes are determined using a statistically valid sample, based on the total population size. The Claims Audit RSV table uses
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
43

Part Two: Technical Proposal
Section Q: Claims Management
an algorithm to determine the level of confidence, expected error rate and the desired precision required, as validated by Aetna Better Health and its affiliate Actuarial Department. The RSV size and total population is documented on each audit file. An automated program is utilized to extract the random claims sample with a proportion of paid or denied claims consistent with the total population.
Payment Accuracy– Reflects the percent of accurate claims. Calculation: The total number of audited claims correctly paid, divided by the total number of claims audited.
Financial Accuracy – Reflects the percent of dollars paid appropriately. Calculation: (Total $ Paid - $ Overpaid) + $ Underpaid = Total Correct Paid then (Total Correct Paid - Total $ Incorrect) / Total Correct Paid.
Claim Audit Process: In this step, contractual appropriateness of the provider attachment to the contract, e.g., fee schedules in accordance to the contract, is validated.
• Provider Validation: All contracted providers have a signed contract on file that is accessible for use by the Claims Department and the designated auditor(s). The auditor validates the contractual appropriateness of the provider attachment to the source documentation and reports any discrepancies, and simultaneously notifies the Network Development Department of the discrepancy and track on the audit file.
• Contract Validation: All provider network contracts should be accessible for use by the Audit Department. Validate the contract system configuration for appropriateness to the source documentation and report any discrepancies, and notify the Business Applications Management Department and track on the audit file. Each claim line is analyzed for appropriateness of contract term selection during the audit process.
• Benefit Validation: Benefits are validated by referring to the listing of Medicaid/DHH covered services, which should be accessible for use by the Audit Department. Validate the benefit system configuration for appropriateness to the source documentation and report any discrepancies, including reporting to the Business Applications Management Department and track on the audit file. Each claim line is analyzed for appropriateness of the benefit term selection during the audit process.
• Claim Validation: Data field validation for each claim can be verified either through viewing the paper claim submitted via Alchemy or viewing the EDI data submitted. All claims are subjected to analysis that involves but is not limited to the following:
− Valid Coding, e.g. proper use of codes and modifier codes;
− Member eligibility;
− Data entry into the systems is accurate;
− Timely Filing;
− Claim is associated with the correct treating provider;
− Prior Authorization requirements;
− Denial reasons applied correctly;
− Benefit application (including limitations and exclusions);
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
44

Part Two: Technical Proposal
Section Q: Claims Management
Coordination of Benefits application;
Claims history review for duplicate claims;
Manual pricing application;
Contracted Provider and Special Provider agreements, such as one-time case agreements and for both ensuring payment amount agrees with contracted rate;
Modifier discounts; and
Claims bundling/unbundling. Claims Payment Accuracy Percentage Report and Audit On average, Aetna Better Health's Claims Audit Department conducts an average of 48 randomized, post-payment audits a year; performing approximately two CMS1500 and two UB04 each month of both paper and electronically processed or paid claims. Auditors review on average 187 Paid/Denied claims per health plan per week, depending on claim volume, as such; we exceed the DHH’s mandate to sample up to 250 claims per year. Additional, the audit unit operates independently of our Claims Department and bears responsibility for submission of the monthly Claims Accuracy Percentage Report to DHH.
Sampling Frame
Random audit of billed claims, up to $49,999.99, on a daily basis
Quality standard maintained at 95% for external procedural (98% for Pennsylvania)
Quality standard maintained at 98% for payment
Quality standard maintained at 99% for financial accuracy
16 calls randomly audited for each CICR analyst on a monthly basis
Quality standard maintained at 95%
100% daily audit of billed claims, $50,000 and greater, on a daily basis
Quality standard maintained at 95% for external procedural (98% for Pennsylvania)
Quality standard maintained at 98% for payment
Quality standard maintained at 99% for financial accuracy
New employees audited at descending rate starting at 100% post training
Quality standard maintained at 95% for external procedural (98% for Pennsylvania)
Quality standard maintained at 98% for payment
Quality standard maintained at 99% for financial accuracy
Random audit of 1% of claims that have been systematically adjudicated
Quality standard maintained at 95% for external procedural
Quality standard maintained at 98% for payment
Quality standard maintained at 99% for financial accuracy
Three closed PCR audited per day, per eligible PDA
Quality standard maintained at 98% accuracy
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
45

Part Two: Technical Proposal
Section Q: Claims Management
Edits Utilized in Support of Claim Adjudication and Accuracy Standards Aetna Better Health maintains claims processing activities that include the application of comprehensive clinical and data related edits supporting the efficient, accurate, effective adjudication of claims. QNXT™, our core claims adjudication application has data related edits configured within its software and is supplemented by two clinical claims editing solutions. The first of the two clinical claims editing solutions, iHealth Technologies’ (iHT) Integrated Claims Management Services (ICM Services), applies select payment policies from one of the industry’s most comprehensive correct coding and Medical Policy content libraries. The second, McKesson’s ClaimCheck®, expands upon those capabilities by enabling our claims management team to define and combine specific claims data criteria, such as eligibility, provider or diagnosis, duplicate claims and other unique edits we set up to deliver enhanced auditing power.
The three applications utilize historic and “new day” claims information to detect questionable billing practices, such as new patient billing codes submitted by the same provider for the same member within a six month period or other improper or invalid coding schematics. These applications also assist in identifying fraudulent and abusive billing patterns by generating reports that indicate trending and outliers of provider billing behavior. Inbound claims are initially checked for items such as member eligibility, covered services, excessive or unusual services for gender or age (e.g. “medically unlikely”), duplication of services, prior authorization, invalid procedure codes, and duplicate claims. Claims billed in excess of $50,000 are automatically pended for review, as are any requiring additional documentation (e.g. medical records) in order to determine the appropriateness of the service provided. Professional claims that reach an adjudicated status of “Pay” are automatically reviewed against nationally recognized standards such as the Correct Coding Initiative (CCI), medical policy requirements [e.g., American Medical Association (AMA)], and other requirements.
QNXT™ Data Edits QNXT™ has over 400 business rules that MCP configures to support enforcement of our claims Policies and Procedures (P&Ps). The application of specific conditions, restrictions, and validation criteria promote the accuracy of claim processing against AHCCCS standards. The edits can result in claims pending or denying depending on the editing logic. For example, if the member is not eligible on the date of service, QNXT™ will automatically deny the claim. In the event that the category of service of the provider of record does not match the procedure code billed the claim will pend for manual review to validate accuracy of provider set-up.
Examples of data edits specific to QNXT™ include the following:
Benefits Package Variations QNXT™ automatically analyzes CPT, REV, and HCPC codes to determine whether specific services are covered under the contract or benefit rules. If services are not covered, the system will automatically deny the respective claim line. The claim line will deny with the appropriate HIPAA remittance remark on the EOB.
Data Accuracy QNXT™ is continually updated based on the most current code sets available (HCPCS, REV, CPT codes) by year. As new codes are added, terminated, or changed, we update the codes in QNXT™ so the system is always in compliance with HIPAA standards. If a network provider
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
46

Part Two: Technical Proposal
Section Q: Claims Management
bills a code that has been terminated, QNXT™ will deny the claim line and advise the provider the code is invalid via remittance advice.
Adherence to Prior Authorization Requirements QNXT™ is configured to enforce the supporting documentation requirements of certain services. In addition, QNXT™ has the ability to configure Prior Authorization (PA) by code, provider type, and place of service. QNXT™ is configured to automatically identify certain types of authorizations for medical director review. Claim edit rules are set to validate the claim against the network provider, member, dates of service, services rendered, and units authorized.
Provider Qualifications QNXT™ provider files are configured by specialty and category of service. This allows for the enforcement of categories of service and provider type on claims validation. Certain procedures can only be performed by select network provider types. For example, QNXT™ will not permit the processing of a claim for in-office heart surgery by a podiatrist. iHealth lends additional support in this regard, reviewing any claim line set to “Pay” for billing appropriateness by specialty.
QNXT™ checks other provider-specific items as well, verifying, for example, that each provider has obtained the requisite National Provider Identifier (NPI) or its equivalent and included the identifier on all claims submissions.
Duplicate Billing Logic QNXT™ uses a robust set of edits to determine duplication of services. Examples are same member, same date, same network provider, same service, or any combination of these criteria. In addition, claim lines set to “Pay” are subjected to iHealth’s duplicate logic. This logic protects against MCP paying for services rendered by the same physician or other physicians within the same provider group
ClaimCheck® Edits ClaimCheck® is a comprehensive code auditing solution that supports QNXT™ by applying expert industry edits from a provider recognized knowledge base to analyze claims for accuracy and consistency with Aetna Better Health policies and procedures. ClaimCheck® clinical editing software identifies coding errors in the following categories:
• Procedure unbundling
• Mutually exclusive procedures
• Incidental procedures
• Medical visits, same date of service
• Bilateral and duplicate procedures
• Pre and Post-operative care
• Assistant Surgeon
• Modifier Auditing
• Medically Unlikely
Network providers do received access to Clear Claim Connection®, a provider reference tool that helps providers optimize their claims submission accuracy. Currently there are 2300
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
47

Part Two: Technical Proposal
Section Q: Claims Management
provider groups have registered to use this web-based tool that providers can use to understand clinical editing logic utilized by Aetna Better Health. This allows them to better understand the rules and clinical rationale affecting adjudication. Providers access Clear Claim Connection® through Aetna Better Health’s internet web portal via secure login.
Various coding combinations can then be entered to determine why, for example, a particular coding combination resulted in a denial. The provider may also review coding combinations prior to claim submission, to determine if applicable auditing rules and clinical rationale will deny the claim before it is submitted.
iHealth Edits iHealth clinically edits claims to assist Aetna Better Health to promote the proper and fair payment of professional DME and outpatient claims.
Coding Accuracy If the services are up-coded, or unbundled, iHealth will alert the Claims Department to deny the claim line along with the specific clinical editing policy justification for the denial. The claim line will deny with the appropriate HIPAA remittance remark on the Explanation of Benefits (EOB).
Duplicate Billing Logic In addition, claim lines set to “Pay” are subjected to iHealth’s duplicate logic. This logic protects against Aetna Better Health paying for services rendered by the same physician or other physicians within the same provider group
Durable Medical Equipment (DME) Editing iHealth Technologies’ (iHT) performs edits related to select DME payment policies that align with Medicaid covered service policies. These DME edits include but are not limited to; DME rentals, oxygen and oxygen systems, hospital beds and accessories, external infusion pumps and anatomic/functional modifiers required for DME services.
Procedure Code Guidelines - iHealth Aetna Better Health follows the AMA CPT-4 Book and CMS HCPCS Book, which both provide instructions regarding code usage. iHT has developed these guidelines into edits. For example, if a vaccine administration code is billed without the correct vaccine/toxoid codes, Aetna Better Health would then deny the code as inappropriate coding based on industry standards. According to the AMA CPT Book, this vaccination must be reported in addition to the vaccine and toxoid code(s).
Procedure Code Definition Policies - iHealth iHT supports correct coding based on the definition or nature of a procedure code or combination of procedure codes. These editing policies will either bundle or re-code procedures based on the appropriateness of the code selection. For example, if a provider attempts to unbundle procedures, iHT will apply editing logic that will bundle all of the procedures billed into the most appropriate code. For example, if a provider bills an office visit and also bills separately for heart monitoring with a stethoscope at the same visit, iHT will rebundle the service into the appropriate evaluation and management or office code.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
48

Part Two: Technical Proposal
Section Q: Claims Management
Fraud & Abuse Aetna Better Health’s Fraud and Abuse Department, under the direction of the VP of Health Plan Operations, utilizes claims payment tracking and trending reports, claims edits, audits and provider billing patterns as indicators of potential fraud and abuse. The Fraud and Abuse Department uses this information to detect aberrant provider billing behavior, prompting additional analysis and investigation. Aetna Better Health’s fraud and abuse personnel work in conjunction with Aetna Better Health’s Provider Services and Compliance Departments to address the questionable behavior(s) through provider education and outreach. If MCP discovers, or becomes aware, that an incident of potential/suspected fraud and abuse has occurred, internal P&Ps mandate that we report the incident to AHCCCS within 10 business days of discovery by completing and submitting the confidential AHCCCS Referral for Preliminary Investigation form.
Claims Audit and Ongoing Accuracy Monitoring – Supportive Tools Aetna Better Health facilitates inter-departmental exchange of information and the external exchange of information between these departments and our providers through reporting and other educational interactions. We then inform providers of, among other things, any issue(s) potentially impacting claim adjudication or any opportunities for provider education. We utilize a suite of tools, including but not limited to, scheduled and ad hoc reports to monitor claim receipts, automated claims processing, manual claims adjudication, and check and remittance advice production/distribution. These tools and reports include, but are not limited to:
Pended Claims and Aging Report – the pended and aging claim reports allow management to effectively intervene when and where necessary to improve accurate and timely adjudication of claims. Populated hourly and reviewed daily, the tool presents claims counts and billed dollars by pend reason and claim age, with drill down capabilities to gather for review detailed claims information.
In-Process Claim Reports – In-process claims report allow management to effectively track and manage all claims in process so that needed interventions may be applied to improve the accuracy and timeliness of claim adjudication.
Claims Payment Processing Reports – This is a set of retrospective claims adjudication reports that are produced and reviewed weekly to provide claims, health plan operations and finance units with data to support reconciliation of claim volume and adjudicated dollars including information to support the reinsurance process.
Monthly Claims Dashboard –This management tool can be used to identify trends related to critical claims metrics. The claims dashboard is reviewed monthly by compliance, encounters, health plan operations, and finance personnel to identify appropriate action plans.
These reports are also utilized to proactively manage claims workflow so that timeliness is addressed before it becomes an issue. For example, based on such analysis, the Claim Department can take proactive action to address any trends that indicate a potential issue such as turnaround times or inventory levels for aging claims. It is our standard operating procedure to immediately determine a root cause and develop and implement the appropriate action plan. In the past, these plans have included one or more of the following:
1) System reconfiguration;
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
49

Part Two: Technical Proposal
Section Q: Claims Management
2) Staff overtime;
3) Workload balancing;
4) Training of personnel and providers; and
5) Hiring and training temporary workers to assist with the reduction of claim inventories.
Based on our claims volume, we adjust hiring to accommodate any increased trends. Additional information on our claims monitoring and resolution of deficiencies process can be found in an illustration following our response.
Corrective Actions Process and Resolution of Deficiencies When pre-payment errors are discovered during the above referenced audits, claims are pended for analysis and adjusted as required for final adjudication. If an error in adjudication of the claim indicates a system configuration problem, the issue is routed to our Business Application Management (BAM) Department for further review, analysis, testing, and correction. If adjudication errors are identified relative to manually adjudicated claims, we review/update pertinent policies and procedures and institute additional training accordingly. If our audit identifies a provider billing issue, the information is forwarded to provider services personnel for provider outreach and education as necessary.
To further support quality reviews of claims processing accuracy, a post-payment audit occurs outside the Claims Department, where stratified random samples and focused audits of paid and denied claims are overseen. The purpose of these activities is to audit compliance of claims adjudication with state regulatory requirements and provider contracts. Audit results are shared with Claims management in order to identify training and/or coaching opportunities, qualify merit-based compensation and implement corrective action as necessary.
It is our standard operating procedure to continuously monitor the adequacy of our claims adjudication process to determine its effectiveness. Aetna Better Health uses the Plan-Do-Study-Act (PDSA) model to assess our claims administration, adjudication and management processes. Our PDSA approach involves the network development and provider services units and leadership from Aetna Better Health’s entire organization. The PDSA model for continuous improvement provides the framework for our approach to developing and implementing network interventions through the following steps:
1. Plan. Recognize an opportunity and plan a change. 2. Do. Test the change. Carry out a small-scale study. 3. Study. Review the test, analyze the results and identify what
we’ve learned. 4. Act. Take action based on what we learned in the study step: If
the change was ineffective, repeat cycle with a different plan. We incorporate successful interventions into our network development/management approach, using what we learned to plan new improvements, beginning the cycle again.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
50

Part Two: Technical Proposal
Section Q: Claims Management
The leadership from Aetna Better Health’s entire organization participates in the PDSA process. Supporting this process is our Service Improvement Committee, the QM/UM Committee and QMOC. Each of these committees includes cross functional and multidisciplinary leadership from across our operations. This means that member services, quality management, utilization management, grievance and appeals, and operations (e.g., claims, etc) are aware of and contribute to our claims administration planning and performance improvement activities. This organizational commitment to meeting the needs of our providers is a hallmark of Aetna Better Health success.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
51

116 Q.3

Part Two: Technical Proposal
Section Q: Claims Management
Q.3 Describe your methodology for ensuring that the requirements for claims processing, including adherence to all service authorization procedures, are met.
Introduction to Aetna Better Health’s Claim System Aetna Better Health along with its affiliates claims processing activities include the application of comprehensive clinical and data related edits that support the efficient, effective adjudication of claims. QNXT™, our core claims adjudication system, has data-related edits configured within its software and is supplemented by two clinical claims editing solutions. The first of the two clinical claims editing solutions, iHealth Technologies’ (iHT) Integrated Claims Management Services (ICM Services), applies select payment policies from one of the industry’s most comprehensive correct coding and Medical Policy content libraries. The second, McKesson’s ClaimCheck®, expands upon those capabilities by enabling our claims management team to define and combine specific claims data criteria, such as provider or diagnosis, to set up unique edits that deliver enhanced auditing power.
Inbound claims are initially checked for items such as member eligibility, covered services, excessive or unusual services for gender or age (e.g. “medically unlikely”), duplication of services, prior authorization compliance, invalid procedure codes, and duplicate claims. Claims billed in excess of $50,000 are automatically pended for review, as are any requiring additional documentation (e.g. medical records) in order to determine the appropriateness of the service provided. Aetna Better Health maintains a staff of qualified, medically trained and appropriately licensed personnel – consistent with NCQA accreditation standards – whose primary duty is to assist in the determination of medical necessity. Professional claims (CMS1500s) that reach an adjudicated status of “Pay” are automatically reviewed against nationally recognized standards such as the Correct Coding Initiative (CCI), medical policy requirements (e.g., American Medical Association (AMA)), and maximum unit requirements supplied by state agencies, with recommendations applied during an automatic re-adjudication process. Other methodologies utilized throughout the auto-adjudication process include, but are not limited to, Multiple Surgical Reductions and Global Day E & M Bundling.
Claims Management System Aetna Better Health uses the QNXT™ management information system, a product of Trizetto Inc., to process Medicaid member health claims. This rules-based system allows us to set multiple edits to test claims validity, allows us to customize the edits, and to otherwise pay or deny claims in accordance with the Louisiana Department of Health and Hospitals’ claims adjudication requirements. The QNXT™ edits include, but are not limited to,
• Verification of member eligibility
• Verification of covered services
• Determining whether services are within the scope of a provider’s specialty
• Valid prior authorization
• Submission of required documentation
• Excessive or unusual services based on the member’s age or gender
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
52

Part Two: Technical Proposal
Section Q: Claims Management
• Duplication of services
• Invalid procedure codes
• Duplicate claims
Based on one or more of these edits, unusual items result in the claim being denied or pended for further review. The system also automatically pends for further review any claims over a certain dollar amount and requires that certain codes be accompanied with supporting medical records to determine the appropriateness of the service provided.
QNXT™ Data Edits in Support of Meeting Claims Processing Requirements QNXT™ has over 400 business rules that Aetna Better Health’s Business Application Management (BAM) Department configures to enforce claims-related Policies and Procedures (P&Ps). The application of specific conditions, restrictions, and validation criteria promotes the accuracy of claim processing against relevant and established state standards. The edits can result in claims pending or denying depending on the editing logic. For example, if the member is not eligible on the date of service, QNXT™ will automatically deny the claim. In the event that the category of service on the provider of record does not match the procedure code billed, the claim will pend for manual review to validate accuracy of provider set-up.
Examples of data edits specific to QNXT™ include the following:
Benefits Package Variations QNXT™ automatically analyzes CPT, REV, and HCPC codes to determine whether specific services are covered under the contract or benefit rules. If services are not covered, the system will automatically deny the respective claim line. The claim line will deny with the appropriate HIPAA remittance remark on the EOB.
Data Accuracy QNXT™ is continually updated based on the most current code sets available (HCPCS, REV, CPT codes) by year. As new codes are added, terminated, or changed, we update the codes in QNXT™ so the system is always in compliance with HIPAA standards. If a network provider bills a code that has been terminated, QNXT™ will deny the claim line and advise the provider the code is invalid via remittance advice.
Adherence to Prior Authorization Requirements QNXT™ is configured to enforce the supporting documentation requirements of certain services. In addition, QNXT™ has the ability to configure Prior Authorization (PA) by code, provider type, and place of service. QNXT™ is configured to automatically identify certain types of authorizations for medical director review. Claim edit rules are set to validate the claim against the network provider, member, dates of service, services rendered, and units authorized.
Provider Qualifications QNXT™ provider files are configured by specialty and category of service. This allows for the enforcement of categories of service and provider type on claims validation. Certain procedures can only be performed by select network provider types. For example, QNXT™ will not permit the processing of a claim for in-office heart surgery by a podiatrist. iHealth lends additional support in this regard, reviewing any claim line set to “Pay” for billing appropriateness by specialty. QNXT™ checks other provider-specific items as well, verifying, for example, that each
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
53

Part Two: Technical Proposal
Section Q: Claims Management
provider has obtained the requisite National Provider Identifier (NPI) or its equivalent and included the identifier on all claims submissions.
Member Eligibility and Enrollment QNXTTM validates the date of service against the member’s enrollment segment to determine if the member was eligible on the date of service. If the member was not eligible on the date of service, the system will automatically deny the claim using the appropriate HIPAA approved remittance comment.
Duplicate Billing Logic QNXT™ uses a robust set of edits to determine duplication of services. Examples are same member, same date, same network provider, same service, or any combination of these criteria. In addition, claim lines set to “Pay” are subjected to iHealth’s duplicate logic. This logic protects against payment for services rendered by the same physician or other physicians within the same provider group
Other Claims Processing Edits and Tools Utilized to Ensure Accuracy Throughout Adjudication Process
ClaimCheck® Edits ClaimCheck® is a comprehensive code auditing solution that supports QNXTTM by applying expert industry edits from a provider recognized knowledge base to analyze claims for accuracy and consistency with relevant P&Ps. ClaimCheck® clinical editing software identifies coding errors in the following categories:
• Procedure unbundling
• Mutually exclusive procedures
• Incidental procedures
• Medical visits, same date of service
• Bilateral and duplicate procedures
• Pre and Post-operative care
• Assistant Surgeon
• Modifier Auditing
• Medically Unlikely Services iHealth Edits Aetna Better Health also uses Integrated Claims Management Services (ICM Services), powered by iHealth Technologies, to enhance QNXT™ edit functionality for professional claims that reach an adjudicated status of “pay”. Aetna Better Health has developed algorithms with iHealth to detect potential claims upcoding, with follow-up procedures for chart audits as appropriate. iHealth clinically edits claims to assist state agencies in promoting proper and fair payment of claims. Examples of applied edits include:
Coding Accuracy If services are up-coded or unbundled, iHealth will alert the Claims Department to deny the claim line along with the specific clinical editing policy justification for the denial. The claim
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
54

Part Two: Technical Proposal
Section Q: Claims Management
line will deny with the appropriate HIPAA remittance remark on the Explanation of Benefits (EOB).
Duplicate Billing Logic In addition, claim lines set to “Pay” are subjected to iHealth’s duplicate logic. This logic protects against payment for services rendered by the same physician or other physicians within the same provider group
Durable Medical Equipment (DME) Editing iHealth Technologies’ (iHT) performs edits related to select DME payment policies that align with state agencies’ respective covered service policies. These edits include but are not limited to, DME rentals, oxygen and oxygen systems, hospital beds and accessories, external infusion pumps and anatomic/functional modifiers required for DME services.
Procedure Code Guidelines Aetna Better Health follows the AMA CPT-4 Book and CMS HCPCS Book, which provide instructions regarding code usage. iHT has developed these guidelines into edits. For example, if a vaccine administration code is billed without the correct vaccine/toxoid codes, we will deny the code as inappropriate coding based on industry standards. According to the AMA CPT Book, this vaccination must be reported in addition to the vaccine and toxoid code(s).
Procedure Code Definition Policies iHT supports correct coding based on the definition or nature of a procedure code or combination of procedure codes. The ability to code in this manner supports prior authorization requirements during claim adjudication. Furthermore, these editing policies will either bundle or re-code procedures based on the appropriateness of the code selection. For example, if a provider attempts to unbundle procedures, iHT will apply editing logic that will bundle all of the procedures billed into the most appropriate code. For example, if a provider bills an office visit and also bills separately for heart monitoring with a stethoscope at the same visit, iHT will rebundle the service into the appropriate E&M or office code.
Claims Development Aetna Better Health has existing policies and procedures whereby we 'develop' claims requiring additional information from a service provider or third party. Non-clean claims are pended and a letter sent to the provider indicating, at a minimum, the nature of the problem, instructions on its remedy (e.g. submission of missing documentation) and the following:
• Member name
• Provider claim number
• Patient account number or unique member identification number
• Date of service
• Total billed charges
• Coordinated Care Network’s (CCN’s) name; and
• The date the report was generated
Claims analysts will attempt to follow up three times within the allotted time; if a response from the provider has not been received within the allotted time, the claim is denied.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
55

Part Two: Technical Proposal
Section Q: Claims Management
Ensuring Adherance to Claims Processing Requirements Claims Monitoring Process Aetna Better Health uses a suite of regularly scheduled and ad hoc reports to monitor claim receipts, production, payment, proper applicability of State mandates and quality activity on a daily, weekly and monthly basis. Sample reports include, but are not limited to, the following:
• Mail Counts and Reconciliation Reports: Used to trend receipts, plan resource allocation and verify that all claims received are accounted for in the system.
• Pended Claims Audit by Provider or Age: Includes all claims that fail auto adjudication or are suspended for manual review.
• Unfinished Claims Report: Identifies all claims by age and processing status category (e.g., open, pay, deny, pend, reverse).
• Denial Analysis: Trends denied claims with corresponding reason for the denial.
• Claims Production: Monitors daily, weekly and monthly manual and auto adjudication production.
• Claims Performance Reporting: Monitors turnaround time for clean claims over selected time periods.
• Quality Review Statistics: Reports by individual and plan as well as error frequency.
Aetna Better Health’s Claims Department uses these and other reports to track specific claims and monitor workflow to see that we meet our processing standards and are compliant with DHH’s standards. In addition, senior management regularly reviews claims key indicators, including claims awaiting payment and a Claims Dashboard Report. Aetna Better Health employs workflow management and comprehensive personnel training to keep claims backlogs to a minimum. Claims Supervisors also monitor daily mail receipt volumes and staffing to monitor whether we are devoting adequate resources to meet processing standards. If our reports reflect a less than favorable trend, we immediately develop and implement appropriate corrective action plans. For example, we might apply additional staffing to clear up a backlog of aged claims through a combination of overtime hours, temporary labor and workload balancing.
Pre and Post-Payment Review Aetna Better Health maintains a Claims Quality Review team to monitor quality standards for all claims processes. Under the direction of the director of Operations Process and Knowledge Management (OPKM), Quality Review Analysts conduct random and focused reviews of processed claims for payment, financial and procedural accuracy. Performance is measured against established department guidelines.
Quality Review Analysts conduct a series of pre-payment audits including: 1) a one percent random sample of system-adjudicated claims, 2) a two percent random sample of all analyst-adjudicated claims, 3) a daily random sample of billed claims up to $49,999.99, and 4) 100 percent of all claims with billed charges over $50,000. When pre-payment errors are discovered during these audits, claims are pended for analysis and adjusted as required for final adjudication. If an error in adjudication of the claim indicates a system configuration problem, the issue is routed to our Business Application Management (BAM) Department for further review, analysis, testing, and correction. If adjudication errors are identified relative to manually
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
56

Part Two: Technical Proposal
Section Q: Claims Management
adjudicated claims, we review/update pertinent policies and procedures and institute additional training accordingly. If our audit identifies a provider billing issue, the information is forwarded to provider services personnel for provider outreach and education as necessary.
To further support quality reviews of claims processing accuracy, an independent (does not report to claims leadership) post-payment Audit Department is responsible for conducting stratified random samples and focused audits of paid and denied claims. The purpose of these activities is to audit compliance of claims adjudication with state regulatory requirements and provider contracts. Audit results are shared with claims management in order to identify training and/or coaching opportunities, qualify merit-based compensation and implement corrective action as necessary.
Electronic Data Interface (EDI) To assist us in processing and paying claims efficiently, accurately and timely, Aetna Better Health encourages providers to submit claims electronically. To facilitate electronic claims submissions, we have developed business relationships with ten major clearinghouses, including RelayHealth, Emdeon, MedAvant, among others. We receive EDI claims directly from these clearinghouses, process them through pre-import edits to see to the validity of the data, HIPAA compliance and member enrollment and then upload them into QNXT™ each business day. Within 24 hours of file receipt, we provide production reports and control totals to all trading partners to validate successful transactions and identify errors for correction and resubmission.
Manual Claims Acquisition (Paper) Providers can submit paper claims to Aetna Better Health’s designated post office box. Each business day, our imaging vendor, FutureVision, retrieves, opens and sorts the mail using our pre-defined criteria for either imaging and scanning or distribution directly to Aetna Better Health. They assign each claim a unique reference number based on the date received and use it to track the claim throughout the entire adjudication process. FutureVision then converts the imaged data into an EDI ready format within 24 to 48 hours of initial receipt and forwards it to Aetna Better Health. Each business day, our IT processing personnel upload the data into QNXT™ via EDI processing. Only users with approved, secured access to claims information can view this information.
If FutureVision, for whatever reason, is unable to scan certain documents, including non-claim submissions (e.g., returned member/provider mail, explanations of benefits, checks, medical records documentation) and certain paper claims (e.g., illegible claims or poor quality printed claims), FutureVision forwards these paper documents to our Claims Administration Department, where we sort and distribute them to the appropriate department(s). We assign each claim document a unique identifying number within 24 hours of receipt and electronic store the document. We then shred the paper claims and store the electronic document in a locked and secure location prior to entering the data into QNXT™, which occurs within 2 days of receipt of the document(s) from FutureVision.
Clear Claim Connection® Aetna Better Health offers network providers access to Clear Claim Connection®, a web-based, code-auditing reference tool designed to mirror how code combinations are evaluated during the auditing of professional claims. Clear Claim Connection® enables Aetna Better Health to disclose its claim auditing rules to providers, along with the clinical rationale inherent to the
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
57

Part Two: Technical Proposal
Section Q: Claims Management
system. Currently, there are approximately 2300 provider groups registered through Aetna Better Health to use this web-based tool. Providers access Clear Claim Connection® through Aetna Better Health’s web portal via secure login. Various coding combinations and claim scenarios can then be entered by the provider (or his/her designated staff) to determine why, for example, a particular coding combination may result (or did result) in a denial. The provider may also review coding combinations prior to claim submission, to determine if applicable auditing rules and clinical rationale will deny the claim before it is submitted or if other supportive information is necessary on the provider’s behalf, in order to promote a clean claim submission. Clear Claim Connection® databases and logic are updated regularly by Aetna Better Health for consistency with claim handling requirements, new procedure codes, current healthcare trends, and/or medical and technological advances.
The table that follows provides a mapping of claims processing methodology requirements to an explanation of Aetna Better Health’s handling or policies in support of compliance.
Requirement Meets or Exceeds
Requirement Explanation
17.2.1 Confirming eligibility on each member as claims are submitted on the basis of the eligibility information provided by DHH and the Enrollment Broker that applies to the period during which the charges were incurred;
Meets Inbound claims are uploaded to QNXT™, our claims processing system, where they are subjected to multiple header and line item edits. Among these are edits that compare service data to eligibility information provided by DHH and the Enrollment Broker in order to confirm members' eligibility during the period to which charges were incurred.
17.2.2 A review of the entire claim within five (5) working days of receipt of an electronic claim, to determine that the claim is not a clean claim and issue an exception report to the provider indicating all defects or reasons known at that time that the claim is not a clean claim. The exception report shall contain at a minimum the following information:
Meets
17.2.2.1 Member name; Meets
17.2.2.2 Provider claim number, patient account number, or unique member identification number;
Meets
17.2.2.3 Date of service; Meets 17.2.2.4 Total billed charges; Meets
17.2.2.5 CCN’s name; and
Meets
Level I and II edits occur at the clearinghouse and handled within 5 working days. The clearinghouse bears responsibility for providing exception reports to the providers.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
58

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
17.2.2.6 The date the report was generated.
Meets
17.2.3 Medical necessity; Meets Clinical edits are capable of verifying when a procedure is for certain gender or an age, e.g., the claim edits will be able to detect if pregnancy-related services are inadvertently being assigned to a male member. Refer to 17.2.4 applies edits accordingly.
17.2.4 Prior Approval – The system shall determine whether a covered service required prior approval and if so, whether the CCN granted such approval;
Meets
17.2.5 Duplicate Claims – The system shall in an automated manner, flag a claim as being exactly the same as a previously submitted claim or a possible duplicate and either deny or pend the claim as needed;
Meets
17.2.6 Covered Services - See that the system verifies that a service is a covered service and is eligible for payment;
Meets
17.2.7 Provider Validation - See that the system shall approve for payment only those claims received from providers eligible to render service for which the claim was submitted;
Meets
17.2.8 Quantity of Service - See that the system shall evaluate claims for services provided to members to see that any applicable benefit limits are applied;
Meets
17.2.9 Perform system edits for valid dates of service, and assure that dates of services are valid dates such as not in the future or outside of a member’s Medicaid eligibility span;
Meets
Aetna Better Health's Business Application Management (BAM) Department is responsible for the accurate and efficient configuration of functional business requirements and rules within QNXT™ necessary for administrative services to occur. This includes meeting claims processing standards and auto-adjudication targets. The objectives of the build are to:
• Analyze business requirements to design and configure an optimal and efficient system build that will minimize the need for manual processing.
• Load the rules and requirements of a new health plan, product or business function in the claims processing system, including eligibility file layout, provider contracts, fee schedules and member benefits and prior authorization requirements.
• Complete configuration documentation while entering the build information.
• Audit and validate the build based on the rules and requirements stated by the health plan and the implementation team.
• Jointly perform unit testing with the Operations Process Knowledge Management (OPKM) Testing team to validate that the system is operational and meets business requirements.
• Participate in end-to-end testing with all impacted departments to see that the system is operating as expected.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
59

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
17.2.10 Perform post-payment review on a sample of claims to see that services provided were medically necessary; and
Meets
17.2.11 Have a staff of qualified, medically trained and appropriately licensed personnel, consistent with NCQA accreditation standards, whose primary duties are to assist in evaluating claims for medical necessity.
Meets
Aetna Better Health maintains an independent (i.e. does not report to claims leadership) post-payment Audit Department responsible for drawing stratified random samples and conducting focused audits of paid and denied claims. The purpose of these activities is to audit compliance of claims adjudication with DHH regulatory requirements and provider contracts. Audit findings are shared with Claims management for root cause analysis and corrective action.
17.3 Explanation of Benefits (EOBs) 17.3.1 The CCN shall within forty-five (45) days of payment of claims, provide individual notices to a sample group of the members who received services. The required notice must specify: 17.3.1.1.1 The service furnished;
17.3.1.1.2 The name of the provider furnishing the service; 17.3.1.1.3 The date on which the service was furnished; and 17.3.1.1.4 The amount of the payment made for the service. 17.3.2 The CCN shall also:
17.3.2.1 Include in the sample, claims for services with hard benefit limits, denied claims with member responsibility, and paid claims (excluding ancillary and anesthesia services). 17.3.2.2 Stratify paid claims sample to see that all provider types (or specialties) are represented in the pool of generated EOBs. To the extent that the CCN considers a particular specialty (or provider) to warrant closer scrutiny, the CCN may over sample the group. The paid claims sample should be a minimum of two hundred (200) to two hundred-fifty (250) claims per year.
Aetna Better Health acknowledges and will comply. All elements required in the Explanation of Benefits will be included in the EOB provided to CCN members. As new EOB requirements and elements are updated, Aetna Better Health will comply and as such, make necessary modifications to existing EOB reported fields as required.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
60

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
17.3.3 The CCN shall track any complaints received from members and resolve the complaints according to its established policies and procedures. The resolution may be member education, provider education, or referral to DHH. The CCN shall use the feedback received to modify or enhance the EOB sampling methodology.
Meets Aetna Better Health maintains an internal, proprietary application that supports the Grievance and Appeals process by tracking member and provider issues from inception to resolution. This affords us the means to address not only issues affecting individual member and provider satisfaction, but potential trends in the delivery system as a whole, permitting health plan personnel to take prompt, corrective steps to minimizing risks to performance standards. Feedback received during this process or feedback received through other means, will be shared with the appropriate personnel within the Claims unit for future handling and modifications in concert with the IT Department.
17.4.1 Each remittance advice generated by the CCN to a provider shall, if known at that time, clearly identify for each claim, the following information:
Meets
17.4.1.1 The name of the member; Meets
17.4.1.2 Unique member identification number;
Meets
17.4.1.3 Patient claim number or patient account number;
Meets
17.4.1.4 Date of service; Meets
17.4.1.5 Total provider charges; Meets
17.4.1.6 Member liability, specifying any co-insurance, deductible, co-payment, or non-covered amount;
Meets
17.4.1.7 Amount paid by the CCN; Meets
17.4.1.8 Amount denied and the reason for denial; and
Meets
QNXT™, Aetna Better Health's core transaction processing system, generates paper Remittance Advices (RAs) for our providers. In addition, providers taking advantage of our Electronic Fund Transfer (EFT) capability have the option of receiving Electronic Remittance Advices (ERAs). Business Application Management (BAM) personnel configure QNXT™ to generate RAs formatted such that required data elements are readily identifiable.
The following statement shall be included on each remittance advice sent to providers: “I understand that payment and satisfaction of this claim will be from federal and state funds, and that any false claims, statements, documents, or concealment of a material fact, may be prosecuted under
Meets Aetna Better Health’s existing remittance advice can be configured to meet this requirement.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
61

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
applicable federal and/or state laws.”
17.5.1.1 The CCN shall see that ninety percent (90%) of all clean claims for payment of services delivered to a member are paid by the CCN to the provider within fifteen (15) business days of the receipt of such claims. 17.5.1.2 The CCN shall process and, if appropriate, pay within thirty (30) calendar days, ninety-nine percent (99%) of all clean claims to providers for covered services delivered to a member.
Aetna Better Health presently manages its claims payment process such that State mandated payment timeframes are either met or exceeded by the Claim’s Unit. For example, in Florida, Aetna Better Health manages the claim process such that the entire claims process is completed with 12 days on average, with an added 7 days tagged on to the process to account for check issuance purposes, so that the total time to process, on average is 20 business days (the requirement is 20 days), thus the claim payment time exceeds the mandatory timeframe in Florida. Aetna Better Health anticipates also exceeding the expectations of the Louisiana Department of Health and Hospitals, which provide for payment of 90% of clean claims within fifteen days and 99% payment within the allotted thirty calendar day timeframe.
17.5.1.3 If a clean claim is denied on the basis the provider did not submit required information or documentation with the claim, then the remittance advice shall specifically identify all such information and documentation. Resubmission of a claim with further information and/or documentation shall not constitute a new claim for purposes of establishing the timeframe for timely filing.
Meets When an otherwise claim denies specifically on the basis of lack of documentation required to process the claim, the remittance advice identifies with specificity the reason for the denial. Providers are instructed to resubmit the claim, along with the required document and to notate that the claim is a resubmission. As such, those claims with the “resubmission” notation receive are adjudicated for timely filing using the original submission date of the claim.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
62

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
17.5.1.4 To the extent that the provider contract requires compensation of a provider on a capitation basis or on any other basis that does not require the submission of a claim as a condition to payment, such payment shall be made to the provider by no later than: ● The time period specified in the provider
contract between the provider and the CCN, or if a time period is not specified in the contract:
− The tenth (10th) day of the calendar month if the payment is to be made by a contractor, or
− If the CCN is required to compensate the provider directly, within five (5) calendar days after receipt of the capitated payment and supporting member roster information from DHH.
Meets Aetna Better Health capitated contracts provide for payment by the 15th calendar day of the month. Network providers indicate their agreement with this timeframe as evidenced by their signing the agreement and the specific provider rate attachment.
17.5.1.5 The CCN shall not deny provider claims on the basis of untimely filing in situations regarding coordination of services or subrogation, in which case the provider is pursuing payment from a third party. In situations of third party benefits, the timeframes for filing a claim shall begin on the date that the third party completes resolution of the claim.
Meets Aetna Better Health acknowledges and will comply. Aetna Better Health acknowledges DHH’s timely failing related to subrogated or COB claims and will comply with said requirements. It is Aetna Better Health’s standard operating procedure to accept claims that are within the statutorily allotted timely filing limits, and those timeframes and other considerations applicable to subrogated claims or coordination of benefits
17.5.1.6 The CCN shall not pay any claim submitted by a provider who is excluded from participation in Medicare, Medicaid, or CHIP program pursuant to Section 1128 or 1156 of the Social Security Act or is otherwise not in good standing with DHH.
Meets As part of our credentialing process, Aetna Better Health queries the listing of excluded individuals, pursuant to the requirements of section 1128 or 1156 of the Social Security Act, and sees that those providers treating members covered under the agreement between Aetna Better Health and the DHH, are in good standing with DHH prior to completing the contracting and credentialing process. At recredentialing, the procedures are followed to make certain good standing with DHH and lack of exclusion or restriction for participation in a Medicaid, Medicare or other government healthcare program. Aetna Better Health, through
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
63

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
its vendor PDS, also conducts queries of non-network providers, on a periodic and random basis, to supplement its existing query processes related to the contracted network.
17.5.2 Claims Dispute Management 17.5.2.1 The CCN shall have an internal claims dispute procedure that shall be submitted to DHH within thirty (30) days of the date the Contract is signed by the CCN, which will be reviewed and approved by DHH.
Meets
17.5.2.2 The CCN shall contract with independent reviewers to review disputed claims.
Meets
17.5.2.3 The CCN shall systematically capture the status and resolution of all claim disputes as well as all associated documentation.
Meets
Aetna Better Health’s Claims Administration Department employs full-time claims inquiry and Research Representatives to respond to provider questions, status inquiries and claims payment disputes via the claims inquiry line from 8:00 a.m. to 5:00 p.m., Monday through Friday. An automated telephone system allows callers to speak directly with a Representative or leave a detailed message regarding their inquiry. Whenever possible, the provider inquiry will be resolved while the provider is on the phone. If the provider’s inquiry cannot be resolved while the provider is on the phone and the provider’s inquiry requires additional research to reach resolution, then a call tracking case will be open for the provider’s issue. It is the department’s goal to research and respond to the provider’s issues within five to ten business days. When it is not possible to resolve the issue within this time frame, then the issue will be call tracked to the appropriate department, and thereafter followed by an independent reviewer. Claim disputes may escalate, at the request of the provider, to the Grievance and Appeals process. As such time, established Grievance and Appeals procedures are followed and applied to the provider’s claim dispute. Aetna Better Health acknowledges and will comply with the requirement to submit its specific claims dispute policies to the DHH within 30 days of contract award. Claim dispute data is captured by Aetna Better Health in its systems and further documented through the Grievance and Appeals process, as applicable.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
64

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
17.5.3 Claims Payment Accuracy Report 17.5.3.1 On a monthly basis, the CCN shall submit a claims payment accuracy percentage report to DHH. The report shall be based on an audit conducted by the CCN. The audit shall be conducted by an entity or staff independent of claims management as specified in this Section of the RFP, and shall utilize a randomly selected sample of all processed and paid claims upon initial submission in each month. A minimum sample consisting of two hundred (200) to two hundred-fifty (250) claims per year, based on financial stratification, shall be selected from the entire population of electronic and paper claims processed or paid upon initial submission.
Exceeds Aetna Better Health maintains a Claims Quality Review Team to monitor quality standards for all claims processes. Under the direction of the director of Operations Process and Knowledge Management (OPKM), Quality Review Analysts conduct random and focused reviews of processed claims for payment, financial and procedural accuracy and provider inquiry calls, which focus on both accuracy and customer service skills. Performance is measured against established department guidelines. Moreover, the Claims Quality Review Team fully audits the work of all new claims analysts for at least one month subsequent to their orientation and training. The audit starts at 100 percent of their work product and decreases to a standard two percent by the fifth week, provided the new claims analyst continues to meet claims accuracy standards. Finally, we review 16 provider calls per Claims Inquiry Representative per month, assessing the quality of service interaction and accuracy of information provided. Individual quality reports are presented to the Representative and their Supervisor for corrective action (e.g., live call monitoring) if appropriate. Quality Review Analysts conduct a series of pre-payment audits including: 1) A one percent random sample of system-adjudicated claims, 2) A two percent random sample of all analyst-adjudicated claims, 3) A daily random sample of billed claims up to $49,999.99, and 4) 100 percent of all claims with billed charges over $50,000. We will have one full time Auditor assigned and we will pull a total of 4 audits per month; two UB (facility) files and two 1500 (physician) files based on a two week paid date/check cycle. Our sample size is 95/2/2 (95% confidence; the error rate is
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
65

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
2%; with a desired precision of +/- 2%) which is an average of 180+ claims reviewed each week. Each file provides Aetna Better Health with Payment and Financial Accuracy findings for the period audited and each file is distributed for review and response to all applicable departments.
17.5.3.2 The minimum attributes to be tested for each claim selected shall include: ● Claim data correctly entered into the
claims processing system; ● Claim is associated with the correct
provider; ● Proper authorization was obtained for
the service; ● Member eligibility at processing date
correctly applied; ● Allowed payment amount agrees with
contracted rate; ● Duplicate payment of the same claim
has not occurred; ● Denial reason applied appropriately; ● Co-payment application considered and
applied, if applicable; ● Effect of modifier codes correctly
applied; and ● Proper coding.
Exceeds Post-payment audits review, at a minimum, include audit for the attributes listed in requirement 17.5.3.2., and also provide for review of: ● Coding, e.g. proper use of codes and modifier
codes; ● Member eligibility; ● Data entry into the systems is accurate; ● Timely Filing; ● Claim is associated with the correct treating
provider; ● Prior Authorization requirements; ● Denial reasons applied correctly; ● Benefit application (including limitations and
exclusions); ● Coordination of Benefits application; ● Claims history review for duplicate claim; ● Manual Pricing application; ● Contracted Provider and Special Provider
agreements, such as one-time case agreements and for both ensuring payment amount agrees with contracted rate;
● Modifier Discounts; and ● Claims bundling/unbundling. ● Contracted Provider and Special Provider
agreements, such as one-time case agreements and for both ensuring payment amount agrees
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
66

Part Two: Technical Proposal
Section Q: Claims Management
Requirement Meets or Exceeds
Requirement Explanation
with contracted rate; ● Modifier Discounts; and ● Claims bundling/unbundling
17.5.3.3 The results of testing at a minimum should be documented to include: ● Results for each attribute tested for each
claim selected; ● Amount of overpayment or
underpayment for each claim processed or paid in error;
● Explanation of the erroneous processing for each claim processed or paid in error;
● Determination if the error is the result of a keying error or the result of error in the configuration or table maintenance of the claims processing system; and
● Claims processed or paid in error have been corrected.
Exceeds Audit documentation comprises, at a minimum, documentation of findings by attribute, the amount of the associated under/overpayment, the root cause and resolution status. Audit files remain 'open' until all identified issues have been resolved and corrections/adjustments implemented accordingly.
17.5.3.4 If the CCN contracted for the provision of any covered services, and the CCN’s contractor is responsible for processing claims, then the CCN shall submit a claims payment accuracy percentage report for the claims processed by the contractor.
Exceeds Delegated vendors are required to match Aetna Better Health’s Claims auditing procedures. To monitor compliance with this contractual requirement, Aetna Better Health conducts a semi-annual and annual evaluation of delegated vendor claims auditing processes, and we will include a review of DHH specific audit requirements as part of our delegation oversight process.
17.5.5 Claims Summary Report 17.5.5.1 The CCN must submit quarterly, Claims Summary Reports to DHH by GSA and by claim type.
Meets Aetna Better Health acknowledges and will comply.
Response to RFP No. 305PUR-DHHRFP-CCN-P-MVA for Geographic Service Areas A, B and C Section Q – Requirement §17
67
Top Related