







Languages
Pages
Legal


1
Pediatric UrologyLuis Guerra, MD
University of Ottawa
Children’s Hospital of Eastern Ontario

2
Evaluation
Historically Urinalysis, IVP and cystoscopy
Recently US, CT, MRI, and endourology
Basic and most important approach starts with Complete history Thorough physical examination
Attention to genitourinary system

3
History Extremely important Always address the child Main complaint, past medical and family history
Antenatal history Prenatal US (hydro, bladder distention, oligohydramnios)
Delivery Uncomplicated, voided in the first 24 hrs, any metabolic unbalance
Urologic Age toilet trained Enuresis or daytime incontinence UTI Intestinal constipation Dysfunctional voiding pattern
Previous surgery Traumas

4
Physical General aspect
Syndromes, social and psycho-emotional behavior Abdomen
Palpation (bladder, kidneys, masses) Lower back
Skin dimples, hairy tufts, discolorations spots, gluteal cleft External genitals
Girls Vulva- Inflammations, labial adhesions, wetness
Boys Penis- Physiologic phimosis, hypospadias, chordee Testicles- Descended, size, texture, scrotal mass

5
Urinary infection in children

6
Urinary infection in children
What is UTI Bacterial infection in the urine May involve bladder and/or kidneys
Incidence: UTIs more common
First year of life Boys (peak at 6 months) >1 yr of life Girls (peak at 2-3 years)
During school age 1.2% of boys and 5% of girls develop UTI

7
Most common etiology
Organisms from bowel flora E. Coli (most common) Less often
Klebsiella, Proteus, Enterococcus, Staphylo saprophyticus
Ascending route is the MC

8
Pathogenesis
3% of girls and 1% of boys will get a prepubertal UTI (Winberg et al, 1974)
Of these, 17% will get infection-related renal scarring
Of those with scarring, 10% to 20% will become hypertensive, and a rare child will progress to renal failure

9
UTI – Clinical presentation
Kidney (pyelonephritis) Fever, abdominal or flank pain, vomit, diarrhea, child is ill
Bladder (cystitis) Dysuria, sp pain, frequency, urgency, incontinence and foul urine
Infants May be vague and without localization Fever 66%, irritability 55%, poor feeding 40%,
vomiting 35%, diarrhea 31%, abdominal distension 10%
10
UTI - Diagnosis
History – Symptoms
Physical There are no signs specific for UTI in the infant
An abdominal mass may be palpated (hydro, bladder,etc) Abdominal, flank, sp, CVA tenderness in older child Active, febrile, dehydrated, septic shock

11
Methods of urine collection
Bag specimen Even after skin cleaning usually reflects perineal and rectal flora It is reliable if: Significant pyuria, grow only 1 bacteria and
child is symptomatic May be useful to “rule out bacteriuria”
Suprapubic aspiration (most reliable but less used) Catheterization (if bag urine is not definitive) Toilet trained children: Midstream void Diagnosis of UTI
At least 10.000 and preferably >100.000 colony-forming units/ml

12
Reliability of urinalysis In a properly collected and processed urinary specimen, the
combination of: Positive leukocyte esterase, Positive nitrite testing, and Microscopic confirmation of bacteria
Has almost 100% sensitivity for detection of UTI
When all (or the leukocyte esterase and nitrite tests) are negative: The negative predictive value approaches 100%( Wiggelinkhuizen et al, 1988; Lohr et al, 1993)
Combination of these 3 tests helps, however the urinalysis cannot replace urinary culture

13
UTI - Radiological evaluation
Recommended in all children < 5 yrs of age All boys, irrespective of age All girls with pyelonephritis (fever) After a 2nd UTI in a girls older than 5 yrs of age
(Palmer, JS and Elder, JS 2003)

14
UTI - What kind of test?
Ultrasound Upper tract abnormalities (hydro, atrophic kidneys, cysts, renal
scarring, etc)
VCUG (voiding cystourethrogram) VUR and posterior urethral valve, assess bladder configuration
If both test are normal, no other evaluation is necessary
Renal scans For assess obstruction and renal function (DMSA, DTPA)

15
Vesicoureteric reflux
16
Vesicoureteric reflux
Wash back of urine to the kidneys (passive, active) Prevalence as high as 1 in 100 births 1:6 Male to female; present in 35-50% of children with UTI Boys are more likely to have high grades (IV and V) Causes
Primary (congenital short intramural tunnel) Normal tunnel length and ureteral orifice is 2.5:1
Secondary (high pressure – PUV, neurogenic bladder,etc) Importance of diagnosis of VUR
VUR + UTI can cause renal damage (scarring)

17
International classification VUR
International classification of vesicoureteral reflux. Copyright © 2003, Elsevier Science (USA)
18
VUR - Treatment
Antibiotic prophylaxis and follow up Follow up
Annual US and cystogram Spontaneous cure rate
20% per year Depends on the grade of VUR, unilateral vs bilateral
Surgery (open or endoscopic) in selected cases Breakthrough UTI (first year of life most likely to get scar) New onset or progressing of renal scarring Decreasing renal function Long follow up, parental preference

19
Treatment of an UTI: 10-14 days
Depends on age and severity of UTI
Septic (pyelonephritis) Neonates or young infants
Admission IV antibiotic (ampi or cephalosporin + genta) and then according to
bacteria sensitivity (change to oral when discharged) Older children oral therapy may suffice (same as for cystitis)
Clinically well (cystitis) Oral antibiotics
(sulfa-trimethoprim, nitrofurantoin, amoxicillin, ampicillin, cephalosporin) Adequate oral intake for hydration

20
Should not be used < 2 mo of age
Sulfa derivatives (Sulfamethoxasole) Displaces protein-bound bilirubin and may interfere with
bilirubin excretion, exacerbating neonatal physiologic jaundice
Nitrofurantoin May cause hemolytic anemia because of glutathione
instability in the erythorocyte

21
Management following a UTI
Adequate fluid intake Avoid intestinal constipation (fiber in the diet) Girls
Proper hygiene (swipe front to back) Void spreading the legs (avoid vaginal voiding and
incomplete voiding) Timed voiding (every 2 to 3 hours)

22
Who should have antibiotic prophylaxis? Patients with abnormalities of the GU tract
All VUR < 5 years of age Some risk factor for UTI (GU obstruction or urinary stasis)
Select cases of PUV, megaureters, hydronephrosis, etc
Patients with normal work-up More than 2 or 3 UTIs in 1 year
Usually sulfamethoxasole-trimethoprim, nitrofurantoin or trimethoprim alone
Little effect on stool’s bacterial flora Dose is 1/3 or 1/2 of the treatment dose
Routine C+S should not be done Amoxicillin or cephalosporine can affect the intestinal flora

23
UTI.., Who I should refer?
All daytime incontinence Diagnosed or suspected of GU abnormalities
VUR, hydronephrosis, megaureters, etc Neurogenic features
Abnormal lower back exam Established neurogenic entities
Sacral agenesis, imperforate anus, tethered cord, etc Known syndromes (VACTERL, 21 trisomy)
Child with recurrent UTIs after proper management of Intestinal constipation Adequate fluid ingestion Regular voiding (every 2-3 hours)
24
Scrotal mass in children

25
Scrotal mass in children Causal conditions
Inguino-scrotal hernia
True scrotal swelling Cystic/Soft
Epididymal cyst (spermatocele) Hydrocele Varicocele (MC on left side)
Solid Benign or malignant tumors (testis, spermatic cord and adnexas ) Testicular torsion / appendix torsion Incarcerated/ strangulated hernias
Trauma (hematocele, hematoma) Infectious (epididymitis)
26
Scrotal mass in children Acute
Testicular torsion Testicular/epidydimis appendix torsion Orchitis-epidydimitis Incarcerated / strangulated hernias Trauma Insect bits
Non-acute Hydrocele Hernia Testicular tumor Varicocele Cysts (epididymis, testis, spermatic cord)

27
Inguinal hernias in children
Persistence of the peritoneal vaginalis conduct
and insertion of abdominal contents into the inguinal canal
Presentation may be Non-acute (inguinal lump, bulging) Incarcerated or strangulated (pain, vomiting, tenderness)

28
Inguinal hernias in children
Treatment Elective surgery to prevent strangulation Urgent exploration if strangulated Dissection of the hernia sac up to internal ring and closure Repair of the posterior wall is generally not necessary in
children but adolescents may need it (or mesh)
29
Hydrocele - characteristics
Is an accumulation of fluid within the tunica vaginalis Usually communicating in children
All hydroceles in infants and children result from persistence of or delayed closure of the processus vaginalis
Present in 1-3% of all children
Greater in premature children
Males (85%)

30
Hydrocele - Anatomy

31
US - Hydrocele

32
Hydrocele - diagnosis Adequate history and physical examination are the hallmarks
of diagnosis
Assess the presence of Characteristic of scrotal swelling (soft or tense) Positive transillumination Inguinal bulge or incarceration (hernia) Important to feel a normal testis (US if necessary)
More frequent on the right and 10% is bilateral
Ultrasound is not usually necessary

33
Hydrocele - Management
Scrotal hydroceles common in newborn Usually resolve first year of life No evidence of testicular injury (even if tense)
Older child Secondary to minor trauma or inflammation
Observation is reasonable

34
Surgical management
Hernias Repaired when recognized Emergently if it is strangulated
Hydroceles Usually repaired after 18 months of age, electively

35
Acute scrotum

36
Testicular torsion

37
Testicular torsion (TT)
Most common in Neonates (extravaginal)
Peripubertal (intravaginal)
16-42% of boys with acute scrotum have TT
Extremely challenging condition One of the true Urologic Emergencies
Diagnostic tests are not entirely reliable
Must rule out in patient with acute scrotal pain/swelling
Diagnosis usually determined from history and physical
38
Testicular torsion - History
Can begins abruptly in early morning/during resting
Severe pain from onset
History of scrotal trauma is common Pain that persists >1 hr after minor trauma is not normal
Often previous episode/s of similar pain

39
TT – Physical exam
Scrotum/ position of testes
Cremasteric reflex - rarely intact in patients with TT
“Hard mass” or “swelling” Depending on how long the onset
Check for flank tenderness and bladder distension
Inguinal region for hernia/spermatic cord
Prehn’s sign Lack of pain relief with elevation suggests TT
Manual detorsion (controversy)

40
Bell clapper

41
Testicular torsion
Don’t delay proper treatment Most of the TT can be saved before 6 hrs of onset
Urinalysis – Not reliable to rule out
Color Doppler U/S: Operator dependant May not demonstrate flow in very young boys Reduced flow may indicate torsion
Gold standard diagnosis of TT – Surgical exploration

42
Doppler US - Arterial flow

43
True testicular torsion

44
Testicular/epididymal appendix
Wolfian duct remnant
Mullerian duct remnant

45
Testicular appendix torsion

46
Testicular appendix torsion Clinical presentation
Usually less severe pain and swelling Upper pole “blue dot” However, it may be mimic TT
Management Reassurance Relative rest Analgesic (acetaminophen, codeine) It takes 1-2 weeks to improve Return to ER if any change in symptoms/findings

47
Testicular tumors

48
(paratesticular rhabdomyosarcoma)

49
Testicular tumors
Uncommon disease 0.5-2 / 100.000 children 1% to 2% of all pediatric solid tumors Incidence of childhood testicular tumors
Peaks at age 2 years Tapers after age 4 years Rises again at puberty
Germ cell tumors account for 65% of prepubertal tus Rare among black and Asian children

50
Diagnosis
Painless firm testicular mass is the MC presentation of a child with a testicular tumor
Negative transillumination Disorders that must be excluded:
Epididymitis Hydrocele Hernia Spermatic cord torsion

51
Investigation US testis Alpha-fetoprotein
High in 90% of Yolk sac tumor Single polypeptide chain amino acid produced by the fetal yolk
sac, liver, and gastrointestinal tract Half-life: 5 days (25-30 days)
β-hCG Made by syncytiotrophoblast Is rarely increased in preadolescent tumors Half-life: 24 hrs (5-7 days)
Serum LDH (lactate dehydrogenase) Chest x-ray and abdominal CT
Retroperitoneal lymph nodes are the 1st site of meta Lung (MC distant site of meta)

52
MC types in children Yolk sac tumor
Most common type in childhood - 60% Mostly in < 2 years of age Persistent AFP elevation post orchiectomy suggests mets
Teratoma Usually benign in children Second most common in childhood (21%) Mean age: 18 months US usually contain complex cysts Germ cell tumor with more than one germ cell layer
Endoderm, ectoderm, and mesoderm Cartilage, bone, mucous glands or muscle
53
Testicular tumor - Treatment
Initial treatment is radical inguinal orchiectomy Stage I disease do not receive additional adjuvant Routine RPLND and/or adjuvant chemotherapy is not
indicated (only if metastasis)
Partial orchiectomy in selected cases Teratoma: No report of metastases in prepubertal males

54
Timely surgery

55
Testicular mass…Who and when I should refer?
All cases of testicular mass should be referred as soon as diagnosed
Even before US is obtained In testicular cancer, time matters

56
Abdominal mass in children

57
Abdominal mass in neonates
Abdominal mass (75% arise in the GU tract) 1-Hydronephrosis is the MC (UPJO, VUR, UVJO, PUV) 2-Multicystic dysplastic kidney (MCDK) 3-Tumors account for 12 %
MC abdominal tumors: Neuroblasoma, congenital mesoblastic nephroma and teratoma (sacrococcygeal)
Hydronephrosis MCDK

58
Abdominal mass in neonates
Neuroblastoma is the MC malignance in neonate
Wilms tumor is extremely rare
Abdominal mass + hematuria: renal vein thrombosis
Girl with abd mass + interlabial bulging: hydrocolpos
CMN is the MC renal tumor

59
Abdominal mass after neonatal period
From 1 month to 1 year of age Hydronephrosis – 40% Solid masses and tumor – 40%
Older than 1 year Tumor is the MC cause of abdominal mass

60
Neuroblastoma Wilms Tumor (Nephroblastoma)

61
Neuroblastoma (NB)
MC malignant tumor of infancy 8% to 10% of all childhood cancers Annual incidence 10 cases per 1 million Median age at diagnosis: 22 mo 50% of cases < 2 years of age (75% <4yrs)
(Fortner et al, 1968)

62
NB- What and Where?
Tumor of the neural crest cell origin Cells that form the adrenal medulla and sympathetic ganglia
75% are retroperitoneal 50% adrenal 25% sympathetic chain (from neck to pelvis)

63
NB - Presentation
Often has systemic symptoms (different from WT) Fever, abdominal pain or distension, abd mass,
weight loss, anemia, bone pain, proptosis and periorbital ecchymoses (retro-orbital metastasis)
Metastases are present in 70% at diagnosis
VMA (vanilmandelic acid), HMA (homovanillic acid) Are elevated in > 90% of the neuroblastomas 24 hs urine collection (catecholamine metabolites)

64
NB - Imaging
US is usually the first exam in child with abdominal mass
CT or MRI Both detect extension beyond midline and hepatic
involvement MRI: better displays the relationship with great
vessels and detects intraspinal extension (tumor of sympathetic chain)
CT may show calcifications (rare in Wilms tumor)

65
NB - Treatment Generally based on risk assessment
Tumor stage Grade Biochemical risk factors Genetic risk factors
Low-stage favorable Sx alone
Higher risk tumor Adj chemo +/- Rt
Very aggressive tumor Autologous bone marrow
transplantation

66
Wilms’ tumor (Nephroblastoma)

67
Wilms' Tumor
MC primary malignant renal tumor of childhood Embryonal tu develops from remnants of immature
kidney Annual incidence 7 to 10 cases per million Median age 3.5 yrs 80% diagnosed < 5 yrs of age Worldwide sex ratio is close to 1
(North America girls slightly > boys)

68
Congenital anomalies and WT
Genitourinary anomalies in 4.5% of WT Renal fusion anomalies Cryptorchidism Hypospadias
(Breslow et al, 1993) These are common disorders and screening for WT
is not necessary in most children with genital anomalies

69
Syndromes associated with WT Without overgrowth
Denys-Drash syndrome (DDS) Male pseudohermaphroditism, renal mesangial sclerosis and WT
( Drash et al, 1970)
Aniridia (Found in 1.1% of patients with WT) WAGR syndrome
(W ilms' tumor, a niridia, g enital anomalies, mental r etardation(Clericuzio , 1993)
Horseshoe kidney (NWTSG found 7 times incidence of WT)
With overgrowth Hemihypertrophy, which may occur alone or with syndromes Beckwith-Wiedemann (BWS), Perlman, Soto, Simpson-Golabi-
Behmel ( Perlman et al, 1975; Neri et al, 1998)

70
Imaging in WT
Ultrasound is the first study performed in most children with an abdominal mass. (solid nature of the lesion)
CT shows the relationship with other organs
MRI is the study of choice if extension of tumor into the inferior vena cava cannot be excluded by ultrasound (Weese et al, 1991)

71
Treatment of WT
Surgical Radical nephrectomy Accurate staging for determination need Rt +/- chemo Exploration of the abdominal cavity
Liver and nodal metastases and peritoneal seeding Formal exploration of the contralateral kidney
Should be performed before nephrectomy Formal retroperitoneal lymph node dissection
Is not recommended

72
Urinary incontinence - Definitions

73
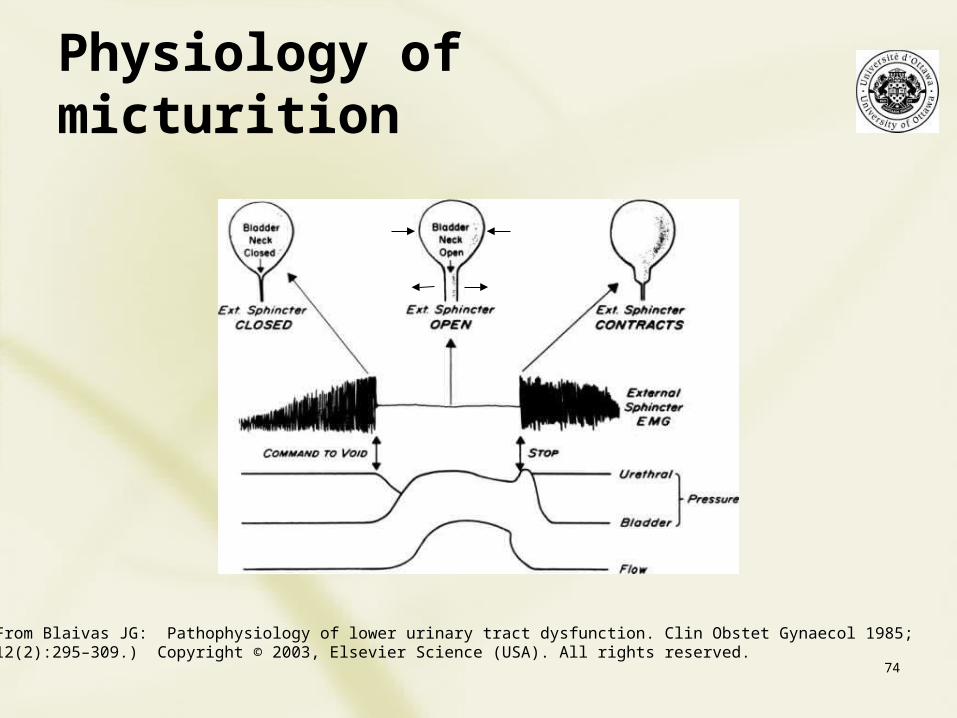
Urinary incontinence Normal voiding
Activation of the micturition reflex
The micturiction reflex Under voluntary control Coordinated by the pontine micturiction center
Two neurological systems involved Sympathetic system (relaxes detrusor and closes internal sphincter) Parasympathetic system (detrusor contraction) Somatic – Pudendal nerve (external urethral sphincter)
Continence Learned behavior
74
Physiology of micturition
From Blaivas JG: Pathophysiology of lower urinary tract dysfunction. Clin Obstet Gynaecol 1985;12(2):295–309.) Copyright © 2003, Elsevier Science (USA). All rights reserved.

75
Transition from childhood to adult pattern of urine control
Many children transiently presents Voiding disturbances or Urinary incontinence that suggest dysfunction But they are simply a normal transition phase
They are in fact a process of bladder function maturation and self limited
76
What is urinary incontinence? Is the involuntary loss of urine
A careful history may determine the cause
Four main categories Continuous Stress Urgency Overflow
77
Nocturnal enuresis

78
Enuresis, Is it a…night or daytime problem?
Nocturnal enuresis Involuntary loss of urine during sleep
Neurological maturation and improve over time
Daytime incontinence Involuntary loss of urine during the day (awake) Need to rule out
Neurological causes Dysfunctional elimination syndrome Other causes (anatomical GU abnormalities)

79
Nocturnal enuresis 15 % at 5 yrs and 1% at 15 yrs of age
It is considered normal until 6 years of age
Often children > 6 yrs should be investigated Exam of lower back
Skin dimple, hairy tufts, discolorations Ultrasound Urinalysis and urine culture
Vast majority these tests will be normal

80
Nocturnal enuresis Number of theories tried to explain the cause
Behavioral, genetic, developmental, neurologic, psychological, urodynamic, and organic causes
There is no single explanation for this symptom
Multiple factors may be involved
Neurological maturation theory is the MC accepted
MNE is a symptom rather than a disease
81
Urodynamics in MNE
Not indicated
Research studies Urodynamics don’t show increased bladder instability Involuntary contractions are not the cause MNE
Therapy aiming at eliminating uninhibited
contractions is generally ineffective (anticholinergic)

82
Vasopressin levels
In normal children Increased production of vasopressin at night 50% less urine is normally excreted at night
Theory
Vasopressin deficiency is the cause for NE Controversy, contradictory studies
However, many children with MNE have similar levels of vasopressin during both the day and the night

83
Hereditary Factors
Likelihood of MNE 77% if it occurred in both parents 43% if 1 parent had NE 15% if neither parent had NE
Twin studies Monozygotic 65-70% Dizygotyic 31-44 %

84
Evaluation Sufficient evaluation for most children with primary MNE
A carefully history Physical examination Urinalysis
Check for a history of Urinary infection Diurnal incontinence Obstructive GU symptoms or signs of neuropathy
In their absence of above risk factors There is generally no indication for radiographic studies or cystoscopy The incidence of associated uropathology is low
However, some authors recommend U/S in children older than 6 yrs

85
Treatment - Enuresis
Controversy Some authors recommend treatment in children after the
age of 5-6 years of age Others wait to treat until the child seems bothered by the
problem Treatment should be individualized

86
Pharmacologic Therapy
Anticholinergic therapy has low effectiveness ranging from only 5% to 40% (Person-Junemann et al, 1993; Kosar et al, 1999)
Imipramine (tricyclic antidepressant) Increases functional bladder capacity Good result in 40% to 50% of cases However, discontinuation causes relapse in up to 60%

87
DDAVP - Desmopressin
Rationale - Reduction of urine output at night Some enuretics have reduced nocturnal vasopressin
concentrations and have nocturnal polyuria (Norgaard et al, 1989c)
The therapeutic effect of DDAVP is temporary
50% to 90% of children relapse after stop treatment(Kahan et al, 1998)

88
Behavior Modification
Should be considered the first-line approach Bladder training (increase bladder capacity) Responsibility reinforcement Classic conditioning therapy with a urinary alarm
Varied success rate (40-60%)
Most effective and reproducible rate of cure

89
Daytime Incontinence

90
Daytime incontinence MC causes of daytime incontinence in children
Dysfunctional voiding Neurological conditions Rarely – Obstructive (PUV or urethral stenosis), fistulas, sphincteric
incontinence, etc
Daytime wetting is of more concern than nocturnal enuresis May be caused by an organic problem
Complete physical Lower back, palpable bladder, neurogenic conditions Girls: Vulvo-vaginitis, labial adhesion (vaginal voiding),
ectopic ureter Boys: Urethral meatal stenosis, fistulas

91
Daytime incontinence,Non-neurological cause Dysfunctional voiding is the MC cause Part of a “behavioral elimination syndrome”
Intestinal constipation Holding urine for too long Abnormal spastic pelvic floor
Voiding and stoolling calendars (3 days record)
Other causes Ectopic ureter, urethral stenosis (overflow), external sphincter
insufficiency, vaginal or rectal fistulas
92
Daytime incontinence,Neurologic causes Tethering of the spinal cord (TC) is the MC cause
Occult spinal dysraphism (primary TC) Stigmata (skin dimple, discoloration, hairy tufts, gluteal
asymmetry) Open spina bifida (secondary TC)
Lipomyelomeningocele, dermal sinus tract, split cord malformations, syringomyelia, etc
Post-operative (myelomeningocele repair)
Other neurological causes Down syndrome, sacral agenesis, VACTERL complex,
imperforate anus, cloacal anomalies, etc

93
Evaluation if Neurogenic cause is suspected
Urodynamics US kidneys and bladder MRI of the spinal cord EMG of the legs and perineum Complete neurological assessment (neurosurgeon)

94
Tx of daytime incontinence
Dysfunctional voiding Increase fluid and fiber in the diet Prompt to void every 2-3 hours Maintain soft and non-painful BM
Stool softener if necessary
Neurogenic According the underlying cause Release of tethered cord Anticholinergic, Clean intermittent bladder catheterizations Bladder augmentation

95
Who I should refer?
All cases of daytime incontinence should be referred to urological assessment
Top Related