





Languages
Pages
Legal


Στοματική κοιλότητα και IBD
Κωνσταντίνος Χ. Κατσάνος
Ιωάννινα, Ιούνιος 2016

Στοματική κοιλότητα και IBD
• ΚΑΛΟΗΘΕΙΣ ΕΚΔΗΛΩΣΕΙΣ
• ΠΡΟ-ΝΕΟΠΛΑΣΜΑΤΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ
• ΝΕΟΠΛΑΣΜΑΤΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ

ΚΑΛΟΗΘΕΙΣ ΕΚΔΗΛΩΣΕΙΣ

• A significant proportion of patients may have one or more manifestations in the oral cavity and in the perioral skin area.
• The prevalence of oral lesions in IBD has been reported to range from 5-50%.
• oral lesions are more common in CD as compared to UC
• more prevalent in children as compared to adults.
ΙBD & ΣΤΟΜΑΤΚΗ ΚΟΙΛΟΤΗΤΑ

• Oral manifestations may be associated with • the disease itself • with nutritional deficiencies • with complications from therapy.
• may precede IBD diagnosis • may or not be associated with active disease • may involve any part of the oral cavity
• They may cause significant symptoms and disability
ΙBD & ΣΤΟΜΑΤΚΗ ΚΟΙΛΟΤΗΤΑ

• two common clinical scenarios:
• 1) oral lesions associated with altered bowel habits
• 2) established IBD but complaining of new oral lesions.
ΙBD & ΣΤΟΜΑΤΚΗ ΚΟΙΛΟΤΗΤΑ

Oral lesions in CD
• Oral lesions have a prevalence rate between 20-50%.
• higher in proximal gastrointestinal tract and/or perianal involvement.
• Aphthous ulcers, the most common
• preceding GI symptoms in 5%-10% of patients.
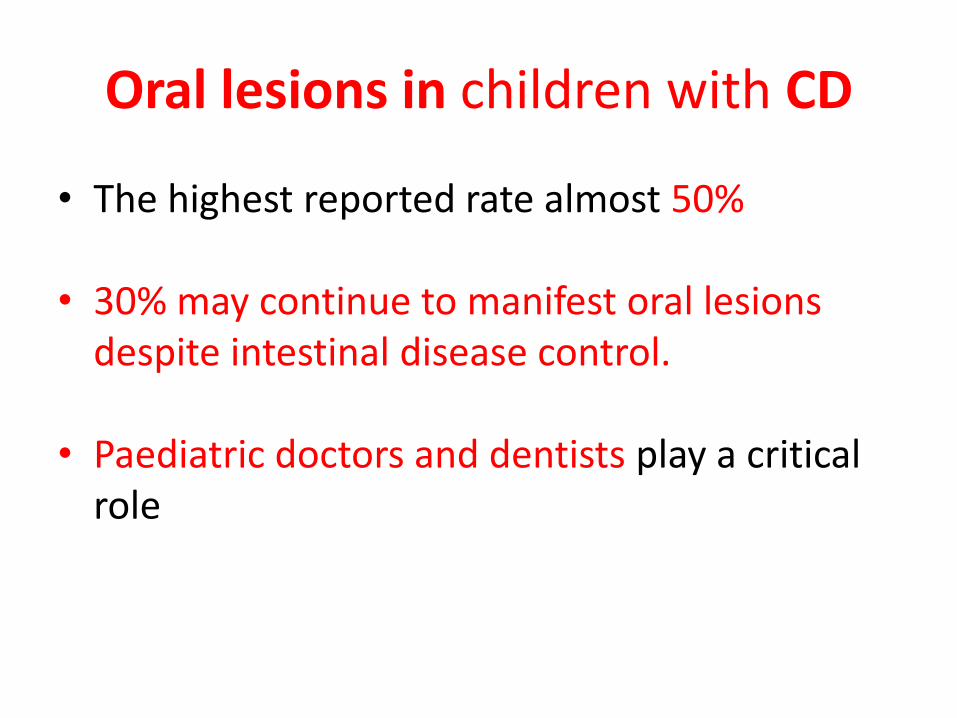
Oral lesions in children with CD
• The highest reported rate almost 50%
• 30% may continue to manifest oral lesions despite intestinal disease control.
• Paediatric doctors and dentists play a critical role

Oral manifestations in UC
• Aphthous ulcers in 10% of UC.
• in pediatric patients with UC in up one third and are usually non-specific.

DIAGNOSIS OF ORAL LESIONS IN IBD
• Oral lesions in IBD can be
• specific
• non-specific

1.Specific oral changes or lesions Description
Orofacial Crohn’s disease Granular cheilitis
Pyostomatitis vegetans
Mostly young patients with Crohn’s
Mostly in Crohn’s disease
In ulcerative colitis and in Crohn’s
2. Non-specific oral changes or lesions
-Oral cavity changes Ulcers, cobblestonning, swelling, abscesses, tags, tongue changes, gingival changes etc.
-Lip changes cheilitis, swelling, redness, scaling, fissures, ulcers
-Malabsorption-related oral changes or lesions
Folic acid deficiency Glossitis and/or cheilitis
Iron deficiency Glossitis and/or cheilitis
Zinc deficiency Oral candidiasis, glossitis
Vitamin A deficiency Oral white patches/keratinization
Vitamin B complex deficiency Stomatitis, glossitis, angular cheilitis, burning mouth syndrome, reduced or altered taste
Vitamin C deficiency Scurvy
Vitamin K deficiency Gum and/or oral cavity bleeding
-Medication-related oral changes or lesions
Adalimumab Infections, angioedema, paradoxical reactions
Azathioprine Sicca syndrome
Budesonide Glossitis, dry mouth
Certolizumab pegol Angioedema, Stevens-Jonhson syndrome/toxic epidermal necrolyis, paradoxical reactions
Cholestyramine Glossitis, altered taste,dental changes, gum bleeding
Cyclosporin Gingivitis, gum hyperplasia
Ciprofloxacin Angioedema,Stevens-Jonhson syndrome/ Toxic epidermal necrolyis, oral candidiasis, loss of taste
Infliximab Infections, angioedema, paradoxical reactions
Loperamide Angioedema, Stevens-Jonhson syndrome/ toxic epidermal necrolyis, dry mouth
Mesalazine Stomatitis, dry mouth, altered taste
Methotrexate Stomatitis, gingivitis
Metronidazole Metallic taste, glossitis, stomatitis, candidiasis, dry mouth
(Methyl)prednisolone Oral candidiasis
Mycophenolate mofetil Sicca syndrome
Sulphasalazine Angioedema, stomatitis, Stevens-Jonhson syndrome/toxic epidermal necrolyis, altered taste
Table Specific and non-specific oral changes in patients with IBD.

Oral involvement in IBD Clinical Signs
Orofacial Crohn disease One or more clinical signs of spectrum: perioral erythema, metastatic Crohn’s of skin of the face with ulcers, facial swelling,
mucosal tags, deep linear ulcers, cobblestoning, lip swelling or fissuring, granulomatous cheilitis, mucogingivitis, papules,
nodules, plaques or persistent swelling.
Oral mucosa
[masticatory or lining
(labial / buccal)]
abscesses (mostly in buccal space)
aphthous lesions (minor or major)
aphthous stomatitis
circumferential ulcers
cobblestoning, cobblestone plaques
diffuse oral edema
fissures
IgA pustulosis, leukoplakia, hairy leukoplakia
linear ulcers ,lumps
mucosal tags ,permanent maloformartions / scarring
pseudopolyps
polypoid lesions,pyostomatitis vegetans
swelling and induration
Lip(s) angular cheilitis
fissuring, induration
granulomatous cheilitis ,macrocheilia with or without fissuring
neoformations of the genian mucosa (papilloma,fibroma) ,swelling
Gingiva non specific gingivitis
hyperplastic granular gingivitis
Hard palate palatal ulcer(s)
Teeth parodontal lesions
paraodontosis
reduction of the alveolar bony tissue
Tongue erosions
glossitis
ulcers
Tonsills granulomatous tonsillitis
tonsillar granulomas
Salivary glands Fistula,granulomatous inflammation,
minor salivary gland enlargement reduced salivation
sicca syndrome
Table Clinical signs of oral involvement in IBD by oral anatomic location.

Dental symptoms Discomfort, pain, infections, dental caries, decay,
periodontal involvement
Oral symptoms dry mouth (sicca syndrome), reduced salivation,difficulty
in speaking and/or swallowing, halitosis
Gingiva gingival hypertrophy, swelling, pain, bleeding
Lip changes swelling, macrocheilia, redness, scaling, fissures
Oral mucosa changes ulcer(s), cobblestoning, polypoid tags, buccal swelling,
leukoplakia, mucosal discoloration
Perioral skin changes perioral erythema with scaling, erythema migrans,
swelling, malformations, scarring
Lymphadenopathy persistent submandibular lymphadenopathy
Tongue changes painful tongue, glossitis in top or lateral or whole tongue,
hairy tongue, metallic dysgeusia
Table Oral symptoms in patients with inflammatory bowel disease.

Oral aphthous or ulcerous or edematous lesions Oral granulomatous lesions
Recurrent aphthous stomatitis (RAS) Orofacial granulomatosis (OFG)
Autoimmune rheumatic diseases
(Reiter's syndrome, systemic lupus erythematosus,
Adamandiadis-Behcet's syndrome)
Melkersson-Rosenthal syndrome
Autoimmune bullous diseases, cicatricial pemphigoid,
pemphigus vulgaris, epidermolysis bullosa acquisita
Cheilitis granulomatosa
(Miescher cheilitis)
Infections
(mucobacterial, systemic fungal infections, parasites,
sexually transmitted infections, herpetic gingivostomatitis,
CMV, Coxsackie, oral histoplasmosis) Oral
staphylococcal (S. aureus) mucositis
Foreign body reaction-sarcoid-like
(Polishing-paste-induced silica granuloma,
delayed hypersensitivity to cobalt, oral cavity
piercing)
Lymphatic edema, lymphangioma, vascular edema, Sarcoidosis
Neutropenias Sjögren syndrome
Desquamative gingivitis Wegener’s granulomatosis
Precancerous lesions (lichen planus) Tuberculosis
Cancer (mouth T-cell lymphoma)
Traumas and Allergies
Tuberculoid leprosy
Table Differential diagnosis of oral aphthous and oral granulomatous lesions in patients with inflammatory bowel disease.

Non-specific oral lesions
In IBD and non-IBD patients
-Malabsorption related
-Medication related
-Other
Highly specific
-“Metastatic”
-Orofacial
-Granulomatous
cheilitis
Highly specific
-pyostomatitis
vegetans
Highly suspicious
-Tag-like lesions
-Cobblestoning
-Mucogingivitis
-Lip swelling &
vertical fissuring
-Deep linear oral
ulcers (buccal sulci)
Spectrum of oral manifestations and lesions in inflammatory bowel disease
Crohn’s disease
Ulcerative colitis

a. Highly specific oral lesions
• Highly specific oral lesions are almost pathognomonic for IBD diagnosis
• orofacial and granulomatous cheilitis in CD
• pyostomatitis vegetans in UC and CD

Orofacial Crohn’s disease
• oral ulcers and cobblestoning appearance in the mouth of patients with CD
• “CD of the mouth”.
• Orofacial CD is a specific manifestation of CD (5-15% )
• relapsing aphthous ulceration with coexisting edema of the oral
cavity and of the lips
• Usually the bowel disease develops within a few months of the orofacial condition, but delays of up to nine years have also been reported.




Orofacial Crohn’s disease
• Orofacial CD is clinically and histologically indistinguishable from orofacial granulomatosis (OFG), which occurs in the absence of any bowel disease.
• OFG encompasses two conditions:
• Granulomatous cheilitis (or Miescher cheilitis or cheilitis granulomatosa)
• Melkersson-Rosenthal syndrome



Granulomatous cheilitis
Melkerson-Rosenthal syndrome Orofacial
Crohn’s
(preceeding
bowel
symptoms) Other causes (i.e sarcoidosis, allergy)
Orofacial
Crohn’s
(extraintestinal
manifestation)
Orofacial granulomatosis
Absence of bowel disease Bowel disease

Granulomatous cheilitis
• Granulomatous cheilitis (or cheilitis granulomatosa or Miescher cheilitis)
• Changes are restricted to the lip, mostly focal granulomatous inflammation of the lower lip.


Pyostomatitis vegetans
• Pyostomatitis vegetans (PV) is a rare condition characterized by erythematous and thickened oral mucosa with multiple pustules and superficial erosions.
• PV is associated with IBD in 75% of cases
• Other differential diagnoses include autoimmune
pemphigoid diseases and sometimes infections. •

b. Highly suspicious oral lesions for IBD
• are highly suggestive of underlying IBD, especially CD
• The most common affected portions are the buccal mucosa, gingiva, lips


c. Non-specific lesions in IBD
Recurrent aphthous stomatitis
• Any patient with recurring or insisting oral ulcers should be evaluated medically for the possible presence of a more serious systemic disease.
• Aphthous-like lesions may be seen in 4-5% of patients with IBD.
• Colonic, rather than small intestinal, CD is more often associated with oral
• The list of differential diagnosis is long

Salivary duct and saliva in IBD
• Patients with IBD may complain of dry mouth, similar to the sicca syndrome observed in transplanted patients under immunosuppressive therapy.
• Granulomatous inflammation of minor salivary gland ducts has been suggested as another oral manifestation of active intestinal CD.

Tongue involvement in IBD
• Rare cases of non-neoplastic tongue involvement in IBD have been described
• Alterations of taste (metallic dysgeusia) may be related with
• disease activity,
• nutritional habits
• therapy with metronidazole.
Dental and gingival manifestations in IBD
• dental infections and dental alterations related to malabsorption and to disease activity of IBD.
• Gingival involvement in CD is infrequent.
• Gingival biopsy may be helpful for early diagnosis of an underlying CD.

Oral lesions secondary to nutritional deficiencies
• Nutritional deficiencies may cause oral lesions, the most common being angular cheilitis associated with iron deficiency.
• deficiencies in iron, folic acid, vitamin B12, potassium, calcium, magnesium, vitamin A, vitamin C, vitamin D, zinc and selenium.

Therapy-related oral lesions
• All medications may cause oral lesions or symptoms
• Oral paradoxical reactions to biologicals include oral lichenoid reaction to infliximab and new onset of oral lichen planus during certolizumab pegol use.

MEDICAL TREATMENT OF ORAL MANIFESTATIONS IN IBD
• topical and/or systemic therapies combined
with dietary instructions
• In refractory or intractable cases the algorithms of management may also include surgical treatment

Medical treatment of oral IBD Surgical treatment of oral IBD
Effective treatment of intestinal IBD
Standard treatment (reported)
-Corticosteroids (methlyprednisolone)
-Azathioprine
-Infliximab
-Thalidomide (refractory cases)
-isotretinoin, dapsone (pyostomatitis)
-Long-term p.os antibiotics (tetracycline, erythromycin, penicillin,
metronidazole)
Other possible options (unreported)
-Methotrexate
-Adalimumab
-Certolizumab
Nutrition
-Total enteral nutrition (selected cases)
-Elemental diet (selected cases)
-Elimination diets (special dietary restrictions i.e cinnamate- and benzoate-
free diet)
-Supplementation formulas, vitamins (A,B,C) and trace elements (zinc)
Major surgery
Oral and oropharyngeal surgery
-Oral surgery
-Orthognathic surgery
-Maxillofacial surgery
Plastic facial and lip surgery
-Reconstructive
-Elimination
Colectomy in intractable oral IBD
Minimal or Elective surgery
-small lesion removal
-small fistula repair
-abcess drainage
- oral biopsies (multiple)
Topical treatement
Local intralesional injections
-corticosteroids
- triamcinolone 0.1%
-Infliximab
-analgesics
-lidocaine 2%,
Local ointments
-corticosteroids(1% hydrocortisone)
-tacrolimus
-non-steroidal anti-inflammatory pastes
Mouthwash
-5-aminosalicylic,-corticosteroids,-antiseptic,Elixirs (dexamethasone)
Local dental surgery
(functional repair and cosmetic)
-Dental surgery
-Biopsy of small oral lesion
-Laser for gingival Crohn's disease
Table Treatment of the oral manifestations in inflammatory bowel diseases.

Treatments of oral IBD Type of oral IBD Author/Year Number
of all
patients
Type of trial
(controlled/C
Uncontrolled/U)
Response rates
Oral Crohn’s Plauth et al,30 1991 12 Topical steroids/ U 7 of 12 (58%) patients
Oral Crohn’s Casson et al,142
2000
3 Topical tacrolimus ointment /U Marked improvement in 1-6 months
Orofacial
franulomatosis/ora
l Crohn’s
Mignogna et al,139
2004
7 Triamcinolone injections
/ U
Response (2 or 3 injection
sessions over 14 or 21
days)
Oral Crohn’s Plauth et al,30 1991 26 Azathioprine and/or systemic
steroids / U
13 of 26 (50%) patients
Oral Crohn’s Williams J et al,145
1991
12 Systemic steroids / U Improvement in all, 3
steroid-dependent
Oral Crohn’s Litsas140 ,
2011
1 Systemic prednisone / U Response after 6 months
Resistant oral
Crohn’s
Hegarty et al,153
2003
5 Thalidomide/ U Response
Oral Crohn’s Campbell et al,163
2013
10 Phenolic acid exclusion diet
with micronutrient
supplementation/ U
7 responded
Oral Crohn’s White et al,161 2006 32 Elimination diets
cinnamon- and benzoate-free
diet (CB-free diet) / U
Response after 8 weeks
Oral Crohn’s Cameron et al,159
2003
1 Elemental diet/ U Response but 2 relapses
Granulomatous
cheilitis
Kano et al,70 1992 1 Metronidazole / U Response
Oral Crohn’s Sánchez et al,147 2005
1 Adalimumab+dapsone/ U Response after 5 months
Oral Crohn’s Cardoso et al,149
2006
1 Infliximab/ U Successful treatment
Fistulizing oral
Crohn’s
Staines et al,151
2007
1 Infliximab/ U Successful treatment

Management of oral aphthous ulcers in IBD
(Target in parallel bowel disease remission)
Topical treatment Antibiotics, tacrolimus ointment, corticosteroids (elixirs, ointments, mouthwashes, intralesional injections), analgesics (lidocaine 2%), antiseptic mouthwashes, NSAID pastes
Elimination diets (Cinnamon, benzoate, glutaminate, cocoa) Vitamin and trace element supplementation
Systemic treatment Corticosteroids, azathioprine, methotrexate, tacrolimus
Systemic treatment for refractory cases
Biological therapy, thalidomide, long-term antibiotics
Figure . Algorithm for management for oral aphthous ulcers in IBD.

Management of oral Crohn’s disease
(Target in parallel bowel disease remission)
Topical treatment Antibiotics, tacrolimus ointment, corticosteroids (elixirs, ointments, mouthwashes, intralesional injections), analgesics (lidocaine 2%), antiseptic mouthwashes, NSAID pastes
Food restriction, Enteral / Parenteral nutrition
Elimination diets (Cinnamon, benzoate, glutaminate, cocoa) Vitamin and trace element supplementation
Surgical treatment Head-neck surgery, oral surgery (for local repair and cosmesis) Dental surgery
Systemic treatment Corticosteroids, azathioprine, methotrexate, tacrolimus, biological therapies
Systemic treatment for refractory cases
Switch to a 2nd biological therapy, thalidomide, long-term antibiotics, dapsone, Cyclosporin A (for pyostomatitis)
Figure. Algorithm for recommended management for oral Crohn’s disease.

SURGICAL TREATMENT OF ORAL MANIFESTATIONS IN IBD
• for severe complications refractory to medical therapy. • Minimal or elective surgery • Local dental surgery
• Major surgical interventions include
• oral and oropharyngeal surgery, (orthognathic and/or maxillofacial
surgery) • plastic surgery (reconstructive, elimination i.e for hyperplastic
gingiva). • Colectomy is reserved as an ultimate option for patients with UC
and intractable or highly resistant oral lesions that significantly affect oral feeding and overall quality of life.


ΠΡΟ-ΝΕΟΠΛΑΣΜΑΤΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ

Environmental factors Sun exposure (UV light), passive smoking(?)
Infections (HPV E6 and E7 oncogenes, HIV, syphilis DNA detected from CMV and EBV in oral cancerous lesions, chronic candidiasis)
Life style (smoking , smokeless tobacco use, pipe smoking, marijuana use, heavy alcohol use, access to medical care or dental care, low consumption of fruits and vegetables)
Drugs (immunosuppressants, anti-TNFa ?, others?)
Alterations in oral homeostasis (xerostomia, reduced salivary flow, candida colonization)
Demographics
(age>40, males, African-American (oral cavity cancer), fair skin (lip cancer)
Education level (Absence of oral screening, no annual oral exam, poor oral hygiene)
Precancerous oral lesions unrecognized and untreated
(leukoplakia, erythroplakia, leukoerythroplakia, chronic candidiasis (?)
Chronic irritation in oral cavity
(traumatic ulcers, poor fitting denture, broken or sharp-edged teeth or fillings)
Underlying conditions (immunodeficiency, transplantation, Plummer-Vinson)
Nutrition deficiencies (low vitamin A, B12, folic acid levels, iron deficiency)
p53 gene alterations-dysplasia-cancer in situ-invasive cancer
Figure. The puzzle of mechanisms and conditions leading to the development of oral precancerous lesions
and oral cancer in inflammatory bowel diseases.

Author Drug Patient Disease Type of
oral lesion
Outcome
Mocciaro et al.54 Certolizumab
pegol
1 Crohn’s Oral lichen
planus
Non evolution
to Ca
Fluckiger et al.55 Azathioprine 1 Ulcerative
colitis
Oral hairy
leukoplakia
Non evolution
to Ca, HIV(-)
Worsnop et al.52 Infliximab 1 Crohn’s Oral lichen
planus
(probable)
Non evolution
to Ca
(Paradoxical
reaction to IFX)
Moss et al.53 Infliximab 1 Crohn’s Oral
lichenoid
reaction to
IFX
Non evolution
to Ca
(Paradoxical
reaction to IFX)
Table. Oral precancerous lesions reported in the form of case reports in patients with inflammatory bowel disease.


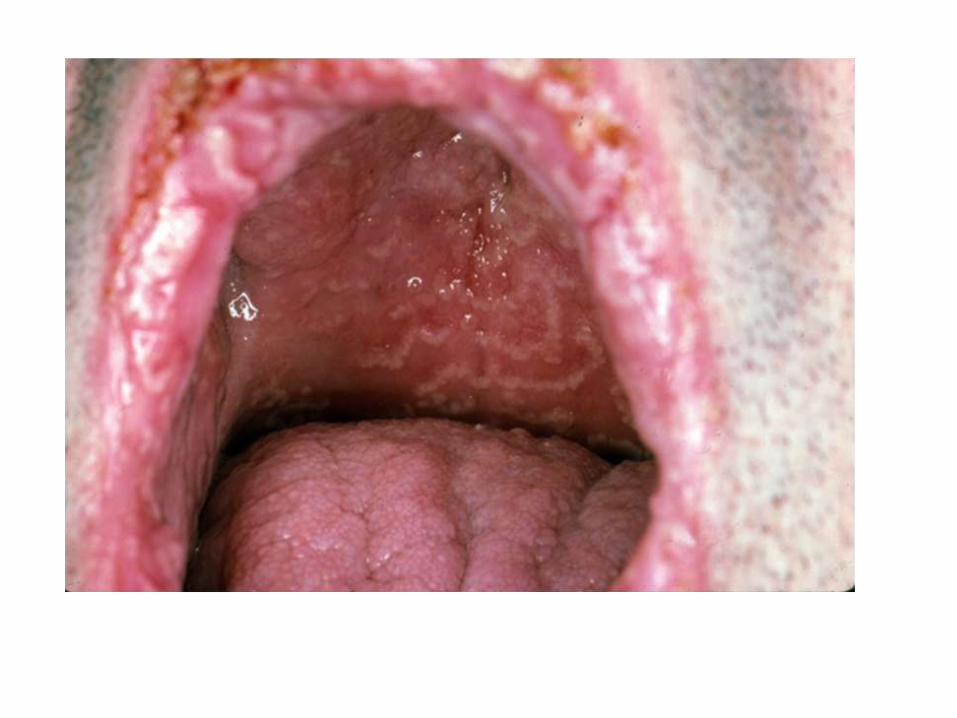
a. Typical oral lichen planus (OLP) of the tongue’s right side. (AB)
b. Diffuse OLP, plaque form, of the entire oral mucosa. Note the leukokeratotic aspect to be distinguished from a leukokeratosis. (AB)
c. Cheek’s OL erosive and planus. (AB & ED)
d. Tongue’s atrophic OLP after a long time evolution. Note the typical network of overlapping white striae of the point. (AB)

ΝΕΟΠΛΑΣΜΑΤΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ
• The incidence and prevalence of oral cancerous and pre-cancerous lesions in IBD is currently unknown.
• No routine oral screening is performed or is advised so far.
• HPV infection!

a.Squamous cell carcinoma (SCC) of the tongue’s point arising on an atrophic oral lichen planus. (ED)
b.SCC of the tongue in a 19-year-old smoker female. The question of the responsability of HPV as cofactors is raised in such a
case. (AB & ED)
c.Typical SCC of the lower lip in a smoker patient arising on a leukokeratosis. (ED)
d.SCC of the lower lip in a young male, rapidly appeared after a kidney transplantation. (ED)

Melanoma of the soft palate in non-IBD non-HIV patient

Kaposi sarcoma of the hard palate in non-IBD non-HIV patient

Author Drug Patient(s) with oral
Ca
Disease Location / Type of
oral cancer
Details
Vilas-Boas et al.61
(case report)
AZA
(9 years)
1 CD Right superior retromollar trigone, SCC /
HPV (-)
Surgery
Li et al.60
(case report)
AZA
(3 years)
1 CD Tongue
SCC (ulcerous in situ)
Surgery
Dulai et al.39
(case report)
IFX+AZA 1 IBD Parotid
Non-Hodgkin lymphoma
Unknown
Biancone et al.26
(multicenter study)
non-biological therapies 1 CD Oropharyngeal
(larynx)
Death
Lichtenstein et al.42
(TREAT cohort registry n=6,773)
IFX
or
Any other therapy
6 CD Oral cavity
(3 patients on IFX)
SIR (95%(CI)
IFX-treated
1.77 (0.37, 5.17)
Any other therapy
1.78 (0.37, 5.21)
Cottone et al.43
(cohort study)
IFX=2,475
ADA=604
1
0
CD Pharyngeal 18 months after IFX
(died)
Pasternak et al.62
(Danish IBD cohort database
n=45,986)
AZA= 5,197 69 IBD Lip/oral cavity/pharynx non-AZA=60
former AZA=4
current AZA=5
RR 95%(CI)
Non-users (referrent)
Former users
1.70 (0.63-4.60)
Users
1.69 (0.57-5.00)
Nyboe- Andersen et al.50
(Danish IBD cohort database)
antiTNF=4,553
non -antiTNF
=51,593
3 IBD Lip/oral cavity/pharynx Crude
1.24 (0.39-3.93)
Adjusted
1.47 (0.43-5.00)
Adjusted for use of azathioprine
1.08 (0.31-3.70)
Colombel et al.44
(Adalimumab cohort trials)
ADA=3,160 1 CD Oral cavity
SCC
1 of total 35 Ca on ADA
<0.1% of the cohort
Sandborn et al.45
(ULTRA cohort study)
ADA=494 1 UC Oral cavity
Beaugerie et al.57 (CESAME cohort
n=17,047)
AZA=7,844 15 IBD 15 ear-nose-throat Ca 3.6% of all Ca (n=428)
Fidder et al.46 (Leuven IFX
cohort n=734 )
AZA (any use pre- or
combo- to IFX)=501
1 IBD Lip SCC patient on combo AZA+IFX
Katsanos et al.47 (EC-IBD
cohort n=681)
AZA=174 2 IBD Lip
(1 BCC in UC on AZA and 1 SCC in UC
not on AZA)
Katsanos et al.48 (Leuven cohort
n=1815)
AZA =725 0 IBD No oral cancer
Fraser et al.49 (Oxford cohort
n=2204)
AZA= 626 2 IBD 1 SCC oral on AZA
1 SCC oral not on AZA
31 Ca in AZA 77 Ca not in AZA
Table. Oral cancers reported in patients with inflammatory bowel disease.


CONCLUSIONS
• The list of oral lesions is extensive.
• may have devastating consequences
• most lesions are easily handled and respond to the treatment of intestinal IBD
• A multidisciplinary approach is essential for the correct diagnosis and management.


The Henry D. Janowitz Division of Gastroenterology at Mt Sinai, NY, USA
+ JAN 12th, 2016





