Zurich Open Repository and Year: 2017 › id › eprint › 126657 › 1 › clr... · A dehiscence...
34
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2017 Randomized clinical study assessing two membranes for guided bone regeneration of peri-implant bone defects: clinical and histological outcomes at 6 months Naenni, Nadja ; Schneider, David ; Jung, Ronald E ; Hüsler, Jürg ; Hämmerle, Christoph H F ; Thoma, Daniel S Abstract: PURPOSE To test whether or not one of two membranes is superior for peri-implant-guided bone regeneration in terms of clinical and histologic outcomes. MATERIAL AND METHODS In 27 patients, 27 two-piece dental implants were placed in single-tooth gaps in the esthetic area. Buccal dehiscence and/or fenestration-type defects were regenerated using demineralized bovine bone mineral and randomly covered with either a resorbable membrane (RES) or a titanium-reinforced non-resorbable membrane (N-RES). Clinical measurements included vertical defect resolution and the horizontal thick- ness of regenerated bone at implant placement and at 6 months. Statistics were performed by means of nonparametric testing. RESULTS The remaining mean vertical defect measured 4 mm (±2.07) (RES) and 2.36 mm (±2.09) (N-RES) (P = 0.044) at baseline and 0.77 mm (±0.85) (RES) and 0.21 mm (±0.80) (N-RES) (P = 0.021) at re-entry. This translated into a defect resolution of 85% (RES) and 90.7% (N- RES) (P = 0.10). The horizontal thickness after augmentation measured 3.46 mm (±0.52) (RES) and 2.82 mm (±0.50) (N-RES) (P = 0.004). The mean loss in horizontal thickness from baseline to re-entry measured 2.23 mm (SD ±1.21) (RES) and 0.14 mm (±0.79) (N-RES) (P = 0.017). The horizontal changes in thickness at the implant shoulder level were statistically significant between the groups (P = 0.0001). CONCLUSIONS Both treatment modalities were clinically effective in regenerating bone as demonstrated by a similar horizontal thickness and vertical defect fill at 6 months. The N-RES group exhibited significantly less horizontal bone thickness reduction from baseline to follow-up. DOI: https://doi.org/10.1111/clr.12977 Posted at the Zurich Open Repository and Archive, University of Zurich ZORA URL: https://doi.org/10.5167/uzh-126657 Journal Article Updated Version Originally published at: Naenni, Nadja; Schneider, David; Jung, Ronald E; Hüsler, Jürg; Hämmerle, Christoph H F; Thoma, Daniel S (2017). Randomized clinical study assessing two membranes for guided bone regeneration of peri-implant bone defects: clinical and histological outcomes at 6 months. Clinical Oral Implants Research, 28(10):1309-1317. DOI: https://doi.org/10.1111/clr.12977
Transcript of Zurich Open Repository and Year: 2017 › id › eprint › 126657 › 1 › clr... · A dehiscence...

Zurich Open Repository andArchiveUniversity of ZurichMain LibraryStrickhofstrasse 39CH-8057 Zurichwww.zora.uzh.ch
Year: 2017
Randomized clinical study assessing two membranes for guided boneregeneration of peri-implant bone defects: clinical and histological outcomes
at 6 months
Naenni, Nadja ; Schneider, David ; Jung, Ronald E ; Hüsler, Jürg ; Hämmerle, Christoph H F ; Thoma,Daniel S
Abstract: PURPOSE To test whether or not one of two membranes is superior for peri-implant-guidedbone regeneration in terms of clinical and histologic outcomes. MATERIAL AND METHODS In 27patients, 27 two-piece dental implants were placed in single-tooth gaps in the esthetic area. Buccaldehiscence and/or fenestration-type defects were regenerated using demineralized bovine bone mineraland randomly covered with either a resorbable membrane (RES) or a titanium-reinforced non-resorbablemembrane (N-RES). Clinical measurements included vertical defect resolution and the horizontal thick-ness of regenerated bone at implant placement and at 6 months. Statistics were performed by means ofnonparametric testing. RESULTS The remaining mean vertical defect measured 4 mm (±2.07) (RES)and 2.36 mm (±2.09) (N-RES) (P = 0.044) at baseline and 0.77 mm (±0.85) (RES) and 0.21 mm (±0.80)(N-RES) (P = 0.021) at re-entry. This translated into a defect resolution of 85% (RES) and 90.7% (N-RES) (P = 0.10). The horizontal thickness after augmentation measured 3.46 mm (±0.52) (RES) and2.82 mm (±0.50) (N-RES) (P = 0.004). The mean loss in horizontal thickness from baseline to re-entrymeasured 2.23 mm (SD ±1.21) (RES) and 0.14 mm (±0.79) (N-RES) (P = 0.017). The horizontalchanges in thickness at the implant shoulder level were statistically significant between the groups (P= 0.0001). CONCLUSIONS Both treatment modalities were clinically effective in regenerating bone asdemonstrated by a similar horizontal thickness and vertical defect fill at 6 months. The N-RES groupexhibited significantly less horizontal bone thickness reduction from baseline to follow-up.
DOI: https://doi.org/10.1111/clr.12977
Posted at the Zurich Open Repository and Archive, University of ZurichZORA URL: https://doi.org/10.5167/uzh-126657Journal ArticleUpdated Version
Originally published at:Naenni, Nadja; Schneider, David; Jung, Ronald E; Hüsler, Jürg; Hämmerle, Christoph H F; Thoma,Daniel S (2017). Randomized clinical study assessing two membranes for guided bone regenerationof peri-implant bone defects: clinical and histological outcomes at 6 months. Clinical Oral ImplantsResearch, 28(10):1309-1317.DOI: https://doi.org/10.1111/clr.12977

Randomized clinical study assessing two membranes for guided
bone regeneration of peri-implant bone defects: clinical and histological
outcomes at 6 months
Nadja Naenni1, David Schneider1, Ronald E. Jung1, Jürg Hüsler, Christoph H.F.
Hämmerle1, Daniel S. Thoma1
Key words: dental implants, bone and bones, bone regeneration, membranes,
alveorlar ridge augmentation (all Mesh terms)
Running title: guided bone regeneration using two different membranes
Address for correspondence:
PD Dr. Daniel S. Thoma Clinic of Fixed and Removable Prosthodontics and Dental Material Science Center of Dental Medicine, University of Zurich Plattenstrasse 11 CH-8032 Zurich, Switzerland Phone: +41 44 634 32 60 Fax: +41 44 634 43 05 e-mail: [email protected]
1 Clinic for Fixed and Removable Prosthodontics and Dental Material Science,
Center of Dental Medicine, University of Zurich, Zurich, Switzerland

Abstract
Purpose: To test whether or not one out of two membranes is superior for peri-
implant guided bone regeneration in terms of clinical and histologic outcomes.
Materials and Methods: In 27 patients, 27 two-piece dental implants were
placed in single-tooth gaps in the esthetic area. Buccal dehiscence and/or
fenestration-type defects were regenerated using demineralized bovine bone
mineral (DBBM) and randomly covered with either a resorbable membrane (RES)
or a titanium-reinforced non-resorbable membrane (N-RES). Clinical
measurements included vertical defect resolution and the horizontal thickness of
regenerated bone at implant placement and at 6 months. Statistics were
performed by means of non-parametric testing.
Results: The remaining mean vertical defect measured 4.00mm (±2.07) (RES)
and 2.36mm (±2.09) (N-RES) (p=0.044) at baseline and 0.77mm (±0.85) (RES)
and 0.21mm (±0.80) (N-RES) (p=0.021) at re-entry. This translated into a
defect resolution of 85% (RES) and 90.7% (N-RES) (p=0.10). The horizontal
thickness after augmentation measured 3.46mm (±0.52) (RES) and 2.82mm
(±0.50) (N-RES) (p=0.004). The mean loss in horizontal thickness from baseline
to re-entry measured 2.23mm (SD±1.21) (RES) and 0.14mm (±0.79) (N-RES)
(p=0.017). The horizontal changes in thickness at the implant shoulder level
were statistically significant between the groups (p=0.0001).
Conclusions: Both treatment modalities were clinically effective in regenerating
bone as demonstrated by a similar horizontal thickness and vertical defect fill at 6
months. The N-RES group exhibited significantly less horizontal bone thickness
reduction from baseline to follow-up.

Introduction
Guided bone regeneration (GBR) procedures are routinely performed in dental
practice to regenerate missing hard tissue volume prior to or simultaneously with
dental implant placement (Hammerle et al., 2002, Bornstein et al., 2008,
Hammerle and Karring, 1998). Various GBR techniques have been proposed and
numerous materials are available to the practitioner (Donos et al., 2008, Esposito
et al., 2006, Aghaloo and Moy, 2007, Jensen and Terheyden, 2009, Benic and
Hammerle, 2014).
Initially, the GBR technique was developed to regenerate periodontal tissues
(Nyman et al., 1982, Gottlow et al., 1984, Gottlow et al., 1986). Later, this
technique was also suggested and applied for bone augmentation around dental
implants (Jovanovic et al., 1992, Karring et al., 1993). For that purpose
autogenous bone or bone substitute materials in combination with non-resorbable
barrier membranes were used. The integration of titanium reinforcements into
non-resorbable expanded polytetrafluorethylene (ePTFE) membranes increased
their stability and allowed the membrane to be formed into an adequate shape.
Despite high clinical success rates (Friedmann et al., 2001, von Arx et al., 2001,
Buser et al., 2002), ePTFE membranes exhibit two main clinical disadvantages: i)
an additional surgery procedure is necessary to remove the membrane; ii)
increased rates of membrane exposure leading to impaired wound healing,
especially during the early healing phase (Piette et al., 1995, Moses et al., 2005)
and, bacterial colonization with subsequent infection of the augmented site
(Becker et al., 1994, Simion et al., 1994, Strietzel, 2001).
In order to overcome these shortcomings, resorbable membranes were
introduced. Among these, collagen membranes are well documented and render
high clinical success rates (Pitaru et al., 1987, Zitzmann et al., 1997, Hockers et
al., 1999, Zitzmann et al., 2001a, Friedmann et al., 2001, Hammerle and Lang,
2001, Hammerle et al., 1998). However, these relatively soft membranes do not

maintain space per se and a compression of the regenerated site can potentially
result in a displacement of the augmentation material (Strietzel et al., 2006,
Friedmann et al., 2002)
To date, there is weak evidence with respect to the morphological changes of the
augmented tissues following GBR procedures around dental implants. A variety of
studies focused on the stability of the mucosal margin (Jemt et al., 2006, Priest,
2003, Grunder, 2000) and the height of the papilla around implant-supported
crowns (Cardaropoli et al., 2006, Chang et al., 1999). However, the changes of
contour and morphology of the labial peri-implant tissues have not been
investigated in detail (Jemt et al., 2006, Jemt and Lekholm, 2003) until recently
(Jensen et al., 2014, Schneider et al., 2014).
The aim of the present study was to test whether or not one of two GBR
membranes is superior to the other in terms of: i) vertical defect resolution and
bucco-oral width of regenerated bone at the implant shoulder at 6 months ii)
postoperative complications during the 6-month follow-up and, iii) histologically
assessed mineralized tissue at 6 months.

Materials and methods
This study was designed as a prospective randomized controlled clinical trial. All
procedures and materials were approved by the local ethical committee (Nr.
2010-0051/5). Twenty-seven patients with a single tooth gap (central incisor to
premolar in the maxilla or mandible) in need of implant treatment were
consecutively recruited at the Clinic of Fixed and Removable Prosthodontics and
Dental Material Science, Center of Dental Medicine, the University of Zurich,
Switzerland. Informed consent was obtained from all patients prior to the start of
the study. The following inclusion criteria were applied:
1. Periodontally healthy patients (periodontal probing depths <4mm)
2. Good oral hygiene (full mouth plaque index <25%) (O'Leary et al., 1972)
3. Adequate control of inflammation (full mouth bleeding on probing <25%
(Ainamo and Bay, 1975)
4. Single tooth gaps with a buccal alveolar bone deficiency
5. Planned implant placement >6 weeks after tooth extraction
6. A dehiscence or fenestration-type defect after implant placement
Patients not meeting all inclusion criteria were not enrolled prior to surgery (1-5)
or excluded from the study after implant placement (6).
Enrolled patients were scheduled for a baseline visit. This examination
encompassed the following assessments: clinical periodontal parameters
(periodontal probing depth (PPD), plaque control record (PCR), bleeding on
probing (BOP), all at six sites around the adjacent teeth; the width of keratinized
tissue (KM) on the buccal side of the two neighboring teeth, a conventional
impression (President, Coltène/Whaledent, Altstätten, Switzerland) and clinical
photographs of the planned implant site. Two to 4 weeks after the baseline visit,
implant surgery was performed.

Surgical protocol
Prior to the start of the surgery, patients had to rinse with a 0.2% Chlorhexidine
solution for one minute and were given antibiotics (Amoxicillin 750mg, Sandoz
Pharmaceuticals, Risch, Switzerland) and analgesics (Mefenacid 500mg, Mepha
Pharma AG, Basel, Switzerland). Local anesthesia was achieved with Articaine
hydrochloride (Rudocaine forte®, Streuli, Switzerland). Following an intrasulcular
incision around the two neighbouring teeth and a vertical releasing incision at the
disto-buccal aspect of the distal neighboring tooth a mucoperiosteal flap was
raised. The implant site was prepared according to the manufacturers
recommendations and a screw type, rough surface two-piece dental implant
(OsseoSpeed, ASTRA TECH Implant System, DENTSPLY Implants, Mölndal,
Sweden) was placed in a prosthetically ideal position using a surgical stent.
Implants had to reach primary stability. Subsequently, the peri-implant osseous
defect was measured using a calibrated periodontal probe (PCP-11, Hu-Friedy,
Chicago, USA). Clinical measurements included defect height, depth, width and
infrabony defect size (Fig.1). If no bone defect was present and no bone
augmentation was needed, the patient was excluded from the study.
Simultaneous GBR was performed using demineralized bovine bone mineral
(DBBM, BioOss spongiosa granules, particle size 0.25-1.0mm; Geistlich Pharma
AG, Wolhusen, Switzerland). At this time-point according to a computer-
generated randomization list and using sealed envelopes (prepared by the study
monitor), either one of two membranes was applied:
i) resorbable collagen membrane (BioGide, Geistlich Pharma AG,
Wolhusen, Switzerland) (RES)
ii) non-resorbable ePTFE-membrane (Gore-Tex®, W.L. Gore & Assoc.,
Flagstaff, Arizona, USA) (N-RES)
The peri-implant defect and the missing hard tissue contour were built up with
DBBM particles. The horizontally augmented thickness on the buccal side was

measured at the level of the implant shoulder (Fig.1). In group RES, the
resorbable membrane was cut to fit the osseous defect covering the respective
bone regenerate. Two to three resorbable pins made of polylactic acid (Inion
Pins; Geistlich AG, Wolhusen, Switzerland) were then used to tack the
membrane buccally onto the underlying bone to avoid membrane and DBBM
displacement. In group N-RES, the ePTFE-membrane was extraorally shaped and
adapted to fit the defect size. Non-resorbable titanium pins (Frios®, Friadent
GmbH, Mannheim, Germany) were used to stabilize the membrane. Both
membranes had to overlap the borders of the augmented site defect by at least
2mm. On the palatal/lingual aspect the membranes were placed under the flap.
Subsequently, releasing incisions within the periosteum were performed on the
buccal aspect of the flap to allow for a tension-free wound closure. Primary
wound closure was obtained using non-resorbable sutures (Gore-Tex suture;
Gore, Flagstaff, AZ, USA).
The patients were then instructed to refrain from mechanical plaque removal in
the surgical area for 7-10 days and had to follow a strict postoperative regimen.
This consisted of rinsing with an aqueous solution of 0.2% chlorhexidine
(Kantonsapotheke, Zurich, Switzerland), of a medication with antibiotics for 5
days (Amoxicillin 750mg, Sandoz Pharmaceuticals, Risch, Switzerland) and
analgesics (Mefenacid 500mg, Mepha Pharma AG, Basel, Switzerland) according
to individual needs.
Follow-up visits
Suture removal was performed 7-10 days after implant placement. Patients were
then recalled at 4 weeks, at 3 and at 6 months to assess the soft tissue condition
(normal, swollen, red, dehiscence). In addition, a conventional impression
(President, Coltène/Whaledent, Altsätten, Switzerland) and clinical photographs
of the implant sites were taken at each time-point. At 6 months, re-entry surgery
was performed in all patients by elevating a full thickness flap to again measure

the vertical defect fill and the horizontal thickness of the bone at the buccal
aspect of the implant with a calibrated periodontal probe (PCP-11, Hu-Friedy,
Chicago, USA). These measurements were performed at the level of the implant
shoulder. In addition, core-biopsies were harvested using a trephine bur with an
inner diameter of 1.8mm. The biopsies were performed at a level of 3mm below
the implant shoulder perpendicular to the long axis of the implant with a sink
depth of 3mm (Figure 3). The cover screw was removed and replaced by a
healing abutment. The mucoperiosteal flap was adjusted and sutured to fit
around the neck of the healing abutment. If a buccal concavity was persisting at
this time-point, a soft tissue grafting procedure (Seibert, 1983, Schneider et al.,
2011, Thoma et al., 2016) was performed and implants left submerged for
another 2 months before performing abutment connection.
Histologic preparation and analyses
The biopsies were fixed in 4% buffered formalin for at least 48 hours. The
specimens were then rinsed in running tap water and demineralized for 72 hours
(USEDECALC BioSystems, Muttenz, Switzerland). After decalcification they were
watered again for 1 hour and dehydrated in a graded series of increasing ethanol
concentrations and thereafter infiltrated with xylol and paraffin in a vacuum
infiltration tissue processor (Tissue-Tek VIP, Sakura-Finetek, Torrance, CA/USA).
Specimens were then embedded in paraffin and cut into 2-5µm thickness using a
paraffin-microtome (MICROM, Medite GmbH, Dietlikon, Switzerland). The
specimens were dried with warm air (Wärmeschrank, Bittmann, Basel,
Switzerland), de-paraffinized with xylol and stained with Haemalaun-Eosin
(Robert Hooke 1665, Böhmer 1865).
A qualitative analysis was performed with a light-microscope (Leica CTR6000,
Leica, Wetzlar, Germany) at a magnification of x200. Pictures of each specimen
were taken with a camera attached to the microscope (Leica DFC450, Leica,

Wetzlar, Germany) for further analysis. All available sections were quantitatively
assessed for different tissue components by applying standard histological
morphometrical techniques (Weibel 1980; Gundersen et al. 1988). The different
components (background, non-mineralized tissue, mineralized tissue and bone
substitute material) and their respective amount calculated in % within a central
region of interest. Measurements were carried out using an image analysis
software (LAS V4.3, Leica, Wetzlar, Germany).
Statistical evaluation and analysis
Outcome measures
The following primary and secondary outcome variables were analyzed:
Primary: vertical defect fill (dehiscence defect at the buccal aspect of the
implant)
Secondary: horizontal thickness of the regenerated bone at the buccal aspect of
the implant; defect depth, defect width and infrabony defect height; soft tissue
condition (dehiscences); clinical parameters (PPD, PCR, BOP,KM),
histomorphometric outcome measures (percentage of newly formed bone,
remaining amount of bone substitute material, bone substitute to bone contact)
Sample size calculation
The sample size was calculated according to a previously performed study using
similar primary and secondary endpoints (Jung et al., 2009). As the primary
endpoint of this study was the vertical defect fill, it was planned to recruit a total
number of 34 patients (17 per group). This would enable to detect a difference of
1mm between the test and control group with a standard deviation of σ=1 and a
significance level of α=0.05 with a power of 80%.
Descriptive statistics were applied to the data. Statistical analysis of the most
important questions was based on non-parametric tests because of small sample

sizes. Significance were determined using the Wilcoxon Mann-Whitney U-test with
SAS 9.4. The level of significance was set at P<0.0083 since 6 tests (hypotheses)
were applied for the 6 primary questions (by Bonferroni correction). A p-value
between 0.05 and 0.0083 may be considered as a borderline significance pointing
on a possible difference. Mean and standard deviations are given in the following
section. In the tables medians are reported which are analyzed by the
nonparametric tests. For analysis of possible confounders a robust mixed model
approach (with the R Package pbkrtest) was applied to a part of the data. All the
other tests were used as explorative investigations.

Results
Demographics
Eligible patients were enrolled between March 2010 and January 2013. 55
patients were initially screened. Finally, a total of 27 patients could be
randomized for treatment and included in the study (14 female, 13 male). All
patients were in good general health and had previously undergone
comprehensive dental care. They were all followed up to 6 months after implant
placement. Thirteen patients were randomized for group RES and 14 patients for
group N-RES. Seven implants were placed in the mandible, whereas 21 implants
were placed in the maxilla. The exact distribution of implant sites and locations is
depicted in Table 1.
The mean age was 51.85 years (standard deviation ±29.7). Six patients were
light smokers (≤ 10cig/day) and three patients had a history of periodontitis.
Defect dimensions at implant placement and at re-entry
All data for defect width, defect depth and infrabony defect size are displayed in
Table 2a. Results for defect width and depth were statistically significant or
borderline for the time-point (p=0.0001/p=0.003) but did not show effect of
group interaction in the more complex mixed model.
The mean vertical defect height after implant placement measured 4.00mm
(±2.07) in group RES and 2.36mm (± 2.09) in group N-RES. At 6 months, the
mean remaining vertical defect height measured 0.77mm (± 0.85) (RES) and
0.21mm (±0.80) (N-RES). Table 2b&c
Differences between the two groups were statistically borderline significant at
both time-points (p=0.044/p=0.021). Mean changes in vertical defect height
from baseline to 6 months measured 3.41mm (±2.33) (RES) and 2.14mm
(±2.06) (N-RES) (p=0.1069). Table 2b&c
This amounted to a vertical defect resolution of 85% (RES) and 90.7% (N-RES).

Seven sites (6 RES / 1 N-RES) demonstrated incomplete vertical regeneration,
whilst one site in group RES even showed an increased vertical defect height at
re-entry compared to baseline (after implant placement).
The mean horizontal thickness at the level of the implant shoulder measured
3.46mm (± 0.52) (RES) and 2.82mm (± 0.50) (N-RES) following grafting with
DBBM (p=0.0040). At 6 months, the mean horizontal thickness was 1.32mm (±
1.38) (RES) and 2.68mm (± 1.05) (N-RES) (p=0.0167). Both groups showed a
loss of horizontal thickness over time with a mean of 2.23mm (±1.21) (RES)
and 0.14mm (±0.79) (N-RES). The differences between the groups were
statistically significant (p=0.0001) See Table 2b&c.
Soft tissue condition
Although primary wound closure was obtained in all patients, a total of six
dehiscences (local adverse event) were observed during the 6-month follow-up.
Four dehiscences were observed in group RES (30%) and two in group N-RES
(14%). Five dehiscences were present at the time of suture removal. Four of
these occurred in the RES group and healed spontaneously until the 4-week
follow-up. One dehiscence in the N-RES group healed between the 4-week and 3-
month follow-up. The second dehiscence in the N-RES group occurred between
suture removal and the 4-week follow-up. This patient was advised to apply local
disinfecting agents (Plak Out Gel, Kerr Hawe SA, Bioggio, Switzerland and
Solcoseryl, Meda Pharma GmbH, Wangen-Brüttisellen, Switzerland) and was
recalled once a week for four weeks and later on once a month. The dehiscence
persisted until the re-entry surgery at 6 months.
The number of dehiscences at the different time-points is displayed in Table 3a.
The soft tissue condition at re-entry is displayed in Table 3b. Overall, in all but
one patient, the soft tissues were rated “normal” at 3 and 6 months after implant
surgery.

Clinical parameters
Probing Pocket Depth (PPD)
Mean PPD values varied between 2.27mm (±0.45mm;mesially) and 2.38mm
(±0.44mm;distally) in group RES and 2.34mm (±0.29mm;mes) and 2.50mm
(±0.42mm;dis) in group N-RES. At 6 months PPD values measured 2.24mm
(±0.32mm;mes) and 2.44mm (±0.47mm;dis) for the RES group and 2.36mm
(±0.25mm;mes) and 2.42mm (±0.35mm;dis). Results were statistically not
significant for neither mesial/distal aspect, nor between the groups and at the
two time points (p>0.05).
Plaque control record (PCR)
Plaque indices at time-point before implant placement and at 6 months did not
show to be statistically significant when compared over time. No statistically
significant differences were measured between the two groups.
Bleeding-on-probing (BOP)
BOP values did not show to be statistically significant over time for mesial values,
but decreased over time for the distal values. These were statistically borderline
significant (p=0.04).
Keratinized Tissue (KM)
The width of keratinized tissue decreased between screening (prior to surgery)
and 6 months from 4.1mm (SD 0.77;mesial) and 4.0mm (±0.43; distal) to
3.4mm (±0.47;mesial) and 2.9mm (±0.26;distal) in group RES . The
corresponding values for group N-RES were 4.3mm (±.04;mesial) and 4.2mm
(±0.2;distal) pre-surgically and decreased to 3.8mm (±0.3;mesial) and 3.6mm
(±0.3;distal) at 6 months. For both groups the differences over time were
borderline statistically significant (P=0.03).

Histologic assessment
In general, the histologic samples revealed loose DBBM particles surrounded to a
large extent by newly formed bone and embedded in a loose connective tissue.
Remodeling of the DBBM particles had taken place and led to the formation of
vacuoles with intimate bone formation along the bone substitute surface. (Fig.4)
The density of the DBBM particles and the newly formed bone as well as the
density of the connective tissue demonstrated great variation within the groups.
The histomorphometric analysis showed a mean amount of newly formed bone of
38.0% (±18.4%) (RES) and of 35.7% (±29.5%) (N-RES). The remaining amount
of DBBM was 36.4% (±8.3%) (RES) and 45.2% (±11.9%) (N-RES) revealing a
slightly better containment of the augmented bone substitute material in group
N-RES. The overall mean amount of mineralized tissue was 73.0% (±19.9%)
(RES) and 69.6% (±16.7%) (N-RES). The surface fraction of bone substitute to
bone contact measured calculated bone to bone substitute contact was 46.4%
(±25.3%) (RES) and 41.1% (±19.1%) (N-RES). The differences between the two
groups were not statistically significantly different for any of the histological
assessments (p>0.05).

Discussion
The results of the present RCT demonstrated that i) both GBR membranes were
successful in regenerating bone on the buccal side of dental implants regarding
vertical defect fill and increase in horizontal thickness; ii) the horizontal thickness
decreased to a significantly greater amount over time in group RES compared to
group N-RES; iii) wound dehiscences occurred at a rate of 30% (RES) and 14%
(N-RES), but healed with one exception during 6 months and without the need for
premature removal of the membrane; iv) the augmented DBBM underwent
remodeling processes and promoted new bone formation.
Augmentation of hard tissue simultaneous with implant placement is considered a
routine procedure with successful short- and long-term results (Chiapasco and
Zaniboni, 2009, Jung et al., 2013, Hammerle et al., 2002). This is demonstrated
by survival rates of implants placed in regenerated bone being similar when
compared to implants placed conventionally into sites without the need for bone
augmentation (Hammerle et al., 2002, Donos et al., 2008). Differences between
resorbable and non-resorbable membranes mainly exist in terms of a need for a
second stage surgery (removal of a non-resorbable membrane), a reported
higher rate of dehiscences (non-resorbable membranes) and a higher risk of a
membrane collapse (resorbable membranes) (Zitzmann et al., 1997, Wiltfang et
al., 1998, Moses et al., 2005).
In the present study, peri-implant defect dimensions were re-assessed 6 months
after GBR procedure. Defect height, width and depth were all significantly lower
at the re-entry time-point compared to the day of implant placement with
simultaneous GBR. This demonstrated a successful bone augmentation in both
groups with mean changes over time (defect resolution) ranging between
3.41mm (RES) and 2.14mm (N-RES) and a very minimal persisting defect height
remaining at reentry (0.77mm (RES) and 0.21mm (N-RES)). The difference in

decrease was statistically significant between the groups. This is supported by a
clinical multicenter study reporting a significant decrease in surface exposure
when non-resorbable membranes were used for the treatment of fenestration or
dehiscence-type defects (Dahlin et al., 1995). The remaining defect heights after
healing periods of 3-6 months measured 1.1mm (±2.3) after an initial defect
height of 4.7mm (±3.0) and were therefore slightly greater compared to the
present study. Data on resorbable collagen membranes used in studies with a
similar design reported dehiscence-type defect resolution for the combination of
DBBM plus collagen membrane of 96% (4.25mm from 4.5mm) (Jung et al. 2009)
and 91% (5.4mm from 5.8mm) (Jung et al. 2003), whereas in the present study
defect resolution amounted to 85% (RES) and 90% (N-RES) respectively. In
contrast, in a previous comparative study mean percentages of bone fill of 92%
for resorbable and 78% for non-resorbable membranes were reported favoring
the use of resorbable collagen membranes. However, in that study the relatively
high rate of membrane exposure with non-resorbable membranes often led to
premature removal due to infection. This was interpreted as the main reason for
the lower defect fill for this type of membrane. (Zitzmann et al., 1997). In the
present study, even though dehiscences occurred, no membranes were removed
prior to the 6-month re-entry time-point. In addition, dehiscences were not
associated with greater residual defect heights.
Apart from the defect resolution, which reflects how well a GBR procedure
performed in a vertical dimension, the horizontal thickness, measured at baseline
(following GBR) and at re-entry surgery, documents the stability of the
augmented area. The GBR principle is based on a membrane, which serves as a
tent to allow for bone regeneration underneath. This space-maintenance can be
obtained using a form-stable membrane or a bone substitute material that
stabilizes a non-form-stable membrane. Since in the present study the same
bone substitute material was used in both groups, the effect of the membrane in

terms of stability and containment of the augmented area could be assessed. The
horizontal thickness at baseline was greater in group RES compared to group N-
RES. At re-entry, however, the horizontal thickness in group N-RES was greater.
Whereas in both groups, a loss of horizontal thickness was observed, the loss in
group N-RES was statistically significantly smaller. This demonstrates that the
collagen membrane tended to collapse even though being supported by the bone
substitute material.
It has previously been reported that in order to avoid vertical bone loss over
time, a minimal buccal bone dimension of 2mm is required (Spray et al., 2000,
Botticelli et al., 2004). One might speculate that for a successful GBR 2mm of
buccal bone should be obtained. Keeping in mind these data and the loss of
volume that predominantly occurred with the resorbable membrane, a buccal
over contouring at the day of surgery might be recommended. The long-term fate
of augmented bone and the optimal amount of bone required for stable results
remains unknown today. More recent data even suggest that in cases with
missing buccal bone on the implant surface, the peri-implant soft tissues might
compensate and provide clinically successful outcomes (Benic et al., 2012,
Kuchler et al., 2015).
In the present study the number of wound dehiscences was comparable to results
reported in previous studies using the same membranes (Moses et al., 2005).
Though more dehiscences occurred in group RES (30%) than in group N-RES
(14%). This to some extent contradicts results from previous studies with rates
for dehiscences ranging from 11% (Dahlin et al., 1995) to 20% for non-
resorbable membranes (Chiapasco and Zaniboni, 2009) compared to rates
ranging between 5% (Chiapasco and Zaniboni, 2009) and 31% for resorbable
membranes (Jung et al., 2009). Most studies however, observed more
dehiscences with non-resorbable membranes compared to resorbable membranes
(Moses et al., 2005, Zitzmann et al., 1997). Dehiscences of non-resorbable

membranes may lead to early removal of the membrane resulting in impaired
bone regeneration. In contrast to previously published data (Moses et al., 2005)
dehiscences in the present study were not associated with obtained residual
defect heights at 6 months. In addition, the two membranes in group N-RES that
had a dehiscence, did not have to be removed prematurely. Due to the strict
application of local desinfecting agents the respective sites could be prevented
from bacterial colonization of the underlying membrane. Similarly, membranes in
group RES with dehiscences healed without the need for further surgical
intervention. One explanation that might be associated with the number of
dehiscences could be the incision design and handling of the flap.
(Dahlin et al., 1995). In the present study the incision design was standardized
and did not depend on the randomization. Incisions were made paracrestal
(palatally or lingually) in order not to compromise blood supply. Subperiosteal
incisions were made to allow for a tension-free adaptation of the wound margins.
Moreover, a factor certainly contributing to the low numbers of wound
dehiscences is a strict maintenance program. All patients in this study were
recalled regularly for a check-up at set time-points, reinstructed for oral hygiene
and supported by a professional cleaning. This was reflected in PCR values being
stable and BOP values even decreasing over time up to 6 months. Another
explantation for the higher number of dehiscences within RES group might be the
following. Being aware of having to prematurely remove non-resorbable
membranes in case of bacterial colonization, one may have tried not to
overcontour the augmentation. It could well be assumed that in order to
compensate for the horizontal resorption the surgeons augmented the sites within
RES group to a greater extent. This is maybe reflected by a higher amount in
horizontal thickness after GBR of 3.46mm (RES) versus 2.82 (N-RES).
Although clinical evidence clearly shows the successfull use of e-PTFE membranes
for bone regeneration procedures, dehiscences do occur quite often and may
compromise the surgical outcome (Zitzmann et al., 1997, Moses et al., 2005). A

possible reason for the vulnerability of these membranes towards microbial
invasion in case of early exposure might be their macroporosity allowing for
bacterial colonization of the membrane and thus leading a subsequent infection.
As an alternative to the use of e-PTFE, non-expanded, a dense
polytetrafluoroethylene (n-PTFE) was proposed due to its inherent characteristics.
Most of the available literature on the use of n-PTFE is based on pre-clinical
studies. Clinical studies are limited to case series only. Clinical procedures having
been investigated including ridge preservation techniques or the placement of
immediate implants with concomittant GBR procedures. Whether or not n-PTFE
membranes can be successfully used for GBR procedures remains to be proven.
(Carbonell et al., 2014)
Both membranes contained the augmented DBBM to a similar extent as
demonstrated by small standard deviations in both groups. In terms of bone
regeneration, great variability was observed between the different sites. The
calculated area fractions of newly formed bone range between 4% and 63%
(RES) and 11% and 98% (N-RES). This rather high heterogeneity in between the
sites is mostly due to the fact that in some biopsies, the obtained tissues
contained a very loose and only slightly mineralized structure with DBBM particles
being surrounded by a loose connective tissue. Since biopsies were taken
superficially at the buccal aspect, some of the GBR material might not have been
completely integrated and might therefore explain these differences. This is in
agreement with a previous clinical study comparing a hydrogel membrane to the
same collagen membrane used in the present study (Jung et al., 2009). In that
study, a similar re-entry surgery at 6 months was performed and revealed a
quality of newly formed bone that ranged from very dense to more soft bone.
Previous studies on peri-implant GBR with harvested biopsies reported similar
clinical observations (Zitzmann et al., 1997, Jung et al., 2009). Histologic data
from biopsies taken 6 months after augmentation surgery with DBBM plus
collagen membrane reported newly formed bone between 23% (Zitzmann et al.,

2001b) and 30% (Jung et al., 2003) and 39% for DBBM plus non-resorbable
membrane (Friedmann et al., 2002). The mean amounts of newly formed bone in
the present study were slightly higher with 38% (RES) and 36% (N-RES) within a
similar observation period.
The outcomes of the study certainly need to be interpreted with caution. This is
mainly due to an imbalance in terms of the initial defect dimension that differed
significantly or were borderline after implant placement. Applying the more
complex mixed model, however, no effect of group interaction was demonstrated.
Moreover, the distribution of sites for the two groups was imbalanced. This short-
coming was due to the nature of the randomization process that took place
immediately after implant placement. This might have impacted the outcomes at
6 months. Interestingly, at 6 months, the differences were from a clinical point of
view negligible (even though for some outcomes measures statistically
significant). Overall, a high number of patients did not fullfill the inclusion criteria.
This was due to the need for primary bone augmentation or a lack of dehiscence
after implant placement. If a GBR was applied on the buccal side of the implant
only for contour reasons, the patient was not included in the study. Furthermore,
the production of the non-resorbable e-PTFE membranes was discontinued and
they were not available for use after the inclusion of 27 patients. This
unfortunately lead to the termination of the recruitment phase and thus did not
allow including more patients in this RCT. Still, other non-resorbable membranes
were put on the market and are available for clinical use today. Therefore, further
follow-up examinations will be performed evaluating longer term outcomes and
trying to answer the question whether or not bone regenerated using resorbable
or non-resorbable membranes around dental implants can be maintained over
time.

Conclusions
Guided bone regeneration for buccal dehiscence and fenestration-type defects
can be achieved using either membrane. This was demonstrated by a similar
vertical defect resolution and a similar horizontal thickness at 6 months in both
groups. As collagen membranes do not maintain space and thus tend to collapse,
the decrease in horizontal thickness was significantly different in favor of the
non-resorbable membrane group at 6 months. Wound dehiscences occurred at a
relatively high frequency in both groups, but were not associated with residual
vertical defect height at 6 months. Histologically, both membranes allowed for
new bone formation and contained a similar amount of bone substitute material
during 6 months.

Acknowledgements
The study was supported by the Clinic of Fixed and Removable Prosthodontics
and Dental Material Science, University of Zurich, Switzerland and by a research
grant from the Swiss Dental Association (SSO), Bern, Switzerland. In addition,
dental implant materials were provided free of charge by Dentsply (DENTSPLY
Implants, Mölndal, Sweden), whereas bone substitute materials and membranes
were provided by Geistlich Pharma AG, Wolhusen, Switzerland. The authors do
not report to have any conflict of interest to any products related to this study.
The authors are grateful to Mrs. Gisela Müller, study monitor at the Clinic for
Fixed and Removable Prosthodontics and Dental Material Science, University of
Zurich, Switzerland for her support with the data preparation for the statistical
analysis and her support during the preparation of the manuscript. The authors
would also like to address gratitude to Ms. Sonja Hitz, Clinic of Fixed and
Removable Prosthodontics and Dental Material Science, University of Zurich for
the preparation of the histologic slides. Thanks also go to Dr.Caroline
Lustenberger for her support in the statistical analysis of the collected data.

Figure Legends
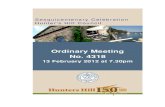
Figure 1 Clinical measurements performed during implant surgery and at re-entry (6 months).
Figure 2 Treatment groups with respective membrane. Collagen membrane in resorbable group (RES) and ePTFE-membrane in non-resorbable group (N-RES).
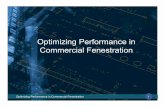
Figure 3 Clinical picture of a site at the time of re-entry 6 months after implant placement and GBR. A trephine bur with an inner diameter of 1.8mm is used to harvest the biopsy at 3mm below the implant shoulder perpendicular to the long axis of the implant with a sink depth of 3mm.
Figure 4 Histological sample harvested with a trephine bur with the respective amounts of: 1) bone substitute material (DBBM), 2) newly formed bone and 3) soft tissue.
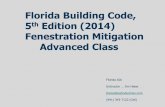
Table 1 Distribution of implant sites and locations in both groups.
Table 2a/b/c Bone defect dimensions and horizontal thickness in millimeters at surgery and after 6 months . Mean values, standard deviations and medians (p-value of the R-test and Wilcoxon Mann-Whitney test 2b/c).
Table 3a/b 3a Number of soft tissue dehiscences at the different time points of assessment. 3b Soft tissue condition at the 6-month re-entry (normal/red/swollen/dehiscence).

References
Aghaloo, T. L. & Moy, P. K. (2007) Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? International Journal of Oral and Maxillofacial Implants 22 Suppl, 49-70.
Ainamo, J. & Bay, I. (1975) Problems and proposals for recording gingivitis and plaque. International Dental Journal 25, 229-235.
Becker, W., Dahlin, C., Becker, B. E., Lekholm, U., van Steenberghe, D., Higuchi, K. & Kultje, C. (1994) The use of e-PTFE barrier membranes for bone promotion around titanium implants placed into extraction sockets: a prospective multicenter study. International Journal of Oral and Maxillofacial Implants 9, 31-40.
Benic, G. I. & Hammerle, C. H. (2014) Horizontal bone augmentation by means of guided bone regeneration. Periodontology 2000 66, 13-40. doi:10.1111/prd.12039.
Benic, G. I., Mokti, M., Chen, C. J., Weber, H. P., Hammerle, C. H. & Gallucci, G. O. (2012) Dimensions of buccal bone and mucosa at immediately placed implants after 7 years: a clinical and cone beam computed tomography study. Clinical Oral Implants Research 23, 560-566. doi:10.1111/j.1600-0501.2011.02253.x.
Bornstein, M. M., Halbritter, S., Harnisch, H., Weber, H. P. & Buser, D. (2008) A retrospective analysis of patients referred for implant placement to a specialty clinic: indications, surgical procedures, and early failures. International Journal of Oral and Maxillofacial Implants 23, 1109-1116.
Botticelli, D., Berglundh, T. & Lindhe, J. (2004) Hard-tissue alterations following immediate implant placement in extraction sites. Journal of Clinical Periodontology 31, 820-828. doi:10.1111/j.1600-051X.2004.00565.x.
Buser, D., Ingimarsson, S., Dula, K., Lussi, A., Hirt, H. P. & Belser, U. C. (2002) Long-term stability of osseointegrated implants in augmented bone: a 5-year prospective study in partially edentulous patients. International Journal of Periodontics and Restorative Dentistry 22, 109-117.
Carbonell, J. M., Martin, I. S., Santos, A., Pujol, A., Sanz-Moliner, J. D. & Nart, J. (2014) High-density polytetrafluoroethylene membranes in guided bone and tissue regeneration procedures: a literature review. International Journal of Oral and Maxillofacial Surgery 43, 75-84. doi:10.1016/j.ijom.2013.05.017.
Cardaropoli, G., Lekholm, U. & Wennstrom, J. L. (2006) Tissue alterations at implant-supported single-tooth replacements: a 1-year prospective clinical study. Clinical Oral Implants Research 17, 165-171.
Chang, M., Wennstrom, J. L., Odman, P. & Andersson, B. (1999) Implant supported single-tooth replacements compared to contralateral natural teeth. Crown and soft tissue dimensions. Clinical Oral Implants Research 10, 185-194.
Chiapasco, M. & Zaniboni, M. (2009) Clinical outcomes of GBR procedures to correct peri-implant dehiscences and fenestrations: a systematic review. Clinical Oral Implants Research 20 Suppl 4, 113-123. doi:10.1111/j.1600-0501.2009.01781.x.
Dahlin, C., Lekholm, U., Becker, W., Becker, B., Higuchi, K., Callens, A. & van Steenberghe, D. (1995) Treatment of fenestration and dehiscence bone defects around oral implants using the guided tissue regeneration technique: a prospective multicenter study. International Journal of Oral and Maxillofacial Implants 10, 312-318.
Donos, N., Mardas, N. & Chadha, V. (2008) Clinical outcomes of implants following lateral bone augmentation: systematic assessment of available options (barrier membranes, bone grafts, split osteotomy). Journal of Clinical Periodontology 35, 173-202.

Esposito, M., Grusovin, M. G., Coulthard, P. & Worthington, H. V. (2006) The efficacy of various bone augmentation procedures for dental implants: a Cochrane systematic review of randomized controlled clinical trials. International Journal of Oral and Maxillofacial Implants 21, 696-710.
Friedmann, A., Strietzel, F. P., Maretzki, B., Pitaru, S. & Bernimoulin, J. P. (2001) Observations on a new collagen barrier membrane in 16 consecutively treated patients. Clinical and histological findings. Journal of Periodontology 72, 1616-1623. doi:10.1902/jop.2001.72.11.1616.
Friedmann, A., Strietzel, F. P., Maretzki, B., Pitaru, S. & Bernimoulin, J. P. (2002) Histological assessment of augmented jaw bone utilizing a new collagen barrier membrane compared to a standard barrier membrane to protect a granular bone substitute material. Clinical Oral Implants Research 13, 587-594.
Gottlow, J., Nyman, S., Karring, T. & Lindhe, J. (1984) New attachment formation as the result of controlled tissue regeneration. Journal of Clinical Periodontology 11, 494-503.
Gottlow, J., Nyman, S., Lindhe, J., Karring, T. & Wennstrom, J. (1986) New attachment formation in the human periodontium by guided tissue regeneration. Case reports. Journal of Clinical Periodontology 13, 604-616.
Grunder, U. (2000) Stability of the mucosal topography around single-tooth implants and adjacent teeth: 1-year results. International Journal of Periodontics and Restorative Dentistry 20, 11-17.
Hammerle, C. H., Bragger, U., Schmid, B. & Lang, N. P. (1998) Successful bone formation at immediate transmucosal implants: a clinical report. International Journal of Oral and Maxillofacial Implants 13, 522-530.
Hammerle, C. H., Jung, R. E. & Feloutzis, A. (2002) A systematic review of the survival of implants in bone sites augmented with barrier membranes (guided bone regeneration) in partially edentulous patients. Journal of Clinical Periodontology 29 Suppl 3, 226-231; discussion 232-223.
Hammerle, C. H. & Karring, T. (1998) Guided bone regeneration at oral implant sites. Periodontology 2000 17, 151-175.
Hammerle, C. H. & Lang, N. P. (2001) Single stage surgery combining transmucosal implant placement with guided bone regeneration and bioresorbable materials. Clinical Oral Implants Research 12, 9-18.
Hockers, T., Abensur, D., Valentini, P., Legrand, R. & Hammerle, C. H. (1999) The combined use of bioresorbable membranes and xenografts or autografts in the treatment of bone defects around implants. A study in beagle dogs. Clinical Oral Implants Research 10, 487-498.
Jemt, T., Ahlberg, G., Henriksson, K. & Bondevik, O. (2006) Changes of anterior clinical crown height in patients provided with single-implant restorations after more than 15 years of follow-up. International Journal of Prosthodontics 19, 455-461.
Jemt, T. & Lekholm, U. (2003) Measurements of buccal tissue volumes at single-implant restorations after local bone grafting in maxillas: a 3-year clinical prospective study case series. Clinical Implant Dentistry and Related Research 5, 63-70.
Jensen, S. S., Bosshardt, D. D., Gruber, R. & Buser, D. (2014) Long-Term Stability of Contour Augmentation in the Esthetic Zone. Histologic and Histomorphometric Evaluation of 12 Human Biopsies 14 to 80 Months After Augmentation. Journal of Periodontology, 1-15. doi:10.1902/jop.2014.140182.
Jensen, S. S. & Terheyden, H. (2009) Bone augmentation procedures in localized defects in the alveolar ridge: clinical results with different bone grafts and bone-substitute materials. International Journal of Oral and Maxillofacial Implants 24 Suppl, 218-236.

Jovanovic, S. A., Spiekermann, H. & Richter, E. J. (1992) Bone regeneration around titanium dental implants in dehisced defect sites: a clinical study. International Journal of Oral and Maxillofacial Implants 7, 233-245.
Jung, R. E., Fenner, N., Hammerle, C. H. & Zitzmann, N. U. (2013) Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12-14 years. Clinical Oral Implants Research 24, 1065-1073. doi:10.1111/j.1600-0501.2012.02522.x.
Jung, R. E., Glauser, R., Scharer, P., Hammerle, C. H., Sailer, H. F. & Weber, F. E. (2003) Effect of rhBMP-2 on guided bone regeneration in humans. Clinical Oral Implants Research 14, 556-568.
Jung, R. E., Halg, G. A., Thoma, D. S. & Hammerle, C. H. (2009) A randomized, controlled clinical trial to evaluate a new membrane for guided bone regeneration around dental implants. Clinical Oral Implants Research 20, 162-168. doi:10.1111/j.1600-0501.2008.01634.x.
Karring, T., Nyman, S., Gottlow, J. & Laurell, L. (1993) Development of the biological concept of guided tissue regeneration--animal and human studies. Periodontology 2000 1, 26-35.
Kuchler, U., Chappuis, V., Gruber, R., Lang, N. P. & Salvi, G. E. (2015) Immediate implant placement with simultaneous guided bone regeneration in the esthetic zone: 10-year clinical and radiographic outcomes. Clinical Oral Implants Research. doi:10.1111/clr.12586.
Moses, O., Pitaru, S., Artzi, Z. & Nemcovsky, C. E. (2005) Healing of dehiscence-type defects in implants placed together with different barrier membranes: a comparative clinical study. Clinical Oral Implants Research 16, 210-219.
Nyman, S., Lindhe, J., Karring, T. & Rylander, H. (1982) New attachment following surgical treatment of human periodontal disease. Journal of Clinical Periodontology 9, 290-296.
O'Leary, T. J., Drake, R. B. & Naylor, J. E. (1972) The plaque control record. Journal of Periodontology 43, 38. doi:10.1902/jop.1972.43.1.38.
Piette, E., Alberius, P., Samman, N. & Linde, A. (1995) Experience with e-PTFE membrane application to bone grafting of cleft maxilla. International Journal of Oral and Maxillofacial Surgery 24, 327-332.
Pitaru, S., Tal, H., Soldinger, M., Azar-Avidan, O. & Noff, M. (1987) Collagen membranes prevent the apical migration of epithelium during periodontal wound healing. Journal of Periodontal Research 22, 331-333.
Priest, G. (2003) Predictability of soft tissue form around single-tooth implant restorations. International Journal of Periodontics and Restorative Dentistry 23, 19-27.
Schneider, D., Grunder, U., Ender, A., Hammerle, C. H. & Jung, R. E. (2011) Volume gain and stability of peri-implant tissue following bone and soft tissue augmentation: 1-year results from a prospective cohort study. Clinical Oral Implants Research 22, 28-37. doi:10.1111/j.1600-0501.2010.01987.x.
Schneider, D., Schmidlin, P. R., Philipp, A., Annen, B. M., Ronay, V., Hammerle, C. H., Attin, T. & Jung, R. E. (2014) Labial soft tissue volume evaluation of different techniques for ridge preservation after tooth extraction: a randomized controlled clinical trial. Journal of Clinical Periodontology 41, 612-617. doi:10.1111/jcpe.12246.
Seibert, J. S. (1983) Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compendium of Continuing Education in Dentistry 4, 437-453.
Simion, M., Baldoni, M., Rossi, P. & Zaffe, D. (1994) A comparative study of the effectiveness of e-PTFE membranes with and without early exposure during the healing period. International Journal of Periodontics and Restorative Dentistry 14, 166-180.

Spray, J. R., Black, C. G., Morris, H. F. & Ochi, S. (2000) The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. Annals of Periodontology 5, 119-128. doi:10.1902/annals.2000.5.1.119.
Strietzel, F. P. (2001) [Risks and complications of membrane-guided bone regeneration. Retrospective analysis]. Mund-, Kiefer- und Gesichtschirurgie 5, 28-32.
Strietzel, F. P., Khongkhunthian, P., Khattiya, R., Patchanee, P. & Reichart, P. A. (2006) Healing pattern of bone defects covered by different membrane types--a histologic study in the porcine mandible. Journal of biomedical materials research. Part B, Applied biomaterials 78, 35-46. doi:10.1002/jbm.b.30452.
Thoma, D. S., Zeltner, M., Hilbe, M., Hammerle, C. H., Husler, J. & Jung, R. E. (2016) Randomized controlled clinical study evaluating effectiveness and safety of a volume-stable collagen matrix compared to autogenous connective tissue grafts for soft tissue augmentation at implant sites. Journal of Clinical Periodontology. doi:10.1111/jcpe.12588.
von Arx, T., Cochran, D. L., Hermann, J. S., Schenk, R. K., Higginbottom, F. L. & Buser, D. (2001) Lateral ridge augmentation and implant placement: an experimental study evaluating implant osseointegration in different augmentation materials in the canine mandible. International Journal of Oral and Maxillofacial Implants 16, 343-354.
Wiltfang, J., Merten, H. A. & Peters, J. H. (1998) Comparative study of guided bone regeneration using absorbable and permanent barrier membranes: a histologic report. International Journal of Oral and Maxillofacial Implants 13, 416-421.
Zitzmann, N. U., Naef, R. & Scharer, P. (1997) Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration. International Journal of Oral and Maxillofacial Implants 12, 844-852.
Zitzmann, N. U., Scharer, P. & Marinello, C. P. (2001a) Long-term results of implants treated with guided bone regeneration: a 5-year prospective study. International Journal of Oral and Maxillofacial Implants 16, 355-366.
Zitzmann, N. U., Scharer, P., Marinello, C. P., Schupbach, P. & Berglundh, T. (2001b) Alveolar ridge augmentation with Bio-Oss: a histologic study in humans. International Journal of Periodontics and Restorative Dentistry 21, 288-295.

Figure 1 Figure 2

Figure 3 Figure 4


Table 1
Table 2a
Table 2b
upper jaw (RES/N-RES) lower jaw (RES/N-RES) total
central incisors 4 (2/2) 0 4
lateral incisors 8 (1/7) 0 8
premolars 9 (9/0) 6 (4/2) 15
total 21 6 27
At Surgery At Re-entry (6m)
RES N-RES RES N-RES p-value
Defect dimensions time group
Width 3.08 (±0.18)
3.00
3.19 (±0.33)
3.00
0.73 (±0.33)
.00
0.23 (±0.23)
.00p=0.0001 p=0.36
Depth 0.92 (±0.23)
1.00
1.00 (±0.28)
.00
0.41 (±0.28)
.00
0.23 (±0.23)
.00p=0.003 p=0.75
Infrabony 0.15 (±0.15)
.00
1.00 (±0.59)
.00
0.0 (±0.0).00
0.0 (±0.0).00 p=0.02
At Surgery
RES N-RES p-value
Vertical & Horizontal Dimensions
Vertical defectmedian
4.00 (±2.07)4.00
2.36 (±2.09)2.50 p=0.0444
Horizontal thicknessmedian
3.46 (±0.52)3.00
2.82 (±0.50)3.00 p=0.0040

Table 2cAt Re-entry (6months)
RES N-RES p-value
Defect dimensions
Vertical defectmedian
0.77 (±0.85)1.00
0.21 (±0.80)0.00 p=0.0213
Horizontal thicknessmedian
1.32 (±1.38)1.00
2.68 (±1.05)3.00 p=0.0167
Loss of vertical defectmedian
3.41 (±2.33)4.00
2.14 (±2.06)2.00 p=0.1069
Loss of horizontal thicknessmedian
2.23 (±1.21)3.00
0.14 (±0.79)0.00 p=0.0001

Table 3a
Table 3b
1 week (suture removal)
4 weeks 3 months At Re-entry (6 months)
RES 4 0 0 0
N-RES 1 2 1 1
normal (e.g. healthy) red/swollen dehiscence
RES 6 2 0
N-RES 7 5 1
percentage 50.5% 25.9% 7.7%