Zigrang Obesity CA012117PCP.pptsyllabus.aace.com/.../presentations/4_Zigrang_Obesity_012117.pdf ·...
69
Etiology and Diagnosis of Obesity OBESITY IS A DISEASE 1
Transcript of Zigrang Obesity CA012117PCP.pptsyllabus.aace.com/.../presentations/4_Zigrang_Obesity_012117.pdf ·...
Etiology and Diagnosis of Obesity
OBESITY IS A DISEASE
1
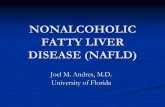
More than Two Thirds of US Adults Are Overweight or Obese
2
since 1962
1.7-foldincrease
in obesity since 1962
NHANES DataU.S. Adults Age ≥20 Years
(Crude Estimate)
BMI, body mass index (in kg/m2); NHANES, National Health and Nutrition Examination Survey (x-axis lists last year of each survey).Flegal KM, et al. Int J Obes Relat Metab Disord. 1998;22:39-47; Flegal KM, et al. JAMA. 2002;288:1723-1727; Flegal KM, et al. JAMA. 2010;303:235-241; Flegal KM, et al. JAMA. 2012;307:491-497. Ogden CL, et al. JAMA. 2014;311:806-814.
BMI ≥30BMI 25-29
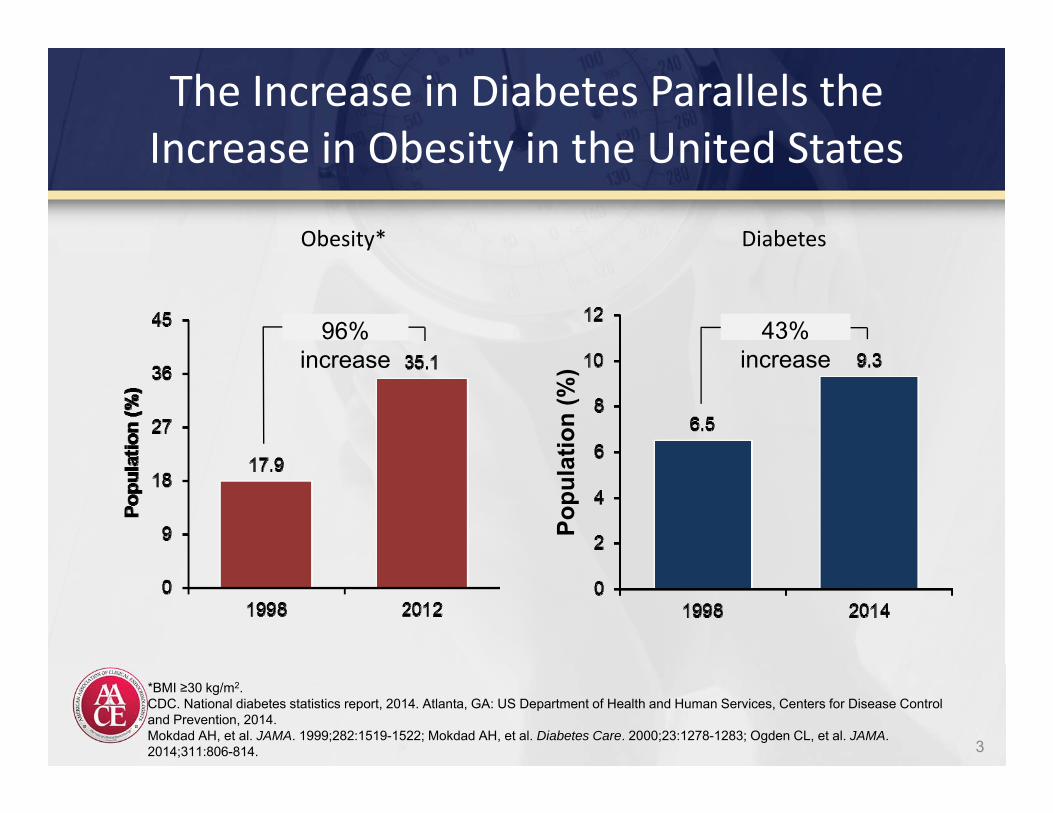
The Increase in Diabetes Parallels the Increase in Obesity in the United States
3
*BMI ≥30 kg/m2.CDC. National diabetes statistics report, 2014. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, 2014.Mokdad AH, et al. JAMA. 1999;282:1519-1522; Mokdad AH, et al. Diabetes Care. 2000;23:1278-1283; Ogden CL, et al. JAMA. 2014;311:806-814.
Obesity* Diabetes
96% increase
43% increase
Popu
latio
n (%
)
Women Men
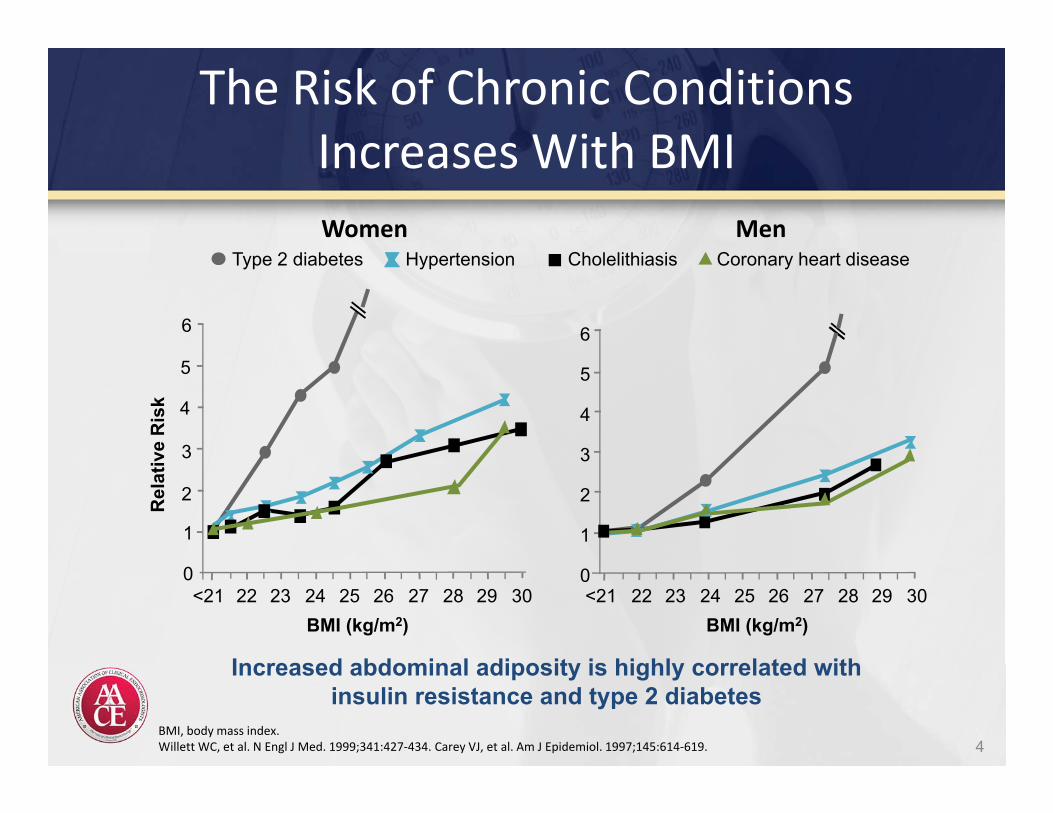
Increased abdominal adiposity is highly correlated with insulin resistance and type 2 diabetes
BMI (kg/m2)<21 22 23 24 25 26 27 28 29 30
6
5
3
2
1
0
4
Rel
ativ
e R
isk
Type 2 diabetes Hypertension Cholelithiasis Coronary heart disease
The Risk of Chronic Conditions Increases With BMI
BMI (kg/m2)
6
5
3
2
1
0
4
<21 22 23 24 25 26 27 28 29 30
BMI, body mass index.Willett WC, et al. N Engl J Med. 1999;341:427‐434. Carey VJ, et al. Am J Epidemiol. 1997;145:614‐619. 4
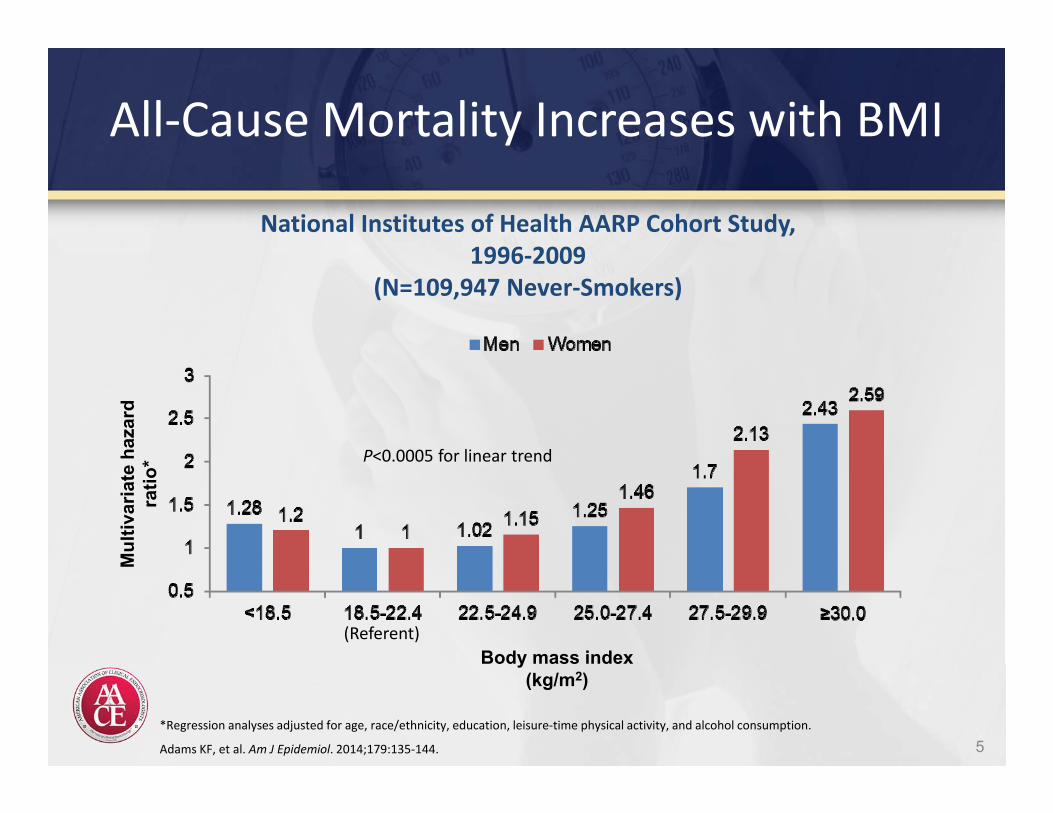
All‐Cause Mortality Increases with BMI
5
National Institutes of Health AARP Cohort Study, 1996‐2009
(N=109,947 Never‐Smokers)
Mul
tivar
iate
haz
ard
ratio
*
*Regression analyses adjusted for age, race/ethnicity, education, leisure‐time physical activity, and alcohol consumption.
Adams KF, et al. Am J Epidemiol. 2014;179:135‐144.
(Referent)
P<0.0005 for linear trend
Body mass index(kg/m2)
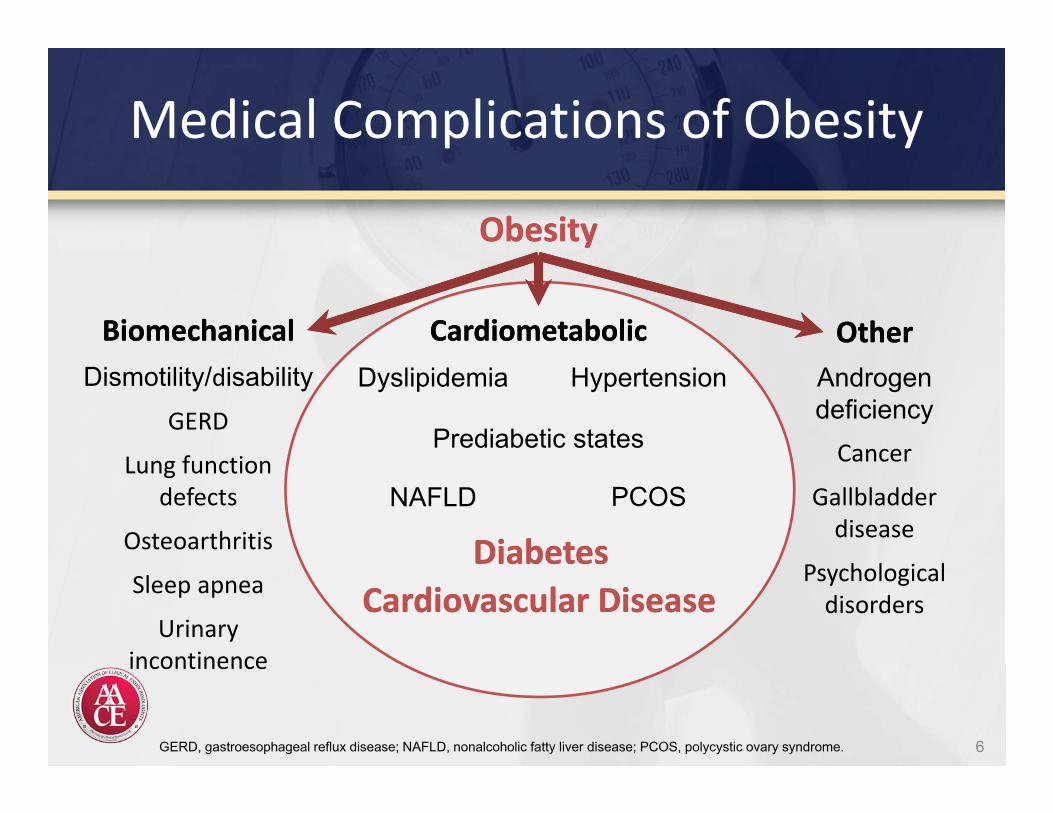
Medical Complications of Obesity
ObesityObesity
NAFLD
Cardiovascular DiseaseCardiovascular Disease
Dismotility/disabilityGERD
Lung functiondefects
Osteoarthritis
Sleep apnea
Urinaryincontinence
Prediabetic states
HypertensionDyslipidemia
PCOS
DiabetesDiabetes
CardiometabolicCardiometabolicBiomechanicalBiomechanical OtherOther
GERD, gastroesophageal reflux disease; NAFLD, nonalcoholic fatty liver disease; PCOS, polycystic ovary syndrome. 6
Androgen deficiencyCancer
Gallbladder disease
Psychologicaldisorders
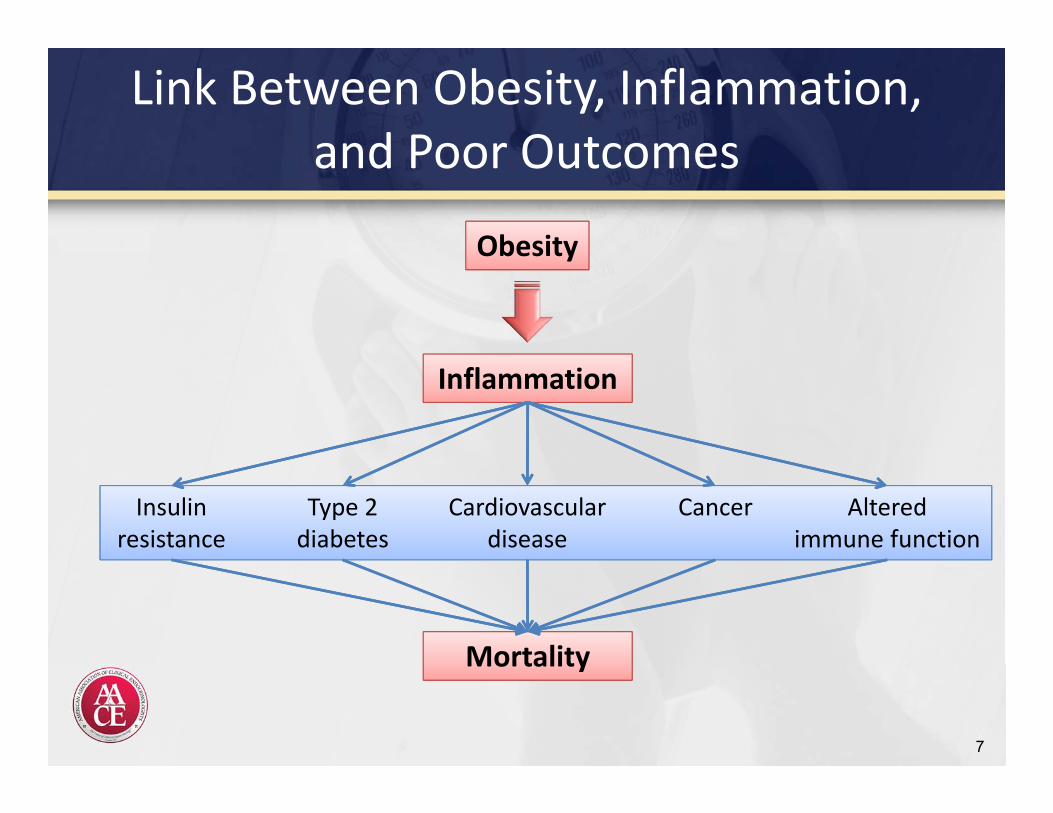
Link Between Obesity, Inflammation, and Poor Outcomes
7
Obesity
Inflammation
Insulin resistance
Type 2 diabetes
Cardiovascular disease
Cancer Alteredimmune function
Mortality
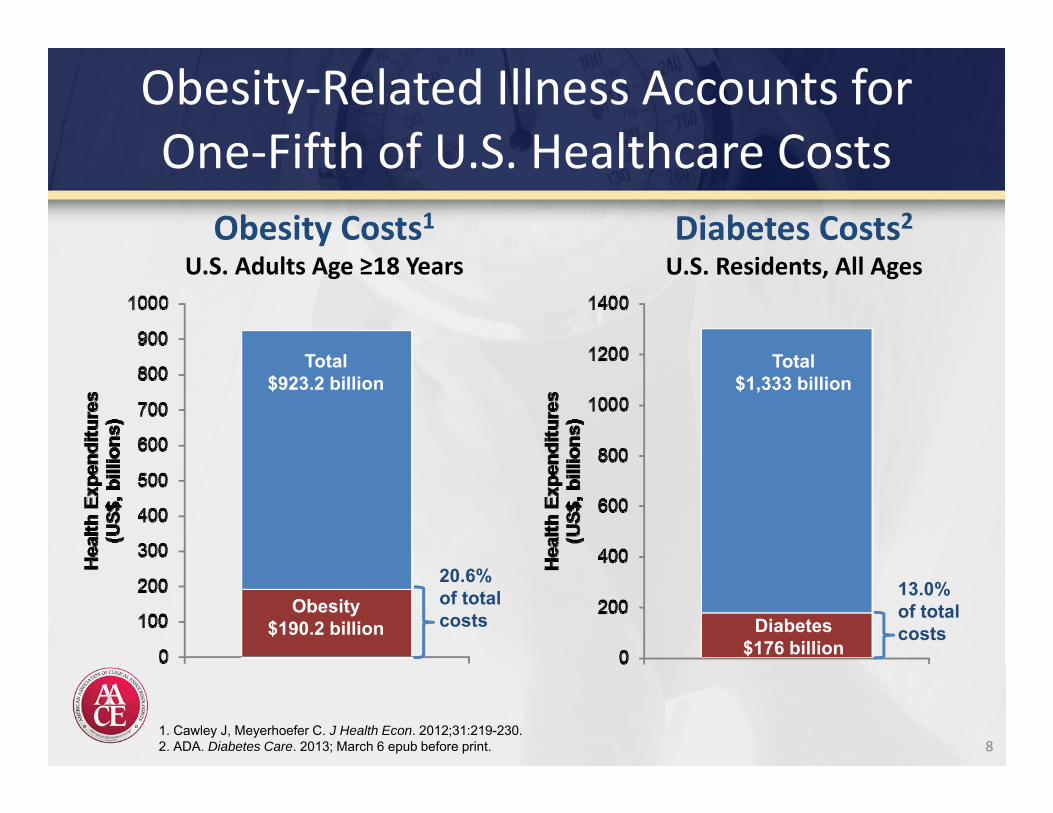
Obesity‐Related Illness Accounts forOne‐Fifth of U.S. Healthcare Costs
8
Total$923.2 billion
Obesity$190.2 billion
20.6% of total costs
1. Cawley J, Meyerhoefer C. J Health Econ. 2012;31:219-230.2. ADA. Diabetes Care. 2013; March 6 epub before print.
Obesity Costs1U.S. Adults Age ≥18 Years
Total$1,333 billion
Diabetes$176 billion
13.0% of total costs
Diabetes Costs2U.S. Residents, All Ages
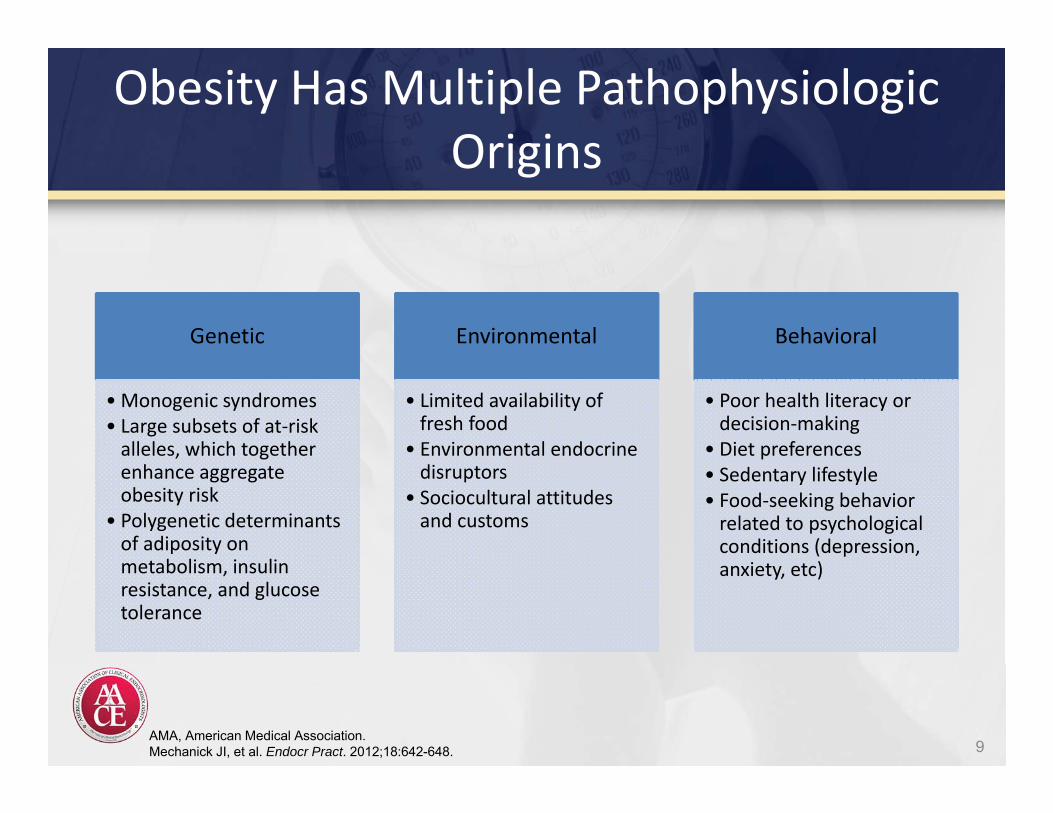
Obesity Has Multiple Pathophysiologic Origins
9
Genetic
• Monogenic syndromes• Large subsets of at‐risk alleles, which together enhance aggregate obesity risk
• Polygenetic determinants of adiposity on metabolism, insulin resistance, and glucose tolerance
Environmental
• Limited availability of fresh food
• Environmental endocrine disruptors
• Sociocultural attitudes and customs
Behavioral
• Poor health literacy or decision‐making
• Diet preferences• Sedentary lifestyle• Food‐seeking behavior related to psychological conditions (depression, anxiety, etc)
AMA, American Medical Association.Mechanick JI, et al. Endocr Pract. 2012;18:642-648.
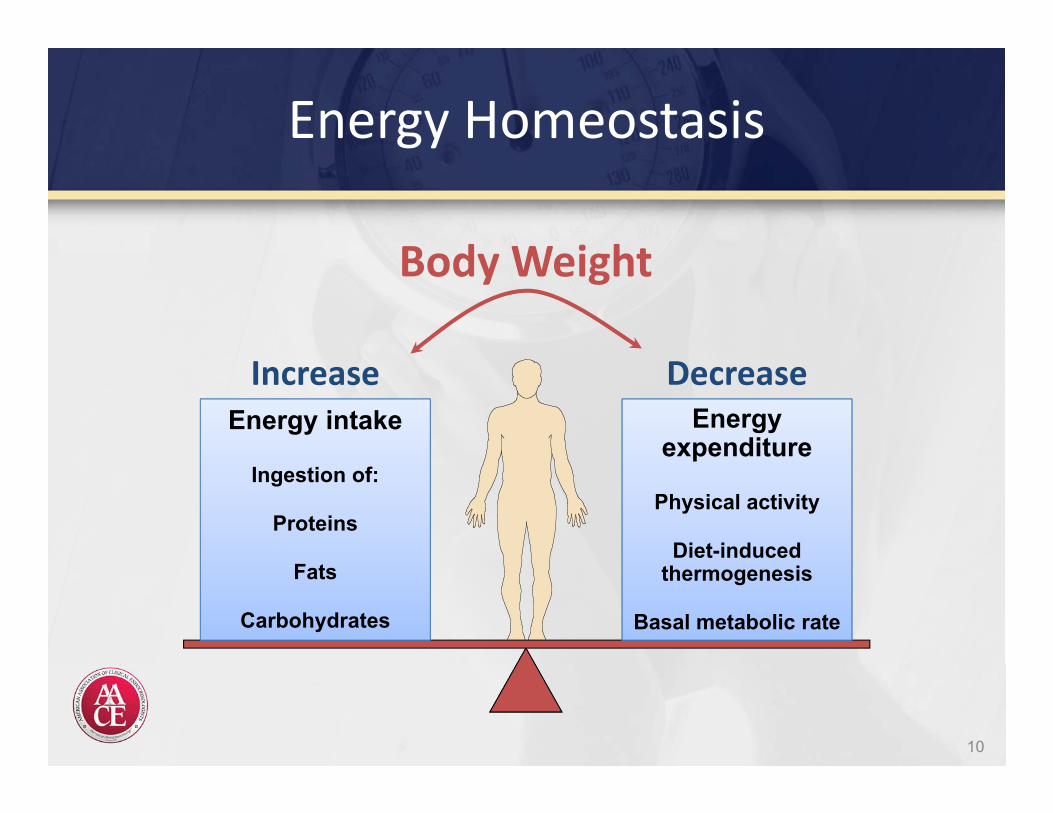
Energy intake
Ingestion of:
Proteins
Fats
Carbohydrates
Energy expenditure
Physical activity
Diet-induced thermogenesis
Basal metabolic rate
Body Weight
Increase
Energy Homeostasis
10
Decrease
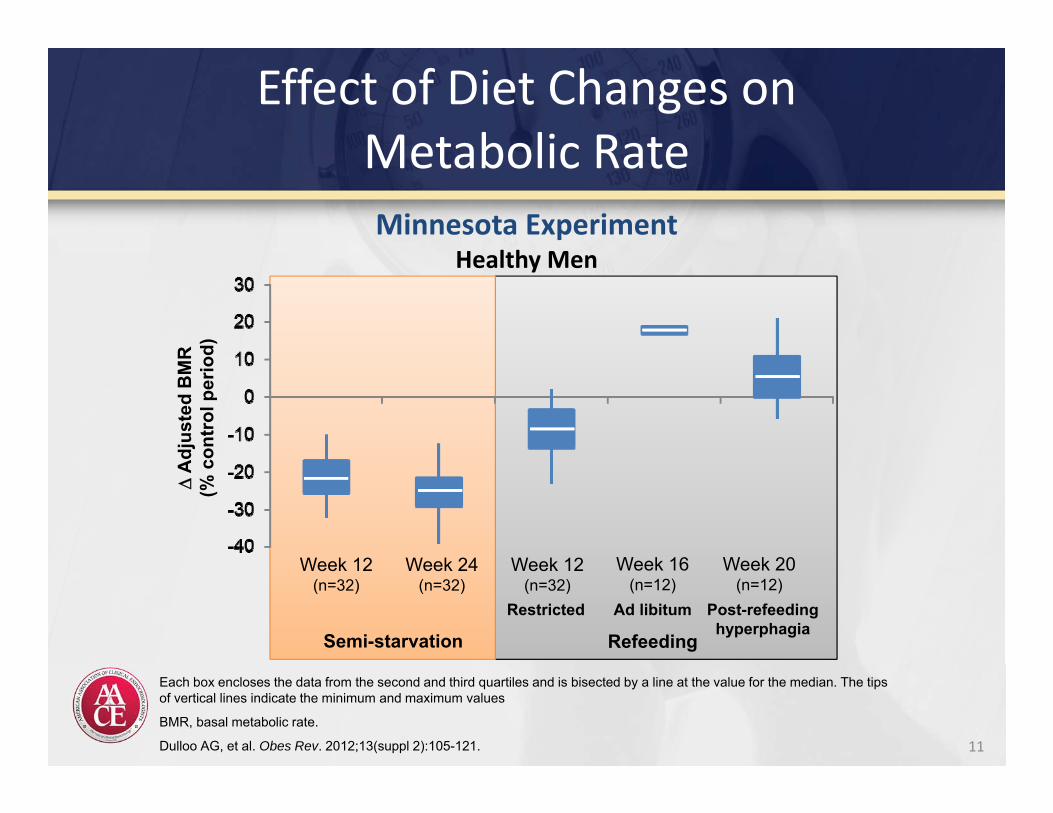
Effect of Diet Changes onMetabolic Rate
11
Each box encloses the data from the second and third quartiles and is bisected by a line at the value for the median. The tips of vertical lines indicate the minimum and maximum values
BMR, basal metabolic rate.
Dulloo AG, et al. Obes Rev. 2012;13(suppl 2):105-121.
Minnesota ExperimentHealthy Men
Week 12(n=32)
Week 24(n=32)
Week 12(n=32)
Week 16(n=12)
Week 20(n=12)
Semi-starvation RefeedingRestricted Ad libitum Post-refeeding
hyperphagia
A
djus
ted
BM
R(%
con
trol
per
iod)
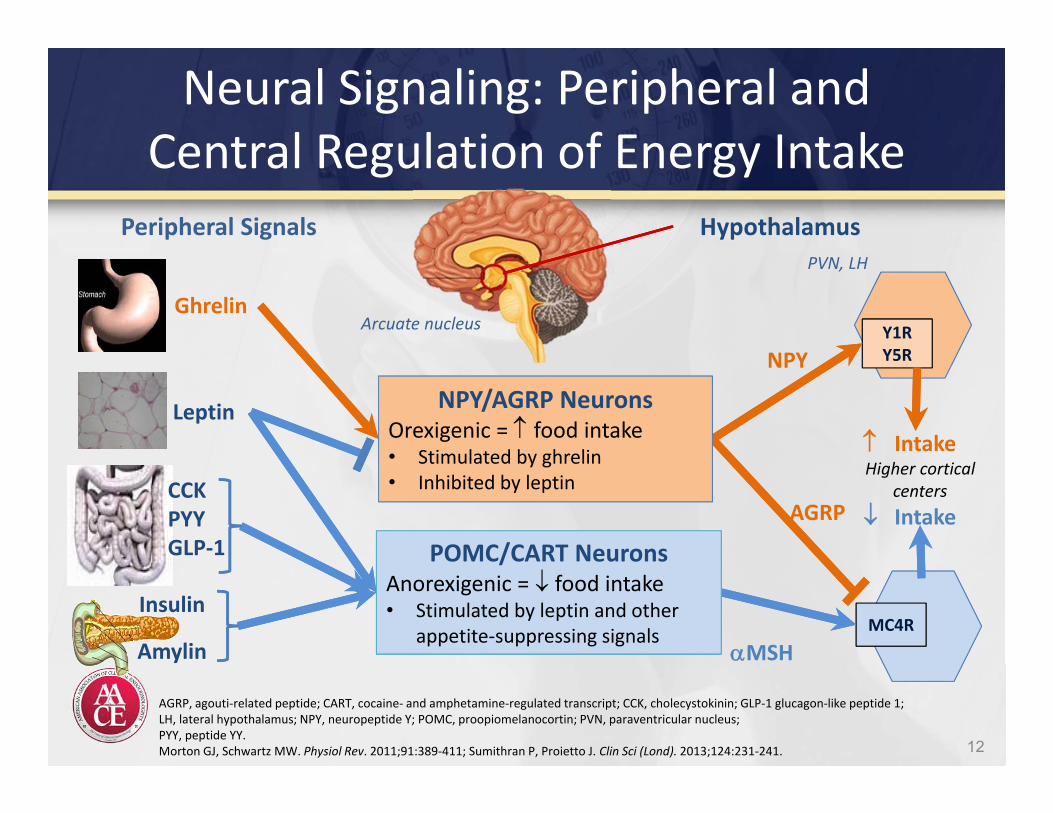
Neural Signaling: Peripheral and Central Regulation of Energy Intake
12
AGRP, agouti‐related peptide; CART, cocaine‐ and amphetamine‐regulated transcript; CCK, cholecystokinin; GLP‐1 glucagon‐like peptide 1; LH, lateral hypothalamus; NPY, neuropeptide Y; POMC, proopiomelanocortin; PVN, paraventricular nucleus;PYY, peptide YY.Morton GJ, Schwartz MW. Physiol Rev. 2011;91:389‐411; Sumithran P, Proietto J. Clin Sci (Lond). 2013;124:231‐241.
Hypothalamus
Ghrelin
CCKPYYGLP‐1
Leptin
Insulin
Amylin
Peripheral Signals
Arcuate nucleus Y1RY5R
MC4R
MSH
AGRP
NPY
PVN, LH
IntakeHigher cortical
centers Intake
POMC/CART NeuronsAnorexigenic = food intake• Stimulated by leptin and other
appetite‐suppressing signals
NPY/AGRP NeuronsOrexigenic = food intake• Stimulated by ghrelin• Inhibited by leptin
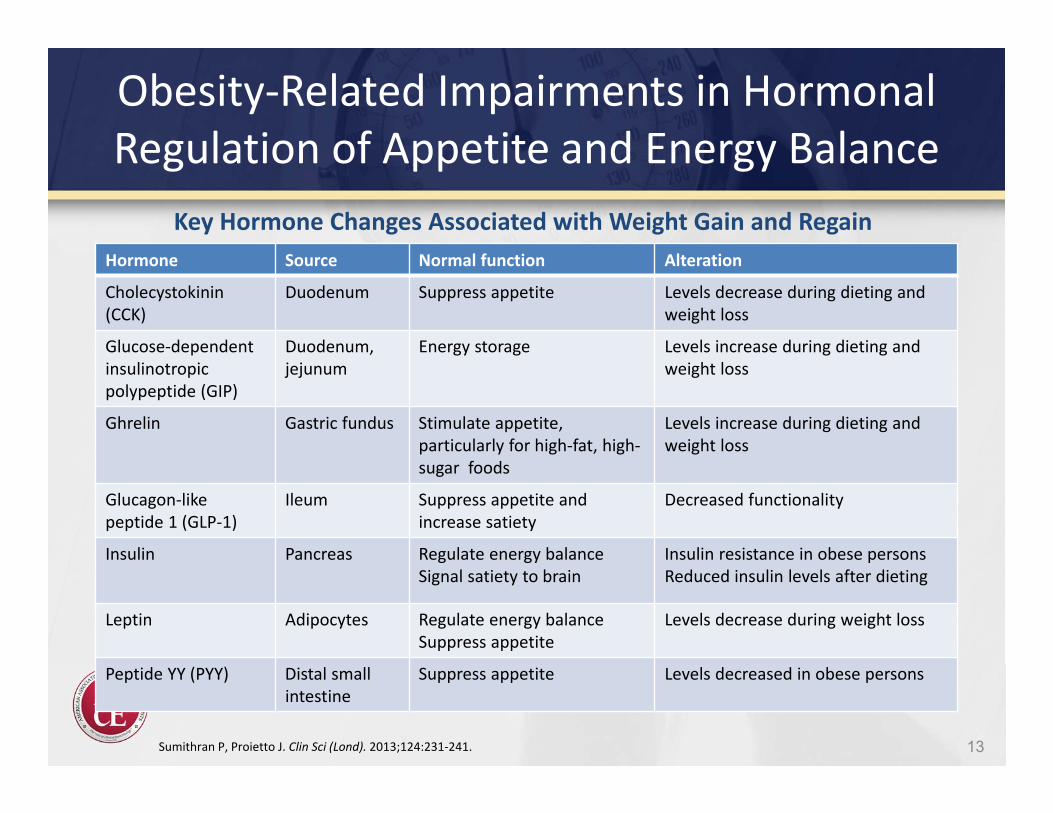
Obesity‐Related Impairments in Hormonal Regulation of Appetite and Energy Balance
Hormone Source Normal function Alteration
Cholecystokinin (CCK)
Duodenum Suppress appetite Levels decrease during dieting and weight loss
Glucose‐dependent insulinotropic polypeptide (GIP)
Duodenum, jejunum
Energy storage Levels increase during dieting and weight loss
Ghrelin Gastric fundus Stimulate appetite, particularly for high‐fat, high‐sugar foods
Levels increase during dieting and weight loss
Glucagon‐like peptide 1 (GLP‐1)
Ileum Suppress appetite and increase satiety
Decreased functionality
Insulin Pancreas Regulate energy balanceSignal satiety to brain
Insulin resistance in obese personsReduced insulin levels after dieting
Leptin Adipocytes Regulate energy balanceSuppress appetite
Levels decrease during weight loss
Peptide YY (PYY) Distal small intestine
Suppress appetite Levels decreased in obese persons
13Sumithran P, Proietto J. Clin Sci (Lond). 2013;124:231‐241.
Key Hormone Changes Associated with Weight Gain and Regain
Assessing Obesity in Clinical Practice
Body Mass Index• PQRI measure
– Overweight: ≥25 to <30 kg/m2
– Obese: ≥30 kg/m2
• Calculated by dividing weight by the square of height (kg/m2)– Free BMI calculator available
from the National Heart, Lung, and Blood Institute
Waist Circumference• Marker of high risk*
– Men >40 inches– Women >35 inches
• Indirect measure of central adiposity, correlated with visceral fat
• Excess abdominal fat is an independent predictor of risk factors and morbidity
14
*WHO waist circumference cutoff varies by race/ethnicity.
NHLBI, National Heart, Lung, and Blood Institute; PQRI, Physician Quality Reporting Initiative; WHO, World Health Organization.
NHLBI. Obesity guidelines. Obesity Res. 1998;6(suppl2):51S‐209S. NHLBI BMI calculator. Available at: http://www.nhlbi.nih.gov/guidelines/obesity/BMI/bmicalc.htm.
Limitations of BMI
Insensitive to small changes in weight Does not distinguish between high weights due to excess body
fat, large muscle mass or edema Does not reveal differences in fat distribution (visceral vs.
subcutaneous) Does not differentiate between men and women Is not accurate when height is compromised (kyphosis, scoliosis) Clinical judgment needed (frail elderly, etc.)
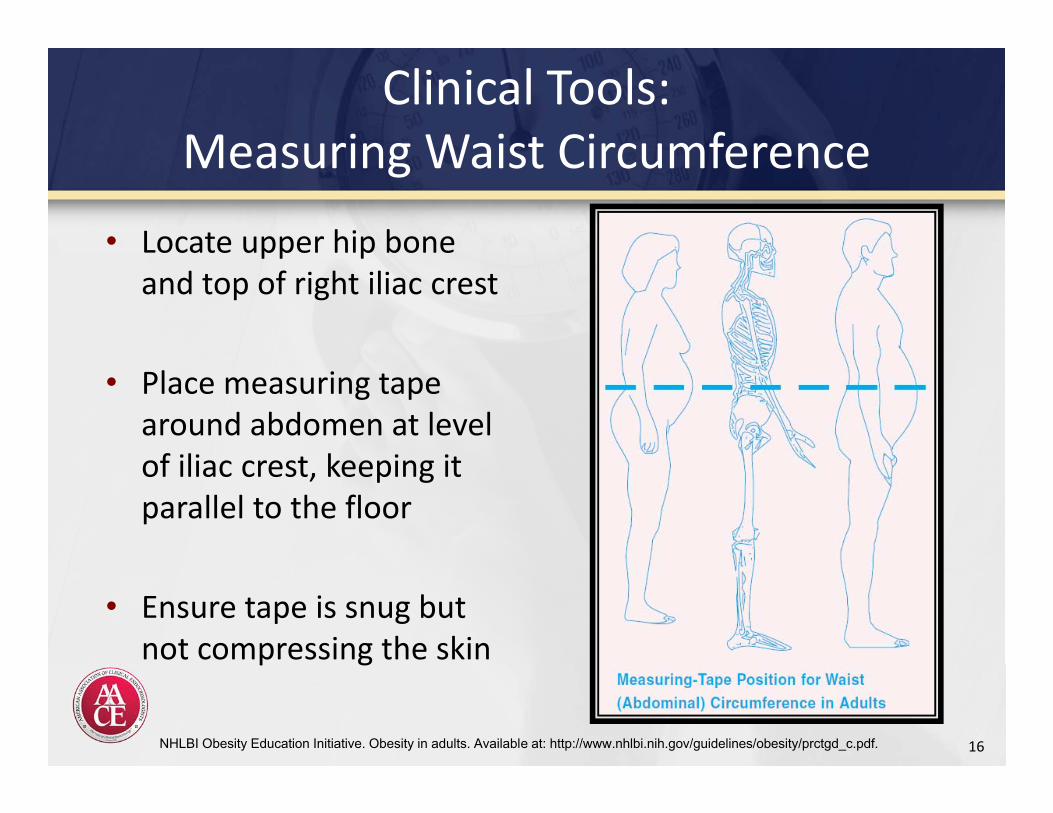
Clinical Tools:Measuring Waist Circumference
• Locate upper hip bone and top of right iliac crest
• Place measuring tape around abdomen at level of iliac crest, keeping it parallel to the floor
• Ensure tape is snug but not compressing the skin
16NHLBI Obesity Education Initiative. Obesity in adults. Available at: http://www.nhlbi.nih.gov/guidelines/obesity/prctgd_c.pdf.
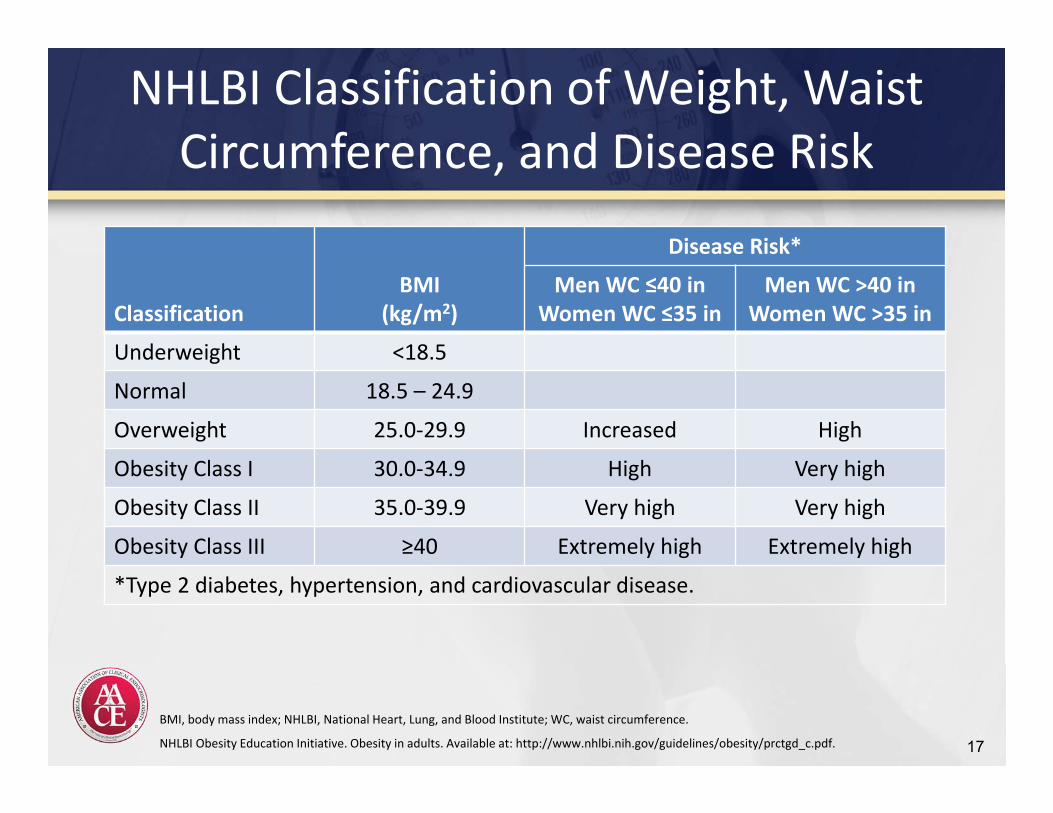
NHLBI Classification of Weight, Waist Circumference, and Disease Risk
ClassificationBMI
(kg/m2)
Disease Risk*
Men WC ≤40 inWomen WC ≤35 in
Men WC >40 inWomen WC >35 in
Underweight <18.5
Normal 18.5 – 24.9
Overweight 25.0‐29.9 Increased High
Obesity Class I 30.0‐34.9 High Very high
Obesity Class II 35.0‐39.9 Very high Very high
Obesity Class III ≥40 Extremely high Extremely high
*Type 2 diabetes, hypertension, and cardiovascular disease.
17
BMI, body mass index; NHLBI, National Heart, Lung, and Blood Institute; WC, waist circumference.
NHLBI Obesity Education Initiative. Obesity in adults. Available at: http://www.nhlbi.nih.gov/guidelines/obesity/prctgd_c.pdf.
Obesity‐Focused History
18
Life Events and Weight Gain• Recap of patient life events that
coincided with weight gain, such as smoking cessation, medication initiation, pregnancy or menopause, job loss, change in marital status, etc
Diet and Activity• Extent of daily physical activity• Sleep habits and difficulties• Food preferences and
frequency/quantity of meals• Psychological assessment
– Mood/anxiety disorders, ADD, PTSD– Eating disorders
A detailed obesity history enables development of tailored treatment
recommendations to address individual patient needs
Weight Loss Readiness• Motivation and social support• Psychiatric status• Presence of stressful life circumstances• Time constraints• Goals and expectations
Kushner RF. Circulation. 2012;126:2870-2877.
Review of Systems• Checklist of obesity‐related
complications
Medical History
Elicit risk factors and symptoms of the manifestations of obesity:
• Dysmetabolic syndrome• Type 2 diabetes• Cardiovascular disease (and angina)• Sleep apnea• Gallstones• Potential Pregnancy
Medical Causes of Obesity
• Hypothyroidism (???YH)• Cushing's syndrome• Depression (Beck’s depression inventory)
Beck AT. The Beck Depression Inventory. San Antonio, TX: The Psychological Corporation; 1987.Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck Inventory: Twenty-five years of evaluation. Clin Psychol Rev. 1988;8:77-100.
Selected Medications That Can Cause Weight Gain
• Psychotropic medications
– Tricyclic antidepressants
– Monoamine oxidase
inhibitors
– Specific SSRIs
– Atypical antipsychotics
– Lithium
– Specific anticonvulsants• -adrenergic receptor blockers
clozapine (Clozaril) 4.4 kg gain*olanzapine (Zyprexa) 4.2 kg*
risperidone (Resperdal) 2.1 kg*Paxil, Prozac
*Allison DB et al. Am J Psychiatry 1999 Nov;156(11):1686-96
Selected Medications That Can Cause Weight Gain Diabetes medications
– Insulin– Sulfonylureas– Thiazolidinediones
Highly active antiretroviral therapy
Tamoxifen
Steroid hormones– Glucocorticoids– Progestational steroids
Psychiatric History
• Comfort Eating (in response to negative emotions)• Boredom• Sadness and Depression • Anger
• Anorexia• Bulimia• Binge eating • Addictions: Smoking
Exercise History
• Exercise habits• Physical activity patterns• Limitations• Preferences
Family and Social Histories
• Identify support networks and cultural factors – May influence the patient’s ability to participate in a
weight management program• Other household members with obesity
– May impact the ability for the patient to modify his or her lifestyle and diet.
• Dietary changes– Easier to implement if the other members of the family
also adopt healthier nutrition habits.
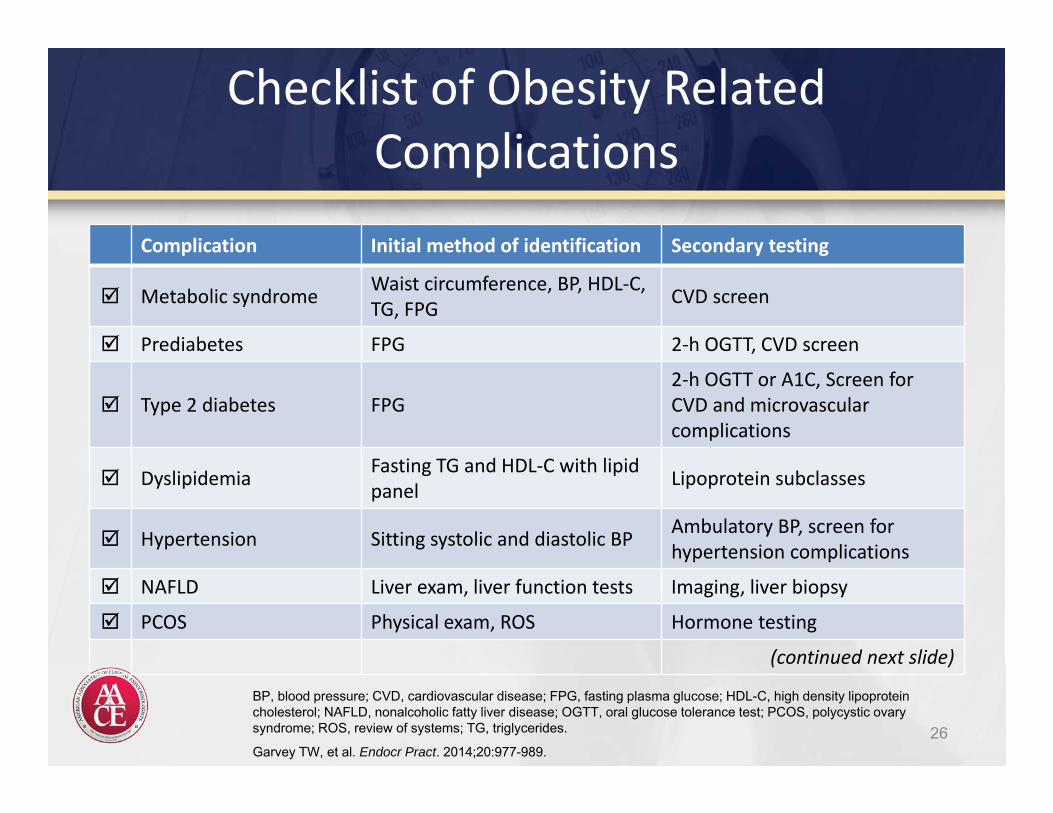
Checklist of Obesity Related Complications
26
Complication Initial method of identification Secondary testing
Metabolic syndrome Waist circumference, BP, HDL‐C, TG, FPG CVD screen
Prediabetes FPG 2‐h OGTT, CVD screen
Type 2 diabetes FPG2‐h OGTT or A1C, Screen for CVD and microvascular complications
Dyslipidemia Fasting TG and HDL‐C with lipidpanel Lipoprotein subclasses
Hypertension Sitting systolic and diastolic BP Ambulatory BP, screen for hypertension complications
NAFLD Liver exam, liver function tests Imaging, liver biopsy
PCOS Physical exam, ROS Hormone testing
(continued next slide)
BP, blood pressure; CVD, cardiovascular disease; FPG, fasting plasma glucose; HDL-C, high density lipoprotein cholesterol; NAFLD, nonalcoholic fatty liver disease; OGTT, oral glucose tolerance test; PCOS, polycystic ovary syndrome; ROS, review of systems; TG, triglycerides.
Garvey TW, et al. Endocr Pract. 2014;20:977-989.
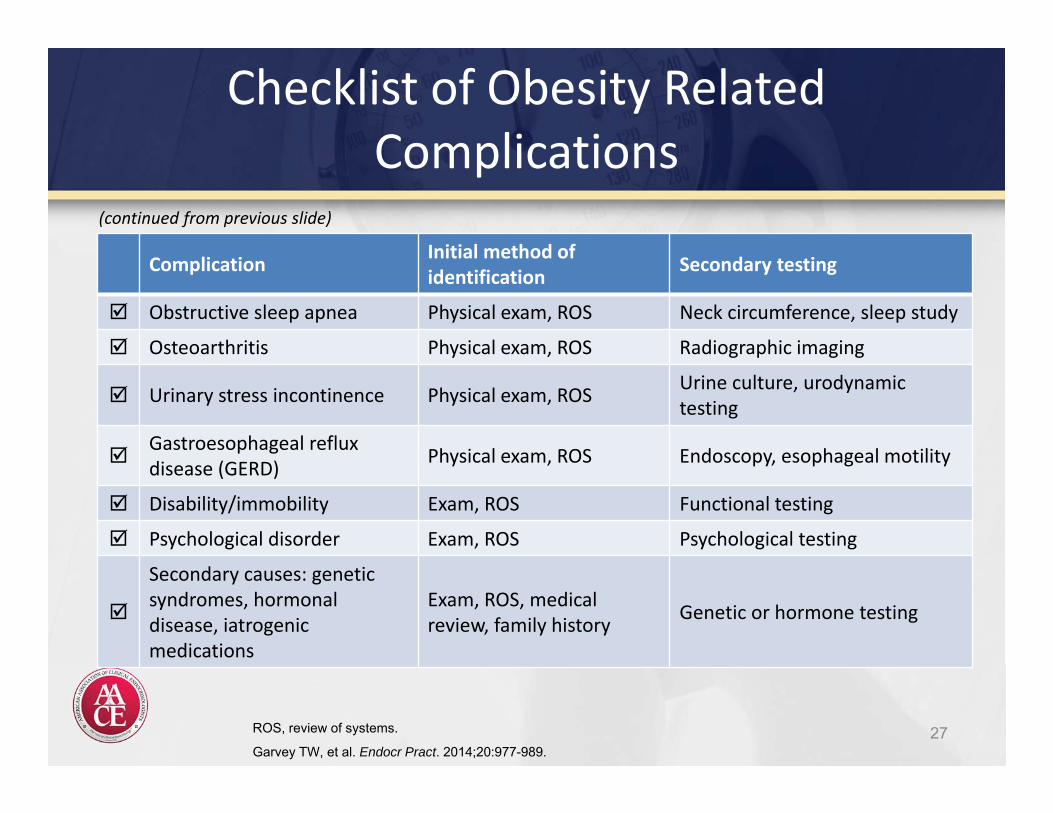
Checklist of Obesity Related Complications
27
(continued from previous slide)
ROS, review of systems.
Garvey TW, et al. Endocr Pract. 2014;20:977-989.
Complication Initial method of identification Secondary testing
Obstructive sleep apnea Physical exam, ROS Neck circumference, sleep study
Osteoarthritis Physical exam, ROS Radiographic imaging
Urinary stress incontinence Physical exam, ROS Urine culture, urodynamic testing
Gastroesophageal reflux disease (GERD) Physical exam, ROS Endoscopy, esophageal motility
Disability/immobility Exam, ROS Functional testing
Psychological disorder Exam, ROS Psychological testing
Secondary causes: genetic syndromes, hormonal disease, iatrogenic medications
Exam, ROS, medicalreview, family history Genetic or hormone testing
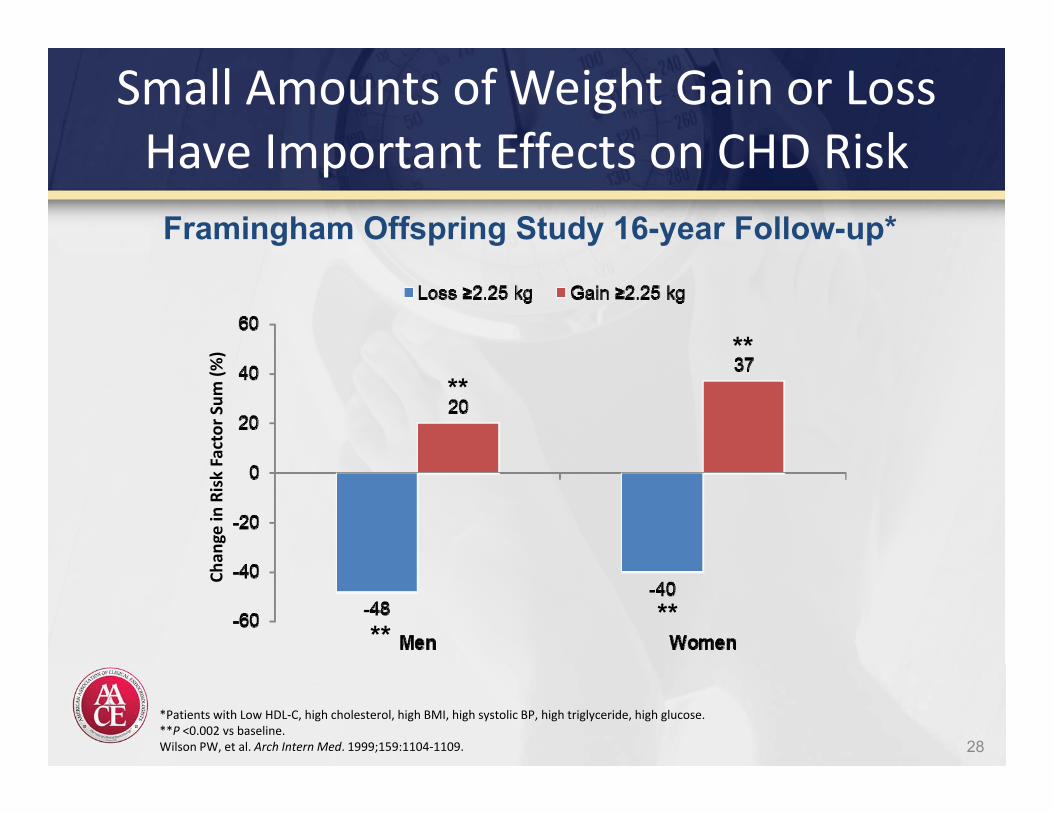
Small Amounts of Weight Gain or Loss Have Important Effects on CHD Risk
28
*Patients with Low HDL‐C, high cholesterol, high BMI, high systolic BP, high triglyceride, high glucose.**P <0.002 vs baseline.Wilson PW, et al. Arch Intern Med. 1999;159:1104‐1109.
Framingham Offspring Study 16-year Follow-up*Ch
ange in
Risk Factor Sum
(%)
****
****
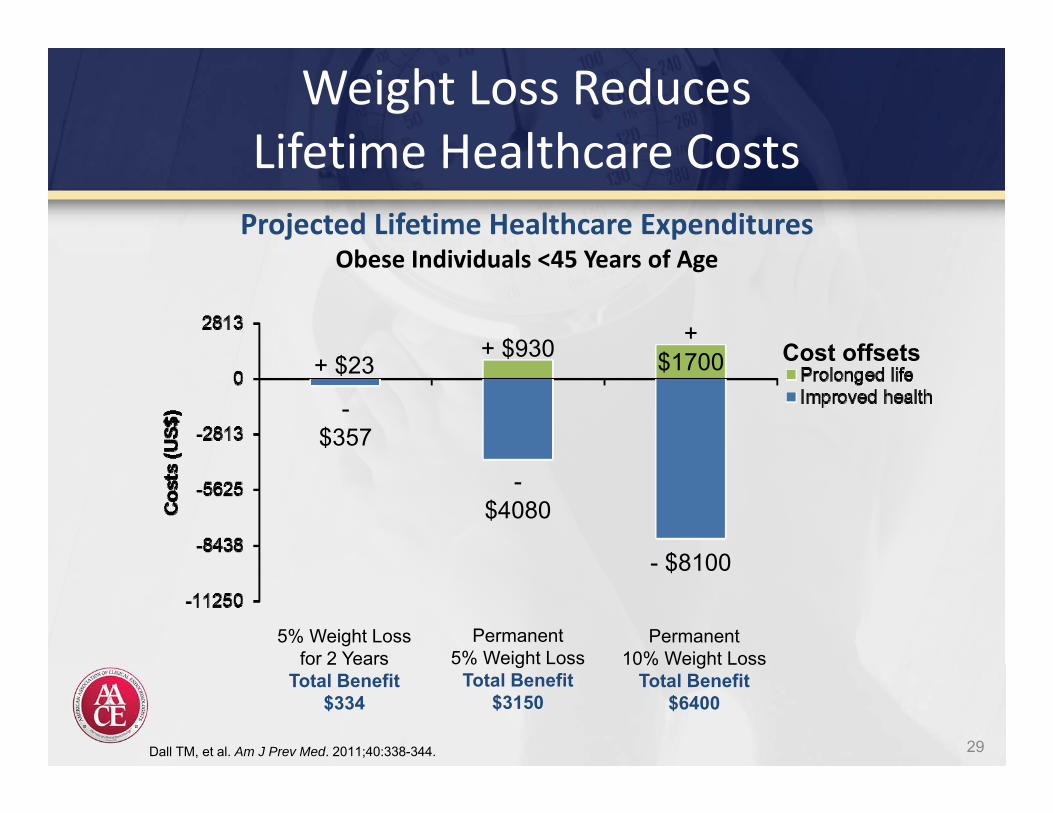
Weight Loss ReducesLifetime Healthcare Costs
29Dall TM, et al. Am J Prev Med. 2011;40:338-344.
Projected Lifetime Healthcare ExpendituresObese Individuals <45 Years of Age
Cost offsets+ $23+ $930 +
$1700
-$357
-$4080
- $8100
5% Weight Lossfor 2 Years
Total Benefit$334
Permanent5% Weight Loss
Total Benefit$3150
Permanent10% Weight Loss
Total Benefit$6400
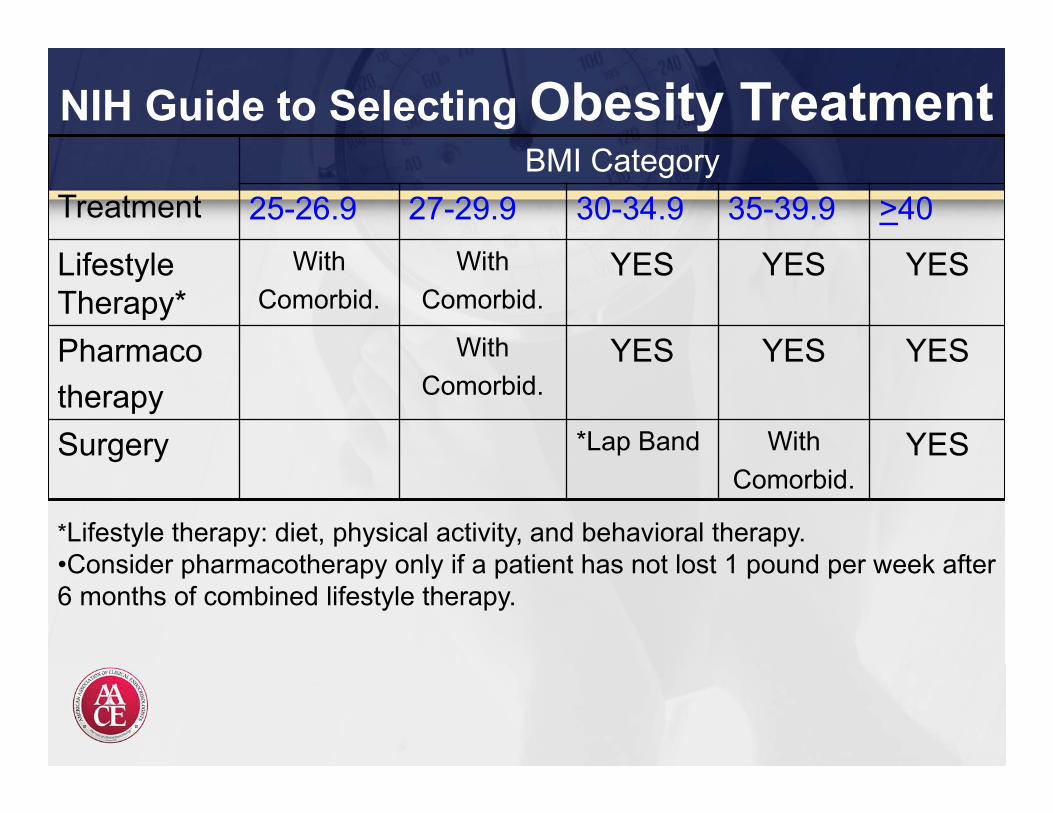
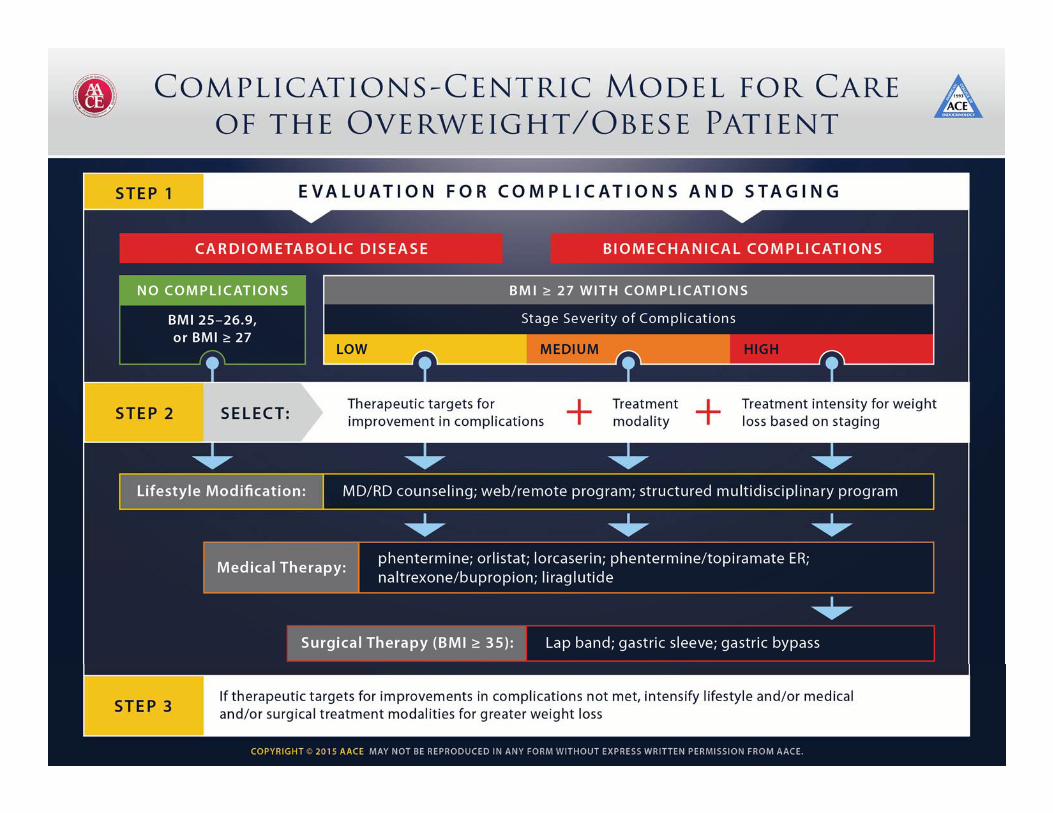
NIH Guide to Selecting Obesity Treatment
TreatmentBMI Category
25-26.9 27-29.9 30-34.9 35-39.9 >40
Lifestyle Therapy*
WithComorbid.
WithComorbid.
YES YES YES
Pharmacotherapy
With Comorbid.
YES YES YES
Surgery *Lap Band WithComorbid.
YES
*Lifestyle therapy: diet, physical activity, and behavioral therapy.•Consider pharmacotherapy only if a patient has not lost 1 pound per week after 6 months of combined lifestyle therapy.
LIFESTYLE IS THE FOUNDATION OF OBESITY MANAGEMENT
Pharmacologic and Surgical Management of Obesity
Components of Therapeutic Lifestyle Change
• Nutrition– Reduced calorie diet– Healthy eating
• Sufficient physical activity• Avoidance of tobacco products• Limited alcohol consumption• Sufficient sleep• Stress reduction (including behavioral therapy as necessary)
33Handelsman Y, et al. Endocr Pract. 2011;17(suppl 2):1-53.
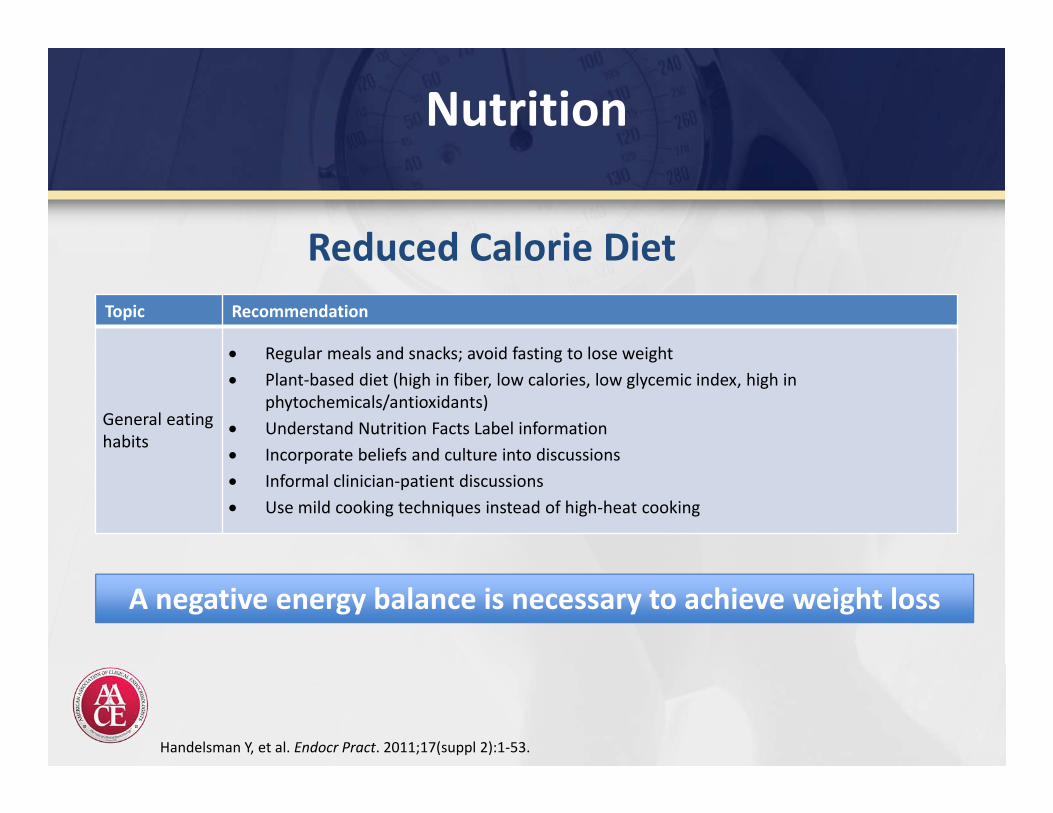
Nutrition
Topic Recommendation
General eating habits
Regular meals and snacks; avoid fasting to lose weight Plant‐based diet (high in fiber, low calories, low glycemic index, high in
phytochemicals/antioxidants) Understand Nutrition Facts Label information Incorporate beliefs and culture into discussions Informal clinician‐patient discussions Use mild cooking techniques instead of high‐heat cooking
Handelsman Y, et al. Endocr Pract. 2011;17(suppl 2):1‐53.
Reduced Calorie Diet
A negative energy balance is necessary to achieve weight loss
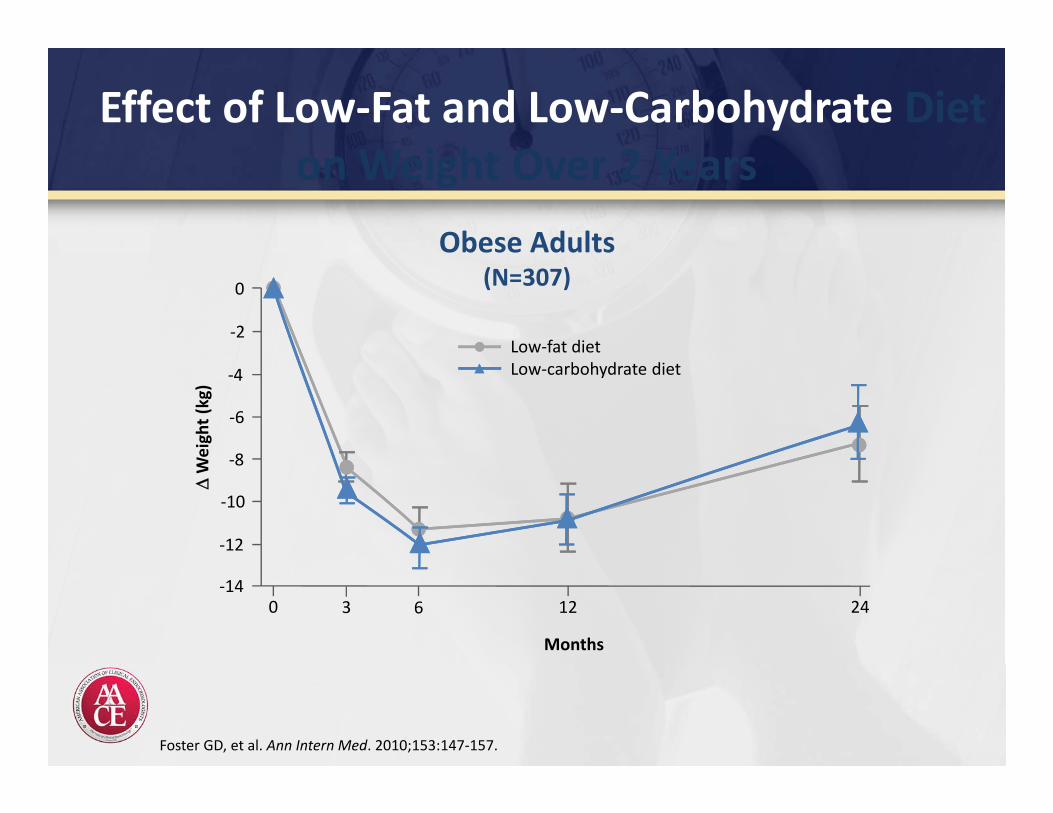
Effect of Low‐Fat and Low‐Carbohydrate Diet on Weight Over 2 Years
Foster GD, et al. Ann Intern Med. 2010;153:147‐157.
Obese Adults(N=307)0
‐8
‐12
‐14
‐10
‐6
0 6 12
Weigh
t (kg)
Months
243
‐4
‐2Low‐fat dietLow‐carbohydrate diet
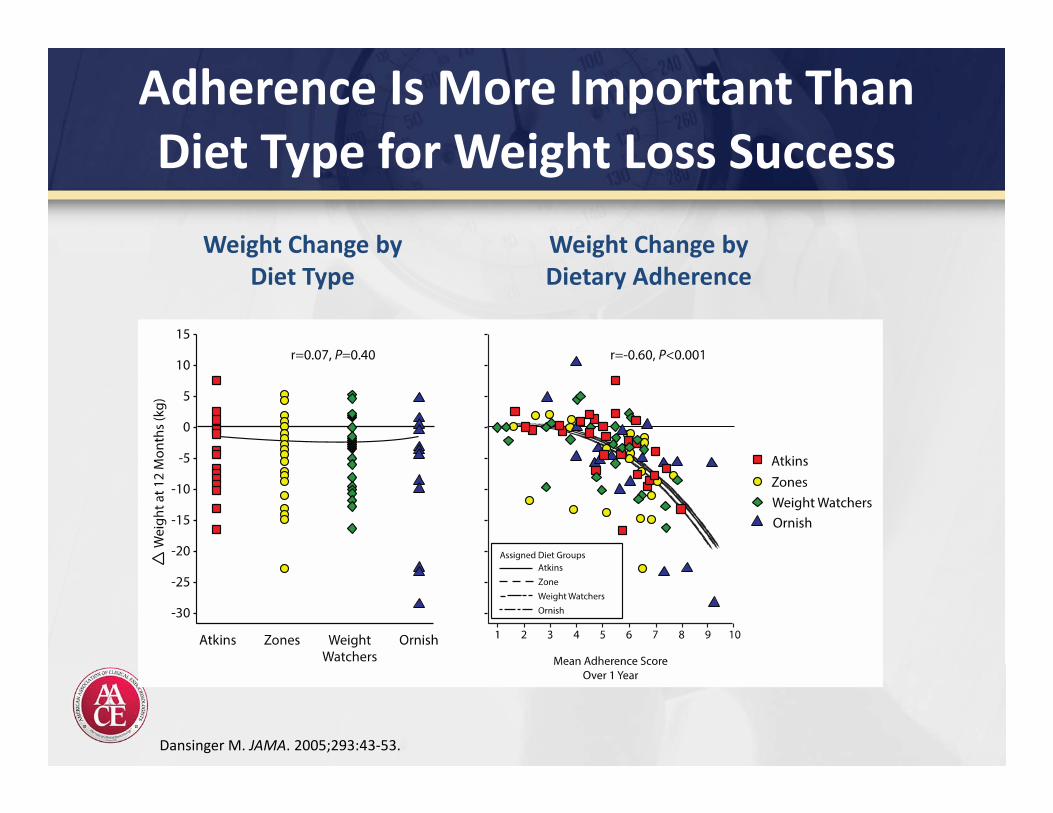
Adherence Is More Important Than Diet Type for Weight Loss Success
Dansinger M. JAMA. 2005;293:43‐53.
Weight Change byDiet Type
Weight Change byDietary Adherence
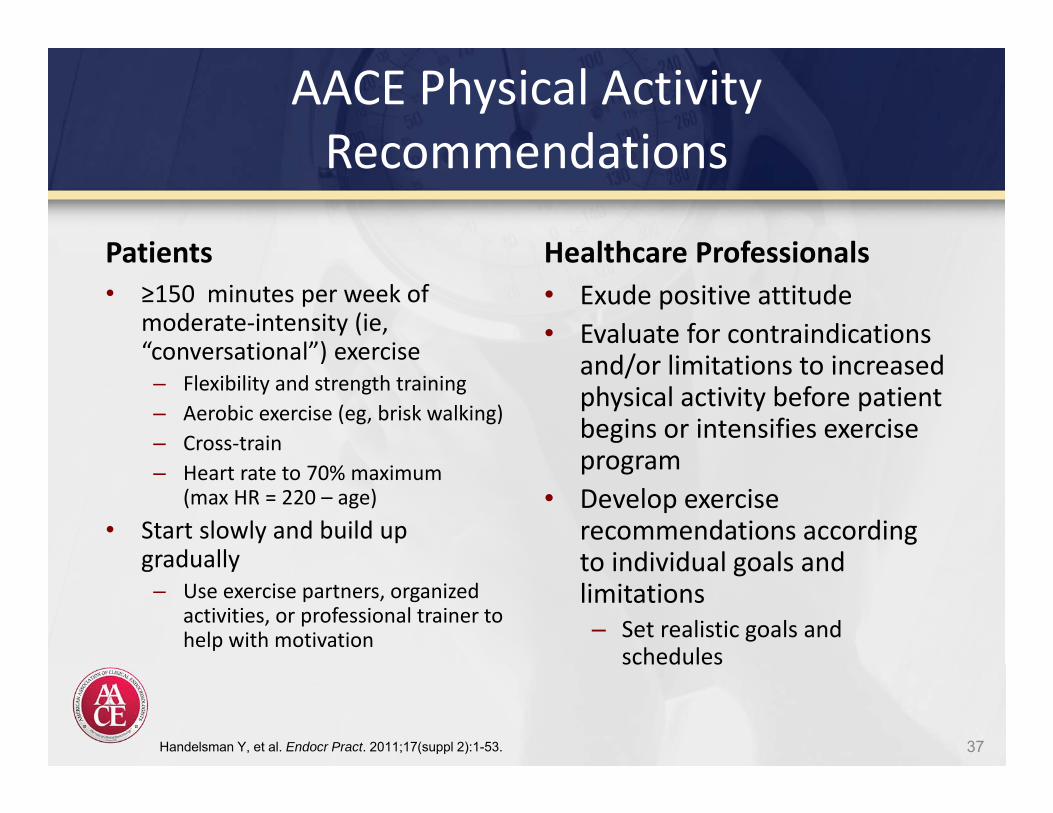
AACE Physical Activity Recommendations
Patients• ≥150 minutes per week of
moderate‐intensity (ie, “conversational”) exercise – Flexibility and strength training– Aerobic exercise (eg, brisk walking)– Cross‐train– Heart rate to 70% maximum
(max HR = 220 – age)• Start slowly and build up
gradually– Use exercise partners, organized
activities, or professional trainer to help with motivation
Healthcare Professionals• Exude positive attitude• Evaluate for contraindications
and/or limitations to increased physical activity before patient begins or intensifies exercise program
• Develop exercise recommendations according to individual goals and limitations– Set realistic goals and
schedules
37Handelsman Y, et al. Endocr Pract. 2011;17(suppl 2):1-53.
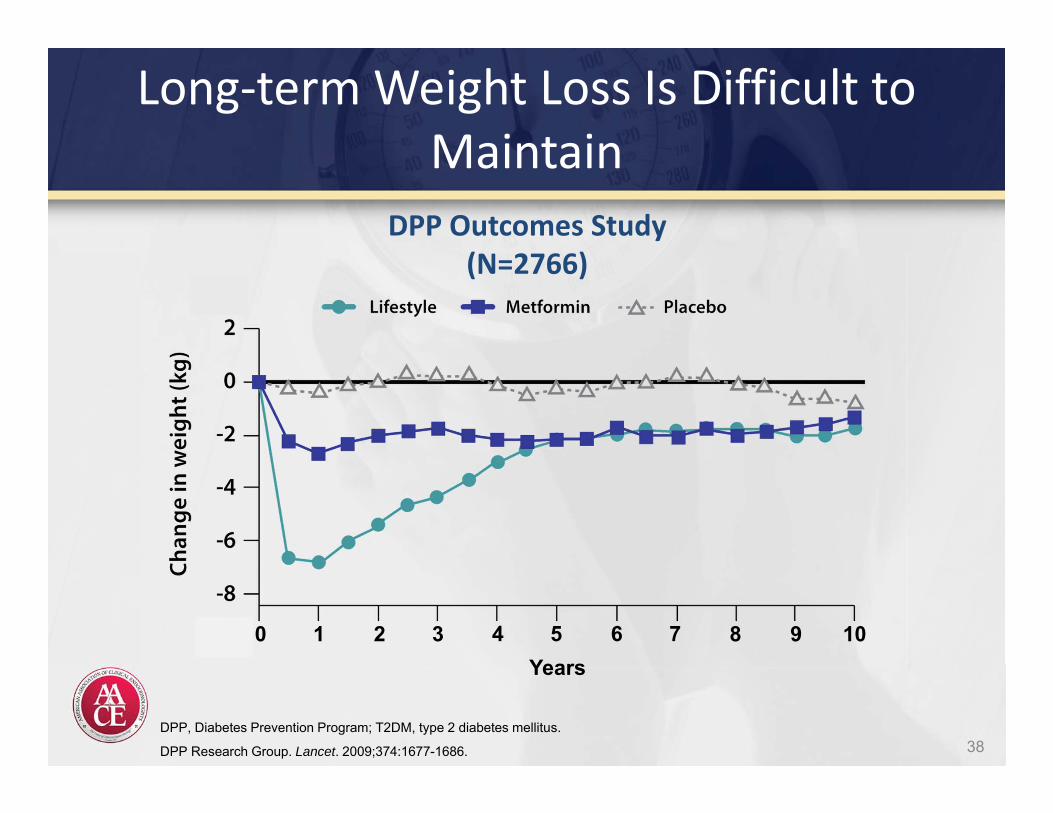
Long‐term Weight Loss Is Difficult to Maintain
38DPP, Diabetes Prevention Program; T2DM, type 2 diabetes mellitus.
DPP Research Group. Lancet. 2009;374:1677-1686.
10 32 54 76 8 109Years
DPP Outcomes Study(N=2766)
PHARMACOTHERAPIESPharmacologic and Surgical Management of Obesity
Lorcaserin
Indications
• Adjunct to diet and exercise in patients with– BMI ≥30 kg/m2
– BMI ≥27 kg/m2 with ≥1 weight‐related comorbidity
• Hypertension• T2DM• Dyslipidemia
• Schedule IV Controlled Substance
Dosing• 10 mg twice daily• Discontinue if 5% weight loss is
not achieved within 12 weeks
DEA, Drug Enforcement Agency.Belviq prescribing information. Woodcliff Lake, NJ: Eisai Inc.; 2012.
See prescribing information for specific instructions
Mechanism of Action
• Specific 5‐HT2C (serotonin) receptor agonist
40
Lorcaserin: Summary of Warnings and Contraindications
Contraindications• Pregnancy
Warnings• Coadministration with other
serotonergic or antidopaminergic agents has not been established
• Valvular heart disease• Cognitive impairment• Psychiatric disorders:
euphoria, dissociation, suicidal thoughts, depression
• Priapism• Increased risk of hypoglycemia
with antidiabetic medications
Belviq prescribing information. Woodcliff Lake, NJ: Eisai Inc.; 2012.
• Headache• Dizziness• Nausea
Adverse Effects
41
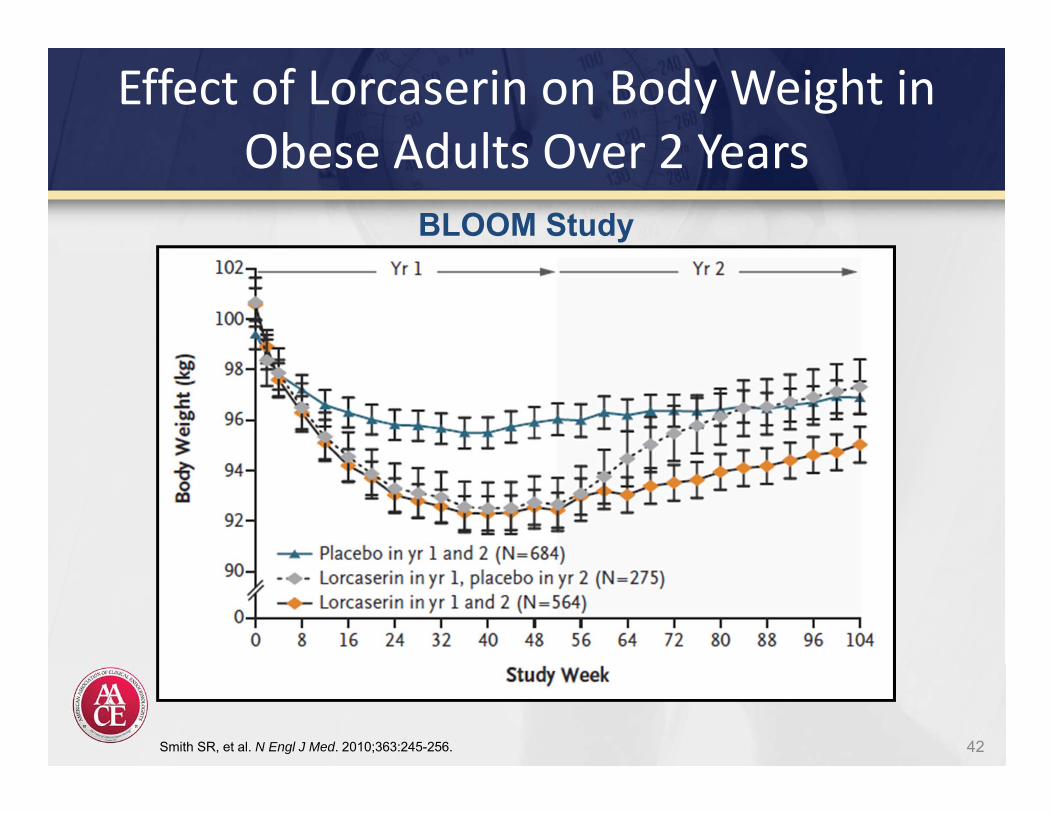
42
Effect of Lorcaserin on Body Weight in Obese Adults Over 2 Years
Smith SR, et al. N Engl J Med. 2010;363:245-256.
BLOOM Study
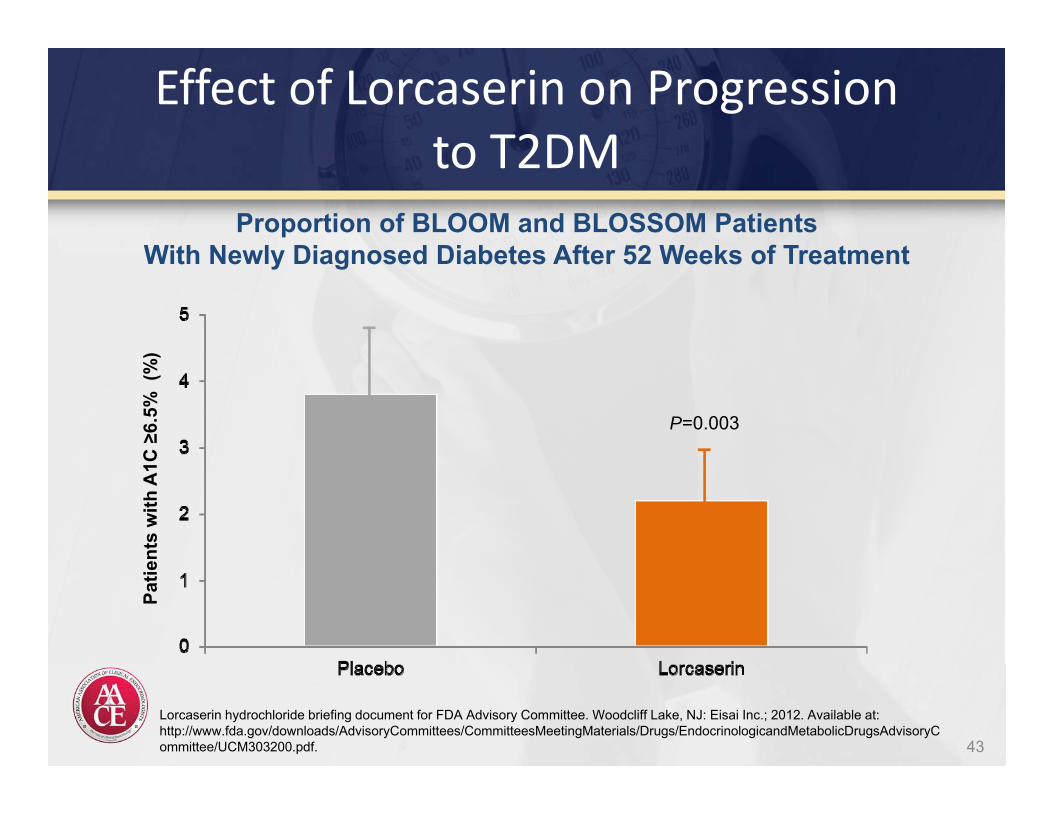
Effect of Lorcaserin on Progressionto T2DM
43
P=0.003
Patie
nts
with
A1C
≥6.
5% (
%)
Proportion of BLOOM and BLOSSOM PatientsWith Newly Diagnosed Diabetes After 52 Weeks of Treatment
Lorcaserin hydrochloride briefing document for FDA Advisory Committee. Woodcliff Lake, NJ: Eisai Inc.; 2012. Available at: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM303200.pdf.
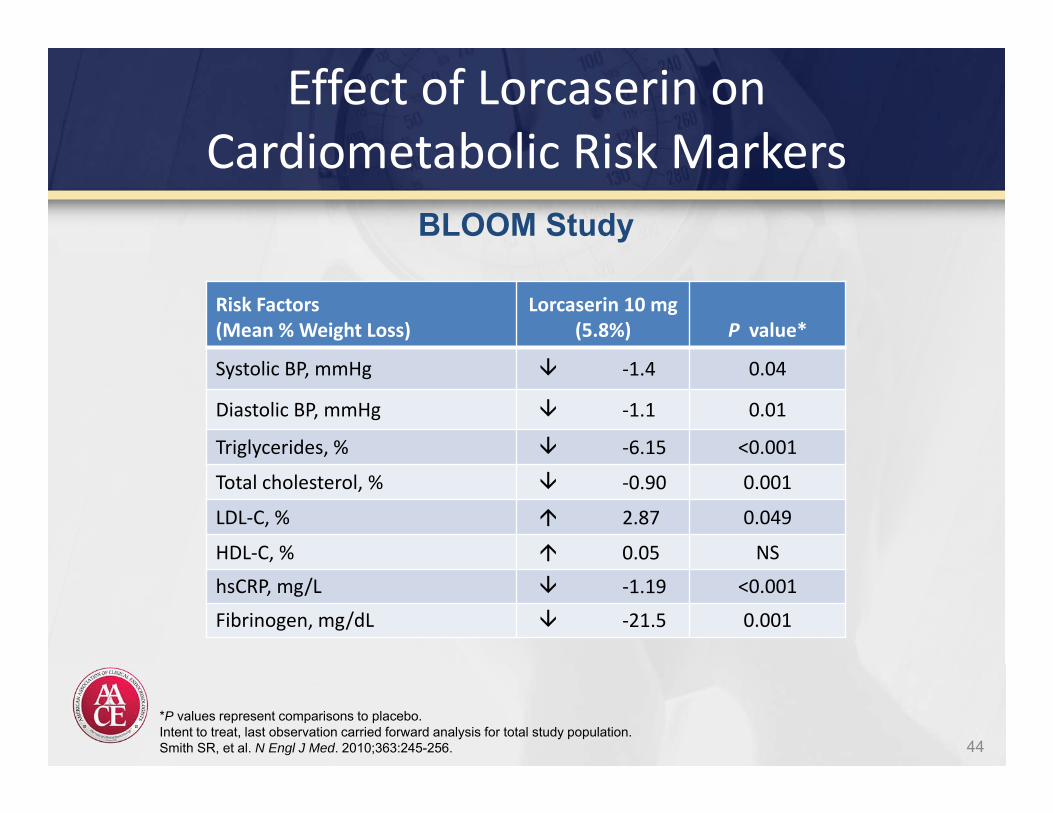
Effect of Lorcaserin on Cardiometabolic Risk Markers
Risk Factors(Mean % Weight Loss)
Lorcaserin 10 mg(5.8%) P value*
Systolic BP, mmHg ‐1.4 0.04
Diastolic BP, mmHg ‐1.1 0.01
Triglycerides, % ‐6.15 <0.001
Total cholesterol, % ‐0.90 0.001
LDL‐C, % 2.87 0.049
HDL‐C, % 0.05 NS
hsCRP, mg/L ‐1.19 <0.001
Fibrinogen, mg/dL ‐21.5 0.001
*P values represent comparisons to placebo.Intent to treat, last observation carried forward analysis for total study population.Smith SR, et al. N Engl J Med. 2010;363:245-256.
BLOOM Study
44
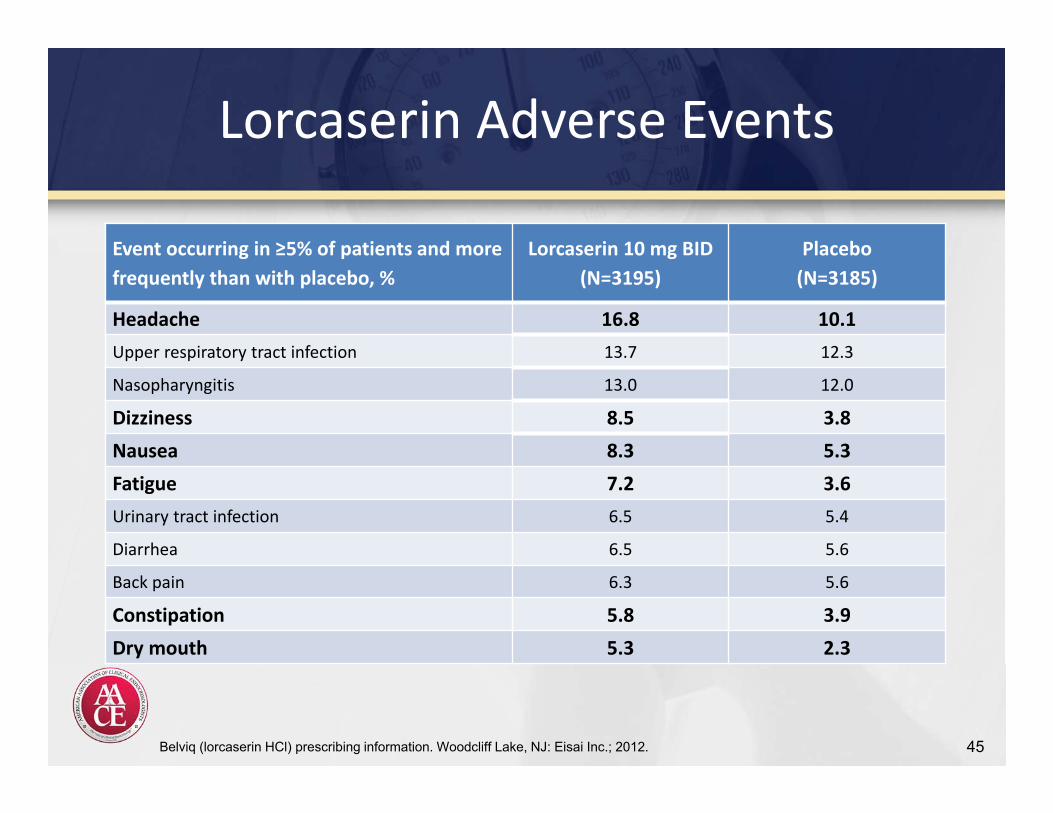
Lorcaserin Adverse Events
Event occurring in ≥5% of patients and more frequently than with placebo, %
Lorcaserin 10 mg BID(N=3195)
Placebo(N=3185)
Headache 16.8 10.1Upper respiratory tract infection 13.7 12.3
Nasopharyngitis 13.0 12.0
Dizziness 8.5 3.8Nausea 8.3 5.3Fatigue 7.2 3.6Urinary tract infection 6.5 5.4
Diarrhea 6.5 5.6
Back pain 6.3 5.6
Constipation 5.8 3.9Dry mouth 5.3 2.3
Belviq (lorcaserin HCl) prescribing information. Woodcliff Lake, NJ: Eisai Inc.; 2012. 45
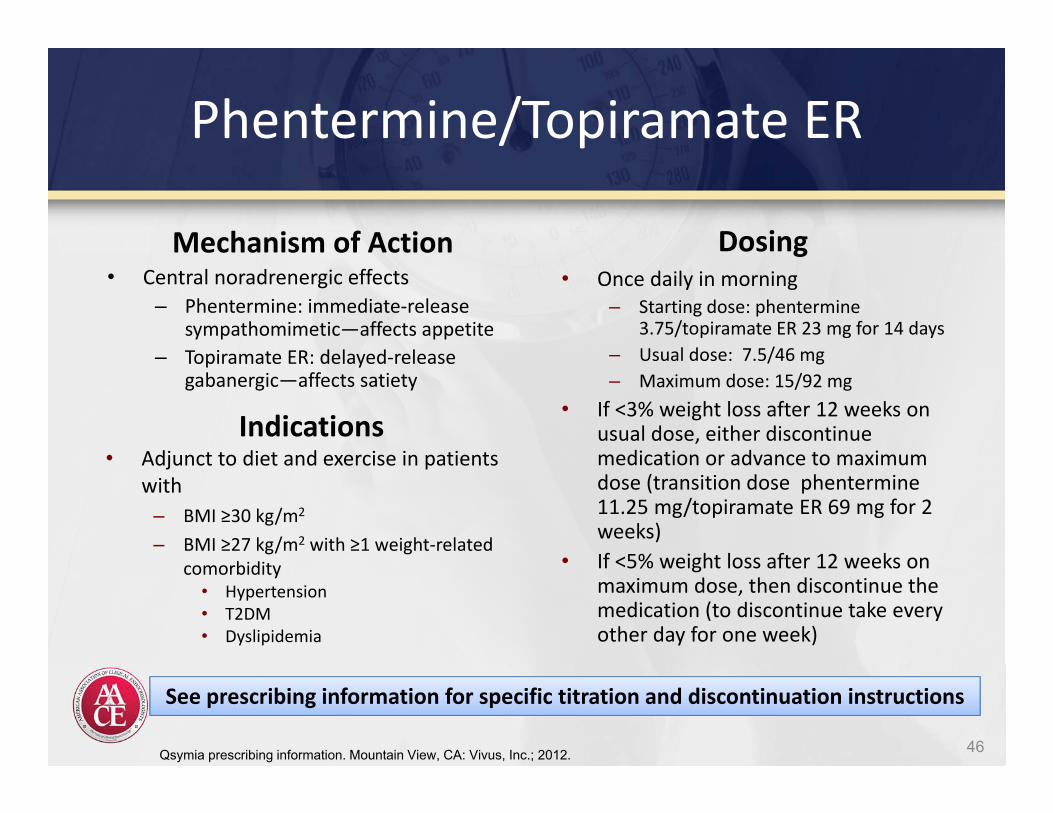
Phentermine/Topiramate ER
Indications• Adjunct to diet and exercise in patients
with– BMI ≥30 kg/m2
– BMI ≥27 kg/m2 with ≥1 weight‐related comorbidity
• Hypertension• T2DM• Dyslipidemia
Dosing• Once daily in morning
– Starting dose: phentermine 3.75/topiramate ER 23 mg for 14 days
– Usual dose: 7.5/46 mg– Maximum dose: 15/92 mg
• If <3% weight loss after 12 weeks on usual dose, either discontinue medication or advance to maximum dose (transition dose phentermine 11.25 mg/topiramate ER 69 mg for 2 weeks)
• If <5% weight loss after 12 weeks on maximum dose, then discontinue the medication (to discontinue take every other day for one week)
Qsymia prescribing information. Mountain View, CA: Vivus, Inc.; 2012.
See prescribing information for specific titration and discontinuation instructions
Mechanism of Action• Central noradrenergic effects
– Phentermine: immediate‐release sympathomimetic—affects appetite
– Topiramate ER: delayed‐release gabanergic—affects satiety
46
Phentermine/Topiramate ER: Summary of Warnings and Contraindications
Contraindications• Pregnancy• Glaucoma• Hyperthyroidism• Treatment with monoamine
oxidase inhibitors (MAOIs)
Warnings• Fetal toxicity• Increased heart rate• Suicide and mood and sleep
disorders• Acute myopia and glaucoma• Metabolic acidosis• Creatinine elevations• Hypoglycemia with concomitant
antidiabetic therapy
Qsymia prescribing information. Mountain View, CA: Vivus, Inc.; 2012.
• Dry mouth• Tingling• Constipation• Altered taste sensation• Upper respiratory infection
Adverse Effects
47
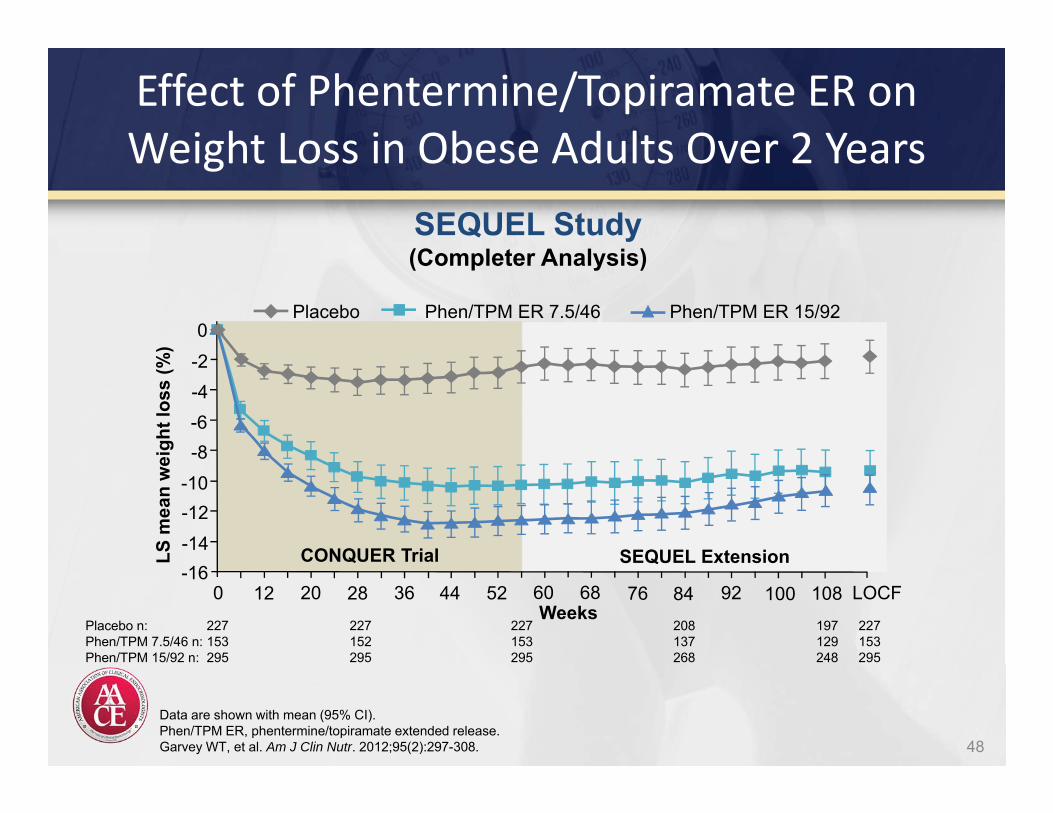
SEQUEL ExtensionSEQUEL ExtensionCONQUER TrialCONQUER Trial
Effect of Phentermine/Topiramate ER on Weight Loss in Obese Adults Over 2 Years
Data are shown with mean (95% CI).Phen/TPM ER, phentermine/topiramate extended release.Garvey WT, et al. Am J Clin Nutr. 2012;95(2):297-308.
SEQUEL Study(Completer Analysis)
Placebo Phen/TPM ER 7.5/46 Phen/TPM ER 15/92
LS m
ean
wei
ght l
oss
(%)
-2-4-6-8
-10-12-14-16
0 12 20 92
0
Weeks28 36 44 52 60 68 76 84 100 108 LOCF
Placebo n: 227 227 227 208 197 227Phen/TPM 7.5/46 n: 153 152 153 137 129 153Phen/TPM 15/92 n: 295 295 295 268 248 295
48
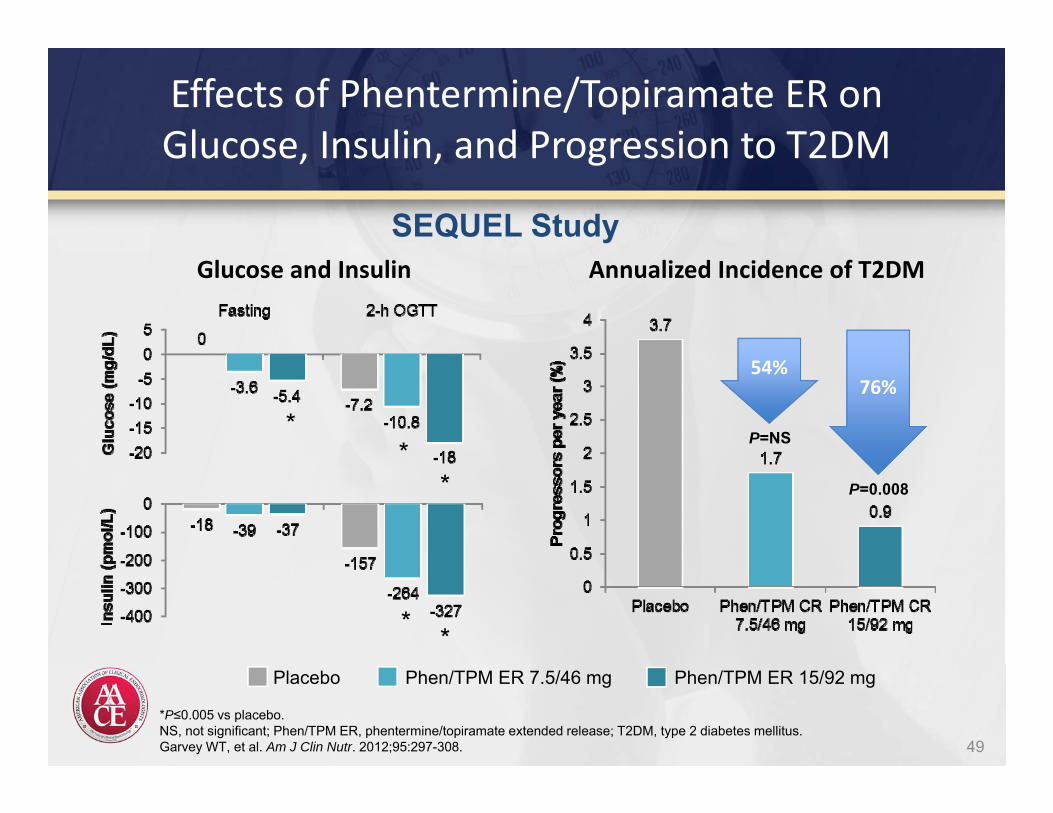
Effects of Phentermine/Topiramate ER on Glucose, Insulin, and Progression to T2DM
Glucose and Insulin
*P≤0.005 vs placebo.NS, not significant; Phen/TPM ER, phentermine/topiramate extended release; T2DM, type 2 diabetes mellitus.Garvey WT, et al. Am J Clin Nutr. 2012;95:297-308.
**
* *
*
Placebo Phen/TPM ER 7.5/46 mg Phen/TPM ER 15/92 mg
SEQUEL StudyAnnualized Incidence of T2DM
P=0.008
76%
P=NS
54%
49
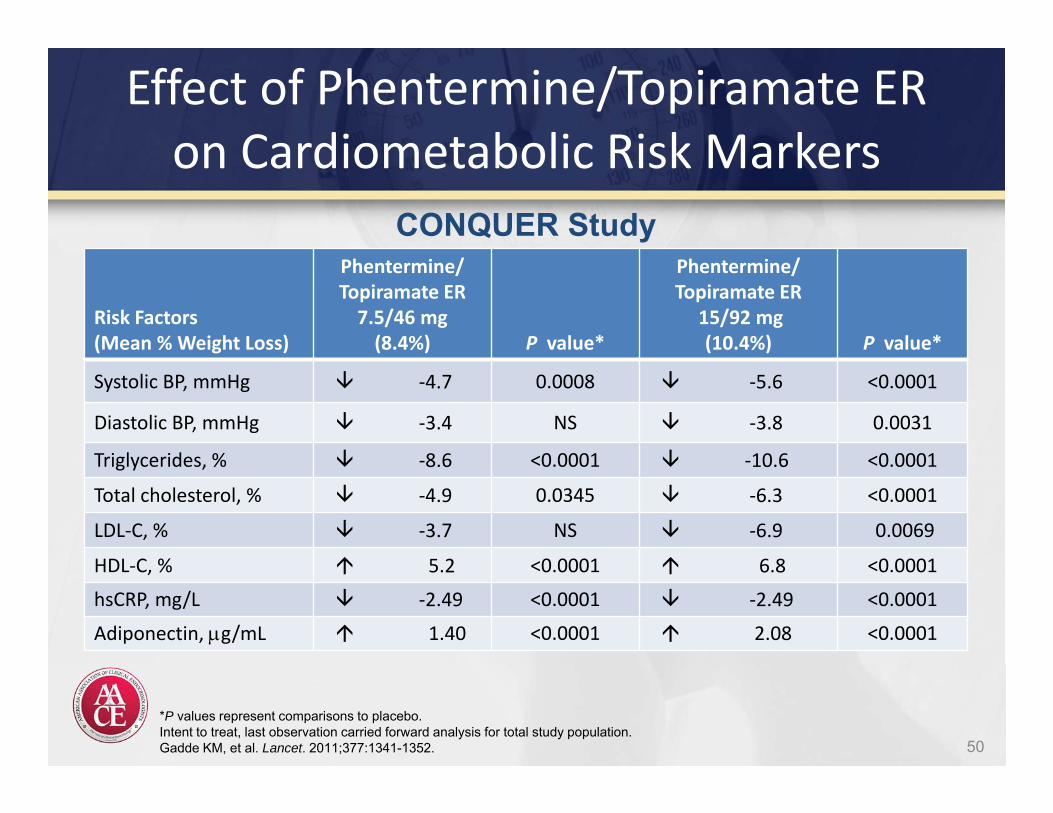
Effect of Phentermine/Topiramate ER on Cardiometabolic Risk Markers
Risk Factors(Mean % Weight Loss)
Phentermine/ Topiramate ER7.5/46 mg(8.4%) P value*
Phentermine/Topiramate ER
15/92 mg(10.4%) P value*
Systolic BP, mmHg ‐4.7 0.0008 ‐5.6 <0.0001
Diastolic BP, mmHg ‐3.4 NS ‐3.8 0.0031
Triglycerides, % ‐8.6 <0.0001 ‐10.6 <0.0001
Total cholesterol, % ‐4.9 0.0345 ‐6.3 <0.0001
LDL‐C, % ‐3.7 NS ‐6.9 0.0069
HDL‐C, % 5.2 <0.0001 6.8 <0.0001
hsCRP, mg/L ‐2.49 <0.0001 ‐2.49 <0.0001
Adiponectin, g/mL 1.40 <0.0001 2.08 <0.0001
*P values represent comparisons to placebo.Intent to treat, last observation carried forward analysis for total study population.Gadde KM, et al. Lancet. 2011;377:1341-1352.
CONQUER Study
50
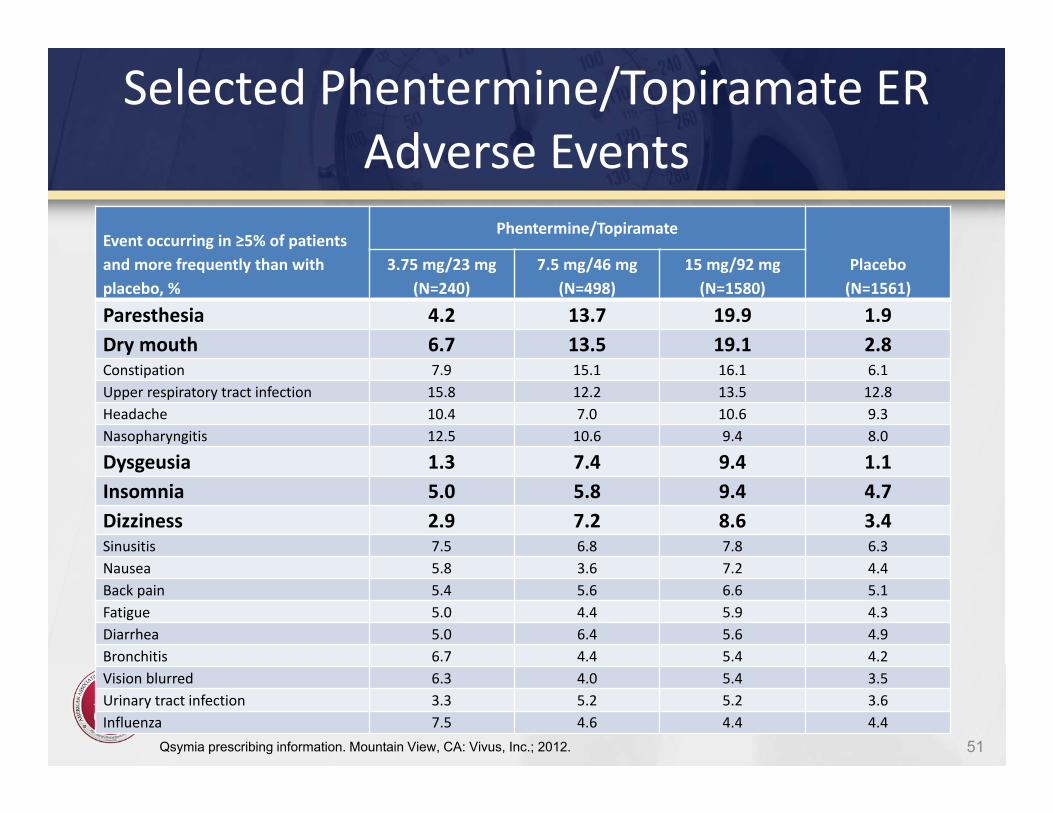
Selected Phentermine/Topiramate ER Adverse Events
Event occurring in ≥5% of patientsand more frequently than with placebo, %
Phentermine/Topiramate
Placebo(N=1561)
3.75 mg/23 mg(N=240)
7.5 mg/46 mg(N=498)
15 mg/92 mg(N=1580)
Paresthesia 4.2 13.7 19.9 1.9 Dry mouth 6.7 13.5 19.1 2.8 Constipation 7.9 15.1 16.1 6.1 Upper respiratory tract infection 15.8 12.2 13.5 12.8 Headache 10.4 7.0 10.6 9.3 Nasopharyngitis 12.5 10.6 9.4 8.0
Dysgeusia 1.3 7.4 9.4 1.1 Insomnia 5.0 5.8 9.4 4.7 Dizziness 2.9 7.2 8.6 3.4 Sinusitis 7.5 6.8 7.8 6.3 Nausea 5.8 3.6 7.2 4.4 Back pain 5.4 5.6 6.6 5.1Fatigue 5.0 4.4 5.9 4.3 Diarrhea 5.0 6.4 5.6 4.9 Bronchitis 6.7 4.4 5.4 4.2 Vision blurred 6.3 4.0 5.4 3.5 Urinary tract infection 3.3 5.2 5.2 3.6 Influenza 7.5 4.6 4.4 4.4
51Qsymia prescribing information. Mountain View, CA: Vivus, Inc.; 2012.
Bupropion/Naltrexone(Contrave)
• Bupropion stimulates hypothalamic pro‐opiomelanocortin neurons
• Naltrexone simultaneously blocks opiod‐mediated pro‐opiomelanocortin autoinhibition
• Both drugs may also have an additional mechanism of action by modulation of mesolimbic reward pathways.
Greenway FL, Fujioka K, Plodkowski RA et al. Lancet. 2010; 376: 595-605
Bupropion/Naltrexone(Contrave)
• 56‐wk, randomized, double‐blind, placebo‐controlled study
• 1742 patients 18‐65 years old• BMI 30‐45 or 27 and 29.9 with co‐mobidity• Top 3 adverse events:
– Dry Mouth– Paraesthesia– Dry mouth
Greenway FL, Fujioka K, Plodkowski RA et al. Lancet. 2010; 376: 595-605
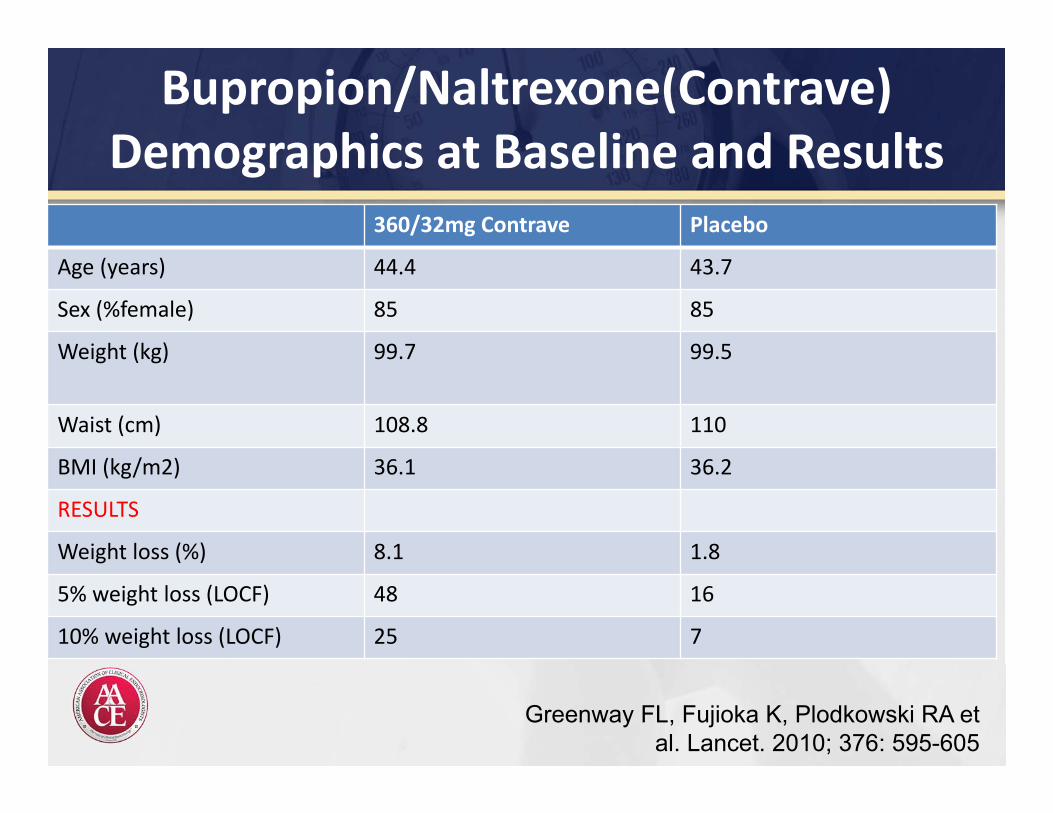
Bupropion/Naltrexone(Contrave) Demographics at Baseline and Results
360/32mg Contrave Placebo
Age (years) 44.4 43.7
Sex (%female) 85 85
Weight (kg) 99.7 99.5
Waist (cm) 108.8 110
BMI (kg/m2) 36.1 36.2
RESULTS
Weight loss (%) 8.1 1.8
5% weight loss (LOCF) 48 16
10% weight loss (LOCF) 25 7
Greenway FL, Fujioka K, Plodkowski RA et al. Lancet. 2010; 376: 595-605
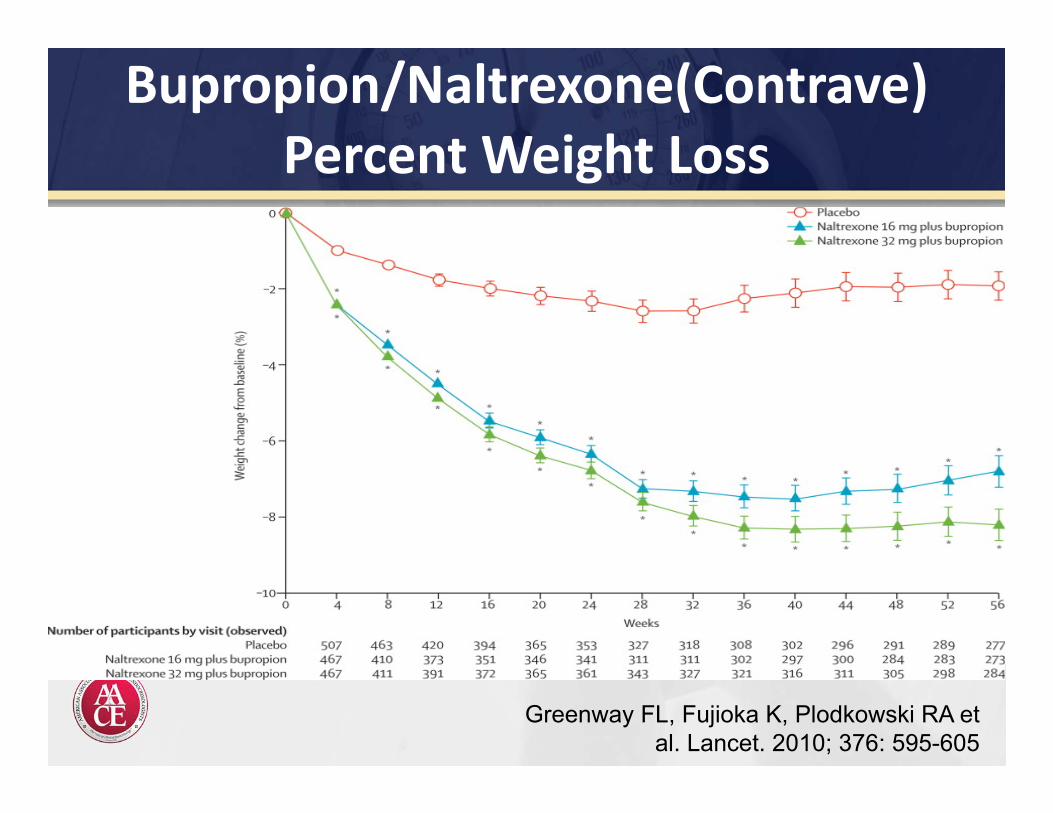
Bupropion/Naltrexone(Contrave)Percent Weight Loss
Greenway FL, Fujioka K, Plodkowski RA et al. Lancet. 2010; 376: 595-605
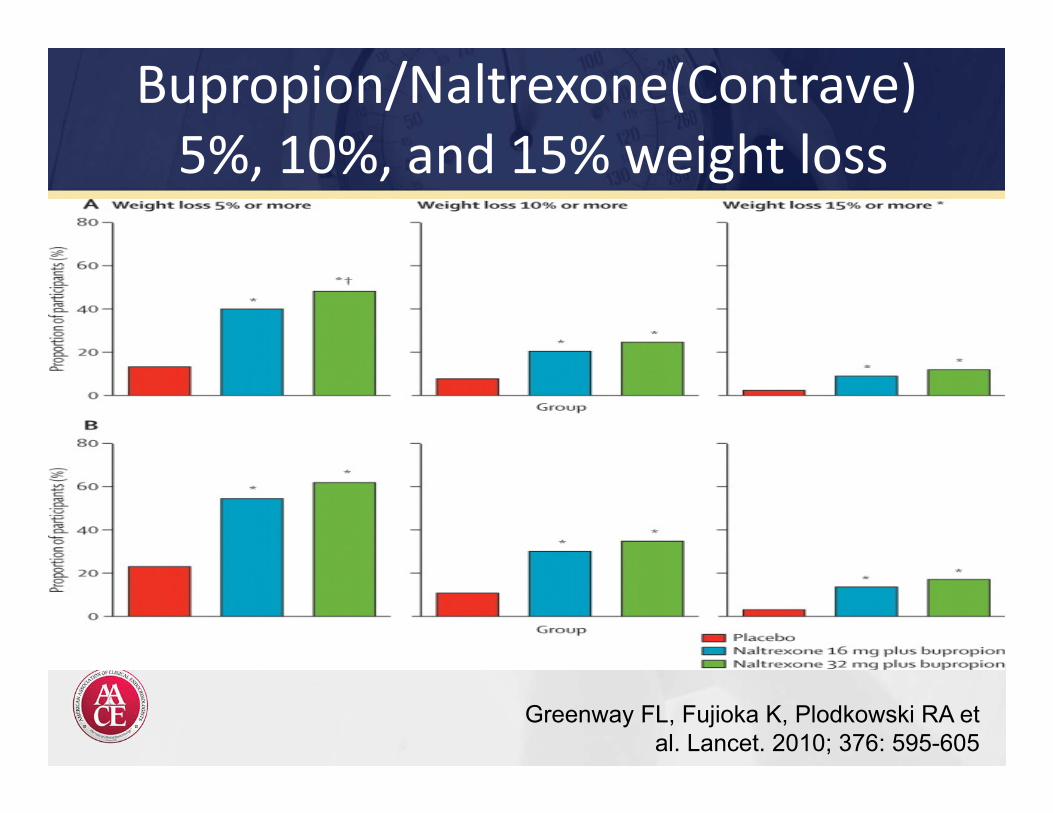
Bupropion/Naltrexone(Contrave)5%, 10%, and 15% weight loss
Greenway FL, Fujioka K, Plodkowski RA et al. Lancet. 2010; 376: 595-605
Liraglutide (Saxenda)
• Liraglutide is an acylated human glucagon‐like peptide‐1 (GLP‐1) receptor agonist with 97% amino acid sequence homology to endogenous human GLP‐1.
• GLP‐1 is secreted from Intestinal endocrine L cells located mainly in the distal ileum and colon.
• GLP‐1 binds to the GLP‐1R expressed in the brain.
Fujioka K et al. Diabetologia. 2014; 57 (Suppl 1): Abstract 904-P
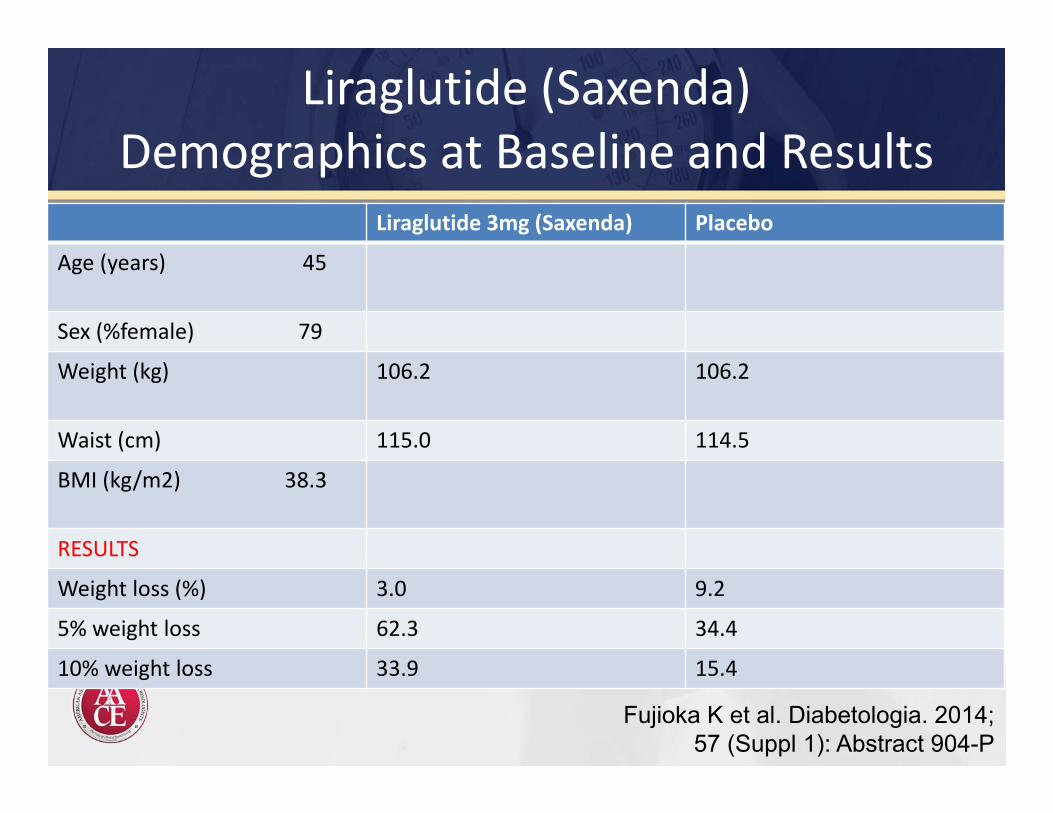
Liraglutide (Saxenda) Demographics at Baseline and Results
Liraglutide 3mg (Saxenda) Placebo
Age (years) 45
Sex (%female) 79
Weight (kg) 106.2 106.2
Waist (cm) 115.0 114.5
BMI (kg/m2) 38.3
RESULTS
Weight loss (%) 3.0 9.2
5% weight loss 62.3 34.4
10% weight loss 33.9 15.4
Fujioka K et al. Diabetologia. 2014; 57 (Suppl 1): Abstract 904-P
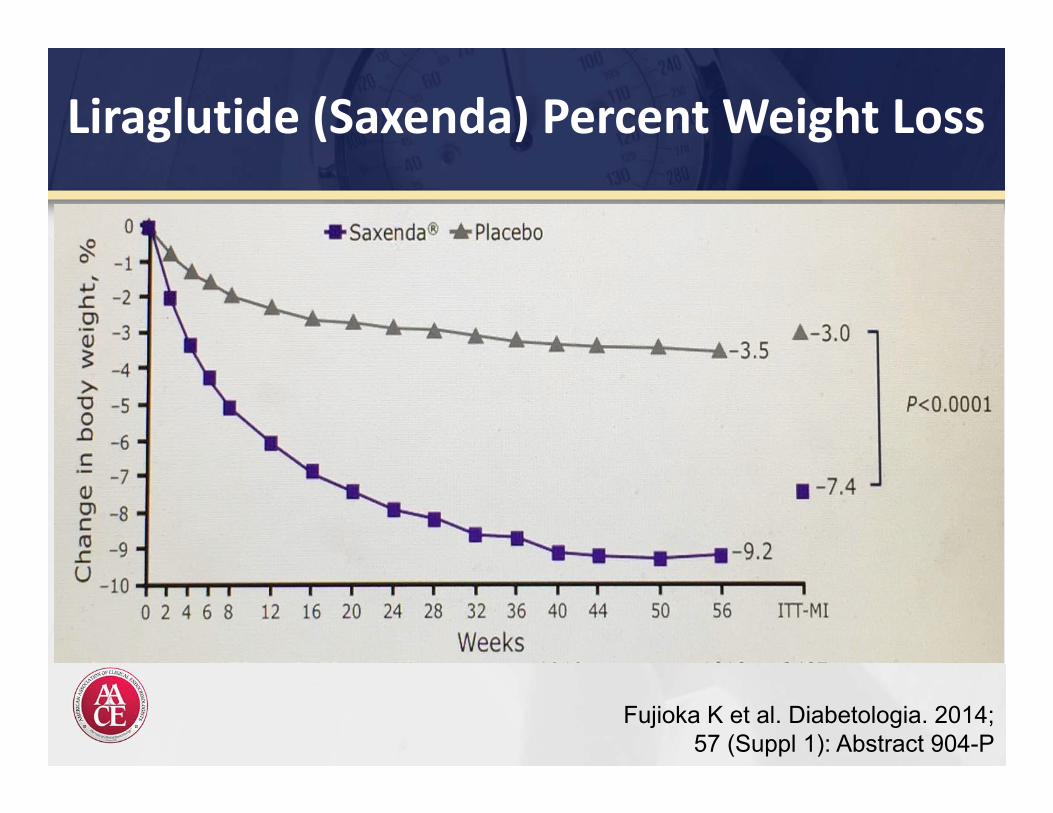
Liraglutide (Saxenda) Percent Weight Loss
Fujioka K et al. Diabetologia. 2014; 57 (Suppl 1): Abstract 904-P
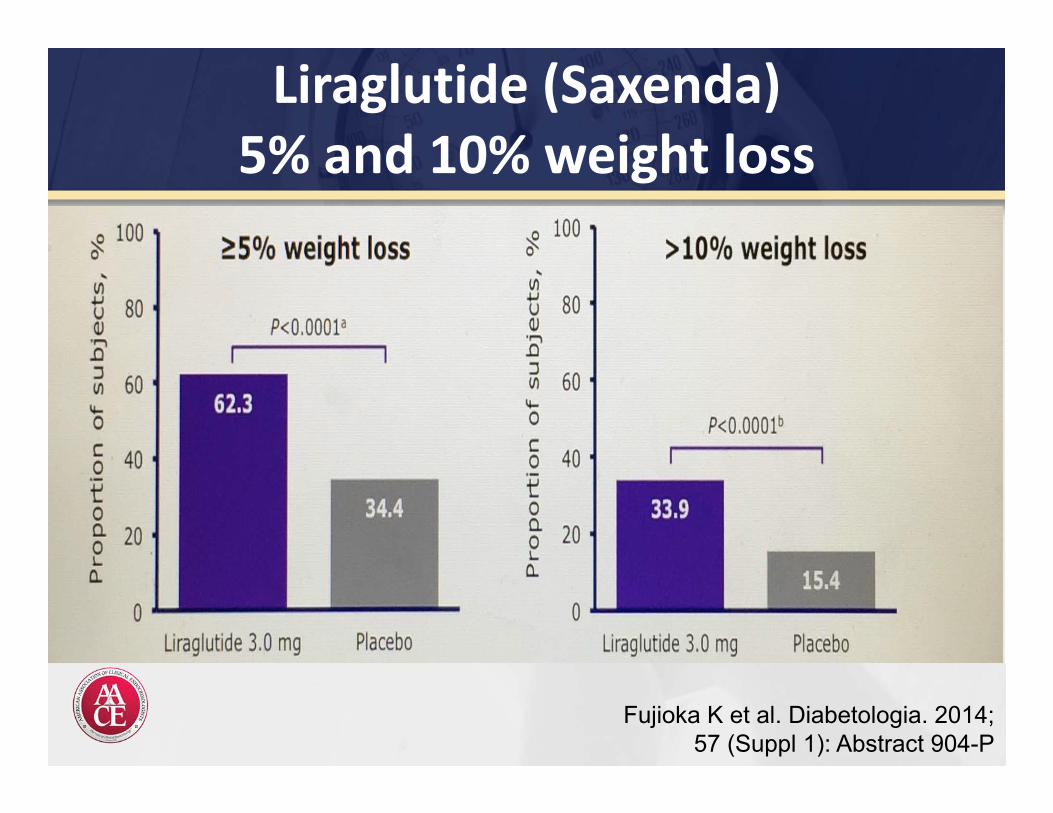
Liraglutide (Saxenda)5% and 10% weight loss
Fujioka K et al. Diabetologia. 2014; 57 (Suppl 1): Abstract 904-P
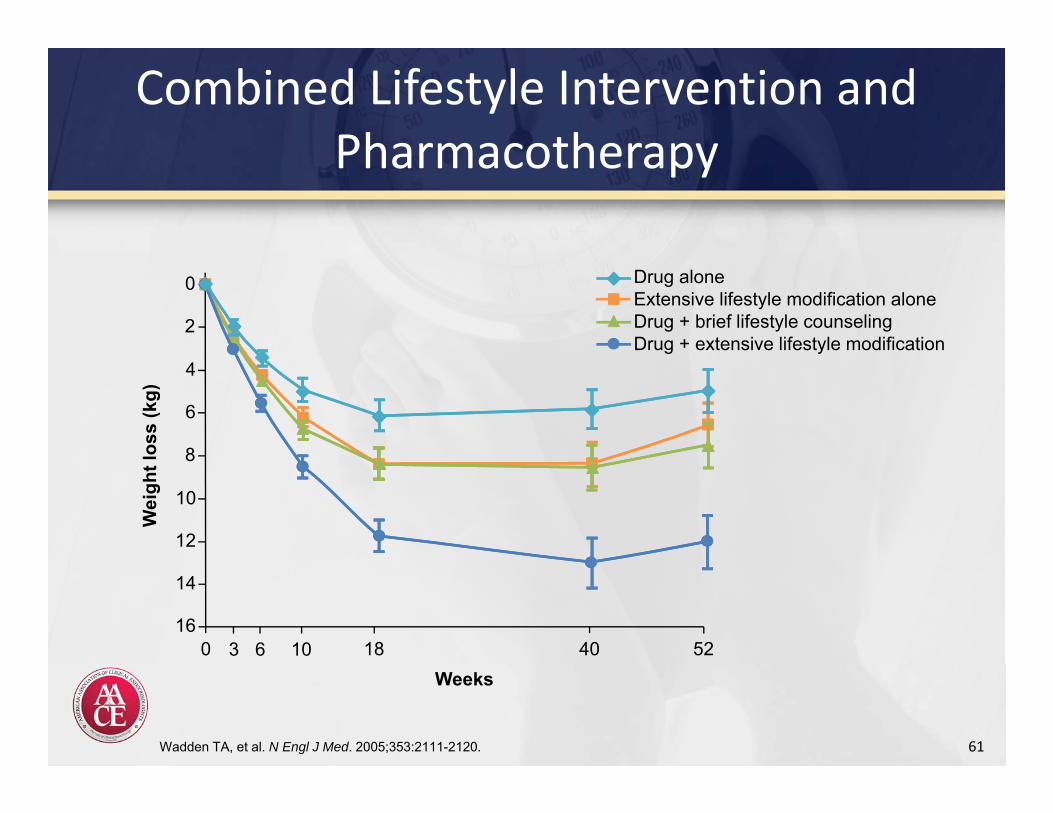
Combined Lifestyle Intervention and Pharmacotherapy
61Wadden TA, et al. N Engl J Med. 2005;353:2111-2120.
Wei
ght l
oss
(kg)
2
4
6
8
10
12
14
160 3 6 10 18 40 52
0
Weeks
Drug aloneExtensive lifestyle modification aloneDrug + brief lifestyle counselingDrug + extensive lifestyle modification
BARIATRIC SURGERY
62
Pharmacologic and Surgical Management of Obesity
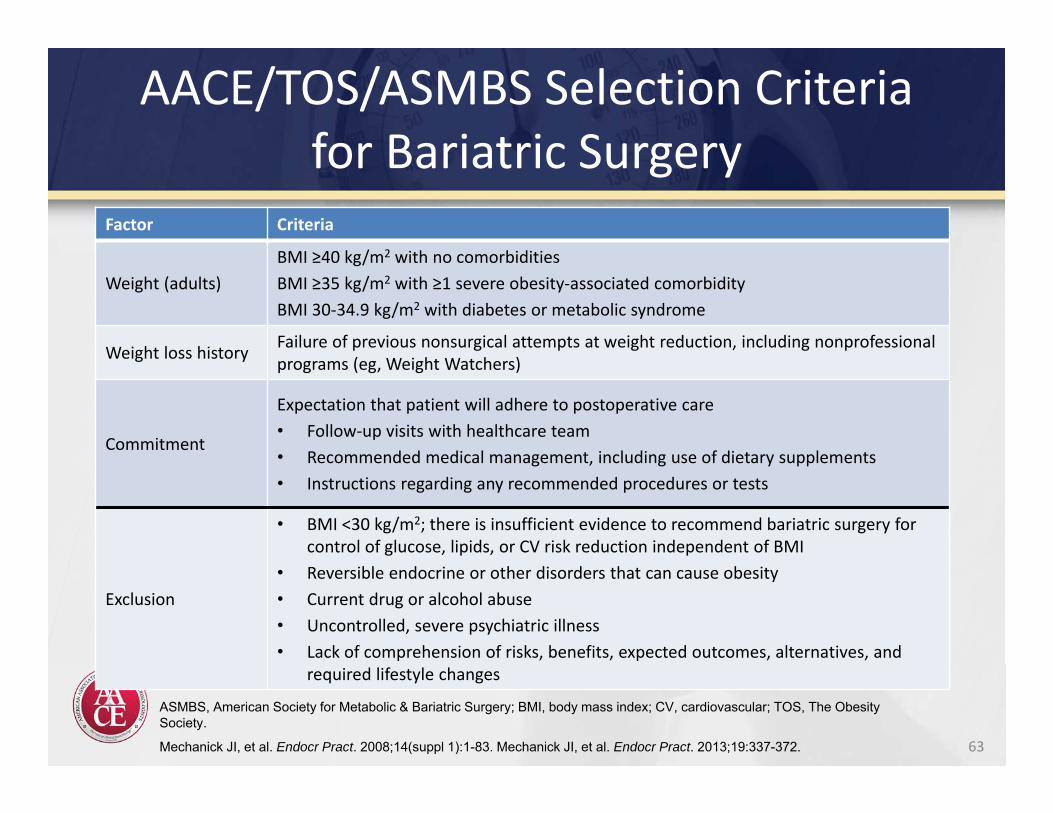
AACE/TOS/ASMBS Selection Criteriafor Bariatric Surgery
Factor Criteria
Weight (adults)BMI ≥40 kg/m2 with no comorbiditiesBMI ≥35 kg/m2 with ≥1 severe obesity‐associated comorbidityBMI 30‐34.9 kg/m2 with diabetes or metabolic syndrome
Weight loss history Failure of previous nonsurgical attempts at weight reduction, including nonprofessionalprograms (eg, Weight Watchers)
Commitment
Expectation that patient will adhere to postoperative care• Follow‐up visits with healthcare team• Recommended medical management, including use of dietary supplements• Instructions regarding any recommended procedures or tests
Exclusion
• BMI <30 kg/m2; there is insufficient evidence to recommend bariatric surgery for control of glucose, lipids, or CV risk reduction independent of BMI
• Reversible endocrine or other disorders that can cause obesity• Current drug or alcohol abuse• Uncontrolled, severe psychiatric illness• Lack of comprehension of risks, benefits, expected outcomes, alternatives, and
required lifestyle changes
63
ASMBS, American Society for Metabolic & Bariatric Surgery; BMI, body mass index; CV, cardiovascular; TOS, The Obesity Society.
Mechanick JI, et al. Endocr Pract. 2008;14(suppl 1):1-83. Mechanick JI, et al. Endocr Pract. 2013;19:337-372.
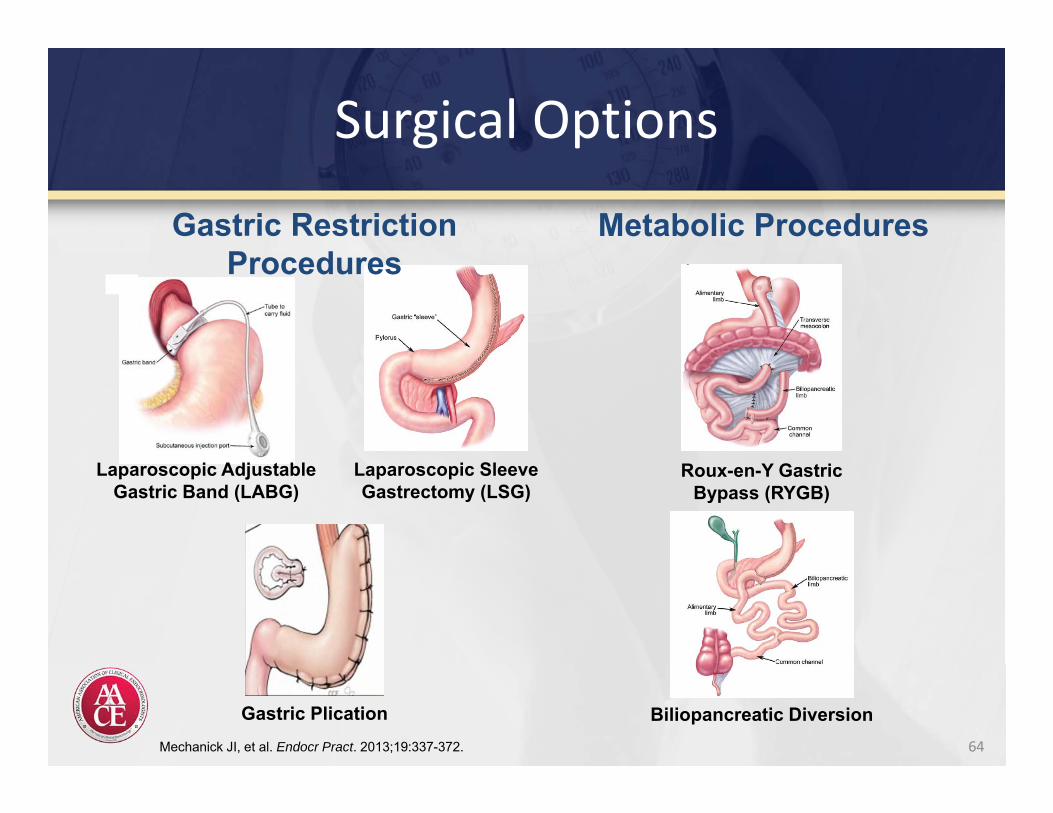
Surgical Options
64
Laparoscopic SleeveGastrectomy (LSG)
Gastric Plication
Roux-en-Y Gastric Bypass (RYGB)
Biliopancreatic Diversion
Gastric Restriction Procedures
Metabolic Procedures
Laparoscopic AdjustableGastric Band (LABG)
Mechanick JI, et al. Endocr Pract. 2013;19:337-372.
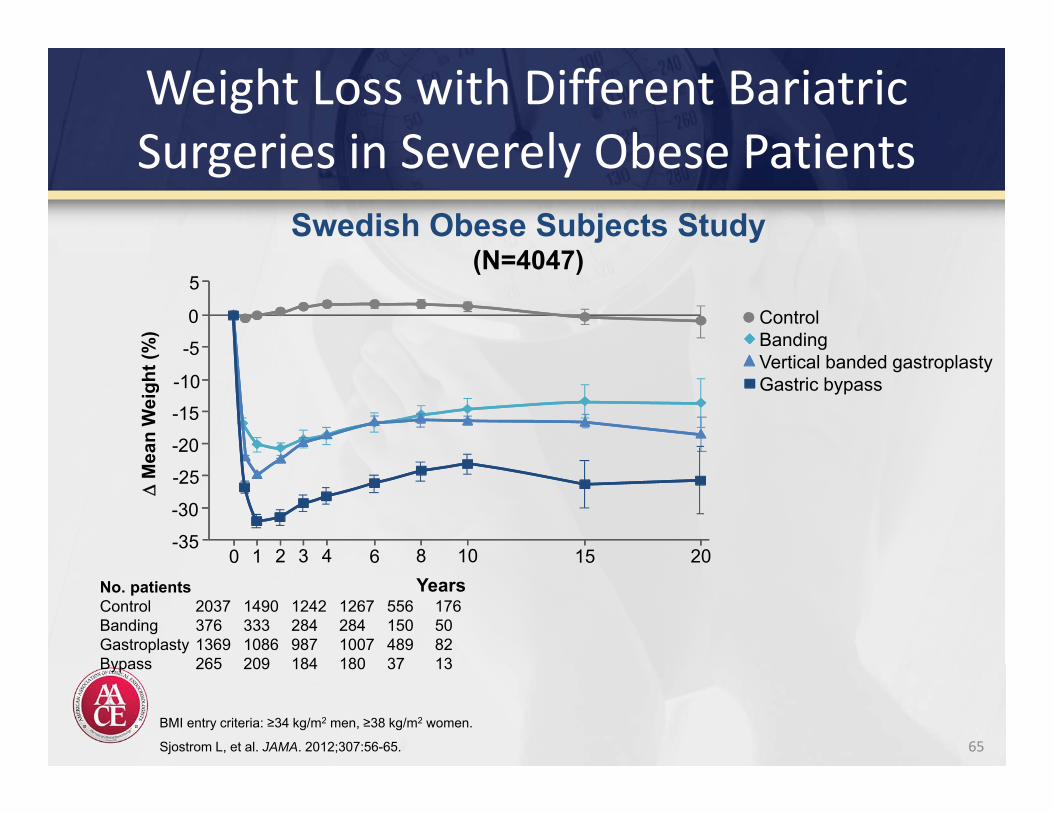
Weight Loss with Different Bariatric Surgeries in Severely Obese Patients
65BMI entry criteria: ≥34 kg/m2 men, ≥38 kg/m2 women.
Sjostrom L, et al. JAMA. 2012;307:56-65.
Swedish Obese Subjects Study(N=4047)
2015108643210-35
-30
-25
-20
-15-10
-5
0
5
Years
M
ean
Wei
ght (
%)
ControlBandingVertical banded gastroplastyGastric bypass
No. patientsControl 2037 1490 1242 1267 556 176Banding 376 333 284 284 150 50Gastroplasty 1369 1086 987 1007 489 82Bypass 265 209 184 180 37 13
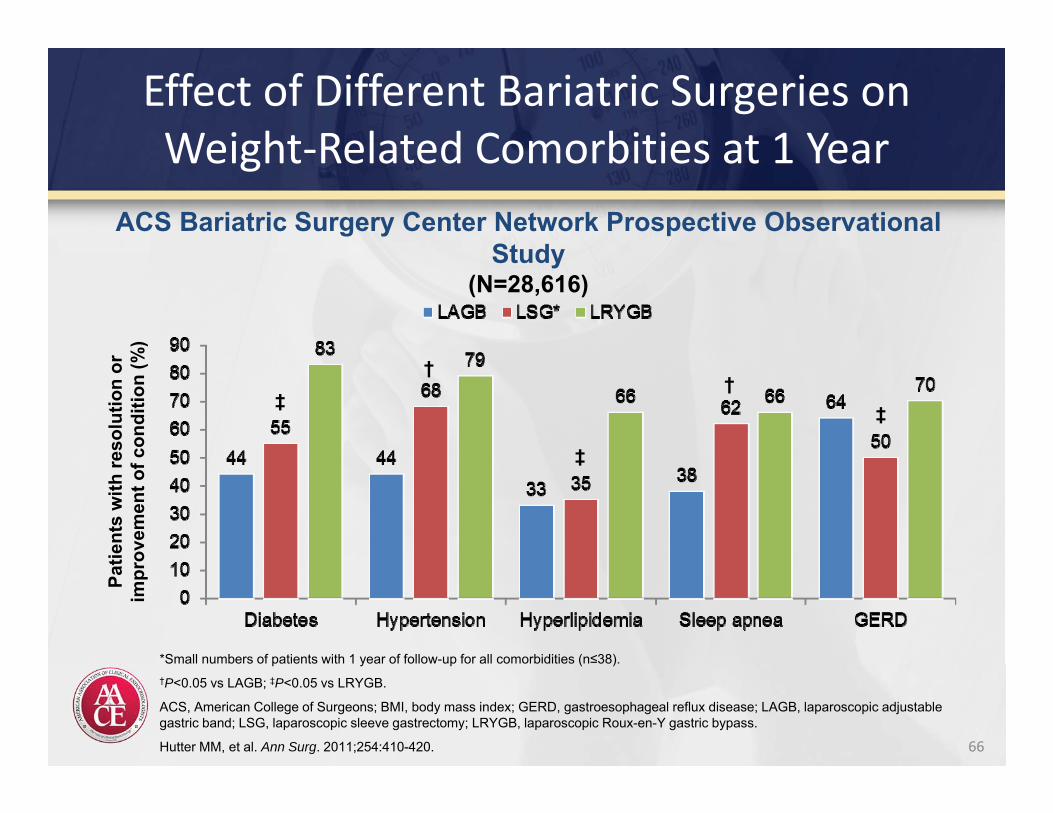
Effect of Different Bariatric Surgeries on Weight‐Related Comorbities at 1 Year
66
*Small numbers of patients with 1 year of follow-up for all comorbidities (n≤38).†P<0.05 vs LAGB; ‡P<0.05 vs LRYGB.
ACS, American College of Surgeons; BMI, body mass index; GERD, gastroesophageal reflux disease; LAGB, laparoscopic adjustablegastric band; LSG, laparoscopic sleeve gastrectomy; LRYGB, laparoscopic Roux-en-Y gastric bypass.
Hutter MM, et al. Ann Surg. 2011;254:410-420.
ACS Bariatric Surgery Center Network Prospective Observational Study
(N=28,616)
Patie
nts
with
reso
lutio
n or
im
prov
emen
t of c
ondi
tion
(%)
‡†
‡
†‡
Summary
• Rates of obesity have risen dramatically in the United States over the past 4 decades– Obesity dramatically increases the risk of diabetes, hypertension, and
dyslipidemia– Obesity contributes to increased costs of healthcare
• Obesity is a disease– The pathophysiology involves neuroendocrine factors involved in
regulating both appetite and energy balance– Impairments in physical and physiologic functioning contribute to high
rates of morbidity and mortality• Obesity can be diagnosed using anthropometric criteria (BMI and
waist circumference)• Obesity is treatable, and weight loss improves patient outcomes
and healthcare costs
67
Summary
• Treatment of obesity should be designed according to severity of comorbidities and complications as well as body mass
• Lifestyle change is the foundation of obesity management and should be maintained even if more intensive approaches are used– Weight loss agents are more effective when combined with lifestyle
change• Pharmacologic therapies
– May be considered for patients with ≥1 mild to moderate complications that can be treated effectively with moderate weight loss
– Should be used for patients with ≥1 severe complications that require more aggressive weight loss therapy
• Bariatric surgery should be considered for patients with ≥1 severe complications that require more aggressive weight loss therapy
68
AACE Obesity ResourceObesity Resource Center website:
http://obesity.aace.com/• Guidelines• Slide Library• Resource Toolkit• Treatment Algorithm