(Z)-3,5,4 -Trimethoxystilbene Limits Hepatitis C and Cancer … · HCV also induces EGFR that...
11
Tumor and Stem Cell Biology (Z)-3,5,4 0 -Trimethoxystilbene Limits Hepatitis C and Cancer Pathophysiology by Blocking Microtubule Dynamics and Cell-Cycle Progression Charles B. Nguyen 1 , Hari Kotturi 2 , Gulam Waris 3 , Altaf Mohammed 1,4,5 , Parthasarathy Chandrakesan 4,6,7 , Randal May 6,7 , Sripathi Sureban 4,6,7 , Nathaniel Weygant 6 , Dongfeng Qu 6,7 , Chinthalapally V. Rao 1,4,5 , Danny N. Dhanasekaran 4,8 , Michael S. Bronze 6 , Courtney W. Houchen 4,6,7 , and Naushad Ali 4,6,7 Abstract Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related deaths worldwide. Chronic hepatitis C virus (HCV) infection causes induction of several tumors/cancer stem cell (CSC) markers and is known to be a major risk factor for development of HCC. Therefore, drugs that simultaneously target viral replication and CSC properties are needed for a risk-free treatment of advanced stage liver diseases, including HCC. Here, we demonstrated that (Z)-3,5,4 0 -trimethoxystilbene (Z-TMS) exhibits potent antitumor and anti-HCV activities without exhi- biting cytotoxicity to human hepatocytes in vitro or in mice livers. Diethylnitrosamine (DEN)/carbon tetrachloride (CCl 4 ) exten- sively induced expression of DCLK1 (a CSC marker) in the livers of C57BL/6 mice following hepatic injury. Z-TMS exhibited hepatoprotective effects against DEN/CCl 4 -induced injury by reducing DCLK1 expression and improving histologic outcomes. The drug caused bundling of DCLK1 with microtubules and blocked cell-cycle progression at G 2 –M phase in hepatoma cells via downregulation of CDK1, induction of p21 cip1/waf1 expres- sion, and inhibition of Akt (Ser 473 ) phosphorylation. Z-TMS also inhibited proliferation of erlotinib-resistant lung adenocarcino- ma cells (H1975) bearing the T790M EGFR mutation, most likely by promoting autophagy and nuclear fragmentation. In conclu- sion, Z-TMS appears to be a unique therapeutic agent targeting HCV and concurrently eliminating cells with neoplastic potential during chronic liver diseases, including HCC. It may also be a valuable drug for targeting drug-resistant carcinomas and cancers of the lungs, pancreas, colon, and intestine, in which DCLK1 is involved in tumorigenesis. Cancer Res; 76(16); 4887–96. Ó2016 AACR. Introduction Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related death worldwide with a dismal 5-year survival rate of 11% (1, 2). Chronic infection with hepatitis C virus (HCV) is a major risk factor for the development of HCC (1, 3). HCV patients coinfected with other viruses or with metabolic comorbidity (obesity and diabetes) exhibit faster progression of liver disease and are difficult to treat with standard interferon- based treatment regimens (3). The combinations of direct-acting antiviral (DAA) drugs against three key HCV nonstructural pro- teins (NS3, NS5A, and NS5B) have shown remarkable efficacy (>90%) for curing the infection (4, 5). However, these drugs are inaccessible to millions of patients and a complete recovery of damaged liver by the HCV treatments alone has not been proven. The majority of HCC cases are normally diagnosed at late stages, and the use of curative surgery or other treatments are less successful (6, 7). Kinase inhibitors have been shown to increase survival only by a few months or are ineffectual in advanced HCC patients (8). The activation of multiple signaling pathways and enrichment of tumor/cancer stem cells (CSC) within the tumor appear to mediate HCC multidrug resistance (9–11). CSCs rep- resent small subpopulations within a tumor that possess self- renewing capabilities and the ability to differentiate into a het- erogeneous lineage within the tumor mass (12–14). We previously demonstrated a positive correlation between the levels of HCV replication and expression of an array of CSC- associated markers, including doublecortin-like kinase 1 (DCLK1; refs. 15, 16). These changes appear to promote cellular dediffer- entiation and the gain of CSC properties in HCV-positive cells. We have further demonstrated that knockdown of DCLK1 results in downregulation of HCV replication, cell migration, and epithe- lial–mesenchymal transition (EMT) in multiple cancer cell lines 1 College of Medicine, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma. 2 Department of Biology, University of Central Oklahoma, Edmond, Oklahoma. 3 Department of Microbiology and Immunology, Rosalind Franklin University of Medicine and Sci- ence, North Chicago, Illinois. 4 Peggy and Charles Stephenson Cancer Center, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma. 5 Center for Cancer Prevention and Drug Develop- ment, Hematology-Oncology Section, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma. 6 Department of Medicine, Section of Digestive Diseases and Nutrition, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma. 7 Department of Veterans Affairs Medical Center, Oklahoma City, Oklahoma. 8 Depart- ment of Cell Biology, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma. Corresponding Authors: Naushad Ali, The University of Oklahoma Health Sciences Center, 975 NE 10th Street BRC1266, Oklahoma City, OK 73104. Phone: 720-427-9758; Fax: 405-271-5450; E-mail: [email protected]; and Court- ney W. Houchen, [email protected] doi: 10.1158/0008-5472.CAN-15-2722 Ó2016 American Association for Cancer Research. Cancer Research www.aacrjournals.org 4887 on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722
Transcript of (Z)-3,5,4 -Trimethoxystilbene Limits Hepatitis C and Cancer … · HCV also induces EGFR that...

Tumor and Stem Cell Biology
(Z)-3,5,40-Trimethoxystilbene Limits Hepatitis Cand Cancer Pathophysiology by BlockingMicrotubule Dynamics and Cell-Cycle ProgressionCharles B. Nguyen1, Hari Kotturi2, Gulam Waris3, Altaf Mohammed1,4,5,Parthasarathy Chandrakesan4,6,7, Randal May6,7, Sripathi Sureban4,6,7,Nathaniel Weygant6, Dongfeng Qu6,7, Chinthalapally V. Rao1,4,5,Danny N. Dhanasekaran4,8, Michael S. Bronze6, Courtney W. Houchen4,6,7, andNaushad Ali4,6,7
Abstract
Hepatocellular carcinoma (HCC) is the third most commoncause of cancer-related deaths worldwide. Chronic hepatitis Cvirus (HCV) infection causes induction of several tumors/cancerstem cell (CSC)markers and is known to be amajor risk factor fordevelopment of HCC. Therefore, drugs that simultaneously targetviral replication and CSC properties are needed for a risk-freetreatment of advanced stage liver diseases, including HCC. Here,we demonstrated that (Z)-3,5,40-trimethoxystilbene (Z-TMS)exhibits potent antitumor and anti-HCV activities without exhi-biting cytotoxicity to human hepatocytes in vitro or in mice livers.Diethylnitrosamine (DEN)/carbon tetrachloride (CCl4) exten-sively induced expression of DCLK1 (a CSC marker) in the liversof C57BL/6 mice following hepatic injury. Z-TMS exhibitedhepatoprotective effects against DEN/CCl4-induced injury by
reducing DCLK1 expression and improving histologic outcomes.The drug caused bundling of DCLK1 with microtubules andblocked cell-cycle progression at G2–M phase in hepatoma cellsvia downregulation of CDK1, induction of p21cip1/waf1 expres-sion, and inhibition of Akt (Ser473) phosphorylation. Z-TMS alsoinhibited proliferation of erlotinib-resistant lung adenocarcino-ma cells (H1975) bearing the T790M EGFRmutation, most likelyby promoting autophagy and nuclear fragmentation. In conclu-sion, Z-TMS appears to be a unique therapeutic agent targetingHCV and concurrently eliminating cells with neoplastic potentialduring chronic liver diseases, including HCC. It may also be avaluable drug for targeting drug-resistant carcinomas and cancersof the lungs, pancreas, colon, and intestine, in which DCLK1 isinvolved in tumorigenesis. Cancer Res; 76(16); 4887–96.�2016 AACR.
IntroductionHepatocellular carcinoma (HCC) is the third most common
cause of cancer-related death worldwide with a dismal 5-yearsurvival rate of 11%(1, 2).Chronic infectionwithhepatitis Cvirus(HCV) is a major risk factor for the development of HCC (1, 3).HCV patients coinfected with other viruses or with metabolic
comorbidity (obesity and diabetes) exhibit faster progression ofliver disease and are difficult to treat with standard interferon-based treatment regimens (3). The combinations of direct-actingantiviral (DAA) drugs against three key HCV nonstructural pro-teins (NS3, NS5A, and NS5B) have shown remarkable efficacy(>90%) for curing the infection (4, 5). However, these drugs areinaccessible to millions of patients and a complete recovery ofdamaged liver by the HCV treatments alone has not been proven.
The majority of HCC cases are normally diagnosed at latestages, and the use of curative surgery or other treatments are lesssuccessful (6, 7). Kinase inhibitors have been shown to increasesurvival only by a fewmonths or are ineffectual in advanced HCCpatients (8). The activation of multiple signaling pathways andenrichment of tumor/cancer stem cells (CSC) within the tumorappear to mediate HCC multidrug resistance (9–11). CSCs rep-resent small subpopulations within a tumor that possess self-renewing capabilities and the ability to differentiate into a het-erogeneous lineage within the tumor mass (12–14).
We previously demonstrated a positive correlation between thelevels of HCV replication and expression of an array of CSC-associatedmarkers, including doublecortin-like kinase 1 (DCLK1;refs. 15, 16). These changes appear to promote cellular dediffer-entiation and the gain of CSCproperties inHCV-positive cells.Wehave further demonstrated that knockdown of DCLK1 results indownregulation of HCV replication, cell migration, and epithe-lial–mesenchymal transition (EMT) in multiple cancer cell lines
1College of Medicine, University of Oklahoma Health Sciences Center,Oklahoma City, Oklahoma. 2Department of Biology, University ofCentral Oklahoma, Edmond,Oklahoma. 3Department ofMicrobiologyand Immunology, Rosalind Franklin University of Medicine and Sci-ence, North Chicago, Illinois. 4Peggy and Charles Stephenson CancerCenter, University of Oklahoma Health Sciences Center, OklahomaCity, Oklahoma. 5Center for Cancer Prevention and Drug Develop-ment, Hematology-Oncology Section, University of Oklahoma HealthSciencesCenter,OklahomaCity,Oklahoma. 6DepartmentofMedicine,Section of Digestive Diseases and Nutrition, University of OklahomaHealth Sciences Center, Oklahoma City, Oklahoma. 7Department ofVeterans Affairs Medical Center, Oklahoma City, Oklahoma. 8Depart-ment of Cell Biology, University of Oklahoma Health Sciences Center,Oklahoma City, Oklahoma.
Corresponding Authors: Naushad Ali, The University of Oklahoma HealthSciences Center, 975 NE 10th Street BRC1266, Oklahoma City, OK 73104. Phone:720-427-9758; Fax: 405-271-5450; E-mail: [email protected]; and Court-ney W. Houchen, [email protected]
doi: 10.1158/0008-5472.CAN-15-2722
�2016 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 4887
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

and in mouse models (15, 17). There is currently no clearchoice for targeting CSCs efficiently (18, 19). DCLK1 is con-sidered to be an important target for the treatment of tumors ofthe liver, pancreas, and colon. HCV also induces EGFR thatfacilitates HCV entry into the cells and promotes progression ofliver diseases (20, 21). The EGFR inhibitor, erlotinib, has beenshown to downregulate HCV RNA levels in a mouse model(20). These observations clearly suggest that cellular kinases(DCLK1 and EGFR) are critical components of HCV-inducedchronic liver diseases.
The naturally occurring antioxidant, resveratrol (RVT) hasbeen extensively studied for possible health benefits (22, 23),including anticancer effects (24–26). However, its potentialbenefits could not be demonstrated in patients with malignan-cy due to poor absorption and extremely low bioavailability(23, 27). The structurally related analogue (Z)-3,5,40-tri-methoxystilbene (Z-TMS), originally isolated from the bark ofVirola elongate, has been shown to inhibit microtubule poly-merization, induce G2–M arrest, and inhibit ornithine decar-boxylase activity (28, 29). Z-TMS also has long half-life andlimited drug clearance when administered intravenously(30, 31). Here, we report mechanism(s) of Z-TMS's antiviraland antitumor activities in several in vitro models and in DEN/CCL4–induced liver injury in C57BL/6 mouse model. Z-TMSexerts its inhibitory effects on tumors by diminishing DCLK1þ
cell population, interference with DCLK1-microtubule dynam-ics, cell-cycle arrest at G2–M phase, promotion of autophagy,and causing nuclear fragmentation. It is considerably effectiveagainst erlotinib-resistant T790M-mutant lung carcinoma cellsand may evolve as a potential candidate for the treatment ofHCV-induced advanced liver diseases, including HCC.
Materials and MethodsReagents, antibodies, cells, and cell culture
The non–small cell lung adenocarcinoma cells (NSCLC,H1975) and primary human hepatocytes were purchased fromATCC and BD Biosciences, respectively. All other cells (endog-enous) were tested before start of the studies using MycoAlertKit (Lonza) and were found negative forMycoplasma. The parentcell line Huh7 and human hepatocytes were recently evaluated(January 14, 2016) for Hantaan virus, LCMV, and Mycoplasmausing PCR by IDEXX Bioresearch and were negative for theseagents. The characteristics of hepatoma Huh7-derived cell lines(Huh7.5, GS5, and FCA4) have been described previously (15,16, 32, 33). HCVþDCLK1þ hepatoma cells were generated bytransducing G418-resistant FCA4 cells with lentivirus expres-sing DCLK1 (isoform 1) tagged with RFP at the N-terminus. Thecells were cultured as described previously (34). Resveratrol(Sigma) and Z-TMS (Cayman Chemical) were prepared inDMSO and stored at �20�C. EGFR (aa 695–1210) and lucif-erase assay kits were purchased from Promega. The antibodieswere purchased from the following sources: DCLK1 (ab31704),NS5B (35586), actin (ab1801), and Abcam; LC3B (2775),cleaved caspase-3 (Asp175; 9664), and p-Akt (4069), fromCell Signaling Technology; and anti-NS3 antibody (217-A)from Virogen.
Z-TMS treatment of hepatoma cells infected with HCVThe cell culture–generated JFH1 HCV-2a infectious particles
(HCVcc) were produced as described previously (35). In brief,JFH1 RNAs were electroporated into Huh7.5 cells and HCVcc
particleswere determined in cell culture supernatant.Huh7.5 cellswere infected with HCVcc at multiplicity of infection of 1 for 48hours. Subsequently, theHCVcc-infected cellswere treatedwithZ-TMS (1 mmol/L) or equivalent amounts ofDMSO in triplicates for48 hours. The untreated infected cells were considered as positivecontrol, whereas uninfected Huh7.5 cells served as negativecontrol for detection of the HCV RNA by qRT-PCR. The HCVRNA copy numbers per microgram of total RNAs in Z-TMS werecalculated and compared with vehicle-treated and -untreatedsamples. JFH-1/GND RNAs (replication defective JFH1 mutant)were used as negative control. In most of the experiments, HCV-infected cells were serum starved for 4 hours before harvesting.Total RNAs from the HCV replicon–expressing cells were isolatedand subjected to RT-PCR as described previously (15).
Western blot analysis, cell survival, and cell proliferationCells treated with resveratrol, Z-TMS, or DMSO were washed
with PBS, collected, and lysedwithmammalian protein extractionreagent (M-PER; Thermo Scientific). Western blots were per-formed using 30–40 mg of cell lysates (15, 34) and antibodieswere diluted as recommended by the manufacturers. Each West-ern blot analysis was repeated three times. To evaluate targetprotein to actin ratio, band intensities were calculated usingGelQuant software andmean ratios were presented. Cell viabilitywas determined using CellTiter 96 AQueous One Solution (Pro-mega) as recommended by the manufacturer.
H1975 cells were cultured in RPMI1640 media supplementedwith 10%FCS. Z-TMS–treated and -untreatedH1975 cells in a 96-well culture plate were stained with DRAQ5 and scanned withOperetta (PerkinElmer). Each treatment was done in quadrupletsand each well was analyzed for five different fields for the analysisof nuclear fragmentation. The images (average of 5 fields for eachwell) were analyzed byColumbus software.Wound-healing assayfor cell migration was carried out as described previously (34).
Cell-cycle analysis using flow cytometryCells treated were with Z-TMS (1 mmol/L) or DMSO for 48
hours, harvested, and washed with PBS. The pelleted cells wereresuspended in PBS containing paraformaldehyde (2%) for 1hour at 4�C, washed twice with ice-cold PBS, resuspended andfixed in 70% ethanol, and incubated overnight at 4�C. The cellswere treated with RNase A (200 mg/mL) and propidium iodide(PI, 50 mg/mL; Sigma) for 30 minutes at 37�C in the dark andstored at 4�C until acquisition of the flow cytometry data. Theinstrument was calibrated with unstained cells and sorted for PIintensity. A total of 10,000 cell events were collected. Flowcytometry data were collected and analyzed using the CELLQuestprogram (Becton Dickinson).
Kinase activitiesEGFR kinase assay was performed using the ADP-Glo kinase
assay and recombinant EGFR representing amino acids 695–1210of the wild type using Promega's protocol. The kinase was treatedwith 1 mmol/L of Z-TMS or erlotinib in triplicates, and luciferaseread-out for the EGFR kinase activities were compared with theuntreated control. The experiment was repeated twice.
HCC survival data and IHC of human liver tissuesTo evaluate the relationship between DCLK1 expression levels
and survival of HCC patients, a Kaplan–Meier plot was generated
Nguyen et al.
Cancer Res; 76(16) August 15, 2016 Cancer Research4888
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

using the liver HCC (LIHC, total 369 cases) data provided by theTCGA Research Network (http://cancergenome.nih.gov/) usingthe UCSC Genome Browser. Immunohistochemical staining ofliver tissues frompatientswithHCVandHCCwere obtained fromthe LTCDS (Minneapolis, MN; refs. 15, 34).
Hepatoma xenografts and treatment of C57BL/6 micewith Z-TMS
All mice studies reported here were preapproved (protocols #12-041 and 15-083) and supervised by the University of Okla-homaHealth Sciences Center (OUHSC) Institutional Animal Careand Use Committee, which adheres to the PHS Policy IV.B.3.Athymic nude Balb/c mice were purchased from The JacksonLaboratory and housed in pathogen-free conditions. One millionHuh7 cells were washed with PBS three times, resuspended in thesame buffer, and injected subcutaneously into the dorsal flanks of4- to 6-week-old mice as reported previously (34). Tumors weremeasured with calipers and the volumes were calculated usingformula: 0.5 � (length � width2).
Adult immunocompetent C57BL/6 mice (n ¼ 30, 8-week-old,generated by in-house breeding at OUHSC Rodent Barrier Facil-ity) were randomized into 6 groups (5 mice/group). Groups 1through 3 received two intraperitoneal injections of diethylni-trosamine [DEN, 25 mg/kg body weight (BW), one injection perweek] followed by twice-weekly injections of CCl4 (1 mL/kg BW)for the next 7 weeks. Except group 1, groups 2 and 3 were alsotreated with 20 and 40 mg/kg BW of Z-TMS dissolved in DMSO,respectively. Group 4 received only Z-TMS (40 mg/kg BW) todetermine its possible toxicity. Groups 5 and 6 served as DMSOand untreated controls, respectively, during the same period. Atthe termination of the experiments, all the animals were eutha-nized and subjected to necropsy for collection and analysis ofblood or tissues of different organs.
Statistical analysisAll experiments were performed in biological replicates of at
least three and repeated to confirm the results. The graphs werepresented as mean � SD. The P values were calculated using theStudent t test. Results with P � 0.05 were considered statisticallysignificant.
ResultsZ-TMS is a potent HCV inhibitor
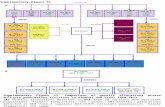
Published reports suggest potential benefits of resveratrol(3,5,40-trihydroxy-trans-stilbene, RVT) and its analogues onhuman health (reviewed in refs. 36, 37). We initially tested theanti-HCV activities of RVT and its natural analogue Z-TMS inhepatoma cell lines (GS5 and FCA4) expressing HCV-1b sub-genomic replicons (16, 34). The results suggested that Z-TMS isnearly 100 timesmorepotent indownregulating the levels ofHCVNS5B polymerase, which is now considered a core target of directantiviral therapy (results not shown). Next, FCA4 cells weretreated with varying amounts (0, 0.05, 0.1, 0.5, 1.0, and 2.5mmol/L) of Z-TMS or equivalent amounts of DMSO for 48 hours.The total lysates prepared from drug-treated and -untreated cellswere analyzed for NS5B and actin (loading control) levels. Thedata suggest that Z-TMS inhibits NS5B expression in a dose-dependent manner (Fig. 1A, lanes 2–6). Similar results wereobtained with GS5 cells (not shown). The DMSO solvent controlhad no inhibitory effect on the NS5B levels (lanes 7–11) ascompared with the untreated control (lane 1). Under these con-
ditions (0.1–1.0 mmol/L Z-TMS for 48-hour treatment), FCA4cells as well as normal human hepatocytes remained fully viable(Fig. 1B and C).
To examinewhether Z-TMS inhibitsHCV replication in anHCVinfection model, Huh7.5 cells were infected with tissue culture–generated JFH1 viruses (HCVcc) for 48 hours to allow replicationof the viral RNA. The infected cellswere then treatedwith1mmol/Lof Z-TMS or vehicle for 48 hours. Total RNAs isolated from thesecells were subjected to qRT-PCR to determine the levels of HCVreplication. As expected, the JFH1 RNA copy number was dras-tically reduced (�10 times) by Z-TMS treatment as comparedwiththe DMSO-treated or -untreated cells (Fig. 1D). The results werefully corroborated by the dramatic reduction inNS3 level (Fig. 1E,lane 3) as compared with the controls (lanes 2 and 4).
Z-TMS disrupts DCLK1-microtubule dynamicsMicrotubules are highly dynamic structures whose regulations
are critical for HCV replication, cell division, cell migration, andcell polarity. The CSC marker DCLK1 associates with microtu-bules and stimulates polymerization of tubulins. We have previ-ously shown that DCLK1 is overexpressed in liver tissues derivedfrom patients with cirrhosis and HCC. Its expression is alsocorrelated with activation of inflammatory and protumorigenicsignals as well as hepatoma cell migration (34). These observa-tions led us to investigate the significance of DCLK1 overexpres-sion inpatient survival and effects of Z-TMSonDCLK1 interactionwith microtubules or microtubule dynamic instability. As shownin Fig. 2A, DCLK1 is overexpressed in liver tissues of HCV-positivepatients with cirrhosis and HCC but not in normal liver. TheKaplan–Meier plot suggests that the 5-year survival rate is approx-imately reduced by three times in HCC patients (n ¼ 369) withhepatic DCLK1 overexpression (Fig. 2B, red and black lines) ascomparedwith the patientswith lowDCLK1 levels (green line). Ina mouse tumor xenograft model described previously (34), largetumors (average size of 4–4.5 cm3) derived from Huh7 cellsexhibited extensive staining for human DCLK1 except the onethat was smaller in size (0.65 cm3; Fig. 2C). Because of DCLK1'simportant roles in microtubule dynamics, HCV replication andtumor growth in addition to the ability of HCVþDCLK1þ hepa-toma cells to form spheroids (15, 16), we examined the effects ofZ-TMS on HCVþDCLK1þ cells. These cells were isolated fromFCA4 cells coexpressing recombinant RFP-DCLK1 and HCV sub-genomic replicon by FACS method. As shown in Fig. 2D, expres-sion of HCV NS5B polymerase in HCVþDCLK1þ hepatoma cellswas significantly reduced by1mmol/Lof Z-TMS treatment (lane 3)as compared with controls (lanes 1 and 2). Z-TMS treatment alsocaused significant inhibition in the proliferative potential of thesecells (Fig. 2E). We carried out confocal immunofluorescencemicroscopy to determine localization of DCLK1 with microtu-bule in these cells after Z-TMS treatment. The results revealedthat Z-TMS induces bundling of microtubules and speckle-likestructures of DCLK1–microtubule complexes (Fig. 2F, bottom).However, the untreated and DMSO-treated cells exhibit normaldistribution of DCLK1 (red) and tubulin (green) or theircomplexes (yellow). Collectively, these results indicate a directrelationship of DCLK1 with the survival of HCC patients andpossibility of targeting HCV-positive DCLK1-overexpressinghepatoma cells by Z-TMS.
We used a 3D magnetic levitation method (38) to culture GS5cells as visible cell spheroids/aggregates (Fig. 3A). The levels ofNS5A-GFP green fluorescence indicated continued HCV
Antiviral and Antitumor Activities of Z-TMS
www.aacrjournals.org Cancer Res; 76(16) August 15, 2016 4889
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

replication in the spheroid-like cultures (Fig. 3A, inset). Immu-nohistochemical staining of these aggregates revealed differentcell phenotypes. Although large cells displayed extensive CK19expression (circulating tumor cell marker) and cell-to-cell con-tacts, a low number of unique small cells were DCLK1 positive.This observation clearly suggests heterogeneous cell phenotypesin the spheroids. Z-TMS successfully inhibited growth of thiscellular mass (Fig. 3B).
Z-TMS causes G2–M cell-cycle arrest, inhibition of Aktphosphorylation, and upregulation of p21Cip1/Waf1 inhepatoma cells
GS5 cells, which express a NS5A-GFP chimeric proteinencoded by HCV-1b subgenomic RNAs, and Huh 7.5 cells weretreated with 1 mmol/L of Z-TMS for 48 hours and stained withPI for cell-cycle analysis. The results clearly suggest that mostGS5 cells and Huh7.5 parent cells were stalled in the G2–Mphase (>90%) with a concomitant reduction in the G1 and S-phases (Fig. 4A). However, DMSO-treated and untreated cellsshowed similar cell-cycle distribution. The result shows that theobserved change in cell cycle was induced by Z-TMS and not bythe DMSO (solvent). Similar Z-TMS effects were observed for
other hepatoma cell lines (Huh7 and FCA4, not shown). Next,total lysates of the drug-treated and -untreated cells weresubjected to Western blot analysis for detection of proteinsinvolved in cell-cycle checkpoints. Z-TMS treatment causeddownregulation of total cyclin-dependent kinase 1 (CDK1)with a concomitant induction of p21Cip1/Waf1 expression (Fig.4B, lane 3), which is a potent inhibitor of CDK1 and CDK2.Also, p21Cip1/Waf1 mediates growth arrest and cellular senes-cence. Activation of Akt overcomes a G2–M cell-cycle check-point induced by DNA damage (39). Therefore, successfulblockage of cancer cells at G2–M phase should also be accom-panied by the downregulation of Akt. Treatment of GS5 cellswith Z-TMS (1 mmol/L) resulted in significant downregulationof Akt (Ser473) phosphorylation without affecting total Aktlevel (Fig. 4C, lane 3). Taken together, Z-TMS appears to induceG2–M cell-cycle arrest by induction of p21Cip1/Waf1 and down-regulation of Akt signaling.
Broad-spectrum antitumor activities of Z-TMSBecause Z-TMS inhibits Akt activation, the status and function
of its upstream regulator EGFR) was examined. Our interest inEGFR investigation stems in part from the observation that
DA
B
0
20
40
60
80
100
120
140
0 0.1 0.5 1 2.5 Z-TMS, μmol/L
Perc
ent c
ell v
iabi
lity
Z-TMS DMSO
HCV replicon–expressing hepatoma cells
0 10 20 30 40 50 60 70 80 90
100 110
0 1 2.5
Perc
ent c
ell v
iabi
lity
Z-TMS DMSO
Z-TMS, μmol/L
Human hepatocytes C
NS3 -
Actin -
(70 kDa)
DMSO
JFH1 infection –
––
+
––
+
++
+
–+
Z-TMS, 1 μmol/L
1 2 3 4E
1
NS5B/Actin:
2 3 4 5 6 7 8 9 10 11
05
101520253035404550
Untreated
Huh7.5control
*DMSO
**Z-TMS
(1 µmol/L)
1.0 0.85 0.66 0.40 0.16 0.16 1.0 0.90 0.85 1.55 1.65
0 0.05 0.1
Z-TMS, µmol/L DMSO (Control)
0.5 1.0 2.5 0.05 0.1 0.5 1.0 2.5
NS5B(68 kDa)
HC
V R
NA
cop
ynu
mbe
rs ×
105
Actin(42 kDa)
Figure 1.
Determination of dose response of Z-TMS for the inhibition of HCV replication and evaluation of cytotoxicity. A, Huh7 hepatoma cells expressing HCV-1b replicon(FCA4)were treated for 48hourswith varying amounts of Z-TMS (lanes 2–6) orDMSO (lanes 7–11). The total lysateswere subjected toWestern blot analysis forNS5B.Lane 1, untreated control. The NS5B band intensities in each lane were quantitated using GelQuant, and NS5B to actin ratios were calculated. The results arerepresentative of three independent experiments. B and C, determination of cytotoxicity of Z-TMS (at 0.1 to 2.5 mmol/L) or corresponding DMSO using cell viabilityassay for FCA4 cells or human hepatocytes cultured on collagen 1–coated plates (P < 0.02). Each treatment was carried out in triplicates, and data arepresented as mean � SD. D, Z-TMS inhibits replication of HCV-2a (JFH1). Huh7.5 cells in 12-well culture plates were infected with JFH1 virus (HCVcc) for 48 hours.Subsequently, the cells were treated with Z-TMS (1 mmol/L) or vehicle in triplicates for the next 48 hours. The HCVcc-infected cells (untreated, solid black bar) wereconsidered as positive control, whereas untreated parent Huh7.5 cells (Huh7.5 control) served as negative control for detection of HCV RNA by qRT-PCR. The HCVRNA copy numbers per microgram of total RNAs in Z-TMS–treated cells (hatched bar) were compared with DMSO-treated (gray bar) and untreated (black bar)samples. The data are presented as mean � SD; � , P < 0.05 and �� , P < 0.0001, respectively. E, Western blot analysis for detection of NS3 in total lysates ofthe Z-TMS–treated and untreated HCVcc-infected cells using well-characterized monoclonal anti-NS3 antibody.
Nguyen et al.
Cancer Res; 76(16) August 15, 2016 Cancer Research4890
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

erlotinib, an EGFR inhibitor, diminishes HCV entry into cells andreduces HCV replication in a mouse model (20). Because of thelack of an EGFR-mutant hepatoma model, we used a well-char-acterized erlotinib-resistant lung adenocarcinoma (NSCLC)H1975 cells that contains the T790M gatekeeper mutation inEGFR to determine the effect of Z-TMS on these cells. As shownin Fig. 5A, Z-TMS significantly reduced survival of H1975 cells inthe 0.1 mmol/L to 1.0 mmol/L range within 48 hours, whereaserlotinib failed to reduce cell survival even though it was fullyactive against the wild-type EGFR kinase domain (aa 695–1210; Fig. 5A and B). The luciferase-based EGFR activity assaysuggests that erlotinib efficiently inhibited (90%) the kinaseactivities, whereas Z-TMS failed to exhibit strong inhibition inspite of reducing H1975 survival. Confocal immunostainingclearly revealed that only Z-TMS but not erlotinib induced micro-
tubule bundling (Fig. 5C, middle). Unlike the intense colocaliza-tion of DCLK1 with microtubules in DCLK1-overexpressing hep-atoma cells (Fig. 2F), we observed mostly punctate staining ofDCLK1 in H1975 probably due to alternatively spliced or post-translationally modified forms that do not preferentially bindmicrotubules (Fig. 5C).
To understand the mechanism of Z-TMS–induced cell death,H1975 cells were cultured in a 96-well plate and treated with Z-TMS (1 mmol/L) in quadruplets. After fixing the cells, nucleiwere stained and the extent of nuclear fragmentation wasassessed. The data suggest that Z-TMS induces nuclear fragmen-tation in nearly 70% to 80% cells as compared with theuntreated or DMSO or cisplatin (50 mmol/L) treated controls(Fig. 5D). Total lysates of H1975 cells treated with the drugs asdescribed above showed activation of autophagy markers,
C
D
EB
A
F
0 24 48 72
Untreated
DMSO
Z-TMS (1 μmol/L)
Time, h
Patient liver tissues
Cirrhosis Normal liver Cirrhosis HCC
0.65 cm3 4.1 cm3 4.4 cm3 4.5 cm3 Tumor size: Huh7-derived tumors stained for DCLK1 (brown)
Normal mouse liver stained for DCLK1
DCLK1 (brown)
DMSO (vehicle control)
TMS (1 μmol/L)
DCLK1 α-Tubulin Merged,
nucleus (blue)
Untreated (control)
10 μm 10 μm 10 μm
10 μm 10 μm 10 μm
10 μm 10 μm 10 μm
Days
Surv
ival
per
cent
age
Normalized DCLK1 expression:
- 0.64–0.67 (medium expression, n = 120) >0.67 (high expression, n = 127)
< - 0.64 (low expression, n = 122)
Untreate
d
DMSOZ-TMS
(1 mm
ol/L)
- NS5B
HCV+DCLK1+ Cells
- Actin
1 2 3
Figure 2.
Z-TMS exhibits anti-HCV and antitumor activities by interfering with DCLK1-microtubules dynamics. A, immunohistochemical staining showing DCLK1's extensiveexpression (brown staining) in the livers of HCV-positive patientswith cirrhosis and HCC (20 cases studied). Blue, nucleus.B,Kaplan–Meier plot showing progressivedecrease in survival rates of HCC patients at low (green line), medium (black line) and high (red line) DCLK1 expression levels. The DCLK1 expressiondata were normalized by subtracting mean expression from individual values. C, immunohistochemical staining of Huh7 cell-derived tumors for DCLK1 expression.For tumor xenografts, each nude mouse received one million cultured Huh7 cells per injection on the flanks as reported previously (34). D, Z-TMS inhibits FCA4-derived HCVþDCLK1þ cells. These cells represent HCV subgenomic replicon–expressing FCA4 cells that overexpress human DCLK1 tagged with RFP at N-terminus(DCLK1-RFP) and treated with Z-TMS (1 mmol/L, lane 3) or DMSO (lane 2) for 48 hours. NS5B levels were analyzed by Western blot analysis in the totalcell lysates. Lane 1, untreated control. E, Z-TMS inhibits HCVþDCLK1þ cell migration. The cells were treated with Z-TMS or DMSO as indicated inwound-healing assay.The space between two broken yellow lines in each sample image indicates the extent of gap/wound. F, confocal microscopy of HCVþDCLK1þ cells (top)after staining for a-tubulin (green) and nucleus (blue). Yellow, colocalization of RFP-DCLK1 (red) with microtubules (green). Unlike controls (top and middle),bundling of microtubules and sequestration of DCLK1 in the microtubule bundles (yellow, extreme right, bottom) are evident in Z-TMS–treated cells.
Antiviral and Antitumor Activities of Z-TMS
www.aacrjournals.org Cancer Res; 76(16) August 15, 2016 4891
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

LC3B-I and LC3B-II proteins in Z-TMS–treated cell lysate (Fig.5E, lane 3), which were much higher than the correspondingcontrols (lanes 1, 2 and 4). Similar Western blot analysissuggested that only cisplatin, but not Z-TMS, induces cleavedcaspase-3 (Asp175), which marks cell death by apoptosis (Fig.5F). Thus, Z-TMS appears to induce H1975 cell death byautophagy and nuclear fragmentation.
Z-TMS protects liver from DEN/CCl4-induced injury, reducesDCLK1þ cell number at injury sites, and promotes hepaticrecovery
The scheduled administration of DEN (one injection) fol-lowed by twice-weekly injections of carbon tetrachloride(CCl4) induces liver injury that further progresses to fibrosisand HCC within 8 to 10 months (40–42). We treated immu-nocompetent C57BL/6 mice with two DEN (25 mg/kg BW)injections once a week followed by administration of CCl4 (1mL/kg BW) alone or with Z-TMS (20 or 40 mg/kg BW) twice perweek for 7 weeks (groups 1 through 3 in Table 1; Fig. 6A). Asexpected, the DEN/CCl4–treated mice developed liver injurycharacterized by histologic perturbations and appearance ofnonepithelial cells in the parenchyma (Fig. 6A, extreme leftpanels). These regions also exhibited unusually high numbersof DCLK1þ cells with intense staining in epithelial and none-pithelial compartments at the injury sites (only two liversections from different mice of the same group are shown intop and bottom). This observation suggests that DEN/CCl4–ledinjury significantly induces DCLK1 expression in liver(highlighted in Fig. 6B). The untreated control (normal) micelivers were largely negative for DCLK1 stain or occasionallyrevealed a fewer DCLK1þ cells within portal triads (extremeright). The mice treated with Z-TMS (groups 2 and 3), whichwere simultaneously receiving DEN/CCL4 doses, exhibitedimproved histologic appearance with significantly reduced
number of DCLK1þ cells as compared with group 1 (DEN/CCl4 treated, Fig. 6A). Both histologic and liver function panel(ALB, ALT, AST, ALKP, and TBIL in Table 1) data clearly suggestthat Z-TMS alone (group 4) does not exhibit hepatotoxicityunder these treatment conditions. Instead, Z-TMS successfullyprotected the liver from toxic agents and improved injury mostlikely by eliminating or suppressing DCLK1þ cells. Mice in anygroup did not lose their body weight.
DiscussionViral hepatitis, steatohepatitis, and metabolic disorders sub-
stantially contribute to the development of cirrhosis and pri-mary HCC. End-stage liver disease due to chronic HCV infec-tion is expected to remain a major health care issue in mostcountries partly due to lack of effective treatment options orinaccessibility to newly discovered drugs. Current HCC anti-neoplastic drugs, sorafenib alone or in combination with otherdrugs, cause considerable toxicity and only improve medianoverall survival by 3 months. Here, we have reported novelproperties of Z-TMS that exerts its antiviral and antitumoractivities by interference with the CSC marker DCLK1, micro-tubule dynamics, induction of autophagy, G2–M arrest andnuclear fragmentation. The combined effects reflect in vitroefficacy of Z-TMS against the drug-resistant tumor cells suchas NSCLC. Z-TMS also promotes hepatic recovery from exten-sive DEN (genotoxic)/CCl4 (hepatotoxic) induced liver injuryin immunocompetent C57BL mice. Thus, Z-TMS may poten-tially block initiation and progression of HCC by targetingDCLK1. This notion is also supported by our observation thatDCLK1 downregulation results in reduction of hepatoma-liketumor growth (43). Although Z-TMS at doses 20 and 40 mg/KgBW did not exhibit hepatic toxicity, 20% mice showed com-plications in gastrointestinal emptying. These observations
H&E Staining
NS5A-GFP
CK19 (brown)
DCLK1 (brown)
A
Untreated DMSO Z-TMS (1 μmol/L) B
10 μm
3D culture of GS5
Figure 3.
Z-TMS inhibits hepatoma cell growth in3Dcell culturemodel.A, characterizationof spheroids/aggregates derived fromGS5 cells (1 million) that were developedin 3 weeks by magnetic levitationmethod. Immunohistochemical staining(H&E andCK19) of the aggregates showscell-to-cell-contacts. Both DCLK1þ andDCLK1� staining was observed,indicating heterogeneity of cells in theaggregates. Blue, nuclear staining. Inset,live image of the same spheroid/aggregates shows expression of HCVNS5A-GFP (green). B, effects of Z-TMSon spheroid growth in a 3D culturemodel. GS5 spheroids/aggregates weregrown as described above for 2 weeksand treated with DMSO or Z-TMS (1mmol/L) or untreated. The visible cellmasses were photographed 4 weeksafter treatment. This experiment wasrepeated once and a representativephotograph is shown.
Nguyen et al.
Cancer Res; 76(16) August 15, 2016 Cancer Research4892
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

warrant us for optimizing drug dosages and duration of treat-ment to gain its maximum health benefits.
Using subgenomic replicons and full-length JFH1 infectionmodels of HCV, we have demonstrated the efficacy of Z-TMSagainst widely prevalent HCV genotypes 1 and 2. The magneticlevitation experiments revealed that growth of HCV-expressingspheroids/aggregates could also be effectively targeted by Z-TMS. The heterogeneity of this cellular mass and cell-to-cellcontacts in the spheroids were revealed by immunohistochem-ical staining showing membranous CK19. It further showedexpected DCLK1þ subpopulations (usually 1%–2% of totalGS5 cells; ref. 15). Our in vivo experiments suggest that Z-TMScan diminish the DCLK1þ population in injured livers. BecauseDCLK1 appears to be involved in HCV replication and hepaticmalignancy (15, 16, 43), it is likely that Z-TMS will be able toeliminate HCV-expressing cancer stem–like cells to preventprogression of liver diseases.
Although normal liver parenchyma lacks detectable DCLK1expression, DCLK1 expression and number of DCLK1þ cells areincreased significantly in the stroma, regenerative cirrhoticnodules, and HCC. Z-TMS clearly targeted DCLK1-microtubuledynamics that promotesHCV replication, cellmigration, and cell-cycle progression. Microtubule-stabilizing drugs (paclitaxel anddocetaxel) and destabilizing drugs (vinblastine and nocodazole)have been extensively used for the treatment of cancer (44, 45). Afew of these drugs have also been shown to hamper movement oftheHCV replication complexes required for viral replication (46).
By sequestering DCLK1 with bundled microtubules, Z-TMS willblock survival, proliferation, and division of DCLK1þ CSC cells.
Cancer/tumor stem cells (CSC) are key contributors of drugresistance, metastasis, and recurrence of tumors. At present, effec-tively targeting CSCs for treatment is challenging (18, 19). Wepreviously demonstrated that HCV induces several CSC markers(CD133, Lgr5, and c-Myc), including DCLK1 (47, 48). Ourcurrent data revealed thatDCLK1 overexpression inHCC-positivepatients considerably reduces survival rate. Z-TMS causes seques-tration of DCLK1 with microtubule bundles accompanied by adramatic decrease in theNS5B polymerase level inHCVþDCLK1þ
hepatoma cells. Z-TMS appears to be effective against DCLK1-positive CSCs. DCLK1 has been shown to play important roles inthe development of intestinal polyps, intestinal response toradiation injury, cell survival, and control of metastasis. In addi-tion, we have shown that DCLK1 positively regulates HCV rep-lication in knockdown andoverexpression systems. Thus, Z-TMS–targeted elimination of HCV-positive cells bearing CSCs foot-prints is likely to benefit patients with advanced liver diseases,including HCC.
The molecular mechanisms of Z-TMS's antiproliferative effectswere also studied. We observed that Z-TMS treatment resulted inG2–Marrest (95%) of hepatoma cells independent ofHCVwithin48 hours. Cell-cycle progression is orchestrated by cyclins andcyclin-dependent kinases (CDK). CyclinB1/CDK1 complex spe-cifically regulates cell entry intomitosis, and enhances mitochon-drial respiration and ATP generation for G2–M transition. In
A
C
P-Akt (Ser473)-
Total Akt-
Actin-
– – +
DMSO – + +
Z-TMS (1 μmol/L)
1 2 3
- 60 kDa
- 60 kDa
- 42 kDa
B
DMSOG1 = 41.95%
G2 = 13.34%S = 44.71%
G1 = 44.82%
DebrisG2 = 12.96%S = 42.23%
G1 = 42.59%
G2 = 14.90%S = 42.50%
G1 = 42.82%
G2 = 13.99%S = 43.19%
G1 = 3.69%
00 50 100 150 200 250
200
400
600
Cou
nts
Pl Fluorescence
800
1,000
00 50 100 150 200 250
0 50 100 150 200 250 0 50 100 150 200 250
200
400
600
Cou
nts
800
1,000
00 50 100 150 200 250
200
400
600
800
1,000
0
200
400
600C
ount
sUntreated
Huh 7.5 Cells GS5 Cells
DMSO(Control)
Z-TMS(1.0 mmol/L)
800
1,000
0
200
400
600
800
1,000
00 50 100 150 200 250
200
400
600
Pl Fluorescence
800
1,000
G2 = 93.75%S = 2.56%
G1 = 3.43%
G2 = 94.13%S = 2.45%
– – +
– + +
Z-TMS (1 μmol/L)
p21Cip1/waf1
Total CDK1
Actin
34 kDa
21 kDa
42 kDa
1 2 3
Figure 4.
Z-TMS induces cell-cycle arrest at G2–M phase that is accompanied by the activation of p21Cip1/waf1, downregulation of CDK1, and dephosphorylation of Akt. A, theGS5-cultured cells well treated with 1 mmol/L of Z-TMS or DMSO (control, vehicle) for 48 hours and subjected to cell-cycle analysis following treatment with PI.B and C, Western blot analysis for Z-TMS–led inhibition of signals that promote cell-cycle progression and cell survival in GS5 cells treated with Z-TMS(lane 3) or vehicle (lane 2). Detection of p21Cip1/waf1 and total CDK1 (B) or activated Akt [determined by P-Akt (Ser473)] and total Akt (C). In each case, untreated cellswere considered as regular (uninhibited) control. Actin band in each lane was used as a loading control. The experiments were repeated three times andrepresentative data are shown.
Antiviral and Antitumor Activities of Z-TMS
www.aacrjournals.org Cancer Res; 76(16) August 15, 2016 4893
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

accordance with these observations, we observed a considerabledecrease in total CDK1 and a concomitant increase in the cell-cycle inhibitor, p21Cip/Waf1, following Z-TMS treatment. Theobserved p21Cip/Waf1 induction after Z-TMS treatments resulted
in inhibition of CDK1 activities and cell-cycle arrest. Akt activa-tion downstream of the PI3K/Akt/mTOR pathway regulates mul-tiple cellular processes such as cell growth, CSC survival, metab-olism, angiogenesis, and proliferation. Phosphorylation of Akt at
C
D
E F
A
B
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
Control Z-TMS Erlotinib
EGFR
kin
ase
activ
ities
(in
RLU
)
- LC3B-I (16 kDa)
- LC3B-II (14 kDa)
Untreate
d
DMSO
Z-TMS
Cisplat
in
- Actin (42 kDa)
1 2 3 4
Untre
ated
DMSO
Z-TMS
Cisplat
in
Cleaved caspase-3 - 17 kDa
- 19 kDa
- Actin (42 kDa)
1 2 3 4
**
*
Nuclear staining with DRAQ5 (red)
α-Tubulin DCLK1
Untreated
Untreated DMSO
Z-TMS, (1 μmol/L)
Z-TMS (1 μmol/L) Cisplatin (50 μmol/L)
Erlotinib, (1 μmol/L)
Merged, nucleus (blue)
10 μm 10 μm 10 μm
10 μm
10 μm
10 μm
10 μm 10 μm
10 μm
0
20
40
60
80
100
0 0.05 0.1 0.5 1 2.5 5
DMSO TMS Erlo�nib
Z-TMS (μmol/L)
Perc
ent c
ell v
iabi
lity
Z-TMS
Erlotinib
DMSO
Figure 5.
Z-TMS inhibits viability of erlotinib-resistant NSCLCs (H1975) bearing the T790M mutation via autophagy and nuclear fragmentation. A, the cells were treated withvarying amounts of Z-TMS, erlotinib or DMSO for 48 hours and subjected to MTS cell viability assay. The experiment was repeated three times and average� SDwasplotted (P < 0.002). B, the kinase activity was measured using ADP-Glow kinase assay for human EGFR (aa 695–1210) and expressed as relative luciferaseunit (RLU). The data are presented as mean� SD; � , P < 0.05 and �� , P < 0.01, respectively. C, confocal microscopy of H1975 cells treated with 1 mmol/L of Z-TMS orerlotinib (middle and bottom, respectively) for 48 hours and stained by immunofluorescence staining protocol for a-tubulin (red) and DCLK1 (green).Blue, nucleus. The untreated cells were used as a control (top). A representative staining pattern for the localization of DCLK1 and microtubules is shown here.D, a representative scanned field image of Z-TMS–treated and untreated H1975 cells following staining with DRAQ5 (red, nucleus). Each treatment was done inquadruplets and each well was analyzed for 5 different fields. E and F, Western blot analysis for Z-TMS–treated (lane 3) and control (lanes 2 and 3) H1975 celllysates probed for LC3B or cleaved caspase-3 (Asp175). Presence of LC3B-II indicates autophagy (E, lane 3). Cisplatin-treated cells were used as a positivecontrol for the apoptosis marked by cleaved caspase-3 (F, lane 4).
Table 1. Determination of hepatotoxicity in Z-TMS–treated and -untreated C57BL mice by measuring serum markers after euthanizing the animals
ALB ALT AST ALKP TBILNormal range 2.5–4.8 28–132 59–247 62–209 0.1–0.9
Group 1 DEN þ CCl4 2.6 � 0.1 78.6 � 15.8 132.2 � 24.6 90.6 � 15.1 0.9 � 0.2Group 2 DEN þ CCl4 þ Z-TMS (20 mg/kg BW) 2.5 � 0.1 60.0 � 12.0 164.3 � 85.1 108.3 � 10.1 0.6 � 0.05Group 3 DEN þ CCl4 þ Z-TMS (40 mg/kg BW) 2.4 � 0.3 109.0 � 17.0 213.5 � 84.5 144.5 � 25.5 0.7 � 0.1Group 4 Z-TMS (40 mg/kg BW) 2.6 � 0.3 50.7 � 6.1 128.7 � 15.4 52.3 � 16.2 0.9 � 0.6Group 5 DMSO (40 mg/kg BW) 2.7 � 0.1 50.5 � 5.3 234.0 � 42.6 119.0 � 11.9 0.6 � 0.1Group 6 Untreated control 2.8 � 0.1 49.0 � 3.4 232.0 � 66.9 135.7 � 5.8 0.5 � 0.1
Abbreviations: ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALKP, alkaline phosphatase; TBIL, total bilirubin.
Nguyen et al.
Cancer Res; 76(16) August 15, 2016 Cancer Research4894
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

Ser473 by mTORC2 is required for its hyperactivation and stabi-lization of its active conformation. We observed a considerableinhibition of Akt (Ser473) phosphorylation following Z-TMStreatment. In addition, Z-TMS induced autophagy that wasaccompanied by nuclear fragmentation. These properties areespecially desirable for the treatment of hard-to-treat drug-resis-tant cancers.
In conclusion, the results presented here collectively sup-port Z-TMS as a unique potent anti-HCV and antitumor drugthat exerts its effects by targeting multiple pathways. Z-TMSsignificantly reduces DCLK1þ CSC populations during hepaticinjury, interferes with DCLK1-microtubule dynamics, arrestscell cycle at G2–M phase, promotes autophagy, and causesnuclear fragmentation. Thus, Z-TMS potentially overridesNSCLC resistance to erlotinib because of its unique mechan-isms of action.
Disclosure of Potential Conflicts of InterestS. Surebanhas ownership interest (including patents) in patents.M.S. Bronze
is a consultant/advisory board member for Genentech/Roche. C.W. Houchenhas ownership interest (including patents) and is a consultant/advisory boardmember for COARE Biotechnology Inc. No potential conflicts of interest weredisclosed by the other authors.
Authors' ContributionsConception and design: C.B. Nguyen, H. Kotturi, G. Waris, A. Mohammed,C.W. Houchen, N. AliDevelopment of methodology: C.B. Nguyen, H. Kotturi, A. Mohammed,C.W. Houchen, N. Ali
Acquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): C.B. Nguyen, H. Kotturi, G. Waris, A. Mohammed,N. AliAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): C.B. Nguyen, H. Kotturi, G. Waris, A. Mohammed,P. Chandrakesan, S. Sureban, D. Qu, C.V. Rao, N. AliWriting, review, and/or revision of the manuscript: C.B. Nguyen, H. Kotturi,A. Mohammed, M.S. Bronze, C.W. Houchen, N. AliAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases):H.Kotturi, R.May, N.Weygant, D.Qu, C.V. Rao,D.N. Dhanasekaran, N. AliStudy supervision: H. Kotturi, A. Mohammed, C.W. Houchen, N. Ali
AcknowledgmentsThe authors are thankful to the Liver Tissue Cell Distribution System,
(Minneapolis, MN). We thank Stephenson Cancer Center Pathology CoreLaboratory for immunohistochemistry.
Grant SupportThis work was partially supported by VA Merit Award and the Frances
and Malcolm Robinson Endowed Chair (C.W. Houchen). N. Ali is par-tially supported by an Institutional Development Award (IDeA) from NIH(1P20GM103639NIH) and COMAA Research Fund Seed Grant (OUHSC).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received October 2, 2015; revised May 20, 2016; accepted June 5, 2016;published OnlineFirst June 10, 2016.
+DEN/CCL4+DEN/CCL4 +Z-TMS (20 mg/kg BW)
+DEN/CCL4 +Z-TMS (40 mg/kg BW)
+Z-TMS (40 mg/kg BW)
Untreated Control
1
2
B
1 2
DCLK1and nucleus
Mouse liver stained for DCLK1 andnucleus
A
Group 1 Group 2 Group 3 Group 4 Group 5
Figure 6.
Z-TMS protects liver from DEN/CCl4-induced injury by downregulating DCLK1 expression and promoting normal healing in C57BL mice. A, immunohistochemicalstaining for DCLK1 (brown) in the liver of mice receiving DEN/CCl4 alone (group 1) or with Z-TMS (group 2, 3). Group 4 received only Z-TMS, whereas group 5received no treatment (na€�ve control). Each group had 5 mice kept under similar conditions. The representative staining results for two different mice(1 and 2) within each group are shown. DEN/CCl4-induced liver injury sites (arrows) were highly enriched in DCLK1þ cells. However, similar areas had fewer orno DCLK1þ cells following treatment with Z-TMS (groups 2 and 3). B, �60 images of the representative mice 1 and 2 [þDEN/CCl4 panel, group 1] showingDCLK1þ cells with intense staining.
Antiviral and Antitumor Activities of Z-TMS
www.aacrjournals.org Cancer Res; 76(16) August 15, 2016 4895
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

References1. Yang JD, Roberts LR. Hepatocellular carcinoma: a global view. Nat Rev
Gastroenterol Hepatol 2010;7:448–58.2. Bartosch B, Thimme R, Blum HE, Zoulim F. Hepatitis C virus-induced
hepatocarcinogenesis. J Hepatol 2009;51:810–20.3. El-SeragHB. Epidemiology of viral hepatitis and hepatocellular carcinoma.
Gastroenterology 2012;142:1264–73.4. Afdhal N, Reddy KR, Nelson DR, Lawitz E, Gordon SC, Schiff E, et al.
Ledipasvir and sofosbuvir for previously treatedHCV genotype 1 infection.N Engl J Med 2014;370:1483–93.
5. Afdhal N, Zeuzem S, Kwo P, ChojkierM, Gitlin N, PuotiM, et al. Ledipasvirand sofosbuvir for untreated HCV genotype 1 infection. N Engl J Med2014;370:1889–98.
6. Bertino G, Demma S, Ardiri A, Proiti M, Gruttadauria S, Toro A, et al.Hepatocellular carcinoma: novel molecular targets in carcinogenesis forfuture therapies. BioMed Res Int 2014;2014:203693.
7. Padhya KT, Marrero JA, Singal AG. Recent advances in the treatment ofhepatocellular carcinoma. Curr Opin Gastroenterol 2013;29:285–92.
8. Llovet JM, Ricci S,Mazzaferro V,Hilgard P, Gane E, Blanc JF, et al. Sorafenibin advanced hepatocellular carcinoma. N Engl J Med 2008;359:378–90.
9. Gauthier A, Ho M. Role of sorafenib in the treatment of advanced hepa-tocellular carcinoma: an update. Hepatol Res 2013;43:147–54.
10. ChowAK,Ng L, LamCS,Wong SK,Wan TM,ChengNS, et al. The Enhancedmetastatic potential of hepatocellular carcinoma (HCC) cells with sora-fenib resistance. PLoS ONE 2013;8:e78675.
11. Chen KF, Chen HL, Tai WT, FengWC, Hsu CH, Chen PJ, et al. Activation ofphosphatidylinositol 3-kinase/Akt signaling pathway mediates acquiredresistance to sorafenib in hepatocellular carcinoma cells. J Pharmacol ExpTher 2011;337:155–61.
12. Kasai T, Chen L,Mizutani A, Kudoh T,MurakamiH, Fu L, et al. Cancer stemcells converted from pluripotent stem cells and the cancerous niche. J StemCells Regen Med 2014;10:2–7.
13. Majumdar A, Curley SA, Wu X, Brown P, Hwang JP, Shetty K, et al. Hepaticstem cells and transforming growth factor beta in hepatocellular carcino-ma. Nat Rev Gastroenterol Hepatol 2012;9:530–8.
14. Yamashita T, Wang XW. Cancer stem cells in the development of livercancer. J Clin Invest 2013;123:1911–8.
15. Ali N, Allam H, May R, Sureban SM, Bronze MS, Bader T, et al. Hepatitis Cvirus-induced cancer stem cell-like signatures in cell culture and murinetumor xenografts. J Virol 2011;85:12292–303.
16. Ali N, Allam H, Bader T, May R, Basalingappa KM, Berry WL, et al.Fluvastatin interferes with hepatitis C virus replication via microtubulebundling and a doublecortin-like kinase-mediatedmechanism. PLoSONE2013;8:e80304.
17. WeygantN,QuD, BerryWL,MayR,ChandrakesanP,OwenDB, et al. Smallmolecule kinase inhibitor LRRK2-IN-1 demonstrates potent activityagainst colorectal and pancreatic cancer through inhibition of doublecor-tin-like kinase 1. Mol Cancer 2014;13:103.
18. Jung Y, Kim WY. Cancer stem cell targeting: are we there yet? Arch PharmRes 2015;38:414–22.
19. Zhou BB, Zhang H, Damelin M, Geles KG, Grindley JC, Dirks PB. Tumour-initiating cells: challenges and opportunities for anticancer drug discovery.Nat Rev Drug Discov 2009;8:806–23.
20. Lupberger J, Zeisel MB, Xiao F, Thumann C, Fofana I, Zona L, et al. EGFRand EphA2 are host factors for hepatitis C virus entry and possible targetsfor antiviral therapy. Nat Med 2011;17:589–95.
21. Diao J, Pantua H, NguH, Komuves L, Diehl L, Schaefer G, et al. Hepatitis Cvirus induces epidermal growth factor receptor activation via CD81 bind-ing for viral internalization and entry. J Virol 2012;86:10935–49.
22. Tresguerres IF, Tamimi F, Eimar H, Barralet J, Torres J, Blanco L, et al.Resveratrol as anti-aging therapy for age-related bone loss. RejuvenationRes 2014;17:439–45.
23. Singh CK, George J, Ahmad N. Resveratrol-based combinatorial strategiesfor cancer management. Ann N Y Acad Sci 2013;1290:113–21.
24. Li J, Chong T,Wang Z, ChenH, LiH, Cao J, et al. A novel anticancer effect ofresveratrol: reversal of epithelialmesenchymal transition in prostate cancercells. Mol Med Rep 2014;10:1717–24.
25. Liu B, Zhou Z, Zhou W, Liu J, Zhang Q, Xia J, et al. Resveratrol inhibitsproliferation in human colorectal carcinoma cells by inducing G1/Sphasecell cycle arrest and apoptosis through caspase/cyclinCDK pathways. MolMed Rep 2014;10:1697–702.
26. KaoCL,Huang PI, Tsai PH, TsaiML, Lo JF, Lee YY, et al. Resveratrol-inducedapoptosis and increased radiosensitivity in CD133-positive cells derivedfrom atypical teratoid/rhabdoid tumor. Int J Radiat Oncol Biol Phys2009;74:219–28.
27. Borriello A, Bencivenga D, Caldarelli I, Tramontano A, Borgia A, Zappia V,et al. Resveratrol: from basic studies to bedside. Cancer Treat Res 2014;159:167–84.
28. MacRaeWD, Towers GH. An ethnopharmacological examination of Virolaelongata bark: a South American arrow poison. J Ethnopharmacol1984;12:75–92.
29. Schneider Y, Chabert P, Stutzmann J, Coelho D, Fougerousse A, Gosse F,et al. Resveratrol analog (Z)-3,5,40-trimethoxystilbene is a potent anti-mitotic drug inhibiting tubulin polymerization. Int J Cancer 2003;107:189–96.
30. Chabert P, Fougerousse A, Brouillard R. Anti-mitotic properties of resver-atrol analog (Z)-3,5,40-trimethoxystilbene. BioFactors 2006;27:37–46.
31. Lin HS, Zhang W, Go ML, Choo QY, Ho PC. Determination of Z-3,5,40-trimethoxystilbene in rat plasma by a simple HPLCmethod: applicationin a pre-clinical pharmacokinetic study. J Pharm Biomed Anal 2010;53:693–7.
32. Guo JT, Bichko VV, Seeger C. Effect of alpha interferon on the hepatitis Cvirus replicon. J Virol 2001;75:8516–23.
33. Nelson HB, Tang H. Effect of cell growth on hepatitis C virus (HCV)replication and a mechanism of cell confluence-based inhibition of HCVRNA and protein expression. J Virol 2006;80:1181–90.
34. Ali N, Chandrakesan P, Nguyen CB,Husain S, Gillaspy AF, HuyckeM, et al.Inflammatory and oncogenic roles of a tumor stem cell marker double-cortin-like kinase (DCLK1) in virus-induced chronic liver diseases. Onco-target 2015;6:20327–44.
35. Iqbal J, McRae S, Banaudha K, Mai T, Waris G. Mechanism of hepatitis Cvirus (HCV)-induced osteopontin and its role in epithelial to mesenchy-mal transition of hepatocytes. J Biol Chem 2013;288:36994–7009.
36. Novelle MG, Wahl D, Dieguez C, Bernier M, de Cabo R. Resveratrolsupplementation: where are we now and where should we go? AgeingRes Rev 2015;21C:1–15.
37. Baur JA, Pearson KJ, Price NL, Jamieson HA, Lerin C, Kalra A, et al.Resveratrol improves health and survival of mice on a high-calorie diet.Nature 2006;444:337–42.
38. Souza GR, Molina JR, Raphael RM, Ozawa MG, Stark DJ, Levin CS, et al.Three-dimensional tissue culture based on magnetic cell levitation. NatNanotechnol 2010;5:291–6.
39. Kandel ES, Skeen J,MajewskiN,Di Cristofano A, Pandolfi PP, FelicianoCS,et al. Activation of Akt/protein kinase B overcomes a G(2)/m cell-cyclecheckpoint induced by DNA damage. Mol Cell Biol 2002;22:7831–41.
40. Uehara T, Ainslie GR, Kutanzi K, Pogribny IP, Muskhelishvili L, Izawa T,et al. Molecular mechanisms of fibrosis-associated promotion of livercarcinogenesis. Toxicol Sci 2013;132:53–63.
41. Dapito DH, Mencin A, Gwak GY, Pradere JP, Jang MK, Mederacke I, et al.Promotion of hepatocellular carcinoma by the intestinal microbiota andTLR4. Cancer Cell 2012;21:504–16.
42. Caviglia JM, Schwabe RF. Mouse models of liver cancer. Methods Mol Biol2015;1267:165–83.
43. Sureban SM, Madhoun MF, May R, Qu D, Ali N, Fazili J, et al. PlasmaDCLK1 is a marker of hepatocellular carcinoma (HCC): targeting DCLK1prevents HCC tumor xenograft growth via a microRNA-dependent mech-anism. Oncotarget 2015;6:37200–15.
44. Yang H, Ganguly A, Cabral F. Inhibition of cell migration and cell divisioncorrelates with distinct effects ofmicrotubule inhibiting drugs. J Biol Chem2010;285:32242–50.
45. Kavallaris M. Microtubules and resistance to tubulin-binding agents. NatRev Cancer 2010;10:194–204.
46. Lai CK, Jeng KS, Machida K, Lai MM. Association of hepatitis C virusreplication complexes with microtubules and actin filaments is dependenton the interaction of NS3 and NS5A. J Virol 2008;82:8838–48.
47. Lin PT, Gleeson JG, Corbo JC, Flanagan L, Walsh CA. DCAMKL1 encodes aprotein kinase with homology to doublecortin that regulates microtubulepolymerization. J Neurosci 2000;20:9152–61.
48. Kim MH, Cierpicki T, Derewenda U, Krowarsch D, Feng Y, Devedjiev Y,et al. The DCX-domain tandems of doublecortin and doublecortin-likekinase. Nat Struct Biol 2003;10:324–33.
Cancer Res; 76(16) August 15, 2016 Cancer Research4896
Nguyen et al.
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722

2016;76:4887-4896. Published OnlineFirst June 10, 2016.Cancer Res Charles B. Nguyen, Hari Kotturi, Gulam Waris, et al. Progression
Cell-CyclePathophysiology by Blocking Microtubule Dynamics and -Trimethoxystilbene Limits Hepatitis C and Cancer′(Z)-3,5,4
Updated version
10.1158/0008-5472.CAN-15-2722doi:
Access the most recent version of this article at:
Cited articles
http://cancerres.aacrjournals.org/content/76/16/4887.full#ref-list-1
This article cites 48 articles, 10 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/76/16/4887.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/76/16/4887To request permission to re-use all or part of this article, use this link
on October 9, 2020. © 2016 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 10, 2016; DOI: 10.1158/0008-5472.CAN-15-2722