YOU can reduce post-surgicalcanjsurg.ca/wp-content/uploads/2015/03/CJS_58-2.pdf · hemodynamic...
76
Canadian Association of General Surgeons Canadian Society of Surgical Oncology Canadian Association of Thoracic Surgeons Department of Surgery, Western University Department of Surgery, Dalhousie University Department of Surgery, University of Alberta Department of Surgery, University of Calgary Département de chirurgie, Université de Sherbrooke Department of Surgery, McMaster University Département de chirurgie, Université de Montréal SPONSORS Vol. 58, No. 2, April/avril 2015 canjsurg.ca A novel method for assessing visual perception of surgical planes Does more than a single chest tube for mediastinal drainage affect outcomes after cardiac surgery? Outcomes of infection following pediatric spinal fusion Canadian practice patterns for pancreaticoduodenectomy
Transcript of YOU can reduce post-surgicalcanjsurg.ca/wp-content/uploads/2015/03/CJS_58-2.pdf · hemodynamic...

Edwards Lifesciences | edwards.comOne Edwards Way | Irvine, California 92614 USASwitzerland | Japan | China | Brazil | Australia | India
32%in your moderate
to high-risk patients.
YOUcan reduce
post-surgicalcomplications
by
1
Edwards.com/ESR
References:1. Grocott et al. Perioperative increase in global blood flow to explicit defined goals and outcomes after surgery: a Cochrane systematic review.
Br J Anaesth 20132. Giglio MT, Marucci M, Testini M, Brienza N. Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery:
a meta-analysis of randomized controlled trials. Br J Anaesth 2009; 103: 637–463. Dalfino L, Giglio MT, Puntillo F, Marucci M, Brienza N. Haemodynamic goal-directed therapy and postoperative infections: earlier is better.
A systematic review and meta-analysis. Crit Care 2011; 15: R1544. Corcoran T et al. Perioperative Fluid Management Strategies in Major Surgery: A Stratified Meta-Analysis. Anesthesia – Analgesia 2012 Edwards, Edwards Lifesciences, the stylized E logo and Enhanced Surgical Recovery are trademarks of Edwards Lifesciences Corporation. All other trademarks are the property of their respective owners.
© 2014 Edwards Lifesciences Corporation. All rights reserved.
A large body of evidence demonstrates that hemodynamic optimization through Perioperative Goal-Directed Therapy (PGDT), utilizing dynamic parameters which are informative in determining fluid responsiveness, has been shown to reduce post-surgical complications.1-4
randomized controlled trials and
meta-analyses confirmedreduction of risk for AKI, anastomotic leaks,
pneumonia, SSI and UTI.1-4
When evidence inspires action, Edwards Enhanced Surgical Recovery program is here to help you implement PGDT. Your vision for reducing post- surgical complications can be realized in a single procedure, or as part of a larger initiative such as iERAS, ERAS, QIP, etc.
Canadian Association of General SurgeonsCanadian Society of Surgical Oncology
Canadian Association of Thoracic SurgeonsDepartment of Surgery, Western University
Department of Surgery, Dalhousie University
Department of Surgery, University of AlbertaDepartment of Surgery, University of CalgaryDépartement de chirurgie, Université de SherbrookeDepartment of Surgery, McMaster UniversityDépartement de chirurgie, Université de Montréal
SponSorS
Vol. 58, No. 2, April/avril 2015canjsurg.ca
A novel method for assessing visual perception of surgical planes
Does more than a single chest tube for mediastinal drainage affect outcomes after cardiac surgery?
Outcomes of infection following pediatric spinal fusion
Canadian practice patterns for pancreaticoduodenectomy

Edwards Lifesciences | edwards.comOne Edwards Way | Irvine, California 92614 USASwitzerland | Japan | China | Brazil | Australia | India
32%in your moderate
to high-risk patients.
YOUcan reduce
post-surgicalcomplications
by
1
Edwards.com/ESR
References:1. Grocott et al. Perioperative increase in global blood flow to explicit defined goals and outcomes after surgery: a Cochrane systematic review.
Br J Anaesth 20132. Giglio MT, Marucci M, Testini M, Brienza N. Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery:
a meta-analysis of randomized controlled trials. Br J Anaesth 2009; 103: 637–463. Dalfino L, Giglio MT, Puntillo F, Marucci M, Brienza N. Haemodynamic goal-directed therapy and postoperative infections: earlier is better.
A systematic review and meta-analysis. Crit Care 2011; 15: R1544. Corcoran T et al. Perioperative Fluid Management Strategies in Major Surgery: A Stratified Meta-Analysis. Anesthesia – Analgesia 2012 Edwards, Edwards Lifesciences, the stylized E logo and Enhanced Surgical Recovery are trademarks of Edwards Lifesciences Corporation. All other trademarks are the property of their respective owners.
© 2014 Edwards Lifesciences Corporation. All rights reserved.
A large body of evidence demonstrates that hemodynamic optimization through Perioperative Goal-Directed Therapy (PGDT), utilizing dynamic parameters which are informative in determining fluid responsiveness, has been shown to reduce post-surgical complications.1-4
randomized controlled trials and
meta-analyses confirmedreduction of risk for AKI, anastomotic leaks,
pneumonia, SSI and UTI.1-4
When evidence inspires action, Edwards Enhanced Surgical Recovery program is here to help you implement PGDT. Your vision for reducing post- surgical complications can be realized in a single procedure, or as part of a larger initiative such as iERAS, ERAS, QIP, etc.
cover-cjsapr15.indd 1 2015-03-10 9:02 AM

canjsurg.ca
©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 73
EDITORIAL • ÉDITORIAL
77 Medical memorialization V. McAlister
78 La commémoration médicale V. McAlister
COMMENTARIES • COMMENTAIRES
80 Dr. Bernard Langer — inductee into the Canadian Medical Hall of Fame P.D. Greig, O.D. Rotstein
83 Amnesia in modern surgery: revisiting Wangensteen’s landmark studies of small bowel obstruction A. Faryniuk, A. MacDonald, P. van Boxel
85 Endovenous radiofrequency ablation for the treatment of varicose veins A. Kayssi, M. Pope, I. Vucemilo, C. Werneck
RESEARCH • RECHERCHE
87 A novel method for assessing visual perception of surgical planes C.M. Schlachta, S. Ali, H. Ahmed, R. Eagleson
92 The integration of minimally invasive surgery in surgical practice in a Canadian setting: results from 2 consecutive province-wide practice surveys of general surgeons over a 5-year period J. Hallet, O. Mailloux, M. Chhiv, R.C. Grégoire, J.-P. Gagné
100 Does more than a single chest tube for mediastinal drainage affect outcomes after cardiac surgery? J. Le, K.J. Buth, G.M. Hirsch, J.-F. Légaré
107 Outcomes of infection following pediatric spinal fusion A. Khoshbin, M. Lysenko, P. Law, J.G. Wright
114 Persistent neuropathic pain after inguinal herniorrhaphy depending on the procedure (open mesh v. laparoscopy): a propensity-matched analysis P. Niccolaï, L. Ouchchane, M. Libier, F. Beouche, M. Belon, J.-M. Vedrinne, B. El Drayi, L. Vallet, F. Ruiz, C. Biermann, P. Duchêne, C. Chirat, S. Soule-Sonneville, C. Dualé, C. Dubray, P. Schoeffler
Vol. 58, No. 2, April/avril 2015canjsurg.ca
Online manuscriptsubmission and peer review
AVAILABLE at
http://mc.manuscriptcentral.com/cjs
contentscjs-apr15.indd 73 2015-03-10 1:12 PM

74 J can chir, Vol. 58, No 2, avril 2015 ©2015 8872147 Canada Inc.
121 Canadian practice patterns for pancreaticoduodenectomy D.P. Cyr, J.L. Truong, J. Lam-McCulloch, S.P. Cleary, P.J. Karanicolas
REVIEW • REVUE
128 Surgical approach in primary total hip arthroplasty: anatomy, technique and clinical outcomes S. Petis, J.L. Howard, B.L. Lanting, E.M. Vasarhelyi
DISCUSSIONS IN SURGERY DISCUSSIONS EN CHIRURGIE
140 Is obesity associated with advanced stage or grade of colon cancer? K. Neumann, S.M. Mahmud, A. McKay, J. Park, J. Metcalfe, D.J. Hochman
143 Supply versus demand: a review of application trends to Canadian surgical training programs R.E. Austin, K.R. Wanzel
© 2015 8872147 Canada Inc. ISSN 0008-428X. For information on permis-sion to reproduce material from the Canadian Journal of Surgery (CJS) see canjsurg.ca.
All editorial matter in CJS represents the opinions of the authors and not necessarily those of the publisher. We assume no responsibility or liability for damages arising from any error or omission or from the use of any information or advice contained in CJS, including articles, editorials, reviews, letters and advertisements. All reproduction rights are reserved.
Printed by Dollco Integrated Print Solutions, Ottawa. Appears in February, April, June, August, October and December.
Return undeliverable Canadian copies to the CMA Member Service Centre, 1870 Alta Vista Dr., Ottawa ON K1G 6R7 (email [email protected]).
© 2015 8872147 Canada Inc. ISSN 0008-428X. Pour obtenir des renseigne-ments au sujet des permissions à obtenir afin de reproduire des extraits du Journal canadien de chirurgie (JCC), consulter canjsurg.ca.
Tous les articles à caractère éditorial dans le JCC représentent les opi nions de leurs auteurs, qui ne sont pas nécessairement celles de l’éditeur. Nous n’assumons aucune respon sabilité pour les dommages résultant de toute erreur ou omission, ou de l’utilisation de renseignements ou de conseils contenus dans le JCC, y compris les articles, éditoriaux, revues, lettres et annonces. Tous droits de reproduction réservés.
La revue est imprimée par Dollco Integrated Print Solutions, Ottawa. Elle paraît en février, avril, juin, août, octobre et décembre.
Retournez toutes copies canadiennes non livrées au Centre des ser vices aux membres, Association médicale canadienne, 1870, prom. Alta Vista, Ottawa (Ontario) K1G 6R7 (courriel : [email protected]).
contentscjs-apr15.indd 74 2015-03-10 1:12 PM

©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 75
COEDITORS CORÉDACTEURS
Edward J. Harvey, MD, Montréal [email protected]
Major Vivian C. McAlister, MB, London [email protected]
ASSOCIATE EDITORS RÉDACTEURS ASSOCIÉS
BASIC SCIENCE AND SURGICAL BIOLOGYIan McGilvray, MD, PhD, Toronto Timothy Daniels, MD, Toronto
BREAST SURGERYMuriel Brackstone, MD, London
CARDIOVASCULAR SURGERYMichel Carrier, MD, Montréal Michael Chu, MD, London
CRITICAL CARERaymond Kao, MD, London
ENDOCRINE SYSTEMSam Wiseman, MD, Vancouver
EVIDENCE-BASED MEDICINEMichelle Ghert, MD, Hamilton
GASTROINTESTINAL AND COLORECTAL SURGERYMarcus Burnstein, MD, Toronto Jason Park, MD, Winnipeg
GLOBAL SURGERYDan Deckelbaum, MD, Montréal
GENERAL SURGERYDaniel Birch, MD, Edmonton
HEPATOBILIARY AND PANCREATIC SURGERYShiva Jayaraman, MD, Toronto
MEDICAL EDUCATIONCarol Hutchison, MD, Calgary
MILITARY MEDICINEHomer Tien, MD, Toronto
ORTHOPEDIC FOOT AND ANKLE SURGERYKarl-André Lalonde, MD, Ottawa
ORTHOPEDIC SURGERYGraham Elder, MD, Sault Ste. Marie
PEDIATRIC SURGERY, GENERALSigmund Ein, MD, Toronto
PEDIATRIC SURGERY, ORTHOPEDICJames G. Wright, MD, MPh, Toronto
SPINAL SURGERYRaja Rampersaud, MD, Toronto
SPORTS MEDICINEPaul Martineau, MD, Montréal
SURGICAL ONCOLOGYGeoff Porter, MD, Halifax
SURGICAL ONCOLOGY, MUSCULOSKELETALFrank O’Dea, MD, St. John’s
SURGICAL ONCOLOGY, SOFT TISSUEChris de Gara, MB MS, Edmonton
THORACIC SURGERYJohn Yee, MD, Vancouver
TRAUMA SURGERY, ORTHOPEDICWilliam Dust, MD, Saskatoon
TRAUMA SURGERY, SOFT TISSUEMary vanWijngaarden-Stephens, MD, Edmonton Morad Hameed, MD, Vancouver
VASCULAR SURGERYKent Mackenzie, MD, Montréal
EDITORIAL STAFF ÉQUIPE DE RÉDACTION
MANAGING EDITOR DIRECTRICE DE LA RÉDACTIONWendy Carroll ([email protected]) tel 800 663-7336 (Canada, USA) or 613 731-8610 x2198; fax 613 565-5471
EDITORIAL COORDINATOR COORDONNATRICE DE LA RÉDACTIONHolly Clark ([email protected]) tel 800 663-7336 (Canada, USA) 613 731-8610 x2018; fax 613 565-5471
TRANSLATION • TRADUCTIONMarie Saumure
PRODUCTION STAFF ÉQUIPE DE PRODUCTION
PRODUCTION MANAGER GESTIONNAIRE DE LA PRODUCTIONDebbie Rupert
PRODUCTION DESIGNERS INFOGRAPHISTES DE LA PRODUCTIONCarole Lalonde, Sarah O’Neill, Jennifer Pershick, Clara Walker
WEB PUBLISHERS ÉDITION EN LIGNEMarla Fletcher, James Harbinson, James Manship
ADVERTISING PUBLICITÉ
ADVERTISING ANNONCES PUBLICITAIRESLaurie McLeod, Susan Ritchie, David Bertrand 613 731-8610 x2107/2041 fax 613 565-7488 [email protected]; [email protected]
ADVERTISING SALES VENTES PUBLICITAIRESBlair Graham ([email protected]) 416 850-1485; cell 416 560-0202; fax 416 850-2242
Trish Sullivan ([email protected]) cell 905 330-8770
PUBLISHING STAFF ÉQUIPE DES SERVICES D’ÉDITION
DIRECTOR AND PUBLISHER DIRECTRICE ET ÉDITRICEGlenda Proctor
ASSOCIATE DIRECTOR, PUBLICATIONS DIRECTRICE ASSOCIÉE, PUBLICATIONSHolly Bodger
PROGRAM MANAGER, JOURNALS GESTIONNAIRE DE PROGRAMMES, JOURNAUXJanis Murrey
The Canadian Journal of Surgery aims to contribute to the effective continuing medical education of Canadian surgical specialists and to provide surgeons with an effective vehicle for the dissemination of observations in the areas of clinical, basic science and education research.Readers can find CJS online at canjsurg.ca.Submission of new manuscripts can be made at http://mc.manuscriptcentral.com/cjs.
Le Journal canadian de chirurgie vise à dispenser une éducation médicale continue efficace aux spécialistes en chirurgie au Canada, et fournir aux chirurgiens un mécanisme efficace pour diffuser les constatations de la recherche clinique, fondamentale et éducative.Les lecteurs trouveront en direct le JCC à l’adresse canjsurg.ca.Nous favorisons l’envoi électronique de manuscrits. Veuillez visiter le http://mc.manuscriptcentral.com/cjs.
Owned and published by 8872147 Canada Inc., a wholly
owned subsidiary of the Canadian Medical Association
1867 prom. Alta Vista Dr. Ottawa ON K1G 5W8
All prescription drug advertisements have been cleared by the Pharmaceutical Advertising Advisory Board.Toutes les annonces de médicaments prescrits ont été approuvés par le Conseil consultatif de publicité pharmaceutique.
masthead-apr15.indd 75 2015-03-10 12:10 PM

For more information or to register, visit:
cma.ca/pmi
LEADERSHIP lives here Complement your clinical expertise with effective leadership skills
Registered trademarks of the Canadian Medical Association used under licence
PMI physician leadership courses�� Developed by the CMA specifically for physicians�� Accredited by the RCPSC and the CFPC�� Set you on a path to achieve the Canadian Certified Physician Executive (CCPE) designation
Open-enrolment courses Developing and Leading System Improvement — June 1–2, 2015, Halifax, NSLeadership Strategies for Sustainable Physician Engagement — June 3–4, 2015, Halifax, NS
Online courses (facilitated) New! Effective Communication Skills for Physician Leaders — April 27–June 7, 2015Leadership Begins with Self-awareness — October 19–November 29, 2015
In-house courses Bring customized PMI physician leadership courses to your workplace, conference or annual meeting.
@cma_learns
3099
“PMI physician leadership courses are important ways for physicians to remain engaged and resilient in today’s complex health care system.”
— Dr. Caroline Gerin-Lajoie Psychiatrist
Ottawa, Ont.
3099_PMI_Single_CJS_01-final.indd 1 2015-03-10 9:46 AMmasthead-apr15.indd 76 2015-03-10 12:10 PM

EDITORIAL • ÉDITORIAL
©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 77
Medical memorialization
T he urge to memorialize is robust in medicine, particularly so on the surgical side of the house. It defies changing times and fashions. The desire
to be remembered may be the instinct that drives surgeons to work harder and longer than their peers in society. Medical memorialization, the desire of society to remember a physician, on the other hand, is a mys tery. It appears to be random and often inaccurate. It is quiet ly revered, but must not be sought.
On Apr. 23, 2015, exactly 100 years after the Second Battle of Ypres, John McCrae will be inducted into the Canadian Medical Hall of Fame. His name had been put forward on 2 previous occasions to fill the single slot reserved each year for posthumous induction. Among this year’s other inductees, who are happily still alive, is Dr. Bernard Langer. Dr. Langer, former head of surgery at the University of Toronto, is being recognized for contributions to medical education, research and patient safety.1 John McCrae, revered for his poem “In Flanders Fields,” was probably elected this time because his wartime service was placed in the context of the advanced state of his medical practice at the time of his enlistment. McCrae’s medical publications demonstrate his pioneering role in Canadian infectious disease medicine and anatomic pathology.2 He would have been remembered as a founder had he not died during the war. For John McCrae, this honour will add little to his fame. Schools and prizes have already been named for him. The Government of Canada designated him to be a “person of national historic significance” 70 years ago. Electing John McCrae to the Canadian Medical Hall of Fame is our way of reclaiming the soldier–poet for medicine. The goal of this article is to honour these physicians and to consider the role of memorialization in medicine.
The origin of memorialization can be traced from prehistorical oral sagas through the statuary of classical times to the monuments of the Victorian era. Memorialization was reserved for the ruling elite; its ultimate expression was a place in the pantheon. The hall of fame is today’s pantheon, and access to it has been democratized.
In the 19th century, advances in bacteriology resulted in the naming of many previously unknown organisms after their discoverer. This process, similar to explorers’ naming newfound landmarks, suggests that discoverers retain naming rights. This is not true in medicine.
Unlike geography, claiming a name for a medical discovery or invention or bestowing it in honour of a third party, such as a sponsor or a member of a royal family, is not accepted. Universities may trade naming rights for donations, but the practice has more to do with the sponsorship of sports arenas than medicine. Neither of these forms constitute medical memorialization.
Eponyms, often considered a prized form of mem o rialization, may be applied for convenience of recall and communication. This is especially true of clinical signs — a cluster of observations that leads a clinician to an instantaneous diagnosis and the eternal faith of a patient. Many eponyms are inaccurate. For example, even though Thomas Cullen credited Joseph Ransohoff with the description of periumbilical staining, we remember it as Cullen’s sign.3 Eponyms applied to surgical procedures are even more inac curate. Novel operations are built upon previous practice. Allen Whipple neither described, nor was the first to perform, the operation we call Whipple’s procedure. In spite of these inaccuracies, there are no protests, no campaigns to right these wrongs. This is because eponyms are derived from those who popu larized the item rather than those who discovered or invented it. They are applied only if they facilitate com munication. This explains why partial pancreaticoduodenectomy is called Whipple’s procedure but liver transplantation is not called Starzl’s procedure. Use of eponyms is therefore not an act of memorialization.
Memorialization is an inherent part of surgical education where we not only teach a procedure or an aspect of knowledge, but also how it was developed. In research it is the appropriate referencing of prior knowledge. These are preferred forms of memor ialization today because they acknowledge the deed rather than remember the person. The statues, busts and portraits of medical pioneers have been removed from our hospitals. But there is a role for acknowledging the individual. There are some signs that portraiture is coming back into fashion, and 3dimensional printing may make sculpture more popular.
The target audience of the Canadian Medical Hall of Fame is the whole of society, especially the young, because the real purpose of memorialization is to inspire. Dr. Langer’s induction will inspire students to choose a career in surgery and emulate his achie vements.
edit-april15.indd 77 2015-03-10 11:03 AM

ÉDITORIAL
78 J can chir, Vol. 58, No 2, avril 2015 ©2015 8872147 Canada Inc.
Dr. McCrae’s induction will remind phy sicians of their obligation to serve their country and the global community.
Vivian McAlister, MD Coeditor, Canadian Journal of Surgery
Competing interests: None declared.
DOI: 10.1503/cjs.003215
References
1. Rotstein O, Greig P. Dr Bernard Langer — inductee into the Canadian Medical Hall of Fame. Can J Surg 2015;58:802.
2. Prescott JF. The extensive medical writings of soldierpoet John McCrae. CMAJ 1980;122:1134.
3. Ullah SM, Grant RC, Johnson M, et al. Scarpa’s fascia and clinical signs: the role of the membranous superficial fascia in the eponymous clinical signs of retroperitoneal catastrophe. Ann R Coll Surg Engl 2013;95:51922.
L e besoin de commémoration est fort en médecine, particulièrement chez nos collègues chirurgiens. Il persiste malgré les modes, quelle que soit
l’époque. C’est peutêtre le désir de passer à l’histoire qui pousse les chirurgiens à travailler plus fort et plus longtemps que leurs pairs dans la société. La commémoration médicale, soit la volonté qu’a une société de perpétuer le souvenir d’un médecin, est, quant à elle, un mystère. Elle semble être aléatoire et se révèle souvent inexacte. Elle est discrètement vénérée, mais ne doit pas être recherchée.
Le 23 avril 2015, 100 ans exactement après la seconde bataille d’Ypres, John McCrae sera intronisé au Temple de la renommée médicale canadienne. Sa candidature avait été soumise 2 fois auparavant pour occuper la seule place réservée chaque année à une intronisation posthume. Le Dr Bernard Langer compte parmi les autres lauréats de cette année, qui sont heureusement toujours en vie. Le Dr Langer, ancien chef du Département de chirurgie de l’Université de Toronto, est reconnu pour ses contributions à l’éducation médicale, à la recherche et à la sécurité des patients1. John McCrae, révéré pour son poème intitulé « Au champ d’honneur », a probablement été sélectionné cette foisci parce que son service en temps de guerre a été placé dans le contexte du niveau avancé de sa pratique médicale au moment de son enrôlement. Les publications médicales du Dr McCrae démontrent son rôle de pionnier dans les domaines des maladies infectieuses et de la pathologie anatomique2. Il aurait été intronisé en qualité de bâtisseur s’il n’était pas mort pendant la guerre. Cette distinction ajoute peu à la renommée du Dr John McCrae : des écoles et des prix
ont déjà été nommés en son honneur et le gouvernement du Cana da l’a désigné « personne d’importance historique nationale » il y a 70 ans. L’intronisation du Dr John McCrae au Temple de la renommée médicale canadienne est notre façon de rapatrier au sein de la médecine le soldatpoète. L’objectif de cet article est d’honorer ces médecins et d’examiner le rôle de la commémoration en médecine.
La commémoration, qui remonte aux sagas préhistoriques transmises oralement, s’est manifestée plus tard dans les statues de l’époque classique et dans les monuments de l’époque victorienne. La commémoration était réservée à l’élite dirigeante et son expression ultime était l’élection au panthéon. Le Temple de la renommée est un panthéon moderne auquel l’accès a été démocratisé.
Au 19e siècle, avec les progrès en bactériologie, de nombreux organismes jusqu’alors inconnus ont été désignés du nom de leur découvreur. Cette pratique, semblable à celle des explorateurs qui baptisaient de nouveaux lieux, laisse entendre que les découvreurs conservent des droits d’appellation. Ce n’est pas le cas en médecine. Contrairement au domaine de la géographie, revendiquer un nom pour une découverte médicale ou une invention ou donner un nom en l’honneur d’un tiers, tel que celui d’un commanditaire ou d’un membre de la famille royale, n’est pas bien vu. Les universités peuvent offrir des droits d’appellation en échange de dons, mais cette pratique relève beaucoup plus de la commandite de complexes sportifs que de la médecine. Aucune de ces 2 formes d’appellation ne constitue une commémoration médicale.
Les désignations éponymes, souvent considérées comme une forme prisée de commémoration, peuvent
La commémoration médicale
edit-april15.indd 78 2015-03-10 11:03 AM

EDITORIAL
Can J Surg, Vol. 58, No. 2, April 2015 79
faciliter la mémorisation et la communication. Cela est particulièrement vrai en ce qui concerne les signes cli-niques — un ensemble d’observations qui conduit le médecin à un diagnostic instantané et résulte en une confiance éternelle du patient. De nombreuses désigna-tions éponymes sont toutefois inexactes. Par exemple, même si Thomas Cullen a attribué la description des taches périombilicales à Joseph Ransohoff, nous nous en souvenons comme du signe de Cullen3. Les appellations éponymes données aux procédures chirurgicales sont encore plus inexactes. Les interventions novatrices sont fondées sur des pratiques antérieures. Allen Whipple n’a ni décrit, ni été le premier à effectuer l’intervention connue sous le nom d’« opération de Whipple ». Mal-gré ces inexactitudes, il n’y a aucune contestation ni aucune campagne pour corriger ces erreurs. Cela est attribuable au fait que les désignations éponymes sont inspirées du nom de la personne qui a popularisé quelque chose plutôt que sur le nom de la personne qui a découvert ou inventé la chose en question. Elles sont utilisées seulement si elles facilitent la communication, ce qui explique pourquoi la pancréaticoduodénectomie se nomme « opération de Whipple » alors que la greffe de foie ne se nomme pas « opération de Starzl ». L’attribution d’une désignation éponyme n’est donc pas un acte de commémoration.
La commémoration est inhérente à la formation en chirurgie, dans laquelle non seulement nous enseignons une procédure ou une facette du savoir, mais aussi la façon dont elle a été développée. En recherche, cela se traduit par une référence ou par un renvoi aux connais-
sances antérieures. Ce sont aujourd’hui les formes privilé-giées de commémoration parce qu’elles reconnaissent l’acte plutôt que la personne. Les statues, bustes et por-traits des pionniers de la médecine ont été retirés de nos hôpitaux. La reconnaissance de l’individu a toutefois un rôle à jouer. Certains signes indiquent que l’art du por-trait revient à la mode, et l’impression tridimensionnelle pourrait rendre la sculpture plus populaire.
Le public cible du Temple de la renommée médicale canadienne est l’ensemble de la société, et particulière-ment les jeunes parce que le véritable objectif de la com-mémoration est d’inspirer. L’intronisation du Dr Langer inspirera les élèves à choisir une carrière en chirurgie et à imiter ses réalisations et celle du Dr McCrae rappellera aux médecins leur devoir de servir leur pays et la com-munauté mondiale.
Vivian McAlister, MD Co-rédacteur, Journal canadien de chirurgie
Intérêts concurrents : Aucuns déclaré.
DOI: 10.1503/cjs.003515
Références
1. Rotstein O, Greig P. Dr Bernard Langer — inductee into the Cana-dian Medical Hall of Fame. Can J Surg 2015;58:80-2.
2. Prescott JF. The extensive medical writings of soldier-poet John McCrae. CMAJ 1980;122:113-4.
3. Ullah SM, Grant RC, Johnson M, et al. Scarpa’s fascia and clinical signs: the role of the membranous superficial fascia in the eponymous clinical signs of retroperitoneal catastrophe. Ann R Coll Surg Engl 2013;95:519-22.
edit-april15.indd 79 2015-03-10 11:03 AM

COMMENTARY • COMMENTAIRE
80 J can chir, Vol. 58, No 2, avril 2015 ©2015 8872147 Canada Inc.
Dr. Bernard Langer — inductee into the Canadian Medical Hall of Fame
D r. Bernard Langer’s induction into the Canadian Medical Hall of Fame acknowledges his profound effect on medicine and surgery in Canada and an impact that has been truly international. In this brief biography,
we highlight the major accomplishments that have made Dr. Langer a pre-eminent leader, innovator, teacher and exemplary surgeon.
“B.L.” or “Bernie,” as his friends and colleagues know him, was born in Toronto, Ont., in 1932. He received his medical degree from the University of Toronto in 1956, graduating with the Cody Gold Medal Award. Following an internship at the Toronto General Hospital (TGH), he completed his surgical training at the University of Toronto in 1962. During his residency, he married Ryna Manson and they began what was to become a family with 4 children: Jack, David, Pearl and Michael. Dr. Langer’s postresidency training, what would today be called a fellowship, was split between oncology with Dr. John Stehlin at M.D. Anderson Hospital in Houston, Tex., and experimental liver transplantation with Dr. Francis Moore at the Brigham Hospital in Boston, Mass.
Dr. Langer’s appointment to full attending staff at TGH in 1963 is recognized as a turning point in breaking down some of the antisemitic barriers in surgery that existed at the time. Although he practised the full range of general surgery, he developed an interest and expertise in the surgical management of portal hypertension and malignancies of the hepatobiliary system and pancreas — the genesis of the hepatico-pancreato-biliary (HPB) surgeon.
In 1972 Dr. Langer was appointed as the head of the Division of General Surgery at TGH, which was transformed under his leadership by his commitment to the emergence of subspecialties. His recruitment of Wayne Johnson and Paul Walker began the discipline of Vascular Surgery; Zane Cohen and Robin McLeod, Colorectal Surgery; Rudy Falk, Ulo Ambus and Lorne Rotstein, Surgical Oncology and Endocrine Surgery; and Bob Stone, Bryce Taylor and one of us (P.G.), HPB Surgery and Transplantation. This model became the standard for future recruitment and development within the Division of General Surgery at TGH and would serve as a model for other hospitals affiliated with the University of Toronto and across the country.
Dr. Langer is a “first generation” HPB and transplant surgeon. Along with the other pre-eminent HPB and transplant pioneers, like Henri Bismuth from France; John Terblanche from South Africa; and Dean Warren, Marshall Orloff and Tom Starzl from the United States, Dr. Langer’s advancement of the discipline of HPB surgery has resulted in it being
Paul D. Greig, MD Ori D. Rotstein, MD
Accepted for publication Feb. 26, 2015
Correspondence to: O. Rotstein St. Michael’s Hospital 30 Bond St. Toronto ON M5B 1W8 [email protected]
DOI: 10.1503/cjs.003315
Dr. Bernard Langer’s induction into the Canadian Medical Hall of Fame acknowledges his profound effect on medicine and surgery in Canada and an impact that has been truly international. In this brief biography, we highlight the major accomplishments that have made Dr. Langer a pre-eminent leader, innovator, teacher and exemplary surgeon.
Summary
langer-rotstein.indd 80 2015-03-10 7:57 AM

COMMENTARY
Can J Surg, Vol. 58, No. 2, April 2015 81
recognized as a specific discipline within general surgery. During his career, he contributed to its understanding, and major advances occurred in the reduction of the mor-bidity and mortality of complex HPB procedures, includ-ing major liver resections and the Whipple pancreatico-duodenectomy. Dr. Langer started the liver transplant program in Toronto and performed Toronto’s first liver transplant in 1985. While pushing forward this specialty, he was also widely recognized as a “surgeons’ surgeon.” He was a gifted clinician and surgeon with very high standards and constantly challenged his colleagues to strive for excellence in patient care. Dr. Langer’s clinical nickname “The Hawk” came from his astute awareness of a patient’s clinical situation and his ability to manage it. Trainees and faculty members alike will recall his morbidity and mortality rounds, where he could inci-sively address the root cause of patient complications, even when these were outside his specific area of clinical expertise.
Dr. Langer’s impact on clinical care extended beyond his own patients. Through his leadership role in Cancer Care Ontario as a member of the Provincial Advisory Committee on Surgical Oncology, the Cancer Quality Council of Ontario and the Cancer Surgery Quality Com-mittee, he championed standards for cancer care, including the Ontario Standards for HPB Surgery. This approach has translated across specialties and has served as a model for other provinces.
In 1982, Dr. Langer succeeded Dr. Donald R. Wilson as the R.S. McLaughlin Professor and chair of the Department of Surgery at the University of Toronto. He was the first non–surgeon-in-chief to do so, and his decade as chair was transformative for Toronto and highly influential across Canada and internationally. His most significant accom-plishment is often identified as the creation of the Surgeon Scientist Program (SSP). He recognized Toronto’s reputa-tion for excellence in clinical training, but saw the need for surgeons to engage in formalized research training as a requirement for the future academic success of individuals and the department. This highly successful program became the standard bearer for clinician–scientist training in facul-ties of medicine across the country. In 1994 the Royal Col-lege of Physicians and Surgeons of Canada established the Clinician Investigator Program, one largely modelled after the SSP. At the University of Toronto Department of Sur-gery, Dr. Langer’s “farm system” sustained and promoted academic excellence in surgery over the next 25 years and presumably will continue to do so into the future.
“As a physician leader, Bernie Langer was a true innova-tor, an extraordinarily gifted surgeon and a great teacher,” says Dr. David Naylor, dean of the University of Toronto Faculty of Medicine and former president of the University of Toronto. “The Surgeon Scientist Program he created has been widely emulated in other clinical departments across Canada and is a cornerstone of the department’s interna-tional reputation.”
Dr. Langer doing what he loves: operating on a complex surgical problem in a team with colleagues and students.
langer-rotstein.indd 81 2015-03-10 7:57 AM

COMMENTAIRE
82 J can chir, Vol. 58, No 2, avril 2015
Dr. Langer proposed and implemented a system of practice plans across the department that balanced individ-ual division/hospital financial autonomy with the academic principle of income-sharing, with a view to fostering sub-specialization and supporting academic initiatives. The challenges in doing so are almost unimaginable, but speak to Dr. Langer’s personal leadership and, in particular, his ability to rally individuals in support of the academic mis-sion. Over the years, the practice plans have evolved, but their underlying raison d’etre, namely the support of activ-ities to promote excellence in clinical care, research and education, has remained unchanged.
While most recall Dr. Langer as a tireless advocate for research in the department, his contributions to educa-tion have also had profound impact. As department chair, he established education as one of the streams for aca-demic promotion. This has served to broadly engage a department filled with individuals who felt distanced from the research mission. He also recognized that improving the quality of education required that our fac-ulty engage in advancing our understanding of surgical education. Today’s department is heavily populated with surgeons who have formal training in medical education and who are not only excellent teachers, but who also contribute through scholarship. Dr. Langer is also recog-nized for his personal contributions to education through his creation of the fellowship in liver surgery, which grew from 1 fellow in 1982 to 3 fellows in transplant and HPB surgery in 1989 to 7 Fellows in 2 separate but integrated fellowships in HPB surgical oncology (accredited by America’s Hepato- Pancreato-Biliary Association and the Fellowship Council) and in abdominal organ transplanta-tion (accredited by the American Society of Transplant Surgeons). At a reunion of former fellows in 2013, Dr. Langer was recognized:
Amongst his notable accomplishments, Dr. Langer has been recognized by the [University Health Network] for “making global impact.” His growing legacy of over 65 fellows practising HPB and transplant surgery throughout the world is tangible evidence of Dr. Langer’s truly remarkable global impact. We thank you, B.L., for your vision in establishing the fellowship, your high standards and clinical excellence in HPB and trans-plant surgery that is carried on in your fellows, and your men-torship that extends beyond clinical surgery.”
Dr. Langer has had significant influence outside of Toronto. He was president of the Canadian Association of General Surgeons in 1988–89 and President of the Society for Surgery of the Alimentary Tract in 1993–94 and subsequently the chair of their Board of Trustees; in 1999 he became the first vice president of the American Surgical Association. Through his engagement with the Royal College of Physicians and Surgeons of Canada, Dr. Langer has contributed to Canadian medicine by advancing many of his priorities. He was president and
chair of the Royal College Council and Executive Com-mittee from 2000 to 2002, and he created the Canadian Patient Safety Institute.
Dr. Langer’s contributions and influence have been recognized through many honours, including the creation of the University of Toronto Department of Surgery Langer Surgeon Scientist Award, the Bernard Langer Annual Lecture in Health Sciences at the University of Toronto, the Bernard and Ryna Langer Chair in General Surgery at the University of Toronto, and the Langer Lecture of the Canadian Association of General Surgeons Annual Meeting held at the Canadian Surgery Forum. He has received honorary fellowships from the Royal Austral-asian College of Physicians, the Colleges of Medicine of South Africa, the American College of Physicians and the Academy of Medicine of Singapore as well as an honorary doctorate from Queen’s University
In 2002 Dr. Langer was appointed Officer of the Order of Canada. His extraordinary accomplishments are found ed on a number of outstanding personal qualities. He always cared deeply for his patients, understanding not only their physical problems, but also personal or emo-tional issues that might be impacting their disease. Excel-lent technical ability was only one aspect of achieving the best outcome for his patients. The high degree of respect in the eyes of his surgical peers also facilitated his ability to influence his colleagues. Dr. Langer also exhibited excep-tional leadership abilities. Teamwork was paramount. He engaged individuals with similar and disparate expertise to tackle tough problems. He promoted faculty, particularly those more junior, by giving them opportunities to partici-pate and to develop their own leadership skills. He sur-rounded himself with excellent colleagues and listened carefully to their advice, but always remained true to his ideals. He was a tough negotiator but always sought the “win–win” outcome, even before this saying became popu-lar. Finally, in an era when attention to personal life and family were considered a weakness, Dr. Langer always rec-ognized the importance of the support of his wife Ryna and his family.
Bernard Langer’s induction into the Canadian Medical Hall of Fame is highly appropriate. The Hall of Fame is “dedicated to celebrating the accomplishments of medical heroes.” Dr. Langer is that, and more. He has been quoted as saying “If you don’t stand tall enough, you can’t see far enough.” Dr. Langer stood very tall and took us very far. He is a visionary, always looking beyond the present into the future.
Affiliations: From the Department of Surgery, University of Toronto (Rotstein, Greig); St. Michael’s Hospital (Rotstein); and the University Health Network (Greig), Toronto, Ont.
Competing interests: None declared.
Contributors: Both authors contributed substantially to the concep-tion, writing and revision of this commentary and approved the final version for publication.
langer-rotstein.indd 82 2015-03-10 7:57 AM

COMMENTARY • COMMENTAIRE
©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 83
Amnesia in modern surgery: revisiting Wangensteen’s landmark studies of small bowel obstruction
D uring recent ward rounds, while reassessing a patient with adhesion-induced partial small bowel obstruction we learned that the nursing staff, at least some of the residents and even some attending staff were
unaware of the exact role of nasogastric suction in its treatment. It called to mind some quotes of Dr. Owen Wangensteen, Chairman of the Department of Surgery at the University of Minnesota from 1930 to 1968. He said, “There exists a feeling among many physicians and students that anything over 10 years old has no pertinence,” and “If you only look forward, it’s tantamount to having a physician with total amnesia. How good would he be?”1 These observations are particularly appropriate to our patient, as Wangensteen liter-ally wrote the book on bowel obstruction and received the 1935 Samuel D. Gross Prize for his research in this area.2
Before the publications of Wangensteen and his colleagues in the early 1930s, bowel obstruction was almost always fatal, and its treatment was inef-fectual. Most surgeons believed that death was due to the production of toxic factors in the gut and their absorption into the blood stream. The source of the gaseous distention was attributed to the action of bacteria on retained food and the production of methane. The excess of fluid in the gut above the point of obstruction was appreciated, but the failure of patients to improve with intravenous infusions of saline was a great disappointment. Patients rarely survived surgical attempts to relieve the obstruction.
Although other investigators were active in the field, the understand-ing of the pathophysiology of obstruction belongs almost entirely to Wangensteen. He reiterated others’ experiments, showing where they were incorrect or misinterpreted. He then developed a series of convincing experiments in dogs that established the cause of the signs and symptoms and subsequently their treatment. His group measured the intraluminal pressures and absorption of fluids in the various parts of the gastrointes-tinal tract in healthy and in obstructed small bowel. They delineated the role of the lymphatics, the capillaries and the venules during obstruction. In addition, they defined the bacteriology of obstruction and its manifesta-tions at various time points and in various areas of the obstructed gut. They tested whether the well-described lethality could be transferred to normal animals by the injection of intestinal secretions or peritoneal fluid from affected animals.
Andrea Faryniuk, MD Allan MacDonald, MD Paul van Boxel, MD
Accepted for publication Sept. 17, 2014
Correspondence to: A. Faryniuk Cumberland Regional Health Care Centre 19428 Hwy 2, RR # 6 Upper Nepean NS B4H 1N6 [email protected]
DOI: 10.1503/cjs.010814
Before the publications of Owen Wangensteen and his colleagues in the early 1930s, bowel obstruction was almost always fatal, and its treatment was ineffec-tual. Patients rarely survived surgical attempts to relieve the obstruction. Although other investigators were active in the field, the understanding of the pathophysiology of obstruction belongs almost entirely to Wangensteen. In this commentary, we review Wangensteen’s landmark studies of small bowel obstruction and how they shaped the treatment of this condition.
Summary
amnesia-faryniuk.indd 83 2015-03-10 1:14 PM

COMMENTAIRE
84 J can chir, Vol. 58, No 2, avril 2015
The most telling investigations were into the origin and make-up of the characteristic gas and fluid accumula-tions in distended gut. The initial part of the experiment was to ligate the mid-ileum in all the experimental ani-mals. Then in half of the animals the esophagus was divided and the upper end brought out to the skin as a mucous fistula. In the other half the gastrointestinal tract, though completely obstructed, was otherwise left intact. All the animals received intravenous electrolyte infusions. The animals that had the esophagus diverted did not become distended with either gas or fluid and survived for prolonged periods. Those with an intact esophagus experienced the classical consequences of small bowel obstruction, from which they died despite the intra-venous fluids. With this insightful series of experiments, Wangensteen proved that swallowed air causing disten-sion was the culprit. In further trials, both in animals and in humans, he showed that removal of the air by means of gastric tubes rescued both experimental animals and patients alike. Under these circumstances, an operation could be done safely or, in many instances, could be avoided altogether. In the absence of swallowed air, healthy gut fluids; saliva; gastric, pancreatic and enteric juices; and bile could be absorbed by the obstructed small intestine. Wangensteen worked out the suction pressures that allow gastric air to be removed and constructed a bedside device that could do this effectively. He demon-strated that the excess fluid accumulation above the obstruction was due to the distension pressure of the swallowed air on the bowel wall impeding venous outflow but not arteriolar inflow. These conditions then inter-rupted fluid absorption by the intestinal mucosa. He also concluded that there was no advantage to advancing the tube beyond the stomach. The essential function of the gastric tube is to remove air, not fluid.
After having clarified the true function of the nasogas-tric tube on our ward rounds, a new question arose. If air is the important element removed by suction, but it is not measured by the suction device, how did Wangensteen know when to remove the tube? In his book, The thera-peutic problem in bowel obstructions: a physiological and clin ical consideration,3 Wangensteen listed the following criteria: 1) cessation of “gas pains;” 2) decrease of abdominal distension; 3) the visualization of gas in the colon on the radiograph in complete obstructions, indi-cating that that the obstruction has been overcome; 4)
less fluid aspirated through the tube, denoting that stasis is no longer prominent; and 5) toleration of temporary discontinuation of suction without recurrence of pain. It is interesting that the amount of fluid aspirated was number 4 on his list of criteria when for many surgeons today it is number 1 — a reflection of the misguided emphasis on intestinal fluid aspiration.
Wangensteen received the Gross Prize for these pio-neering research studies, and their description is incor-porated as Part I in his landmark book.3 The remaining sections are devoted to clinical aspects and the recogni-tion, diagnosis and guiding principles of treatment. Chap-ters are devoted to the various subtypes of congenital and acquired large and small bowel obstruction. In its subse-quent revised editions, the book became a bible for the next 30 years and still guides the way surgeons approach this common problem.
Surgeons of a certain vintage will remember when the bedside apparatus was called the Wangensteen Suction. Paradoxically, the nasogastric tube is still called the Levin tube, although its invention in 1921 was as an investiga-tive aid for radiology and antedated its use in bowel obstruction. Many of the authors writing in today’s stan-dard textbooks of surgery do not properly describe these principles on which current decompression of the gut is based, probably assuming that they are self-evident.
The aphorism that those who don’t know history are condemned to repeat it happily applies to current surgeons who treat bowel obstructions as Wangensteen taught us — even if many don’t understand why.Affiliations: From the Department of Surgery, Cumberland Regional Health Care Centre (Faryniuk, van Boxel), and the Department of Surgery, Dalhousie University (Faryniuk, MacDonald, van Boxel), Halifax, NS.
Competing interests: None declared.
Contributors: All authors contributed substantially to the conception and design and writing of the manuscript and revised and approved the final version for publication.
References
1. Wangensteen O. A surgical pilgrimage. Some current-day problems of surgical education. Every man his own Boswell. JAMA 1968;205: 841-5.
2. Philadelphia Academy Of Surgery. Samuel D. Gross Prize 1935. Available: www.academyofsurgery.org/awards/awards3.html (accessed 2014 Dec. 18).
3. Wangensteen O. The therapeutic problem in bowel obstructions: a physio-logical and clinical consideration. Springfield (Ill): Charles C. Thomas; 1937.
amnesia-faryniuk.indd 84 2015-03-10 1:14 PM

COMMENTARY • COMMENTAIRE
©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 85
Endovenous radiofrequency ablation for the treatment of varicose veins
V aricose veins affect approximately 26% of the adult population and are a frequent cause of discomfort, loss of productivity and deterioration in health-related quality of life.1 Numerous therapies have been
de veloped for the treatment of this condition. Conventional open surgical interventions include ligation of the great saphenous vein at the saphenofem-or al junction and stripping. Smaller veins have also been treated with phlebec-tomies. More recently, less invasive modalities, such as foam sclerotherapy, endovenous laser therapy (EVLT) and endovenous radiofrequency ablation (RFA), have also been used. While endovenous approaches are associated with fewer postoperative complications, such as hematoma, pain or saphenous nerve injury, there is currently no strong evidence to suggest an overall advan-tage for any particular treatment approach.2
The RFA procedure involves using a catheter electrode to deliver a high-frequency alternating radiofrequency current that leads to venous spasm, col-lagen shrinkage and physical contraction.3 The patient’s leg is prepped with antiseptic solution and draped in a sterile fashion. With ultrasound guidance, the vein is cannulated, and local tumescent anesthetic is then injected around the target venous segment. The catheter is then introduced through a sheath. The radiofrequency current is then delivered, resulting in circular homogen-eous denaturation of the venous collagen matrix and endothelial destruction at a temperature of 110–120° C. Venous segments 3–7cm in length are treated in 20-second cycles. Patients are instructed to wear 20–30 mm Hg graduated elastic compression stockings for at least 14 days.
Compared with conventional open surgery, RFA can be performed in the outpatient setting without the requirement for hospital admission or general anesthesia. However, the procedure is not feasible in tortuous or very small or large veins, and it may be less cost-effective than open surgery because of the cost of the catheters.
To our knowledge, our institution was the first in Canada to offer RFA for the management of varicose veins using the venefit procedure with second-generation ClosureFast catheters (Covidien). Between 2010 and 2013, 173 pa tients underwent RFA performed by 3 vascular surgeons. The average age of the patients was 52 ± 14 years, and 143 (83%) of the patients were women. Our patients were referred to the clinic either by their family doctors
Ahmed Kayssi, MD, MSc, MPH Marc Pope MD, MSc Ivica Vucemilo, MD Christiane Werneck, MD, MScCH
Accepted for publication Oct. 15, 2014
Correspondence to: C. Werneck Division of Vascular Surgery University of Toronto 89 Queensway West, Suite 500 Mississauga ON L5B 2V2 [email protected]
DOI: 10.1503/cjs.014914
Varicose veins are a common condition that can be treated surgically. Available operative modalities include saphenous venous ligation and stripping, phlebec-tomy, endovenous laser therapy and radiofrequency ablation. Radiofrequency ablation is the newest of these technologies, and to our knowledge our group was the first to use it in Canada. Our experience suggests that it is a safe and effective treatment for varicose veins, with high levels of patient satisfaction reported at short-term follow-up. More studies are needed to assess long-term effectiveness and compare the various available treatment options for varicose veins.
Summary
endovenous-kayssi.indd 85 2015-03-10 8:03 AM

COMMENTAIRE
86 J can chir, Vol. 58, No 2, avril 2015
or another vein clinic, and they underwent preoperative Doppler ultrasonography to identify reflux within the target vein. The decision to offer a patient RFA was based on the target vein anatomy and diameter. The maximum vein diameter considered for the procedure was 1.8 cm, and the minimum was 0.4 cm. Elderly patients also underwent arterial duplex scans to rule out arterial insufficiency.
Most (72%) patients underwent treatment of a single limb, and 89% of patients underwent treatment of a single vein. The great saphenous vein was most frequently treated (81%), followed by the small saphenous (7%) and the accessory great saphenous (1%).
Postoperatively, the median time that patients took off work was 2 days. While 80 (69%) patients needed no postoperative analgesia, 35 (30%) patients used over the counter oral analgesics, such as acetaminophen or ibuprofen. Only 1 patient needed an opioid analgesic. Duplex ultrasonography performed 2–4 weeks after the procedure demonstrated successful vein occlusion in 99% of patients. Only 1 patient showed evidence of partial recanalization on followup. Two (1%) patients reported persistent pain at 30day followup, and 6 (4%) patients demonstrated skin discoloration. Eight (5%) patients with residual large veins returned to our clinic after the followup period and underwent phlebectomy procedures.
Telephone interviews were conducted several weeks after the procedure to assess patient satisfaction. Of the 111 (65%) patients contacted, 83% were extremely satisfied, 12% were very satisfied, 3% were somewhat satisfied, and 2% were not too satisfied with their RFA experiences. However, all of those who responded indicated that they would have this procedure again and would recommend it to a friend.
Our experience suggests that RFA is a safe and effective treatment for the management of varicose veins that is associated with a high success rate and patient satisfaction. Only 1 patient in our series demonstrated targetvein recanalization on followup. This was a cirrhotic patient with a history of hepatic failure who was on chronic anticoagulation therapy for multiple medical comorbidities. Her vein was also 1.5 cm in diameter, which was close to the cutoff of 1.8 cm that we accept in our practice.
To our knowledge, our group is the first to describe the successful implementation of RFA in Canada, where public health insurance guidelines have greatly restricted the criter ia
for reimbursing venous procedures and where many vein surgeries are performed at private clinics. In the face of this changing reimbursement landscape, we believe that RFA is a viable alternative to more conventional open vein surgeries and EVLT, which are more widely available in Canada.
Our work as well as studies by other groups will hopefully continue to enrich the debate on the most suitable intervention for the management of venous disease. A 2011 review by Ontario’s Medical Advisory Secretariat found that RFA was superior to open vein surgery when comparing postoperative pain, duration of recovery, major adverse effects and patient preference, while open surgery was less costly than RFA.4 However, the same review found no evidence to suggest major differences in postoperative pain between RFA and EVLT when pain was adjusted for analgesic use, and any differences did not persist after 1month followup. Furthermore, the 2 procedures did not differ when comparing treatment effectiveness or durability. This was mostly because of a lack of studies that have assessed longterm recurrence after either treatment. Prospective, longterm studies are thus clearly needed to compare the clinical and costeffectiveness of both treatments and provide health care consumers with the best standard of care.Affiliations: All authors are from the Division of Vascular Surgery, Trillium Health Partners, University of Toronto, Mississauga, Ont.
Competing interests: None declared.
Contributors: All authors contributed substantially to writing and/or revising and to the conception and design of the manuscript and approved the final version for publication.
References
1. Gloviczki P, Comerota AJ, Dalsing MC, et al. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg 2011;53:2S48S.
2. Nesbitt C, Eifell RK, Coyne P, et al. Endovenous ablation (radiofrequency and laser) and foam sclerotherapy versus conventional surgery for great saphenous vein varices. Cochrane Database Syst Rev 2011;CD005624. Medline
3. Bergan JJ, Kumins NH, Owens EL, et al. Surgical and endovascular treatment of lower extremity venous insufficiency. J Vasc Interv Radiol 2002;13:5638.
4. Health Quality Ontario. Endovascular radiofrequency ablation for varicose veins: an evidencebased analysis. Ont Health Technol Assess Ser 2011;11:193.
endovenous-kayssi.indd 86 2015-03-10 8:03 AM

©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 87
A novel method for assessing visual perception of surgical planes
Background: Recognition of tissue planes during surgery appears to be a skill acquired with experience. We conducted a pilot study to test this hypothesis using a novel method for evaluating this skill in a simulated environment.
Methods: Twelve surgeons of varying levels of experience were shown 16 captured images from a mesorectal excision. For each image, they were asked to draw the ideal dissection plane with a stylus on a tablet computer. We used a novel metric for comparing agreement between lines to determine the level of precision observed between junior and senior trainees and consultant surgeons and measure the accuracy of junior and senior trainees compared with consultant surgeons.
Results: We observed significant differences in precision for 9 of 16 images; 7 of these followed the predicted stepwise pattern associated with level of experience. Using consultant surgeons as the reference standard, we observed significant differences in accuracy between senior and junior trainees for 11 images, with senior trainees being more accurate in 10 of them. Only 2 images failed to contribute significant findings to our analysis.
Conclusion: The findings of this pilot evaluation of a novel method for measuring a surgeon’s ability to recognize tissue planes in a simulated model show that skill improves with experience. Further evaluation of this method will reveal its utility as an assessment tool and possibly as a training instrument.
Contexte : La reconnaissance des différents plans tissulaires durant la chirurgie semble être une compétence qui s’acquiert avec l’expérience. Nous avons procédé à une étude pilote pour vérifier cette hypothèse à l’aide d’une nouvelle méthode d’évaluation de cette compétence dans un environnement simulé.
Méthodes : Nous avons montré 16 images provenant d’une excision mésorectale à 12 chirurgiens de divers degrés d’expérience. Pour chaque image, ils devaient dessiner le plan de dissection idéal avec un stylet sur une tablette électronique. Nous avons utilisé un nouvel outil de mesure pour comparer la concordance entre les lignes et déterminer ainsi le degré de précision observé entre les résidents juniors et seniors et les chirurgiens consultants et comparer la précision des résidents juniors et seniors à celle des chirurgiens consultants.
Résultats : Nous avons observé des différences significatives quant à la précision pour 9 images sur 16; 7 d’entre elles étaient conformes aux séquences prévues compte tenu du degré d’expérience. En utilisant les chirurgiens consultants comme norme de référence, nous avons observé des différences significatives quant à la précision entre les résidents seniors et juniors pour 11 images, les résidents seniors étant plus précis pour 10 de ces images. Seulement 2 images n’ont pas permis d’alimenter de façon significative notre analyse.
Conclusion : Les résultats de cette évaluation pilote d’une nouvelle méthode de mesure de l’aptitude des chirurgiens à reconnaître les plans tissulaires dans un modèle simulé montrent que les habiletés s’améliorent avec l’expérience. Il faudra approfondir l’examen de cette méthode pour en confirmer l’utilité comme outil d’évaluation et instrument potentiel de formation.
Christopher M. Schlachta, BSc, MDCM Syed Ali, MD, MSc Hammood Ahmed, MD Roy Eagleson, PhD
This paper was presented at the 2013 Canadian Surgery Forum by S. Ali and was recipient of the CAGS Basic Science Award.
Accepted for publication Jul. 30, 2014
Correspondence to: C.M. Schlachta Schulich School of Medicine and Dentistry Western University Canadian Surgical Technologies and Advanced Robotics London Health Sciences Centre 339 Windermere Rd London ON N6A 5A5 [email protected]
DOI: 10.1503/cjs.007414
RESEARCH • RECHERCHE
novel-schlachta.indd 87 2015-03-10 7:55 AM

RECHERCHE
88 J can chir, Vol. 58, No 2, avril 2015
I t is considered a fundamental principle of good surgical technique to respect tissue planes during surgery. Tis-sue planes tend to be avascular; therefore, bleeding can
be reduced. In addition, there is growing evidence of improved oncologic outcomes associated with adherence to dissection along tissue planes. This has been demon-strated clearly for rectal cancer resections.1 There is com-pelling evidence to suggest this is also true for colon cancer surgery2 and hepatobiliary surgery.3
One of the challenges encountered when teaching train-ees to operate within tissue planes is how to facilitate the trainee’s recognition of the plane. What is intuitively ob vious to the expert surgeon is not always obvious to the trainee. There are likely visual clues that allow the expert to see what the novice does not yet appreciate. Currently it is not clear how this visual skill is learned during the course of clinical apprentice-based training.
Our hypothesis is that if the ability to perceive tissue planes is an acquired skill, then it should be possible to develop a visual test of that skill that discriminates between novice and expert surgeons.
Methods
We captured a series of 16 digital images representing progressive stages of a mesorectal excision from digitally recorded video. The chosen procedure was a da Vinci-assisted (Intuitive Surgical) laparoscopic proctectomy, and we obtained consent from the patient for the recording and use of the images for surgical instruction. The use of a da Vinci-assisted procedure, as opposed to a laparoscopic procedure, was of no particular consequence. We chose this particular case simply because the image quality and exposure of the tissue planes captured in the video were of such high quality that they seemed ideally suited for our pilot study. The images themselves were selected from video and chosen on the basis of clear views unobstructed by surgical instruments; they represented multiple view-points of the mesorectal envelope, as seen from the pos-ter ior, anterior, left and right dissection planes. Images were labelled minimally for orientation only.
Images were transferred to an iPad 2 (Apple Inc.) and presented in Sketchbook Pro software (Autodesk Inc.). Study participants were able to draw on the presented image using a stylus for capacitive touch screens (Slim Sty-lus, Targus). Each surgeon’s line was saved in a separate layer for later analysis.
We recruited 12 surgeons with varying levels of exper-tise to view the images on the iPad. Since this was a pilot study and we had no preconception as to what kind of results to expect, we did not perform any sample size or power analy sis calculations.
The participating surgeons included 4 consultant sur-geons experienced in performing a mesorectal excision, 4 senior trainees and 4 junior trainees. For each image, we
instructed the surgeons to draw a free line representing the dissection plane on the image as if the stylus were a scalpel or preferred dissecting instrument. The surgeons were instructed to draw the line as precisely as possible and to extend the line for as long as they felt they could comfort-ably appreciate the dissection plane. They were permitted to erase and redraw the line, if needed.
Statistical analysis
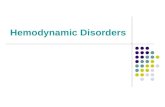
To compare one drawn line with another, we formulated a distance metric (similar to the Hausdorff measure used in computational geometry4) based on the Euclidean dis-tance between evenly spaced points along the arc. Using Matlab (MathWorks), each line was iteratively bisected 3 times (b = 3), resulting in 8 segments specified by pairs of Cartesian coordinates (p = 2b+1; 9 pairs for the present study; Fig. 1). For each study group (G), this distance metric between any 2 lines (a, b) for a given image (i) was calculated as the summed distance (d), in pixels, between each of the coordinate pairs (x, y) as follows:
Within each study group, there were 6 possible pairs of lines that could be compared for each image. Across the set of images, we calculated the means ± standard deviations of these 6 pairs for each of the 3 study groups.
The mean distance metric is inversely related to group precision (i.e., the greater the mean distance metric, the less agreement or consensus there is within that group with respect to the location of the ideal dissection plane). For each image, we compared this measure of precision for all
Fig. 1. Distance metric between 2 lines calculated as sum of Euclid-ean distance between 9 evenly spaced points along each line.
Rectum
Sacrum
novel-schlachta.indd 88 2015-03-10 7:55 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 89
3 study groups using 1-way analysis of variance (ANOVA) with a significance level of p = 0.05. When significant differ-ences were found, we performed pairwise comparisons using the Student t test. We used Šidàk’s equation to correct the level of significance for multiple comparisons: α[PT] = 1 – (1 – α[PF])1/c , where α[PT] is the corrected probability of a type-1 error for an individual test and α[PF] is the probabil-ity of a type-1 error for a family of tests. For 3 comparisons and α[PF] = 0.05, then α[PT] = 0.017.
Since there is no “correct” line representing the tissue plane in each image, and therefore no gold standard with which to compare the accuracy of each line, for the purpose of our analysis we considered the consultant surgeons to be the experts. Accordingly, for each image, we compared each trainee line with each consultant surgeon line in the fashion described above. This produced 16 comparisons (4 × 4) per group per line. The average of these 16 comparisons repre-sents group accuracy, with smaller distances associated with greater accuracy. These were analyzed using the Student t test, with significance set at p = 0.05.
Results
For 9 of the 16 images (1–3, 5, 6, 9–11, 16), we observed a stepwise increase in precision according to level of experi-ence from junior trainees to senior trainees to consultant surgeons, although not all were significantly different (Table 1). We observed significant differences in precision in 9 of the 16 images (2, 4–7, 9, 10, 13, 16). Considering these 9 images only, pairwise comparisons revealed signifi-cant differences in precision between 10 pairings. In only 1 image (7), significantly greater precision was found in the senior trainee group than in the consultant surgeon group.
In 13 of 16 images, the accuracy of the senior trainee group was greater than that of the junior trainee group (Table 2). These differences were significant for 10 of the images (3–7, 9–11, 14, 16). For image 12, the junior train-ees appeared to be significantly more accurate than the senior trainees. We used the results for image 5 as a repre-sentative example of these findings. Lines drawn by con-sultant surgeons (Fig. 2), senior trainees (Fig. 3) and junior trainees (Fig. 4) differed significantly on 1-way ANOVA but not by pairwise comparison (Table 1). For this image, senior trainees were significantly more accurate than junior trainees (Table 2).
Images 8 and 15 contributed no significant findings to any of our analyses.
Discussion
Visual processing of the spatial relations of image proper-ties is known as visual spatial ability. It has been proposed that visual spatial ability can be classified in 5 categories: edge and surface extraction, edge orientation encoding, whole object recognition, mental visualization involving the spatial relations of object parts in 2 dimensions (2D), and mental visualization involving 2D and 3-dimensional (3D) spatial rotations and translations. These represent a hier-archy of ability ranging from low- to high-level ability.5,6
Nonverbal, visual–spatial problem solving abilities and the ability to distinguish essential from nonessential detail has been shown to correlate with superior surgical skill in general surgery trainees.7 This finding was based on cor-rel ation between a battery of tests measuring visual–spatial perception, motor sequencing and fine-motor coordin-ation and stress tolerance with a novel rating scale of
Table 1. Mean within-group difference between lines for each surgical image
Mean distance ± SD (pixels) 1-way ANOVA Group comparisons (p < 0.017)*
Image Consultant Senior Junior F p value C v. S C v. J S v. J
1 1081 ± 327 1496 ± 744 2159 ± 894 3.646 0.05
2 731 ± 356 1530 ± 480 1973 ± 479 12.158 0.001 Yes Yes NS
3 1406 ± 545 2087 ± 760 2917 ± 1888 2.322 0.13
4 479 ± 336 343 ± 174 1108 ± 373 10.620 0.001 NS NS Yes
5 738 ± 429 1468 ± 494 1846 ± 713 6.098 0.012 NS NS NS
6 770 ± 318 1161 ± 392 1497 ± 610 3.801 0.046 NS NS NS
7 1393 ± 651 693 ± 242 2480 ± 689 15.249 < 0.001 Yes NS Yes
8 1619 ± 991 2007 ± 935 1838 ± 691 0.292 0.75
9 551 ± 237 1050 ± 302 1942 ± 770 12.075 0.001 NS Yes NS
10 366 ± 81 801 ± 214 1152 ± 199 30.347 < 0.001 Yes Yes Yes
11 1665 ± 974 1869 ± 934 2184 ± 932 0.458 0.64
12 1511 ± 543 1867 ± 1001 931 ± 370 2.802 0.09
13 451 ± 102 2066 ± 1130 1257 ± 324 8.430 0.004 NS Yes NS
14 1054 ± 371 1733 ± 549 1309 ± 402 3.525 0.06
15 988 ± 653 2064 ± 1194 1503 ± 641 2.304 0.13
16 758 ± 274 904 ± 302 1631 ± 631 6.973 0.007 NS NS NS
ANOVA = analysis of variance; C = consultant surgeons; J = junior trainees; NS = nonsignificant; S = senior trainees; SD = standard deviation. *p = 0.05, corrected for 3 comparisons.
novel-schlachta.indd 89 2015-03-10 7:55 AM

RECHERCHE
90 J can chir, Vol. 58, No 2, avril 2015
surgical performance. This rating scale was composed of 12 items assessing mainly technical performance.
Since publication of that report, a growing body of evidence has been produced that demonstrates correlation between performance on various tests of visual–spatial ability and surgical performance.8 These studies have focused on a range of topics from measures of whole surgical tasks assessed in a laboratory setting to overall assessment of clinical performance. There seems to be stronger correlation between task performance and high-level visual–spatial abilities, such as 3D spatial rotations.
Relevant to the performance of laparoscopic surgery, a unique method for gauging the perceived depth relations of objects presented in a 2D display provided some support for the claim that visual perceptual skills necessary for understanding 3D structure can be improved with prac-tice.9 However, some neurophysiological studies10,11 have suggested that in specific perceptual learning, the benefits of perceptual training would be relatively limited.
In the present study, we focused on the initial percep-tion and spatial reasoning skills needed to initiate perform-ing a particular surgical procedure. Based on the presump-tion that in order to dissect a tissue plane one must first be able to visualize that plane, we developed a novel technique for assessing the ability of surgeons to identify dissection planes on static images acquired from actual surgical pro-cedures. It was the goal of this pilot study to evaluate the tool by determining whether there are measurable per-form ance differences between surgeons and trainees.
Despite our small number of participants, we found significant differences consistent with our a priori hypoth-esis that recognition of surgical planes is a skill acquired through experience. Considering the within-group vari-ability as an inverse measure of concordance or group precision, we found that we were able to demonstrate a stepwise increase in precision from junior trainees to consult ant surgeons.
Table 2. Mean difference from consultant group
Mean distance ± SD (pixels)
Image S v. C J v. C p value
1 1481 ± 789 1470 ± 988 0.97
2 1051 ± 541 1559 ± 844 0.05
3 1694 ± 917 3183 ± 1365 0.001
4 477 ± 274 1642 ± 667 < 0.001
5 1133 ± 503 1610 ± 526 0.014
6 1019 ± 412 1557 ± 144 < 0.001
7 1245 ± 669 1956 ± 533 0.002
8 1711 ± 1046 1963 ± 712 0.43
9 776 ± 286 1329 ± 327 < 0.001
10 584 ± 248 1271 ± 456 < 0.001
11 1747 ± 782 2605 ± 767 0.004
12 1706 ± 683 731 ± 398 < 0.001
13 1843 ± 1282 1296 ± 462 0.13
14 1384 ± 495 1861 ± 596 0.020
15 1766 ± 1178 2068 ± 780 0.40
16 774 ± 332 1685 ± 843 < 0.001
C = consultant surgeons; J = junior trainees; S = senior trainees; SD = standard deviation.
Fig. 2. Consultant surgeons’ responses for image 5.
Rectum
Sacrum
Fig. 3. Senior trainees’ responses for image 5.
Rectum
SacrumFig. 4. Junior trainees’ responses for image 5.
Rectum
Sacrum
novel-schlachta.indd 90 2015-03-10 7:55 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 91
Limitations
One of the limitations of our methodology is the unavail-ability of a “correct” plane to use as a reference standard. Therefore, in order to assess accuracy we chose to consider the expert (consultant surgeons) group as the reference standard against which we compared trainee groups. We argue that in many instances the perfect plane of dissection may be a matter of conjecture. Using the experts as a con-trol group, we preserved the variability inherent in multi-ple opinions. We anticipate that a larger number of experts would narrow this variability or improve the precision of the expert group. Interestingly, for this pilot study our small sample size was still sufficient to demonstrate that senior trainees were predominantly more accurate than junior trainees, which was consistent with our hypothesis.
One of the potential confounders of this study is con-tent validity. It is possible that rather than testing differ-ences in ability to perceive tissue planes, we are simply testing differences in trainees’ familiarity with this particu-lar surgical procedure based on their experience and recall. Some of the lines drawn by junior trainees were not only away from the ideal plane, but also clearly demonstrated a lack of recognition of either the anatomy or the next step in the procedure. Future study will need to include an assessment of procedure-specific experience to determine whether this represents an overriding factor.
Another potential weakness is the small number of par-ticipants in this pilot study. Despite the ability to appreci-ate significant differences among the study groups for many of the images, the response of a single individual has the potential to have a large effect on the group. This will be addressed in future studies with larger study groups.
It would be a valid criticism to argue that in practice many factors contribute to the dynamic recognition of sur-gical planes. The purpose of this pilot was simply to deter-mine if our methodology would be sensitive enough to dis-criminate between novices and experts based on static images alone. Given that we demonstrated the ability of this methodology to detect expected differences among study groups, we now have the possibility in future endeav-ours to study the effect of additional clues. This is an area ripe for further investigation, including the use of lead-in video to static images, the contribution of innate psycho-motor ability, the difference in visual clues obtained from open compared with laparoscopic surgery or even the role of narrow band imaging. Some of these areas are already being pursued at our institution.
Not all of the images used in this study contributed to significant findings, which may be a result of type-II error owing to the small sample size. It is also possible that some images were less discriminating than others. Future study will require evaluating a larger library of images so that a better understanding of what represents a discriminating image can be developed.
ConClusion
Our pilot study demonstrated a novel method of evalu-ating visual perception and spatial reasoning of surgical tissue planes. This method shows promise as a tool that possesses the sensitivity to discriminate between levels of experience of surgical trainees. Many questions remain to be addressed through future study and work already in progress. With further development, this methodology has the potential to be developed into both an assessment tool and a training tool to enhance surgical instruction.Acknowledgements: This research was supported in part by a grant from the Ontario Research Fund, Research Excellence program.
Affiliations: From the Canadian Surgical Technologies and Advanced Robotics, London Health Sciences Centre (Schlachta, Ali, Ahmed, Eagleson); the Department of Surgery, Schulich School of Medicine and Dentistry, Western University (Schlachta, Ali, Ahmed); and the Faculty of Engineering, Western University (Eagleson), London, Ont.
Competing interests: None declared.
Contributors: C. Schlachta and R. Eagleson designed the study. C. Schlachta acquired the data, which all authors analyzed. C. Schlachta and R. Eagleson wrote the article, which all authors reviewed and approved for publication.
References
1. Wibe A, Moller B, Norstein J, et al. A national strategic change in treatment policy for rectal cancer — implementation of total meso-rectal excision as routine treatment in Norway. A national audit. Dis Colon Rectum 2002;45:857-66.
2. West NP, Morris EJA, Rotina O, et al. Pathology grading of colon cancer surgical resection and its association with survival: a retro-spect ive observational study. Lancet Oncol 2008;9:857-65.
3. Imamura H, Seyama Y, Kokudo N, et al. One thousand fifty-six hepatectomies without mortality in 8 years. Arch Surg 2003;138: 1198-206.
4. Hausdorff F. Dimension und äusseres mass [article in German]. Math Ann 1918;79:157-79.
5. Marr D. Vision: a computational investigation into the human repre-sentation and processing of visual information. New York (NY): Free-man; 1982.
6. Anastakis DJ, Hamstra SJ, Matsumoto ED. Visual–spatial abilities in surgical training. Am J Surg 2000;179:469-71.
7. Schueneman AL, Pickleman J, Hesslein R, et al. Neuropsychologic predictors of operative skill among general surgery residents. Surgery 1984;96:288-95.
8. Maan ZN, Maan IN, Darzi AW, et al. Systematic review of predict-ors of surgical performance. Br J Surg 2012;99:1610-21.
9. Sidhu RS, Tompa D, Jang RW, et al. Interpretation of three- dimensional structure from two-dimensional endovascular images: implications for educators in vascular surgery. J Vasc Surg 2004;39: 1305-11.
10. Fahle M. Specificity of learning curvature, orientation, and vernier discriminations. Vision Res 1997;37:1885-95.
11. Yotsumoto Y, Watanabe T, Sasaki Y. Different dynamics of per-form ance and brain activation in the time course of perceptual learn-ing. Neuron 2008;57:827-33.
novel-schlachta.indd 91 2015-03-10 7:55 AM

RESEARCH • RECHERCHE
92 J can chir, Vol. 58, No 2, avril 2015 ©2015 8872147 Canada Inc.
The integration of minimally invasive surgery in surgical practice in a Canadian setting: results from 2 consecutive province-wide practice surveys of general surgeons over a 5-year period
Background: Although minimally invasive surgery (MIS) has been quickly embraced, the introduction of advanced procedures appears more complex. We assessed the evo-lution of MIS in the province of Quebec over a 5-year period to identify areas for improvement in the modern surgical era.
Methods: We developed, test-piloted and conducted a self-administered question-naire among Quebec general surgeons in 2007 and 2012 to examine stated MIS prac-tice, MIS training and barriers and facilitators to the use of MIS.
Results: Response rates were 51.3% (251 of 489) in 2007 and 31.3% (153 of 491) in 2012. A significant increase was observed for performance of most advanced MIS pro-cedures, especially for colectomy for benign (66.0% v. 84.3%, p < 0,001) and malig-nant diseases (43.3% v. 77.8%, p < 0,001) and for rectal surgery for malignancy (21.0% v. 54.6%, p < 0.001). More surgeons practised 3 or more advanced MIS pro-ced ures in 2012 than in 2007 (82.3% v. 64.3%, p < 0,001). At multivariate analysis, the 2007 survey administration was associated with fewer surgeons practising advanced MIS (odds ratio 0.13, 95% confidence interval 0.06–0.29). In 2012, more respondents stated they gained their skills during residency (p = 0.028).
Conclusion: From 2007 to 2012 there was a significant increase in advanced MIS pro-cedures practised by general surgeons in Québec. This technique appears well estab-lished in current surgical practice. The growing place of MIS in residency training seems to be a paramount part of this development. Results from this study could be used as a baseline for studies focusing on ways to further improve the MIS practice.
Contexte : Malgré l’adoption récente rapide de la chirurgie minimalement invasive (CMI), son utilisation pour les procédures complexes semble plus ardue. Afin d’identifier comment améliorer sa pratique, nous avons examiné l’utilisation de la CMI dans la province de Québec sur une période de 5 ans.
Méthodes : Nous avons développé, piloté, et distribué un questionnaire auto- administré aux chirurgiens généraux du Québec en 2007 et en 2012, afin d’examiner la pratique auto-rapportée de la CMI, la formation en CMI, et les barrières et facilitateurs à l’utilisation de la CMI.
Résultats : Le taux de réponse était de 51,3 % (251 sur 489) en 2007 et 31,3 % (153 sur 491) en 2012. L’utilisation de la majorité des procédures avancées de CMI a aug-menté, particulièrement la colectomie pour maladie bénigne (66,0 % c. 84,3 %, p < 0,001) et maligne (43,3 % c. 77,8 %, p < 0,001), et la résection rectale pour cancer (21,0 % c. 54,6 %, p < 0,001). Plus de chirurgiens pratiquaient 3 procédures avancées de CMI ou plus en 2012 qu’en 2007 (82,3 % c. 64,3 %, p < 0,001). L’analyse multi-variée a indiqué que l’administration du questionnaire en 2007 était associée avec moins de chirurgiens pratiquant des procédures avancées de CMI (rapport de cote 0,13, intervalle de confiance à 95 % 0,05–0,29). En 2012, plus de répondants ont indiqué avoir obtenu leur expertise en CMI durant la résidence (p = 0,028).
Conclusion : De 2007 à 2012, la pratique de procédures avancées de CMI a augmenté significativement dans la province de Québec. L’approche minimalement invasive apparait solidement établie dans la pratique chirurgicale actuelle. La place grandissante de la CMI dans les programmes de résidence semble avoir été cruciale dans cet essor. Les résultats de cette étude peuvent maintenant servir à développer d’autres projets visant à améliorer encore davantage la pratique de la CMI.
Julie Hallet, MD Olivier Mailloux, MD Mony Chhiv, MD Roger C. Grégoire, MD Jean-Pierre Gagné, MD, LLM
This paper was submitted as an abstract for presentation at the SAGES 2013 Annual Meeting.
Accepted for publication Aug. 20, 2014
Correspondence to: J.P. Gagné 10, rue de l’Espinay CHU de Québec — Hôpital Saint-François d’Assise Québec QC G1L 3L5 [email protected]
DOI: 10.1503/cjs.019713
integra-hallet.indd 92 2015-03-10 7:58 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 93
L aparoscopic surgery has been one of the most important revolutions in surgery in the last century. The widespread use of this technique grew to be known as
minimally invasive surgery (MIS). Many reports have now highlighted the benefits of the laparoscopic over the open approach for the treatment of a variety of conditions, mainly through a decrease in pain, blood loss, length of hospital stay and complications.1,2
Most surgeons quickly adopted laparoscopic cholecystectomy, but the introduction of major procedures can appear more complex. General surgeons in Canada have been able to follow the trend of the rising popularity of MIS to satisfy health services and increased public expectations, but the use of advanced MIS procedures has been variable.3,4 The implementation of an MIS practice requires multiple conditions, such as technical skills and adapted tools. As these conditions vary among hospitals, the use of MIS may differ within a single health system. Moreover, the last few years have witnessed a quest for the least invasive procedure possible, with the advent of natural orifice transluminal endoscopic surgery (NOTES), singleport surgery or robotic surgery. Before considering widespread introduction of these latter techniques in current surgical practice, we need to better understand how previous developments have already been integrated.
To assess the current state of modern surgical practice, our aim was to describe the practice of MIS in the province of Quebec, the factors affecting it and its evolution over a 5year timeframe. Therefore, in 2007 and 2012, we conducted practice surveys of Quebec general surgeons to determine selfreported MIS practice and training as well as the factors perceived to affect this surgical activity.
Methods
Sampling frame
The survey population was composed of Quebec’s general surgeons working in both universityaffiliated and com mun ity hospitals. In 2007 and 2012, postal or email addresses of potential respondents were obtained through the membership database of the Quebec Surgical Association (QSA), membership in which is mandatory. The final list included 489 potential respondents in 2007 and 491 in 2012.
Questionnaire development
The questionnaire was developed by a group of experts composed of academic surgeons specialized in MIS who identified important domains and specific issues within those domains, highlighting those most pertinent to MIS practice. We first generated items without restriction, grouped them into domains, and proceeded to item reduction in order to retain only the most relevant ones.5
The questionnaire was designed using this final list of domains and items. The chosen domains were 1) parameters of surgical practice, 2) stated type of MIS practice, 3) MIS training, 4) barriers to MIS practice and 5) facilitators of MIS practice. Questions were constructed using closed answers. Advanced MIS procedures included all MIS procedures other than appendectomy, cholecystectomy and diagnostic laparoscopy. As both community and academic general surgeons in Quebec practise thoracic, endocrine or liver surgery, subspecialized procedures were included in this list. We used a 5point Likert scale to assess the perceived importance of potential barriers and facilitators on an agree–disagree continuum. We testpiloted the original questionnaire by inviting 5 surgeons to complete it. These individuals were asked to provide feedback about the flow, the clarity and the ease of administration of the questionnaire. The questionnaire was reviewed accordingly.
Questionnaire administration
In 2007, the survey was selfadministered in French in a written form. No incentive was offered to complete the questionnaire. Each potential respondent received a mailed invitation to complete the survey. Two reminders were sent over a 6month period. An administrative assistant compiled the final database of completed questionnaires. No identifying information was included. In 2012, the survey was administered in a webbased format using SurveyMonkey, and email invitations were sent to all potential respondents. Reminders and compilation of data were done in a similar way as in 2007.
Data analysis
By aiming for a 60% response rate, we expected a precision of 5.7% in both 2007 and 2012. The precision for these surveys was 6.2% in 2007 and 7.9% in 2012.5 We first performed descriptive analysis of completed questionnaires for both administration periods separately. Continuous data are expressed using means ± standard deviations (SDs) or medians and interquartile ranges (IQRs), as appropriate, and categorical data are reported as numbers and proportions. We conducted a univariate analysis to compare answers from respondents in 2007 and 2012, using a 2sample t test, Fisher exact test or Pearson χ2 test, as appropriate. We performed multivariate analysis using logistic regression to assess the variables associated with an advanced MIS practice (≥ 3 advanced MIS procedures). The year of survey administration as well as potential confounding variables were included in this model. Results are presented as odd ratios (ORs) with 95% confidence intervals (CIs). Data were considered to be significant at p < 0.05. Statistical analyses were conducted using XLSTAT version 2011.5 (Addinsoft SARL) for Microsoft Excel.
integra-hallet.indd 93 2015-03-10 7:58 AM

RECHERCHE
94 J can chir, Vol. 58, No 2, avril 2015
Results
In 2007, 251 (51.3%) of the general surgeons surveyed completed the questionnaire, whereas 153 (31.3%) completed it in 2012. There were 12 exclusions in 2007 (retired surgeons) and none in 2012 (Fig. 1).
Demographic characteristics and surgical practice parameters
Demographic data and surgical practice parameters of respondents are presented in Table 1. No significant difference was observed between the characteristics of respondents in 2007 and 2012, except that there were fewer respondents working in areas with a population of 50 000–500 000 individuals in 2007 (45,7% v. 57.9%, p = 0.020). Parameters of the surgical practice of respondents did not differ significantly between 2007 and 2012.
MIS practice characteristics
Table 2 presents MIS practice characteristics. Regarding basic MIS procedures, there was a significant increase in the
number of surgeons practising laparoscopic appendectomies from 2007 to 2012 (82.3% v. 94%, p = 0.003). More surgeons reported always using an open technique for pneumoperitoneum establishment in 2012 (63.5% v. 76% p = 0.011). The 2012 survey showed an increased number of surgeons reporting the practice of 3 or more advanced MIS procedures (64.3% v. 82.3%, p < 0.001).
Details regarding the type of advanced MIS procedures performed are included in Table 2. The most commonly performed procedure reported in both surveys was colectomy for benign disease followed by the same surgery for malignancy. More surgeons reported practising these procedures in 2012 for both benign (66.%0 v. 84.3%, p < 0.001) and malignant indications (43.3% v. 77.8%, p < 0.001). The least often performed procedures at both time points were liver and lung resections.
MIS training
Perceptions of respondents on MIS training are reported in Table 3. From 2007 to 2012, the number of respondents stating that they gained their skills during residency (p = 0.028) or by selftraining (p < 0.001) increased. In
Fig. 1. Flow diagram of respondents. QSA = Québec Surgical Association.
Potential respondents identi�ed (members of the QSA)
n = 489
Potential respondents identi�ed (members of the QSA)
n = 491
Mailed invitations sent out n = 489
Email invitations sent out n = 491
Questionnaires completed n = 251
Questionnaires completed n = 153
Questionnaires excluded
n = 12 (retired surgeons)
Questionnaires included in descriptive analysis
n = 239
Questionnaires included in descriptive analysis
n = 153
Questionnaires excluded n = 0
Questionnaires included in comparison analysis
n = 392
integra-hallet.indd 94 2015-03-10 7:58 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 95
both 2007 and 2012, most respondents perceived that the responsibility of MIS training lies with provincial surgical societies (92.0% in 2007 and 90.4% in 2012), national surgical societies (82.1% in 2007 and 91.7% in 2012) and universities (57.4% in 2007 and 62.5% in 2012).
Barriers and facilitators to MIS practice
Significant differences in barriers and facilitators to MIS practice were observed between 2007 and 2012. More respondents in 2012 disagreed or strongly disagreed that
Table 2. Comparison of the characteristics of MIS practice between 2007 and 2012
Characteristic 2007 survey 2012 survey p value
Basic MIS procedures performed, no. (%)
Cholecystectomy 214 (90) 141 (94,0) 0.45
Diagnostic laparoscopy 214 (90) 145 (96,0) 0.09
Appendectomy 196 (82,3) 141 (94,0) 0.003
Technique used for pneumoperitoneum, no. (%)
Always open (Hasson) 141 (63.5) 114 (76) 0.011
Always closed (Veress) or both 81 (36.5) 36 (24) 0.011
Number of advanced MIS procedures performed, no. (%)
No advanced procedure 36 (15.1) 10 (6.5) 0.011
1–2 advanced procedures 49 (20.6) 17 (11.1) 0.013
≥ 3 advanced procedures 153 (64.3) 126 (82.3) < 0.001
Type of advanced procedures performed, no. (%)
Nissen fundoplication 90 (37.8) 75 (49) 0.029
Heller myotomy 52 (21.8) 51 (33.3) 0.012
Gastric resection 30 (12.6) 51 (33.3) < 0.001
Liver resection 13 (5.46) 9 (5.9) 0.86
Biliary tract exploration 31 (13) 20 (13.1) 0.18
Distal pancreatectomy 21 (8.8) 27 (17.6) 0.009
Splenectomy 111 (46.6) 105 (68.6) < 0.001
Adrenalectomy 60 (25.2) 50 (32.7) 0.109
Colectomy (benign disease) 157 (66) 129 (84.3) < 0.001
Colectomy (malignant disease) 103 (43.3) 119 (77.8) < 0.001
Rectal resection (benign disease) 87 (36.5) 97 (63.8) < 0.001
Rectal resection (malignant disease) 50 (21) 83 (54.6) < 0.001
Inguinal hernia repair 73 (30.7) 55 (36.2) 0.28
Ventral hernia repair 92 (38.7) 105 (68.6) < 0.001
General video assisted thoracoscopy (pneumothorax or pleural effusion)
74 (31.1) 53 (34.6) 0.47
Video-assisted thoracoscopy for lung resection 33 (13.9) 16 (10.5) 0.32
MIS = minimally invasive surgery.
Table 1. Comparison of respondents’ demographics and practice characteristics between 2007 and 2012
Characteristic 2007 survey 2012 survey p value
Age, mean ± SD yr 45.1 ± 10.6 43.7 ± 10 0.20
Male sex, no. (%) 141 (70.8) 106 (70.7) 0.97
Fellowship training, no. (%) 74 (31.1) 46 (30.7) 0.93
Surgical experience, mean ± SD yr 14.8 ± 10.7 13.5 ± 9.6 0.24
Community practice, no. (%) 114 (48.1) 85 (55.6) 0.15
Population, no. (%)
< 50 000 54 (22.9) 26 (17.1) 0.17
50 000–500 000 108 (45.7) 88 (57.9) 0.02
> 500 000 individuals 74 (31.4) 38 (25) 0.18
Weekly operating time, mean ± SD d 1.4 ± 1.5 1.6 ± 1.3 0.32
Waiting time for malignant disease, mean ± SD wk 3.2 ± 2.0 3.7 ± 3.3 0.10
Waiting time for benign disease, mean ± SD wk 18 ± 31.2 17.3 ± 23.3 0.84
SD = standard deviation.
integra-hallet.indd 95 2015-03-10 7:58 AM

RECHERCHE
96 J can chir, Vol. 58, No 2, avril 2015
insufficient operative time (p < 0.001), lack of hospital resources (p < 0.001), lack of training opportunities (p < 0.001), lack of support from the hospital (p < 0.001) or insufficient remuneration (p = 0.06) were important barriers to MIS practice. In both surveys, most respondents did not believe that that the lack of scientific evidence or medicolegal issues were obstacles to the implementation of MIS (Table 4).
Multivariate analysis
On multivariate analysis, the 2007 survey administration was associated with significantly fewer surgeons reporting an advanced MIS practice (≥ 3 advanced MIS procedures; OR 0.13, 95% CI 0.06–0.29). Other variables associated with not practising advanced MIS were age (56–65 yr: OR 0.33, 95% CI 0.13–0.82; > 65 yr: OR 0.15, 95% CI 0.03–0.81), working in a community of fewer than 50 000 individuals (OR 0.4, 95% CI 0.19–0.83) and not performing MIS appendectomy (OR 0.04, 95% CI 0.01–0.10). The
surgeons’ experience (years in practice), community practice setting and the lack of fellowship training were not associated with the number of advanced procedures performed (Table 5).
Discussion
The benefits of MIS over open surgery are well established in terms of decreased postoperative pain, blood loss, length of hospital stay and complications,1,2 and this technique is now part of modern general surgery practice; MIS even represents the standard of care in some cases.6–9 The ability of general surgeons to learn and apply these new skills is paramount to keep up with the rapidly evolving field of general surgery. Our study illustrates the evolution of MIS practice in Quebec over a 5year period 30 years after its introduction. We observed a significant increase in the number of advanced MIS procedures practised in the province from 2007 to 2012, with more surgeons performing 3 or more advanced techniques in 2012
Table 3. Comparison of respondents’ perceptions regarding MIS training between 2007 and 2012
Respondents, no. (%)
Sources of MIS training, yrStrongly disagree Disagree Neutral Agree
Strongly agree p value
During residency
2012 24 (17,0) 8 (5.7) 3 (2.1) 44 (31.2) 62 (44.0)
2007 49 (25.9) 16 (8.5) 8 (4.2) 63 (33.3) 53 (28) 0.028
Self-training
2012 5 (3.5) 8 (5.6) 12 (8.3) 73 (50.7) 4 (31.9)
2007 23 (10.9) 11 (5.2) 28 (13.3) 85 (40.5) 63 (30) < 0.001
Help of colleagues
2012 11 (7,9) 8 (5,7) 9 (6,5) 83 (59,7) 28 (20,1)
2007 19 (9,3) 10 (4,9) 27 (13.2) 94 (45,8) 55 (26,8) 0.28
QSA CME seminars
2012 30 (20.7) 13 (9.9) 19 (14.4) 50 (37.9) 20 (15.1)
2007 58 (30.4) 21 (11) 24 (12.6) 59 (30.9) 29 (15.2) 0.54
MIS fellowship
2012 61 (52.6) 12 (10.3) 21 (18.1) 14 (12.1) 8 (6.9)
2007 100 (60.6) 8 (4.8) 18 (11) 19 (11.5) 20 (12.1) 0.09
Organizations responsible for MIS training
University
2012 2 (1.4) 3 (2.1) 7 (4.8) 70 (48.3) 63 (43.4) 0.09
2007 7 (3.8) 9 (4.9) 17 (9.2) 69 (37.5) 82 (44.6)
QSA
2012 1 (0.7) 2 (2.0) 10 (6.8) 87 (59.1) 46 (31.3) 0.045
2007 12 (6.5) 2 (1.1) 19 (10.3) 91 (49.8) 59 (42.2)
CAGS
2012 8 (5.9) 9 (6.6) 34 (25) 60 (44.1) 25 (18.4) 0.41
2007 20 (11.8) 10 (5.9) 42 (24.8) 63 (37.3) 34 (20.1)
CAGS = Canadian Association of General Surgeons; CME = continued medical educatiuon; MIS = minimally invasive surgery; QSA = Québec Surgical Association
integra-hallet.indd 96 2015-03-10 7:58 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 97
(64.3% v. 82.3%, p < 0.001). Colectomy for benign dis-ease remained the most commonly performed MIS according to both surveys (66.0% in 2007 and 84.3% in
2012). Most respondents stated that they acquired their MIS skills during residency or by self-training. Major variables of surgical practice, including operating time and
Table 4. Comparison of respondents’ perceptions barriers to MIS practice between 2007 and 2012
Respondents, no. (%)
Barriers to MIS practice, yrStrongly disagree Disagree Neutral Agree
Strongly agree p value
Insufficient operating time
2012 42 (29.2) 51 (35.4) 10 (6.9) 31 (21.5) 10 (6.9)
2007 49 (22.6) 35 (16.1) 21 (9.7) 46 (21.2) 66 (30.4) < 0.001
Lack of hospital resources
2102 31 (21.7) 53 (37.1) 12 (9.1) 43 (30.1) 2 (2.1)
2007 40 (18.4) 38 (17.5) 39 (18) 66 (30.4) 34 (15.7) < 0.001
Lack of training opportunities
2012 37 (26.1) 62 (43.7) 12 (9.9) 24 (16.9) 5 (3.5)
2007 58 (27.7) 58 (27.7) 42 (20) 31 (14.8) 21 (10) < 0.001
Lack of support from the hospital
2012 41 (28.5) 59 (40.1) 19 (13.2) 23 (16) 2 (1.4)
2007 48 (22.3) 51 (23.7) 46 (21.4) 41 (19.1) 29 (13.5) < 0.001
Insufficient remuneration
2012 43 (29.9) 42 (29.2) 23 (16) 30 (20.1) 6 (4.2)
2007 61 (28.4) 31 (14.4) 48 (22.3) 44 (20.5) 21 (14.4) 0.006
Insufficient evidence-based data
2012 55 (38.5) 57 (38.9) 17 (11.9) 14 (9.8) 0 (0)
2007 71 (33.3) 68 (32) 43 (20.2) 26 (12.2) 5 (2.3) 0.05
Medicolegal issues
2012 58 (41.11) 48 (34) 23 (16.3) 10 (7.1) 2 (1.4)
2007 89 (42) 55 (26) 43 (20.2) 18 (8.5) 7 (3.3) 0.40
MIS = minimally invasive surgery.
Table 5. Mutlivariate regression of variables associated with advanced MIS practice (performance of 3 or more MIS procedures performed)*
VariableCoefficient estimate SD OR† (95% CI) p value‡
Intercept 3.77 0.75 < 0.001
2007 survey administration –2.02 0.40 0.13 (0.06–0.29) < 0.001
Female sex –0.48 0.37 0.62 (0.3–1.27) 0.19
Surgeon age, yr
< 35 0.53 0.53 1.70 (0.6–4.85) 0.32
46–55 0.30 0.46 1.35 (0.54–3.33) 0.52
56–65 –1.11 0.46 0.33 (0.13–0.82) 0.021
> 65 –1.88 0.85 0.15 (0.03–0.81) 0.030
> 10 years in practice –0.31 0.42 0.73 (0.32–1.69) 0.46
No fellowship training 0.34 0.43 1.4 (0.6–3.28) 0.43
Population
< 50 000 –0.93 0.38 0.4 (0.19–0.83) 0.011
> 500 000 0.63 0.47 1.88 (0.75–4.72) 0.18
Community practice –0.47 0.43 0.62 (0.27–1.45) 0.27
Weekly operating time (days) 0.05 0.12 1.05 (0.84–1.32) 0.67
Open technique for pneumoperitoneum
–0.38 0.34 0.68 (0.35–1.34) 0.27
Not performing MI appendectomy
–3.2 0.46 0.04 (0.02–0.1) < 0.001
CI = confidence interval; MI = minimally invasive; MIS = minimally invasive surgery; OR = odds ratio; SD = standard deviation. *Number of advanced MIS procedures performed (< 2 v. ≥ 3) compared using logistic regression, Nagelkerke R2 = 0.453. †OR > 1 denotes increased practice of ≥ 3 MIS procedures; OR < 1 denotes decreased practice of ≥ 3 MIS procedures. ‡Wald χ2 test.
integra-hallet.indd 97 2015-03-10 7:58 AM

RECHERCHE
98 J can chir, Vol. 58, No 2, avril 2015
hospital resources, were not perceived to be barriers to MIS practice, a trend that became more polarized in 2012.
When discussing the benefits of MIS for the treatment of various surgical conditions, the importance of surgical expertise in achieving these results is often highlighted: advanced MIS procedures are deemed beneficial if performed by experienced hands.10 Our data show that the practice of basic and advanced MIS has significantly increased in Quebec in the last 5 years. Advanced MIS procedures that were once restricted to tertiary care settings have now widely spread. Multivariate analysis confirmed that the year of survey administration was significantly associated with an advanced MIS practice (OR 0.13 OR, p < 0.001) for the 2007 administration.
Appendectomy was one of the first procedures to be per-formed laparoscopically and is now one of the first laparo-scopic techniques taught to general surgery residents. How-ever, only 60.3% of general surgeons in Ontario performed minimally invasive (MI) appendectomies in 2004, as reported in a study from that province published in 2004.4 Our survey had more encouraging results, with 94% of Quebec general surgeons practising MI appendectomy in 2012, which repre-sents a significant increase over 2007 (82.3%, p = 0.003). In 2002–2003, a review of the practice of appendectomy in Quebec revealed that MIS was favoured in only 35% of cases of appendicitis.11 The growing place of MIS in surgical prac-tice may parallel this continued rising trend for MI appen-dectomy. Indeed, the Ontario survey observed that surgeons who practised MI appendectomy were more prone to do advanced MIS on univariate analysis (81.5% v. 39.1%, p < 0.05). Multivariate analysis from the present study revealed that not practising MI appendectomy was associated with a lower proportion of surgeons with an advanced MIS practice (OR 0.04, 95% CI 0.02–0.1). Poulin and colleagues12 sug-gested that laparoscopic appendectomy is an interesting training procedure with which to transition toward laparo-scopic colectomy. Ultimately, one may hypothesize that sur-geons who do not practise MI appendectomy could be less comfortable with more advanced MI procedures.
The new generation of practising surgeons who have been trained in the MIS era may also contribute to the observed spread of advanced MIS procedures. Evolution over a few decades has allowed better integration of MIS not only in practice, but also in training with the development of new teaching tools and curricula.13–16 In the United States, specific requirements for MIS training have even been added by the Accreditation Council for Graduate Medical Education Resi-dency Review Committee, and the Fundamentals of Laparo-scopic Surgery course is now mandatory for the American Board of Surgery.17,18 Surveys of residents conducted in the early 2000s reported a perceived need for additional training in MIS both in Canada and in the United States.19,20 In 2003, Canadian general surgery residents identified limited advanced case volume, limited opportunity in the operating room and lack of attending surgeon interest as factors with a
negative impact on their MIS training.19 With the evolution of the practice, this seems to have changed. In our survey, more respondents attributed their MIS training to residency (p = 0.028) in 2012 than in 2007. This reflects the adaptation of surgical training programs. Interestingly, universities were the last institution identified by respondents as being respon-sible for MIS training, which appear to contradict previously discussed findings. One hypothesis would be that with better MIS residency training, respondents feel that additional train-ing for either maintenance of competence or acquisition of new skills then lies with surgical societies.
The practice of MIS relies on training but also on the available material resources and support, such as operating time or proper, up-to-date equipment. It takes time to build facilities and practice settings favouring adequate use of surgeons’ skills, such as MIS. The 5-year lapse between our surveys seems to have allowed for these conditions to be united. Indeed, respondents did not identify significant institutional or clinical barriers to MIS practice. This was even more polarized in 2012, which may represent improvement in hospital resources. Interestingly, operat-ing time was less of an issue in 2012 than in 2007. This could simply be related to a change in availability of oper-ating time for general surgeons, but it could also represent a better use of this time by surgeons more efficient in MIS.
Other findings from our survey parallel the evolution of data in MIS and testify to the changing culture in this field. First, the number of surgeons who practise colorectal resec-tions for malignancy has nearly doubled in 5 years. This is in keeping with the acceptance of the MIS approach as a safe oncological procedure for colonic malignancies and the grow-ing evidence for laparoscopic treatment of rectal cancer.21–23 Second, the number of MI inguinal hernia repairs performed did not differ between 2007 and 2012 (30.7% v. 36.2%, p = 0.28). Indeed, after being subject to great interest in the late 1990s and early 2000s, this technique lost popularity because of a reported higher rate of severe complications.24,25 Third, we observed a significant difference in the preferred tech-nique for pneumoperitoneum creation. More respondents reported always using an open technique in 2012 than 2007 (63.5% v. 76%, p = 0.011). Although this viewpoint has been challenged, the literature suggests that the open approach is superior to the closed entry technique because it is less likely to cause complications.26–28 Our data are also in keeping with a survey of Canadian general surgeons reporting that more than 80% of them use the open technique.29
Limitations
The 51.3% and 31.3% response rates in 2007 and 2012 tem-per with the conclusions to be drawn from this survey. This represents an inherent challenge of survey studies, and is not out of the ordinary for a physician survey.5 The difference in the number of responses in both administrations might be due to the change of the administration tool from a written form
integra-hallet.indd 98 2015-03-10 7:58 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 99
to a web-based electronic platform. This renders the signifi-cant differences observed in the study more prone to the response bias inherent to survey studies. Indeed, surgeons with a greater interest or an established practice in MIS may have been keener to complete the questionnaire. Furthermore, this low response rate may also portend underpower issues, where lack of difference has to be interpreted with caution. We also acknowledge that our data represent stated intentions and per-ceptions of one’s practice that may change with time and are not a perfect reflection of reality. Furthermore, questions addressed the number of surgeons performing MIS proced-ures but not the proportion of procedures actually performed using an MIS approach. Despite these limitations, we have collected interesting data about the evolution of MIS in Que-bec. Beyond a snapshot of MIS practice, this study allows us to focus on the evolution of MIS in the modern surgical era.
ConClusion
We observed that from 2007 to 2012 there was a signifi-cant increase in the practice of advanced MIS procedures by general surgeons in Quebec. More surgeons have inte-grated MIS procedures in their practices, and this tech-nique now appears well established in current surgical practice. The growing place of MIS in residency training seems to be a paramount part of this development over the last 5 years. Results from this survey could be used as a baseline for studies focusing on ways to further improve the existing MIS practice and examine the need for inte-grating newer technological advances in the current prac-tice in relation with evidence-based data in the field.Acknowledgements: The authors thank the administrative staff from the Québec Surgical Association for their collaboration in conducting this survey.
Affiliations: From the Division of General Surgery, Sunybrook Health Sciences Centre — Odette Cancer Centre, Toronto, Ont. (Hallet); the Department of Surgery, University of Toronto, Toronto, Ont. (Hallet); the Department of Surgery, Université Laval, Québec, Qué. (Mailloux, Chhiv, Grégoire, Gagné); and the Department of Surgery, CHU de Qué-bec — Hôpital Saint-François d’Assise, Québec Centre for Minimally Invasive Surgery (QCMIS), Québec, Qué. (Chhiv, Grégoire, Gagné).
Competing interests: None declared.
Contributors: J. Hallet, M. Chhiv, R. Grégoire and J.-P. Gagné designed the study. O. Mailloux, M. Chhiv, R. Grégoire and J.-P. Gagné acquired the data, which all authors analyzed. J. Hallet and J.-P. Gagné wrote the article, which all authors reviewed and approved for publication.
References
1. Sauerland S, Jaschinski T, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev 2010;(10):CD001546.
2. Keus F, de Jong JAF, Gooszen HG, et al. Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database Syst Rev 2006; (4):CD006231.
3. Wexler MJ, Hinchey EJ, Sampalis J, et al. Canadian laparoscopic surgery survey. Can J Surg 1993;36:217-24.
4. Chiasson PM, Pace DE, Schlachta CM, et al. Minimally invasive sur-gical practice: a survey of general surgeons in Ontario. Can J Surg 2004;47:15-9.
5. Burns KEA, Duffett M, Kho ME, et al. A guide for the design andconduct of self-administered surveys of clinicians.CMAJ 2008;179:245-52.
6. Smith CD, Weber CJ, Amerson JR. Laparoscopic adrenalectomy: new gold standard. World J Surg 1999;23:389-96.
7. Glasgow RE, Yee LF, Mulvihill SJ. Laparoscopic splenectomy: the emerging standard. Surg Endosc 1997;11:108-12.
8. Kuo PC, Johnson LB, Sitzmann JV. Laparoscopic donor nephrec-tomy with a 23-hour stay: a new standard for transplantation surgery. Ann Surg 2000;231:772–9.
9. Schlachta CM, Mamazza J, Gregoire R, et al. Could laparoscopic colon and rectal surgery become the standard of care? A review and experience with 750 procedures. Can J Surg 2003;46:432-40.
10. Tjandra JJ, Kilkenny JW, Buie WD, et al. Practice parameters for the management of rectal cancer. Dis Colon Rectum 2005;48:411-23.
11. Gagné J-P, Billard M, Gagnon R, et al. Province-wide population survey of acute appendicitis in Canada. New twists to an old disease. Surg Endosc 2007;21:1383-7.
12. Poulin EC, Gagné J-P, Boushey RP. Advanced laparoscopic skills acquisition: the case of laparoscopic colorectal surgery. Surg Clin North Am 2006;86:987-1004.
13. Fried GM, Feldman LS, Vassiliou MC, et al. Proving the value of simulation in laparoscopic surgery. Ann Surg 2004;240:518–25.
14. Palter VN, Grantcharov TP. Development and validation of a com-prehensive curriculum to teach an advanced minimally invasive pro-cedure: a randomized controlled trial. Ann Surg 2012;256:25-32.
15. Hamad GG, Curet M. Minimally invasive surgery. Am J Surg 2010; 199:263-5.
16. Fowler DL, Hogle N. The impact of a full-time director of min-imally invasive surgery: clinical practice, education, and research. Surg Endosc 2000;14:444-7.
17. Fundamentals of Laparoscopic Surgery website. Available: www .flsprogram.org (accessed 2012 Sept. 24).
18. Residency Review Committee [ACGME website]. Available: www.acgme .org/acWebsite/RRC_440/440_policyArchive.asp (accessed 2012 Sept. 24).
19. Chiasson PM, Pace DE, Schlachta CM, et al. Minimally invasive surgery training in Canada: a survey of general surgery. Surg Endosc 2003;17:371-7.
20. Rattner DW, Apelgren KN, Eubanks WS. The need for training oppor-tunities in advanced laparoscopic surgery. Surg Endosc 2001;15:1066-70.
21. Leung KL, Kwok SPY, Lam SCW, et al. Laparoscopic resection of rec-tosigmoid carcinoma: prospective randomised trial. Lancet 2004;363: 1187-92.
22. Jayne DG, Guillou PJ, Thorpe H, et al. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol 2007;25:3061-8.
23. Lujan J, Valero G, Biondo S, et al. Laparoscopic versus open surgery for rectal cancer: results of a prospective multicentre analysis of 4,970 patients. Surg Endosc 2012;27:295-302.
24. McCormack K, Scott NW, Go PM, et al. EU hernia trialists collab-oration. Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Database Syst Rev 2003; (1):CD001785.
25. O’Reilly EA, Burke JP, O’Connell PR. A meta-analysis of surgical morbidity and recurrence after laparoscopic and open repair of pri-mary unilateral inguinal hernia. Ann Surg 2012;255:846–53.
26. Merlin TL, Hiller JE, Maddern GJ, et al. Systematic review of the safety and effectiveness of methods used to establish pneumoperi-toneum in laparoscopic surgery. Br J Surg 2003;90:668-79.
27. Byron JW, Markenson G, Miyazawa K. A randomized comparison of Verres needle and direct trocar insertion for laparoscopy. Surg Gynecol Obstet 1993;177:259-62.
28. Bonjer HJ, Hazebroek EJ, Kazemier G, et al. Open versus closed establishment of pneumoperitoneum in laparoscopic surgery. Br J Surg 1997;84:599-602.
29. Compeau C, McLeod NT, Ternamian A. Laparoscopic entry: a review of Canadian general surgical practice. Can J Surg 2011;54:315-20.
integra-hallet.indd 99 2015-03-10 7:58 AM

RESEARCH • RECHERCHE
100 J can chir, Vol. 58, No 2, avril 2015 ©2015 8872147 Canada Inc.
Does more than a single chest tube for mediastinal drainage affect outcomes after cardiac surgery?
Background: The use of 1 or more mediastinal chest tubes has traditionally been routine for all cardiac surgery procedures to deal with bleeding. However, it remains unproven whether multiple chest tubes offer a benefit over a single chest tube.
Methods: All consecutive patients undergoing cardiac surgery (2005–2010) received at least 1 chest tube at the time of surgery based on surgeon preference. Patients were grouped into those receiving a single chest tube (SCT) and those receiving multiple chest tubes (MCT). The primary outcome was return to the operating room for bleeding or tamponade.
Results: A total of 5698 consecutive patients were assigned to 2 groups: 3045 to the SCT and 2653 to the MCT group. Patients in the SCT group were older, more often female and less likely to undergo isolated coronary artery bypass graft than those in the MCT group. Unadjusted outcomes for SCT and MCT, respectively, were return to the operating room for bleeding or tamponade (4.7% v. 5.0%; p = 0.50), intensive care unit stay longer than 48 hours (25.5% v. 27.9%; p = 0.041, postoperative stay > 9 days (31.5% v. 33.1%; p = 0.20) and mortality (3.8% v. 4.6%; p = 0.16). Logistic regression analysis, adjusted for clinical differences between groups, showed that the number of chest tubes was not associated with return to the operating room for bleeding or tamponade.
Conclusion: The use of multiple mediastinal chest tubes after cardiac surgery confers no advantage over a single chest tube in preventing return to the operating room for bleeding or tamponade.
Contexte : De tout temps, lors de chirurgies cardiaques, on a posé 1 ou plusieurs drains thoraciques médiastinaux pour gérer les saignements. Or, il n’a pas été démontré que la pose de plusieurs drains plutôt que d’un seul confère un avantage.
Méthodes : On a posé au moins un drain thoracique à tous les patients consécutifs soumis à une chirurgie cardiaque (2005–2010) au moment de l’intervention, selon la préférence des chirurgiens. Les patients ont été regroupés selon qu’on leur avait posé un seul drain thoracique (SDT) ou plusieurs (PDT). Le paramètre principal était le retour au bloc opératoire pour hémorragie ou tamponnade.
Résultats : En tout 5698 patients consécutifs ont été scindés en 2 groupes : 3045 dans le groupe SDT et 2653 dans le groupe PDT. Les patients du groupe SDT étaient plus âgés, plus souvent de sexe féminin et moins susceptibles de subir un pontage aortocoronarien isolé comparativement au groupe PDT. Les paramètres non ajustés pour les groupes SDT et PDT, respectivement, ont été retour au bloc opératoire pour hémorragie ou tamponnade (4,7 % c. 5,0 %; p = 0,50), séjour de plus de 48 heures à l’unité des soins intensifs (25,5 % c. 27,9 %; p = 0,04), durée du séjour postopératoire > 9 jours (31,5 % c. 33,1 %; p = 0,20) et mortalité (3,8 % c. 4,6 %; p = 0,16). L’analyse de régression logistique ajustée pour tenir compte des différences cliniques entre les groupes a révélé l’absence de lien entre le nombre de drains thoraciques et un retour au bloc opératoire pour hémorragie ou tamponnade.
Conclusion : La pose de plusieurs drains thoraciques plutôt que d’un seul après la chirurgie cardiaque ne confère aucun avantage en ce qui concerne le retour au bloc opératoire pour hémorragie ou tamponnade.
Jeffrey Le, MSc Karen J. Buth, MSc Gregory M. Hirsch, MD Jean-Francois Légaré, MD
Accepted for publication Aug. 25, 2014
Correspondence to: J.-F. Légaré Division of Cardiovascular Surgery The Maritime Heart Centre 2269-1796 Summer St. Halifax NS B3H 3A7 [email protected]
DOI: 10.1503/cjs.006814
does-legare.indd 100 2015-03-10 2:11 PM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 101
A s a part of standard of care in cardiac surgery, mediastinal and pleural chest tubes are placed to provide drainage of serosanguineous fluids from
the mediastinum.1 This practice has become a standard perioperative procedure to monitor bleeding and possibly prevent complications, such as pericardial effusion, hemo-thorax and tamponade.2,3
Despite their necessity, chest tubes are potentially a source of pain and irritation for patients. Some have sug-gested that the insertion of more than 1 chest tube per patient may exacerbate pain and discomfort, causing a decrease in ambulation that could negatively influence patient outcome.4–6 Currently, no evidence-based guide-line exists that dictates whether a single (SCT) or multi-ple chest tubes (MCT) should be used. The number of chest tubes inserted is largely left at the discretion of the individual surgeon based on low-level evidence or tradi-tional practice.
Though the literature suggests that SCT may provide adequate drainage, to our knowledge no studies have com-pared SCT with MCT in terms of patient outcomes. The objective of our study was to evaluate whether the number of chest tubes used could impact return to the operating room for bleeding or tamponade.
Methods
We retrospectively collected data on all patients who underwent coronary artery bypass grafting (CABG), valve or combined CABG plus valve surgery via a median ster-notomy at the Queen Elizabeth II Health Sciences Centre (QEII HSC) in Halifax, NS, between Jan. 1, 2005, and Dec. 31, 2010. Patients were excluded from final analysis if surgery was not performed via median sternotomy or if they also underwent insertion of a ventricular assistance device, extracorporeal membrane oxygenation, pericar-dectomy, transmyocardial laser revascularization or a complex congenital procedure. Patients were grouped according to whether they received SCT or MCT at the time of their original operation.
Operative technique
During the study period 10 different cardiac surgeons practised in Halifax. The choice of SCT or MCT was entirely left to surgeon preference rather than fixed cri-teria. All interventions were performed via a midline sternotomy, and cardiopulmonary bypass was performed in a standardized manner. Briefly, body temperature during the procedure was allowed to drift to 32°C. Intermittent cold cardioplegia solution (a blood: crystalloid ratio of 1:4 at a temperature of 8–10°C) was delivered antegrade via the aortic root unless otherwise indicated. Patients in the SCT group had their drainage tube placed on the surface of the diaphragm into the
pericardial well. Patients in the MCT had a combina-tion of mediastinal and/or pleural positioning for the drainage tube. In most patients, the chest tube used was a modified 32-FR urethral catheter (Bard) in which additional holes were made to improve drainage from the mediastinum.
In all cases in which an internal mammary artery was used, the pleura was opened unless lung adhesions were present. The pericardium was left open to allow communi-cation with the pleural space when opened to allow for serosanguinous drainage from the mediastinum to pleural space. It was standard practice that all drainage tubes were removed within 24 hours of surgery unless a persistent air leak was present or the patient experienced severe bleeding (> 50 mL/hr).
Data sources
Data were obtained from the Maritime Heart Centre Cardiac Surgery Registry, which is a clinical database that contains pre-, intra- and postoperative information on all patients undergoing cardiac surgery at the QEII HSC. This study was conducted with the full approval of the Capital District Health Authority Research Eth-ics Board. The requirement to obtain informed consent was waived under Section 2.1c of the Tri-Council Pol-icy Statement. All personal identifiers were stripped before data analysis to ensure patient anonymity and confidentiality.
Variable selection
Preoperative variables of interest included age, sex, left ventricular ejection fraction (EF), diabetes, hypertension, serum creatinine, congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD). Procedure-related variables were isolated CABG, isolated valve, CABG plus valve, and CABG and/or valve plus other pro-cedure. Urgency of surgery was categorized as emergent (immediate), urgent (within 24 hours), in-hospital (hos-pitalization required before surgery) or elective (waiting at home).
Statistical analysis
Categorical variables were reported as frequencies and percentages and were analyzed using a χ2 or Fisher exact test, as appropriate. Design variables were created for reference-level coding of categorical variables with more than 2 levels. A nonparsimonious multivariate logistic regression model was generated to examine the association of SCT and MCT with return to the operating room for bleeding or tamponade, adjusting for clinical differences between groups. Model discrimination was assessed by the area under the receiver operating characteristic (ROC)
does-legare.indd 101 2015-03-10 2:11 PM

RECHERCHE
102 J can chir, Vol. 58, No 2, avril 2015
curve. We performed a bootstrap procedure to obtain 1000 subsamples with replacement, and the 95% confidence interval (CI) of the ROC was obtained from the 2.5 and 97.5 percentiles of the bootstrap distribution. Model calibration was assessed using the Hosmer–Lemeshow goodness of fit statistic and applying linear regression analysis to the calibration plot of deciles of observed versus predicted mortality. We considered results to be significant at p < 0.05. All statistical analyses were performed using the SAS software package version 9.3.
Results Study population
A total of 5698 consecutive patients were included in our study. All patients were assigned to 2 groups based on the number of chest tubes placed at completion of the surgery: 3045 patients in the SCT and 2653 patents in the MCT group. Figure 1 illustrates the frequency of the use of MCT among 10 cardiac surgeons within our institution. The figure demonstrates how 5 surgeons predominantly used MCT in every patient, whereas 4 surgeons used MCT in 5% or fewer patients and, as such, used predominantly SCT.
Unadjusted univariate comparison between groups
The characteristics of the study patients are shown in Table 1. Patients in the SCT group were older, more often female, less likely to undergo isolated CABG and more likely to undergo a valve procedure than patients in the MCT group. The unadjusted outcomes between the groups are shown in Table 2. The overall unadjusted in-hospital mortality was 4.2% (3.8% in the SCT group v. 4.6% in the MCT group, p = 0.16). Similarly, 26.6% of patients required a stay in the intensive care unit (ICU) longer than 48 hours (25.5% in the SCT group v. 27.9% in the MCT group, p = 0.041) and 32.2% had a postoperative stay longer than 9 days (31.5% in the SCT group v. 33.1% in the MCT group, p = 0.20). Patients in the SCT group had a lower occurrence of internal mammary artery use than those in the MCT group (49.2% v. 50.7%, p < 0.001; Table 2).
A total of 276 (4.8%) patients returned to the operating room for bleeding or tamponade, and there was no signifi-cant difference between groups (4.7% in the SCT group v. 5.0% in the MCT group, p = 0.50). Blood products were required in 35.6% of patients (33.2% in the SCT group v. 38.3% in the MCT group, p < 0.001). Similarly, signifi-cantly more red blood cells, fresh frozen plasma, platelets
Fig. 1. Surgeon use of chest tubes. Each letter represents a single surgeon. The results are expressed as a percentage of the total number of cases performed by each surgeon.
19%
5%
93%
62%
5% 4%
86%
5%
98%
83%
0
10
20
30
40
50
60
70
80
90
100
A B C D E F G H I J
Per
cent
age
of c
ases
rece
ivin
g m
ultip
le c
hest
tube
s
Surgeon
does-legare.indd 102 2015-03-10 2:11 PM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 103
and cryoprecipitate were used in patients in the MCT group than those in the SCT group (Table 3).
Nonparsimonious multivariate model to predict return to the operating room for bleeding or tamponade
We created a nonparsimonious multivariate logistic regression model to adjust for the differences between the SCT and MCT groups. Variables that emerged as independent predictors of return to the operating room for bleeding or tamponade were urgent/emergent surgery (odds ratio [OR] 2.1, 95% confidence interval [CI] 1.4–3.2), in-house surgery (OR 1.5, 95% CI1.1–2.0), renal dysfunction with creatinine greater than 176 μmol/L (OR 1.6, 95% CI 1.0–2.5), age 80 years or older (OR 2.4, 95%
CI 1.6–3.6), CABG plus valve surgery (OR 2.2, 95% CI 1.5–3.1) and CABG and/or valve plus other procedure (OR 2.4, 95% CI 1.7–3.6; Fig. 2). What is novel about our predictive model is that we also included individual surgeons as variables. Some surgeons emerged as in depend ent predictors of the primary outcome or return to the OR, whereas others were protective and were less likely to return to the OR. Particularly relevant to the present study is the fact that the number of chest tubes used was not predictive of returning to the OR after adjusting for clinical differences between groups (OR 1.0, 95% CI 0.7–1.4). The ROC of the logistic regression model was 70% with a 95% CI of 68%–74%.
In the present study we did not look systematically at the prevalence of radiographic pleural effusions. We did, however, look at the prevalence of thoracentesis
Table 1. Demographic and clinical characteristics of patients who received single or multiple chest tubes during the study period
Group, no. (%)
Characteristic SCT, n = 3045 MCT, n = 2653 p value
Age, yr 0.004
≥ 80 366 (12.0) 256 (9.6)
70–79 933 (30.6) 801 (30.2)
60–69 887 (29.1) 865 (32.6)
< 60 859 (28.2) 731 (27.6)
Female sex 876 (28.8) 633 (23.9) < 0.001
Chronic renal failure 0.57
Creatinine > 176 μol/L 182 (6.0) 158 (6.0)
Creatinine 110–176 μol/L 712 (23.4) 652 (24.6)
Creatinine < 110 μol/L 2151 (70.6) 1843 (69.5)
Diabetes 1029 (33.8) 952 (35.9) 0.10
Ejection fraction ≤ 50% 872 (28.8) 746 (28.3) 0.68
COPD 478 (15.7) 431 (16.2) 0.57
Urgency of the procedure 0.44
Elective 1420 (46.6) 1246 (47.0)
In-hospital 1295 (42.5) 1095 (41.3)
Urgent/emergent 330 (10.8) 312 (11.8)
Type of procedure < 0.001
Isolated CABG 1669 (54.8) 1862 (70.2)
Isolated valve 685 (22.5) 334 (12.6)
CABG and valve 344 (11.3) 252 (9.5)
CABG and/or valve plus other procedure 347 (11.4) 205 (7.7)
CABG = coronary artery bypass graft; COPD = chronic obstructive pulmonary disease; MCT = multiple chest tubes; SCT = single chest tube.
Table 2. Unadjusted major morbidity and mortality outcomes between patients who received single or multiple chest tubes during the study period
Group, no. (%)
Outcome SCT, n = 3045 MCT, n = 2653 p value
Return to OR for bleeding or tamponade 142 (4.7) 134 (5.0) 0.50
In-hospital mortality 116 (3.8) 121 (4.6) 0.16
ICU stay > 48 hours 775 (25.5) 739 (27.9) 0.041
Postoperative stay > 9 d 959 (31.5) 878 (33.1) 0.20
IMA use 1788 (49.2) 1844 (50.7) < 0.001
ICU = intensive care unit; IMA = internal mammary artery; MCT = multiple chest tubes; OR = operating room; SCT = single chest tube.
does-legare.indd 103 2015-03-10 2:11 PM

RECHERCHE
104 J can chir, Vol. 58, No 2, avril 2015
while in hospital. The unadjusted rates of thoracentesis suggest that the overall prevalence was low and did not differ between the SCT and MCT groups (1.4% v. 1.3%, p = 0.67).
Discussion
There is a paucity of literature to support the use of either SCT or MCT in cardiac surgery. Most of the recent
Fig. 2. Adjusted odds ratios on a logarithmic scale showing our findings from the multivariate analysis designed to evalu-ate predictors of return to the operating room for bleeding or tamponade. CABG = coronary artery bypass graft; CHF = con-gestive heart failure; COPD = chronic obstructive pulmonary disease; EF = ejection fraction; HTN = hypertension; MCT = multiple chest tubes; SCT = single chest tube.
0.1 1 10
SCT
MCT
Isolated CABG
Isolated Valve
CABG + Valve
CABG and/or Valve plus Other
Age <60
Age 60-69
Age 70-79
Age >= 80
EF >50
EF <=50
CHF
HTN
Creatinine <110
Creatinine 110-176
Creatinine >176
COPD
Elective
Inhouse
Urgent/Emergent
Surgeon A
Surgeon B
Surgeon C
Surgeon D
Surgeon E
Surgeon F
Surgeon G
Surgeon H
Surgeon I
Surgeon J
Table 3. Blood products used in patients who received single or multiple chest tubes during the study period
Group, no. (%)
Variable SCT, n = 3045 MCT, n = 2653 p value
RBC 947 (31.1) 937 (35.4) < 0.001
FFP 294 (9.7) 434 (16.4) < 0.001
Platelets 228 (7.5) 409 (15.4) < 0.001
Cryoprecipitate 71 (2.3) 223 (8.4) < 0.001
FFP = fresh frozen plasma; MCT = multiple chest tubes; RBC = red blood cells; SCT = single chest tube.
does-legare.indd 104 2015-03-10 2:11 PM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 105
literature has focused on the type of drainage tubes used.1,7 The choice of the number of chest tubes used has tradi-tionally been based on surgeon preference, which in turn has largely been derived from their experience, training or institutional policies. This was clearly illustrated in our data: some surgeons used predominantly SCT, whereas others used MCT regardless of the surgical procedure per-formed. One needs to acknowledge that the choice to use 32-FR urethral catheters as chest tubes is unusual and was based on a long-established history of their use in our institution. We claim without clear proof that these tubes are soft and malleable, allowing for additional drainage holes to be added easily (by simply cutting extra holes) and are convenient for stripping when the patient is in the ICU to ensure that patency is maintained. Our findings and practice have not been compared with newer chest tube technologies, such as Blake drains, or tubes with differing methods of mechanical active tube clearance technologies that are currently available as alternative means of drain-age. The literature is inconclusive with respect to the su peri ority of these new technologies. To date, a limited number of publications are available, suggesting that it has been traditionally difficult to prove 1 method of drainage is superior to another.11,12
The primary outcome of our study was to determine if the number of chest tubes used could impact return to the operat-ing room for bleeding or tamponade. Using a logistic regres-sion analysis to adjust for the clinical differences between patients in the SCT and MCT groups, we were unable to demonstrate whether the number of chest tubes used pre-dicted return to the operating room or was protective.
We did, however, identify several important predictors of return to the operating room for bleeding or tampon-ade. These independent predictors, such as urgent proced-ures, complex procedures and renal dysfunction,8 are not surprising given their association with bleeding risk. For reasons that are unclear, age 80 years or older was shown to be an independent predictor of return to the operating room. The implications for this observation are important as an increasing number of octogenarians undergo cardiac surgery, suggesting that special considerations, such as the use of antiplatelet agents and perioperative anticoagulants, should be considered to reduce this risk in these patients.9
We were able to demonstrate how the operating surgeon was predictive of return to the operating room, either by increasing or decreasing the likelihood independent of patient or procedure variables. This observation likely illus-trates variations in clinical practices in which a variable threshold exists for returning to the operating room.
Limitations
We acknowledge this study was not designed to capture all the benefits or harms of using SCT or MCT. We chose our primary outcome based on the primary function
of chest tubes being drainage of serosanguinous fluids from the mediastinum, which as such is a surrogate pre-dictor of fluid accumulation (return to the operating room for bleeding or tamponade). The present study was retro-spective and therefore not designed to capture detailed information on total chest tube drainage or radiographic evidence of pleural effusion, which is not available in our registry. Furthermore, our study cannot fully address dif-ferences among surgeons, including the possibility that some surgeons using more than 1 chest tube (MCT group) may have limited their incidence of return to the operating room if they had only used 1 chest tube.
Despite these limitations, and in support of our find-ings, we report an unadjusted prevalence of thoracentesis that was low and that did not differ between groups, sug-gesting that the use of chest tubes may have minimal clin-ical impact on the prevalence of pleural effusion. We can also say that the unadjusted prevalence of blood product use as a surrogate for bleeding was not higher in the SCT than the MCT group, which could have masked inappro-priate drainage. However, one should note that detailed information on the exact time all antiplatelet agents or anticoagulants were stopped before surgery was not avail-able for analysis, but could explain why urgency independ-ently increased the likelihood of return to the operating room for bleeding. The standard practice in our institution is to maintain the use of acetylsalicylic acid but to hold clopidogrel for a min imum of 48 hours unless patients require urgent surgery.
ConClusion
Our study indicates that within our institution the use of MCT offered no overall benefit compared with SCT after cardiac surgery in terms of limiting the risk of returning to the operating room for bleeding or tamponade. Further-more, others have shown that MCT can result in severe postoperative pain and discomfort.4–10 Thus, we advocate the use of SCT in patients undergoing open heart surgery. However, these results should be interpreted with caution given the limitations outlined in our discussion.Affiliations: All authors are from the Department of Surgery, Division of Cardiac Surgery, QEII Health Science Centre, Dalhousie University, Halifax, Nova Scotia, Canada.
Competing interests: None declared.
Contributors: J. Le and J.-F. Légaré designed the study. K. Buth acquired the data, which all authors analyzed. J. Le wrote the article, which all authors reviewed and approved for publication.
References
1. Ege T, Tatli E, Canbaz S, et al. The importance of intrapericardial drain selection in cardiac surgery. Chest 2004;126:1559-62.
2. Lancey RA, Gaca C, Vander Salm TJ. The use of smaller, more flexible chest drains following open heart surgery: an initial evaluation. Chest 2001;119:19-24.
3. Shalli S, Saeed D, Fukamachi K, et al. Chest tube selection in cardiac
does-legare.indd 105 2015-03-10 2:11 PM

RECHERCHE
106 J can chir, Vol. 58, No 2, avril 2015
and thoracic surgery: a survey of chest tube-related complications and their management. J Card Surg 2009;24:503-9.
4. Akrofi M, Miller S, Colfar S, et al. A randomized comparison of three methods of analgesia for chest drain removal in postcardiac sur-gical patients. Anesth Analg 2005;100:205-9.
5. Mueller XM, Tinguely F, Tevaearai HT, et al. Impact of duration of chest tube drainage on pain after cardiac surgery. Eur J Cardiothorac Surg 2000;18:570-4.
6. Eryilmaz S, Emiroglu O, Eyileten Z, et al. Effect of posterior peri-cardial drainage on the incidence of pericardial effusion after ascend-ing aortic surgery. J Thorac Cardiovasc Surg 2006;132:27-31.
7. Moss E, Miller CS, Jensen H, et al. A randomized trial of early versus delayed mediastinal drain removal after cardiac surgery using silastic and conventional tubes. Interact Cardiovasc Thorac Surg 2013;17:110-5.
8. Arora RC, Legare JF, Buth KJ, et al. Identifying patients at risk of
intraoperative and postoperative transfusion in isolated CABG: toward selective conservation strategies. Ann Thorac Surg 2004; 78:1547-54.
9. Herman CR, Buth KJ, Kent BA, et al. Clopidogrel increases blood transfusion and hemorrhagic complications in patients undergoing cardiac surgery. Ann Thorac Surg 2010;89:397-402.
10. Légaré JF, Hirsch GM, Buth KJ, et al. Preoperative prediction of prolonged mechanical ventilation following coronary artery bypass grafting. Eur J Cardiothorac Surg 2001;20:930-6.
11. Sakopoulos AG, Hurwitz AS, Suda RW, et al. Efficacy of Blake® drains for mediastinal and pleural drainage following cardiac opera-tions. J Card Surg 2005;20:574-7.
12. Wallen M, Morrison A, Gillies D, et al. Mediastinal chest drain clearance for cardiac surgery. Cochrane Database Syst Rev 2004; CD003042.
Mark your calendar and plan to attend the 2015 Canadian Surgery Forum! September 17-20, 2015
Québec City Convention Centre & Hilton Québec Hotel The Forum is intended for community and academic surgeons, residents in training, researchers,
surgical and operating room nurses, Fellows and medical students. The 2015 Forum will offer outstanding opportunities for continuing professional development,
dialogue on educational and research issues, and networking.
ABSTRACTS & VIDEOS WILL BE ACCEPTED UNTIL APRIL 1, 2015!
For more information, please visit www.canadiansurgeryforum.com.
does-legare.indd 106 2015-03-10 2:11 PM

RESEARCH • RECHERCHE
©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 107
Outcomes of infection following pediatric spinal fusion
Background: Removal of instrumentation is often recommended as part of treatment for spinal infections, but studies have reported eradication of infection even with instrumentation retention by using serial débridements and adjuvant antibiotic phar-macotherapy. We sought to determine the effect of instrumentation retention or removal on outcomes in children with spinal infections.
Methods: We retrospectively reviewed the cases of patients who experienced early (< 3 mo) or late (≥ 3 mo) infected spinal fusions. Patients were evaluated at least 2 years after eradication of the infection using the following protocol outcomes: follow-up Cobb angle, curve progression and nonunion rates.
Results: Our sample included 35 patients. The mean age at surgery was 15.1 ± 6.0 years, 65.7% were girls, and mean follow-up was 41.7 ± 26.9 months. The mean Cobb angle was 63.6° ± 14.5° preoperatively, 29.4° ± 16.5° immediately after surgery and 37.2° ± 19.6° at follow-up. Patients in the implant removal group (n = 21) were more likely than those in the implant retention group (n = 14) to have a lower ASA score (71.4% v. 28.6%, p = 0.03), fewer comorbidities (66.7% v. 21.4%, p = 0.03), late infections (81.0% v. 14.3%, p = 0.01) and deep infections (95.2% v. 64.3%, p = 0.03). Implants were retained in 12 of 16 (75.0%) patients with early infections and 2 of 19 (10.5%) with late infections. Patients with implant removal had a higher pseudarthrosis rate (38.1% v. 0%, p = 0.02) and a faster curve progression rate (5.8 ± 9.8° per year v. 0.2 ± 4.7° per year, p = 0.04).
Conclusion: Implant retention should be considered, irrespective of the timing or depth of the infection.
Contexte : Le retrait des implants est souvent recommandé lors du traitement des infections rachidiennes, mais des études ont démontré qu’il est possible d’éliminer les infections tout en maintenant les implants en place, en ayant recours à des débride-ments répétés et à une antibiothérapie adjuvante. Nous avons voulu mesurer l’effet de la préservation ou du retrait des implants sur les résultats chez les enfants souffrant d’infections rachidiennes.
Méthodes : Nous avons passé en revue de manière rétrospective des cas de fusions rachidiennes infectées à un stade précoce (< 3 mois) ou tardif (≥ 3 mois). Les patients ont été évalués au moins 2 ans après l’éradication de l’infection à l’aide des paramètres suivants : angle de Cobb, progression de la courbure et taux de non fusion au moment du suivi.
Résultats : Notre échantillon comprenait 35 patients. L’âge moyen au moment de la chirurgie était de 15,1 ± 6,0 ans; 65,7 % étaient des filles et le suivi moyen s’est éche-lonné sur 41,7 ± 26,9 mois. L’angle de Cobb moyen était de 63,6 ° ± 14,5 ° en période préopératoire, de 29,4 ° ± 16,5 ° immédiatement après la chirurgie et de 37,2 ° ± 19,6 ° au moment du suivi. Les patients du groupe soumis au retrait de l’implant (n = 21) étaient plus susceptibles que les patients du groupe chez qui l’implant est demeuré en place (n = 14) de présenter un score ASA plus bas (71,4 % c. 28,6 %, p = 0,03) et un nombre moindre de comorbidités (66,7 % c. 21,4 %, p = 0,03), d’infections tardives (81,0 % c. 14,3 %, p = 0,01) et d’infections profondes (95,2 % c. 64,3 %, p = 0,03). Les implants sont demeurés en place chez 12 patients sur 16 (75,0 %) atteints d’infections précoces et chez 2 patients sur 19 (10,5 %) atteints d’infections tardives. Les patients chez qui l’implant a été retiré ont présenté un taux plus élevé de pseudar-throse (38,1 % c. 0 %, p = 0,02) et un taux de progression plus rapide de la courbure (5,8 ± 9,8 ° par année c. 0,2 ± 4,7 ° par année, p = 0,04).
Conclusion : Il y a lieu d’envisager le maintien des implants, indépendamment du moment d’apparition de l’infection et de sa profondeur.
Amir Khoshbin, MD Magdalena Lysenko, BSc, MA Peggy Law, BSc, MSc James. G. Wright, MD, MPH
Presented as a poster at the European Pediatric Orthopaedic Society Annual Meeting, Apr. 17–20, 2013, and at the Canadian Orthopaedic Association Annual Meeting, June 20–22, 2013
Accepted for publication Sept. 17, 2014
Correspondence to: J.G. Wright The Hospital for Sick Children (SickKids) Division of Orthopedic Surgery 555 University Ave. Toronto ON M5G 1X8 [email protected]
DOI: 10.1503/cjs.006014
outcome-wright.indd 107 2015-03-10 11:08 AM

RECHERCHE
108 J can chir, Vol. 58, No 2, avril 2015
S urgical site infections (SSIs) are the second most common adverse event in hospitalized patients.1 The incidence of postoperative infections is approx-
imately 1%–5% in spinal fusions for idiopathic scoliosis and approximately 4%–14% for neuromuscular scoliosis.2 Neuromuscular scoliosis, the use of allograft bone, the need for postoperative blood transfusions, urinary tract infections (UTIs), increased duration of surgery or of hos-pital admission and fusions extending distally to the sacrum have all been associated with an increased likelihood of SSIs in pediatric spinal fusions.3–6 Postoperative infections can lead to the need for revision surgery, ongoing pain, prolonged hospitalization, osteomyelitis and death.2
Removal of instrumentation is often recommended as part of treatment for spinal infections.1,7 However, other studies have reported eradication of infection even with instrumentation retention by using serial débridements and adjuvant antibiotic pharmacotherapy.8,9 The goal of this study was to determine the effect of instrumentation reten-tion or removal on patient outcomes (e.g., Cobb angle at follow-up, curve progression rate, nonunion) in spinal infections in patients 2 years after infection eradication.
Methods
We retrospectively reviewed the cases of all patients younger than 18 years treated with instrumented spinal arthrodesis for scoliosis (of various etiologies) at The Hos-pital for Sick Children in Toronto, Ont., between Jan. 1, 2000, and Dec. 31, 2009. Ethics approval was obtained from our institution. All specimens were cultured for 7 days. We used a modified Center for Disease Control–National Health Safety Network (CDC-NHSN) definition of SSIs, which was presence of at least 1 of the following: purulent discharge, positive cultures, evidence of infection on physical examination (tenderness, swelling, redness or heat), wound dehiscence, abscess discovery upon reopera-tion or evidence of infection on histopathological or radio-logic examination.10,11 Infections were categorized as early (< 3 mo) or late (≥ 3 mo), as described by Hedequist and colleagues.1 Infections were also categorized as being super-ficial or deep, as described by the CDC-NHSN and by Horan and colleagues.11 Deep infections were located in deep soft tissues (e.g., fascial and muscle layers) of the inci-sion and involved the following structures: intervertebral disc, vertebra and paravertebral muscles.11,12 Superficial infections were located in the skin and subcutaneous tissue and above the fascial layer.11 Infection eradication was defined as no signs of infection on physical examination and no reported pain with normal blood parameters, as described by Ahmed and colleagues.13
All patients were categorized in either the implant removal group or the implant retention group based on their postinfection treatment management. Data on preop-erative, perioperative, postoperative and follow-up clinical
information as well as diagnostic imaging pertinent to the index surgery, infection, treatment course and outcome were collected for each patient.
Preoperative variables included age, sex, weight, time to follow-up from index surgery, scoliosis etiology, neuro-logic motor level, Cobb angle, Scoliosis Research Society (SRS) curve type, hematocrit, past medical and surgical history. Perioperative variables included American Society of Anesthesiologists (ASA) score, surgical approach, peri-operative antibiotic use, duration of surgery, drain usage, type of instrumentation, bone graft usage, blood loss, peri-operative transfusion, volume of packed red blood cells (pRBCs) transfused, distal extent of instrumentation and the number of motion segments instrumented. The post-operative factors included immediate Cobb angle, postop-erative transfusion, volume of pRBCs transfused and UTI within 2 weeks of the index surgery.
With respect to the infection, variables included timing, location, duration of the antibiotic therapy, culture results and removal versus retention of instrumentation. The number of irrigation and débridements performed as part of the treatment plan, either before infection eradication (implant retention group) or before implant removal, was also recorded.
Patient outcomes included Cobb angle at follow-up, change in Cobb angle (defined as the percent change of the primary Cobb angle at follow-up with respect to the immediate postoperative state), curve progression rate (defined as the change of the primary Cobb angle per year since the immediate postoperative state), and pseudarthro-sis (defined as motion radiographically and/or motion dur-ing surgical exploration).14,15
Statistical analysis
Statistical analyses were performed using SAS software version 9.1, with the α value predefined at 0.05. Data were evaluated using analysis of covariance for continuous data (assuming unequal variance between groups) and the χ2 test for categorical data (or Fisher exact test for cells con-taining fewer than 5 patients). Patients were analyzed based on implant removal or implant retention as part of their treatment course.
Results
Between 2000 and 2009, 827 pediatric patients under-went instrumented spinal fusions for scoliosis. Among them, we identified 35 patients (idiopathic: n = 17, 48.9%; neuromuscular: n = 11, 31.4%; congenital/other: n = 7, 20%) who experienced an early (n = 16, 45.7%) or late infection (n = 19, 54.3%), resulting in a total infec-tion rate of 4.2%. Of these 35 patients, the implants were removed in 21 and retained in 14 patients. The mean age of patients at the time of surgery was 15.1 ±
outcome-wright.indd 108 2015-03-10 11:08 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 109
6.0 years; 65.7% were girls and 34.3% were boys. The types of metal used in patients who experienced infec-tions were stainless steel (n = 15, 42.9%), titanium (n = 2, 5.7%) and unknown (n = 18, 51.4%); the latter group of patients did not have any information written in their charts. Mean follow-up from the time of surgery was 41.7 ± 26.9 (median 38.0, range 12–123) months. Preop-erative Cobb angles were 63.6 ± 14.5° and immediate postoperative Cobb angles were 29.4 ± 16.5°, resulting in a 55.2 ± 19.6% curve correction. Follow-up Cobb angles were 37.2 ± 19.6°. Eradication of infection was successful in all 35 patients at the time of follow-up (Table 1).
With respect to baseline preoperative variables, patients who had, compared with those who did not have, implant removal were more likely to have no neurologic deficit (85.7% v. 42.9%, p = 0.019) and were generally healthier, with fewer medical comorbidities (66.7% v. 21.4%, p = 0.031; Table 1).
For peri- and postoperative variables, late infections were more prevalent in the implant removal than the
implant retention group (81.0% v. 14.3%, p = 0.001), with the majority of these infections being deep (95.2% v. 64.3%, p = 0.017). In the implant retention group, 7 (50.0%) patients had 1 irrigation and débridement, 2 (14.3%) patients had 4, and 5 (35.7%) patients did not have any (they had superficial infections only) before infection eradication (Tables 2 and 3). In the implant removal group, 1 (4.8%) patient had 2 irrigation and débridements, 3 (14.3%) patients had 3, 1 (4.8%) patient had 5, 1 (4.8%) patient had 8, and 15 (71.4%) patients had concurrent irrigation and débridements with their defini-tive implant removal. The mean number of irrigation and débridements was 1.14 ± 2.15 in the implant removal group and 1.07 ± 1.33 in the implant retention group (p = 0.90; Table 3).
In terms of outcomes, patients in the implant removal group had a significantly higher rate of associated pseudarthrosis at follow-up than those in the implant retention group (38.1% v. 0% pseudarthrosis, p = 0.012). Of the 8 patients with pseudarthrosis, 7 had late
Table 1. Preoperative variable of patients with infected spinal fusions in the implant retention and removal groups
Group, no. (%)*
VariableAll patientsn = 35
Implant retentionn = 14
Implant removal n = 21 p value
Sex
Male 12 (34.3) 7 (50) 5 (23.8) 0.11
Female 23 (65.7) 7 (50) 16 (76.2)
Age, yr 15.1 ± 6.0 16.8 ± 8.4 14.0 ± 3.6 0.20
Follow-up, mean ± SD mo 41.7 ± 26.9 39.0 ± 26.9 43.5 ± 27.4 0.63
Weight, mean ± SD kg 50.7 ± 22.7 51.0 ± 28.3 50.5 ± 18.8 0.96
Diagnosis 0.11
Idiopathic 17 (48.9) 4 (28.6) 13 (61.9)
Neuromuscular 11 (31.4) 7 (50.0) 4 (19.1)
Congenital/other 7 (20.0) 3 (21.4) 4 (19.1)
Neurologic motor level 0.019
Thoracic 9 (25.7) 6 (42.9) 3 (14.3)
Lumbar/sacral 2 (5.7) 2 (14.3) 0 (0)
Nil 24 (68.6) 6 (42.9) 18 (85.7)
Primary Cobb angle, mean ± SD 63.6 ± 14.5 61.7 ± 17.3 64.8 ± 12.5 0.54
SRS curve 0.77
Thoracic 18 (52.9) 8 (57.1) 10 (50.0)
Thoracolumbar 12 (35.3) 4 (28.6) 8 (40.0)
Lumbar 4 (11.8) 2 (14.3) 2 (10.0)
Previous surgery 0.22
Nonspinal surgeries 11 (32.4) 6 (46.2) 5 (23.8)
Spinal surgeries 5 (14.7) 3 (23.1) 2 (9.5)
Nil 18 (52.9) 4 (30.8) 14 (66.7)
Medical history 0.031
Nil 17 (48.6) 3 (21.4) 14 (66.7)
Respiratory, cardiac, renal, GI 11 (31.4) 7 (50.0) 4 (19.1)
Multiple 7 (20.0) 4 (28.6) 3 (14.3)
Hematocrit, mean ± SD 0.34 ± 0.04 0.34 ± 0.04 0.35 ± 0.04 0.63
GI = gastrointestinal; SD = standard deviation; SRS = Scoliosis Research Society. *Unless otherwise indicated.
outcome-wright.indd 109 2015-03-10 11:08 AM

RECHERCHE
110 J can chir, Vol. 58, No 2, avril 2015
infections and 7 had deep infections. Implant removal also resulted in a faster curve progression rate. For the 14 patients in the implant retention group the progres-sion was 0.2° per year for a mean follow-up of 39.0 (range 12–87) months, whereas for patients in the implant removal group the progression was 5.8° per year for a mean follow-up of 43.5 (range 12–123) months (p = 0.036). Of the 16 patients who experienced early infections, 12 (75%) were in the implant retention group and had a change in Cobb angle of 18.8 ± 43.4% and 4 (25%) were in the implant removal group and had a change in Cobb angle of 24.8 ± 30.2% (p = 0.91). For the 19 patients who experienced late infections, 2 (10.5%) were in the implant retention group (1 superfi-cial and 1 deep infection) and had a change in Cobb angle of 29.8 ± 42.1% and 17 (89.5%) patients were in the implant removal group (89.5%) and had a change in Cobb angle of 80.0 ± 122.4% (p = 0.47; Table 3).
Discussion
Data from the SRS Morbidity and Mortality database pub-lished in 2011 indicated an overall infection rate of 0.8%
for superficial and 1.3% for deep infections for pediatric scoliosis surgery.16 The reported infection rate for neuro-muscular scoliosis was 5.5% (31.4% in our study popula-tion) and 1.4% for idiopathic scoliosis (48.9% in our study population).16 Thus, given the high percentage of neuro-muscular scoliosis among patients who received surgery during our study period, our overall infection rate of 4.2% is comparable to those reported in other series.8,17–19
Spinal infections may be eradicated using several strat-egies, but implant removal has often been advocated owing to the potential for biofilm creation on spinal implant.20 Routine implant removal has also been recom-mended if Propoinibacter is isolated.21 In our series, 50.0% of cultures grew gram-positive microbes, without any doc-umented cases of Propoinibacter. While the timing of infec-tions has also been suggested as a determinant for whether implant retention or removal is chosen, the definitions of early and late infections are inconsistent in the literature, with definitions of late or delayed infections ranging from 30 days to more than 1 year postinstrumentation.1,7,11,22,23
Kowalski and colleagues,22 who defined late infections as those occurring 30 days after instrumentation, reported a failure rate of 22.7% for patients who had early infections
Table 2. Perioperative variables of patients with infected spinal fusions in the implant retention and removal groups
Group, no. (%)*
VariableAll patientsn = 35
Implant retentionn = 14
Implant removaln = 21 p value
ASA score 0.033
I-II 19 (54.3) 4 (28.6) 15 (71.4)
> III 16 (45.7) 10 (71.4) 6 (28.6)
Approach 0.19
Anterior 1 (2.9) 1 (7.1) 0 (0)
Posterior 23 (65.7) 7 (50.0) 16 (76.2)
Combined 11 (31.4) 6 (42.9) 5 (23.8)
Perioperative antibiotic use 35 (100) 14 (100) 21 (100) > 0.99
Duration of surgery, mean ± SD, min 492.6 ± 152.7 504.5 ± 144.7 484.6 ± 160.9 0.71
Instrumentation 0.20
Pedicle screws/rods 20 (57.1) 6 (42.9) 14 (66.7)
Sublaminar wiring/ rods 14 (40.0) 8 (57.1) 6 (28.6)
Growing rods 1 (2.9) 0 (0) 1(4.8)
Bone graft 0.009
Autograft 20 (57.1) 5 (35.7) 15 (71.4)
Allograft 10 (28.6) 4 (28.6) 6 (28.6)
Both 5 (14.3) 5 (35.7) 0 (0)
Blood loss, mean ± SD, mL/kg 26.1 ± 23.5 30.6 ± 27.1 23.1 ± 20.9 0.37
Transfusion 24 (68.6) 10 (71.4) 14 (66.7) 0.77
Volume of transfusion, mean ± SD, mL/kg 9.8 ± 9.9 12.1 ± 12.2 8.4 ± 8.0 0.29
Distal fusion level 0.66
Thoracic 1 (2.9) 0 (0) 1 (4.8)
Lumbar 31 (88.6) 13 (92.9) 18 (85.7)
Sacrum/pelvis 3 (8.6) 1 (7.1) 2 (9.5)
Fusion length, mean ± SD, no. of segments 12.4 ± 3.5 12.9 ± 3.5 12.1 ± 3.5 0.50
Drain usage 15 (42.9) 8 (57.1) 7 (33.3) 0.16
ASA = American Society of Anesthesiologists; SD = standard deviation. *Unless otherwise indicated.
outcome-wright.indd 110 2015-03-10 11:08 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 111
and whose treatment consisted of débridement, implant retention and suppressive (parenteral followed by oral) antimicrobial therapy (n = 5). However, the failure rate was 21.9% for patients who had late infections treated with débridement and implant removal (n = 7) and 53.8% for those with late infections treated with débridement and implant retention (n = 7).22 Hedequist and colleagues,1 who defined late infections as those presenting more than 3 months after the index surgery, reported that no patient was cleared of infection without implant removal (n = 26). They recommended performing immediate implant removal for all patients with late infections and revision surgery at a later date, if needed, for progressive deformity or pseudarthrosis. Ho and colleagues,7 who defined late infections as those that occurred more than 6 months after the initial oper ation, reported a nearly 50% reoccurrence rate (20 of 43 pa tients) if the spinal implant was retained after the initial irrigation and débridement.7 While many additional irrigation and débridements were performed, 13 of 22 (59%) of patients with late infections ultimately did not have their implants removed. Hahn and col-leagues,23 who defined late infections as those appearing a min imum of 57 weeks after the index instrumentation,
reported 100% eradication of late infections with instru-mentation removal. In our study, 10.5% of implants were retained in patients who experienced late infections (≥ 3 mo); in patients who experienced late, deep infec-tions, 31.0% of implants were retained.
Implant removal is not without its drawbacks. Implant removal has been associated with a loss of coronal correc-tion of approximately 10° in the main thoracic curve in adolescent patients with idiopathic scoliosis.7 Ho and col-leagues7 reported on 10 patients treated with implant removal (mean follow-up 10 months); 6 of them experi-enced a more than 10° increase in deformity in at least 1 plane. Muschik and colleagues24 reported a progression of 6° for thoracic curves and 5° for lumbar curves at an average follow-up of 3.6 years after implant removal. Our patients had accelerated curve progression, both in abso-lute and proportional terms, when implants were removed. In our series, the change in Cobb angle at follow-up compared with the immediate postoperative state was higher in the implant removal group than the implant retention group, but the difference was not significant (69.5% ± 112.3% v. 20.3% ± 41.8%, p = 0.08). Furthermore, patients in the implant removal group had a
Table 3. Postoperative and outcome variables of patients with infected spinal fusions in the implant retention and removal groups
Group, no. (%)*
VariableAll patients n = 35
Implant retention n = 14
Implant removaln = 21 p value
Initial irrigation and débridements, mean ± SD 1.11 ± 1.84 1.07 ± 1.33 1.14 ± 2.15 0.90
Antibiotic use (48 h postoperative) 34 (97.1) 14 (100) 20 (95.2) 0.41
Immediate postoperative Cobb angle, mean ± SD 29.4 ± 16.5 29.5 ± 15.8 29.2 ± 17.3 0.96
Length of hospital stay, mean ± SD, d 16.0 ± 19.8 20.4 ± 27.8 13.3 ± 12.6 0.32
Transfusion 4 (11.4) 1 (7.1) 3 (14.3) 0.52
Volume of transfusion, mean ± SD, mL/kg 1.1 ± 3.6 0.4 ± 1.6 1.6 ± 4.4 0.36
UTI 7 (21.2) 3 (21.4) 4 (21.1) 0.98
Timing < 0.001
Early 16 (45.7) 12 (85.7) 4 (19.1)
Late 19 (54.3) 2 (14.3) 17 (80.9)
Location 0.017
Superficial 6 (17.1) 5 (35.7) 1 (4.8)
Deep 29 (82.9) 9 (64.3) 20 (95.2)
Pseudarthrosis 8 (22.9) 0 (0) 8 (38.1) 0.012
Adjuvant antibiotic therapy 33 (94.3) 13 (92.9) 20 (95.2) 0.77
Duration of antibiotic therapy, mean ± SD, d 117.9 ± 107.1 122.9 ± 111.6 114.6 ± 106.6 0.83
Culture 0.014
Gram-positive 17 (50.0) 6 (46.2) 11 (52.4)
Gram-negative 5 (14.7) 5 (38.5) 0 (0)
Atypicals 2 (5.9) 0 (0) 2 (9.5)
None isolated 5 (14.7) 0 (0) 5 (23.8)
Polymicrobial 5 (14.7) 2 (15.4) 3 (14.3)
Follow-up Cobb angle, mean ± SD 37.2 ± 19.6 33.0 ± 17.6 39.7 ± 20.6 0.36
Percent coronal loss, mean ± SD 49.8 ± 93.2 20.3 ± 41.8 69.5 ± 112.3 0.08
Curve progression rate, mean ± SD, °/yr 3.8 ± 8.7 0.2 ± 4.7 5.8 ± 9.8 0.036
SD = standard deviation; UTI = urinary tract infection. *Unless otherwise indicated.
outcome-wright.indd 111 2015-03-10 11:08 AM

RECHERCHE
112 J can chir, Vol. 58, No 2, avril 2015
faster curve progression rate (5.8° ± 9.8° per year v. 0.2° ± 4.7° per year, p = 0.036) at an average follow-up of 3.48 ± 2.24 years.
As noted by Viola and colleagues,17 it is difficult to determine whether spinal infections lead to pseudarthrosis or if pseudarthrosis is a predisposing risk factor for infec-tions. Previously, Katonis and colleagues12 reported that no association existed between pseudarthrosis and early infections in patients who had spinal fusions. However, an association between late infections and pseudarthrosis has previously been reported to range from 20% to 62%,17,20 which is consistent with our findings. Of the 17 patients with late infections in our study, 7 (41.1%) patients had pseudarthrosis at a mean follow-up of 50.6 (range 13–78) months. Only 1 case of pseudarthrosis occurred in a patient who experienced an early infection.
Limitations
Our study has several limitations. First, we defined suc-cessful outcomes only with respect to clinical and radio-graphic parameters. However, Mok and colleagues25 reported that after treatment (in an adult population) of infection in 16 patients with spinal rods (12 treated with implant retention and 4 treated with implant removal), patients with infections reported similar SF-36 scores to matched controls who underwent spinal fusion but did not experience infections. Second, owing to the low inci-dence of SSIs, our sample size was small, and thus our ability to examine treatment was minimal. However, infection was eradicated successfully in all patients, and the main difference in treatment was the decision to remove or retain the instrumentation.
ConClusion
While implant removal may be needed for the treatment of infected spinal fusions, removal of instrumentation often reveals a pseudoarthrosis and is associated with a high risk of scoliosis progression. When clinically possi-ble, a trial of implant retention should be considered, irrespective of the timing or depth of the infection, and probably no definition of late infections should be used as an absolute indication for immediate rod removal.
Acknowledgements: The authors thank Derek Stephens for his help and guidance with the statistical analysis of this data.
Affiliations: From the University of Toronto Faculty of Orthopaedic Surgery (Koshbin, Wright) and the Hospital for Sick Children (Koshbin, Lysenko, Law, Wright), Toronto, Ont.
Funding: This study was funded by the SickKids Foundation.
Competing interests: None declared.
Contributors: J. Wright designed the study. A. Khoshbin and M. Lysenko acquired the data, which all authors analyzed. A. Khoshbin wrote the article, which all authors reviewed and approved for publication.
References
1. Hedequist D, Haugen A, Hresko T, et al. Failure of attempted implant retention in spinal deformity delayed surgical site infections. Spine 2009;34:60-4.
2. Master DL, Poe-Kochert C, Son-Hing J, et al. Wound infections after surgery for neuromuscular scoliosis risk factors and treatment outcomes. Spine 2011;36:E179-85.
3. Mohamad F, Parent S, Pawelek J, et al. Perioperative complications after surgical correction in neuromuscular scoliosis. J Pediatr Orthop 2007;27:392-7.
4. Sponseller PD, LaPorte DM, Hungerford MW, et al. Deep wound infections after neuromuscular scoliosis surgery — a multicenter study of risk factors and treatment outcomes. Spine 2000;25:2461-6.
5. Mohammed Ali MH, Koutharawu DN, Miller F, et al. Operative and clinical markers of deep wound infection after spine fusion in children with cerebral palsy. J Pediatr Orthop 2010;30:851-7.
6. Labbé AC, Demers AM, Rodrigues R, et al. Surgical-site infection following spinal fusion: a case-control study in a children’s hospital. Infect Control Hosp Epidemiol 2003;24:591-5.
7. Ho C, Skaggs DL, Weiss JM, et al. Management of infection after instrumented posterior spine fusion in pediatric scoliosis. Spine 2007;32:2739-44.
8. Lonstein J, Winter R, Moe J, et al. Wound infection with harrington instrumentation and spine fusion for scoliosis. Clin Orthop Relat Res 1973;222-33.
9. Wenger DR, Mubarak SJ, Leach J. Managing complications of pos-terior spinal instrumentation and fusion. Clin Orthop Relat Res 1992;24-33.
10. Ballard MR, Miller NH, Nyquist AC, et al. A multidisciplinary approach improves infection rates in pediatric spine surgery. J Pediatr Orthop 2012;32:266-70.
11. Horan TC, Gaynes RP, Martone WJ, et al. CDC definitions of noso-comial surgical site infections, 1992 — a modification of CDC defini-tions of surgical wound infections. Infect Control Hosp Epidemiol 1992;13:606-8.
12. Katonis P, Tzermiadianos M, Papagelopoulos P, et al. Postoperative infections of the thoracic and lumbar spine — a review of 18 cases. Clin Orthop Relat Res 2007;114-9.
13. Ahmed R, Greenlee JDW, Traynelis VC. Preservation of spinal instrumentation after development of postoperative bacterial infec-tions in patients undergoing spinal arthrodesis. J Spinal Disord Tech 2012;25:299-02.
14. Dawson EG, Clader TJ, Bassett LW. A comparison of different methods used to diagnose pseudarthrosis following posterior spinal fusion for scoliosis. J Bone Joint Surg Am 1985;67:1153-9.
15. Kim YJ, Bridwell KH, Lenke LG, et al. Pseudarthrosis in long adult spinal deformity instrumentation and fusion to the sacrum: preva-lence and risk factor analysis of 144 cases. Spine 2006;31:2329-36.
16. Smith JS, Shaffrey CI, Sansur CA, et al. Rates of infection after spine surgery based on 108,419 procedures a report from the scoliosis research society morbidity and mortality committee. Spine 2011;36:556-63.
17. Viola RW, King HA, Adler SM, et al. Delayed infection after elect-ive spinal instrumentation and fusion — a retrospective analysis of eight cases. Spine 1997;22:2444-50.
18. Benson ER, Thomson JD, Smith BG, et al. Results and morbidity in a consecutive series of patients undergoing spinal fusion for neuro-muscular scoliosis. Spine 1998;23:2308-17.
outcome-wright.indd 112 2015-03-10 11:08 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 113
19. Drummond DS, Moreau M, Cruess RL. Results and complications of surgery for the paralytic hip and spine in myelomeningocele. J Bone Joint Surg Br 1980;62-B:49-53.
20. Richards BS. Delayed infections following posterior spinal instru-mentation for the treatment of idiopathic scoliosis. J Bone Joint Surg Am 1995;77:524-9.
21. Collins I, Wilson-MacDonald J, Chami G, et al. The diagnosis and management of infection following instrumented spinal fusion. Eur Spine J 2008;17:445-50.
22. Kowalski TJ, Berbari EF, Huddleston PM, et al. The management and outcome of spinal implant infections: contemporary retrospec-tive cohort study. Clin Infect Dis 2007;44:913-20.
23. Hahn F, Zbinden R, Min K. Late implant infections caused by propi-onibacterium acnes in scoliosis surgery. Eur Spine J 2005;14: 783-8.
24. Muschik M, Luck W, Schlenzka D. Implant removal for late- developing infection after instrumented posterior spinal fusion for scoliosis: Reinstrumentation reduces loss of correction. A retrospec-tive analysis of 45 cases. Eur Spine J 2004;13:645-51.
25. Mok JM, Guillaume TJ, Talu U, et al. Clinical outcome of deep wound infection after instrumented posterior spinal fusion a matched cohort analysis. Spine 2009;34:578-83.
CJS’s top viewed articles*
1. Research questions, hypotheses and objectives Farrugia et al. Can J Surg 2010;53(4):278-81 2. Complications associated with laparoscopic
sleeve gastrectomy for morbid obesity: a surgeon’s guide
Sarkhosh et al. Can J Surg 2013;56(5):347-52 3. Managing complications associated with
laparoscopic Roux-en-Y gastric bypass for morbid obesity
Sahle Griffith et al. Can J Surg 2012;55(5):329-36 4. Hardware removal after tibial fracture has healed Sidky and Buckley Can J Surg 2008;51(4):263-8 5. Tracheostomy: from insertion to decannulation Engels et al. Can J Surg 2009;52(5):427-33 6. Complications of Meckels diverticula in adults Dumper et al. Can J Surg 2006;49(5):353-7 7. Complications associated with adjustable
gastric banding for morbid obesity: a surgeon’s guide
Eid et al. Can J Surg 2011;54(1):61-1 8. Treatment of an infected total hip replacement with the PROSTALAC system Scharfenberger et al. Can J Surg 2007;50(1):24-8 9. Thoracic needle decompression for tension pneumothorax: clinical correlation with catheter length Ball et al. Can J Surg 2010;53(3):184-810. All superior pubic ramus fractures are not created equal Steinitz et al. Can J Surg 2004;47(6):422-5
*Based on page views on PubMed Central of research, reviews, commentaries and discussions in surgery. Updated Mar. 4, 2015.
outcome-wright.indd 113 2015-03-10 11:08 AM

RESEARCH • RECHERCHE
114 J can chir, Vol. 58, No 2, avril 2015 ©2015 8872147 Canada Inc.
Persistent neuropathic pain after inguinal herniorrhaphy depending on the procedure (open mesh v. laparoscopy): a propensity-matched analysis
Background: A greater incidence of persistent pain after inguinal herniorrhaphy is suspected with the open mesh procedure than with laparoscopy (transabdominal pre-peritoneal), but the involvement of neuropathy needs to be clarified.
Methods: We examined the cumulative incidence of neuropathic persistent pain, defined as self-report of pain at the surgical site with neuropathic aspects, within 6 months after surgery in 2 prospective subcohorts of a multicentre study. We com-pared open mesh with laparoscopy using different analysis, including a propensity-matched analysis with the propensity score built from a multivariable analysis using a generalized linear model.
Results: Considering the full patient sample (242 open mesh v. 126 laparoscopy), the raw odds ratio for neuropathic persistent pain after inguinal herniorrhaphy was 4.3. It reached 6.8 with the propensity-matched analysis conducted on pooled subgroups of 194 patients undergoing open mesh and 125 undergoing laparoscopy (95% confi-dence interval 1.5–30.4, p = 0.012). A risk factor analysis of these pooled subgroups revealed that history of peripheral neuropathy was an independent risk factor for per-sistent neuropathic pain, while older age was protective.
Conclusion: We found a greater risk of persistent pain with open mesh than with laparoscopy that may be explained by direct or indirect lesion of nerve terminations. Strategies to identify and preserve nerve terminations with the open mesh procedure are needed.
Contexte : On soupçonne que l’incidence de la douleur persistante à la suite d’une hernioplastie inguinale est plus élevée avec la mise en place d’un filet par voie ouverte qu’avec la laparoscopie (transabdominale prépéritonéale), mais encore faut-il clarifier le rôle de la neuropathie.
Méthodes : Nous avons mesuré l’incidence cumulative de la douleur neuropathique persistante, décrite comme une douleur au site opératoire accompagnée d’éléments neuropathiques déclarés par le patient dans les 6 mois suivant la chirurgie, auprès de 2 sous-cohortes prospectives d’une étude multicentrique. Nous avons comparé la mise en place d’un filet par voie ouverte et la laparoscopie à l’aide de différentes analyses, dont une analyse avec appariement des scores de propension, les scores de propension découlant d’une analyse multivariée générée à partir d’un modèle linéaire généralisé.
Résultats : En tenant compte de tout l’échantillon de patients (242 soumis à la mise en place d’un filet par voie ouverte c. 126 soumis à la laparoscopie), le rapport des cotes brut pour la douleur neuropathique persistante après l’hernioplastie inguinale était de 4,3. Il a atteint 6,8 à l’analyse par appariement des scores de propension réali-sée auprès de sous-groupes réunis de 194 patients soumis à la technique ouverte avec treillis et 125 soumis à la laparoscopie (intervalle de confiance à 95 % 1,5–30,4, p = 0,012). Une analyse des facteurs de risque pour ces sous-groupes réunis a révélé que des antécédents de neuropathie périphérique constituaient un facteur de risque indépendant à l’égard de la douleur neuropathique persistante, tandis que l’avancée en âge a conféré un effet protecteur.
Conclusion : Nous avons observé un risque plus élevé de douleur persistante associée à la mise en place d’un filet par voie ouverte qu’avec la laparoscopie, ce qui pourrait s’expliquer par des lésions directes ou indirectes aux terminaisons nerveuses. Des stra-tégies s’imposent pour identifier et préserver les terminaisons nerveuses lors de la mise en place d’un filet par voie ouverte.
Patrick Niccolaï, MB Lemlih Ouchchane, MD, PhD Maurice Libier, MB Fayçale Beouche, MB Monique Belon, MB Jean-Marc Vedrinne, MB Bilal El Drayi, MB Laurent Vallet, MB Franck Ruiz, MB Céline Biermann, MD Pascal Duchêne, MB Claudine Chirat, MB Sylvie Soule-Sonneville, MS Christian Dualé, MD, PhD Claude Dubray, MD, PhD
Pierre Schoeffler, MD
Accepted for publication Sept. 29, 2014
Correspondance to: C. Dualé CPC / CIC, bâtiment 3C CHU de Clermont-Ferrand Rue Montalembert, BP69, 63003 Clermont-Ferrand Cedex 1, France [email protected]
DOI: 10.1503/cjs.008314
persist-duale.indd 114 2015-03-10 8:00 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 115
A recent systematic review estimated the risk of post-surgical persistent pain (PSPP) to be 7%–12% after inguinal herniorrhaphy, depending on the method
of meta-analysis.1 This finding may have relevant conse-quences for public health, as inguinal herniorrhaphy is one of the most frequently practised surgeries in industrialized countries. Furthermore, a proportion of the re ported cases of PSPP after inguinal herniorraphy is suspected to be neuro pathic, as nerve dysfunction has been reported after inguinal herniorrhaphy.2 In addition, a literature-based esti-mation that took into account certain symptoms of persist-ent pain, such as numbness, paroxysmal pain or touch-evoked allodynia, stated that 30.5% of persistent pain was probably or definitely of neuropathic origin.1 It has also been suggested that there is less risk of persistent pain with laparoscopic than with open inguinal hernia repair.3 How-ever, it is unknown whether this difference between the 2 techniques is maintained for neuropathic aspects of per-sistent pain. This mechanism is widely considered to be a factor of severity and chronicization.4 In a recently pub-lished prospective open-ended French multicentric cohort study, the risk of persistent neuropathic pain in the 6 months following inguinal hernia repair was estimated at 12.4% for open mesh surgery and 3.2% for laparoscopic surgery.5 We further studied these 2 subcohorts to assess the risk of persistent neuropathic pain associated with lapa-roscopic and open inguinal hernia repair. Our observational nonrandomized design resulted in unequal distributions of relevant covariates between comparison groups, but the level of evidence was improved by using an analysis based on propensity score.
Methods
Our methodology is described in detail elsewhere.5 Briefly, this multicentric French study was approved by the appropriate institutional research ethics boards (CCPPRB d’Auvergne and CPP Sud-Est VI for amend-ments), and the trial was registered on ClinicalTrials.gov (NCT00812734). In each centre, the study was coordin-ated by a referent anaesthetist and conducted by the anes-thesiology team.
The study population consisted of prospective adult patients who, having given written informed consent, were scheduled in a recruitment centre for primary inguinal her-niorrhaphy. We examined 2 procedures: open mesh and laparoscopy (transabdominal preperitoneal). The study cen-tres were selected on the basis of their activity for these 2 procedures, aiming at a balance between them. The exclu-sion criteria for both procedures were planned laparotomy, reoperation, surgery for eventration, expected difficulty in the patient’s ability to understand or complete the question-naires and potential inability to reach the patient during the 6 months following surgery. The exclusion criterion specific to the open mesh procedure was a bilateral or intraperi-
toneal procedure. Laparoscopy had to be planned as such. Consecutive recruitment of patients was required.
The assessment of patients for inclusion in the study occurred 1–2 weeks before surgery. Patients completed a questionnaire about their working activities and history of previous pain, then the physician recorded information on potential symptoms of peripheral neuropathy and possible risk factors for peripheral neuropathy. The medical data sheet was completed on discharge from the surgical ward and included information on the strategies used for anes-thesia, peri- and postoperative analgesia and the occur-rence of early complications. At 3 and 6 months after sur-gery, patients received by mail a questionnaire in which they were asked to report whether they felt pain at the sur-gical site. If so, patients were asked to describe the inten-sity of this pain over the previous 48 hours using a visual analogue scale (VAS). Other questions concerned the time course of the pain since surgery and the clinical features; some questions were derived from the DN4 diagnostic questionnaire6 and included within our questionnaire. If questionnaires were not completed and returned, we con-tacted the patients by telephone.
Postsurgical persistent pain was defined as self-reported pain at the surgical site; the pain was considered neuro-pathic in cases of 4 or more positive responses to the DN4 questions. Throughout the follow-up period, patients were able to visit a referent practitioner for analgesic treatment if required, or they could request a referral to the closest specialist pain centre. The primary outcome was the cumulative incidence of neuropathic postsurgical persistent pain, defined by occurrence at either the 3-month or 6-month follow-up. The primary end point was the effect of procedure type (open mesh v. laparoscopy) on the pri-mary outcome, adjusted for covariates likely to influence either the occurrence of persistent pain or the choice of a given procedure.
Statistical analysis
We performed our analyses using SAS software version 9.3 (SAS Institute Inc.). Results are expressed as means ± standard deviations for normally distributed data and as medians and interquartile ranges for non-normally dis-tributed data. Categorical data are expressed as number of cases and percentage of the total. Type-I error was set at 5%. We conducted risk factor analyses on the pooled data from the 2 subcohorts. The covariates to be considered in the multivariate analyses were first defined on the basis of their likelihood to influence the dependent outcome. These covariates were age, sex, body mass index (BMI), the centre at which the surgery took place, Pain Catastro-phizing Scale score,7 type of surgery, location of preopera-tive pain (if any), history of peripheral neuropathy, report of a putative neurotoxic condition (see Dualé and col-leagues5 for a detailed description of these 2 preceding
persist-duale.indd 115 2015-03-10 8:00 AM

RECHERCHE
116 J can chir, Vol. 58, No 2, avril 2015
composite outcomes), the use and time of use of locore-gional anesthesia, the use of intraoperative opioids and of intra- or postoperative ketamine, and the report of any early postoperative complications. Owing to the large number of centres, the centre where surgery was per-formed was not retained in the analysis.
To assess the risk of persistent neuropathic pain depend-ing of the type of surgery, we calculated odds ratios (ORs) and their 95% confidence intervals (CIs) using different methods with a presumed progressive level of relevance: raw univariate analysis; multivariate analysis with simple adjustment, selection of factors and propensity score adjust-ment; and propensity score matching. Open mesh surgery was considered to be the reference to which laparoscopy was compared. We conducted the multivariable risk factor analysis using a multistep approach: 1) reduction of the number of covariates either by eliminating those with very low variability or by building new composite variables with greater relevance; 2) transformation of the continuous vari-ables into ordinal variables according to their terciles taken as cut-off values to avoid bias due to a nonlinear relation with the dependent outcome; 3) elimination of the covari-ates for which the p value of the univariate Wald test exceeded 0.25 (with the exception of centre, age and BMI, which were forced into the model regardless of the p value); and 4) logistic regression with an automated backward elimination procedure with a significance threshold of p < 0.05 to stay in the model. We used a propensity score to represent the probability that a patient with particular back-ground characteristics (i.e., preoperative outcomes) would undergo the open mesh technique instead of laparoscopy. This score was calculated using logistic regression, with type of surgery as the dependent variable and all back-ground characteristics as explanatory variables, as selected on the basis of their putative association with either the dependent outcome or exposure to the surgical procedure.8 These characteristics were sex, BMI, age, Pain Catastroph-izing Scale score, history of peripheral neuropathy, putative neurotoxic condition and existence/location of preoperative pain. Continuous variables were separated in terciles. The hypothesis was that background characteristics in both groups would be similarly distributed within propensity score strata. We performed a multivariate analysis with pro-pensity score adjustment for additional perioperative covariates. The final step consisted of constructing 2 sam-ples of patients (1 in each subcohort), matched according to a 1:2 algorithm without replacement within 0.25 standard deviations of the logit of their estimated propensity scores. Conditional logistic regression, accounting for correlation within matched pairs, was used to compare the outcome of interest between patients who underwent the open mesh technique and those who underwent laparoscopy.
The sample size calculation was performed on the basis of the prevalence of persistent pain after inguinal hernior-rhaphy, as reported in the literature. As different rates were
reported in the literature, we estimated a 30% rate after pooling all the related studies available at the time of our study (see Dualé and colleagues5 for details). With a risk a set at 5%, a precision measure set at 5% and a prediction of 20% loss to follow-up during the study, we planned an in itial sample of 389 patients for each subcohort.
Results
We had some difficulty recruiting patients for the lapa-roscopy cohort; the results of an intermediate analysis of the primary outcome undertaken in September 2009 showed a cumulative incidence clearly inferior to the expected one, and the recruitment was discontinued at 40% of the initial objective. For the open mesh cohort, the same intermediate analysis showed a cumulative inci-dence slightly inferior to the expected one, and the recruitment was discontinued at 96% of the initial objec-tive. A total of 530 patients were included (156 in the lap-aroscopy group, 374 in the open mesh group), and the surgeries took place between June 2006 and December 2008. Our analyses included only the patients for whom complete information on the studied outcomes was avail-able: 126 patients who underwent laparoscopy and 242 who underwent open mesh repair, representing 80.7% and 64.7%, respectively, of all patients. The demographic and clinical characteristics of both subcohorts are sum-marized in Table 1; a full description is available else-where.5 Ten patients were taking medication for pain 6 months after surgery, and 4 of them were considered to have neuropathic pain based on positive responses to the DN4 diagnostic questionnaire. When graded according to the World Health Organization’s (WHO) analgesic ladder, 4 patients had a first-step and 3 had a second-step treatment, and 1 was treated for neuropathic pain (anti-depressant plus gabapentin).
The centre where surgery was undertaken was not retained as a factor in the multivariate analysis, because the number of centres was too large and the number of patients per centre was too small and because, overall, each centre predominantly performed 1 of the 2 types of sur-gery. The intraoperative use of systemic opioids was the only factor representing the anesthetic practice that was retained for analysis, as it was less associated with the type of surgery and represented both the practice of general anesthesia and the time course of locoregional anesthesia (e.g., systemic opioids are not given for a surgery per-formed under successful spinal anesthesia). Two factors facilitating the incidence of neuropathic pain were identi-fied by the stepwise logistic regression model: open mesh surgery (Table 2) and history of neuropathic event (OR 3.19, 95% CI 1.45–7.05, p = 0.004). Age older than the third tercile was found to be a protective factor (OR 0.18, 95% CI 0.06–0.53, p = 0.049). Table 2 shows the different ORs for the risk of occurrence of postsurgical persistent
persist-duale.indd 116 2015-03-10 8:00 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 117
Table 1. Demographic and clinical characteristics of the study sample
Group, no. (%)*
Characteristic Laparoscopy, n = 126 Open mesh, n = 242
Male sex 122 (96.8) 219 (90.5)
Age (mean ± SD), yr 55.9 ± 12.4 59.5 ± 14.2
Weight (mean ± SD), kg 75.5 ± 9.2 74.5 ± 11.4
Height (mean ± SD), cm 174.7 ± 6.4 172.5 ± 7.8
Body mass index (mean ± SD) 24.7 ± 2.7 25.0 ± 3.4
Recruiting centre
HR-1 23 (18.3) 10 (4.1)
HR-2 0 (0) 18 (7.4)
HR-3 0 (0) 26 (10.7)
HR-4 0 (0) 44 (18.2)
HR-5 10 (7.9) 0 (0)
HR-6 0 (0) 3 (1.2)
HR-7 44 (34.9) 1 (0.4)
HR-8 0 (0) 82 (33.9)
HR-9 0 (0) 44 (18.2)
HR-10 1 (0.8) 1 (0.4)
HR-11 2 (1.6) 0 (0)
HR-12 0 (0) 3 (1.2)
HR-13 46 (36.5) 0 (0)
HR-14 0 (0) 10 (4.1)
Catastrophizing Pain Score (preoperative), median [IQR] 9.5 [3 –17] 9 [3 –18]
Preoperative pain
No pain 46 (36.5) 86 (35.5)
Elsewhere 18 (14.3) 35 (14.5)
Unknown location 24 (19.0) 44 (18.2)
Close to the site of surgery 33 (26.2) 74 (30.6)
At the site of surgery 5 (4.0) 74 (30.6)
History of peripheral neuropathy 30 (23.8) 74 (30.6)
Putative neurotoxic condition 3 (2.4) 34 (14.0)
Perioperative outcomes
General anesthesia 124 (98.4) 185 (76.4)
Intraoperative use of systemic opioids 124 (98.4) 180 (74.4)
Locoregional anesthesia
None 109 (86.5) 79 (32.6)
Postoperative only 12 (9.5) 11 (4.5)
Peroperative only 5 (4.0) 106 (43.8)
Peri- and postoperative 0 (0) 46 (19.0)
Perioperative use of ketamine 80 (63.5) 50 (20.7)
Postoperative complication 5 (4.0) 10 (4.1)
Persistent pain at 3 mo†
All cases 29 (21.0) 55 (21.7)
Positive response to DN4 4 (2.9) 29 (11.4)
Pain score (VAS out of 10), median [IQR]
DN4 (–) 2.3 [1.6 – 2.9] 1 [0.8 – 2.5]
DN4 (+) Missing data§ 2.4 [1.5 – 3.2]
Persistent pain at 6 mo‡
All cases 18 (14.0) 60 (18.3)
Positive response to DN4 1 (0.8) 26 (7.9)
Pain score (VAS out of 10), median [IQR]
DN4 (–) 1.5 [0.8 – 2.1] 1.1 [0.6 – 1.9]
DN4 (+) Missing data¶ 2.3 [1.4 – 5.1]
Report of persistent neuropathic pain, any time 4 (3.2) 30 (12.4)
DN4 = DN4 diagnostic questionnaire; IQR = interquartile range; SD = standard deviation; VAS = visual analogue scale. *Unless otherwise indicated. †n = 138 in the laparoscopy group and n = 254 in the open mesh group. ‡n = 128 in the laparoscopy group and n = 328 in the open mesh group. §The 3 available pain scores were 1.2, 2.2 and 2.4 /10. ¶The pain score was 10/10 for the only case.
persist-duale.indd 117 2015-03-10 8:00 AM

RECHERCHE
118 J can chir, Vol. 58, No 2, avril 2015
neuropathic pain (open mesh v. laparoscopy). For the mul-tivariate analysis with propensity-score adjustment, the use of perioperative ketamine and the occurrence of postoper-ative complications were taken as additional perioperative covariates. The ORs were quite stable regardless of the method of analysis used with the exception of propensity-matched analysis, which had a lower precision owing to a smaller sample size. The OR tended to increase with the level of evidence, reaching a value slightly inferior to 7 for the propensity-matched analysis.
Discussion
The main result of the present substudy is the strong dif-ference in risk of occurrence of persistent neuropathic pain, with a nearly 7-fold greater risk of pain associated with open mesh compared with laparoscopic surgery. On the other hand, the risk of persistent pain, regardless of the suspected mechanism, was not substantially greater after open mesh than laparoscopic surgery (Table 1). This information adds to the debate about the optimal tech-nique for herniorrhaphy, as a neuropathic mechanism is considered a factor of severity and chronicization of post-surgical persistent pain.4,9 In addition, the role of preoper-ative history of peripheral neuropathy in the occurrence of persistent neuropathic pain, as shown previously,5 was confirmed in our subcohorts. In addition, we observed no protective role of locoregional anesthesia, probably because this technique acts to block central sensitization rather than neuropathic processes.
Since both open mesh and laparoscopic surgery were developed in the late 1990s as an alternative to meshless herniorrhaphy, the issue of long-term complications of these 2 concurrent techniques has been addressed. Two meta-analyses conducted by the European Hernia Soci-ety, which covered the publication periods before and after May 2008, respectively,10,11 failed to show a different risk of persistent pain between the 2 techniques. How-ever, a recent review suggested a 3-fold greater risk (18% v. 6%) with open surgery than with laparoscopy,12 and this finding is supported by a focus on the most promi-nent randomized trials13–17 or well-sized prospective
cohort studies.18–20 It must be noted that pain was not the primary outcome in the trials and that none of these studies quantified the neuropathic aspect of pain. More information was recently provided by a prospective study of persistent pain 6 months after herniorrhaphy in 244 patients who underwent Lichtenstein and and 198 who underwent laparoscopic procedures, respectively, with clinical and psychophysical examination.3 The adjusted OR for persistent pain was 0.45 (95% CI 0.23–0.87) for the laparoscopic compared with the Lichten-stein procedure (i.e., open mesh doubled the risk). The study also showed that patients who underwent open mesh surgery exhibited increased thresholds to warm and hot sensations in the groin area, a symptom suggesting nerve lesion.2,21 It must be noted that, in that study, each centre offered only 1 type of surgery, but no adjustment based on propensity score was performed. Such adjust-ment reduces the bias due to factors that could influence the likelihood for each patient to undergo one procedure over another.22
As stated in the sample size estimation, based on the available literature we expected a 30% rate of persistent pain, regardless of the neuropathic features, at least for open mesh surgery. The rates observed in the present study were lower than expected, although this did not alter the statistical precision in estimating the risk. This is also consistent with a recent meta-analysis of 89 studies that estimated a 7%–12% risk of persistent pain after hernior-rhaphy, regardless of the technique performed.1 This decrease in global risk over the years may be explained either by an improvement in surgical techniques or by bet-ter precision in assessing pain. The authors also estimated that 30.5% of the pain reported was probably or definitely neuropathic, which is consistent with the observation of raw prevalence rates of pain at 6 months after open mesh surgery (18.3% for all pain and 7.9% for neuropathic pain). The lack of literature related to the association between neuropathic pain and laparoscopy makes any comparison with the present results difficult. The internal validity of the present study is supported by the results of the risk factor analysis, as a protective role of older age has been previously suggested in inguinal herniorraphy.18
Table 2: Analyses of persistent neuropathic pain following open mesh versus laparoscopic surgery
No. of patients
Method All Laparoscopy Open meshReporting
neuropathic pain OR (CI 95%)* p value
Univariate analysis 368 126 242 34 4.3 (1. 5–12.5) 0.007
Multivariate analysis, adjusted 368 126 242 34 5.0 (1.4–17.1) 0.011
Multivariate analysis, selected 368 126 242 34 4.6 (1.5–13.8) 0.006
Multivariate analysis, PS-adjusted 368 126 242 34 4.1 (1.3–13.0) 0.016
PS-matched analysis 319 125 194 30 6.8 (1.5–30.4) 0.012
CI = confidence interval; OR = odds ratio; PS = propensity score. *OR estimated following 5 different techniques (see the Methods section).
persist-duale.indd 118 2015-03-10 8:00 AM

RESEARCH
Can J Surg, Vol. 58, No. 2, April 2015 119
Limitations
The present study has some methodological limitations. First, self-report screening questionnaires for neuropathic pain do not have a 100% sensitivity and specificity, and diagnosis should be confirmed by clinical examination.23 Second, details of the precise location of neuropathic pain were not collected, although this information is important to estimate which nerve termination(s) may be involved. Third, information about the device used for open mesh repair (e.g., flat mesh, plug, bilayer) was not recorded. Techniques of nerve preservation were not noted either, as they had not been identified as a standard technique at the time of survey administration; there was no notion during our study period of any practice of intentional neur ectomy for herniorrhaphy in France.
In addition, the incidence rates reported here do not imply that all cases will turn into chronic pain with rele-vant consequences on daily life. Severe cases of reported pain made up only about 4% of the whole cohort (18/458) 6 months after surgery, and few patients had treatment beyond the first step of the WHO analgesic ladder. This is in accordance with the literature, with respective rates of 2%–7% for severe persistent pain and 1%–3% for need for a treatment.20,24–26 It cannot be ruled out that pain spontaneously resolved in some patients, as some studies with longitudinal follow-up showed a decrease in the rate of persistent pain with postsurgical delay.27–29 At this point, only long-term cohorts who undergo clinical examinations can help to obtain relevant information.
ConClusion
The results of the present study are not sufficient to rec-ommend the systematic use of laparoscopic surgery instead of open mesh for inguinal herniorrhaphy. First, laparoscopic repair may have disadvantages, such as a lon-ger duration of the procedure and a higher rate of serious complications, including visceral and vascular injuries.19 Second, the surgeons’ experience, the patients’ preference and their confidence in the team are well-known factors influencing the quality of the results. A recent review con-ducted by a collective of expert surgeons pointed out the challenge in developing strategies to identify and encour-age the correct handling of the nerves involved in this sur-gery (i.e., ilioinguinal, iliohypogastric and genitofemoral nerves). There is still no high-level evidence to recom-mend a particular nerve-preserving technique.30 It must be added that intraoperative nerve lesion is not the only pos-sible mechanism of neuropathic pain. In patients who experience neuropathic pain and have been reoperated for this reason, examination has revealed not only cases of transection, neuroma or entrapment by sutures, but also entrapment in the fibrosis around the sutured mesh.31,32
Acknowledgements: The authors thank the physicians who helped with patient inclusions and/or in hospital data collection, the clinical research assistancts who conducted local coordination and data moni-toring and the assistants who conducted the data transfer, management and quality control.
Affiliations: From CH Princesse Grâce de Monaco, Anesthésie- Réanimation, Monaco (Niccolaï); CHU Clermont-Ferrand, Pôle Santé Publique, Clermont-Ferrand, France (Ouchchane); Université Cler-mont, Clermont-Ferrand, France (Ouchchane, Dubray, Schoeffler); CNRS, ISIT, UMR6284, BP10448, Clermont-Ferrand, France (Ouchchane); Clinique de La Louvière, Anesthésie-Réanimation, Lille, France (Libier); CHU Nice, Anesthésie-Réanimation Ouest, Hôpital de l’Archet 2, Nice, France (Beouche); CHG Aurillac, Anesthésie-Réanimation, Aurillac, France (Belon); Clinique du Tonkin, Anesthésie-Réanimation, Villeurbanne, France (Vedrinne); CHG Thiers, Anesthésie-Réanimation, Thiers, France (El Drayi); CHG Riom, Anesthésie-Réanimation, Riom, France (Vallet); CHG Vichy, Anesthésie-Réanimation, Vichy, France (Ruiz); CHU Strasbourg, Pôle d’Anesthésie Réanimations chirurgicales-SAMU-SMUR, Hôpital de Hautepierre, Strasbourg, France (Biermann); Clinique de la Pergola, Chirurgie, Vichy, France (Duchêne); CHG Montluçon, Anesthésie-Réanimation, Montluçon, France (Chirat); CHU Clermont-Ferrand, Centre de Pharmacologie Clinique (Inserm CIC1405), Clermont- Ferrand, France (Soule-Sonneville, Dualé, Dubray); Inserm, U1107 “Neuro-Dol”, Clermont-Ferrand, France (Dualé, Dubray, Schoeffler); and CHU Clermont-Ferrand, BLOC-ARCHI (Anesthésie- Réanimation), Clermont-Ferrand, France (Schoeffler).
Competing interests: C. Dualé declares support from Pfizer for the con-duct of the study in the form of subsides paid to the University Hospital of Clermont-Ferrand, for communication about the results of the study and postsurgical persistent neuropathic pain during the EFIC Congress in Hamburg, Germany (September 2011), and for training materials for pri-mary and secondary care physicians, to highlight the prevalence of postsur-gical persistent neuropathic pain. No other competing interests declared.
Contributors: L. Ouchchane, C. Dualé and C. Dubray designed the study. N. Patrick, M. Libier, F. Beouche, M. Belon, J.-M. Vedrinne, B. El Drayi, L. Vallet, F. Ruiz, C. Biermann, P. Duchêne, C. Chirat, S. Soule-Sonneville, C. Dualé and P. Schoeffler acquired the data, which L. Ouchchane and C. Dualé analyzed. C. Dualé wrote the article, which all authors reviewed and approved for publication.
Funding: Funding was provided by the French program for hospital clinical research (Programme Hospitalier de Recherche Clinique, appel d’offre national 2005) and Pfizer. The funding sources had no role in the design, practice or analysis of this study.
References
1. Haroutiunian S, Nikolajsen L, Finnerup NB, et al. The neuropathic component in persistent postsurgical pain: a systematic literature review. Pain 2013;154:95-102.
2. Aasvang EK, Brandsborg B, Christensen B, et al. Neurophysiological characterization of postherniotomy pain. Pain 2008;137:173-81.
3. Aasvang EK, Gmaehle E, Hansen JB, et al. Predictive risk factors for persistent postherniotomy pain. Anesthesiology 2010;112:957-69.
4. Attal N, Lanteri-Minet M, Laurent B, et al. The specific disease burden of neuropathic pain: results of a French nationwide survey. Pain 2011;152:2836-43.
5. Dualé C, Ouchchane L, Schoeffler P, et al. Neuropathic aspects of persistent postsurgical pain: a French multicenter survey with a 6-month prospective follow-up. J Pain 2014;15:24.e1.
6. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005;114:29-36.
7. Sullivan MJ, Bishop S, Pivik J. The Pain Catastrophizing Scale: development and validation. Psychol Assess 1995;7:524-32.
8. Brookhart MA, Schneeweiss S, Rothman KJ, et al. Variable selection for propensity score models. Am J Epidemiol 2006;163:1149-56.
9. McDermott AM, Toelle TR, Rowbotham DJ, et al. The burden of
persist-duale.indd 119 2015-03-10 8:00 AM

RECHERCHE
120 J can chir, Vol. 58, No 2, avril 2015
neuropathic pain: results from a cross-sectional survey. Eur J Pain 2006;10:127-35.
10. Simons MP, Aufenacker T, Bay-Nielsen M, et al. European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia 2009;13:343-403.
11. Miserez M, Peeters E, Aufenacker T, et al. Update with level 1 studies of the European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia 2014;18:151-63.
12. Aasvang E, Kehlet H. Chronic postoperative pain: the case of ingui-nal herniorrhaphy. Br J Anaesth 2005;95:69-76.
13. Neumayer L, Giobbie-Hurder A, Jonasson O, et al. Open mesh ver-sus laparoscopic mesh repair of inguinal hernia. N Engl J Med 2004;350:1819-27.
14. The MRC Laparoscopic Groin Hernia Trial Group. Laparoscopic versus open repair of groin hernia: a randomised comparison. Lancet 1999;354:185-90.
15. Grant AM, Scott NW, O’Dwyer PJ. Five-year follow-up of a ran-domized trial to assess pain and numbness after laparoscopic or open repair of groin hernia. Br J Surg 2004;91:1570-4.
16. Bueno J, Serralta A, Planells M, et al. Inguinodynia after two inguinal her-niorrhaphy methods. Surg Laparosc Endosc Percutan Tech 2004;14:210-4.
17. Douek M, Smith G, Oshowo A, et al. Prospective randomised con-trolled trial of laparoscopic versus open inguinal hernia mesh repair: five year follow up. BMJ 2003;326:1012-3.
18. Nienhuijs S, Staal E, Strobbe L, et al. Chronic pain after mesh repair of inguinal hernia: a systematic review. Am J Surg 2007;194:394-400.
19. McCormack K, Scott NW, Go PM, et al. Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Database Syst Rev 2003;CD001785.
20. Heikkinen T, Bringman S, Ohtonen P, et al. Five-year outcome of lap-aroscopic and Lichtenstein hernioplasties. Surg Endosc 2004;18:518-22.
21. Dualé C, Guastella V, Morand D, et al. Characteristics of the neur-opathy induced by thoracotomy: a 4-month follow-up study with
psychophysical examination. Clin J Pain 2011;27:471-80.22. Rosenbaum PR, Rubin DB. Constructing a control group using mul-
tivariate matched sampling methods that incorporate the propensity score. Am Stat 1985;39:33-8.
23. Treede RD, Jensen TS, Campbell JN, et al. Neuropathic pain: redef-inition and a grading system for clinical and research purposes. Neurology 2008;70:1630-5.
24. Stark E, Oestreich K, Wendl K, et al. Nerve irritation after laparo-scopic hernia repair. Surg Endosc 1999;13:878-81.
25. Page B, Paterson C, Young D, et al. Pain from primary inguinal her-nia and the effect of repair on pain. Br J Surg 2002;89:1315-8.
26. Hindmarsh AC, Cheong E, Lewis MP, et al. Attendance at a pain clinic with severe chronic pain after open and laparoscopic inguinal hernia repairs. Br J Surg 2003;90:1152-4.
27. Schmedt CG, Daubler P, Leibl BJ, et al. Simultaneous bilateral lapa-roscopic inguinal hernia repair: an analysis of 1336 consecutive cases at a single center. Surg Endosc 2002;16:240-4.
28. Bay-Nielsen M, Nilsson E, Nordin P, et al. Chronic pain after open mesh and sutured repair of indirect inguinal hernia in young males. Br J Surg 2004;91:1372-6.
29. Picchio M, Palimento D, Attanasio U, et al. Randomized controlled trial of preservation or elective division of ilioinguinal nerve on open inguinal hernia repair with polypropylene mesh. Arch Surg 2004;139:755-8.
30. Alfieri S, Amid PK, Campanelli G, et al. International guidelines for prevention and management of post-operative chronic pain following inguinal hernia surgery. Hernia 2011;15:239-49.
31. Vuilleumier H, Hubner M, Demartines N. Neuropathy after herni-orrhaphy: indication for surgical treatment and outcome. World J Surg 2009;33:841-5.
32. Loos MJ, Verhagen T, Scheltinga MR, et al. A randomised con-trolled trial of injection therapy versus neurectomy for post- herniorrhaphy inguinal neuralgia: rationale and study design. Hernia 2010;14:593-7.
persist-duale.indd 120 2015-03-10 8:00 AM

RESEARCH • RECHERCHE
©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 121
Canadian practice patterns for pancreaticoduodenectomy
Background: Discordant practice patterns may be a consequence of evidence– practice gaps or deficiencies in knowledge translation. We examined the current strategies used by hepato-pancreatico-biliary (HPB) surgeons in Canada for the perioperative manage-ment of pancreaticoduodenectomy (PD).
Methods: We generated a web-based survey that focused on the perioperative meas-ures surrounding PD. The survey was distributed to all members of the Canadian Hepato-Pancreatico-Biliary Association.
Results: The survey was distributed to 74 surgeons and received a response rate of 50%. Many similarities in surgical techniques were reported; for example, most surgeons (86.5%) reconstruct the pancreas with pancreaticojejunostomy rather than pancreatico-gastrostomy. In contrast, variable techniques regarding the use of peritoneal drainage tubes, anastomotic stents, octreotide and other intraoperative modalities were reported. Most surgeons (75.7%) reported that their patients frequently required preoperative biliary drainage, yet there was minimal agreement with the designated criteria. There was variability in postoperative care, including the use of epidural analgesia and timing of postoperative oral nutrition.
Conclusion: We identified heterogeneity among Canadian HPB surgeons, suggest-ing a number of evidence–practice gaps within specific domains of pancreatic resec-tions. Focused research in these areas may facilitate technical agreement and improve patient outcomes following PD.
Contexte : La discordance entre les modes de pratique pourrait être due à des lacunes au plan des pratiques fondées sur des preuves ou à une déficience du transfert des con-naissances. Nous avons étudié les stratégies actuellement utilisées par les chirurgiens hépato-pancréato-biliaires (HPB) au Canada pour la prise en charge périopératoire de la pancréatoduodénectomie (PD).
Méthodes : Nous avons préparé un questionnaire électronique sur les mesures péri-opératoires entourant la PD. Le questionnaire a été distribué à tous les membres de l’Association hépato-pancréato-biliaire canadienne.
Résultats : Le questionnaire a été distribué à 74 chirurgiens et a généré un taux de réponse de 50 %. De nombreuses similitudes dans les techniques chirurgicales ont été signalées : par exemple, la majorité des chirurgiens (86,5 %) reconstruisent le pancréas par pancréatojéjunostomie plutôt que par pancréatogastrostomie. En revanche, on a observé une variabilité dans les techniques d’utilisation des drains péritonéaux, des endoprothèses anastomotiques, des octréotides et autres modalités peropératoires. La majorité des chirurgiens (75,7 %) ont signalé que leurs patients avaient souvent besoin de drains biliaires préopératoires et pourtant, les critères désignés ne semblaient pas faire l’unanimité. On a aussi noté des différences dans les soins postopératoires, y compris en ce qui concerne le recours à l’analgésie péridurale et le moment de la reprise de l’alimentation orale après la chirurgie.
Conclusion : Nous avons observé une hétérogénéité dans la pratique des chirurgiens HPB canadiens, ce qui donne à penser qu’il existe des lacunes au plan des pratiques fondées sur des preuves pour certains aspects précis des résections pancréatiques. Une recherche plus approfondie sur ces aspects pourrait favoriser le consensus technique et améliorer les résultats chez les patients après une PD.
David P. Cyr, MSc Jessica L. Truong, BHSc Jenny Lam-McCulloch, PhD Sean P. Cleary, MD, MSc, MPH Paul J. Karanicolas, MD, PhD
Accepted for publication Sept. 29, 2014
Correspondence to: P.J. Karanicolas Sunnybrook Health Sciences Centre Department of Surgery 2075 Bayview Ave, Rm T2-016 Toronto ON M4N 3M5 [email protected]
DOI: 10.1503/cjs.011714
practice-cyr.indd 121 2015-03-10 1:24 PM

RECHERCHE
122 J can chir, Vol. 58, No 2, avril 2015 .
P ancreatic ductal adenocarcinoma is the fourth leading cause of cancer-related deaths worldwide.1 In 2014, there were an estimated 4700 new cases of pancreatic
cancer in Canada and 4400 deaths, with a 5-year relative sur-vival rate of 8%.2 Although there have been recent advances in understanding the underlying pathophysiology of pancreatic cancer as well as the diagnosis, staging and treatment of early-stage tumours, minimal progress has been made in the early detection, prevention and treatment of late-stage disease.3,4
Surgery remains the only potential curative intervention; however, owing to the late clinical presentation of disease only 15%–20% of pancreatic tumours are technically resectable.5 The treatment of choice for resectable tumours found within the pancreatic head or uncinate process is pancreaticoduodenectomy (PD), also known as a Whipple resection.6 Pancreaticoduodenectomy is a high-risk proced-ure that is typically performed by specialized surgeons at high-volume centres;7 however, despite significant reduc-tions in postoperative mortality and morbidity over the past few decades, overall prognosis after resection for patients with pancreatic adenocarcinoma remains poor.8–10
The improved perioperative outcomes may be credited to recent technical advancements in the surgical manage-ment of pancreatic malignancies; however, rapid evolution of perioperative care has the potential to introduce hetero-geneity into surgical practice.11,12 The process of translating new research findings into routine clinical practice may be stagnant and inconsistent, yet failing to do so (known as an evidence–practice gap) can negatively affect the quality of patient care.13–15
Our objective was to survey Canadian surgeons who perform PD to understand current perioperative prac-tice patterns. We sought to elucidate the existence of evidence– practice gaps in this population and identify domains in which future research opportunities may yield fruitful findings.
Methods
We generated a survey to evaluate the current practice patterns in Canada for the surgical treatment of pancreatic cancer. The survey contained 41 questions with multiple domains of interest, including training and practice; peri-operative management of all pancreatic cancer; and pre-operative, intraoperative and postoperative measures for PD. Three hepato-pancreatico-biliary (HPB) surgeons piloted the survey, and we used their feedback to optimize the clarity of the survey.
This web-based survey was designed and distributed using the online survey tool SurveyMonkey. It was distributed by email to all members of the Canadian Hepato-Pancreatico-Biliary Association and to surgeons affiliated with the HPB CONCEPT Team, a national collaborative group of HPB surgeons. Following a modified Dillman method,16 we gave recipients 5 weeks to respond to the survey and sent them
weekly electronic reminders. After this 5-week period, each nonresponder was sent an individualized reminder to com-plete the survey. All responses were collected anonymously. We conducted a random draw for a token gift as an incentive for recipients to complete our survey.
Survey data were descriptively analyzed and illustrated using GraphPad Prism software version 5.03 (GraphPad Software, Inc.).
Results
Of the 74 Canadian surgeons invited to participate, 37 (50.0%) completed the survey in its entirety. Nearly all respondents practised in academic hospitals located in urban centres (Table 1). Most surgeons had subspecialty training in HPB (73.0%), followed by transplantation (43.2%) and surgical oncology (27.0%). Most participants (67.6%) devoted more than 75% of their practices to HPB surgeries, with a diverse range of years in practice and in the volume of surgeries performed annually. All surgeons actively performed PD.
Participants were asked a variety of questions regarding perioperative techniques when performing the pancreati-coenteric reconstruction during PD. Nearly all surgeons (86.5%) reported always performing pancreaticojejunos-tomy (PJ) rather than pancreaticogastrostomy (PG) (Fig. 1A). Furthermore, nearly all surgeons (94.4%) reported using the duct-to-mucosa method rather than the dunking method when performing PJ. The use of octreo-tide and other somatostatin analogues was polarized, with the majority of respondents either never (54.1%) or always (27.0%) administering it (Fig. 1B). Hemostatic agents, such as fibrin glue or Tisseel, were not commonly used, with most surgeons citing occasionally or not at all using them (Fig. 1C). In contrast, there was great variability regarding the use of PJ anastomotic stents (Fig. 1D).
Participants were asked about their use of various drains and endoluminal catheters. Most surgeons reported that their patients frequently undergo preoperative biliary drainage (75.7%; Fig. 2A). There was significant variability in the cri-teria used to select patients for stenting, including laboratory tests (liver function tests, serum bilirubin), clinical symptoms (jaundice) and surgical wait times. There was minimal agree-ment on the intraoperative placement of peritoneal drainage tubes (Fig. 2B). Just over half (59.5%) of surgeons reported always using nasogastric (NG) suction tubes (Fig. 2C).
In the postoperative setting, there is no discernible con-sensus for the ideal method of analgesia after PD. A greater number of surgeons reported always (29.7%) or frequently (56.8%) using epidural analgesia than surgeons who reported always (10.8%) or frequently (37.8%) using intravenous patient-controlled analgesia (IV PCA; Fig. 3). Two surgeons described occasionally using transversus abdominis plane (TAP) blocks. Heterogeneity was also observed regarding the timing of oral nutrition introduction postoperatively. A
practice-cyr.indd 122 2015-03-10 1:24 PM

RESEARCH
. Can J Surg, Vol. 58, No. 2, April 2015 123
large proportion of respondents reported that they start clear fluids at 49–72 hours (43.3%) and solid foods at 73– 120 hours (45.9%), yet many surgeons cited earlier and later times (Fig. 4). Interestingly, only a small number of participants (37.8%) described implementing standardized postoperative pathways, such as an enhanced recovery after surgery (ERAS) program.
Discussion
Reconstruction of pancreaticoenteric continuity is a critic al step following PD owing to its association with major postoperative complications. A leak of the pancreatic anastomosis and subsequent fistula formation remains the most significant contributor to morbidity and mortality.17 Potential interventions that are subject to ongoing debate include the anastomotic technique, octreotide, hemostatic agents and anastomotic stents.
In the present study, there was remarkable agreement among surgeons regarding the preferred reconstruction technique, with the majority always performing PJ compared with PG. Many studies have compared PJ with PG, and a consensus over the most effective technique remains to be determined; although several reports have shown similar outcomes between the 2 manoeuvres,18–21 others have found that PG reduces the incidence of postoperative fistula.22–24 Given the overwhelming preference for PJ over PG, quality evidence supporting a single technique has the potential to drastically change the postoperative course for patients undergoing PD.
Octreotide and other somatostatin analogues function to inhibit the release of endocrine and exocrine pancreatic secretions,25 a process that effectively reduces the volume of secretions and may decrease the incidence of anastomotic leaks and pancreatic fistulas. The precise role of prophylactic octreotide remains controversial; a number of recent studies have reported inconsistent effects on postoperative complications, yet a Cochrane review on the subject concluded that perioperative complications were reduced following somatostatin analogue treatment during pancreatic resections.26 Interestingly, despite this evidence most Canadian surgeons do not administer somatostatin analogues. It is unclear whether this apparent lack of knowledge translation is a result of knowledge deficits or critical appraisal of the existing data.
Other modalities that have been investigated in an attempt to optimize the pancreaticoenteric reconstruction have not been shown to be of great benefit. Hemostatic agents, such as a fibrin glue sealant, have recently been found to have no significant impact on the incidence of pancreatic leak, fistula formation or other postoperative complications.27,28 Moreover, PJ anastomotic stents, which have been hypothesized to facilitate drainage of secretions from the pancreatic duct and reduce the rate of leaks and fistulas, have not been convincingly shown to be of benefit.29,30
There remains considerable controversy surrounding the role of biliary stenting before PD. Patients with pancreatic cancer often present with obstructive jaundice due to biliary obstruction, placing them at risk for coagulation disturbances, hepatic dysfunction and cholangitis, thus promoting biliary decompression. More recently, the routine use of preoperative biliary drainage has been linked to increased perioperative infectious complications, morbidity and mortality.31 Despite this evidence, the use of biliary drains has increased over the last 2 decades.32 Given this
Table 1. Characteristics of study population (n = 37)
Charactertistic No. (%)
Province of practice
Alberta 4 (10.8)
British Columbia 1 (2.7)
Manitoba 1 (2.7)
New Brunswick 0 (0.0)
Newfoundland & Labrador 1 (2.7)
Nova Scotia 2 (5.4)
Ontario 22 (59.5)
Prince Edward Island 0 (0.0)
Quebec 5 (13.5)
Saskatchewan 1 (2.7)
Territories 0 (0.0)
Years in practice
< 5 9 (24.3)
5–10 11 (29.7)
11–15 6 (16.2)
> 15 11 (29.7)
Practice setting (population)
> 250 000 35 (94.6)
100 000–250 000 2 (5.4)
< 100 000 0 (0.0)
Practice setting
Academic (university-affiliated) 36 (97.3)
Community 1 (2.7)
Subspecialty/fellowship training
Laparoscopy 3 (8.1)
HPB 27 (73.0)
Surgical oncology 10 (27.0)
Transplantation 16 (43.2)
None 1 (2.7)
Percentage of practice devoted to HPB surgery
< 25% 3 (8.1)
25–50% 3 (8.1)
51–75% 6 (16.2)
> 75% 25 (67.6)
No. of HPB surgeries performed in past year*
< 20 0 (0.0)
20–40 8 (21.6)
41–60 6 (16.2)
61–80 9 (24.3)
81–100 9 (24.3)
> 100 5 (13.5)
HPB = hepato-pancreatico-biliary. *Includes transplants.
practice-cyr.indd 123 2015-03-10 1:24 PM

RECHERCHE
124 J can chir, Vol. 58, No 2, avril 2015 .
Fig. 1. Frequency of various perioperative techniques used for pancreaticoenteric anastomosis during pancreaticoduodenectomy (PD). PJ = pancreaticojejunostomy.
0
20
40
60
80
100
Pancreaticojejunostomy
0
20
40
60
80
100
Fibrin glue
0
20
40
60
80
100
PJ anastomotic stent
Octreotide
0
20
40
60
80
100
Never (< 5%)Occasionally (5–50%)
Frequently (51–95%)
Always (> 95%)
A B
C D
Res
pond
ents
, %R
espo
nden
ts, %
Res
pond
ents
, %R
espo
nden
ts, %
Fig. 2. Frequency of various perioperative drainage procedures surrounding pancreaticoduo-denectomy (PD).
Never (< 5%)Occasionally (5–50%)
Frequently (51–95%)
Always (> 95%)
A
B C
0
0 0
20
40
60
80
Res
pond
ents
, %R
espo
nden
ts, %
Res
pond
ents
, %
20
40
60
80
20
40
60
80
Pre-op biliary drainage
Peritoneal drainage tube Nasogastric suction
practice-cyr.indd 124 2015-03-10 1:24 PM

RESEARCH
. Can J Surg, Vol. 58, No. 2, April 2015 125
apparent discordance between strong level-I evidence and actual clinical practice, the development of guidelines regarding the role for preoperative biliary drainage are needed. Indications may include the presence of cholangi-tis, liver dysfunction, severe jaundice and delayed time to surgery.33 This is a target for future research and know-ledge translation to avoid unnecessary preoperative biliary drainage and associated complications.
The use of prophylactic intraperitoneal drains has his-torically been routine practice following pancreatic surgery with the intent to remove postoperative fluid collections and to facilitate early detection of anastomotic leaks, fistu-las and hemorrhages. Contrary to this dogma, a growing body of evidence has failed to demonstrate a decrease in the frequency and severity of postoperative complications or the necessity for intervention and that the use of intra-peritoneal drains after PD should not be mandatory.34–37 However, a randomized controlled trial was recently stopped early by the Data Safety Monitoring Board because mortality increased from 3% to 12% in patients undergoing PD without intraperitoneal drainage; these patients also had increased frequency and severity of com-plications.38 The authors cautioned against abandoning the use of intraperitoneal drains in all patients undergoing PD, explicitly stating that this would not be safe. This study’s divergent findings from the literature emphasize that fur-ther investigation into the utility and safety of this practice are of paramount importance.
Nasogastric suction has also historically been standard practice after major intra-abdominal procedures. Propon-ents postulate that NG suction decreases the risk of post-operative complications, such as ileus, anastomotic leaks, fistulas and wound dehiscence.39 More recent studies chal-lenge this dogma and suggest that routine NG decompres-sion is not warranted after elective abdominal surgeries.40 Specifically, routine NG tubes after PD may negatively impact the postoperative course and result in unnecessary patient discomfort. They also contribute to prolonged hos-pital stays, and their early removal is a critical component of fast-track surgical pathways.41 Thus, many authors advo-cate NG placement selectively in patients with delayed gastric emptying.42,43 Our data demonstrate that the major-ity of respondents always or frequently use NG suction after PD, indicating an important evidence–practice gap in the surveyed population.
Our study identified further variability regarding the optimal method of postoperative analgesia, with epidural analgesia somewhat favoured over IV PCA. Interestingly, this observation reflects the general opinion throughout the surgical literature. Epidural analgesia provides superior pain relief after PD than IV PCA;44 however, the impact of epidural analgesia on postoperative morbidity and mortal-ity is not completely understood. Recent studies have sug-gested that epidural use results in fewer postoperative complications;45 in contrast, epidural analgesia has been
found to promote hemodynamic instability following PD and possibly contributes to an increased incidence of vari-ous gastrointestinal and respiratory complications.46 Fur-ther research is warranted to determine the appropriate method of analgesia following PD in order to optimize pain relief and minimize complications.
The ERAS program is a novel, multimodal, structured concept that is designed to accelerate postoperative recov-ery, shorten the length of stay in hospital and decrease the rate of complications. The ERAS program has recently been safely applied to major pancreatic resections, such as PD, with demonstrated improved short-term outcomes.41,47–49 One of the most reproducible predictors of successful ERAS is early oral nutrition, with clear fluids often initiated on postoperative day 1 and solid foods on postoperative days 3–5; this is earlier than reported by the majority of our study population, who are mostly not practising ERAS. Other critical features of ERAS include minimizing epidural use,
Fig. 4. Time to the initiation of postoperative oral nutrition following pancreaticoduodenectomy (PD).
Res
pond
ents
, %
50
40
20
0
Fluids Solids
< 24 h24–48 h
49–72 h
73–120 h
> 120 h
30
10
Fig. 3. The use of various methods to manage postoperative pain following pancreaticoduodenectomy (PD). IV PCA = intraven ous patientcontrolled analgesia.
60
40
20
0
Epidural IV PCA
Never (< 5%)Occasionally (5–50%)
Frequently (51–95%)
Always (> 95%)R
espo
nden
ts, %
practice-cyr.indd 125 2015-03-10 1:24 PM

RECHERCHE
126 J can chir, Vol. 58, No 2, avril 2015 .
limiting postoperative NG suction, removing drains early and ambulating early. Many of these measures have been described in the present study, and ERAS is one strategy to promote their use and narrow the evidence–practice gap.
Limitations
Our study has some limitations. We relied on surgeons self-reporting practice patterns rather than auditing actual prac-tice patterns; it is possible that surgeons perceive or report practising differently than they actually do. There were a moderate absolute number of respondents; however, this is intrinsic to the study given that HPB care is centralized to high-volume, academic centres in Canada compared with other countries.7 Despite this homogeneous survey popula-tion, our study still demonstrated heterogeneous responses, contesting the impact of any possible selection bias. Finally, our study was limited by its descriptive nature and the inability to determine why there is disagreement among surgeons’ practices. Further research is needed to deter-mine whether the variability identified is associated with ineffective knowledge translation or evidence–practice gaps.
ConClusion
We have evaluated Canadian practice patterns for PD. Our primary objective was to determine areas of agree-ment in perioperative technique and to identify evidence–practice gaps between what procedures are supported throughout the literature versus those that are routinely practised. Given the rapid evolution of surgical practices and the growing number of pancreatic cancer diagnoses and subsequent resections,2 these conflicts may signifi-cantly impact morbidity and mortality. We identified sig-nificant heterogeneity in perioperative techniques and the existence of numerous evidence–practice gaps, indicating opportunities to guide future effective research and know-ledge translation strategies.Affiliations: From the Department of Surgery, University of Toronto, (Cyr, Lam-McCulloch, Cleary, Karanicolas); the Department of Surgery, Sunnybrook Health Sciences Centre (Cyr, Truong, Lam-McCulloch, Karanicolas); and the Department of Surgery, University Health Net-work (Cleary); Toronto, Ont.
Competing interests: None declared.
Contributors: All authors designed the study and acquired and ana-lyzed the data. D. Cyr wrote the article, which all authors reviewed and approved for publication.
References
1. Hariharan D, Saied A, Kocher HM. Analysis of mortality rates for pancreatic cancer across the world. HPB 2008;10:58-62.
2. Canadian Cancer Society’s Steering Committee on Cancer Statistics. Canadian Cancer Statistics 2014. Toronto, ON: Canadian Cancer Society; 2014. Available: www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian -Cancer-Statistics-2014-EN.pdf (accessed 2015 Feb. 23).
3. Hidalgo M. Pancreatic cancer. N Engl J Med 2010;362:1605-17.
4. Li D, Xie K, Wolff R, et al. Pancreatic cancer. Lancet 2004;363:1049-57. 5. He J, Page AJ, Weiss M, et al. Management of borderline and locally
advanced pancreatic cancer: Where do we stand? World J Gastroenterol 2014;20:2255-66.
6. Whipple AO, Parsons WB, Mullins CR. Treatment of carcinoma of the ampulla of vater. Ann Surg 1935;102:763-79.
7. Dixon E, Vollmer CM, Bathe O, et al. Training, practice, and referral patterns in hepatobiliary and pancreatic surgery: survey of general surgeons. J Gastrointest Surg 2005;9:109-14.
8. Crist DW, Sitzmann JV, Cameron JL. Improved hospital morbidity, mortality, and survival after the Whipple procedure. Ann Surg 1987; 206:358-65.
9. Sener SF, Fremgen A, Menck HR, et al. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985-1995, using the National Cancer Database. J Am Coll Surg 1999; 189:1-7.
10. Winter JM, Cameron JL, Campbell KA, et al. 1423 pancreaticoduo-denectomies for pancreatic cancer: a single-institution experience. J Gastrointest Surg 2006;10:1199-210, discussion 1210-1.
11. Sandhu L, Fox A, Nhan C, et al. Assessing the management of hepatic colorectal cancer metastases: Is treatment consistent in Ontario? HPB 2012;14:409-13.
12. Wei AC, Sandhu L, Devitt KS, et al. Practice patterns for the manage-ment of hepatic metastases from colorectal cancer: a mixed methods analysis. Ann Surg Oncol 2013;20:1567-74.
13. McGlynn EA, Asch SM, Adams J, et al. Quality of health care delivered to adults in the United States. N Engl J Med 2003;348:2635-45.
14. Westfall JM, Mold J, Fagnan L. Practice-based research — “blue highways” on the NIH Roadmap. JAMA 2007;297:403-6.
15. Grimshaw JM, Eccles MP, Lavis JN, et al. Knowledge translation of research findings. Implement Sci 2012;7:50.
16. Dillman DA, Phelps G, Tortora R, et al. Response rate and measure-ment differences in mixed-mode surveys using mail, telephone, inter-active voice response (IVR) and the internet. Soc Sci Res 2009;38:1-18.
17. Gouma DJ, van Geenen RC, van Gulik TM, et al. Rates of complica-tions and death after pancreaticoduodenectomy: risk factors and the impact of hospital volume. Ann Surg 2000;232:786-95.
18. Wellner UF, Sick O, Olschewski M, et al. Randomized controlled single-center trial comparing pancreatogastrostomy versus pancreati-cojejunostomy after partial pancreatoduodenectomy. J Gastrointest Surg 2012;16:1686-95.
19. Wente MN, Shrikhande SV, Müller MW, et al. Pancreaticojejunostomy versus pancreaticogastrostomy: systematic review and meta-analysis. Am J Surg 2007;193:171-83.
20. Duffas J-P, Suc B, Msika S, et al. A controlled randomized multicenter trial of pancreatogastrostomy or pancreatojejunostomy after pancre-atoduodenectomy. Am J Surg 2005;189:720-9.
21. Yeo CJ, Cameron JL, Maher MM, et al. A prospective randomized trial of pancreaticogastrostomy versus pancreaticojejunostomy after pancreaticoduodenectomy. Ann Surg 1995;222:580-8.
22. Shen Y, Jin W. Reconstruction by pancreaticogastrostomy versus pancre-aticojejunostomy following pancreaticoduodenectomy: a meta-analysis of randomized controlled trials. Gastroenterol Res Pract 2012;2012:1–7.
23. Topal B, Fieuws S, Aerts R, et al. Pancreaticojejunostomy versus pan-creaticogastrostomy reconstruction after pancreaticoduodenectomy for pancreatic or periampullary tumours: a multicentre randomised trial. Lancet Oncol 2013;14:655-62.
24. McKay A, Mackenzie S, Sutherland FR, et al. Meta-analysis of pan-creaticojejunostomy versus pancreaticogastrostomy reconstruction after pancreaticoduodenectomy. Br J Surg 2006;93:929-36.
25. Lembcke B, Creutzfeldt W, Schleser S, et al. Effect of the somatosta-tin analogue sandostatin (MS 201-995) on gastrointestinal, pancreatic and biliary function and hormone release in normal men. Digestion 1987;36:108-24.
26. Koti RS, Gurusamy KS, Fusai G, et al. Meta-analysis of randomized controlled trials on the effectiveness of somatostatin analogues for pancreatic surgery: a Cochrane review. HPB 2010;12:155-65.
practice-cyr.indd 126 2015-03-10 1:24 PM

RESEARCH
. Can J Surg, Vol. 58, No. 2, April 2015 127
27. Martin I, Au K. Does fibrin glue sealant decrease the rate of anasto-motic leak after a pancreaticoduodenectomy? Results of a prospective randomized trial. HPB 2013;15:561-6.
28. Lillemoe KD, Cameron JL, Kim MP, et al. Does fibrin glue sealant decrease the rate of pancreatic fistula after pancreaticoduodenectomy? Results of a prospective randomized trial. J Gastrointest Surg 2004; 8:766-72.
29. Xiong JJ, Altaf K, Mukherjee R, et al. Systematic review and meta-analysis of outcomes after intraoperative pancreatic duct stent placement during pancreaticoduodenectomy. Br J Surg 2012;99:1050-61.
30. Sachs TE, Pratt WB, Kent TS, et al. The pancreaticojejunal anasto-motic stent: Friend or foe? Surgery 2013;153:651-62.
31. Van der Gaag NA, Rauws EAJ, van Eijck CHJ, et al. Preoperative biliary drainage for cancer of the head of the pancreas. N Engl J Med 2010;362:129-37.
32. Jinkins LJ, Parmar AD, Han Y, et al. Current trends in preoperative biliary stenting in patients with pancreatic cancer. Surgery 2013; 154:179-89.
33. Iacono C, Ruzzenente A, Campagnaro T, et al. Role of preoperative biliary drainage in jaundiced patients who are candidates for pancre-atoduodenectomy or hepatic resection: highlights and drawbacks. Ann Surg 2013;257:191-204.
34. Conlon KC, Labow D, Leung D, et al. Prospective randomized clinical trial of the value of intraperitoneal drainage after pancreatic resection. Ann Surg 2001;234:487-93.
35. Fisher WE, Hodges SE, Silberfein EJ, et al. Pancreatic resection without routine intraperitoneal drainage. HPB 2011;13:503-10.
36. Adham M, Chopin-Laly X, Lepilliez V, et al. Pancreatic resection: Drain or no drain? Surgery 2013;154:1069-77.
37. Mehta VV, Fisher SB, Maithel SK, et al. Is it time to abandon routine operative drain use? A single institution assessment of 709 consecutive pancreaticoduodenectomies. J Am Coll Surg 2013;216:635-42.
38. Van Buren G, Bloomston M, Hughes SJ, et al. A randomized pro-
spective multicenter trial of pancreaticoduodenectomy with and without routine intraperitoneal drainage. Ann Surg 2014;259:605-12.
39. Sagar PM, Kruegener G, MacFie J. Nasogastric intubation and elec-tive abdominal surgery. Br J Surg 1992;79:1127-31.
40. Nelson R, Tse B, Edwards S. Systematic review of prophylactic naso-gastric decompression after abdominal operations. Br J Surg 2005; 92:673-80.
41. Robertson N, Gallacher PJ, Peel N, et al. Implementation of an enhanced recovery programme following pancreaticoduodenectomy. HPB 2012;14:700-8.
42. Kunstman JW, Klemen ND, Fonseca AL, et al. Nasogastric drainage may be unnecessary after pancreaticoduodenectomy: a comparison of routine vs selective decompression. J Am Coll Surg 2013;217:481-8.
43. Fisher WE, Hodges SE, Cruz G, et al. Routine nasogastric suction may be unnecessary after a pancreatic resection. HPB 2011;13:792-6.
44. Choi DX, Schoeniger LO. For patients undergoing pancreatoduo-denectomy, epidural anesthesia and analgesia improves pain but increases rates of intensive care unit admissions and alterations in analgesics. Pancreas 2010;39:492-7.
45. Amini A, Patanwala AE, Maegawa FB, et al. Effect of epidural analgesia on postoperative complications following pancreaticoduodenectomy. Am J Surg 2012;204:1000-4, discussion 1004-6.
46. Pratt WB, Steinbrook RA, Maithel SK, et al. Epidural analgesia for pancreatoduodenectomy: a critical appraisal. J Gastrointest Surg 2008; 12:1207-20.
47. Di Sebastiano P, Festa L, De Bonis A, et al. A modified fast-track pro-gram for pancreatic surgery: a prospective single-center experience. Langenbecks Arch Surg 2011;396:345-51.
48. Balzano G, Zerbi A, Braga M, et al. Fast-track recovery programme after pancreaticoduodenectomy reduces delayed gastric emptying. Br J Surg 2008;95:1387-93.
49. Berberat PO, Ingold H, Gulbinas A, et al. Fast track-different impli-cations in pancreatic surgery. J Gastrointest Surg 2007;11:880-7.
We believe in open access to researchTo ensure continued worldwide free access to all CJS content, articles submitted for publication as of Jan. 1, 2014, are subject to a submission fee of $100 (Canadian funds). Submission fees will be waived for corresponding authors affiliated with CJS sponsors.
Accepted Research, Review and Continuing Medical Education articles are subject to a publication fee of $700, and Commentaries and Discussions are subject to a publication fee of $500, payable on acceptance in Canadian funds.
Benefits of open access
• For researchers and institutions: increased visibility, usage and impact for their work• For government: a better return on investment for funding research• For society: efficient, effective patient care resulting in better outcomes
CJS articles are available free of charge on the journal website (canjsurg.ca) and in PubMed Central.
practice-cyr.indd 127 2015-03-10 1:24 PM

REVIEW • REVUE
128 J can chir, Vol. 58, No 2, avril 2015 ©2015 8872147 Canada Inc.
Surgical approach in primary total hip arthroplasty: anatomy, technique and clinical outcomes
Total hip arthroplasty (THA) has revolutionized the treatment of hip arthritis. A number of surgical approaches to the hip joint exist, each with unique advantages and disadvantages. The most commonly used approaches include the direct anterior, direct lateral and posterior approaches. A number of technical intricacies allow safe and efficient femoral and acetabular reconstruction when using each approach. Hip dislocation, abductor insufficiency, fracture and nerve injury are complications of THA, although their relative risk varies by approach. Numerous clinical trials have sought to elicit differences in patient-reported outcomes, complication rates and return to function among the surgical approaches. This review outlines some of the technical pearls of performing a THA through either a direct anterior, direct lateral or posterior approach. A literature review outlines the impact of surgical approach on clinical outcomes and clinically relevant complication rates.
L’arthroplastie pour prothèse totale de la hanche (PTH) a révolutionné le traitement de l’arthrite de la hanche. Il existe plusieurs approches chirurgicales pour l’articulation de la hanche, et chacune comporte ses avantages et inconvénients pro-pres. Les approches les plus souvent utilisées sont l’approche antérieure directe, l’approche latérale directe et les approches postérieures. Plusieurs détails techniques contribuent à une reconstruction fémorale et acétabulaire sécuritaire et efficace avec chaque approche. La dislocation de la hanche, l’insuffisance des abducteurs, la frac-ture et les lésions nerveuses sont les complications de la PTH, quoique leur risque relatif varie d’une approche à l’autre. Plusieurs essais cliniques ont voulu mettre en lumière les différences quant aux résultats, aux taux de complications et au rétablisse-ment fonctionnel déclarés par les patients selon les différentes approches chirurgi-cales utilisées. La présente synthèse résume quelques-unes des « perles techniques » pour l’exécution de la PTH soit par approche antérieure directe, latérale directe ou postérieure. Une revue de la littérature résume l’impact de l’approche chirurgicale sur les résultats cliniques et les taux de complications cliniquement importants.
S ince its inception in the 1960s, total hip arthroplasty (THA) has revolu-tionized the treatment of painful hip arthritis.1 More than 24 000 THA procedures are performed annually in Canada.2 Surgical approach in
THA is a recent area of interest in the literature. Each approach requires a thorough understanding of anatomy to optimize femoral and acetabular visual-ization, minimize complications and optimize patient outcomes.
The purpose of this review is to outline the anatomy and the technical aspects of the 3 commonly used surgical approaches to the hip: the direct anter-ior, direct lateral and posterior approaches. We conducted an evidence-based review examining studies that compared various clinical outcomes and compli-cation rates across the 3 approaches. Although surgeon experience and anec-dotal success are important factors when choosing surgical approaches for THA, our review demonstrates many important differences among the approaches that may influence surgeon choice in the future.
Methods
We performed a comprehensive literature search using PubMed and Medline. The keywords “hip,” “arthroplasty,” and “approach” were used to identify papers examining the topic of interest. The terms “anterior,” “lateral” and
Stephen Petis, MD, MSc James L. Howard, MD, MSc Brent L. Lanting, MD, MSc Edward M. Vasarhelyi, MD, MSc
Accepted for publication Sept. 19, 2014
Correspondence to: E.M. Vasarhelyi Division of Orthopedic Surgery London Health Sciences Centre University Hospital 339 Windermere Rd London ON N6A 5A5 [email protected]
DOI: 10.1503/cjs.007214
surg-petis.indd 128 2015-03-10 11:11 AM

REVIEW
Can J Surg, Vol. 58, No. 2, April 2015 129
“posterior” were added to our search in order to identify articles that were approach-specific. We included compar-ative studies published from 2000 to 2014 in our review. Study titles and abstracts were reviewed to determine level of evidence to ensure high-quality literature (i.e. meta-analyses, systematic reviews, randomized controlled trials) was included. We included articles published earlier than 2000 if they contributed to the discussion on surgical tech-nique or the incidence of particular complications.
Direct anterior approach
Overview
The direct anterior approach to the hip was first described by Smith-Peterson in the 1940s, and was later modified by Heuter in the 1950s.3 Internationally, this approach is gaining popularity in the hip arthroplasty community.4
Advocates of this approach consider its advantages to be the muscle-sparing nature of its internervous intervals, earlier restoration of gait kinematics and low dislocation rates.5–9 The direct anterior approach can be performed
with or without the use of a specialized table or fluoros-copy.10,11 Our institution favours the use of a specialized table and intraoperative fluoroscopy, which is described later in this section.
Anatomy and technical considerations
The procedure begins by positioning the patient supine on a specialized traction table (Fig. 1). Both feet are firmly secured to boots attached to lever arms that permit posi-tioning of each lower extremity and applying traction to either limb. The perineal post located between the legs stabilizes the patient on the operating room table and pro-vides a point of counter-traction.10
The surgical incision begins 2–4 cm lateral to the anterior superior iliac spine of the pelvis (Fig. 2). It is then carried dis-tally and laterally for about 8–12 cm at 20° from the sagittal plane of the patient toward the lateral aspect of the patient’s ipsilateral knee. The lateral femoral cutaneous nerve (LFCN) is identified, transposed medially and protected.
After protecting the LFCN, the fascia overlying the tensor fascia latae (TFL) is incised, and a plane is then developed
Fig. 1. Example of the specialized table (Hana fracture table, Mizuho OSI) used during a direct anterior approach. Boots attached to lever arms allow traction and free positioning of the leg during each procedure. A perineal post provides counter-traction, and a motorized lift allows improved femoral exposure.
Perineal post
Post for bone hook bracket
surg-petis.indd 129 2015-03-10 11:11 AM

REVUE
130 J can chir, Vol. 58, No 2, avril 2015
between the TFL and sartorius. The surgeon will then encounter the interval between the rectus femoris and gluteus medius. A Charnley hip retractor displaces the rectus femoris medially and the gluteus medius laterally to expose the anterior joint capsule of the hip. After coagulating or suture ligating the ascending branch of the lateral femoral circumflex artery, a Mueller retractor is placed inferior to the femoral neck, and a capsulotomy is performed. The joint capsule is incised along the length of the femoral neck from the acetabulum to the intertrochanteric line (Fig. 3).
Gentle traction is then applied to the operative limb. Mueller and Hohmann retractors are placed intracapsularly around the femoral neck. A reciprocating saw is used to make a femoral neck osteotomy. The femoral head is then removed with a corkscrew (Fig. 4). The osteotomy can be repeated and the resultant napkin ring of bone removed to increase the ease of removing the femoral head.10,12
Once the femoral head is removed, traction is released and the leg is externally rotated to improve exposure for acetabular preparation. The Charnley hip retractor maintains exposure medially. Placement of the final acetabular component is facilitated by the use of an offset inserter handle to minimize soft tissue injury (Fig. 5). Intraoperative fluoroscopy is used to optimize component anteversion and inclination.
Femoral preparation can be difficult owing to limited proximal femoral exposure with this approach. The operative limb is carefully placed in a position of extension, adduction and external rotation to improve the accessibility of the proximal femur. Overly forceful external rotation can result in soft tissue injuries to the knee and ankle as well as intraoperative fracture. A specialized bone hook is then inserted around the posterior aspect of the femur just proximal to the insertion of the gluteus maximus tendon. This bone hook can be used manually to elevate the proximal femur anteriorly. In the subset of patients in whom the femur cannot be sufficiently mobilized anteriorly, sequential release of the conjoint tendon and piriformis can also improve mobilization of the femur. Rarely, a release of the anterior 1–2 cm of the origin of the TFL off the iliac wing may be required. An offset femoral broach handle eases access to the proximal femur during preparation (Fig. 6). Trialing can be combined with intraoperative fluoroscopy to assess leg length and offset. Femoral anteversion is identified based on the posterior cortex of the proximal femur or by using the femoral epicondyles as a reference point. Once the final implants are in situ and the hip is reduced, implant positioning is verified with fluoroscopy, and the stability of the construct can be assessed out of traction.10–12
Direct lateral approach
Overview
The direct lateral approach to the hip was described by Hardinge in 1982.13 Approximately 60% of Canadian
Fig. 3. Once the hip joint capsule is exposed, a capsulotomy is per-formed along the long axis for the femoral neck. Heavy braided suture tags are often used to assist in retracting the joint capsule to expose the femoral neck and identify the capsule for closure.
Anterior superior iliac spine
Hip joint capsule, incised
Femoral neck
Fig. 2. The skin incision used for the direct anterior approach to the hip.
Anterior superior iliac spine
Anterior approach skin incision
Fig. 4. After femoral neck osteotomy, the femoral head is removed using a corkscrew. The femoral head often requires manipulation to ensure the corkscrew is positioned eccentrically in the femoral head.
Femoral head
Corkscrew
Femoral head
surg-petis.indd 130 2015-03-10 11:11 AM

REVIEW
Can J Surg, Vol. 58, No. 2, April 2015 131
orthopedic surgeons perform THAs using a direct lateral approach.14 This approach provides adequate exposure of both the proximal femur and acetabulum.12 It has the bene-fit of providing an extensile exposure to the femur as required. A very low dislocation rate has also been re port ed in clinical follow-up.15,16
Anatomy and technical considerations
The procedure begins by positioning the patient in the lateral decubitus position. The operative limb is draped freely to assist with dislocating the hip and exposing the proximal femur and acetabulum. A sterile bag is incorpor-ated into the extremity drape to allow the surgeon to dis-locate the hip and visualize the femur during preparation.
A longitudinal incision is made extending 3–5 cm proximal and about 5–8 cm distal to the tip of the greater trochanter (Fig. 7). The fascia is split at the interval between the TFL and gluteus maximus in line with the skin incision. A Charnley retractor is then used to retract the incised fascia latae. The tendon and muscle fibres of the gluteus medius are then visualized and split at the midway point between the most anterior and posterior extent of the muscle, or in a one-third anterior/ two-thirds posterior fashion. The split is carried distally to the vastus ridge, leaving a cuff of gluteus medius ten-don for repair following the procedure (Fig. 8). The gluteus minimus and joint capsule are split either in line with the neck of the femur or in line with the tendinous fibres of the gluteus minimus. Some surgeons perform a capsulectomy to facilitate dislocating the hip. The sur-geon then dislocates the femoral head by externally rotating and flexing the hip and knee. The foot is posi-tioned in the sterile bag anteriorly. Hohmann retractors
are positioned around the femoral neck, allowing the surgeon to safely perform a femoral neck osteotomy using an oscillating saw.
Once the femoral neck osteotomy is completed, the surgeon will have access to the acetabulum and proximal femur. The acetabulum is prepared with the leg exter-nally rotated and the knee in extension on the table. Hohmann retractors are carefully placed anteriorly, pos-teriorly and inferiorly around the acetabulum to provide adequate visualization. A Hibbs retractor or additional Hohmann retractor can be used to retract superior soft tissues if visualization is impaired (Fig. 9). Soft tissue landmarks, such as the transverse acetabular ligament, reamer positioning relative to the floor and cup posi-tioning guides, can be used to verify acetabular version and inclination.
Fig. 6. (A) An offset femoral broach handle permits easier access to the proximal femur during preparation. (B) A bone hook assists with anterior displacement of the femur and can be secured in position using a sterile bracket.
A
B
Offset femoral broach handle
Femoral broach
Proximal femoral metaphysis
Sterile bracket
Bone hook
Fig. 5. Example of retractor placement during implantation of the acetabular component. Note the use of an offset inserter handle to minimize soft tissue trauma during insertion.
Hohmann retractors
Acetabular component
Offsetacetabular inserter
surg-petis.indd 131 2015-03-10 11:11 AM

REVUE
132 J can chir, Vol. 58, No 2, avril 2015
When preparing the proximal femur, the hip is flexed to near 90° and externally rotated, and the foot is placed in the sterile bag anteriorly with the knee flexed. Two Hohmann retractors, 1 blunt placed posteriorly around the lateral aspect of the proximal femur and 1 sharp placed medially around the proximal femur, allow slight anterior displacement of the femur. A third Hohmann retractor is stationed posteriorly in line with the long axis of the femur to protect the abductors during femoral preparation.
Posterior aPProach
Overview
The posterior approach to the hip was popularized by Moore in the 1950s.12 A recent survey of surgeons from around the world suggests that the posterior approach is the most common surgical approach used internationally for THAs.4 In Canada, about 36% of arthroplasty sur-geons use this approach.14 It provides adequate visualiza-tion of both the acetabulum and femur during both recon-structive procedures. The approach spares the abductor muscles during surgical exposure of the acetabulum and femur.12 It also has the benefit of providing an extensile exposure to the femur and acetabulum as required.
Anatomy and technical considerations
Similar to the direct lateral approach, for the posterior approach the patient is placed in the lateral decubitus posi-tion. Again, the involved limb is draped freely to facilitate dislocating the hip and to permit maneuverability of the limb to improve visualization throughout the procedure.
The skin incision begins 5 cm distal to the greater tro-chanter, centred on the femoral diaphysis. The incision continues proximal to the greater trochanter. At that point, it curves toward the posterior superior iliac spine for 6 cm. Alternatively, the incision can continue proximally in line with the femur with the hip flexed to 90° (Fig. 10).
The surgeon then incises the fascia latae overlying the gluteus maximus and bluntly splits the muscle down to the short external rotators (Fig. 11). A Charnley retractor is positioned to retract the gluteus maximus. The sciatic nerve is carefully protected as it travels immediately posterior to the short external rotators. After identification of the pirifor-mis, the short external rotators and piriformis are then
Fig. 8. (A) The gluteus medius muscle fibres and associated ten-dinous insertion on the greater trochanter. (B) A tenotomy is performed through this tendinous insertion, leaving a cuff of tis-sue for repair during closure.
A
B
Muscle �bres of gluteus medius
Tendinous insertion of gluteus medius
Vastus Lateralis
Gluteus medius tenotomy
Vastus lateralis
Fig. 7. The skin incision used for the direct lateral approach to the hip.
Outline of greater trochanter
Tip of greater trochanter
Anterior and posterior extent of lateral femoral shaft
Skin incision
Fig. 9. Visualization of the acetabulum using a direct lateral approach following careful retractor placement.
Hibbs retracting superior soft tissue
Acetabulum
Anterior Hohmann
Inferior Hohmann
Femoral neck osteotomy
Posterior Hohmann
surg-petis.indd 132 2015-03-10 11:11 AM

REVIEW
Can J Surg, Vol. 58, No. 2, April 2015 133
tenotomized at their insertion onto the greater trochanter. They are then tagged with a braided suture for identification and repair at the end of the procedure. This will then expose the posterior joint capsule, which is incised to reveal the femoral neck and head. Alternatively, the joint capsule can be incised with the short external rotators in a single layer during tenotomy. The femoral head is then dislocated by internally rotating the hip. A femoral neck osteotomy is then performed using Hohmann retractors anteriorly and posteriorly to protect soft tissues.
Once the osteotomized bone is removed, access is gained to the acetabulum and proximal femur. Careful placement of Hohmann retractors around the acetabulum permits adequate exposure for the reconstruction (Fig. 12). The femur is retracted anteriorly to expose the acetabulum to allow adequate restoration of acetabular anteversion. A posterior retractor or selfretaining retractor can be used to retract the posterior joint capsule to facilitate acetabular visualization. During acetabular preparation, soft tissue landmarks, such as the transverse acetabular ligament, reamer position relative to the floor and cuppositioning guides, are used to verify acetabular version and inclination.
The proximal femur is exposed with the leg internally rotated, flexed and slightly adducted. This places the long axis of the tibia vertically. Blunt bone skids or Hohmann retractors can be used to elevate the femur to improve exposure (Fig. 13). Femoral preparation can then be
completed in this position. Following the reconstruction, the short external rotators and posterior capsule are repaired through transosseous bone tunnels in the proximal femur or a direct repair to soft tissues.
ExtEnsilE ExposurEs
Extensile exposures of the hip allow the surgeon to access more of the proximal femur or acetabulum in patients requiring management of complex acetabular or femoral bone defects; revision surgery; surgery for pathologic lesions of the proximal femur or acetabulum; or intraoperative complications, such as fracture. One of the disadvantages of the direct anterior approach is that exposure of the proximal femur is limited. As the direct anterior approach is part of the classic Smith–Peterson approach, acetabular exposure is adequate for THA. Access to the posterior acetabulum may require a 2incision technique. Further proximal femoral exposure may require substantial soft tissue stripping of the vastus lateralis or a second incision using a lateral approach.17
Fig. 11. Exposure of the short external rotators during a posterior approach.
Greater trochanter
Vastus lateralis
Split gluteus maximus
Short external rotators
Fig. 12. Retractor placement and acetabular exposure using a posterior approach. The tagging suture helps retract the short external rotators, draping them over the sciatic nerve.
Femoral neck osteotomy
Acetabulum
Short external rotators tagged with suture
Fig. 10. The skin incision used for a posterior approach to the hip. A curvilinear incision or, alternatively, a straight incision with the hip flexed 90° can be used.
Skin incision
Tip of greater trochanter
Outline of greater trochanter
surg-petis.indd 133 2015-03-10 11:11 AM

REVUE
134 J can chir, Vol. 58, No 2, avril 2015
Both the direct lateral and posterior approaches have extensile approaches. A trochanteric osteotomy or slide can improve access to the posterior column of the acetabulum using a direct lateral approach. Another option to access the posterior aspect of the acetabulum is to develop a plane posteriorly between the gluteus minimus and medius. The direct lateral approach can also be extended distally by splitting the vastus lateralis to access more of the proximal femur. Extending the exposure proximally is limited by the proximity of the superior gluteal nerve approximately 5 cm proximal to the tip of the greater trochanter. To extend the posterior approach distally along the femoral shaft, the gluteus maximus insertion can be detached.12,17
Risks and complications
Dislocation
Postoperative dislocation following THA has a deleterious effect on patient outcomes and, when required, revision surgery incurs tremendous costs to the health care system.18,19 Medicare data from more than 58 000 elective
THAs in the United States suggest a dislocation rate of approximately 4%.20 However, this rate may be influenced by surgical approach at the time of the index procedure.
One of the purported benefits of the anterior and lateral approaches is lower dislocation rates than the posterior approach. A study by Sariali and colleagues21 prospectively followed 1764 patients who underwent primary THA performed through an anterior approach; patients were followed for 1 year postoperatively and had a dislocation rate (all dislocated anteriorly) of 1.5%. Another large series by Siguier and colleagues5 reported a dislocation rate of 0.96% in 1037 patients who underwent primary THA.Matta and colleagues6 reviewed 494 primary THAs performed through a direct anterior approach and reported 3 dislocations for a rate of 0.61%. The low dislocation rate has been attributed to verifying both acetabular and femor al component positioning via fluoroscopy and preserving static stabilizers, such as the posterior joint capsule.5,6
Preservation of the posterior soft tissue envelope may also explain the low dislocation rate observed with the lateral approach. A large retrospective review by Demos and colleagues22 reported 6 dislocations in 1515 patients (0.4%) undergoing a primary THA through a lateral approach.Masonis and Bourne15 performed a systematic review of the literature and determined a dislocation rate of 0.55% for 3438 THAs using the lateral approach. The definition of what constitutes a lateral approach may vary from study to study; therefore, the results of systematic reviews should be interpreted with scrutiny.
Dislocation rates for the posterior approach reported in the literature vary from 1% to 5%.16,23–26 Careful reconstruction of the capsule and short external rotators may decrease the risk of postoperative dislocation.12,16,27 Kwon and colleagues16 performed a metaanalysis to determine the rate of dislocations using a posterior approach with and without posterior soft tissue repair and found an 8 times greater relative risk of dislocation when soft tissue repair was not performed. Several repair techniques have been described for the posterior soft tissues. Examples include capsulorrhaphy of the capsule and short external rotators in 1 layer and transosseous bone tunnels in the greater trochanter.23,28
Abductor insufficiency
Abductor muscle insufficiency is a common clinical scen ario following a direct lateral approach. It can cause abductor muscle weakness, a Trendelenburg gait or sign, inefficient gait mechanics and peritrochanteric pain.15,29–31 The insufficiency likely results from failure of the repaired tenotomy following a direct lateral approach, chronic degeneration of the gluteus medius tendon preoperatively, or irreparable tears at the time of THA in up to 20% of patients undergoing the procedure.32,33 The latter point, as well as technical pitfalls, such as inadequate restoration of femoral offset, may explain why some patients undergoing primary THA
Fig. 13. Exposure of the proximal femur using a posterior approach. Note the position of the operative limb, held in posi-tion by a surgical assistant. Hohmann retractors or bone skids can help elevate the proximal femur during preparation.
Operative limb in internal rotation and slightadduction
Proximal femoral exposure
Blunt bone skid
surg-petis.indd 134 2015-03-10 11:12 AM

REVIEW
Can J Surg, Vol. 58, No. 2, April 2015 135
through a posterior or anterior approach may still exhibit abductor insufficiency postoperatively.34 Masonis and Bourne15 reviewed more than 2400 THAs involving a direct lateral approach and reported an incidence of 4%–20% for abductor insufficiency postoperatively. Careful closure of abductor tenotomy during the direct lateral approach and guided rehabilitation focusing on abductor and core strengthening in patients with preoperative abductor insuffi-ciency can help improve patient outcomes.
Fracture
Intraoperative fractures can be a devastating complication resulting in increased duration of surgery, difficult postop-erative mobilization due to weight-bearing modifications, prolonged functional recovery and poor patient outcomes. Jewett and Collis35 reviewed their experience with the direct anterior approach in 800 patients who underwent primary THA. The authors reported 19 (2.3%) intraoper-ative trochanteric fractures and no ankle fractures; most fractures occurred during femoral elevation with a bone hook and soft tissue avulsion. Interestingly, 15 of the intraoperative fractures occurred within the first 200 cases of the series. Matta and colleagues6 reviewed 494 direct anterior THAs and reported 7 (1.4%) intraoperative prox-imal femur fractures (4 fractures of the medial calcar dur-ing femoral broaching and 3 fractures of the greater tro-chanter during bone hook elevation). Three (0.6%) nondisplaced ankle fractures occurred when using isolated external rotation of the limb to dislocate the hip.
There is a paucity of literature examining the rate of intraoperative fracture risk with the direct lateral and pos-terior approaches. A retrospective review by Hendel and colleagues36 of 372 primary THAs revealed 15 intraopera-tive greater trochanter fractures (4.0%) using a lateral approach. Similar to the reports using the direct anterior approach, the authors suggest increased soft tissue tension and resultant avulsion during femoral preparation as the cause of the fractures.
There are some central tenets that can be applied in order to reduce the risk of intraoperative fracture. Examin-ation of soft tissue tension before and after leg manipula-tion with any surgical approach can help reduce the rate of fracture. Soft tissue releases, such as the short external rotators for improved femoral exposure with a direct anter-ior approach, should be a part of every surgeon’s reper-toire. Finally, surgeon experience with novel techniques undoubtedly plays a role in reducing the incidence of intraoperative complications.35,37,38
Nerve injury
The prevalence of nerve injuries during THA has been reported to be around 1%.39 Nerve injury can occur under several different circumstances, including direct trauma
during dissection or placement of devices, such as wires or acetabular screws; retraction; thermal injury from methyl-methacyrlate; compression due to hematoma; leg length-ening; and component positioning.40 Commonly injured nerves include the superior gluteal, lateral femoral cutane-ous, sciatic and femoral nerves.
A superior gluteal or femoral nerve palsy is a potential complication following a direct lateral approach to the hip. The superior gluteal nerve passes between the gluteus medius and minimus muscles approximately 5 cm proximal to the greater trochanter.41 Retrospective and prospective studies suggest an incidence of 2.2%–42.5% for superior gluteal nerve injuries following reconstructive hip proced-ures using a direct lateral approach.41–44 This nerve palsy can lead to abductor insufficiency and poorer functional outcomes following THA; fortunately, many cases improve spontaneously. One study reported persistent electromyo-graphic abnormalities in the gluteus medius 1 year postop-eratively in 3 of 40 patients who underwent THA through a lateral approach. Interestingly, only 1 of these patients demonstrated clinical signs of abductor insufficiency (i.e., Trendelenburg sign) at latest follow-up.44
Neurapraxia of the lateral femoral cutaneous nerve can occur in 15%–80% of patients undergoing THA through a direct anterior approach45,46 owing to the nerve’s variable course around the anterior superior iliac spine and as it crosses the surgical plane at the sartorial-TFL plane more distally.6,47 Most of these neuropraxic injuries resolve with-out any long-term sequelae.6,8 A postoperative neuroma is a potential complication leading to increased pain, although this complication is rarely reported in the literature.46,48
The risk of sciatic nerve injury is greater during the posterior approach.49 Schmalzried and colleagues40 reviewed more than 3000 THAs and found an incidence of isolated sciatic nerve palsy of 1.3%. In most patients, sen-sory or motor deficits resolved spontaneously. Another study identified 14 sciatic motor nerve palsies in a cohort of more than 27 000 patients who underwent primary THA. Nine of these 14 patients had either partial or no recovery of residual motor deficits at a mean of 83 months postoperatively.49 Therefore, preserving the integrity of the nerve in order to optimize patient outcomes following THA cannot be understated.50
The femoral nerve is at risk with over-rigorous place-ment of soft tissue retractors over the anterior aspect of the acetabulum for all approaches. The rate of femoral nerve palsies for THA ranges from 0.1% to 2.4%.39,51 Mulliken and colleagues52 did not identify any femoral nerve injuries in 770 consecutive patients who underwent THA with a direct lateral approach. The highest reported rate of femoral nerve palsy using a direct lateral approach was that in a study by Simmons and colleagues.53 They reported 10 palsies in 440 hips, with all patients experiencing a full functional recovery 1 year postoperatively. Matta and colleagues6 reported 1 femoral nerve palsy in 494 patients. In all cases
surg-petis.indd 135 2015-03-10 11:12 AM

REVUE
136 J can chir, Vol. 58, No 2, avril 2015
reported in the literature, the palsy was attributed to retractor placement over the anterior rim of the acetabulum.
Review of clinical outcomes
Lateral versus posterior approach
The direct lateral and posterior approaches are fundamentally similar in that they are both musclesplitting ap proach es to the hip.12,13 However, as illustrated earlier, the surgical anatomy and potential complications differ between these approaches, which can influence patient outcomes.
The most important determinants of a successful THA are based on its goals of treatment: mitigation of pain, improved quality of life and restoration of function.54 Barber and colleagues55 prospectively followed for 2 years 28 patients undergoing direct posterior and 21 undergoing direct lateral THA, each performed by a single surgeon. Both groups had similar improvements on the Harris Hip Score (HHS) at the 2year followup and had no observable differences in dislocations or in the incidence of a Trendelenburg gait.
A more recent prospective study56 randomly assigned 60 patients to undergo THA through either a posterior or lateral approach. The primary end point was the HHS at the 12week followup. The authors also captured data from the Western Ontario and McMaster Osteoarthritis Index (WOMAC) and the ShortForm 36 (SF36) questionnaires as well as information on complications, such as dislocations and periprosthetic fractures. Both approaches showed similar improvements across the HHS, WOMAC and SF36 questionnaires at multiple time points up to and including 12 weeks postoperatively. The rate of dislocation and fracture did not differ significantly between the groups.
A common comparator between the posterior and lateral approach is the incidence of abductor insufficiency. Several studies have suggested the direct lateral approach has an increased incidence of abductor insufficiency following THA.15,24,30,56 The reported incidence varies from 0% to 16% for the posterior approach and from 4% to 20% for the direct lateral approach.15 However, there is tremendous heterogeneity in the methods used to diagnose abductor insufficiency in many of these studies. Many studies use subjective findings, such as the presence of Trendelenburg gait or sign or lateral trochanteric pain, which may lead to poor interrater reliability, to make the diagnosis. Magnetic resonance imaging (MRI) is becoming a popular method for assessing soft tissue pathology following THA.57–60 Several studies have shown that metal suppression pulsed MRI sequences can identify abductor damage in patients with symptomatic abductor tears following THA.59–61 Future prospective studies using MRI to assess soft tissue integrity postoperatively will provide a more objective measure of the incidence of abductor tears.
Anterior versus lateral approach
The direct anterior approach is increasing in popularity and is the preferred surgical approach of 10% of orthopedic surgeons performing THA.4 Reduced blood loss, earlier functional recovery, low dislocation rates and shorter stays in hospital have been attributed to the muscle sparing properties of the anterior approach.6 The literature also suggests that minimizing muscle damage during surgery is a reason for patients to choose particular surgeons who practise musclesparing techniques.37 Thus, several recent studies have compared the direct anterior approach to both the direct lateral and posterior approaches.
From 2006 to 2009, Alecci and colleagues62 retrospectively reviewed peri and intraoperative outcomes of THAs performed through either a direct lateral (n = 198) or direct anterior (n = 221) approach. The mean duration of surgery was 8 minutes longer in the direct anterior group, which was a statistically significant difference between the groups. The direct lateral group experienced increased perioperative blood loss and blood transfusions compared with the direct anterior group. Finally, length of stay in hospital was reduced significantly from 10 to 7 days when a THA was performed through an anterior approach.
A similar study by Restrepo and colleagues63 randomly assigned 100 patients to either the direct anterior or lateral approach to THA. Interestingly, the authors found no signifi cant differences in duration of surgery, blood loss, need for blood transfusions or length of stay in hospital between the 2 groups. The authors also examined patient outcome measures. The direct anterior group outperformed the direct lateral group on the HHS, SF36 and WOMAC questionnaires at 6 weeks postoperatively. However, these significant differences in clinical outcomes were abated when revisited at 2 years postoperatively. This study suggests that the direct anterior approach may be associated with greater early postoperative improvements in patientreported outcomes than the direct lateral approach.
Earlier discharge from hospital may be associated with better pain mitigation after surgery. Goebel and colleagues64 retrospectively reviewed pain perception using a visual analogue scale (VAS), consumption of pain medication and length of stay in hospital in 200 patients undergoing either an anterior or lateral approach to THA. There was a significant reduction in perceived pain and consumption of pain medication in the direct anterior group during the first 24 hours postoperatively. The direct anterior group spent an average of 3 fewer days in hospital than the direct lateral group. Again, improved pain mitigation and earlier discharge were attributed to the musclesparing properties of the anterior approach. However, the accuracy of these data are limited by the retrospective study design and by pain assessment using a VAS and multiple different assessors.
There may be anatomic pathology that can explain the discrepancy in perceived pain between the groups. Bremer
surg-petis.indd 136 2015-03-10 11:12 AM

REVIEW
Can J Surg, Vol. 58, No. 2, April 2015 137
and colleagues65 obtained an MRI 1 year postoperatively in 50 patients who underwent THA through either a direct anterior or lateral approach. The authors noted significant increases in the number of abductor tears or detachments, greater trochanteric fluid collections, gluteus medius tendin osis and fatty atrophy of the abductor muscles in the direct lateral group. The abductor complex is a pain generator following the direct lateral approach and may explain differences in early pain perception between the groups.29 However, a limitation of the study by Bremer and colleagues is the absence of a clinical outcome measures assessment. They did not obtain a preoperative MRI, which could have identified patients with evidence of abductor pathology before the procedure, a common finding in patients with hip arthritis.33 Future research should compare clinical outcomes and findings on advanced im aging modalities to explain discrepancies in pain and functional outcomes.
Anterior versus posterior approach
Several studies have compared the anterior and posterior approaches, with recent literature examining the extent of muscle damage incurred by either approach. A prospective randomized trial by Barrett and colleagues66 compared 43 direct anterior and 44 direct posterior approaches to THA. The primary end point was the ability to climb stairs and walk unlimited distances, as assessed with the HHS at 6 weeks, 3 months, 6 months and 12 months postoperatively. The authors also captured intraoperative data, including total duration of surgery, and postoperative data, including length of stay in hospital. The total duration of surgery was on average 23.8 minutes longer in the direct anterior than the direct posterior group. The mean length of stay in hospital was 2.28 days for the direct anterior group and 3.02 days for the direct posterior group. At the 6week followup visit, significantly more patients were walking limitlessly, were able to climb stairs normally and had a higher total HHS in the direct anterior than the direct posterior group. These differences dissipated by the 3month mark and remained insignificant up to and including 1 year postoperatively. These results support the claim that the direct anterior approach provides earlier restoration of function after THA.
One of the purported benefits of earlier return of function is earlier discharge from hospital. Martin and colleagues67 retrospectively reviewed 41 direct anterior and 47 direct posterior approaches for THA. Length of stay in hospital was significantly shorter for the anterior than the posterior group (2.9 d v. 4.0 d). The mean duration of surgery was significantly longer with the anterior than the posterior approach (141 min v. 114 min). Both groups performed similarly on the SF36 and WOMAC clinical outcome measures at the 6month followup. This study was limited by selection bias, as the mean body mass index (BMI) was significantly higher in the posterior than the
anterior group (34.1 v. 28.5). Patients with elevated BMI (> 40) were told that there was a greater risk of wound complications associated with an anterior approach and opted to undergo a posterior approach. Elevated BMI has become a relative contraindication to an anterior approach in our institution. A statistically significant difference in BMI between study cohorts is an important confounder, as obese patients require more assistance with early mobilization, thereby influencing the difference in length of stay between the groups. In the study by Martin and colleagues,67 the earlier discharge from hospital was attributed to earlier mobilization owing to the musclesparing properties of the anterior approach.
There is considerable interest in the degree of muscle damage sustained during surgical approaches to the hip. An interesting study by Bergin and colleagues68 compared various blood markers indicative of muscle damage in patients undergoing THA through either a direct anterior or posterior approach. This methodology has been used previously to justify the use of tissuesparing techniques, such as laparoscopy in other surgical subspecialties.69,70 The investigators measured pre and postoperative values of various acute phase reactant proteins, such as creatine kinase (CK), C reactive protein (CRP), interleukin (IL)6, tumour necrosis factor (TNF)α and IL1 in 57 patients undergoing THA. They found a significant increase in CK in the posterior approach group compared with the anterior approach group immediately following the procedure as well as cumulatively 2 days after THA. The other acute phase reactants did not change significantly between the groups.68 However, the duration of surgery was longer in the posterior approach than the anterior approach group (mean 118 min v. 78 min). A more prolonged period of immobilization on the operating room table could have contributed to the accumulation of additional serum CK.71 Serum CK clearance also depends on renal function,72 which was not accounted for in the study by Bergin and colleagues.68
Another study73 examined the extent of gluteus medius/minimus, TFL, rectus femoris and short external rotator muscle damage in THAs performed on 12 cadaveric hips (6 direct anterior and 6 direct posterior approaches). Minimal damage was sustained to the gluteus medius muscle with both approaches. The posterior approach caused more damage to the gluteus minimus muscle than the anterior approach (18% v. 8.5% of the mean surface area). The short external rotators were released in all posterior approach specimens and were damaged in 50% of the anterior approach specimens to improve visualization of the proximal femur. Using an anterior approach, 31% and 12% of the mean surface area of the TFL and rectus femoris muscles, respectively, was damaged. No damage to either of these muscles was sustained using a posterior approach.73 This study challenges the claim that the anterior approach is truly a musclesparing approach. Future studies using gait analysis could elicit the clinical effects of this muscle damage.
surg-petis.indd 137 2015-03-10 11:12 AM

REVUE
138 J can chir, Vol. 58, No 2, avril 2015
ConClusion
Surgical approach in THA is an area of debate among orthopedic surgeons. This review has demonstrated that the anterior, lateral and posterior approaches each have unique advantages and disadvantages. High-quality clinical compar-isons among the approaches are lacking in the literature; therefore, surgeon preference is likely more a function of training and anecdotal success. The surgical approaches dis-cussed all enable performance of a safe and clinically effica-cious THA; therefore, we recommend that surgeons choose the approach with which they have the most experience and ease. Future research should elicit the long-term implica-tions of surgical approach on clinical outcomes, restoration of function (i.e. gait analysis) and health economics.Affiliations: From the Division of Orthopedic Surgery, London Health Sciences Centre, University Hospital, London, Ont., Canada
Competing interests: E. Vasarhelyi is a consultant with DePuy and Smith and Nephew and has received institutional and research support from DePuy, Smith and Nephew and Stryker. No other competing interests declared.
Contributors: All authors designed the study and analyzed the data. S. Petis and E. Vasarhelyi acquired the data. S. Petis and J. Howard wrote the article, which all authors reviewed and approved for publication.
References
1. Charnley J. Arthroplasty of the hip. A new operation. Lancet 1961;1:1129-32.
2. Information CIfH. Hip and knee replacements in Canada: 2012-2013 Quick Stats 2013. Available: www.cihi.ca/CIHI-ext-portal/xlsx /internet/STATS_CJRR2012-2013_EN (accessed 2015 Feb. 12).
3. Light TR, Keggi K. Anterior approach to hip arthroplasty. Clin Orthop Relat Res 1980; 152:255-60.
4. Chechik O, Khashan M, Lador R, et al. Surgical approach and pros-thesis fixation in hip arthroplasty worldwide. Arch Orthop Trauma Surg 2013;133:1595-600.
5. Siguier T, Siguier M, Brumpt B. Mini-incision anterior approach does not increase dislocation rate: a study of 1037 total hip replace-ments. Clin Orthop Relat Res 2004; 426:164-73.
6. Matta JM, Shahrdar C, Ferguson T. Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res 2005;441:115-24.
7. Kennon RE, Keggi J, Wetmore R, et al. Total hip arthroplasty through a minimally invasive anterior surgical approach. J Bone Joint Surg Am 2003;85-A:39-48.
8. Nakata K, Nishikawa M, Yamamoto K, et al. A clinical comparative study of the direct anterior with mini-posterior approach: two con-secutive series. J Arthroplasty 2009;24:698-704.
9. Mayr E, Nogler M, Benedetti M, et al. A prospective randomized assessment of earlier functional recovery in THA patients treated by minimally invasive direct anterior approach: a gait analysis study. Clin Biomech (Bristol, Avon) 2009;24:812-8.
10. Horne PH, Olson S. Direct anterior approach for total hip arthro-plasty using the fracture table. Curr Rev Musculoskelet Med 2011; 4:139-45.
11. Lovell TP. Single-incision direct anterior approach for total hip arthroplasty using a standard operating table. J Arthroplasty 2008; 23:64-8.
12. Hoppenfeld S, DeBoer P, Buckley R. Surgical exposures in orthopaedics: the anatomic approach. Philidelphia, PA: Lippincott Williams and Wilkins; 2009.
13. Hardinge K. The direct lateral approach to the hip. J Bone Joint Surg Br 1982;64:17-9.14. Burnett R. Total hip arthroplasty: techniques and results. BCMJ
2010;52:455-64.15. Masonis JL, Bourne R. Surgical approach, abductor function, and total
hip arthroplasty dislocation. Clin Orthop Relat Res 2002;405:46-53.16. Kwon MS, Kuskowski M, Mulhall K, et al. Does surgical approach
affect total hip arthroplasty dislocation rates? Clin Orthop Relat Res 2006;447:34-8.
17. Masterson EL, Masri B, Duncan C. Surgical approaches in revision hip replacement. J Am Acad Orthop Surg 1998;6:84-92.
18. Vanhegan IS, Malik A, Jayakumar P, et al. A financial analysis of revi-sion hip arthroplasty: the economic burden in relation to the national tariff. J Bone Joint Surg Br 2012;94:619-23.
19. Singh JA, Lewallen D. Operative diagnosis for revision total hip arthroplasty is associated with patient-reported outcomes (PROs). BMC Musculoskelet Disord 2013;14:210.
20. Phillips CB, Barrett J, Losina E, et al. Incidence rates of dislocation, pul-monary embolism, and deep infection during the first six months after elective total hip replacement. J Bone Joint Surg Am 2003;85-A:20-6.
21. Sariali E, Leonard P, Mamoudy P. Dislocation after total hip arthro-plasty using Hueter anterior approach. J Arthroplasty 2008;23:266-72.
22. Demos HA, Rorabeck C, Bourne R, et al. Instability in primary total hip arthroplasty with the direct lateral approach. Clin Orthop Relat Res 2001; (393):168-80.
23. Chiu FY, Chen C, Chung T, et al. The effect of posterior capsulor-rhaphy in primary total hip arthroplasty: a prospective randomized study. J Arthroplasty 2000;15:194-9.
24. Jolles BM, Bogoch E. Posterior versus lateral surgical approach for total hip arthroplasty in adults with osteoarthritis. Cochrane Database Syst Rev 2006;CD003828.
25. Ho KW, Whitwell G, Young S. Reducing the rate of early primary hip dislocation by combining a change in surgical technique and an increase in femoral head diameter to 36mm. Arch Orthop Trauma Surg 2012;132:1031-6.
26. Sierra RJ, Raposo J, Trousdale R, et al. Dislocation of primary THA done through a posterolateral approach in the elderly. Clin Orthop Relat Res 2005;441:262-7.
27. Pellicci PM, Potter H, Foo L, et al. MRI shows biologic restoration of posterior soft tissue repairs after THA. Clin Orthop Relat Res 2009;467:940-5.
28. Pellicci PM, Bostrom M, Poss R. Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop Relat Res 1998;355:224-8.
29. Lachiewicz PF. Abductor tendon tears of the hip: evaluation and management. J Am Acad Orthop Surg 2011;19:385-91.
30. Iorio R, Healy W, Warren P, et al. Lateral trochanteric pain follow-ing primary total hip arthroplasty. J Arthroplasty 2006;21:233-6.
31. Valente G, Taddei F, Jonkers I. Influence of weak hip abductor mus-cles on joint contact forces during normal walking: probabilistic modeling analysis. J Biomech 2013;46:2186-93.
32. Miozzari HH, Dora C, Clark J, et al. Late repair of abductor avulsion after the transgluteal approach for hip arthroplasty. J Arthroplasty 2010;25:450-7.e1.
33. Howell GE, Biggs R, Bourne R. Prevalence of abductor mechanism tears of the hips in patients with osteoarthritis. J Arthroplasty 2001;16:121-3.
34. Kiyama T, Naito M, Shinoda T, et al. Hip abductor strengths after total hip arthroplasty via the lateral and posterolateral approaches. J Arthroplasty 2010;25:76-80.
35. Jewett BA, Collis D. High complication rate with anterior total hip arthroplasties on a fracture table. Clin Orthop Relat Res 2011;469: 503-7.
36. Hendel D, Yasin M, Garti A, et al. Fracture of the great trochanter during hip replacement: a retrospective analysis of 21/372 cases. Acta Orthop Scand 2002;73:295-7.
surg-petis.indd 138 2015-03-10 11:12 AM

REVIEW
Can J Surg, Vol. 58, No. 2, April 2015 139
37. Dosanjh S, Matta J, Bhandari M. The final straw: a qualitative study to explore patient decisions to undergo total hip arthroplasty. Arch Orthop Trauma Surg 2009;129:719-27.
38. Woolson ST, Pouliot M, Huddleston J. Primary total hip arthro-plasty using an anterior approach and a fracture table: short-term results from a community hospital. J Arthroplasty 2009;24:999-1005.
39. Schmalzried TP, Noordin S, Amstutz H. Update on nerve palsy associated with total hip replacement. Clin Orthop Relat Res 1997; 344:188-206.
40. Schmalzried TP, Amstutz H, Dorey F. Nerve palsy associated with total hip replacement: risk factors and prognosis. J Bone Joint Surg Am 1991;73:1074-80.
41. Khan T, Knowles D. Damage to the superior gluteal nerve during the direct lateral approach to the hip: a cadaveric study. J Arthroplasty 2007;22:1198-200.
42. Oldenburg M, Muller R. The frequency, prognosis and significance of nerve injuries in total hip arthroplasty. Int Orthop 1997;21:1-3.
43. Ramesh M, O’Byrne J, McCarthy N, et al. Damage to the superior gluteal nerve after the Hardinge approach to the hip. J Bone Joint Surg Br 1996;78:903-6.
44. Picado CH, Garcia F, Marques W. Damage to the superior gluteal nerve after direct lateral approach to the hip. Clin Orthop Relat Res 2007;455:209-11.
45. Goulding K, Beaule P, Kim P, et al. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res 2010;468:2397-404.
46. Bhargava T, Goytia R, Jones L, et al. Lateral femoral cutaneous nerve impairment after direct anterior approach for total hip arthro-plasty. Orthopedics 2010;33:472.
47. Ropars M, Morandi X, Huten D, et al. Anatomical study of the lat-eral femoral cutaneous nerve with special reference to minimally invasive anterior approach for total hip replacement. Surg Radiol Anat 2009;31:199-204.
48. Grossman MG, Ducey S, Nadler S, et al. Meralgia paresthetica: diagnosis and treatment. J Am Acad Orthop Surg 2001;9:336-44.
49. Farrell CM, Springer B, Haidukewych G, et al. Motor nerve palsy following primary total hip arthroplasty. J Bone Joint Surg Am 2005;87:2619-25.
50. DeHart MM, Riley L Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-11.
51. Fox AJ, Bedi A, Wanivenhaus F, et al. Femoral neuropathy following total hip arthroplasty: review and managment guidelines. Acta Orthop Belg 2012;78:145-51.
52. Mulliken BD, Rorabeck C, Bourne R, et al. A modified direct lateral appraoch in total hip arthroplasty: a comprehensive review. J Arthroplasty 1998;13:737-47.
53. Simmons C, Izant T, Rothman R, et al. Femoral neuropathy follow-ing total hip arthroplasty: anatomic study, case reports, and literature review. J Arthroplasty 1991;6:S57-66.
54. Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet 2007;370:1508-19.
55. Barber TC, Roger D, Goodman S, et al. Early outcome of total hip arthroplasty using the direct lateral vs the posterior surgical approach. Orthopedics 1996;19:873-5.
56. Witzleb WC, Stephan L, Krummenauer F, et al. Short-term outcome after posterior versus lateral surgical approach for total hip arthro-plasty: a randomized clinical trial. Eur J Med Res 2009;14:256-63.
57. Potter HG, Nestor B, Sofka C, et al. Magnetic resonance imaging after total hip arthroplasty: evaluation of periprosthetic soft tissue. J Bone Joint Surg Am 2004;86-A:1947-54.
58. Potter HG, Foo L, Nestor B. What is the role of magnetic resonance imaging in the evaluation of total hip arthroplasty? HSS J 2005;1:89-93.
59. Müller M, Thotz S, Springer I, et al. Randomized controlled trial of abductor muscle damage in relation to the surgical approach for pri-mary total hip replacement: minimally invasive anterolateral versus modified direct lateral approach. Arch Orthop Trauma Surg 2011; 131:179-89.
60. Pfirrmann CW, Notzli H, Dora C, et al. Abductor tendons and muscles assessed at MR imaging after total hip arthroplasty in asymptomatic and symptomatic patients. Radiology 2005;235: 969-76.
61. Twair A, Ryan M, O’Connell M, et al. MRI of failed total hip replace-ment caused by abductor muscle avulsion. AJR Am J Roentgenol 2003;181:1547-50.
62. Alecci V, Valente M, Crucil M, et al. Comparison of primary total hip replacements performed with a direct anterior versus the standard lat-eral approach: perioperative findings. J Orthop Traumatol 2011; 12:123-9.
63. Restrepo C, Parvizi J, Pour A, et al. Prospective randomized study of two surgical approaches for total hip arthroplasty. J Arthroplasty 2010;25:671-9.e1.
64. Goebel S, Steinert A, Schillinger J, et al. Reduced post-operative pain in total hip arthroplasty after minimal-invasive anterior approach. Int Orthop 2012;36:491-8.
65. Bremer AK, Kalberer F, Pfirrmann C, et al. Soft-tissue changes in hip abductor muscles and tendons after total hip replacement: com-parison between the direct anterior and the transgluteal approaches. J Bone Joint Surg Br 2011;93:886-9.
66. Barrett WP, Turner S, Leopold J. Prospective randomized study of direct anterior vs posterolateral approach for total hip arthroplasty. J Arthroplasty 2013;28:1634-8.
67. Martin CT, Pugely A, Gao Y, et al. A comparison of hospital length of stay and short-term morbidity between the anterior and the pos-terior approaches to total hip arthroplasty. J Arthroplasty 2013;28: 849-54.
68. Bergin PF, Doppelt J, Kephart C, et al. Comparison of minimally invasive direct anterior versus posterior total hip arthroplasty based on inflammation and muscle damage markers. J Bone Joint Surg Am 2011;93:1392-8.
69. Grande M, Tucci G, Adorisio O, et al. Systemic acute-phase response after laparoscopic and open cholecystectomy. Surg Endosc 2002;16:313-6.
70. Suter M, Martinet O, Spertini F. Reduced acute phase response after laparoscopic total extraperitoneal bilateral hernia repair com-pared to open repair with the Stoppa procedure. Surg Endosc 2002; 16:1214-9.
71. Khan FY. Rhabdomyolysis: a review of the literature. Neth J Med 2009;67:272-83.
72. Lappalainen H, Tiula E, Uotila L, et al. Elimination kinetics of myo-globin and creatine kinase in rhabdomyolysis: implications for follow-up. Crit Care Med 2002;30:2212-5.
73. Meneghini RM, Pagnano M, Trousdale R, et al. Muscle damage dur-ing MIS total hip arthroplasty: Smith-Peterson versus posterior approach. Clin Orthop Relat Res 2006;453:293-8.
surg-petis.indd 139 2015-03-10 11:12 AM

DISCUSSIONS IN SURGERY DISCUSSIONS EN CHIRURGIE
140 J can chir, Vol. 58, No 2, avril 2015 ©2015 8872147 Canada Inc.
Is obesity associated with advanced stage or grade of colon cancer?
Population-based studies from Europe have suggested that obesity is associ-ated with more advanced stage colorectal cancer on presentation. Obesity is an even more prevalent issue in North America, but comparable data on asso-ciations with cancer are lacking. We reviewed the cases of 672 patients with colon cancer diagnosed between 2004 and 2008 in the province of Manitoba who underwent surgical resection at a Winnipeg Regional Health Authority–affiliated hospital. We tested if obesity was associated with more advanced cancer stage or grade. On multivariate analysis, after adjusting for age, sex, tumour location and socioeconomic status, we were unable to show any sig-nificant associations between body mass index of 30 or more and advanced stage or grade cancer on presentation. The reasons for the lack of association are likely multifactorial, including the pathophysiology of the disease and process factors, such as screening habits and colonoscopic diagnostic success rates in obese patients.
C olorectal cancer (CRC) is the third most common cancer1 and the sec-ond most frequent cause of cancer-related death among men and women in Western countries.2 There appears to be an obesity-related
risk associated with many cancers. The strongest associations with obesity observed in men include esophageal, thyroid and colon cancer; in women, the strongest associations include endometrial and gall bladder cancer.3 Several authors have proposed that in patients with colon cancer, obesity may be asso-ciated with the formation of advanced adenomatous polyps, its precursor lesion. Siddiqui and colleagues4 found that for every 1-unit increase in body mass index (BMI) above 30, there was a corresponding 1% increase in the fre-quency of finding advanced adenomatous polyps.
More recent literature suggests that obesity may be associated with not only the development of CRC, but also with more advanced cancers on pre-sentation. A prospective population-based study from Sweden by Brändstedt and colleagues,5 which included 28 098 patients, demonstrated an association between obesity and increased risk of more advanced-stage CRC (T3/T4, N1, or M1 disease), especially in men. This association was seen in all anthropo-metric factors, including weight, hip circumference, waist circumference, BMI, and waist:height ratio measurements, except body fat percentage. These authors also found sex-related differences in the association between obesity and expression of various CRC-associated mutations, including catenin, cyclin D1, p53 and microsatellite instability screening status, as well as BRAF and KRAS profiles.6,7
Obesity is an important issue in Canada that is growing at an alarming rate, with a prevalence of 25%, as reported by the Public Health Agency of Canada and the Canadian Institute for Health Information in 2011. How-ever, comparable data sets examining obesity and risk of more advanced CRC in Canadian populations are lacking. We therefore performed a large-scale review of patients undergoing surgery for colon cancer in Manitoba,
Katerina Neumann, MSc, MD Salaheddin M. Mahmud, MD Andrew McKay, MD, MSc Jason Park, MD, MEd Jennifer Metcalfe, MD David J. Hochman, MD
This work was presented in poster format at the Canadian Surgical Forum in Calgary, Alta., in September 2012, and at the Amer-ican Society of Colon and Rectal Surgeons meeting in Phoenix, AZ, in April 2013.
Accepted for publication Sept. 10, 2014
Correspondence to: K. Neumann St. Boniface Hospital Z3048-409 Tache Ave. Winnipeg MB R2H 2A6 [email protected]
DOI: 10.1503/cjs.004414
Summary
obesity-neumann.indd 140 2015-03-10 1:23 PM

DISCUSSIONS IN SURGERY
. Can J Surg, Vol. 58, No. 2, April 2015 141
Canada, investigating the association between BMI and colon cancer stage and grade; the primary outcome was the odds of presenting with higher stage (Stage III/IV), and the secondary outcome was the odds of presenting with higher grade (Grade 3) colon cancer. Our study included 687 patients who underwent surgery for colon cancer in Winnipeg Regional Health Authority (WRHA)–affiliated hospitals between 2004 and 2008. Data were abstracted from the Manitoba Cancer Registry and from the patient charts. Two logistic regression models were built, 1 for testing the risk of having a more advanced stage and 1 for having a higher grade of tumour. In our cohort, 358 (53%) patients had stage I-II disease, and 314 (47%) had higher stage (237 Stage III, 77 Stage IV) disease. Lower grade cancer was found in 545 (81%) patients, while high grade cancer was found in 127 (19%) patients
The mean BMI was 27.9 in the overall cohort (28.1 in those with lower stage and 27.6 in those with higher stage cancers, and 28.0 in those with lower grade and 26.9 in those with higher grade cancers; Fig. 1). On multivariate analysis, after adjusting for age, sex, tumour location and socioeconomic status, we did not find any significant associations between obesity (BMI ≥ 30) and odds of presenting with higher stage (odds ratio [OR] 0.91, 95% confidence interval [CI] 0.64–1.30) or higher grade (OR 0.70, 95% CI 0.43–1.12) disease.
There are several possible reasons for the differences in findings between our study and those of the Swedish study. First, BMI is a labile variable, especially in patients with cancer. It is affected by multiple factors, including individual eating habits, stress, level of physical activity
and the biology of the disease itself. It may be difficult to distinguish between risk factors for advanced disease ver-sus the consequences of progressing disease. It is possible that the cancer itself decreases BMI in some patients, owing to factors such as obstruction-related symptoms or cancer-induced cachexia, even before diagnosis. We chose to use patient BMIs recorded just before surgery as a snapshot for each patient in order to achieve some con-sistency in time points for BMI data collection before the effects of surgery and any adjuvant treatments could play a role. In comparison, the anthropometric factors in the Swedish study were collected prospectively as part of the Mälmo Diet and Cancer Study from a nationwide population-based cohort. The data were thereby col-lected before the diagnosis of cancer, which may be a bet-ter representation of the patients’ true BMI before any cancer effects on body mass. A further limitation to our study, considering the data were reviewed retrospectively, was that we could not verify whether all height and weight measurements were made directly by clinic staff in the preoperative anesthesia data forms as per protocol or whether patient estimates were included. A power calcu-lation estimated the need for 400 of each high and low stage, as well as high and low grade cancers to demon-strate a statistically significant association with obesity, thereby rendering our study underpowered, especially for grade. Finally, we reviewed only patients who underwent surgical resection in order to obtain accurate information on tumour stage and grade from the pathology speci-mens. Other nonsurgical patients with colon cancer, many of whom likely had stage IV disease, were not included, possibly introducing selection bias.
Fig. 1. Mean body mass index of study population based on cancer stage and grade on presentation. Low stage includes Stage I/II. High stage includes Stage III/IV. Low grade includes Grade 1/2. High grade includes Grade 3. Error bars denote standard deviation.
10
20
30
40
Low stage High stage Low grade High grade
Bod
y m
ass
inde
x
obesity-neumann.indd 141 2015-03-10 1:23 PM

DISCUSSIONS EN CHIRURGIE
142 J can chir, Vol. 58, No 2, avril 2015
Even if an association between obesity and more advanced colon cancer could have been demonstrated, as in the Swedish study, the question remains as to whether this association is due to the biology of the disease itself, such as invasiveness and proliferative ability, or other factors related to the processes of care in obese patients. The recent discoveries in associations between sex- specific anthropometric factors and biological activity of CRC cancer with respect to gene expression profiles are certainly intriguing.6,7 Another compelling and perhaps equally contributing theory is that the association is due to process variables, such as patient or practitioner-related screening habits or technical diagnostic success rates that may differ in obese patients. Colon cancer stage and grade at the time of diagnosis are likely a result of multiple factors, including biology of the disease; host characteristics, such as BMI; and diagnostic limitations and variability in patient behaviours relating to screening and frequency of health care visits. Further studies are needed to ascertain whether there is an association between obesity and risk of more advanced cancers. If we can unravel the mechanisms behind such an association, there may be areas to target, including process or bio-logical factors, in improving primary or secondary pre-vention and in the treatment of the disease.
Affiliations: From the Department of Surgery, (Neumann, McKay, Park, Metcalfe, Hochman) and Department of Community Health Sciences (Mahmud), University of Manitoba, Winnipeg, Man.; and Cancer Care Manitoba, Winnipeg, Man. (Mahmud, McKay, Park, Hochman).
Competing interests: None declared.
Contributors: All authors contributed substantially to writing and/or revising and to the conception and design of the manuscript and approved the final version submitted for publication.
References
1. American Cancer Society. Cancer statistics 2009. Available: www .cancer .org (accessed 2014 Dec. 12).
2. Parkin DM, Pisani P, Ferlay J. Global cancer statistics. CA Cancer J Clin 1999;49:33-64.
3. Renehan AG, Tyson M, Egger M, et al. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observa-tional studies. Lancet 2008;371:569-78.
4. Siddiqui A, Pena Sahdala HN, Nazario HE, et al. Obesity is associated with an increased prevalence of advanced adenomatous colon polyps in a male veteran population. Dig Dis Sci 2009;54:1560-4.
5. Brändstedt J, Wangefjord S, Nodin B, et al. Gender, anthropometric factors and risk of colorectal cancer with particular reference to tumour location and TNM stage: a cohort study. Biol Sex Differ 2012;3:23.
6. Brändstedt J, Wangefjord S, Borgquist S, et al. Influence of anthropo-metric factors on tumor biological characteristics of colorectal cancer of men and women: a cohort study. J Transl Med 2013;11:293.
7. Brändstedt J, Wangefjord S, Nodin B, et al. Associations of anthropo-metric factors with KRAS and BRAF mutation status of primary colorectal cancer in men and women: a cohort study. PLoS One 2014;6:1.
Change of addressWe require 6 to 8 weeks’ notice to ensure uninterrupted service. Please send your current mailing label, new address and the effective date of change to:
CMA Member Service Centre
1870 Alta Vista Dr. Ottawa ON K1G 6R7
tel 888 855-2555 or 613 731-8610 x2307 fax 613 236-8864 [email protected]
Changement d’adresseIl nous faut de 6 à 8 semaines d’avis afin de vous assurer une livraison ininterrompue. Veuillez faire parvenir votre étiquette d’adresse actuelle, votre nouvelle adresse et la date de la prise d’effet du changement, à l’attention du
Centre des services aux membres de l’AMC
1870, prom. Alta Vista Ottawa ON K1G 6R7
tél 888 855-2555 ou 613 731-8610 x2307 fax 613 236-8864 [email protected]
obesity-neumann.indd 142 2015-03-10 1:23 PM

DISCUSSIONS IN SURGERY DISCUSSIONS EN CHIRURGIE
©2015 8872147 Canada Inc. Can J Surg, Vol. 58, No. 2, April 2015 143
Supply versus demand: a review of application trends to Canadian surgical training programs
T he Royal College of Physicians and Surgeons of Canada recently reported that 16% of newly graduated specialist physicians are unable to find employment, sparking debate over the supply–demand balance
of specialist physicians across Canada.1 Though this debate remains unre-solved from a societal viewpoint, there is another important, yet rarely dis-cussed perspective, shaping the future of health care in Canada: the graduating medical student entering the workforce.
The supply of Canadian medical graduates has never been higher; there were 2827 graduates in 2014 compared with 1255 graduates in 2002. How-ever, demand for surgical residency positions has declined for more than a decade. Data from the Canadian Resident Matching Service (CaRMS; www .carms.ca/en/data-and-reports) shows that the number of students selecting a surgical specialty as their first choice has dropped to its lowest point since CaRMS began reporting statistics (13.0% in 2014 v. 20.8% in 2002). During the same time period, despite a 260% increase in the number of residency training positions, family medicine experienced an 18.9% average increase in first choice applications. Compare this to urology, which witnessed a 1.2% decrease in first choice applicants, equating to 34 fewer applicants per year in a specialty with only 31 residency training positions nationwide.
Potentially more concerning is that the students currently applying to surgery may be less competitive applicants. The CaRMS data reveal that the average number of unmatched surgical residency positions has been increas-ing over the past 6 years, peaking in 2009 with 27 unmatched surgical resi-dency positions across Canada. The quality of applicants has dropped to the point where programs would rather leave a position unmatched than accept a candidate.
There has been a decrease in interest in our plastic surgery program at the University of Toronto, which has prompted the question: Does this trend affect only our program, only plastic surgery programs across the country, or is it a phenomenon afflicting all surgical programs?
To examine the current status of Canadian surgical training, we analyzed appli-cation trends to the 6 largest surgical specialties (Table 1). We divided the data set
Ryan E. Austin, MD Kyle R. Wanzel, MD, MEd
Accepted for publication Aug. 25, 2014
Correspondence to: Dr. R.E. Austin 149 College St., 5th Floor Toronto ON M5T 1P5 [email protected]
DOI: 10.1503/cjs.006614
Despite increases in medical school enrolment, applications to surgical residency programs in Canada have been in decline over the past decade, with an increasing number of unmatched surgical residency positions. We examined the current status of surgical residency in Canada and analyzed application trends (2002–2013) for sur-gical training programs across Canada. Our findings suggest that most undergradu-ate medical schools across Canada are having difficulty fostering interest in surgical careers. We propose that a lack of adequate early exposure to the surgical specialties during undergraduate training is a critical factor. Moving forward, we must examine how the best-performing institutions and surgical programs have maintained inter-est in pursuing surgical careers and adapt our recruitment methods to both maintain and grow future interest. As Mary Engelbreit said, “If you don’t like something, change it; if you can’t change it, change the way you think about it.”
Summary
supply-austin.indd 143 2015-03-10 11:14 AM

DISCUSSIONS EN CHIRURGIE
144 J can chir, Vol. 58, No 2, avril 2015
in half (2002–07 and 2008–13) and compared averages from these 2 periods. Trends were further analyzed based on the academic institution from which applicants graduated (Appendix, Tables S1 and S2, available at canjsurg.ca).
Unfortunately, there is no pervasive and uniform pattern to surgical applications across Canada (Appendix, Table S1); however, of 78 programs examined, 63% experienced a decrease in first choice applicants. Furthermore, 85% experienced a decrease in at least 3 of 6 surgical specialties, and no institution experienced an increase in the number of first choice applicants for all specialties.
Why does this concerning trend exist? How can we improve?
Though one may presume that future employment concerns are the driving force contributing to this ebb in surgical interest, the literature is inconclusive regarding the impact of job opportunities on career selection. Another theory is that medical graduates today are of a generation increasingly opting for lifestyle-centered careers.2 The current generation (Generation Y, born between 1982 and 2005) has grown up and thrived in a closely supported environment, protected from failure, where teamwork has replaced hierarchy.2 This differs greatly from traditional surgical training, which may deter the Generation Y student from a surgical career. However, the concept of a generation gap is not new. Rohrich3 highlighted many of these same challenges in a discussion on the difficulties of training surgeons from Generation X (born between 1961 and 1981). It seems that any time there is a transition between generations, intergenerational conflict rooted in resistance toward change develops. It is how one bridges this gap that determines success moving forward.
Interestingly, our data set overlaps the transition period from Generation X to Generation Y. One can easily conceive that between 2008 and 2013 the proportion of Generation Y students graduating from medical school was increasing as Generation X numbers decreased. Though convenient to blame the mindset of a new generation of physicians, if this were simply a generational effect one would expect minimal variability among geographic locations and academic institutionws and a more uniform, pervasive pattern.4
Although certainly multifactorial, we believe the key determinant of interest in a surgical career is adequate
exposure. Studies have shown that early exposure to surgical specialties has a positive influence on career choice.5 Unfortunately, in 2010–11 our institution reduced the amount of time that medical students spend on core surgical rotations from 12 to 8 weeks. Alongside duty hour restrictions, call limitations and decreased surgical teaching in medical school, students now receive much less surgical exposure than their predecessors. For example, only 3 hours of teaching is devoted to plastic surgery topics within the current 4-year curriculum at the University of Toronto. It is, therefore, not surprising that plastic surgery at our institution experienced one of the largest overall application decreases nationwide. How can a student become interested in a specialty when the curriculum essentially overlooks it?
Moving forward, the next step would include analyzing surgical teaching curricula at the institutions fostering greater interest in surgical careers to determine what sets them apart. Perhaps there is greater exposure to surgery and more involved surgical role models touting surgery as a rewarding career. Furthermore, we should survey the students themselves to determine their perceived exposure, which can differ from reality if the students lack a thorough understanding of a specialty’s scope of practice. We may also benefit from a better understanding of what students desire from us as surgical educators.
So how can we improve the horizon for surgical training in Canada? While the first step is to admit a problem exists, the next step is for surgeons to develop creative solutions to maintain interest in our specialties. Creativity and progressive thinking is exactly what the fast-paced, multitasking Generation Y student demands. Though seemingly counterintuitive, we must shed the competitive stigma associated with surgical residency before demand drops so low that we become, in essence, obsolete.2
Affiliations: Division of Plastic & Reconstructive Surgery, Department of Surgery, University of Toronto, Toronto, Ont., Canada (Austin, Wanzel), and the Division of Plastic Surgery, St. Joseph’s Health Cen-tre, Department of Surgery, University of Toronto, Toronto, Ont., Canada (Wanzel).
Competing interests: None declared.
Contributors: Both authors contributed substantially to writing and/or revising and to the conception and design of the manuscript and approved the final version submitted for publication.
References
1. Frechette D, Hollenberg D, Shrichand A, et al. What’s really behind Canada‘s unemployed specialists? Too many, too few doctors? Findings from the Royal College’s employment study. Ottawa, Ont.: The Royal College of Physicians and Surgeons of Canada, 2013.
2. Eckleberry-Hunt J, Tucciarone J. The challenges and opportunities of teaching “Generation Y.” J Grad Med Educ 2011;3:458-61.
3. Rohrich RJ. Training the Generation X plastic surgeon: Dispelling the myths? Plast Reconstr Surg 2001;108:1733-4.
4. Schlitzkus LL, Schenarts KD, Schenarts PJ. Is your residency program ready for Generation Y? J Surg Educ 2010;67:108-11.
5. Erzurum VZ, Obermeyer RJ, Fecher A, et al. What influences medical students’ choice of surgical careers. Surgery 2000;128:253-6.
Table 1. National data from the CaRMS match for surgical specialties (comparing 2008–2013 to 2002–2007)
Surgical specialtyΔ Average no. residency
training positionsΔ Average no. first choice
residency applications
General surgery +26.00 –0.8%
Neurosurgery +2.17 –23.1%
Orthopedic surgery +27.50 –4.6%
Otolaryngology +11.50 –16.1%
Plastic surgery +11.17 –15.3%
Urology +11.33 –18.0%
CaRMS = Canadian Resident Matching Service.
supply-austin.indd 144 2015-03-10 11:14 AM

CLINICAL LECTURER OR ASSISTANT PROFESSOR TRANSPLANT AND HEPATOBILIARY SURGERY
St. George Campus (downtown Toronto, Ontario)The Division of General Surgery at the University Health Network and the University of Toronto are inviting applications for a full-time faculty position as an academic Transplant and Hepatobiliary Surgeon, at the level of Clinical Lecturer or Assistant Professor. The effective date of this position is flexible, but preferably by January 1, 2016.
The successful candidate will support the clinical programs and academic mission of University Health Network, which is an academic institution affiliated with the University of Toronto. The University Health Network is comprised of the Toronto General Hospital, Toronto Western Hospital, Princess Margaret Cancer Centre and the Toronto Rehabilitation Institute. UHN is recognized internationally for excellence in patient care, innovation, research and education. The Division of General Surgery currently has 23 surgeons, 10 of whom specialize in transplant and hepatobiliary surgery. Case volumes place the HPB and Transplant programs within the busiest programs in North America.
Responsibilities will include surgery, call (currently as often as one in three), practical and didactic teaching of general surgery junior and senior residents, as well as general surgery oncology and transplant fellows, all of whom are on service continuously. This position entails 20 to 30 hours of didactic undergraduate medical student teaching per year, in addition to supervision of 10 to 20 on-service medical students per year.
The successful candidate will lead a new clinical and research academic initiative focused on the interface between hepatobiliary surgical oncology and abdominal transplantation. The candidate will have demonstrated a strong academic commitment, manifested by prior publications and international collaborations in the field of interest. Evidence of productivity, excellence, and the potential to become an international leader is essential. Start-up research support and mentoring will be provided.
The successful candidate will have completed a residency program in general surgery as well as a hepatobiliary and transplant fellowship. She/He will hold or plan to obtain a graduate degree (Masters or PhD) in Clinical Epidemiology. She/He will have demonstrated outstanding technical skills, the ability to work within a multidisciplinary team and to teach trainees at all levels. She/He will hold, or be eligible for, licensure with the College of Physicians and Surgeons of Ontario.
Starting salary will be between the range of $150,000 - $400,000, commensurate with qualifications and experience. This estimate is based on fee for service billings, in addition to support from the University Health Network Division of General Surgery practice plan.
Please submit a letter of intent, CV and the name of three referees by May 15, 2015, to:
Allan Okrainec, MD, MHPE, FRCSC, FACS Head, Division of General Surgery, UHN
Peter A. Crossgrove, Chair in General Surgery Toronto General Hospital, 10 Eaton, Room 217
200 Elizabeth St., Toronto, Ontario, Canada M5G 2C4
Questions and correspondence should be directed to:
Deborah Wilson Email [email protected] • Tel 416 340-3573
The University of Toronto is strongly committed to diversity within its community and especially welcomes applications from visible minority group members, women, Aboriginal persons, persons with disabilities, members of sexual minority groups, and others who may contribute to the further diversification of ideas. All qualified candidates are encouraged to apply; however, Canadians and permanent residents will be given priority.
For more information about the Faculty of Medicine/Department of Surgery, please visit our home page at http://surgery.utoronto.ca
S-7
67
S-767-IBC-classified ad.indd 1 2015-03-06 1:55 PM
Edwards Lifesciences | edwards.comOne Edwards Way | Irvine, California 92614 USASwitzerland | Japan | China | Brazil | Australia | India
32%in your moderate
to high-risk patients.
YOUcan reduce
post-surgicalcomplications
by
1
Edwards.com/ESR
References:1. Grocott et al. Perioperative increase in global blood flow to explicit defined goals and outcomes after surgery: a Cochrane systematic review.
Br J Anaesth 20132. Giglio MT, Marucci M, Testini M, Brienza N. Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery:
a meta-analysis of randomized controlled trials. Br J Anaesth 2009; 103: 637–463. Dalfino L, Giglio MT, Puntillo F, Marucci M, Brienza N. Haemodynamic goal-directed therapy and postoperative infections: earlier is better.
A systematic review and meta-analysis. Crit Care 2011; 15: R1544. Corcoran T et al. Perioperative Fluid Management Strategies in Major Surgery: A Stratified Meta-Analysis. Anesthesia – Analgesia 2012 Edwards, Edwards Lifesciences, the stylized E logo and Enhanced Surgical Recovery are trademarks of Edwards Lifesciences Corporation. All other trademarks are the property of their respective owners.
© 2014 Edwards Lifesciences Corporation. All rights reserved.
A large body of evidence demonstrates that hemodynamic optimization through Perioperative Goal-Directed Therapy (PGDT), utilizing dynamic parameters which are informative in determining fluid responsiveness, has been shown to reduce post-surgical complications.1-4
randomized controlled trials and
meta-analyses confirmedreduction of risk for AKI, anastomotic leaks,
pneumonia, SSI and UTI.1-4
When evidence inspires action, Edwards Enhanced Surgical Recovery program is here to help you implement PGDT. Your vision for reducing post- surgical complications can be realized in a single procedure, or as part of a larger initiative such as iERAS, ERAS, QIP, etc.
cover-cjsapr15.indd 4 2015-03-10 9:02 AM

CLINICAL LECTURER OR ASSISTANT PROFESSOR TRANSPLANT AND HEPATOBILIARY SURGERY
St. George Campus (downtown Toronto, Ontario)The Division of General Surgery at the University Health Network and the University of Toronto are inviting applications for a full-time faculty position as an academic Transplant and Hepatobiliary Surgeon, at the level of Clinical Lecturer or Assistant Professor. The effective date of this position is flexible, but preferably by January 1, 2016.
The successful candidate will support the clinical programs and academic mission of University Health Network, which is an academic institution affiliated with the University of Toronto. The University Health Network is comprised of the Toronto General Hospital, Toronto Western Hospital, Princess Margaret Cancer Centre and the Toronto Rehabilitation Institute. UHN is recognized internationally for excellence in patient care, innovation, research and education. The Division of General Surgery currently has 23 surgeons, 10 of whom specialize in transplant and hepatobiliary surgery. Case volumes place the HPB and Transplant programs within the busiest programs in North America.
Responsibilities will include surgery, call (currently as often as one in three), practical and didactic teaching of general surgery junior and senior residents, as well as general surgery oncology and transplant fellows, all of whom are on service continuously. This position entails 20 to 30 hours of didactic undergraduate medical student teaching per year, in addition to supervision of 10 to 20 on-service medical students per year.
The successful candidate will lead a new clinical and research academic initiative focused on the interface between hepatobiliary surgical oncology and abdominal transplantation. The candidate will have demonstrated a strong academic commitment, manifested by prior publications and international collaborations in the field of interest. Evidence of productivity, excellence, and the potential to become an international leader is essential. Start-up research support and mentoring will be provided.
The successful candidate will have completed a residency program in general surgery as well as a hepatobiliary and transplant fellowship. She/He will hold or plan to obtain a graduate degree (Masters or PhD) in Clinical Epidemiology. She/He will have demonstrated outstanding technical skills, the ability to work within a multidisciplinary team and to teach trainees at all levels. She/He will hold, or be eligible for, licensure with the College of Physicians and Surgeons of Ontario.
Starting salary will be between the range of $150,000 - $400,000, commensurate with qualifications and experience. This estimate is based on fee for service billings, in addition to support from the University Health Network Division of General Surgery practice plan.
Please submit a letter of intent, CV and the name of three referees by May 15, 2015, to:
Allan Okrainec, MD, MHPE, FRCSC, FACS Head, Division of General Surgery, UHN
Peter A. Crossgrove, Chair in General Surgery Toronto General Hospital, 10 Eaton, Room 217
200 Elizabeth St., Toronto, Ontario, Canada M5G 2C4
Questions and correspondence should be directed to:
Deborah Wilson Email [email protected] • Tel 416 340-3573
The University of Toronto is strongly committed to diversity within its community and especially welcomes applications from visible minority group members, women, Aboriginal persons, persons with disabilities, members of sexual minority groups, and others who may contribute to the further diversification of ideas. All qualified candidates are encouraged to apply; however, Canadians and permanent residents will be given priority.
For more information about the Faculty of Medicine/Department of Surgery, please visit our home page at http://surgery.utoronto.ca
S-7
67
S-767-IBC-classified ad.indd 1 2015-03-06 1:55 PM
Edwards Lifesciences | edwards.comOne Edwards Way | Irvine, California 92614 USASwitzerland | Japan | China | Brazil | Australia | India
32%in your moderate
to high-risk patients.
YOUcan reduce
post-surgicalcomplications
by
1
Edwards.com/ESR
References:1. Grocott et al. Perioperative increase in global blood flow to explicit defined goals and outcomes after surgery: a Cochrane systematic review.
Br J Anaesth 20132. Giglio MT, Marucci M, Testini M, Brienza N. Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery:
a meta-analysis of randomized controlled trials. Br J Anaesth 2009; 103: 637–463. Dalfino L, Giglio MT, Puntillo F, Marucci M, Brienza N. Haemodynamic goal-directed therapy and postoperative infections: earlier is better.
A systematic review and meta-analysis. Crit Care 2011; 15: R1544. Corcoran T et al. Perioperative Fluid Management Strategies in Major Surgery: A Stratified Meta-Analysis. Anesthesia – Analgesia 2012 Edwards, Edwards Lifesciences, the stylized E logo and Enhanced Surgical Recovery are trademarks of Edwards Lifesciences Corporation. All other trademarks are the property of their respective owners.
© 2014 Edwards Lifesciences Corporation. All rights reserved.
A large body of evidence demonstrates that hemodynamic optimization through Perioperative Goal-Directed Therapy (PGDT), utilizing dynamic parameters which are informative in determining fluid responsiveness, has been shown to reduce post-surgical complications.1-4
randomized controlled trials and
meta-analyses confirmedreduction of risk for AKI, anastomotic leaks,
pneumonia, SSI and UTI.1-4
When evidence inspires action, Edwards Enhanced Surgical Recovery program is here to help you implement PGDT. Your vision for reducing post- surgical complications can be realized in a single procedure, or as part of a larger initiative such as iERAS, ERAS, QIP, etc.
cover-cjsapr15.indd 3 2015-03-10 9:02 AM