
Year in Infectious Diseases - Welcome to CCEHS · Year in Infectious Diseases J. Alex Viehman, MD,...
71
Year in Infectious Diseases J. Alex Viehman, MD, Clinical Assistant Professor of Medicine Division of Infectious Disease, University of Pittsburgh Medical Center
Transcript of Year in Infectious Diseases - Welcome to CCEHS · Year in Infectious Diseases J. Alex Viehman, MD,...

Year in Infectious Diseases
J. Alex Viehman, MD, Clinical Assistant Professor of MedicineDivision of Infectious Disease, University of Pittsburgh Medical Center

Disclosures I have no financial disclosures to report
I will not discuss any off-label medication use

Overview New FDA antibiotic approvals for Gram negatives Community acquired pneumonia HIV treatment initiation Vertebral osteomyelitis Intra-abdominal infections Urinary tract infections

New Antibiotics: The Most Urgent Need Multiple recent drug approvals drugs Gram positives
(MRSA, VRE) Tedozlid, Telavancin, Ceftaroline, Dalbavancin, Oritivancin
The biggest threat has been Gram Negative Rods Fewer active drugs More mechanisms of resistance (Porins, Beta-lactamases) Mobile genetic elements (Plasmids)

Nomenclature: KPC and CRE KPC: Klebsiella pneumoniae carbapenemase A specific beta-lactamase (class A)
CRE: Carbapenem-resistant Enterobacteriaceae
There are other mechanisms of carbapenem-resistance
All KPC are CRE, but not all CRE are KPC
Slide adapated from Brian Potoski

CRE
KPC Efflux + porinUncommon
enzymes (IMI, IMP)
Affinity for PBPs
Klebsiella pneumoniae Escherichia coli
Enterobacter cloacae Enterobacter aerogenes (Pseudomonas aeruginosa)
Slide adapated from Brian Potoski

Recent Approvals In the past year, two predominantly gram negative acting
agents have been approved by the FDA Ceftolozane/Tazobactam (UTI/Pyelo, IAI) Ceftazidime/Avibactam (UTI/Pyelo, IAI)
Both are beta-lactam/beta-lactamase combinations
Each agent has one previously approved component (Tazobactam, Ceftazidime) and one new component: Avibactam: Non-beta-lactam, beta-lactamase inhibitor Ceftolozane: Novel antipseudomonal cephalosporin

Clinical Data Ceftazidime/Avibactam Phase II Trial on complicated UTI (Vazquez, Current Medical
Research & Opinion 2012) Phase II Trial on complicated Intra-abdominal
infections (IAI) (Lucasti JAC 2013)
Ceftolozane/Tazobactam Phase III trial on complicated UTI* (Wagenlehner, Lancet 2015) Phase III trial on complicated IAI* (Solomkin, CID
2015) * Published after FDA approval

Intra-abdominal Infections: Ceftaz/Avi Phase II Trial: “Comparative study of the efficacy and
safety of ceftazidime/avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infections in hospitalized adults”
P: IAI with an operation for source control 1: Ceftaz/Avi + Metro 5-14 days C: Mero + placebo 5-14 days O: Clinical Response at “Test of Cure” Resolution or significant reduction of infection 2 week after
last dose, with no further antibitoics or surgeries
Lucasti C et al. JAC 2013: 68 183-1192

Exclusion Abdominal wall abscess, SBO, ischemic bowel prior Abx x72 hours, concurrent infection APACHE II >25, Elevated LFTS, or GFR<50, Prednisone >20/day,CD4<200,
Lucasti C et al. JAC 2013: 68 183-1192

Results ME Population: Clinical response at test of cure Ceftaz/Avi 91.2% (62/68)
Meropenem 93.4% (71/76)
“Study not powered to show non-inferiority”
Lucasti, C et al JAC 2013: 68 183-1192

Ceftazidime/Avibactam: Take home Good efficacy in this trial Except: Wrong bugs… (Mostly carbapenem-sensitive E. coli) Wrong hosts… (severely immunocompromised excluded) Wrong setting… (Lower APACHE II predominated) With controllable infections easily eradiated by an operation
Compare with patients who need this drug Liver transplant recipient in septic shock with abscess due to
KPC Klebsiella pneumoniae
Intra-abdominal Infections: Ceftolozane/Tazobactam
Much larger trial (~800pts) Pts : IAI, Operation/percutaneous drainage Intervention: Ceftolozane/tazo + metronidazole 4-14d Control: Meropenem + placebo 4-14d Outcome: Clinical cure at 24-32 days after therapy end Inclusion: More broad Dx Exclusion: No source control, need for staged repair, GFR < 30
Solomkin J et al. CID 2015;60(10): 1462-71

Analyses Multiple analyses, but primary endpoint was for
Microbiologic Intention to Treat
Powered to be a non-inferiority trial, with non-inferiority (NI) margin of -10% difference in clinical cure
Solomkin, J et al CID 2015;60(10): 1462-71

Results: Solomkin et al
Pseudomonas Clinical Cure: n~30 eachCeftolozane/Tazo: 100% Meropenem: 93.1%
Ceftolozane/Tazobactam: Take Home Phase III trials can often give you better data Non-inferior to meropenem (reasonable NI margin) Suggestion of better clinical efficacy in key pathogens Pseudomonas ESBL
No great data in sick patients (higher APACHE, low GFR)

How to use these agents (2016 Edition)1. Clinical data is difficult to extrapolate- Reasonable indication
for ID consultation if these drugs are considered2. Reserve Ceftazidime/Avibactam for CRE due to KPC Does not work against NDM or other metalo-beta-lactamases Does not work against OXA beta-lactamases in Acinetobacter Not reliable against Carbapenem-R Pseudomonas Do not presume sensitivity (try to get confirmation)
3. Reserve Ceftolozane/Tazobactam for MDR Pseudomonas Do not presume sensitivity (try to get confirmation) For ESBL that remains susceptible to to carbapenem: carbapenem
remains first line beta-lactam
HIV Infection/Treatment Initial trials of HIV treatment focused on treating AIDS or
preventing progression to AIDS Combination ART started in mid 1990s Early 2000s, large RCT called the SMART study CD4 at baseline >350
Is “Drug Conservation” better than continuous ART? Control Arm: ART initiated per guidelines Experimental ARM:
ART start <250 ART stop >350 ART restart <250 again

AIDS events (opportunistic disease) and Non-AIDS events (CV, renal, and hepatic) predominated in the interrupted treatment group
Conclusion: “The drugs may be bad for you, but the virus is worse”The Strategies for Management of Antiretroviral Therapy (SMART) Study Group. N Engl J Med 2006;355:2283-2296.

The question remained: When is the best time to start ART?
START Study Initiated in 2009 Multinational trial to evaluate early vs delayed ART initiation 1:1 Randomized Controlled Trial
Patients: HIV +, treatment naïve, CD4 >500 Intervention: ART at study enrollment Control: Defer ART until CD4 <350 Outcome: Combined serious AIDS & non-AIDS events Serious AIDS events: AIDS defining illness or Death from AIDS Serious Non-AIDS events: MI/stent, CVA, ESRD, ESLD, Non-
AIDS Cancer, or Death (non-AIDS)

Interval Developments 2011- HPTN 052:
Serodiscordant couples randomized to early ART had decreased transmission to partners “Treatment as Prevention
Era” 2012- US HHS treatment
guidelines changed: Treat at >500 CD4 cells (B-
III recommendation) May 2015- Early
termination of START Trial
Cohen MS et al. N Engl J Med 2011;365:493-505

May 2015 Early Termination
August 2015 Publication of results
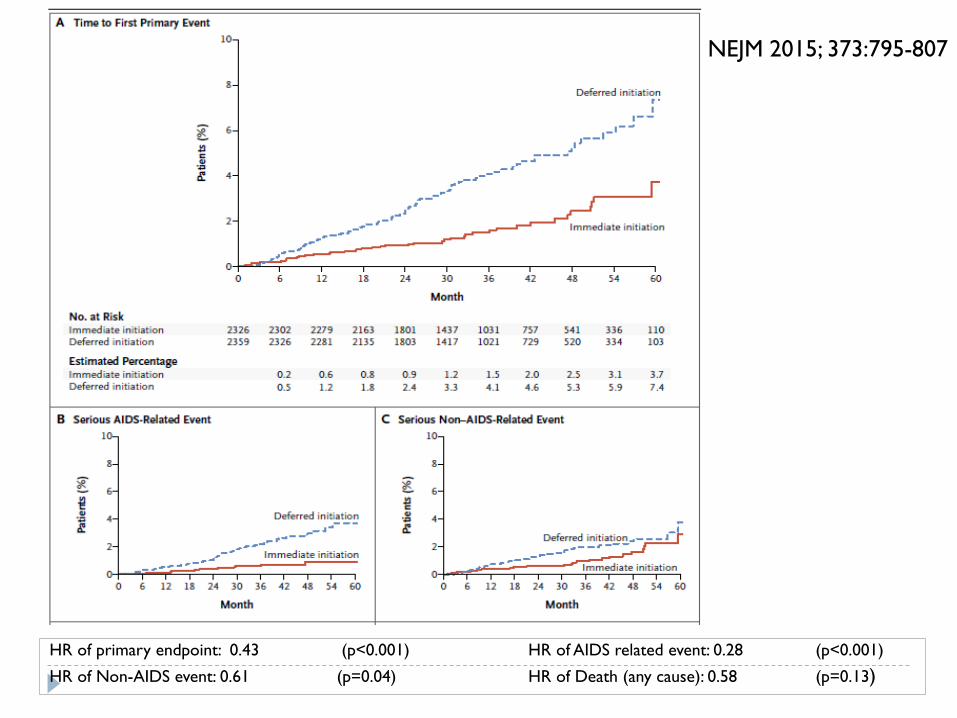
NEJM 2015; 373:795-807
HR of primary endpoint: 0.43 (p<0.001) HR of AIDS related event: 0.28 (p<0.001)
HR of Non-AIDS event: 0.61 (p=0.04) HR of Death (any cause): 0.58 (p=0.13)

Implications Both AIDS and non-AIDS complications decreased by early
ART Mortality difference not shown (p=0.13)
Only median 2.8 years of follow-up (early termination)
Strong data now exists to treat all HIV patients early To prevent disease progression To prevent transmission (previous studies)
International guidelines will likely change Largest benefit still with lower CD4 Challenges in resource-limited settings
Ethical implications Clinical trials continuation after standard-of-care changes How else would we get the best data?

Pneumonia Medical Student Question: What causes Community-
Acquired Pneumonia (CAP) ?
Answer: Streptococcus pneumoniae and some other stuff
In 2016 does this hold true?

Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults
Seema Jain, M.D., Wesley H. Self, M.D., M.P.H., Richard G. Wunderink, M.D., Sherene Fakhran, M.D., M.P.H., Robert Balk, M.D., Anna M. Bramley, M.P.H., Carrie
Reed, Ph.D., Carlos G. Grijalva, M.D., M.P.H., Evan J. Anderson, M.D., D. Mark Courtney, M.D., James D. Chappell, M.D., Ph.D., Chao Qi, Ph.D., Eric M. Hart, M.D., Frank Carroll, M.D., Christopher Trabue, M.D., Helen K. Donnelly, R.N., B.S.N., Derek
J. Williams, M.D., M.P.H., Yuwei Zhu, M.D., Sandra R. Arnold, M.D., Krow Ampofo, M.D., Grant W. Waterer, M.B., B.S., Ph.D., Min Levine, Ph.D., Stephen Lindstrom, Ph.D., Jonas M. Winchell, Ph.D., Jacqueline M. Katz, Ph.D., Dean
Erdman, Dr.P.H., Eileen Schneider, M.D., M.P.H., Lauri A. Hicks, D.O., Jonathan A. McCullers, M.D., Andrew T. Pavia, M.D., Kathryn M. Edwards, M.D., Lyn
Finelli, Dr.P.H., for the CDC EPIC Study Team
N Engl J MedVolume 373(5):415-427
July 30, 2015

Community-Acquired Pneumonia (EPIC) Active Population-Based Surveillance Cohort-type study
Goal: Define CAP- etiology + epidemiology Setting: 3 Hospitals in Chicago and 2 in Nashville Timeframe: 1/2010 through 6/2012 Patients: Hospitalized Fever/hypothermia; Leukopenia/Leukocytosis; AMS (surrogate) Acute respiratory illness: Cough/CP/SOB/Respiratory failure CXR: Consistent with PNA <48 hours of admission
Exclusions: HAP/HCAP Nursing home residents Prior 28d hospital (90d if immunocompromised) Clear other infection/diagnosis CF, Cancer + neutropenia, SOT/SCT (90d) or GVHD, HIV CD4<200
Jain, S et al, NEJM 2015 373(5):415-427

What did they test? (CDC testing) Most patients: Blood cultures Urinary Antigens: S. pneumoniae/L. pneumophila NP/OP PCR swabs (Viruses/Chlamydophila/Mycoplasma) Sputum for culture (attempted) and L. pneumophila PCR
Some patients: Pleural fluid PCR for most bacteria (GNRs, Strep/Staph) BAL cultures Paired serum serologies (respiratory viruses)
Jain, S et al, NEJM 2015 373(5):415-427

Jain, S et al, NEJM 2015 373(5):415-427

Pathogen Detection among U.S. Adults with Community-Acquired Pneumonia Requiring Hospitalization, 2010–2012.
Jain, S et al, NEJM 2015 373(5):415-427

Makes ID Physicians Feel Sad and Scared! Sad: Diagnostics not where they need to be
Scared: Lack of data breed uncertainty Uncertainty breeds anxiety Anxiety breeds “all patients on vancomycin and piperacillin-
tazobactam with no stop date syndrome” (rampant empiricism)
Rampant empiricism breeds resistance

The Missing 62 Percent (My Opinion) Most likely sources of the missing 62% Wrong diagnosis (CHF, COPD exacerbations/bronchitis etc.) Poor specimens/missing specimens
NP/OP submitted from 98% Blood cultures from 91% Urine Ag from 85% 41% had a sputum submitted 12% had a high-quality sputum submitted
Diagnostics not great- may be improving (more later) Pre-treatment with antibiotics (next slide)

Supplementary Data
Jain, S et al Accessed NEJM.org
Opposing View A recent study used 2 different bundle approaches Blood/sputum cultures Nasal Influenza + S. pneumoniae/S. aureus PCRs Urine/Serum Ag for S. pneumoniae/L. pneumophila Serum procalitonin
Commercial Nasal Multiplex PCR (FilmArray) (included atypical bacteria)
OR a Nasal “Homebrew” Viral PCR panel
Gelfer G et al Diagnostic Microbiology and Infectious Disease 2015 Dec;83(4):400-6

Pathogen Identification: Gelfer et al
Diagnostic Microbiology and Infectious Disease 2015 Dec;83(4):400-6
• Much smaller sample size• Fewer “No Pathogen Identified”• Despite lower pathogen ID, commercial PCR was favorable due to turn around time

Take Home: CAP in 2016 and Beyond Streptococcus pneumoniae may be less common than before Likely due to vaccinating children with a good vaccine
PCV7 ~2000, PCV 13 ~ 2008 Whether vaccinating adults > 65 will make a difference is unclear
Pre-treatment with antibiotics and poor sputum specimen collection may cause us to underdiagnose bacterial causes
Viruses cause a significant amount of classic pneumonia Rhinovirus (!) Procalcitonin testing may reassure us
Newer diagnostics (non-culture related) may help Implementation/bundling strategies required to make this useful
(keep patients safe, decrease antibiotic use, optimize costs, etc.)

Vertebral Osteomyelitis Duration of antibiotics not well studied in the past Considerable variability in practice French RCT (open label) designed to test duration 71 hospitals participated
P: Acute OM of spine due to bacteria Microbiologically confirmed Hardware or AFB/fungus excluded
I: 6 weeks of antibiotics (IV and po) C: 12 week of antibiotics (IV and po) O: Cure at 1 year (No fever/pain and low CRP); QOL secondary outcome
Analysis: Intention to treat Design: Non-inferiority, NI margin set at -10%
Bernard, L et al Lancet 2015; 385:875-82
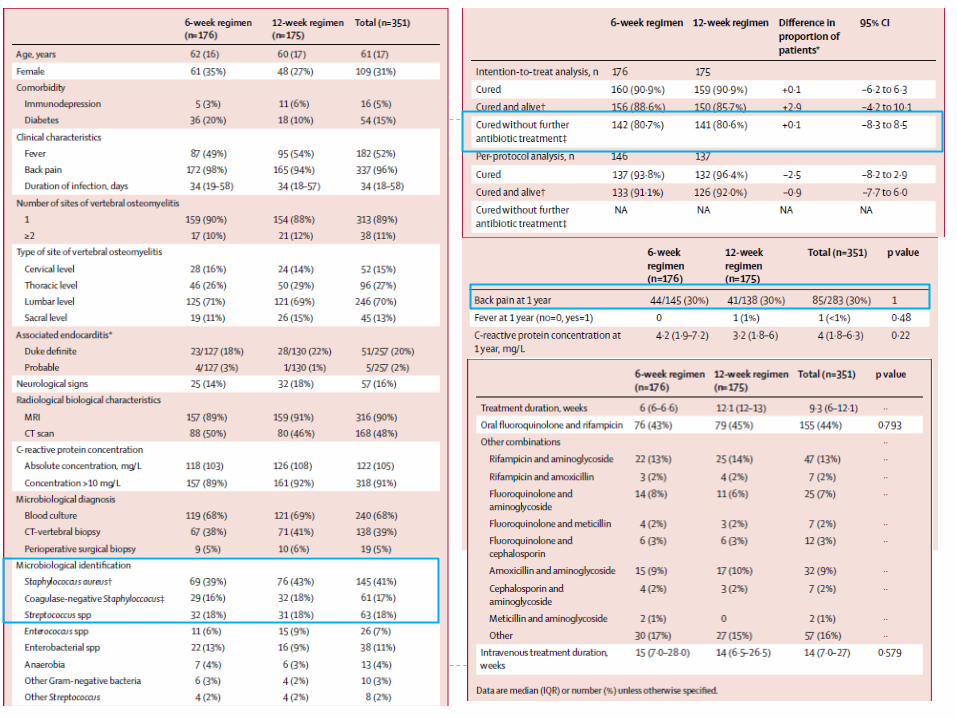

Take home for treating Vertebral OM Nearly identical results with both length regimens Extra 6 weeks does not appear to be useful QOL life also did not differ
Low-moderate rate of endocarditis (20%) 90% vs 80% (initial Rx) vs 70% (Any back pain free) effective ~50% getting 2 weeks or less of IV abx, followed by po Very little MRSA (8/145) High usage of RQ + RIF RIF/FQ with high oral bioavailability likely responsible for success No report of TMP/SMX + RIF
Ok for 6 weeks total, may be able to use less IV Long term outcome is good, but patients do not feel better at
week 6 or even week 12

Intra-abdominal Infections Two important papers published this year Asked similar questions Can we safely perform fewer operations? Can we safely use fewer antibiotics?
Results are interesting and contribute to our understanding

Case #1 54 year old male has 2 day onset of worsening Left Lower
Quadrant pain. He has a low grade fever and WBC is 13.5. A CT of the abdomen shows uncomplicated sigmoid
diverticulitis without perforation or abscess He is started on IV antibiotics, “bowel rest” x2-3 days, and
discharged home on oral antibiotics (and told not to eat popcorn anymore)
On follow-up he feels well. The surgeon tells him: “If the diverticulitis does not recur, you don’t need a sigmoid colectomy”

Case #2 54 year old male has 2 day onset of worsening Right
Lower Quadrant pain. He has a low grade fever and WBC is 13.5.
A CT of the abdomen shows uncomplicated appendicitis without fecolith/abscess/perforation.
Surgeon tells him “We’ll operate in the morning” Why is it that Case #2 cannot be treated like Case #1? This is the question asked by the authors of the APPAC trial

6 centers in Finland, Adult Patients (18-60), with CT scans showing uncomplicated appendicitis in the ED
Excluded: Other Dx, AKI/CKD or other reasons to not get contrast CT, peritonitis, serious systemic illness, AMS
Surgical Rx: Appy with Cefuroxime/Metro prophylaxis Primary outcome: Appendectomy
Experimental Rx: 3 days Ertapenem, then 7 days oral Levofloxacin/Metro Primary outcome: Resolution of appendicitis without surgery AND
no recurrence in 1 year
JAMA. 2015 Jun 16;313(23):2340-8.

Non-inferiority Planed as a non-inferiority trial Prior studied indicated need for large NI margin
NI margin set at 24% Secondary rationale was that complications would be
higher in surgical group Recruited to power 0.89, expected 0.86 due to dropouts
Wilms IM et al, Cochrane Database Syst Rev. 2011 Nov 9;(11):CD008359.

Results
Primary outcome: Surgical Group: 99.6% (95%CI, 98.0%-100.0%) Antibiotic Group: 72.7%; (95%CI, 66.8%to 78.0%) Difference: −27.0% (95% CI, −31.6% to Infinity) P = .89
Result: Antibiotics were not non-inferior
Salminen P et al, JAMA. 2015 Jun 16;313(23):2340-8.

Further results and secondary outcomes Of the 70 pts in the antibiotic group who had surgery 15 had complicated appendicitis 4 had surgical complications
Of note, 45 patients original surgical group had complications
Salminen P et al, JAMA. 2015 Jun 16;313(23):2340-8.

Recent update to the literature In May 2016, JAMA Surgery published a “Patient Choice”
trial for non-operative management of Pediatric Uncomplicated Acute Appendicitis
102 families offered Surgery vs non-operative management (antibiotics)
Of the 37 that chose, non-operative management, 76% had success (lack of appendectomy) at 1 year, consistent with the results of APPAC trial Similarly there were fewer days lost to disability in non-
operative group
Minneci PC et al JAMA Surgery 2016 May 1;151(5):408-15.

Take Home: APPAC Trial Appendectomy is still first line therapy for uncomplicated
appendicitis There are settings where non-operative management may be
appropriate (e.g. resource limited settings, patient preference) Unclear if choice of antibiotic makes a difference Risks of not operating are: 25% chance of eventually needing an operation (1 year) Risk of having complicated appendicitis Potential for drug resistance (not evaluated by this study)
Risks of operating are: Standard operative risk Increased time lost (sick leave as a proxy for time of recovery)

Antibiotics for Intra-abdominal Infections Guidelines suggest 4-7 day of therapy Often patients are on 14 days or more of antibiotics High rates of complications Lack of good data whether longer therapy can prevent them
Thus a randomized trial was performed.

Trial of Short-Course Antimicrobial Therapy for Intraabdominal Infection
(A.K.A. STOP-IT)
Robert G. Sawyer, M.D., Jeffrey A. Claridge, M.D., Avery B. Nathens, M.D., Ori D. Rotstein, M.D., Therese M. Duane, M.D., Heather L. Evans, M.D., Charles H.
Cook, M.D., Patrick J. O’Neill, M.D., Ph.D., John E. Mazuski, M.D., Ph.D., Reza Askari, M.D., Mark A. Wilson, M.D., Lena M. Napolitano, M.D., Nicholas Namias, M.D., Preston R. Miller, M.D., E. Patchen Dellinger, M.D., Christopher M. Watson, M.D., Raul
Coimbra, M.D., Daniel L. Dent, M.D., Stephen F. Lowry, M.D., Christine S. Cocanour, M.D., Michaela A. West, M.D., Ph.D., Kaysie L. Banton, M.D., William G. Cheadle, M.D., Pamela A. Lipsett, M.D., Christopher A. Guidry, M.D., and Kimberley
Popovsky, B.S.N.
N Engl J MedVolume 372(21):1996-2005
May 21, 2015

Study to Optimize Peritoneal Infection Therapy (STOP-IT) Inclusion criteria: Age ≥ 16 years. Hospitalized for intraabdominal infection requiring open,
laparoscopic, or percutaneous intervention WBC > 11,000, Fever or GI dysfunction (no po x24 h) “Adequate source control”
Stoppage of ongoing contamination of the peritoneal cavity Removal of majority of the contaminated intraperitoneal contents No further acute intervention necessary
Sawyer RG et al, NEJM 2015; 372(21):1996-2005

Exclusion Criteria High likelihood of death < 72h Perforated gastric ulcer or duodenal ulcer <24h Traumatic injury to the bowel <12 Non-perforated appendicitis or cholecystitis Gangrenous peritonitis/ischemic bowel without
confirmatory cultures Necrotizing pancreatitis, SBP, or PD catheter infection Pregnancy Primary closure of open laparotomy over diffuse
peritonitis Planned re-laparotomy
Sawyer RG et al, NEJM 2015; 372(21):1996-2005
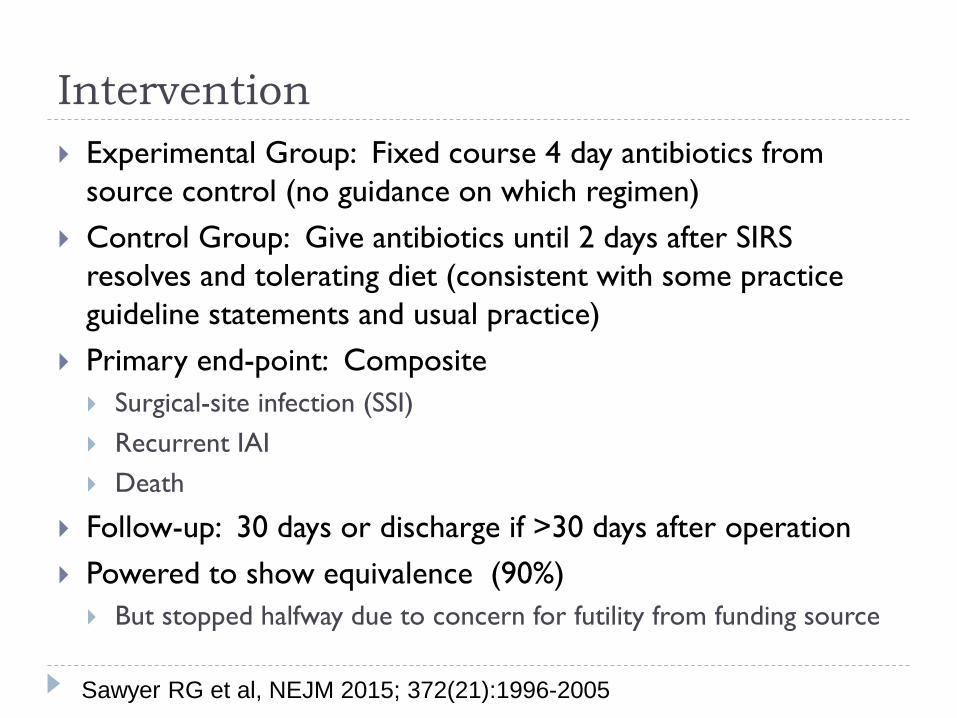
Intervention Experimental Group: Fixed course 4 day antibiotics from
source control (no guidance on which regimen) Control Group: Give antibiotics until 2 days after SIRS
resolves and tolerating diet (consistent with some practice guideline statements and usual practice)
Primary end-point: Composite Surgical-site infection (SSI) Recurrent IAI Death
Follow-up: 30 days or discharge if >30 days after operation Powered to show equivalence (90%) But stopped halfway due to concern for futility from funding source
Sawyer RG et al, NEJM 2015; 372(21):1996-2005

Sawyer RG et al, NEJM 2015; 372(21):1996-2005

Sawyer RG et al. NEJM 2015;372:1996-2005

Pre-specified Subgroup Analysis
Sawyer RG et al, NEJM 2015; 372(21):1996-2005

Take Home Points: STOP-IT More is not better Longer index antibiotics do not prevent recurrent infections or SSI
Source control is paramount (pts without it were excluded) Do not extracting this data for uncontrolled infection
Trial done by surgeons; good data. ?Adoption Choice of antibiotic not studied No data on bug/drug combos
Applicable for “Bread and Butter” patients Does not apply to most patients on ID service at UPMC
Trend: Short duration antibiotics for infections Cellulitis, CAP, UTI ≤7 days
More is not better

Baddour LM et al Circulation, Epub ahead of print September 15, 2015
Infective Endocarditis

Overview Always go to the guidelines when treating endocarditis
A few key updates in this document (first since 2005) are worth noting Echocardiography Antibiotics for MSSA/MRSA infective endocarditis Antibiotics for Enterococcus IE

Echocardiography TTE should be performed in all cases of suspected IE
TTE and TEE are complementary TTE: Better for right-sided lesions, ventricular dysfunction,
filling pressures TEE: better left sided lesions, obese patients etc.
Usually should start with TTE

S. Aureus Gentamicin should not be used for treatment of NVE
caused by MSSA or MRSA (Class III; Level of Evidence B). Nafcillin-gentamicin therapy decreased bacteremia by ~1 day
but had increased AKI and had no effect on mortality
MSSA should be treated with anti-staphylococcal penicillins not vancomycin or cefazolin but not vancomycin
MRSA: Vancomycin (trough 10-20)
Cosgrove S et al. Clin Infect Dis. 2009;48:713–72; Adapted from Ghady Haidar, MD

Enterococcus (Ampicillin S) Ampicillin + gentamicin (3 mg/kg IBW divided BID/TID)
(class IIa, level B) 4 weeks for patients with NVE and symptoms < 3 months 6 weeks for NVE with symptoms > 3 months or PVE
Ampicillin + ceftriaxone (2 grams q12) (class IIa, level B) 6 weeks “Recommended for patients with initial creatinine clearance
<50 mL/min or who develop creatinine clearance <50 mL/min during therapy with gentamicin-containing regimen”
Fernandez-Hidalgo N et al, CID 2013;56:1261–1268 ; Adapted from Ghady Haidar, MD

Urinary Tract Infections Vancomycin-Resistant Enterococcus (VRE) is a problem in
both the community and hospitalized patients This organism frequently colonizes bladder, and/or urinary
catheters in patients with prior antibiotics or other medical system contact
Occasionally also causes infections Many of the usual treatments are costly, parenteral,
limited in renal dysfunction, and/or associated with side effects E.g. fosfomycin, daptomycin, nitrofurantoin, and linezolid

VRE How best the treat? (when we do need to treat)
Key point: Minimum inhibitory concentrations (MICs) are set based on
blood achievable concentrations of antimicrobials Isolates are considered susceptible to ampicillin at MICs of ≤ 8
mg/liter and resistant at MICs of ≥16 mg/liter Due to renal excretion, oral amoxicillin and IV ampicillin are
able to concentrate in the bladder at levels an order of magnitude higher than this

Retrospective cohort, single center Inpatients Started with all Urine VRE isolates over 24 months Utilized chart review: Included patients with symptomatic UTI, treated with either
ampicillin or amoxicillin (with or without beta-lactamase inhibitor) vs those treated with non-betalactam
Endpoint: clinical cure: Resolution/improvement symptoms No additional antibacterial drug (for UTI) No microbiologic persistence
Antimicrobial Agents and Chemotherapy. 2015 Dec;59(12):7362-6.
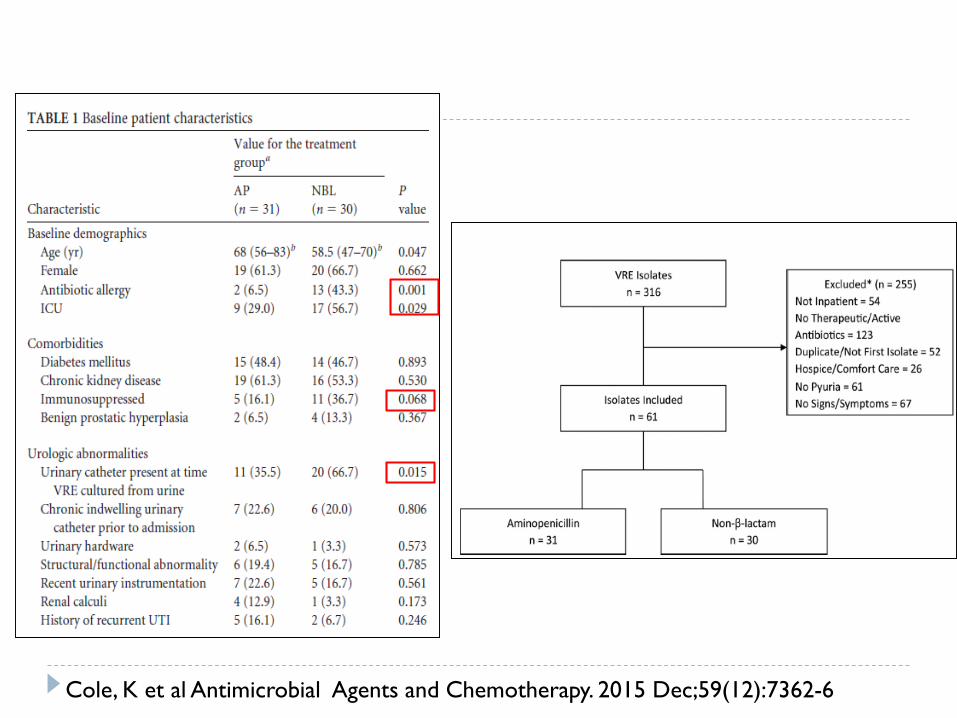
Cole, K et al Antimicrobial Agents and Chemotherapy. 2015 Dec;59(12):7362-6

Results
Aminopenicillin: 41.9% E. faecium, 58.1% E. faecalis,
Non-Beta-Lactam: 88.5% E. faecium11.5% E. faecalis
No difference primary end point
No difference 30 day mortality, 30 day retreatment or 30 day readmission
ICU, DM, CKD subgroups performed simliarly
33% of isolates 67% of isolates
Cole, K et al Antimicrobial Agents and Chemotherapy. 2015 Dec;59(12):7362-6

Take Home Points Suggests that many VRE isolates in the urine may be able to be
treated with or oral amoxicillin or IV ampicillin Limitations Small sample size Some baseline differences Not a RCT
Given that VRE is often indolent, starting with an amino-penicillin may be useful is some patients, with NBL therapy for those who do not respond
Further studies needed Follow-up studies Utility of direct measuring of VRE-ampicillin MIC on urine isolates

Conclusions Use new antibiotics judiciously CAP is caused by viruses and bacteria, often unknown
cause Antibiotics alone inferior to appendectomy With good source control, intra-abdominal infections
should be treated with 4 days of antibiotics No more need for Gentamicin for NVE with S. aureus
(and moving away from it for Enterococcus spp.)

Acknowledgements Course Organizers
Dr. Mark Gladwin and Dr. John Mellors
Slide and figure assistance Ghady Haidar Brian Potoski










