XGR Gloor SFI
4
f -- ,_ . . J pOSTMARK NEBRASKA ( i ! J ! i - ~ _ ~ \ ) •. ACCOUNT ABILITY AND DATE . • . DISCLOSURE COMMISSION STATEMENT MICROFILM 7 9 9 0 0 9 2 t t" Floor, State Capitol NUMBER O F .o. B o x 950~6 H F C F ~ ~ F J Q a USEONLY Lincoln, NE 68509 FINANCIAL ' : ~ I ~ i( CL ~ f " f ; p , ~£ t~ J \ ! 3 ~ ~ { :\ (40 2) 471-2522 INTERESTS 2 0 0 9 " DR 2 0 A N 9 : 0 9 I I B EFO RE C OMP LET IN G READ FILING REQUIREMENTS ~ ~E . \ C COUNr l~ > B } L IT · ' { 8 ~ NADC FORM C-1 D~ SC O S U H E C m ' jH 1 S S l m ~ ' Z #S6 • Candidates for designated offices and holders of designated offices and positions must file this statement. See Sections 1A and 18 of the instructions. • Candidates (including incumbents) subject to this . filing requirement must file with the Comm i ssion and with the appropriate election offic i al (See Instructions) . • D es ign at ed of fi ceh ol der s a~ d ho lde rs o f d es igna te d po si ti ons must fi l e t hi s s ta tem en t w it h t he C omm is si on a nnu al ly . • Dollar values need not be report for any item , e xc ep t I tem 11 . • Persons who fails to fi e as required is sublect to a civil penalty of U P to $2,000. ITE . M 1 I YOUR NAME, ADDRESS AND PHONE NUMBER Name GL o oR. IY\t0~~J ~"-{ T lephone No· 30S , 3 &:l., & - S]. , 2. LAST . . FIRST MIDDL . . Address <~I \ S- hJ~ &lVTwOOJl c . e CLE.. (.,I].. : /V J 'C'l [ 5 LKrV D "Jb . C ? fffO( STREETADDRESSOR RURALROUTE CITY STATE ZIP CODE ITEM 2 I OCCASION FOR FILING (Check Appropriate Box) . .. , o A candidate for elective office o Left office or position ~nnual officeholder's or state employee's report o Newly appointed to off i ce or position ITEM 3 I OFFICE HELD & TERM OF OFFICE (Incumbent elected/appointed officials and state employees. See IB of i ns tr uc ti on s) List the office or posi t ion you currently hold which requ i res th i s f il in g. I f y ou ha ve I EJ fto ff i ce, list the office you held . O{/13 ffice or Position : S~ bdn-< . Term: 0(/()(} L~G,I SL A TLtR...Ji BJ:GINS ENDS Name of City, County, District, or State Agency: ITEM 4 I OFFICE SOUGHT (Candidates only. See 1A of instructions) List the o fice sought which requires this filing. Office: Name of City , Cou n ty, District, or State Office: ITEMS I PERIOD COVERED BY THIS STATEMENT T hi s s tat em en t mu st c ov er a ll f in an ci al i nt er es ts f o r the entire "preceding calendar year"and not just as of year-end. If you have left of fic e , t hi s s tat em ent mu st c ov er a ll . financi al interests from t he end of the calendar yea for which you previously filed up to and i nc lu di ng t he d at e y ou le ft o ff ic e. . . ~ Th i s statement covers the preceding calendar year January1 through December 31 , ;2.008 D L ef t o ff ic e , this statement covers the period January 1, to ( DAT EYOU LEFTOFFICEOR POSITI ON ) I Revised Aug ust 200 7
-
Upload
nebraskawatchdog -
Category
Documents
-
view
227 -
download
0
Transcript of XGR Gloor SFI
8/14/2019 XGR Gloor SFI
http://slidepdf.com/reader/full/xgr-gloor-sfi 1/4
f--,_. .JpOSTMARKNEBRASKA
( i! J ! i - ~ _
~\)•.
ACCOUNT ABILIT Y ANDDATE
. • .
D ISCLOSURE COMM ISS ION STATEMENT MICROFILM 7990092t t" Floor, State Capitol
NUMBER
OF.o. Box 950~6 H F C F ~ ~ F J Q aUSEONLYLincoln, NE 68509 FINANCIAL ' : ~ I~ i( C L ~f " f ; p ,~£ t~J \ ! 3 ~ ~ {:\(402) 471-2522
INTERESTS 2 0 0 9 " D R 2 0 A N 9 : 0 9I I
BEFORE COMPLETING
READ FILING REQUIREMENTS ~~E.\CCOUNrl~ >B}LIT· '{ 8~NADC FORM C-1 D~SC O S U H E C m 'jH 1SS lm ~
'Z # S 6• Candidates for designated off ices and holders of designated offices and positions must file this statement. See Sections 1A and18 of the instructions.
• Candidates (including incumbents) subject to this .filing requirement must file with the Commission and with the appropriateelection official (See Instructions).
• Designated officeholders a~d holders of designated positions must file this statement with the Commission annually.
• Dollar values need not be report for any item, except Item 11.
• Persons who fails to file as required is sublect to a civil penalty of UP to $2,000.
ITE.M 1 IYOUR NAME, ADDRESS AND PHONE NUMBER
Name GLooR.
IY\ t0~~J~"-{ TelephoneNo·30S, 3&:l., & -S].,2.
LAST. . FIRST MIDDL . .
Address <~I \ S- hJ~&lVTwOOJl c.e CLE.. (.,I].. :/V J 'C' l [ 5 LKrV D "Jb. C ? ff fO(STREETADDRESSOR RURALROUTE CITY STATE ZIP CODE
ITEM 2 IOCCASION FOR FILING (Check Appropriate Box). ..,
oA candidate for elective office o Left of fice or posit ion
~nnual officeholder's or state employee's report o Newly appointed to office or position
ITEM 3 I OFFICE HELD & TERM OF OFFICE (Incumbent elected/appointed officials and state employees. See
IB of instructions)
List the office or position you currently hold which requires this fil ing. If you have IEJftoffice, list the office you held.
O{/13ffice or Position: S~ bdn-< . Term: 0(/()(}
L~G,I SLA TLtR...Ji
BJ:GINS ENDS
Name of City, County, District, or State Agency:
ITEM 4 IOFFICE SOUGHT (Candidates only. See 1A of instructions)
List the office sought which requires this filing.
Office:
Name of City, County, District, or State Office:
ITEMS IPERIOD COVERED BY THIS STATEMENT
This statement must cover all f inancial interests for the entire "preceding calendar year"and not just as of year-end. If you have
left office, this statement must cover all.financial interests from the end of the calendar year for which you previously filed up to andincluding the date you left office. . .
~This statement covers the preceding calendar year January1 through December 31, ;2.008
D Left office, this statement covers the period January 1, to
(DATEYOU LEFTOFFICEOR POSITION)
Revised August 2007
8/14/2019 XGR Gloor SFI
http://slidepdf.com/reader/full/xgr-gloor-sfi 2/4
I f..t.--~ 1
. . -
! i
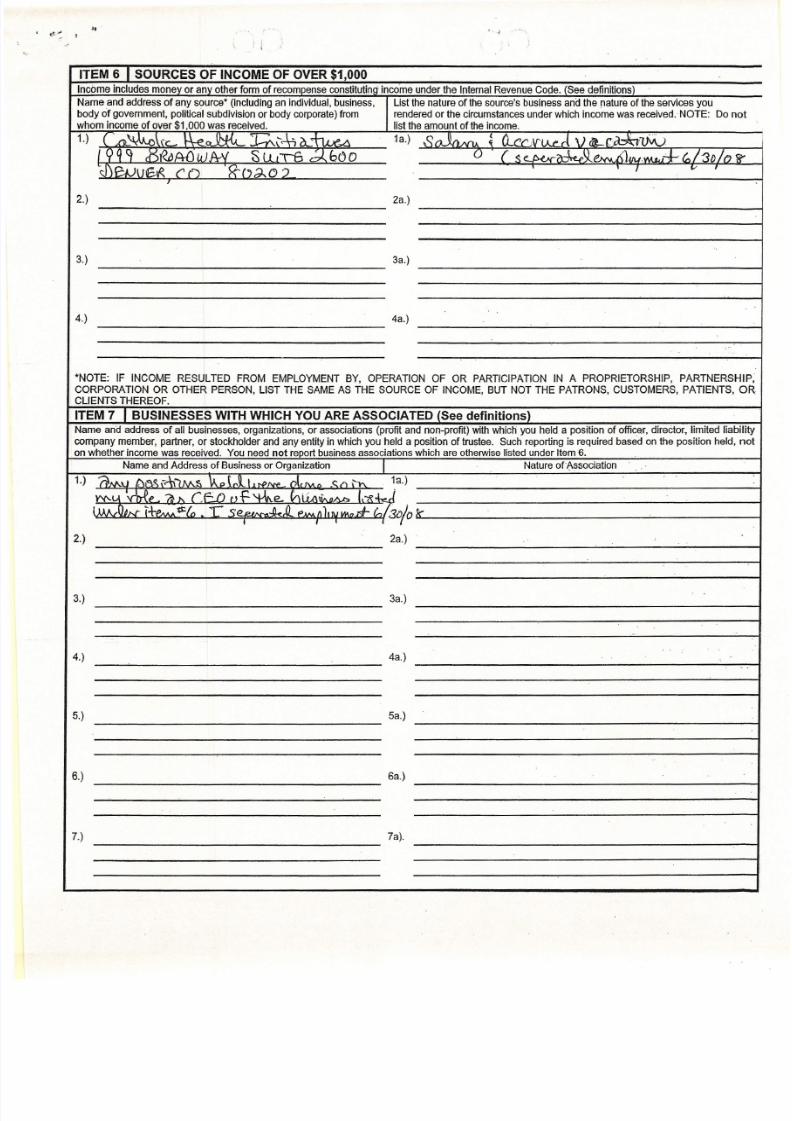
ITEM 6 r SOURCES OF INCOME OF OVER $1,000
Income includes money or any other form of recompense constitutlnq income under the Infernal Revenue Cope. (See definitions)
Name and address of any source" (including an individual, business, Lisf the nature of the source's business and the nature of the services you
body of government, poli tical subdivision or body corporate) from rendered or the ci rcumstances under which income was received. -NOTE: Do
whom income of over $1,000 was received. list the amount of the income.
1.) ( ,rL~\fr \ - \ - e o ! ! - l < . t T:.. '-.-4o....~ 1a.) soJln .NU ~ D.. .cc-,V 'LV '~ \) tLr~vVv
199't ;r)«cAfJlJJPrV SLu\6 d-.b00 0 (Se..1'. _~. .s. .JJ"k A') 'M~1+t, /3D/{j1r 'd')p-.• )1 t.CtR ('() . x - - ( , ~ c » _ I v
r
2.) 2a.)
3.) 3a.)
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
4a.).)
"NOTE: IF INCOME RESULTED FROM EMPLOYMENT BY, OPERATION OF OR PARTICIPATION IN A PROPRIETORSHIP, PARTNERS
CQRPORATION OR OTHER PERSON, LIST THE SAME AS THE SOURCE OF INCOME, BUT NOT THE PATRONS. CUSTOMERS, PATIENTS.
CLIENTS THEREOF.
ITEM 7 I BUSINESSES WITH WHICH YOU ARE ASSOCIATED (See definitions)
Name and address of all businesses, organizations, or associations (profit and non-profit) with which you held a position of officer. director, limited li
company member, partner, or stockholder and any entity in which you held a posit ion of trustee. Such reporting is required based on the position held
on whether income was received. You need not report business associat ions which are otherwise l isted under Item 6.
Name and Address of Business or Organization I Nature ofAssociatlon
1.) 7 .\ AAlJ tV ,> ." " '\ \" " 7 . \" , ~ v . . " L , ' L I NJ fv.p rk I\. ~<:....... "'" 1a.)
YV--U 'Me n" r . r . J J nf.%.e. IrIUA\i,...nAb "~-kr iIIILOA (1" 'PAAAt t .(" T C~ ~ ( p, ~),nJw.nd-(::,/30Jok~ _'__
I , • 7 '
2.) 2a.)
3.) 3a.)
4.) 4a.)
- - - - ~ - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
5a.).)
6a.).)
7.) 7a).
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
8/14/2019 XGR Gloor SFI
http://slidepdf.com/reader/full/xgr-gloor-sfi 3/4
. , 'f
~ I . , ,,
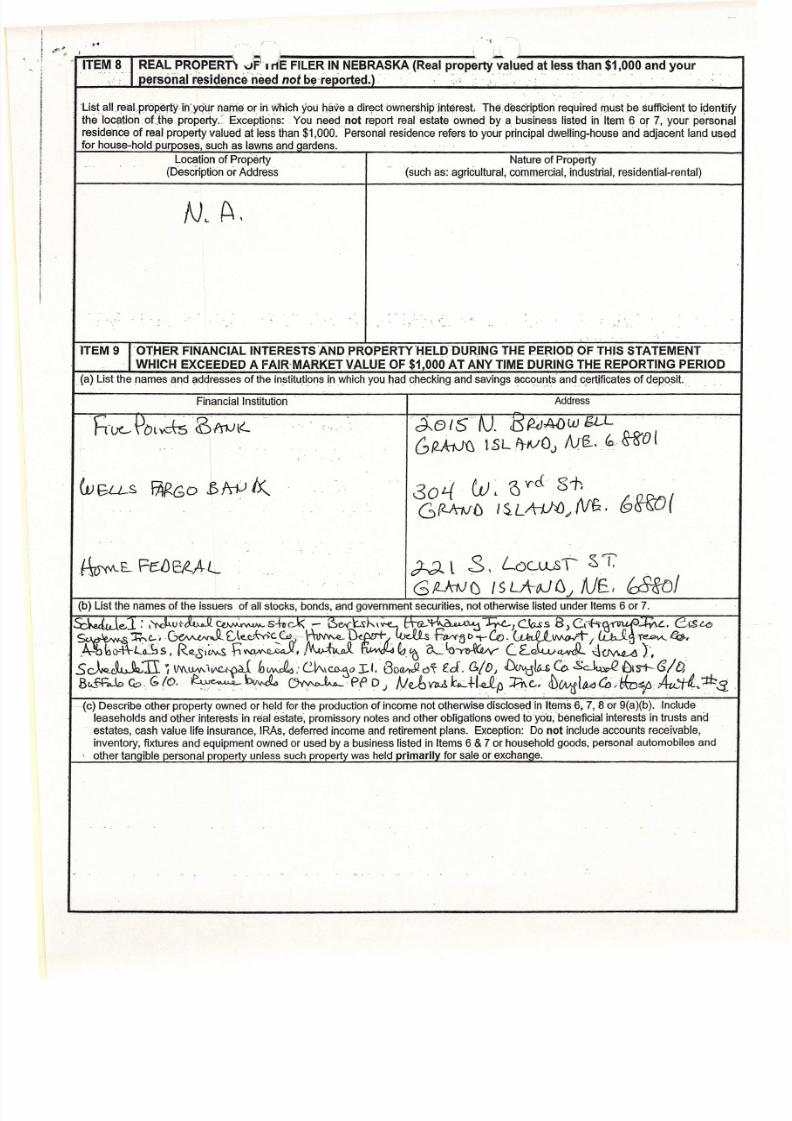
ITE~8. J::~~:a~:~d~~:~~1~~:~~~!~o~~~~SKA (Real p~~perty'Val~edates~ than $1 ,O~Oand your
'List all r~alpr6p.ertYih·.yQ(jr narhi3 or in which you have a direct ownership.interest The.descrlptlon required must be sufflcient to identify
the location otjh~ property.' Exceptions: . You need not report real estate owned bya business listed in Item 6 or 7, your persona
residence of real property valued at less than $1,000. 'Personal residence refers to your principal dwelling-house arid adjacent land used
for house-hold purposes, such as lawns and qardens.
Location of Property Nature of Property
(Description or Address (such as: agricultural, commercial, industrial, residential-rental)
N~ A .
.... '.
..' .
. ,
ITEM9 rOTHERFINANCIAL INTERESTSANDPRQPERTYHELP'DURING THE PERIOQ OF THIS STATEMENT
. . WHICH EXCEEDED A FAIR-MARKETALUEOF $1,000 AT ANYTIME DURING THE REPORTING PERIOD
(a) List the names and addresses of the Institutions in which you had checking and savings accounts' and certflcates of deposit.
Financial Institution Address
' h - u e - - {JtH~--ts dS l1 1 Jl '- . · d -.e (5' f V . J : ) ~A()W tjL.L ....
:
G~ tSLf}IVOJ
~. ~~!
WGU-S i = M G O iS~~ 30'--( w . a '( 'c i. 8i;
G(U'nJ{J IS . L A:iHJ pN f ;. , ~'~(
:
ST,~E- Fe:D&Al. ~l S, L()Cu.AI
, .
fc8rol/LktJ f:J I s LA-- t06 .1 A lE I
. (b) List the names of the issuers ofall stocks, bonds, and government securities, not otherwise listed under Items 6 or 7.
S:kJu le ,l.. : "'Nj~uc-~~~-hcJ< . .- P&(\::Sl--\~\IA..~ '" <.l~}c..~s B)Ci~ca~~C. e,:$~~~~.~(,te.e;,~c,S \~lk~ -: ~c>;-Co.~vwwt-/CVJ~.~,
.. bo--tt -L -ib s. R~llt...s - h ~ .1~. C : t . 't ~Ia~ C Ec k..vcwJl J~ t .s~~TI ~\M.~1V'C.-~ll b~ :C .lt -- \C !> ..~ oI.1 . BoWc,.~ ed. ~/{)I ~1{j.$co.~~rs-t--(5/l3
. B l:< -ffi.k C O , (;10. ~b~ ~pp. D J N ~ vMb.:..+I:e 1 ,o Ae-" J )W ift t1C(D 'Mvo /lAu..,~ '": : ths.
. (c) Describe other property owned or held forthe production of income not otherwise disclosed in Items 6, 7, 8 or 9(a)(b).lnciude .
leaseholds andotherlnterestsin real estate, promissory notes and other obligations owed toyou.beneflclal interests in trusts and
estates, cash value life insurance,IRAs,. deferred income and retirement plans. Exception:. Do not include accounts receivable,
inventory, fixtures and equipment owned or used by a business listed in Items 6 & 7 or household goods, personal automobiles and
other tangible personal property unless such property was held primarilv for sale or exchanoe.
-, ..
8/14/2019 XGR Gloor SFI
http://slidepdf.com/reader/full/xgr-gloor-sfi 4/4
, , - . '"
ITEM 10 I CREDITORS TO W HOM $1,000 OR MORE W AS OW ED OR GUARANTEED BY YOU OR A MEMBER OF
YOUR IMMED IA TE F AM IL Y.
Exception: Loans from a relative and land contracts which have been recorded with the County Clerk or Register of Deeds need not bereported. Accounts payable, debts arising out of retail installment transactions or loans made by a financial institution in the ordinary
course of business need n~t be reported.
Name Address
N.,4 ,
ITEM 11 I SOURCES OF G IFTS OF A VALUE OF MORE THAN $100 RECEIVED EXCEPT G IFTS FROM RELATIV ES.(See defin it ions) .
Name and address of Donor Occupation or nature of business of Value of Gift Description of Gift and
Donor (See Key Below) Circumstances or Occasion for
Gift
N '. A,Choose Value:
Choose Value:
Choose Value:,
Choose Value:
Choose Value:
Choose Value:
Choose Value:
Choose Value:
The monetary value of each gift shall be categorized based on the good faith estimate of the filer. For each reported gift insert in the
Value column the letter which corresponds to the value category of the gift. The value categories are:
A) $100.01 to $200; B) $200.01 to $500; C) $500.01 to $1,000; D) $1,000.01 or more.
ITEM 121 SIG NA TU RE O F FIL ER A ND DATE.
I hereby state, that I have used all reasonable diligence. in the preparation of this Statement and that to the best of my knowledge it is true
and comolete.
. 0 ,3/19/f)9 .l( O A r . t leu
(Signaturl(of Filer) (Date),