Www.aids2014.org HCV cure: new treatment paradigms for HCV infection Sanjay Bhagani Consultant...
29
www.aids2014.org HCV cure: new treatment paradigms for HCV infection Sanjay Bhagani Consultant Physician/Senior Lecturer Royal Free Hospital/UCL London
-
Upload
payton-gupton -
Category
Documents
-
view
217 -
download
0
Transcript of Www.aids2014.org HCV cure: new treatment paradigms for HCV infection Sanjay Bhagani Consultant...

www.aids2014.org
HCV cure: new treatment paradigms for HCV infection
Sanjay BhaganiConsultant Physician/Senior Lecturer
Royal Free Hospital/UCL
London

www.aids2014.org
HCV/HIV co-infection – ‘shades of grey’

www.aids2014.org
Outline
• Impact of HCV in the HIV-infected patient– The importance of treating HCV
• PegIFN/ribavirin – a bygone era• DAAs for HCV and HCV/HIV
– IFN ‘sparing’ and IFN-free regimens
• Is this still a ‘Special Population’?• New Guidelines

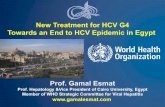
D:A:D: Liver-related death is a frequent cause of non-AIDS death in HIV-infected
patients
Weber R, et al. AIDS 2012. Washington USA. Oral presentation THAB0304.
0
20
40
60
80
100
29
13 11 14
33Death
s (
%)
Liver-related disease
Cardio-vascular or other
heart disease
OtherAIDS Non-AIDS malignancie
s
D:A:D Study: Causes of death in n=49,734 HIV-infected patients followed 1999–2011

www.aids2014.org
HIV/HCV – double-trouble for the liver
Chen J Nat Rev Gastroenterol Hep 2014 doi:10.1038/nrgastro.2014.17

www.aids2014.org
Faster progression even when controlling for alcohol and other co-morbidities
Kirk D, et al. Ann Intern Med 2013; 158: 658

HIV/HCV – a contribution to multiple organ dysfunction
Adapted from Operskalski EA and Kovacs A. Curr HIV/AIDS Rep 2011;8:12–22.
Immuneactivation
Immunedysfunction
HIV/HCVLiver
diseaseHIV disease progression
Metabolicdisorders
GI tract
Neurologicdisease
Cardio-vascular
Kidneydisease
Bonedisorders
• CD4 apoptosis• Abnormal T-cell responses and cytokine production• Cytotoxic T-cell accumulation in liver• Impaired CD4 recovery post-HAART• Severe immunodeficiency
• Diabetes mellitus• Insulin resistance
• Microbial translocation
• Steatosis• Fibrosis• Cirrhosis• End-stage liver
disease• Liver-related death
• Global cognitive impairment• Cognitive-motor impairment• Dementia• Peripheral neuropathy
• Cerebrovascular disease
• Acute myocardial infarction
• Opportunistic infections
• Wasting syndrome
• Proteinuria• Acute renal failure• Chronic kidney
disease
• Osteonecrosis• Osteoporosis• Bone fracture

www.aids2014.org
A) Overall-Mortality
Observation time[days]]
500040003000200010000
Cu
mu
lati
ve s
urv
ival
1,1
,9
,7
,5
,3
P<0.0001
Patients with HAART
Patients with dual ARvs untreated Patients
6000
Patients under observation:HAART-group: 93 79 33 - - - ART-group: 55 46 30 15 9 1Untreated-group: 13794 49 37 32 27
6000500040003000200010000
1,1
,9
,7
,5
,3
B) Liver-related-Mortality
P<0.018
Patients with HAART
Patients with dual ARvs untreated Patients
Overall and Liver-related Mortality - effect of HAART
Qurishi N et al. Lancet, 2004
Cu
mu
lati
ve s
urv
ival
Observation time[days]]
Patients under observation:HAART-group: 93 79 33 - - - ART-group: 55 46 30 15 9 1Untreated-group: 13794 49 37 32 27

www.aids2014.org
‘Hepatotoxcity’ commoner in co-infected patients
Vispo, et al. AIDS 2013:27: 1187

HCV/HIV SVR24 with pegIFN and RIBAVIRIN
0
25
50
75
100
G1 G2/3
Monoinfection
APRICOTACTGRIBAVICLaguno et al.PRESCO
Genotype 1SVR 14–38%
Genotype 3SVR 44–73%
Genotype
SVR
(%)
Adapted from: Fried et al, NEJM 2002;347:975-982, Torriani et al, NEJM 2004;351:438-50, Chung R, et al, NEJM 2004;351:451-9 Carrat F, et al, JAMA 2004;292:2839-42, Laguno et al, AIDS 2004;18:F27-F36, Nunez et al, JAIDS 2007;45:439-44

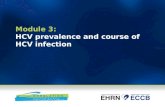
HCV Life Cycle and DAA Targets – drug classes and nomenclature
Adapted from Manns MP, et al. Nat Rev Drug Discov. 2007;6:991-1000.
Receptor bindingand endocytosis
Fusion and
uncoating
Transportand release
(+) RNA
Translation and
polyprotein processing
RNA replication
Virionassembly
Membranousweb
ER lumen
LD
LDER lumen
LD
NS3/4 protease inhibitors NS5B polymerase inhibitors
Nucleoside/nucleotideNonnucleoside
*Role in HCV life cycle not well defined
NS5A* inhibitors
..PREVIR
..ASVIR …UVIR

HCV Life Cycle and DAA Targets – drugs
Adapted from Manns MP, et al. Nat Rev Drug Discov. 2007;6:991-1000.
Receptor bindingand endocytosis
Fusion and
uncoating
Transportand release
(+) RNA
Translation and
polyprotein processing
RNA replication
Virionassembly
Membranousweb
ER lumen
LD
LDER lumen
LD
NS3/4 protease inhibitors NS5B polymerase inhibitors
Nucleoside/nucleotideNonnucleoside
*Role in HCV life cycle not well defined
NS5A* inhibitors
TelaprevirBoceprevirFaldaprevirSimeprevirABT 450/rAsunaprevirMK-5172
DaclatasvirLedipasvirOmbitasvirMK-8742GS-5816
Sofosbuvir
DasabuvirBMS-791325

ALL
Relapsers
Breakth
rough
Partial R
esponse
Null Resp
onseF0
–F2F3
/F4ATV/r
Raltegra
vir0
20
40
60
80
100
53
90
0
61
24
56
4841
70
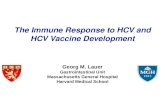
ANRS studies TelapreVIH and BocepreVIH inTE HCV GT 1 HIV/HCV co-infected patients
1. Cotte L, et al. CROI 2014; Oral #668; 2. Poizot Martin I, et al. CROI 2014. Oral #659.
SVR24 in HIV/HCV PEG-IFN/RBV experienced treated with PEG-IFN/RBV + TVR (69) or BOC (64); 4 weeks lead in + 44 weeks standard +
24 additional weeks if HCV RNA at Week 8 >15IU/mL. ATV/r: ritonavir boosted atazanavir; TE: treatment-experienced
TVR BOC
SV
R24
(%
)
SV
R12
(%
)
ALL
Relapsers
Breakth
rough
Partial R
esponse
Null Resp
onseF0
–F2F3
/F4ATV/r
Raltegra
vir0
20
40
60
80
100
8074
83
100
71
81 78 81
71

www.aids2014.org
‘Real-life’ experience PegIFN/R + TVR/BOC – pan-European data
Rx discontinuation Rx response ITT and OT
8
36
50
0
20
40
60
80
100
platelets ≥100/µL +albumin ≥3.5 g/dL
platelets ≥100/µL +albumin <3.5 g/dL orplatelets <100/µL +albumin ≥3.5 g/dL
platelets <100/µL +albumin <3.5 g/dL%
of pa
tient
s who
disc
ontin
ued a
ll the
rapy
Neukam K, Munteanu D, et al. CROI 2014

Second generation DAAs + PEG-IFN/RBV in HIV/HCV co-infected patients
1. Dieterich D, et al. EACS 2013. PS9/5; 2. Rockstroh J, et al. EACS 2013 .PS9/7; 3. Rodriguez-Torres M, et al. ID Week 2013. Poster #714.
Follow-up
SMV + PR
Week 12 36 60
SMV + PR (RGT)
Follow-up
Follow-up
48 72
PR
PR
PR
24
Partial response Null response Cirrhotic patients (F4)
Genotype 1a/b• HCV treatment-naïve Prior PR relapsers
FDV 120 mg + PR PR or follow up (RGT)
FDV 240 mg + PR
FDV 240 mg + PR
PR
PR or follow up (RGT)
SOF + PR
SVR4 SVR12 SVR24
Follow-up
C2121
STARTVerso42
SOF + PR3
DAA: direct-acting antiviral agents; FDV: faldaprevir; PR: PEG-IFN/RBV; RGT: response guided therapy; SMV: simeprevir
Protease inhibitors
Nucleoside polymerase inhibitor
Genotype 1a/b Treatment Naïve Relapse 15% Compensated
Cirrhotic patients (F4)
Genotype 1-4• HCV treatment-naïve

C212: SVR12 by concomitant ART use(ITT population)
*0/1 patients; SVR12, sustained virologic response 12 weeks after end of treatment; n/a, not applicable
Overall Naïves Relapsers Partial Null0
20
40
60
80
100 On ARTNot on ART
81
70
62
75
87
78
70/93 8/13 7/10 1/215/267/913/1535/43 n/a 0*
58
50
SV
R12
(%
)

www.aids2014.org
STARTVerso4: SVR12 overall population
87/123 134/185 221/308Pro
port
ion
of p
atie
nts
with
SV
R12
(%
)

www.aids2014.org
Study 1910: SVR12
Rodriguez-Torres M et al. IDWeek 2013, poster 714
100
80
60
40
20
0
HC
V R
NA
<LL
OQ
(%
)
89%
17/19
GT1
1/1
GT2
2/2
GT3
1/1
GT4
LLOQ: lower level of quantification

PHOTON-1 studyNaggie S, et al. CROI 2014. Oral #26
C-WORTHY studySulkowski M, et al. EASL 2014. Oral #63
LDV/SOF STRERADICATE studyOsinusi A, et al. EASL 2014. Oral #14
IFN-free DAA regimens in HIV/HCV co-infected patients

PHOTON-1: Virological response
Naggie S, et al. CROI 2014. Oral #26.
GT 1 GT 2 GT 3 GT 2 GT 30
20
40
60
80
100
76
88
67
92 94
SVR1
2 (%
)
TN TE
12 weeks
24 weeks
SOF + RBV
• No HCV resistance (S282T) observed in virological failures (deep sequencing)– HCV breakthrough in 2 patients due to non-adherence to SOF – HIV breakthrough in 2 patients due to non-adherence to ART
16/17
28/42
22/24
23/26
87/114

www.aids2014.org
TW4 TW8 TW12 SVR40
102030405060708090
100100 100 100 97100
90 90 90
MK-5172 + MK-8742 + RBV (n=29)
MK-5172 + MK-8742 (No RBV; n=30)
Week
% H
CV
RN
A <
25 I
U/m
LC-Worthy Virologic Response
ITT Population
2929
21
28 29
2929
2929
3030
2629*
2730
2730
Virologic Failures: 1 relapse in +RBV arm; 2 breakthrough and 1 lost to follow up in No
RBV arm* One patient has not yet reached FU4

www.aids2014.org
The IFN and RBV free regimen of LDV/SOF in HCV/HIV co-infected patients resulted in SVR12 of 100% in ARV untreated patients and SVR4 of 100% in ARV treated patients
LDV/SOF STR was generally well tolerated with no discontinuations Actively enrolling ION-4 (target of 300 GT 1 and GT 4 HCV/HIV patients). NCT 02073656.
ERADICATE - Treatment Response
Week 4 Week 8 EOT SVR4 SVR8 SVR120
20
40
60
80
100100 100 100 100 100 100100 100 100 100
ARV Untreated ARV Treated%
of p
atie
nts
with
HC
V R
NA
<
LL
OQ
13/13
37/37
13/13
37/37
13/13
30/30
12/12
22/22
10/10
10/10
Osinusi A, EASL, 2014, O14

SVR12 - PEG-IFN/RBV + TVR, SMV, FDV and SOF in HCV GT1 TN patients: HIV+ vs HIV–
TVR + PR SMV + PR FDV + PR SOF + PR0
20
40
60
80
100
7479
72
91
79 80 80
91
HIV+HIV-
1. Sulkowski M, et al. AASLD 2012. Oral #54; 2. Janssen Cilag International. INCIVO (Telaprevir), Summary of product characteristics, September 2011; 3. Dieterich D, et al. CROI 2014 Abstract #24; 4. Jacobson I, et al. AASLD 2013. Poster #1122; 5. Dieterich D, et al. APASL 2014. Oral‘#681; 6. Ferenci P, et al. EASL 2013. Abstract #1416; 7. Rodriguez-Torres M, et al. ID week 2013. Poster #714; 8. Lawitz E, et al. APASL 2013. Oral #LB-02.
419/521
42/53
296/327
21/23
285/363
28/38
414/520
221/308
24 or 48 weeks 12 weeks24 or 48 weeks 12 or 24 weeks
SVR1
2 (%
)
Cirrhosis Excluded12%3 9%411%1 6%2 15%5 6%6
5,6 7,8
NOTE: not head-to-head comparisons.
1,2 3,4

www.aids2014.org
Adjusteda SVR12 (%)
HIV Co-infection
No (reference)
Yes
72.3
85.0
Genotype
1a (reference)
1b
74.2
83.2
FDV dose
120 mg (reference)
240 mg
79.0
78.3
Comparisons of SVR12 rates of interest adjusted for important predictors of response across the STARTVerso studies, excluding PI- and EFV-treated patients
from STARTVerso4
Adjusted difference in SVR12 (95% CI)
-20 -15 -10 0 10 15 20
12.6 (5.7, 19.5)
9.0 (4.2, 13.8)
30
5
-0.7 (-5.0, 3.6)
-5
a Adjusted for IL28B, race, fibrosis stage, baseline HCV RNA, age, baseline GGT and baseline platelet count.
Deitrich, APASL 2014, o681

New online EASL HCV recommendations
Same treatment regimens can be used in HIV/HCV patients as in patients without HIV infection, as the virological results of therapy are identical (A1)
EASL recommendations April 2014 http://files.easl.eu/easl-recommendations-on-treatment-of-hepatitis-c-summary.pdf

New EASL HCV recommendations – treatment combination options
EASL recommendations April 2014 http://files.easl.eu/easl-recommendations-on-treatment-of-hepatitis-c-summary.pdf
SOF + PEG-IFN/RBV
SMV + PEG-IFN/RBV
Daclatasvir + PEG-IFN/RBV
SOF + SMV (± RBV)
SOF + daclatasvir (± RBV)
12 weeks
12 weeks + RGT 12/36
12 weeks + RGT 12
12 weeks
12–24 weeks
SOF + RBV 12–24 weeks
G1, 3, 4
G1, 4
G1, 2, 3, 4
G4
G1, 4
G1, 2, 3, 4, 5, 6

www.aids2014.org
S.Khoo, 15th Intl. W’shop, 2014

www.aids2014.org
Conclusions
• The era of DAA based therapy has arrived– IFN-sparing and IFN-free therapy a reality
• Responses in HIV+ similar to HIV-• Beware DDIs• Still a ‘Special Population’ – aggressive,
multi-system disease, urgent need of Rx• Need for improved cascade of care and
access to Rx

www.aids2014.org
HCV/HIV co-infection – ‘shades of grey’