Wrong Site Spine Surgery JAAOS
9
Wrong-site Spine Surgery Abstract Wrong-site spine surgery is an adverse event that has potentially devastating consequences for the patient as well as the surgeon. Despite substantial efforts to prevent wrong-site spine surgery, this complication continues to occur and has the potential for serious medical, personal, and legal repercussions. Although systems- based prevention methods are effective in identifying the proper patient, procedure, and region of the spinal column, they cannot be relied on to establish the correct vertebral level during the operation. The surgeon must design and implement a patient- specific protocol to ensure that the appropriate operation is performed on the correct side and level or levels of the spinal column. W rong-person, wrong-proce- dure, and wrong-site surgery were the most common sentinel events reported by the Joint Com- mission on Accreditation of Health- care Organizations (JCAHO) from 2004 to 2011. 1 These events are among the most serious of medical errors, often leading to clinical mor- bidity, increased healthcare costs, and legal action. Both the patient and physician typically suffer signifi- cant emotional harm. Wrong-site spine surgery (WSSS) occurs when a surgeon performs a decompression, resection, or recon- structive procedure on an unin- tended anatomic location along the spinal axis. WSSS encompasses both wrong-level surgery (ie, an operation performed on an incorrect vertebra or spinal motion segment) and wrong-side surgery. 2-7 Surgical expo- sure of a spinal segment in proximity to the intended surgical level is com- mon and should not be considered a wrong-site operation. Despite ongoing efforts to prevent WSSS, it continues to occur, with up to 50% of spine surgeons reporting performance of at least one wrong- level operation during the course of their careers. 7 The surgeon must re- main particularly vigilant against wrong-level spine surgery (WLSS) given the challenge of intraoperative localization of the correct vertebral segment. Precise identification of the correct spinal level requires special- ized knowledge and meticulous anal- ysis of radiographic imaging and an- atomic landmarks. Patient factors such as body habitus, spinal defor- mity, and variant vertebral morphol- ogy can introduce error or uncer- tainty with regard to the correct spinal level. 8,9 Systems-based prevention is effec- tive for confirming the proper pa- tient and planned procedure and identifying the appropriate region of the spinal column (ie, cervical, tho- racic, or lumbar). 9,10 These preven- tion systems, however, cannot be re- lied on to establish the correct vertebral level during the operation. Accordingly, the use of preoperative checklists is just one component of the overall approach to prevent WSSS. Mark A. Palumbo, MD Aaron J. Bianco, MD Sean Esmende, MD Alan H. Daniels, MD From the Department of Orthopaedic Surgery, the Warren Alpert Medical School of Brown University, Providence, RI. Dr. Palumbo or an immediate family member is a member of a speakers’ bureau or has made paid presentations on behalf of and serves as a paid consultant to Globus Medical, Stryker, and Medtronic and has received research or institutional support from Globus Medical. Dr. Daniels or an immediate family member has received research or institutional support from Synthes Spine and Flexuspine. Neither of the following authors nor any immediate family member has received anything of value from or has stock or stock options held in a commercial company or institution related directly or indirectly to the subject of this article: Dr. Bianco and Dr. Esmende. J Am Acad Orthop Surg 2013;21: 312-320 http://dx.doi.org/10.5435/ JAAOS-21-05-312 Copyright 2013 by the American Academy of Orthopaedic Surgeons. Review Article 312 Journal of the American Academy of Orthopaedic Surgeons
-
Upload
louis-okafor -
Category
Documents
-
view
85 -
download
3
Transcript of Wrong Site Spine Surgery JAAOS

Wrong-site Spine Surgery
Abstract
Wrong-site spine surgery is an adverse event that has potentiallydevastating consequences for the patient as well as the surgeon.Despite substantial efforts to prevent wrong-site spine surgery, thiscomplication continues to occur and has the potential for seriousmedical, personal, and legal repercussions. Although systems-based prevention methods are effective in identifying the properpatient, procedure, and region of the spinal column, they cannot berelied on to establish the correct vertebral level during theoperation. The surgeon must design and implement a patient-specific protocol to ensure that the appropriate operation isperformed on the correct side and level or levels of the spinalcolumn.
Wrong-person, wrong-proce-dure, and wrong-site surgery
were the most common sentinelevents reported by the Joint Com-mission on Accreditation of Health-care Organizations (JCAHO) from2004 to 2011.1 These events areamong the most serious of medicalerrors, often leading to clinical mor-bidity, increased healthcare costs,and legal action. Both the patientand physician typically suffer signifi-cant emotional harm.
Wrong-site spine surgery (WSSS)occurs when a surgeon performs adecompression, resection, or recon-structive procedure on an unin-tended anatomic location along thespinal axis. WSSS encompasses bothwrong-level surgery (ie, an operationperformed on an incorrect vertebraor spinal motion segment) andwrong-side surgery.2-7 Surgical expo-sure of a spinal segment in proximityto the intended surgical level is com-mon and should not be considered awrong-site operation.
Despite ongoing efforts to preventWSSS, it continues to occur, with upto 50% of spine surgeons reporting
performance of at least one wrong-level operation during the course oftheir careers.7 The surgeon must re-main particularly vigilant againstwrong-level spine surgery (WLSS)given the challenge of intraoperativelocalization of the correct vertebralsegment. Precise identification of thecorrect spinal level requires special-ized knowledge and meticulous anal-ysis of radiographic imaging and an-atomic landmarks. Patient factorssuch as body habitus, spinal defor-mity, and variant vertebral morphol-ogy can introduce error or uncer-tainty with regard to the correctspinal level.8,9
Systems-based prevention is effec-tive for confirming the proper pa-tient and planned procedure andidentifying the appropriate region ofthe spinal column (ie, cervical, tho-racic, or lumbar).9,10 These preven-tion systems, however, cannot be re-lied on to establish the correctvertebral level during the operation.Accordingly, the use of preoperativechecklists is just one component ofthe overall approach to preventWSSS.
Mark A. Palumbo, MD
Aaron J. Bianco, MD
Sean Esmende, MD
Alan H. Daniels, MD
From the Department ofOrthopaedic Surgery, the WarrenAlpert Medical School of BrownUniversity, Providence, RI.
Dr. Palumbo or an immediate familymember is a member of a speakers’bureau or has made paidpresentations on behalf of andserves as a paid consultant toGlobus Medical, Stryker, andMedtronic and has receivedresearch or institutional support fromGlobus Medical. Dr. Daniels or animmediate family member hasreceived research or institutionalsupport from Synthes Spine andFlexuspine. Neither of the followingauthors nor any immediate familymember has received anything ofvalue from or has stock or stockoptions held in a commercialcompany or institution relateddirectly or indirectly to the subject ofthis article: Dr. Bianco andDr. Esmende.
J Am Acad Orthop Surg 2013;21:312-320
http://dx.doi.org/10.5435/JAAOS-21-05-312
Copyright 2013 by the AmericanAcademy of Orthopaedic Surgeons.
Review Article
312 Journal of the American Academy of Orthopaedic Surgeons

The spine surgeon is the solehealthcare provider with access toand knowledge of all the informationnecessary to identify the correct ver-tebral level or levels and the extentof pathology during surgery. Onlythe surgeon possesses the training tointerpret the preoperative and intra-operative imaging studies, correlatethe radiologic findings with surgicalanatomy, and execute a procedurethat addresses the pathologic lesion.Thus, the surgeon has primarily re-sponsibility for the design and imple-mentation of a patient-specific proto-col to ensure that the appropriateprocedure is performed at the correctlevel or levels and side of the spinalcolumn.
Historical Background
The JCAHO5 and the North Ameri-can Spine Society (NASS)10 have
published guidelines that promotecommunication among the surgicalteam, anesthesia providers, nursingstaff, and the patient to reduce therisk of performing an incorrect inva-sive procedure. In 2003, the JCAHOpromoted the Universal Protocol,which was designed to preventwrong-site, wrong-procedure, andwrong-person surgery.5 This protocolhas been endorsed by the AmericanAcademy of Orthopaedic Surgeonsand NASS. It emphasizes three mini-mum requirements: preoperative ver-ification, site marking, and a “timeout” in the operating room. SinceJuly 2004, all accredited hospitalsand ambulatory care and office-based surgery facilities have been re-quired to implement this protocol.
The NASS guidelines are dividedinto two parts. The Sign, Mark, &X-ray (SMaX) protocol10 is a check-list that can be used to guide the en-
tire surgical team through a series ofevents intended to decrease the po-tential for WSSS (Table 1). The sec-ond component is the Take-HomeSheet: Patient Diagnosis Diagram.This diagram is provided to the pa-tient and is designed to enhance thepatient’s understanding of the spinaldiagnosis and the surgical plan, withinstructions provided for identifica-tion of the site and side of surgery.NASS recommends that the patientpresent the sheet to all healthcareproviders on the day of surgery to re-duce the risk of WSSS.
Despite these prevention efforts,wrong-patient, wrong-site, orwrong-procedure events were stillthe most common sentinel eventsfrom 2004 to 2012, accounting for928 of 6,994 events (13.3%).1 Therate of wrong-site surgical proce-dures before and after implementa-tion of the Universal Protocol man-date appears unchanged11 and, evenunder optimal conditions, the proto-col may not prevent all cases ofwrong-site surgery.12
Little evidence exists to indicatethe effectiveness of the UniversalProtocol or the NASS guidelines indecreasing the rate of WSSS.3 Al-though these prevention systems rec-ommend obtaining an intraoperativeradiograph to confirm the correctspinal level, the subtleties of spinalsegment localization during surgeryare not addressed. Therefore, it isunlikely that the goal of eliminatingWSSS will be met by adhering solelyto the NASS guidelines or the Uni-versal Protocol.
Incidence
The true incidence of WSSS has beendifficult to quantify because of limi-tations in obtaining an accuratecount of events and patients at riskover a specific time period. Devineet al3 reviewed scientific evidence to
Table 1
North American Spine Society Sign, Mark, & X-ray (SMaX) Checklist
Involve the patient in confirming the surgical site either through informed consent orduring the actual marking. Surgeons are encouraged to personally obtain informedconsent. Copies of the surgical permit/informed consent form should state the siteand side of surgery and be shared with the patient, surgeon, anesthesiologist, assis-tant or scrub nurse, and circulating nurse.
Sign your name to the surgical site.Each member of the surgical team should verify the correct site.Verify that radiographs and medical records are for the correct patient, as well as con-
firming the identity of the patient.Each of the following items should be double checked against the marked site:
Medical recordRadiographs and other imaging studies (marked “L” or “R” to prevent being placed
backwards on the light box)Informed consentOperating room/anesthesia record
Consider having your assistant or scrub nurse always stand opposite the side wherethe surgeon should stand.
Consider or suggest obtaining an intraoperative radiograph after exposure, usingmarkers that do not move to confirm the vertebral level to be operated. Consider aradiology reading.
Complete all items listed. Relying on a single preventative effort only can result in er-rors.
Adapted from North American Spine Society: Sign, Mark & X-ray (SMax): Prevent wrong-sitesurgery. Available at: http://www.spine.org/Pages/PracticePolicy/ClinicalCare/Smax/Default.aspx.
Mark A. Palumbo, MD, et al
May 2013, Vol 21, No 5 313

determine the incidence of WSSS andfound that the overall strength of theevidence was poor. Despite the sub-optimal quality of evidence, severalstudies have reported that the inci-dence of wrong-level lumbar surgeryranges from 0.04 to 5.3%.2,3,7,11,13-15
In the only prospective investigationof WSSS, Ammerman et al16 reportedon a case series of lumbar diskec-tomy procedures and documented a15% rate of wrong-level exposurebut no cases of WSSS.
Kwaan et al12 analyzed the inci-dence of wrong-site surgery based onclaims submitted to a malpractice in-surer between 1985 and 2004. In to-tal, 1,426,901 inpatient surgical pro-cedures and 1,399,466 outpatientsurgical procedures were analyzed.Of the 40 cases of wrong-site surgeryidentified, 15 (37.5%) involved thewrong level or wrong side of the ver-tebral column. Among the reviewedspine cases, 7 of 10 were lumbar op-erations, 5 of which involved anoma-lous lumbosacral anatomy. In threecases, intraoperative imaging wasnot used.
Jhawar et al14 surveyed neurosur-geons regarding their experiencewith WSSS in a series of 4,695 lum-bar and 2,649 cervical diskectomies.The incidence of wrong-level lumbarsurgery was 12.8 per 10,000 proce-dures, and the incidence of wrong-level cervical surgery per 10,000 cer-vical diskectomy and craniotomyprocedures was 7.6 and 2.0, respec-tively. In this 2007 study, only 68%of surgeons reported using intraoper-ative radiographs for lumbar disksurgery.
Groff et al17 reported on the resultsof a survey of neurosurgeons withregard to their experience withwrong-level lumbar surgery. Of 569respondents, 175 (31.5%) reportedperforming surgery at the wronglumbar level once; 72 (13.6%) per-formed surgery at the wrong lumbarlevel more than once; 53 (9.3%) per-
formed surgery on the wrong sideonce; and 6 (1.1%) performed sur-gery on the wrong side more thanonce. In 67.8% of cases in whichwrong-level or wrong-side surgerywas performed, the error was identi-fied intraoperatively, and the correctsurgery was executed.
Mody et al7 also conducted a sur-vey of neurosurgeons’ experiencewith regard to WLSS. The authorsreceived 415 responses to more than3,000 surveys sent to neurosurgeons(12% response rate). Fifty percent(207) of those surveyed reported per-forming one or more wrong-level op-erations during their career. Therewas a significant reduction in the an-nual risk for WLSS associated withincreased duration of practice (P <0.001). No significant difference wasfound in the reported WLSS rate forsurgeons in academic versus privatepractice or for surgeons with higherannual surgical load.
In a retrospective study of Ameri-can Board of Orthopaedic Surgerycandidates from 1999 to 2010, thenumber of wrong-site surgeries per-formed by candidates eligible forboard certification was assessed.11 Atotal of 897 orthopaedic spine sur-geons submitted 324,085 spinal pro-cedures during the study period.Thirty-one surgeons (3.5%) reporteda WSSS during their 6-month collec-tion period, for an overall estimatedWSSS rate of 0.041%. Of the 26wrong-level spine procedures re-ported, 14 cases involved the lumbarspine, 2 involved the thoracic spineand 8 involved the cervical spine. In-traoperative radiographs were ob-tained in all cases. Misinterpretationof the radiograph by the surgeon wasthe most common reason given forwrong-level cervical and lumbar sur-gery.
Minimally invasive and endoscopicspine surgery may also contribute toWLSS. Matsumoto et al15 conducteda survey of the members of the Japa-
nese Orthopaedic Society. Of 6,239endoscopic spinal procedures per-formed in 2007, 6 wrong-level oper-ations and 1 wrong-side operationwere reported. We believe that un-recognized movement of the tubularretractor during minimally invasiveprocedures may contribute to inter-vention at the wrong spinal level.
Risk Factors
The overall strength of the dataavailable to establish the risk factorsfor WSSS has been rated as “low.”3
Potential factors that contribute toWSSS include emergent surgery, pa-tient factors (eg, morbid obesity), an-atomic variations secondary to de-formity or previous surgery, timepressure to initiate or complete sur-gery, unusual equipment or setup,multiple surgeons involved in thesurgery, multiple procedures beingperformed during a single surgery,and communication breakdownbetween the surgical team andthe patient and/or the patient’sfamily.2,3,7,11,14,17-20 WLSS has alsobeen associated with failure to local-ize the correct vertebral level with anintraoperative radiograph.5 Evenwhen a spinal radiograph is ob-tained, performance of a procedureat an incorrect level may not be obvi-ated because the surgeon may misin-terpret the radiograph.4,11
Repercussions
As stated previously, WSSS can haveserious medical, legal, and emotionalconsequences. From a clinical stand-point, the pathologic process and thepatient’s symptomatology are not ad-dressed in the setting of WSSS.Incorrect-side or -level decompres-sion will traumatize the paraspinalsoft tissues, disrupt the osseoliga-mentous stabilizing structures, andproduce epidural fibrosis. Unplanned
Wrong-site Spine Surgery
314 Journal of the American Academy of Orthopaedic Surgeons

tissue disruption may subject the pa-tient to increased postoperative pain,prolonged recovery, and an acceler-ated degenerative process at thewrong surgical site. In the case ofwrong-level arthrodesis, the addedlevel of fusion and/or instrumenta-tion may adversely affect spinal bio-mechanics and increase the potentialfor adjacent segment degeneration. Ifnot detected intraoperatively, WSSSwill delay execution of the correctprocedure and symptom resolution.
Although many cases of WSSS gounreported, this complication canand often does result in legal action.Therefore, WSSS identified intraop-eratively (with the correct procedureultimately performed) must be distin-guished from WSSS identified post-operatively in which the pathoanat-omy is not addressed. These twosituations may have different clinicaloutcomes; however, no studies havereported on the relative risk of subse-quent litigation. Goodkin and Laska5
reported on data from 69 cases ofWLSS from 1984 to 2000. Thirty-seven cases were settled; a plaintiffverdict was rendered in 18, and a de-fense verdict was rendered in 13. In-demnity payments ranged from$62,000 to $1,500,000.
In addition to legal consequences,emotional and social harm often resultsfrom WSSS. Patients may suffer sub-stantial despair and psychologic dis-tress and may lose trust not only in thesurgeon but possibly in all physicians.The responsible surgeon may experi-ence embarrassment, guilt, and fear.The situation is often perceived as thephysician’s worst nightmare because ofthe impending personal, professional,and legal repercussions.21
Strategies to AchieveCorrect Site Surgery
To avoid WSSS, the JCAHO andNASS guidelines must be supple-
mented with a surgeon-driven,patient-specific protocol.
Preoperative PlanningFor all nonemergent cases, a specificsurgical plan should be establishedwell in advance of the date of sur-gery. This requires the surgeon to an-alyze all relevant radiographic stud-ies and to specify the procedure,laterality, and the exact vertebrallevel or levels to be addressed. Alongwith advanced neuroradiographicimaging, the surgeon should obtainspecific plain radiographic views ofthe spine preoperatively; these viewswill be compared with the sameviews obtained intraoperatively forlocalization purposes during surgery.The planned surgical level or levelsmust be identified on plain radio-graphs after correlation with themagnetic resonance images and/orCT myelogram. The radiologist’s in-terpretation should never be used inisolation; images should be directlyinterpreted by the surgeon.22 The tech-nical plan documented in the outpa-tient office record should be transferredaccurately to the surgical consent andthe hospital medical record.
On the day of surgery, the surgeonshould review all pertinent documen-tation (eg, office notes, surgical con-sent, history, physical examination)before proceeding with the JCAHOand/or NASS protocol. The neurora-diographic studies and plain radio-graphs should be displayed in theoperating room throughout the pro-cedure. Confirmation of the correctpatient name and study date is man-datory. The level or levels and later-ality of the pathoanatomy should becorrelated with the patient’s symp-toms and signs. It is useful to markthe intended surgical level or levelson the preoperative plain radio-graphs and to display a written sur-gical plan that can be referenced byall operating room personnel.
Intraoperative LocalizationPrinciplesAccording to the American Academyof Orthopaedic Surgeons, “Spinalsurgery done at the wrong level canbe prevented with an intraoperativex-ray that marks the exact vertebrallevel (site) of surgery.”23 However, noconsensus exists regarding the spe-cific radiologic protocol, and consid-erable variability exists in the sur-geon’s methodology for spinalsegment localization.17
Radiographic localization is a criti-cal step in performing spine surgeryat the correct level. When the pathol-ogy is unclear based on the patient’sanatomy or a previous procedure, aradiograph can be obtained beforethe incision is made, with a ra-diopaque skin marker used to con-firm appropriate incision placement.After dissection to the spinal column,radiographic imaging is performedwith a metallic instrument attachedto a fixed osseous structure. This ra-diograph should be compared to theanalogous preoperative image toconfirm the correct surgical site.
Accurate radiographic identifica-tion of the correct vertebral levelmay pose a significant challenge evenfor the experienced spine surgeon.This is particularly true for spinallevels at a distance from the lum-bosacral or craniocervical junction.In cases of difficult localization, thepotential for misinterpretation canbe reduced by obtaining another in-terpretation of the image by a secondsurgeon or a radiologist.
It is important to note that obtaininga radiograph does not guarantee thatsurgery will be performed at the correctlevel. Limitations of intraoperative ra-diography include (1) image misinter-pretation secondary to variant spinalanatomy and/or incorrect counting ofthe spinal level; (2) suboptimal imagequality related to inadequate film ex-posure, body habitus, or the surgical
Mark A. Palumbo, MD, et al
May 2013, Vol 21, No 5 315

table; and (3) failure to recognize theabsence of expected pathology at thesurgical level.5,24
Cervical Spine LocalizationIn most cases, accurate localizationof a cervical level can be achieved us-ing a combination of anatomic land-marks and a lateral radiograph ofthe cervical spine. For the anteriorcervical approach, palpation of thecarotid tubercle on C6 can serve as aguide to the adjacent C5-6 and C6-7disk spaces. Prominent ventral endplate osteophytes at or adjacent tothe planned surgical level also can beused as a preliminary guide to thecorrect disk space or spaces. Al-though identification of osseouslandmarks is useful, it should beviewed as a preliminary step in thelocalization process.
A lateral radiograph of the spineshould be obtained after the diskspace is marked to definitively iden-tify the correct surgical level. Meth-ods to verify the correct level include
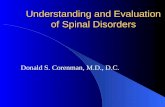
(1) placing a distractor pin in the ver-tebral body above or below the disk,(2) affixing a clamp to the anteriorlongitudinal ligament, or (3) placinga bent spinal needle into the selecteddisk space (Figure 1, A). Methodsthat do not penetrate the annuluscan theoretically prevent iatrogenicinjury to the disk when an unin-tended level is initially marked. Oncethe correct disk space is confirmedon imaging, electrocautery is used tomark the annulus.
For a posterior approach, the largeand often palpable C2 and T1spinous processes can be used forpreliminary localization in the upperand lower cervical spine, respec-tively. The endomorphic patient witha short neck poses a specific chal-lenge to definitive radiographic lo-calization (Figure 1, B). Althoughplacing traction on the shoulders us-ing tape can be helpful for visualiz-ing the lower cervical levels, it maynot be possible to obtain lateral im-ages that are adequate for localiza-
tion purposes. During posterior sur-gery at the cervicothoracic junction,the challenge of localizing levels canoften be overcome by obtaining anAP radiograph with a marker placedat the T1 spinous process. The firstthoracic vertebra can be easily identi-fied by its large lamina and trans-verse processes, which articulatewith the first rib. An alternative ap-proach involves attaching an instru-ment to a more cranial spinous pro-cess, which is visible on a lateralradiograph. Counting spinous pro-cesses downward to determine thecorrect spinal level is effective but re-quires additional exposure of uppercervical segments.
Cervical anomalies, such as con-genital fusion of vertebrae associatedwith Klippel-Feil syndrome, maylead to WLSS. A block vertebra atC2-C3 may lead the surgeon to mis-take the C3 body for the C2 body.Identification of this abnormality onpreoperative images and due dili-gence during surgery are required toavoid a wrong-level procedure.
Thoracic LocalizationThoracic spine pathology withoutassociated radiologic abnormality(eg, thoracic disk herniation, epi-dural space-occupying lesion) re-quires special consideration. Preoper-ative MRI must include a sagittalview that spans from the sacrum tothe thoracic level of interest. WhenMRI is contraindicated, a CT myelo-gram of the spine with enlarged APand lateral scout radiographs andnumbered vertebral levels should beobtained. The enlarged view of thesagittal magnetic resonance image orthe scout radiographs must be avail-able to the surgeon before and dur-ing surgery.
Identification of the pathologiclevel on preoperative plain radio-graphs is a mandatory step in achiev-ing accurate intraoperative localiza-
Definitive identification of the surgical level achieved using a lateralradiograph of the spine. A, Intraoperative lateral radiograph of the cervicalspine demonstrating the placement of a bent spinal needle in the C5-6 diskspace for cervical localization. B, Intraoperative lateral radiograph of thecervical spine in a patient with a short neck. Note the incomplete imaging ofC6, C7, and T1 on this view, which makes it inadequate for identifying lowerspinal levels.
Figure 1
Wrong-site Spine Surgery
316 Journal of the American Academy of Orthopaedic Surgeons

tion. Preoperative AP and laterallong-cassette scoliosis radiographsare useful for identifying variation inthe usual number of 12 rib-bearingthoracic vertebrae and 5 non-rib–bearing lumbar vertebrae. If full-length films of the entire spinal axisare not available, then large-cassetteAP and lateral radiographs that spanfrom the pelvis to the level of tho-racic pathology typically will be ade-quate. The preoperative plain radio-graphs must be correlated to the
screening neuroradiologic image todefine the appropriate level beforethe day of surgery. The pathologicvertebral segment or segmentsshould be identified on both AP andlateral projections by counting levelsup from the sacrum based on thepreoperative sagittal magnetic reso-nance image.
To avoid counting error, the samepreoperative localization methodshould be repeated at the time of sur-gery (Figure 2). A standard intraop-
erative counting method involvesplacement of a radiopaque marker ata fixed point in the thoracic spineand then counting up from the sa-crum to the level of interest. If cas-sette size is limited, it may be neces-sary to obtain serial fluoroscopic orplain radiographic images, withmarkers placed at intervals spanningmultiple vertebrae. Localization ofthe relevant level on an AP radio-graph may be necessary for proce-dures performed with the patient inthe decubitus position and when dif-ficulty in obtaining a high-qualitylateral radiograph is anticipated (eg,upper thoracic pathology, morbidlyobese patient).
Several methods to improve the ac-curacy of thoracic localization havebeen described, including the use of ra-diopaque skin markers,25 methyleneblue dye injection,26 and oblique ra-diographs.27 Although these methodsmay be useful in select cases as an ad-junct to standard radiographic meth-ods, they do not guarantee correct lo-calization. Skin markers cannot berelied on because the skin moves rela-tive to fixed osseous structures duringthe positioning process. Methylene bluedye may be neurotoxic and should beinjected only superficially; dye spreadinto the subcutaneous tissue layer cancompromise precise identification of aspinal level. Oblique radiographicviews avoid beam penetration throughmuch of the torso and shoulder mus-culature and may aid the surgeon in vi-sualizing the cervicothoracic junction.However, poor bone quality, non-prone patient positioning, and ana-tomic anomalies may make this strat-egy insufficient for prevention oflocalization errors.
More invasive methods of ensuringaccurate intraoperative localizationhave been proposed. Preoperative in-jection of barium-infused polymethylmethacrylate cement into a vertebralbody is one such strategy.28 Anothermethod of localization before surgical
Imaging studies demonstrating thoracic counting error as a result of countingfrom C2 rather than counting from the sacrum. A, Sagittal T2-weightedmagnetic resonance image demonstrating a lesion involving a verterbal body.When counted caudally from C2, the lesion is described as a T7 lesion.B, Sagittal CT scan of the spine in the same patient. When countingcephalad from the sacrum, the same lesion is described as a T8 lesion.(Reproduced with permission from Hsu W, Kretzer RM, Dorsi MJ, GokaslanZL: Strategies to avoid wrong-site surgery during spinal procedures.Neurosurg Focus 2011;31[4]:E1-5.)
Figure 2
Mark A. Palumbo, MD, et al
May 2013, Vol 21, No 5 317

intervention involves placement of a ra-diopaque coil adjacent to the desiredthoracic pedicle.29 A third alternativedescribed by Upadhyaya et al30 con-sists of preoperative CT-guided fidu-cial screw placement in the thoracicspine. When MRI or localizing fluo-roscopy is not obtainable, such as incases of extreme obesity, CT-guidedplacement of a metallic bead withinthe posterior elements may be per-formed for spinal level localization.Concerns regarding these strategiesinclude exposure of the patient to asecond invasive procedure, potentialcomplications associated with thesupplemental localization technique,and additional financial cost.
Lumbosacral LocalizationAlthough localization in the lumbarregion typically is straightforward,two factors warrant heightenedawareness. The first relates to theprevalence of monoradiculopathy,
which requires a unilateral decom-pressive procedure. As a supplementto the JCAHO and NASS protocols,the correct surgical side should beverified by directly questioning thepatient in the operating room. Thepatient’s response is then correlatedwith the preoperative documentationof the laterality of symptoms and thepathoanatomy as identified on neu-roradiologic imaging studies.
The second factor is the presenceof a lumbosacral transitional verte-bra (LSTV), a relatively commoncongenital anomaly that may resultin WLSS. The overall reported preva-lence ranges from 4% to 35.6% inthe general population.8,9,24,31
In the most common form ofLSTV, the fifth lumbar segmentshows signs of assimilation to the sa-crum, a condition termed sacraliza-tion. Lumbarization refers to anoma-lous osseous morphology in whichthe first sacral vertebra shows signs
of transition to a lumbar configura-tion. These spinal abnormalitiesmust be identified on preoperativeplain radiographs to plan the intra-operative localization process. Con-sistent nomenclature referring to the“last lumbar motion segment” mayassist in communication and docu-mentation. Diligent review and cor-relation of the preoperative MRI (orCT myelogram) with the AP and lat-eral radiographs is especially impor-tant in the setting of variant lum-bosacral anatomy.
A logical protocol for intraopera-tive lumbosacral localization duringa posterior approach involves the useof the iliac crest as a surface land-mark to approximate the L4-5 diskspace (Figure 3, A). A sterile, 18-gauge 3.5-inch-long spinal needle isplaced percutaneously at the approx-imated level of surgery. Preferably,the needle is embedded in a bonystructure such as a spinous process.
Lateral radiographs of the spine demonstrating lumbar localization via three methods. A, Localization is performed viapercutaneous placement of a spinal needle at the level of the L4 spinous process. Indigo carmine dye is then injectedto mark the spinous process before the incision is made to aid in the approach. B, A clamp is placed on the L4spinous process, indicating the correct level for decompression. C, Lumbar diskectomy localization is confirmed byinserting a Penfield 4 elevator within the L4-5 disk space to confirm the appropriate level of the performed diskectomy.
Figure 3
Wrong-site Spine Surgery
318 Journal of the American Academy of Orthopaedic Surgeons

A lateral radiograph of the spineprovides precise localization of theincision based on the position of theneedle relative to the pathologic spi-nal motion segment. Injection of in-digo carmine dye to mark the rele-vant spinous process before creatingthe incision can be helpful. After dis-section and exposure of the lamina,the vertebral level is definitively iden-tified by obtaining a second lateralradiograph after a clamp is attachedto the spinous process or a probe isplaced within the interlaminar space(Figure 3, B). If the pathologic lesionis not obvious during the decompres-sive procedure, a final radiographmay be obtained with a radiopaquemarker situated within the disk space(Figure 3, C). Marking the pedicle byplacing a clamp on the appropriatetransverse process may also be help-ful in arthrodesis procedures.
Intraoperative CTIntraoperative CT is increasinglyused to guide screw placement in thecervical,32 thoracic,33,34 and lumbosacralspine.35,36 Although this imaging mo-dality appears to improve the accu-racy of instrumentation place-ment,33,36 routine use of CT forvertebral level localization is not prac-tical. If the surgeon anticipates a chal-lenging localization process (secondaryto anatomic anomaly or complex de-formity), intraoperative CT may be ap-propriate. However, the potential ben-efit must be weighed against thefinancial cost and a significant increasein radiation exposure to the patient andsurgical personnel.
Procedure FollowingWSSS Identification
When WSSS does occur, the risk-management department of the hos-pital should be contacted immedi-ately. The surgeon should accuratelyrecord the events in the medical re-
cord.23 The patient and, when appro-priate, the patient’s family should benotified of the incident. Discrete dis-closure to patients and families as-sists in retaining their trust in thesurgeon, decreases the likelihood oflitigation, and initiates the healingprocess for both surgeon and pa-tient.37 Hospital systems may havesupport systems in place for the sur-geon, operating room staff, and thepatient involved in the incident.21
Summary
WSSS is a potentially devastating eventfor the patient and the surgeon. Despitemajor efforts aimed at prevention,wrong-site spinal operations continueto occur, with the potential for seriousmedical, personal, and legal repercus-sions. Systems-based prevention meth-ods are effective in identifying theproper patient, the correct region of thespinal column, and the planned proce-dure. However, these standardized pro-tocols cannot be relied upon to estab-lish the correct vertebral level duringthe operation. The spine surgeon is theonly healthcare provider with access toall the information necessary to iden-tify the correct spinal segment at thetime of surgery. Thus, the JCAHO andNASS guidelines must be supplementedby a patient-specific protocol designedand implemented by the surgeon to en-sure that the appropriate operation isperformed at the correct site within thespinal column.
References
Evidence-based Medicine: Levels ofevidence are described in the table ofcontents. In this article, there are nolevel I studies. References 3 and 16 arelevel II studies. References 8, 13, 30,and 32-37 are level III studies.References 1, 2, 5, 7, 9, 11, 12, 14, 15,17, 18, 24, and 26-29 are level IV
studies. References 10, 20-23, 25, and31 are level V expert opinion.
References printed in bold type arethose published within the past 5 years.
1. The Joint Commission: Summary data ofsentinel events reviewed by the JointCommission: December 31, 2012.Available at: http://www.jointcommission.org/sentinel_event_statistics_quarterly.Accessed February 28, 2013.
2. Ammerman JM, Ammerman MD:Wrong-sided surgery. J Neurosurg Spine2008;9(1):105-106.
3. Devine J, Chutkan N, Norvell DC,Dettori JR: Avoiding wrong site surgery:A systematic review. Spine (Phila Pa1976) 2010;35(9 suppl):S28-S36.
4. Fager CA: Malpractice issues inneurological surgery. Surg Neurol 2006;65(4):416-421.
5. Goodkin R, Laska LL: Wrong disc spacelevel surgery: Medicolegal implications.Surg Neurol 2004;61(4):323-342.
6. Hsu W, Kretzer RM, Dorsi MJ,Gokaslan ZL: Strategies to avoid wrong-site surgery during spinal procedures.Neurosurg Focus 2011;31(4):E5.
7. Mody MG, Nourbakhsh A, Stahl DL,Gibbs M, Alfawareh M, Garges KJ: Theprevalence of wrong level surgery amongspine surgeons. Spine (Phila Pa 1976)2008;33(2):194-198.
8. Apazidis A, Ricart PA, Diefenbach CM,Spivak JM: The prevalence oftransitional vertebrae in the lumbarspine. Spine J 2011;11(9):858-862.
9. Harmon PH: Congenital and acquiredanatomic variations, includingdegenerative changes of the lowerlumbar spine; role in production ofpainful back and lower extremitysyndromes. Clin Orthop Relat Res 1966;44:171-186.
10. North American Spine Society: Sign,Mark & X-ray (SMax): Prevent wrong-site surgery. Available at: http://www.spine.org/Pages/PracticePolicy/ClinicalCare/Smax/Default.aspx.Accessed February 28, 2013.
11. James MA, Seiler JG III, Harrast JJ, Em-ery SE, Hurwitz S: The occurrence ofwrong-site surgery self-reported bycandidates for certification by theAmerican Board of Orthopaedic Surgery.J Bone Joint Surg Am 2012;94(1):e2(1-12).
12. Kwaan MR, Studdert DM, Zinner MJ,Gawande AA: Incidence, patterns, andprevention of wrong-site surgery. ArchSurg 2006;141(4):353-358.
13. Barrios C, Ahmed M, Arrótegui J,
Mark A. Palumbo, MD, et al
May 2013, Vol 21, No 5 319

Björnsson A, Gillström P: Microsurgeryversus standard removal of the herniatedlumbar disc: A 3-year comparison in 150cases. Acta Orthop Scand 1990;61(5):399-403.
14. Jhawar BS, Mitsis D, Duggal N: Wrong-sided and wrong-level neurosurgery: Anational survey. J Neurosurg Spine 2007;7(5):467-472.
15. Matsumoto M, Hasegawa T, Ito M,et al: Incidence of complicationsassociated with spinal endoscopicsurgery: Nationwide survey in 2007 bythe Committee on Spinal EndoscopicSurgical Skill Qualification of JapaneseOrthopaedic Association. J Orthop Sci2010;15(1):92-96.
16. Ammerman JM, Ammerman MD,Dambrosia J, Ammerman BJ: Aprospective evaluation of the role forintraoperative x-ray in lumbardiscectomy: Predictors of incorrect levelexposure. Surg Neurol 2006;66(5):470-474.
17. Groff MW, Heller JE, Potts EA,Mummaneni PV, Shaffrey CI, Smith JS:A survey-based study of wrong-levellumbar spine surgery: The scope of theproblem and current practices in place tohelp avoid these errors. WorldNeurosurg 2012;April 2 [epub ahead ofprint].
18. A follow-up review of wrong-sitesurgery. Sentinel Event Alert 2001;24:1-3.
19. Patient safety first alert: Implementing acorrect site surgery policy and procedure.AORN J 2002;76(5):785-788.
20. Pheasant H: Sources of failure inlaminectomies. Orthop Clin North Am1975;6(1):319-329.
21. Ring DC, Herndon JH, Meyer GS: Caserecords of The Massachusetts GeneralHospital: Case 34-2010. A 65-year-oldwoman with an incorrect operation onthe left hand. N Engl J Med 2010;363(20):1950-1957.
22. Young PM, Berquist TH, Bancroft LW,Peterson JJ: Complications of spinalinstrumentation. Radiographics 2007;27(3):775-789.
23. American Academy of OrthopaedicSurgeons: Information statement:Wrong-site surgery. Available at: http://www6.aaos.org/news/PDFopen/PDFopen.cfm?page_url=http://www.aaos.org/about/papers/advistmt/1015.asp. Revised December 2008.Accessed February 28, 2013.
24. Konin GP, Walz DM: Lumbosacraltransitional vertebrae: Classification,imaging findings, and clinical relevance.AJNR Am J Neuroradiol 2010;31(10):1778-1786.
25. Rosahl SK, Gharabaghi A, Liebig T,Feste CD, Tatagiba M, Samii M: Skinmarkers for surgical planning forintradural lesions of the thoracic spine:Technical note. Surg Neurol 2002;58(5):346-348.
26. Paolini S, Ciappetta P, Missori P, RacoA, Delfini R: Spinous process marking: Areliable method for preoperative surfacelocalization of intradural lesions of thehigh thoracic spine. Br J Neurosurg2005;19(1):74-76.
27. Singh H, Meyer SA, Hecht AC, JenkinsAL III: Novel fluoroscopic technique forlocalization at cervicothoracic levels.J Spinal Disord Tech 2009;22(8):615-618.
28. Hsu W, Sciubba DM, Sasson AD, et al:Intraoperative localization of thoracicspine level with preoperativepercutaneous placement of intravertebralpolymethylmethacrylate. J Spinal DisordTech 2008;21(1):72-75.
29. Binning MJ, Schmidt MH: Percutaneousplacement of radiopaque markers at thepedicle of interest for preoperativelocalization of thoracic spine level. Spine(Phila Pa 1976) 2010;35(19):1821-1825.
30. Upadhyaya CD, Wu JC, Chin CT,Balamurali G, Mummaneni PV:Avoidance of wrong-level thoracic spinesurgery: Intraoperative localization with
preoperative percutaneous fiducial screwplacement. J Neurosurg Spine 2012;16(3):280-284.
31. O’Connor JF, Cranley WR, McCartenKM, Radkowski MA: Radiographicmanifestations of congenital anomaliesof the spine. Radiol Clin North Am1991;29(2):407-429.
32. Hecht AC, Koehler SM, Laudone JC,Jenkins A, Qureshi S: Is intraoperativeCT of posterior cervical spineinstrumentation cost-effective and does itreduce complications? Clin Orthop RelatRes 2011;469(4):1035-1041.
33. Ughwanogho E, Patel NM, Baldwin KD,Sampson NR, Flynn JM: Computedtomography-guided navigation ofthoracic pedicle screws for adolescentidiopathic scoliosis results in moreaccurate placement and less screwremoval. Spine (Phila Pa 1976) 2012;37(8):E473-E478.
34. Cui G, Wang Y, Kao TH, et al:Application of intraoperative computedtomography with or without navigationsystem in surgical correction of spinaldeformity: A preliminary result of 59consecutive human cases. Spine (PhilaPa 1976) 2012;37(10):891-900.
35. Houten JK, Nasser R, Baxi N: Clinicalassessment of percutaneous lumbarpedicle screw placement using the O-armmultidimensional surgical imagingsystem. Neurosurgery 2012;70(4):990-995.
36. Costa F, Cardia A, Ortolina A, Fabio G,Zerbi A, Fornari M: Spinal navigation:Standard preoperative versusintraoperative computed tomographydata set acquisition for computer-guidance system. Radiological andclinical study in 100 consecutivepatients. Spine (Phila Pa 1976) 2011;36(24):2094-2098.
37. Kachalia A, Kaufman SR, Boothman R,et al: Liability claims and costs beforeand after implementation of a medicalerror disclosure program. Ann InternMed 2010;153(4):213-221.
Wrong-site Spine Surgery
320 Journal of the American Academy of Orthopaedic Surgeons