
Wound Care Binders & Bandages Use of Heat and Cold Module 8, Part A, B and C.
99
Wound Care Binders & Bandages Use of Heat and Cold Module 8, Part A, B and C
-
Upload
garry-daniel-blair -
Category
Documents
-
view
213 -
download
0
Transcript of Wound Care Binders & Bandages Use of Heat and Cold Module 8, Part A, B and C.

Wound CareBinders & Bandages
Use of Heat and Cold
Module 8, Part A, B and C
WHY IS WOUND CARE DONE?WHY IS WOUND CARE DONE?
General purposes of dressings• Protecting a wound from microorganism
contamination• Aiding hemostasis• Promoting healing by absorbing drainage and
debriding a wound• Supporting or splinting the wound site• Protecting the client from seeing the wound• Promoting thermal insulation to the wound surface• Providing maintenance of high humidity between
the wound and dressing

Definitions
• Abscess – a cavity containing pus and surrounded by inflamed tissue, formed as a result of suppuration in a localized infection. Healing usually occurs when an abscess drains or is incised.
• Collagen – a protein consisting of bundles of tiny reticular fibrils, which combine to form the white, glistening, inelastic fibers of tendons, ligaments, and fasciae.

• Debridement – removal of dirt, foreign objects, damaged or dead tissue, and cellular debris from a wound or a burn to prevent infection and to promote healing.
• Eschar – a scab or dry crust resulting from a thermal or chemical burn, infection, or excoriating skin disease.
• Exudate – fluid, cells, or other substances that have been slowly exudated, or discharged, from cells or blood vessels through small pores or breaks in cell membranes. Perspiration, pus, and serum are sometimes identified as exudates.

• Fibroblast – a flat, elongated undifferentiated cell in the connective tissue that gives rise to various precursor cells, such as the chondroblast, collagenoblast, and osteoblast, that form the fibrous, binding, and supporting tissue of the body.
• Fistula – an abnormal passage from an internal organ to the body surface or between two internal organs, caused by a congenital defect, injury, infection, the spreading of a malignant lesion, radiotherapy of a cancerous growth, or trauma during childbirth.
• Granulation – any soft, pink, fleshy projections that form during the healing process in a wound not healing by first intention.

• Inflammation – the protective response of the tissues of the body to irritation or injury.– May be acute or chronic; its cardinal signs are redness,
heat, swelling, and pain, accompanied by loss of function.
• Maceration – the softening and breaking down of skin from prolonged exposure to moisture. – May be caused by prolonged exposure to amniotic
fluid in a post term infant or dead fetus.
• Necrosis – localized tissue death that occurs in-groups of cells in response to disease or injury.
• Pus – a creamy, viscous, pale yellow, or yellow-green fluid exudate that is the result of fluid remains of liquefactive necrosis of tissues. Bacterial infection is its most common cause.
• Purulent – producing or containing pus.• Regeneration – new growth• Sanguineous – pertaining to blood or containing
blood.• Serous – pertaining to, resembling, or producing
serum.• Serosanguineous – thin and red; composed of
serum and blood.• Ulceration – the process of ulcer formation
Review of A&P
• Skin is the body’s largest organ
• Functions1. protective barrier
2. sensory organ for pain temperature and touch
3. synthesize vitamin D
• Two layers– separated by membrane dermal-epidermal junction
1. epidermis
2. dermis

Stages of wound healing
1. Inflammatory Phase – begins within minutes of injury and lasts about 3 days.
2. Destructive Phase (granulation) – begins before inflammation ends and lasts for about 2-5 days.
3. Proliferative Phase (granulation) – begins and lasts from 3-24 days.
4. Maturation Phase – the final stage of healing and may take more than a year

Stages of wound healing Inflammatory Phase
• Reparative processes control bleeding (hemostasis), deliver blood and cells to the injured area, and form epithelial cells at the injury site.
• During hemostasis, injured blood vessels constrict and platelets gather to stop bleeding.
• Clots form a fibrin matrix that later provides a framework for cellular repair.
Inflammatory Phase
• Damaged tissue and mast cells secrete histamine, resulting in vasodilatation of surrounding capillaries and exudation of serum and WBC’s into damaged tissues resulting in localized redness, edema, warmth & throbbing

Inflammatory Phase
• Leukocytes reach the wound within a few hours. The primary WBC is the neutrophil, which begins to ingest bacteria and small debris.
• The second WBC is the monocyte, which transforms into macrophages, which clean a wound of bacteria, dead cells, and debris by phagocytosis.

Inflammatory Phase
• After macrophages clean the wound and make it ready for tissue repair, epithelial cells gather under the wound space for about 48 hours forming a barrier against infectious organisms and toxic materials.
Stages of wound healing Destructive Phase (granulation)
• Begins before inflammation ends
• Lasts for about 2-52-5 days.
• Macrophages continue the process of cleaning the wound, attracting more macrophages, and stimulating formation of fibroblasts, the cells that synthesize collagen.
• Collagen can be found as early as the second day and is the main component of scar tissue, it provides strength and structural integrity to a wound.

Stages of wound healing Proliferative Phase (granulation)
• Lasts from 3-24 days.
• During this period the wound begins to close with new tissue.
• As reconstruction progresses, the tensile strength of the wound increases, and the risk of wound separation or rupture is less likely.

Stages of wound healing Maturation Phase
• Final stage of healing
• May take more than a year, depending on the depth and extent of the wound.
• Collagen scar continues to gain strength and undergoes remodeling or organization before assuming their normal appearance.
• A healed wound usually does not have the strength of the tissue it replaces
Types of wound healing
Can be •Primary•Secondary•Tertiary

Types of wound healing
Primary Intention – refers to wounds where there is not tissue loss and skin edges are well approximated.
These wounds have a low risk of infection and heal quickly, with little scarring i.e). surgical incision

Types of wound healing
Secondary Intention – refers to wounds where there is tissue loss and the skin edges are not approximated, such as in a pressure ulcer
These wounds tend to heal slowly and have a higher rate of infection.
Types of wound healing
Tertiary Intention – can be called delayed primary intention or third-intention healing, refers to surgical incisions that are left open because of edema or infection or to allow drainage, and are then closed to heal.


Handout: Factors affecting wound healing
1. Age 2. Malnutrition3. Obesity4. Impaired oxygenation 5. Smoking 6. Drugs 7. Diabetes8. Radiation9. Wound stress
Complications of Wound Healing
HemorrhageHemorrhage InfectionInfection DehiscenceDehiscence Evisceration:Evisceration: Fistula Fistula Delayed Wound HealingDelayed Wound Healing

Hemorrhage
• Bleeding from wound site is normal during & immediately after the initial trauma.
• Hemostasis occurs within several minutes unless large vessels are involved or the pt has impaired clotting function
• Bleeding after hemostasis could indicate:slipped suture dislodged clot infection erosion of a blood vessel by a foreign object (ie a
drain).

Hemorrhage
• Can occur internally or externally. – Internal can be detected by observing for
distention, swelling, change in the type or amount of drainage or signs of hypovolemic shock Hematoma – a localized collection of blood under the tissues.
– External – more obvious, all wounds monitored, esp surgical wounds for the 1st 24 – 48hrs post-op
Infection• Wound infection is 2nd most common nosocomial
infection• Chances of wound infection are greater
– when the wound contains dead or necrotic tissue, – when there are foreign bodies in or near the wound,– and when blood supply & local tissue defenses are
reduced
• A contaminated or traumatic wound may show signs of infection early (within 2-3days)
• A surgical wound infection does not develop until the 4th or 5th day
Dehiscence• Partial or total separation of wound layers• When a wound fails to heal properly, the layers of skin &
tissue may separate• Most commonly occurs during the 3rd to 11th day (before
collagen formed)• Those at risk:
– Obese (stain placed on wounds & fatty tissue heals poorly)
• Often occurs with straining (coughing, vomiting, sitting up, walking)
• Pt will report feeling of “something's given way”• Increase in serosanguineous drainage from a wound, think
Dehiscence (may lead to evisceration…)
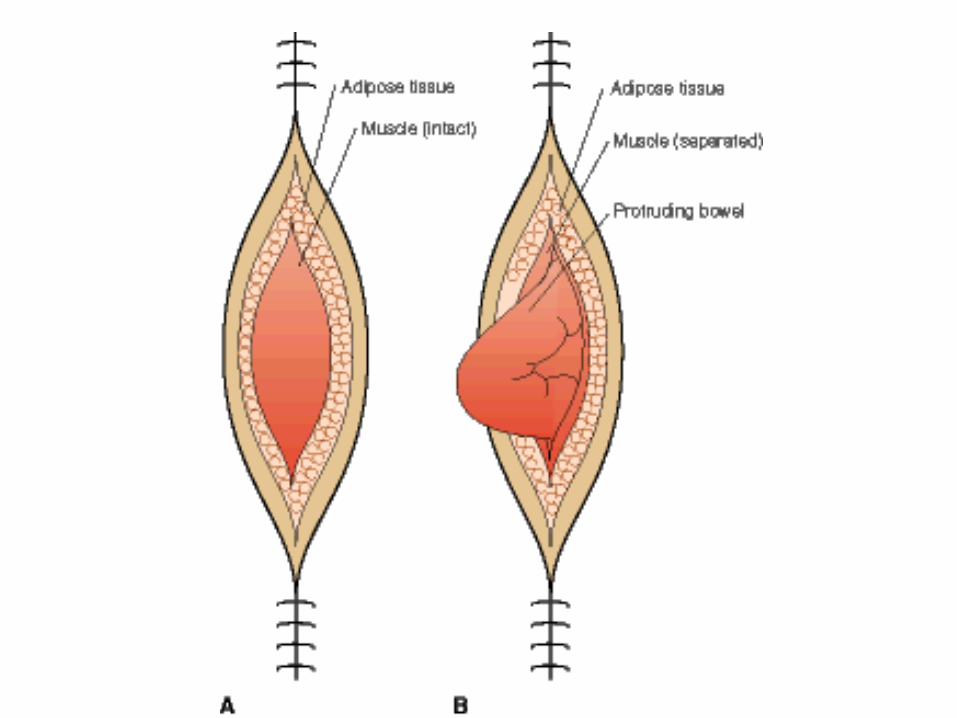
Evisceration
• Is the protrusion of visceral organs through a wound opening
• May occur with total separation of wound layers (ie. Total dehiscence)
• A MEDICAL EMERGENCY, will require surgical repair
• If it occurs, STERILE towels soaked in sterile saline are place over the extruding organs to reduce chances of bacterial invasion & drying
• If organs protrude thru the wound, blood supply to the tissues is compromised
Fistula • An abnormal passage between 2 organs or
between an organ & the outside of the body
• May be created for therapeutic reasons (as in gastrostomy tube for feedings) but MOST form as a result of poor wound healing where tissue layers are prevented from closing properly
• Fistulas increase the risk of infection and loss of fluid or electrolytes
• Chronic fluid drainage can also predispose the person to skin breakdown

Delayed Wound Healing• Sometimes referred to as third intention wound
healing
• Delayed wound closure is a deliberate attempt by a surgeon to allow effective drainage of a clean-contaminated or contaminated wound
• Wound not closed until all evidence of edema & debris removed (may be weeks).
• Wound covered by occlusive dressing to prevent bacterial contamination
• Wound then closed to heal by first intention

Factors affecting Wound Healing
1. Age:
2. Nutrition:
3. Obesity:
4. Impaired Oxygenation:
5. Smoking:
6. Drugs:
7. Diabetes:
8. Radiation:
9. Wound stress:

Types of dressings• Generally most drsg have 3 layers:
a)Contact layer. Fibrin, and debris adhere to this layer. If the drsg sticks, moisten it to remove carefully
– If the objective is debridement, then the adherence is OK such that removing the dressing pulls away the necrotic tissue and debris
b)Absorbent layer is a reservoir for secretions. The wicking action pulls the extra moisture away from the wound.
c)Outer layer is a barrier to keep bacteria and other contaminants away.
Types of Dressings
1) Transparent adhesive films (opsite, Tegaderm) p. 1545
2) Impregnated nonadherent dressing (Vaseline gauze)
3) Hydrocolloids (Duoderm) p. 15454) Hydrogel (intrasite gel) 15465) Polyurethane foams (lyofoam)6) Exudate absorbers (debrisan)7) Gauze dressings (dry to dry, wet to dry, wet
to damp or wet) 1541-1545

Telfa (Box of 100) 2" x 3"Ouchless Non-Adherent Dressing

How are dressings attached?
1.Tape– How do you put it on?– How do you remove it?
2.Ties3.Bandages 4.Anchoring material (netting)5.Binders

• 6. Measures to minimize discomforta. Careful removal of tape, gentle cleansing of
wound edges, and careful manipulation of dressings and drains minimize stress on sensitive tissues
b. Careful turning and positioning also reduce strain on a wound
• Administration of analgesic medications 30-60 minutes before dressing changes

How do you assess a wound?
• Who changes dressings?• What does the nurse note for charting?
– Are the wound edges closed?• Is there inflammation?• Discoloration?
– What is the nature of the wound drainage?• Amount?• Color and consistency?• Odor?• Response to palpation?• Pain?

WOUND CULTURES
•Do not collect wound culture from old drainage.
•Cleanse the wound with NS to remove skin flora

Procedure
1. use a microbiology requisition
2. cleanse the site with saline
3. make certain you note the following information:
– specimen location– request: C&S. gram stain (gm stain)– history (usually disease) – antibiotics (WHY?)
4. CHART what you have done.

CHANGING A DRESSING• To prepare:
– the nurse must know: type of dressing, the presence of underlying drains, and the type of supplies needed.
How do you find that out?
1. physician’s order should indicate dressing type, frequency of changing, and any solutions or ung.
2. chart for operative reports
3. nurses notes
4. other staff
5. the patient

General Recommendations
1) hand wash before and after
2) an open or fresh wound should be touched only with sterile gloves
3) a sealed wound dressings may be handled with clean gloves.
4) dressings should be changed when they become wet, or if the client has S&S of infection.
Common cleaning solutions• Soap & water for minor abrasions, lacerations, small
puncture wounds• Povidone-Iodine solution = for staphylococcus aureus• Dakin’s solution= diluted & is a bacteriocidal for
staphylococcal and streptococcal organisms. Very irritating to skin around the wound.
• Acetic acid solution= effective against gram-positive and gram-negative bacteria
• Hydrogen peroxide is a debriding agent. It should not be applied to granulation tissue.
• Saline is most often used to debride wounds. It maintains the moist surface needed to promote epithelial tissue growth.

Principles
• Clean from least contaminated to more contaminated (*ie clean to dirty)
• NNeverever use the same piece of gauze to cleanse twice– Wound is considered LESS contaminated than
the surrounding skin– Drain site is considered MORE contaminated
than an incisional site. Cleansing moves from the incisional site to the drain.
– Isolated drain site the site is LESS contaminated than the skin near it.
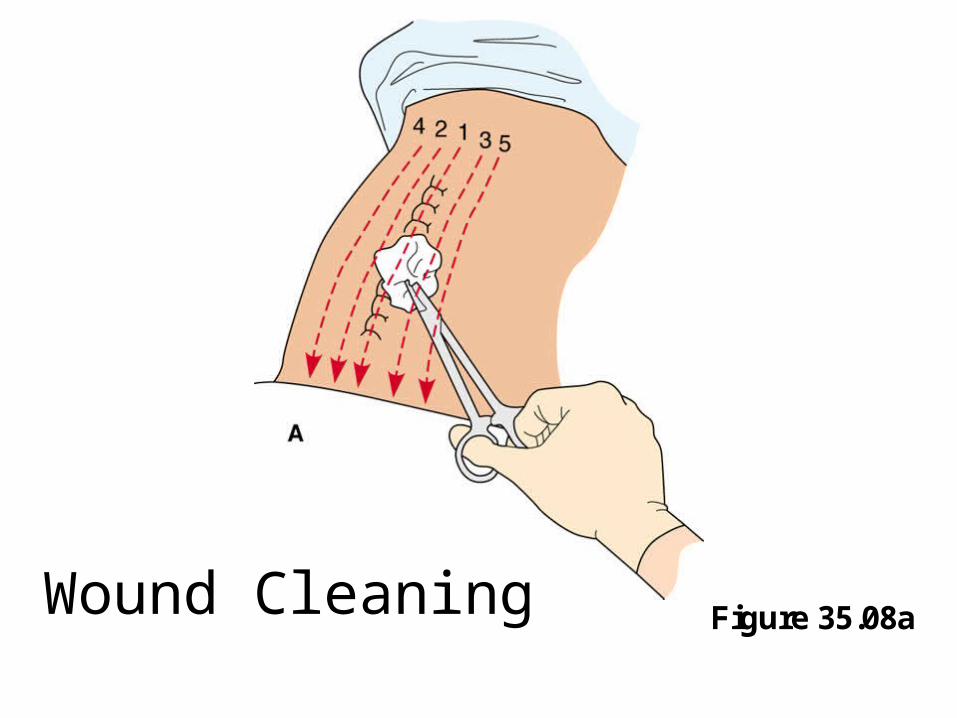
Figure 35.08aWound Cleaning
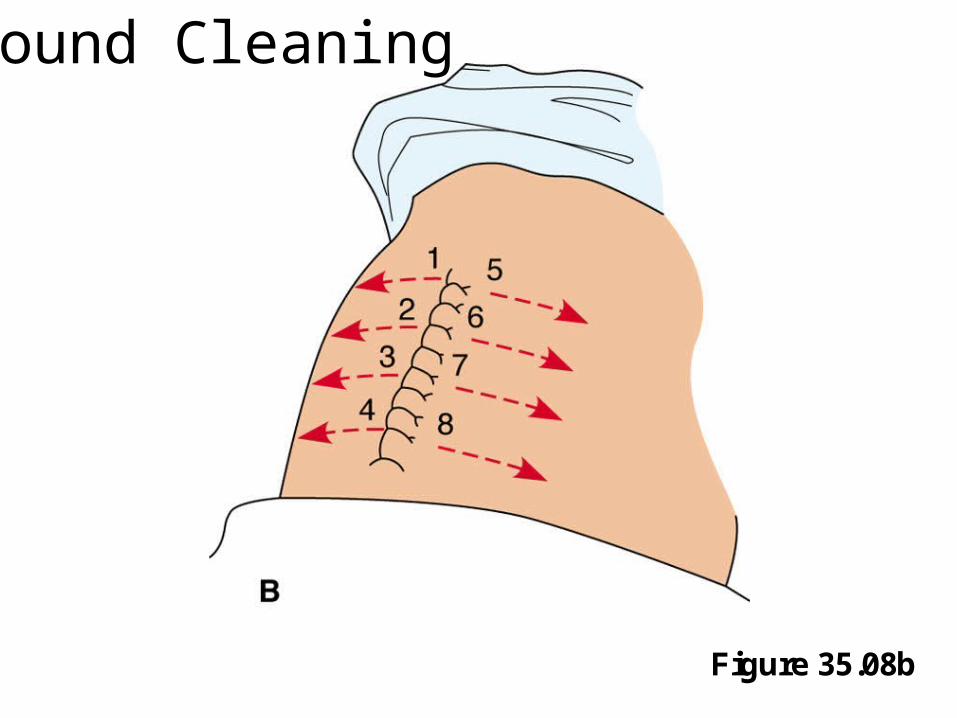
Figure 35.08b
Wound Cleaning

DrainsDrains• Inserted into or close to a surgical
wound if large amounts of drainage is expected if keeping wound layers closed is
especially important
• If fluid is allowed to accumulate under tissues, the inner wound edges wound never close
DrainsDrains
• Nurses’ responsibility is to:1)Assess drain placement,
patency2)Assess character of drainage3)Observe condition of collecting
apparatus (must be measured as ‘output’ when emptied)

TYPES OF DRAINSTYPES OF DRAINS
• Penrose – No suction– Usually secured by a pin
• Hemovac & Jackson-Pratt – Low-suction – Containers need to be emptied
• T-Tube – T shaped tube gravity drainage
• SOMETIMES use colostomy bags

Hemovac

Jackson-Pratt

Hemovac

Figure 35.08c
Wound Cleaningwith drain in place

Critical Elements for Wound Care• Maintains sterile technique• Removes soiled dressings appropriately• Cleanses “clean to dirty”• Maintains wound integrity (correct solution, uses each
sponge only once)• Assesses wound drainage and selects appropriate cover
(for the amount of exudate)• Applies dressing, if needed, in appropriate fashion• Reports and records as per facility policy (includes:
color and amount of drainage, incision line, type of dressing, client response)

Critical Elements
Collection of Specimens• Gathers appropriate equipment
• Provides appropriate asepsis: medical or surgical
• Follows procedures
• Charts date, time type of collection


definitions • AKAAKA – above the knee amputation• BKABKA – below the knee amputation• BlanchingBlanching – to become white or pale, as
from vasoconstriction Capillary return• CyanosisCyanosis – bluish discoloration of the
skin and mucous membranes caused by an excess of deoxygenated hemoglobin in the blood

• CWCMCWCM – colour, warmth, circulation, and movement
• Dependent edemaDependent edema – a fluid accumulation in the tissues & influenced by gravity. It is usually greater in the lower part of the body than in tissues above the level of the heart.
• DistalDistal – away from or being the farthest from the midline or central point
• ProximalProximal – nearer to a point of reference, usually the truck of the body, than other parts of the body.

IndicationsIndications for applying binders & bandages Binders and bandages applied over or around
dressings can provide extra protection and therapeutic benefits by:Creating pressureImmobilizing a body part Supporting a wound
(abdominal binder applied over a large abdominal incision and dressing).
Reducing or preventing edema Securing a splintSecuring dressings

Types of bandages and binders• Available in rolls of varying widths and materials e.g.
gauze, elasticized knit, elastic webbing, flannel, muslin– Gauze bandages are lightweight, inexpensive and mould
easily around a limb, and permit air to circulate– Elastic conforms to body parts, but as well can be used to
exert pressure over a body part– Flannel and muslin are thicker than gauze and thus are
stronger. A flannel bandage also insulates to provide warmth
– Binders and bandages that are made of large pieces of material to fit a specific body part
– Binders are usually made of elastic, cotton, muslin or flannel
Principles for applying bandages & binders
Position body part to be bandage in comfortable position of normal anatomical alignment
Prevent friction between and against skin surfaces by applying gauze or cotton padding
Apply bandages securely to prevent slippage during movement

Principles for applying bandages & binders
When bandaging extremities apply bandage first at distal end and progress toward trunk
Apply bandages firmly with equal tension exerted over each turn or layer. Avoid excess overlapping of bandage layers
Position pins, knots, or ties away from wound or sensitive skin
BeforeBefore a bandage or binder is applied, the nurse’s responsibilities include the following:
• Inspecting the skin for abrasions, edema, discoloration, or exposed wound edges
• Covering exposed wounds or open abrasions with a sterile dressing
• Assessing the condition of underlying dressings and changing them if soiled

The nurse’s responsibilities include the following:
• Assessing the skin of underlying body parts and parts that will be distal to the bandage for signs of circulatory impairment (coolness, pallor or cyanosis, diminished or absent pulses, swelling, numbness, and tingling) to provide a means for comparing changes in circulation after bandage application

• After a bandage is applied, nurse assesses, documents, & immediately reports changes in circulation, skin integrity, comfort level, and body function such as ventilation and movement.

CHARTING
The nurse must chart:
• The type of bandage
• Area of the body involved
• Comfort level
• CWCM
• Skin integrity
• Body function
• Bandage may be loosened or tightened but it must be monitored
SlingsSlings•Slings support arms with sprains or fractures
•Usually a large triangular piece of cloth
SlingsSlings
• Client may sit or lie
• Bend afflicted arm, bringing arm across chest
• Open part of sling fits under the afflicted arm and across the chest
• Base of triangle under the wrist and the triangle's point at the client's elbow

SlingsSlings• One end fits around the back of client's
neck• Loose end is brought up and over
afflicted arm and tied in back of neck• Knots are tied at side of neck so it does
not press,• Fingers must be supported• Hand higher than wrist

Scultetus (many-tailed) binder •a rectangular piece of cotton
with 6 to 12 tails attached to each side
•used to provide support to the abdomen or to retain dressings. – apply while patient is supine– line bottom up with pubic bone– apply tails upward alternately– assess breathing when patient sits up– pins last flap
Heat and cold application

Bodily responses to heat and cold
• Exposure to heat and cold can result in both a systemic and a local response
• SYSTEMICSYSTEMIC responses occur through heat-loss mechanisms (sweating and vasodilatation) or through mechanisms that conserve heat (vasoconstriction and piloerection)
• LOCALLOCAL responses occur through stimulation of temperature sensitive nerve endings within the skin

• The body can tolerate wide variations
• Normal skin temperature is 34° C, but the receptors will adapt to temperatures between 45° and 15°C
• Pain develops when temperatures outside this range–Too much heat = burning sensation
–Too cold = numbing sensation

Therapeutic effects
• HeatHeatvasodilationreduced blood viscosityreduced muscle tensionincreased tissue metabolismincreased capillary permeability

Therapeutic effects
• ColdColdvasoconstrictionlocal anesthetic reduced cell metabolismincreased blood viscositydecreased muscle tension
Uses for heatUses for heat
• Inflamed or edematous body parts
• New wounds with swelling (e.g. perineal)
• Infected wounds
• Arthritis
• Back and joint pain
• Muscle strain
• Menstrual pain
• Henmorroidal, perianal, vaginal inflammation
• Inflammation

Uses for coldUses for cold
• Direct injury or trauma (strains sprains, fractures, muscle spasms)
• Superficial lacerations or puncture wounds
• Minor burns
• Arthritis and joint pain
• Injections

Safety issues
• If heat is used too long–reflex vasoconstriction
–damage to epithelial cells
• If cold is used too long–reflex vasodilation

Factors affecting heat and cold tolerance
• duration of application
• body part.
• damage to body surface
• prior skin temperature
• body surface area
• age and physical conditions

Conditions that increase risk of injury
1. age
2. open wounds or broken skin
3. areas of edema or scar formation
4. peripheral vascular disease.
5. confused or unconsciousness
6. spinal cord injury
7.abscessed tooth or appendix

Assessment
• assess the client to determine risk factors for tolerance to heat and cold.
• observe the area to be treated
• establish a baseline.
• are there any conditions that would directly contraindicate the use of heat and cold?
• check the equipment to be used

CONTRAINDICATIONS
• To HeatHeat– Bleeding – Appendix – CV problems
• To ColdCold– Site of injury is edematous – Impaired circulation
• Both– Confusion or unconsciousness– Unsafe equipment -

Applying heat and cold
• in institution doctor's order required– the body site to be treated type, frequency and
duration of application
• follow the agency's policies• teaching:
– purpose of the therapy, – symptoms for temperature exposure– precautions to prevent injury
SAFETY– Explain the sensations to be felt– Instruct patient to report sensation changes or pain– Provide patient with a timer or clock– Keep the call light with in reach– Know the agency's policies– Do not allow the patient to adjust temperature– Do not allow the patient to move application– Do not position patient so they cannot move away – Do not leave unattended a client who cannot sense
temperature changes
Choice of moist or dry applications
• Both heat and cold can be applied in a moist or a dry form
• Choice is made according to:
– Type of wound or injury
– Location of body part
– Presence of drainage
– Presence of inflammation
Advantages
• MOIST– Reduces drying of skin– Softens exudate– Fit to body area being treated– Penetrate deeply into tissue layers– Does not promote sweating
• DRY– Less risk of burns to skin– Does not cause skin maceration– Retains temperature longer
Disadvantages
• MOIST– Prolonged exposure may cause maceration– Cools rapidly because of evaporation– Creates greater risk for burns
• DRY– Increases body fluid loss through sweating– Does not penetrate deeply into tissues– Causes increased drying of the skin

Hot moist compresses • May be used for open wounds
– They improve circulation– Relieve edema– Promote consolidation of pus and drainage
• Heat from hot compresses dissipates quickly
• Nurse must change the compress often or apply an aquathermic pad over top OR a waterproof-heating pad.
• With moist heat there is evaporation and the client may feel chilly.
Applying a hot moist compress• inspect condition of exposed skin and wound• assess client to sensitivity to temperature• check physician’s order• prepare equipment• explain procedure• make client comfortable• wash hands• procedure is sterile• after procedure
– inspect affected area– chart

Methods• Hot water bottleHot water bottle
– Filled to approximately 2/3 full– Remaining air is expelled and top secured– Bag is dried and held upside down to test for
leakage– Wrapped in a cover– Usually stays hot for 45 minutes
• TEMPERATURES – Normal adult 52°– Debilitated or unconscious 40-46°– Child 40- 45°

Aquathermia (water flow) pad
• Device through which warm distilled water circulates
• Distilled water circulates through hollowed channels in the pad to the control unit where the temperature is set to either heat or cool
• Water reservoir must be kept 2/3 full• Temperature is set with a key• Cover is placed between pad and skin• Secured with tape NEVER pins• Application is 20-30 minutes• patient is never allowed to lie on the pad,
Heating pads
– C/o an electric coil enclosed in a waterproof pad covered with cotton
– Pad connected to an electric cord with a temperature control
• CAUTIONCAUTION– Never use the high setting– Never lie on the pad– Safety pins and/or water may result in
electrical shock

Commercial hot or cold packs
• Hot packs– Apply warm dry heat to an area
– Instructions tell how to initiate the heating (knead, hit or snap the bag)
– These list the time for which they are effective
– They are considered disposable
• COLD PACKS– Same as for heat packs

Ice collar/ bags
• Ice bag is a rubber or plastic bag with a removable cap
• Ice collar is similar but is long and narrow• Ice glove rubber or plastic glove filled with ice
chips and tied at the end • PROCEDUREPROCEDURE
– Crushed ice is placed in container until 2/3 full– Air is expelled– Top secured and cover tightened– Put onto body part so it moulds– Apply for 30 minutes. Reapply in 1 hour

Sitz Baths
– Used for rectal surgery, episiotomies, hemorrhoids, vaginal inflammation
– only the perineal area is immersed – Patient uses a special tub or a plastic basin– Disposable sitz baths have a bag into which hot
water is placed to run in slowly – Treatment usually 20 minutes– Client must be kept warm– Feet flat on the floor– No pressure on the sacrum

Warm soaks• Promotes circulation• Lessens edema• Increases muscle relaxation• May assist debridement• Allows the application of medication• PROCEDURE
– Position the patient comfortably– Put waterproofing on the bed– Heats solution to 40-43°– Immerse the body part– Cover container and person to prevent heat loss– Change solution q 10 min
• There are also cold soaks
Treating Injuries effectively
• When do you use ice?When do you use ice?– immediately after injury and up to 72 hours if
the S&S of inflammation are no longer present
– Use for 20 minutes with an hour off.
• When do you use heat?When do you use heat?– AVOID immediately after an injury and for
up to 72 hours– Apply for 20 minutes. Repeat several times a
day

Critical ElementsCritical Elements
Checks for the physician's orderFollows the agency's policiesAssesses the patient and the wound before
the application and afterKnows the risks and benefits of heat and cold
applicationsKnows how to correctly apply the various types of
heat and cold applicationsKnows the time limits for applicationProvides teaching: for the patient















![[Cat26s027] Shadowrun 5e - Bullets & Bandages](https://static.fdocuments.net/doc/165x107/55cf9687550346d0338c180b/cat26s027-shadowrun-5e-bullets-bandages.jpg)


