Wound Bed Preparation and Infected Wounds in … · Wound Bed Preparation and Infected Wounds in...
28
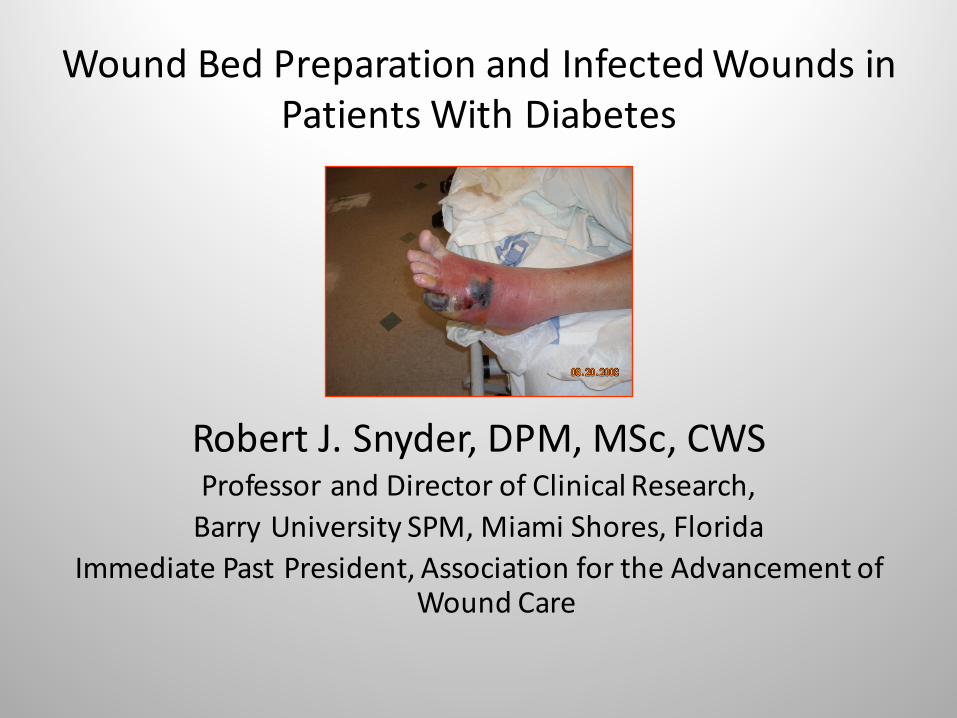
Wound Bed Preparation and Infected Wounds in Patients With Diabetes Robert J. Snyder, DPM, MSc, CWS Professor and Director of Clinical Research, Barry University SPM, Miami Shores, Florida Immediate Past President, Association for the Advancement of Wound Care
Transcript of Wound Bed Preparation and Infected Wounds in … · Wound Bed Preparation and Infected Wounds in...
WoundBedPreparationandInfectedWoundsinPatientsWithDiabetes
RobertJ.Snyder,DPM,MSc,CWSProfessorandDirectorofClinicalResearch,BarryUniversitySPM,MiamiShores,Florida
ImmediatePastPresident,AssociationfortheAdvancementofWoundCare
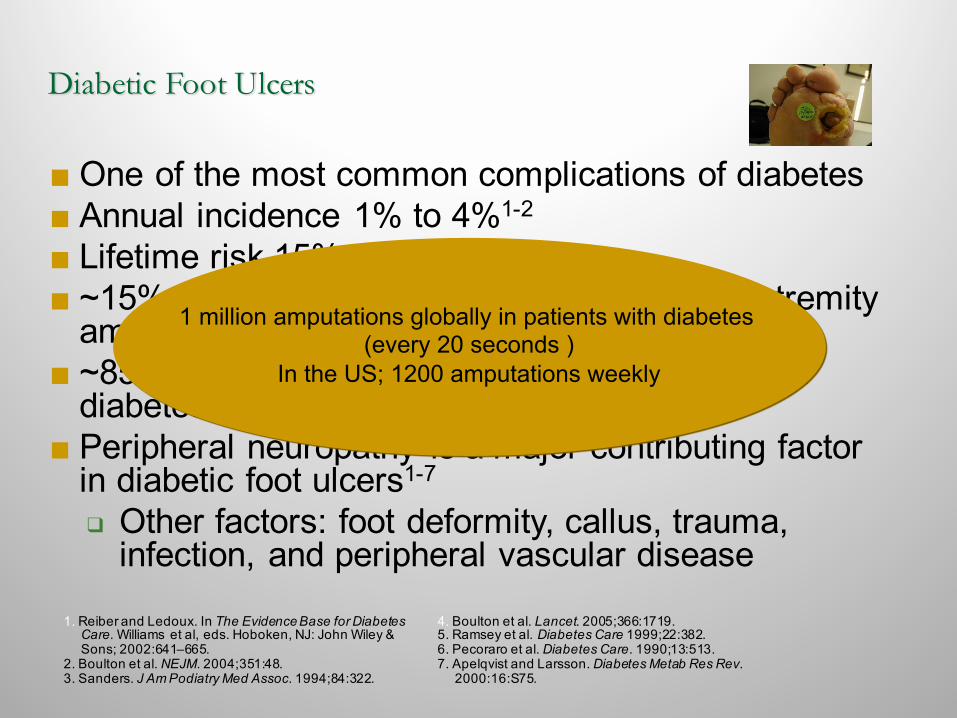
Diabetic Foot Ulcers
■One of the most common complications of diabetes■ Annual incidence 1% to 4%1-2
■ Lifetime risk 15% to 25%3-4
■ ~15% of diabetic foot ulcers result in lower extremity amputation3,5
■ ~85% of lower limb amputations in patients with diabetes are proceeded by ulceration6-7
■ Peripheral neuropathy is a major contributing factor in diabetic foot ulcers1-7
❑ Other factors: foot deformity, callus, trauma, infection, and peripheral vascular disease
1. Reiber and Ledoux. In The Evidence Base for Diabetes Care. Williams et al, eds. Hoboken, NJ: John Wiley & Sons; 2002:641–665.
2. Boulton et al. NEJM. 2004;351:48.3. Sanders. J Am Podiatry Med Assoc. 1994;84:322.
4. Boulton et al. Lancet. 2005;366:1719.5. Ramsey et al. Diabetes Care 1999;22:382.6. Pecoraro et al. Diabetes Care. 1990;13:513.7. Apelqvist and Larsson. Diabetes Metab Res Rev.
2000:16:S75.
1 million amputations globally in patients with diabetes (every 20 seconds )
In the US; 1200 amputations weekly
DFU…PathophysiologyFinalCommonPathways
q Infectionq Ischemia/hypoxiaq Cellularfailureq Pressure/traumaq Inflammation
Snyderetal.OstomyWoundManagement.2010;56(Suppl4):S1-S24
All final common pathways are implicated in DFU healing failure!!
Deep infection
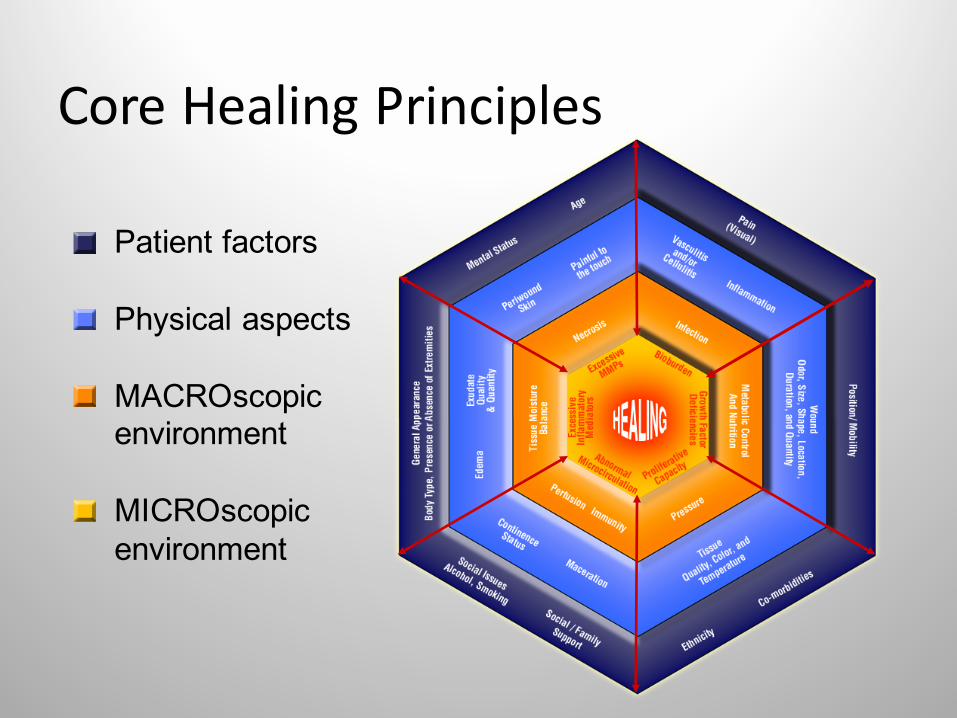
CoreHealingPrinciples
Patient factors
Physical aspects
MACROscopicenvironment
MICROscopicenvironment
“Thinklikeaninternist,beforeyouactlikeasurgeon”Wm.Ennis,DO
Woundmanagementoftenrequiresasubtlebalancebetweenmedicalandsurgicalinterventions.
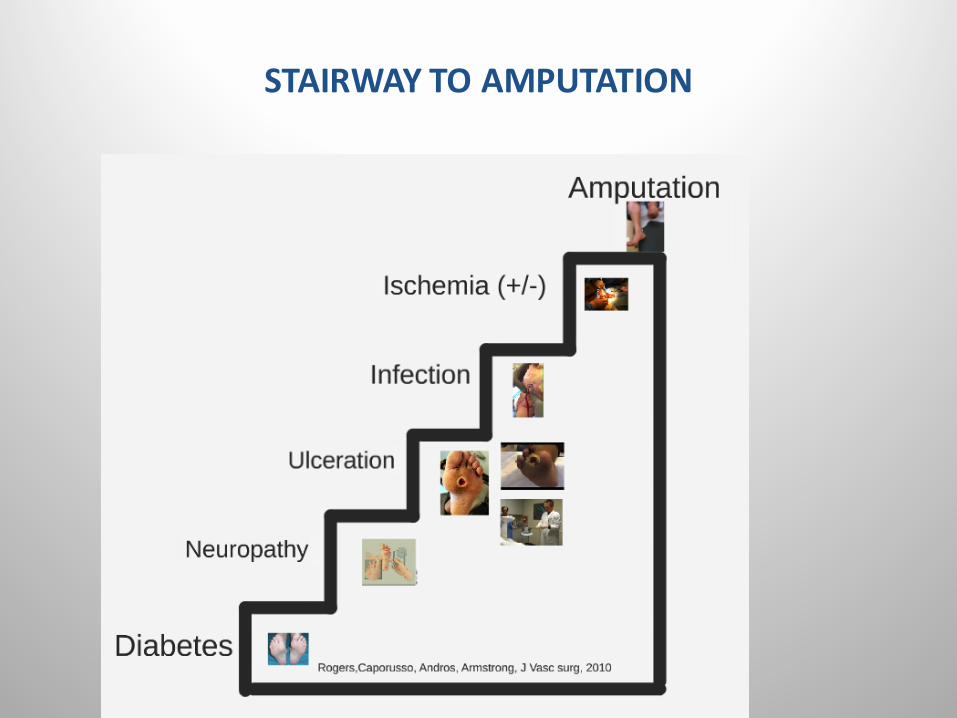
STAIRWAYTOAMPUTATION
ClassicSignsandSymptomsofInfection
• Heat• Pain• Redness• Swelling
Clinicians should diagnose infection based on the presence of at least 2
classic symptoms or signs of inflammation or purulent secretions
Lipsky et al. Clinical Infectious Diseases. 2012;54(12):132-173
Clinicallyinfectedwoundsusuallyrequiresystemicantibiotics,whileclinicallyuninfectedwounds thatarehealingasexpecteddonot
requireantimicrobialsLipskyB,Hoey C.ClinicalInfectiousDiseases.2009;49:1541-9
ValidityofSecondaryClinicalSignsandSymptomsofChronicWoundInfection
• Secondaryclinicalsignsofinfectionwithpositivepredictivevalue…– Serousdrainagewithinflammation– Delayedhealing– Discolorationofgranulationtissue– Friablegranulationtissue– Pocketingatbaseofwound– Foulodor– Woundbreakdown– Increasingpain
Gardner, et al. Wound Rep Reg 2001; 9:178-186
Cliniciansshouldconsiderthepossibilityofinfectionoccurringin
any footwoundinapatientwithdiabetes
Lipsky et.Al.Clinical InfectiousDiseases.2012;54(12)”132-173
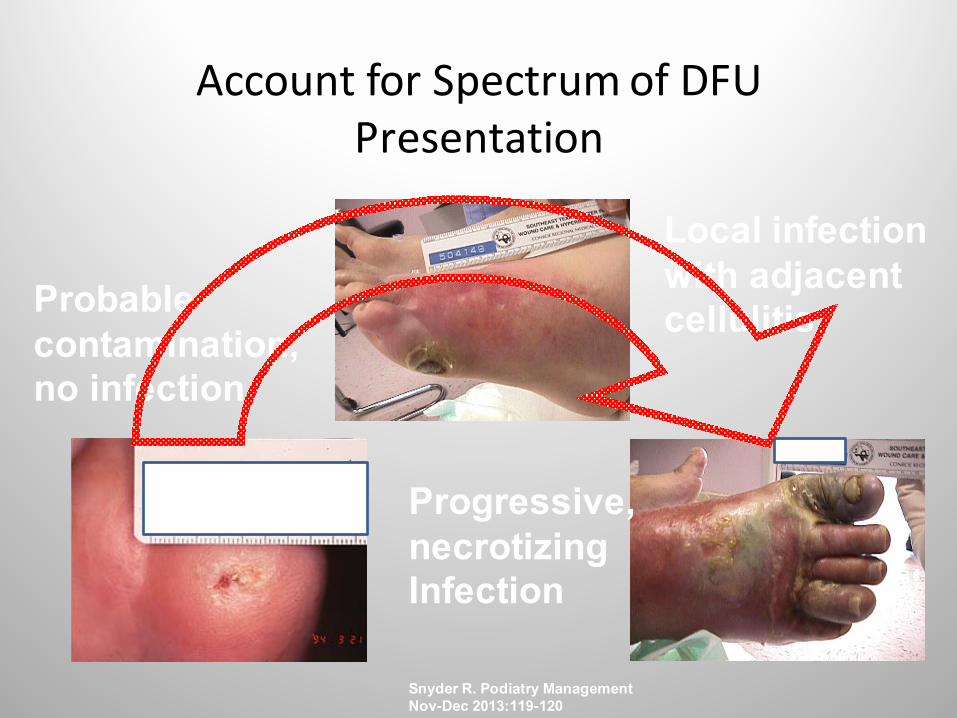
AccountforSpectrumofDFUPresentation
Probable contamination,no infection
Local infectionwith adjacent cellulitis
Progressive, necrotizingInfection
Snyder R. Podiatry ManagementNov-Dec 2013:119-120
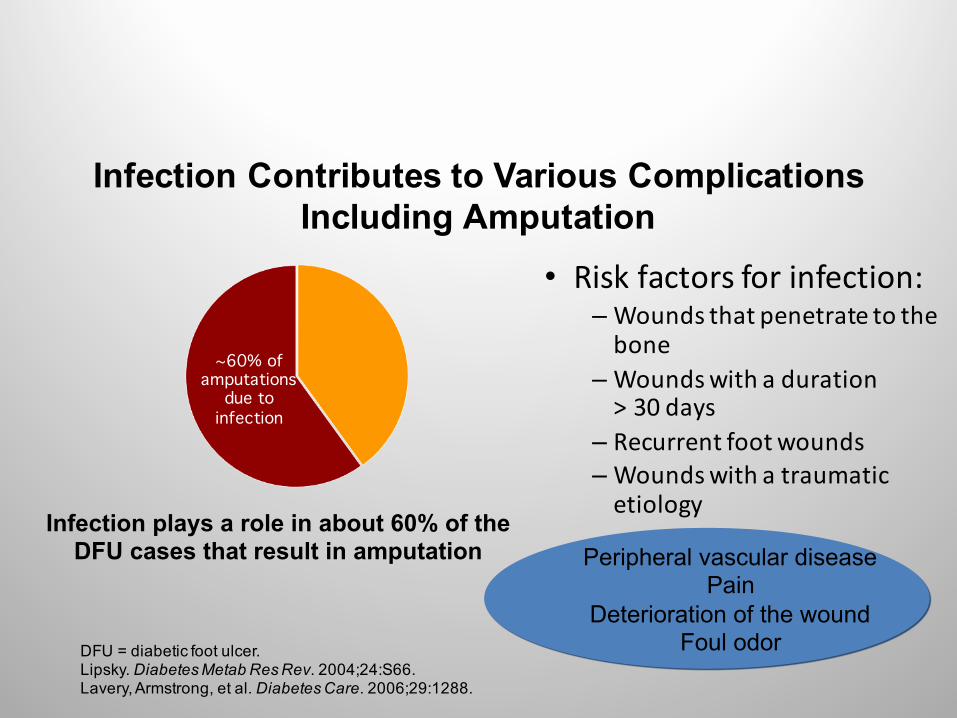
~60% of amputations
due to infection
• Riskfactorsforinfection:– Woundsthatpenetratetothebone
– Woundswithaduration>30days
– Recurrentfootwounds– Woundswithatraumaticetiology
Infection plays a role in about 60% of theDFU cases that result in amputation
DFU = diabetic foot ulcer.Lipsky. Diabetes Metab Res Rev. 2004;24:S66.Lavery, Armstrong, et al. Diabetes Care. 2006;29:1288.
Infection Contributes to Various Complications Including Amputation
Peripheral vascular diseasePain
Deterioration of the woundFoul odor
Wound bed preparation isan important step in treating and
protecting againstwound infection
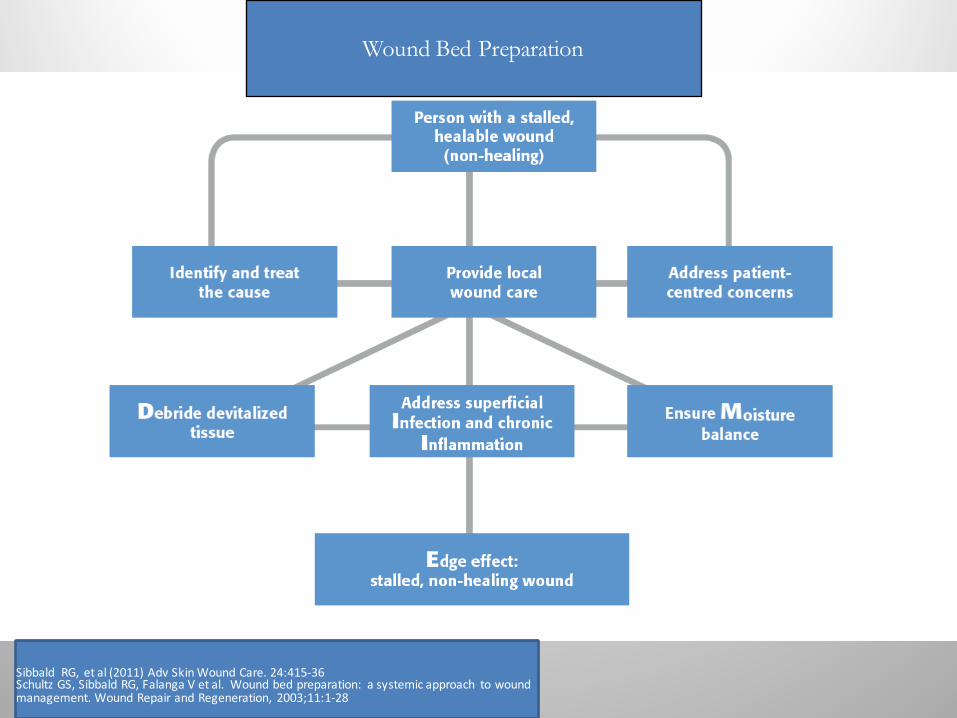
DIME
Wound Bed Preparation
SibbaldRG, etal(2011)AdvSkinWoundCare.24:415-36SchultzGS,SibbaldRG,FalangaVetal.Woundbedpreparation: asystemicapproach towoundmanagement.WoundRepairandRegeneration, 2003;11:1-28

Saap LJ, Falanga V. Wound Rep Reg 2002; 10:354-359.
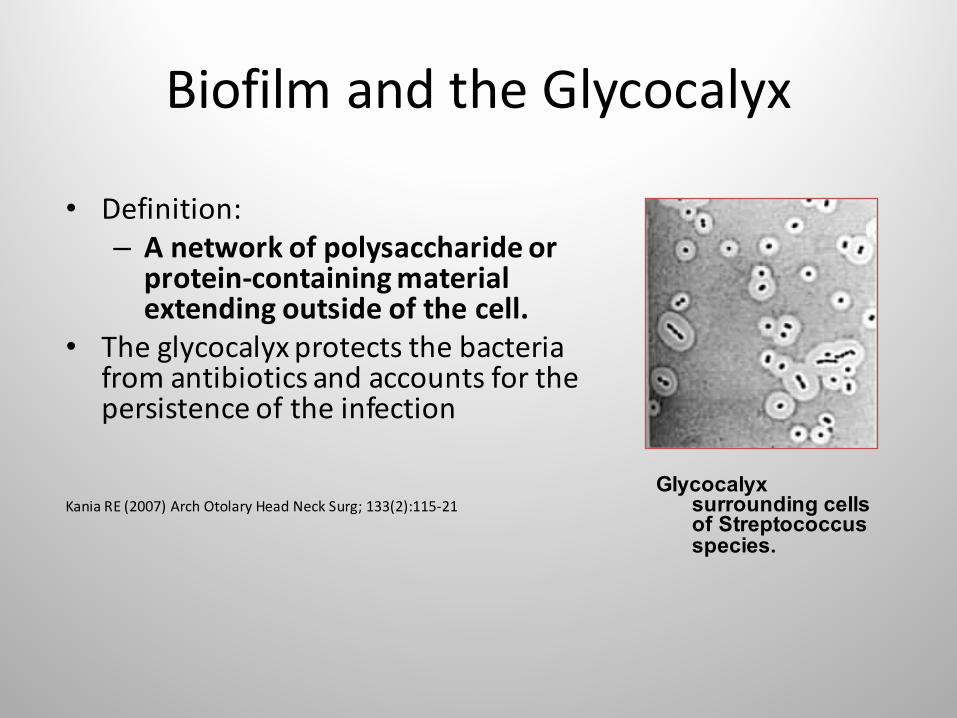
BiofilmandtheGlycocalyx
• Definition:– Anetworkofpolysaccharideorprotein-containingmaterialextendingoutsideofthecell.
• Theglycocalyxprotectsthebacteriafromantibioticsandaccountsforthepersistenceoftheinfection
KaniaRE(2007)ArchOtolaryHeadNeckSurg;133(2):115-21Glycocalyx
surrounding cells of Streptococcus species.
BiofilmsareProblematic:
• Resistanttohostimmuneresponses• Markedlyresistanttopenetrationbytopicalantibioticsandbactericidals
• Mixedbacterialspeciesmayenhancethevirulence-synergistically
• Commonindevitalizedtissue
Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lappin-Scott HM. Microbial biofilms. Annu Rev Microbiol. 1995;49:711-745.Xu KD, McFeter GA, Stewart PS. Biofilm resistance to antimicrobial agents. Microbiology. 2000;146:547-549.
Biofilmcanbe500xmoreresistanttoantibacterialagents
Costerton JW,etal.Annu RevMicrobiol1995;49:711-745
APotentialModelforDisruptingProblematicBiofilm
(Theoretical)• SharpDebridement andutilizationoftopicalantimicrobialstolowerplanktonic bacteriallevels;thiswilldecreasenewbiofilm colonies
• Continuesharpdebridementonaregularbasistocontinuallydisruptandpotentiallyweakenthebiofilm/glycocalyx.(i.e.Biofilm canpotentiallyreturnwithin3-24hours.)
• Thereisin-vitroevidenceusingbiofilmmodelswhichdemonstratestheabilityofsometopicalantimicrobialdressingstodisruptbiofilm(i.e.iodine,silver)
Hill et. al 2010
Rememberthatitisstillnotknownwhetherallbiofilm are“bad”
Muchmoreresearchisrequiredinthisfield

WoundBedPreparationinPractice
SnyderR,FifeC,MooreZ.TheDIMEandQualityMeasures.
AdvancesSkinWoundCareScheduledforPublication2015
Wound Bed Preparation
SibbaldRG, etal(2011)AdvSkinWoundCare.24:415-36SchultzGS,SibbaldRG,FalangaVetal.Woundbedpreparation: asystemicapproach towoundmanagement.WoundRepairandRegeneration, 2003;11:1-28
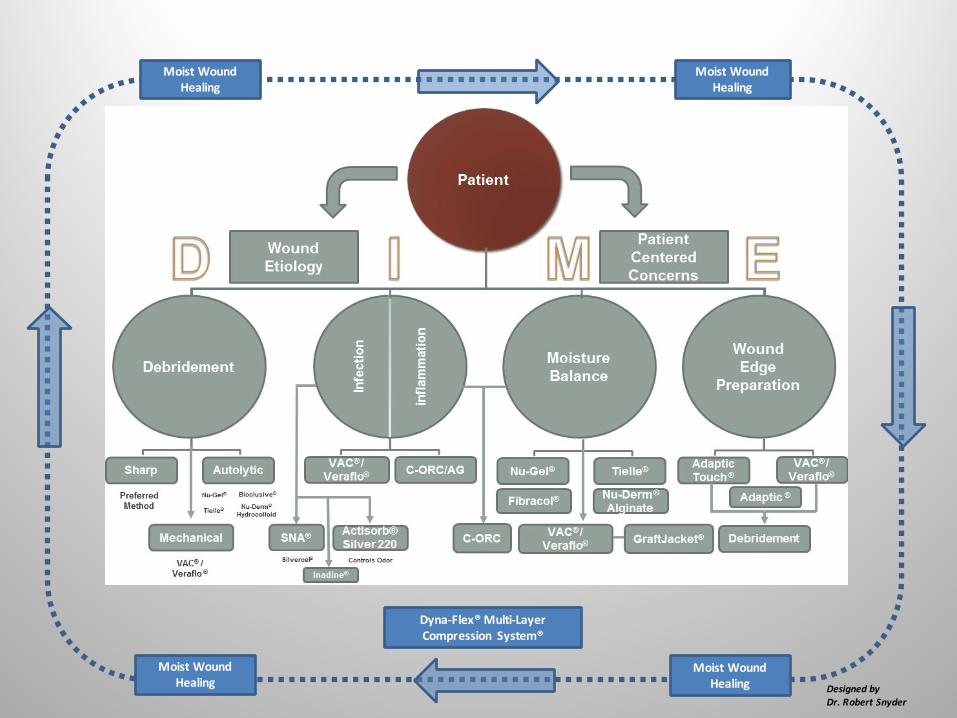
MoistWoundHealing
MoistWoundHealing
MoistWoundHealing
MoistWoundHealing
WoundBedPreparation
DesignedbyDr.RobertSnyder
Dyna-Flex®Multi-LayerCompression System®
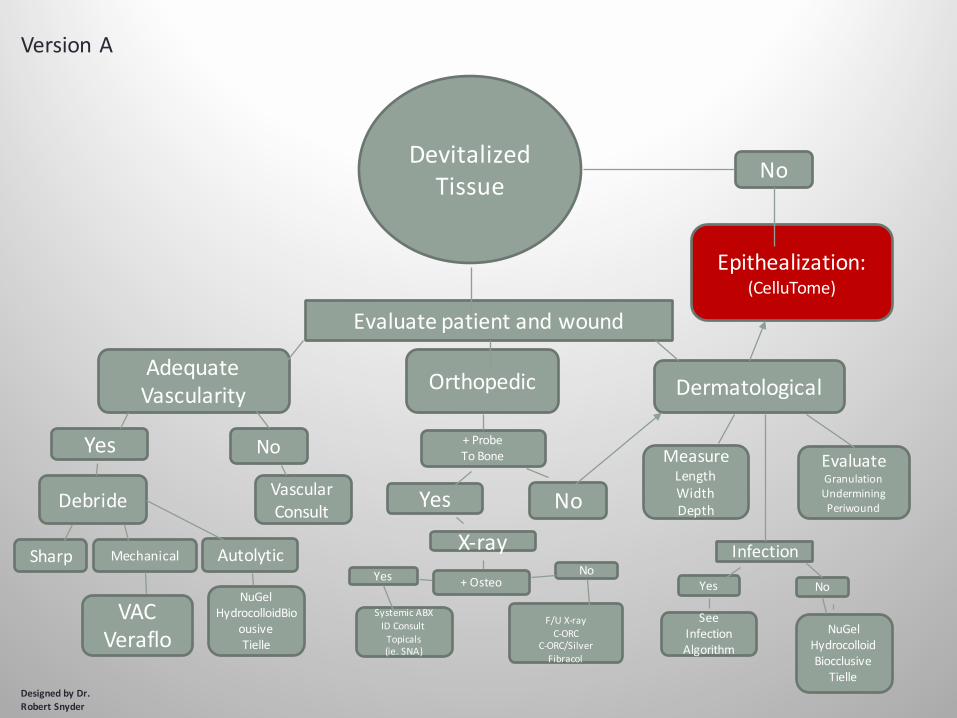
DevitalizedTissue
Evaluatepatientandwound
AdequateVascularity Orthopedic Dermatological
Yes No
Debride VascularConsult
Sharp Mechanical Autolytic
NuGelHydrocolloidBio
ousiveTielle
VACVeraflo
+ProbeToBone
Yes No
X-ray+OsteoYes No
SystemicABXIDConsultTopicals(ie.SNA)
F/UX-rayC-ORC
C-ORC/SilverFibracol
MeasureLengthWidthDepth
EvaluateGranulationUnderminingPeriwound
Infection
Yes No
SeeInfectionAlgorithm
NuGelHydrocolloidBiocclusive
Tielle
Epithealization:(CelluTome)
No
DesignedbyDr.RobertSnyder
VersionA
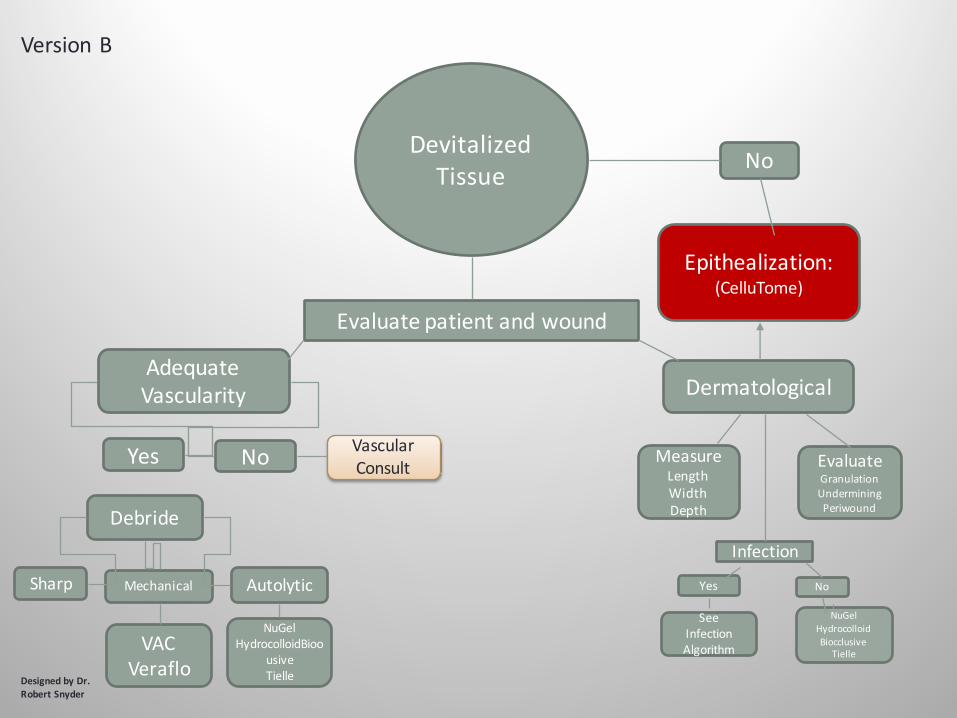
DevitalizedTissue
Evaluatepatientandwound
AdequateVascularity Dermatological
Yes
Debride
VascularConsult
Sharp Mechanical Autolytic
NuGelHydrocolloidBioo
usiveTielle
VACVeraflo
MeasureLengthWidthDepth
EvaluateGranulationUnderminingPeriwound
Infection
Yes No
SeeInfectionAlgorithm
NuGelHydrocolloidBiocclusive
Tielle
Epithealization:(CelluTome)
No
DesignedbyDr.RobertSnyder
VersionB
No
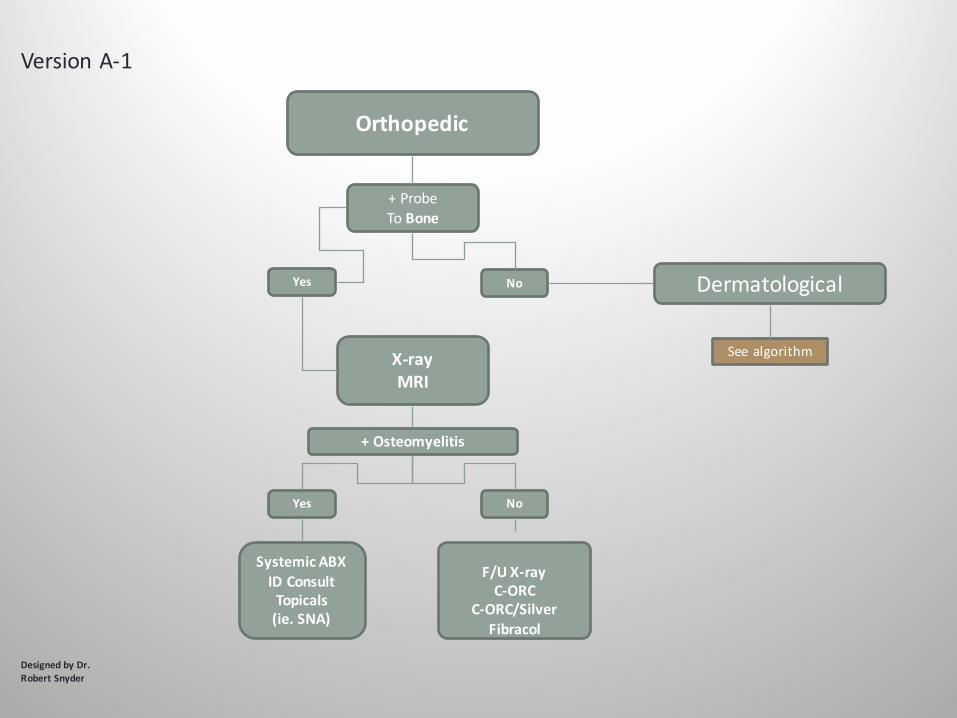
Orthopedic
+ProbeToBone
X-rayMRI
+Osteomyelitis
Yes
SystemicABXIDConsultTopicals(ie.SNA)
F/UX-rayC-ORC
C-ORC/SilverFibracol
Dermatological
See algorithm
DesignedbyDr.RobertSnyder
VersionA-1
No
Yes No
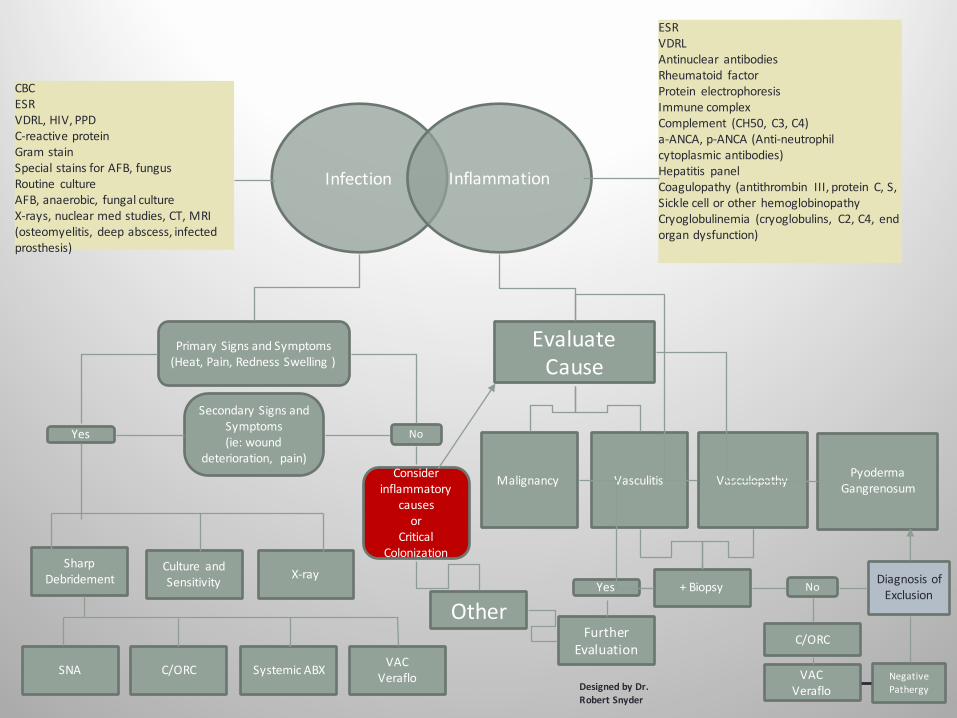
Infection
PrimarySignsandSymptoms(Heat,Pain,RednessSwelling)
Yes
SecondarySignsandSymptoms(ie:wound
deterioration, pain)
No
Considerinflammatory
causesor
CriticalColonization
SharpDebridement
Culture andSensitivity X-ray
SNA C/ORC SystemicABX VACVeraflo
EvaluateCause
Malignancy Vasculitis PyodermaGangrenosumVasculopathy
+BiopsyYes No
FurtherEvaluation
DiagnosisofExclusion
C/ORC
VACVeraflo
NegativePathergy
Other
CBCESRVDRL,HIV,PPDC-reactiveproteinGramstainSpecialstainsforAFB,fungusRoutine cultureAFB,anaerobic, fungalcultureX-rays,nuclearmedstudies,CT,MRI(osteomyelitis, deepabscess,infectedprosthesis)
ESRVDRLAntinuclear antibodiesRheumatoid factorProtein electrophoresisImmunecomplexComplement (CH50, C3,C4)a-ANCA,p-ANCA(Anti-neutrophilcytoplasmicantibodies)Hepatitis panelCoagulopathy(antithrombin III,protein C,S,Sicklecellorother hemoglobinopathyCryoglobulinemia (cryoglobulins, C2,C4, endorgandysfunction)
Inflammation
DesignedbyDr.RobertSnyder
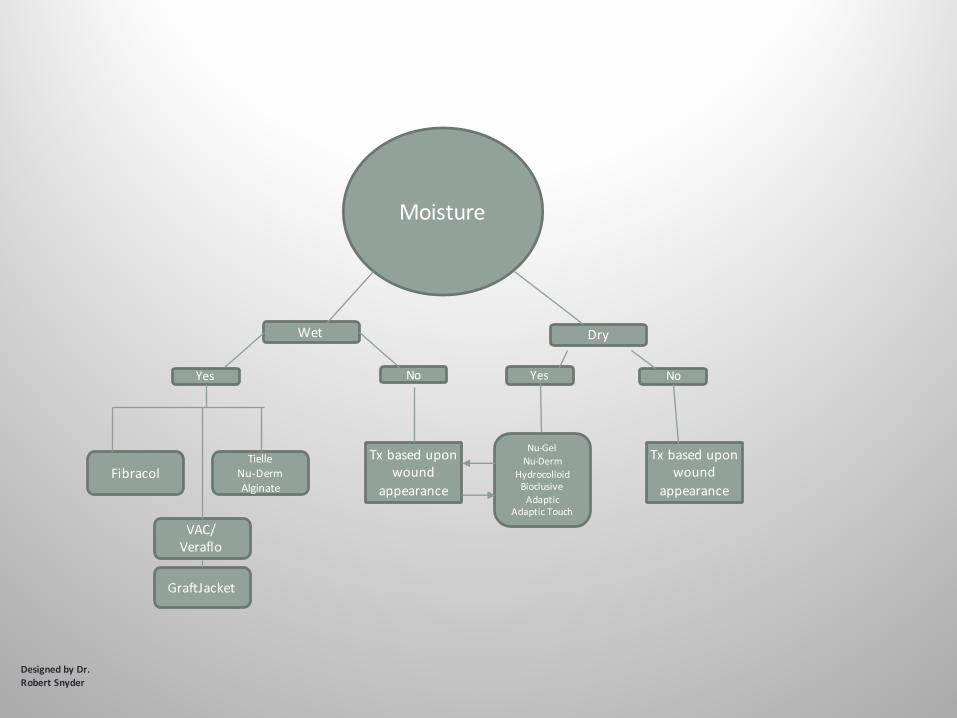
Moisture
Wet Dry
Yes No
Fibracol
VAC/Veraflo
TielleNu-DermAlginate
Txbaseduponwound
appearance
Yes No
Nu-GelNu-Derm
HydrocolloidBioclusiveAdaptic
AdapticTouch
GraftJacket
Txbaseduponwound
appearance
DesignedbyDr.RobertSnyder
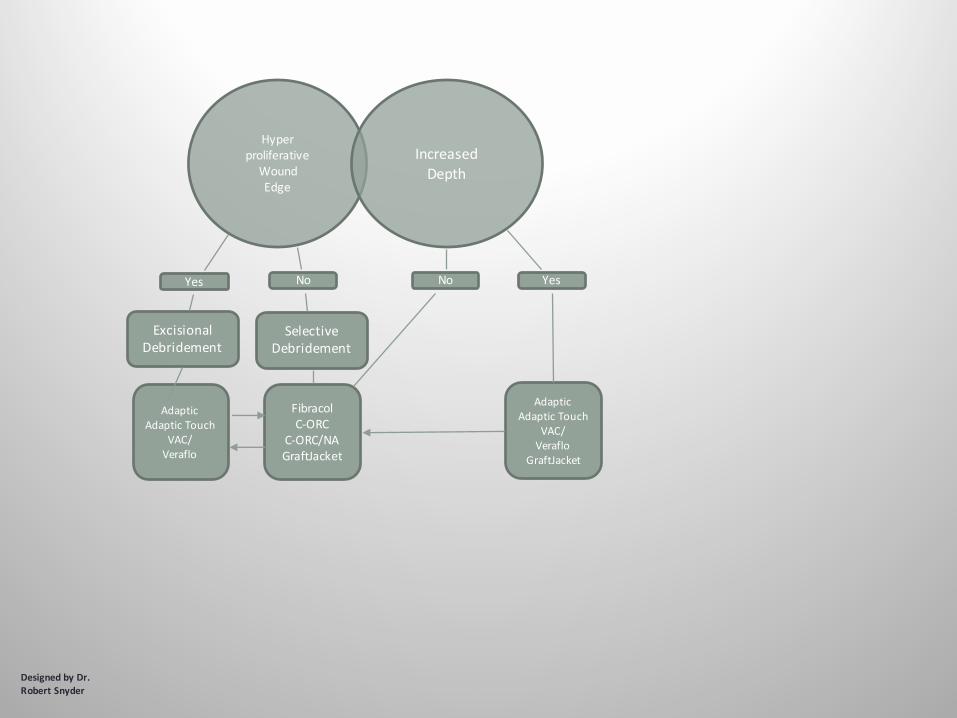
HyperproliferativeWoundEdge
IncreasedDepth
Yes No No Yes
ExcisionalDebridement
AdapticAdapticTouch
VAC/Veraflo
SelectiveDebridement
FibracolC-ORC
C-ORC/NAGraftJacket
AdapticAdapticTouch
VAC/Veraflo
GraftJacket
DesignedbyDr.RobertSnyder
ASurgicalPathwayShouldBeConsideredWhenAnAbscessorBoneInfectionisSuspected
SnyderR,etal.OWM2001
Surgicaldebridementisanimportantcomponentofboththeevaluationandidentificationofinfection
aswellastreatmentofinfection
SnyderRJetal.OWM.2001;47(3):24-41
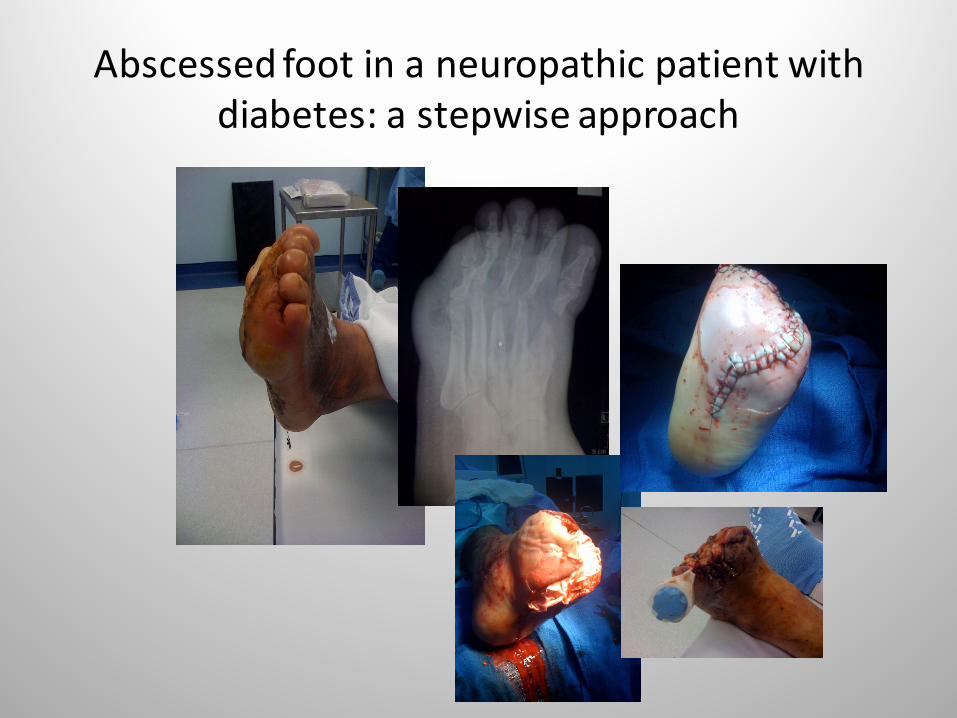
Abscessedfootinaneuropathicpatientwithdiabetes:astepwiseapproach
Summary• Infectionrepresentsaserioussequelaeinacuteandchronicwoundsinpatientswithdiabetes
• Knowledgeofclinicalpathwaystomakingadiagnosisremainscritical:IDSAGuidelines
• Biofilmmayplayanimportantroleinresistantinfections
• Recentliteraturesupportstheuseofappropriatewoundbedpreparation,systemicantibiotics,sometopicalantiseptics,debridement,andsurgicalstrategiesinthetreatmentofwoundinfection
ThankYou