
Work, Health and Well-being: an interdisciplinary approach to managing health in the workplace
84
description
Work, Health and Well-being: an interdisciplinary approach to managing health in the workplace. - PowerPoint PPT Presentation
Transcript of Work, Health and Well-being: an interdisciplinary approach to managing health in the workplace


Work, Health and Well-being: an interdisciplinary approach to managing health in
the workplace • The Work, health and well-being network has been funded for a
10-month period to build new multi-disciplinary teams as part of the Lifelong Health and Wellbeing Project (LLHW). This is a major cross-council initiative supporting multi-disciplinary research addressing factors across the life course that influence healthy ageing and wellbeing in later life. The objectives of the LLHW initiative are to:
• Target factors over the life course that may be major determinants of health and wellbeing in later life.
• Identify and develop effective interventions that lead to improved health and quality of life in later life.
• Inform policy and practice including the development of services and technologies to support independent living.
• Increase capacity and capability in ageing-relevant research

Aims of the network
• To develop an interdisciplinary network focusing upon health transitions in employment.
• The project will have a particular focus on the management of two of the main reasons for work loss (stress and musculoskeletal conditions) occurring during the middle and later phases of working life.
• The aim of the proposed network is to examine the influence of particular health conditions on work transitions at particular points of the life course.
• The network will focus on the two most common health reasons for work loss in the United Kingdom: (1) mental health problems relating to stress in the workplace; and (2) musculoskeletal disorders.
• This proposal brings together a range of disciplinary backgrounds to examine the influence of specific health conditions affecting work transitions in middle and later life.

Network website
• http://www.keele.ac.uk/research/pchs/pcmrc/WHW_Network/index.htm

Symposium- Work, Health and Well-being: Older Workers
Chris Phillipson and Ross Wilkie ‘Health and social issues in extending working life’
David Lain ‘Measuring Ill-health and older workers: a comparison of the US and the UK’
Joanne Ross ‘Does an understanding of occupational identity help to explain vocational rehabilitation for older workers?’
Sarah Vickerstaff ‘Understanding the impact of health and health pessimism on the extending work life agenda’
Health and Social Issues in Extending Working Life
Chris Phillipson and Ross Wilkie

Debates on older workers
• 50s/60s: Labour force retention
• 70s/80s: Labour market exit
• 90s/early 2000s: Extending work
• Late 2000s: Extension - Exclusion

Employment/Population Ratios and Activity: men and Women 55 - 64
1990 1994 1997 2004 2007
UK Men Labour participation rate 68.1 64.0 63.6 67.9 68.9
Employment /population ratios 62.4 56.6 58.6 65.4 66.1
UK Women Labour participation rate 38.7 40.7 40.3 48.3 50.1
Employment /population ratios 36.7 38.5 38.7 47.3 49.0
USA Men Labour participation rate 67.8 65.5 67.6 68.7 69.6
Employment /population ratios 65.2 62.6 65.5 66.0 67.6
USA Women Labour participation rate 45.2 48.9 50.9 56.3 58.3
Employment /population ratios 44.0 47.0 49.5 54.3 56.6
Source: OECD Employment Outlook: 1998 and 2008

Factors behind increase in employment
Policies less important than:
• Demand-side factors: economic growth
• Supply-side factors: impact of shift from DB to DC pensions on retirement behaviour
• Closure of early exit pathways: tightening of eligibility criteria for unemployment/disability benefits
• Bridging employment: expansion of self-employment among older workers

Is extending working life possible?Policy drivers• Raising of pension ages (Pension
Regulator, Turner: retirement at 70?)
• Age discrimination and equality at work
(Employment Equality Age Regulations, 2006)
• Promotion of health and well-being in the workplace
(Black, 2008, Working for a Healthier Tomorrow)
• Economic and social value of older workers (‘Building a
Society for All Ages’, DWP, 2009)

Is extending working life possible?
• Policy Barriers
- rise in unemployment with older
workers targeted for redundancy;
- uncertainty about ‘extended work’
agenda (Vickerstaff et al., 2008);
- relationship to other events in the life
course (Schmid, 2002).

Is extending life possible?
• What do we know of the key barriers in respect of health and workplace issues?
• Data sets:
British Household Panel Survey
English Longitudinal Survey of Ageing
Labour Force Survey

Is extending working life possible?
Key barriers
• Impact of transitions through work
• Impact of health issues in the workplace
• Impact of detachment from work

• IMPACT OF TRANSITIONS

Work status of cohorts of men: Stable transitions
Transition Type
45-49 (52-56)
50-54 (57-61)
55-59 (62-66)
60-64 (67-71)
Stable Full-time throughout 57.4 33.5 18.0 3.1
Part-time throughout 0.0 0.7 0.8 0.9
Unemployed
throughout
0.0 0.4 0.9 0.0
Inactive throughout 3.8 8.0 19.7 39.5
61.2 42.6 39.4 43.5
Source: British Household Panel Survey, Waves A-H (base = 1,132) (own calculations)

Occupational status of cohorts of men: Bridging transitions
Transition Type
45-49
(52-56)
50-54
(57-61)
55-59
(62-66)
60-64
(67-71)
Bridging
Full-time + part-time 4.3 11.9 5.3 2.5
Full-time + part-time + unemployed 2.0 2.9 2.3 0.0
Full-time + part-time + inactive 1.5 5.0 7.2 4.7
Full-time part-time + unemployed +
inactive
0.9 1.1 1.0 2.0
8.7 20.9 15.8 9.2
Source: British Household Panel Survey, Waves A-H (base = 1,132) (own calculations)

Occupational status of cohorts of men: unemployment transitions
Transition Type
45-49
(52-56)
50-54
(57-61)
55-59
(62-66)
60-64
(67-71)
Unemployed/inactive
Full-time + unemployed 11.3 6.3 0.5 0.0
Full-time + inactive 8.2 16.1 28.8 23.7
Unemployed + inactive 4.8 5.2 6.4 12.1
Full-time + unemployed +
inactive
4.8 8.3 5.8 2.7
Other 1.0 0.6 2.3 8.7
30.1 36.5 43.8 47.2
Source: British Household Panel Survey, Waves A-H (base = 1,132) (own calculations)

• IMPACT OF HEALTH FACTORS

Main reason for early retirementMen
Cell percentages Age Total
50-55
55-59
60-64
Offered reasonable financial terms to retire early 22 31 31 30 Own ill health 49 24 24 27 Made redundant etc 5 15 15 14 To enjoy life while still young and fit enough 19 11 13 13 Fed up with job and wanted a change - 8 8 7 Ill health of a relative/friend 3 5 4 4 To spend more time with partner/family - 2 1 1 To retire at the same time as husband/wife /partner - - 1 * Do not know 3 4 3 3 Total 100 100 100 100 Base: all respondents 32 104 209 345
Source: English Longitudinal Study of Ageing (ELSA), Wave 1 2002 (own calculations)

Main reason for early retirementWomen
Cell percentages Age Total
50-55
55-59
Own ill health 27 35 33 Offered reasonable financial terms to retire early 9 16 14 To spend more time with partner/family 5 15 12 Made redundant 9 9 9 Fed up with job and wanted a change 14 7 9 To enjoy life while still young and fit enough 14 4 7 Ill health of a relative/friend 5 6 6 To retire at the same time as husband/ wife/partner 9 3 4 Could not find another job - 1 1 Do not know 9 4 56 Total 100 100 100 Base: all respondents 26 84 110
Source: English Longitudinal Study of Ageing (ELSA), Wave 1 2002 (own calculations)

Percentage of individuals aged 50 to 65 in paid work in 2002-03 who stay in paid work or move out of paid
work between 2002-03 and 2004-05, job type and self-reported health status in 2002-03 (men only)
Manual Workers Non-Manual Workers
Fair/poor Good V.good
/Excellent
Fair/poor Good V.good/
Excellent
% % % % % %
Working, working 68.8 86.9 87.2 80.5 84.8 88.3
Working, not working 31.2 13.1 12.8 19.5 15.2 11.7
Source: English Longitudinal Study of Ageing, Wave 2 (Emmerson & Tetlow, 2004)

Health problems (for those who report a problem) by gender (cell%)
Male Female Health problem lasting more than a year: Yes 45 41 No 55 59 Base 9,745 7,468 If yes, nature of problem Problem with arms, hand 21 29 Problems with legs or feet 29 32 Problems with back or neck 29 35 Heart, blood pressure, circulation 30 20 Other 58 57 Base 4,743 3,241 Note: Approximately a quarter of men and women received benefits. Male (50-64) Women (50-59) Source: Labourforce Survey (Cappellari et al, 2005)

Expected chances of returning to paid employment for economically inactive individuals below SPA
Cell percentages Sample
Size Fraction reporting zero
chance of working in future
Average percentage chance of returning to
work Men, 50-59 All inactive 409 65 15 Inactive and retired 141 75 9 Men, 60-64 All inactive 404 83 6 Inactive and retired 240 84 5 Women, 50-54 All inactive 270 64 15 Inactive and retired 29 - - Women, 55-59 All inactive 440 74 9 Inactive and retired 122 74 8
Note: Men below 60 are asked the chances of their being in paid employment at or after age 60; those between ages 60 and 64 are asked the same question with reference to age 65 . Women below age 55 are asked the chances of their being in paid employment at or after age 55; those between ages 55 and 59 are asked the same question with reference to age 60. Source: English Longitudinal Study of Ageing (ELSA) (Banks and Casanova, 2003)

Reported desired changes to working situation among those reporting that they have health problems that limit
their ability to work in their current job
42.9
25.9
7.8
15
3.1
5.8
11.1
0 5 10 15 20 25 30 35 40 45 50
Any change
Less physically demanding
Special equipment/workplace adaption
Less mentally demanding/stressful
Flexible hours
Working from home sometimes
Fewer hours/job sharing
Percentage
Source: English Longitudinal Study for Ageing, Wave 3 (Emmerson & Tetlow, 2004)

Proportion of men and women who had the opportunity to work past retirement age by
previous occupational category
01020304050607080
%
Source: English Longitudinal Study of Ageing (ELSA), Wave 1 2002 (own calculations)

Proportion of employees who have attended a formal educational or training course during the past 12
months
Source: English Longitudinal Study of Ageing (ELSA), Wave 1, 2002
Key messages on barriers
• Health status – especially major health changes - most important factor ‘pushing’ people out of work.
• Earlier the retirement the more it is driven by health.
• Men and women in lower social class social groups more likely to cite health factors.
• Working class groups more limited opportunities of working up to 65.
• Once out of work unlikely to return.

Problems in current policies• Raising pension age reinforces health inequalities.• Under-pensioned groups ‘forced’ to remain in
labour market despite health problems (especially manual workers, ethnic minorities).
• ‘Triple jeopardy’ of poor health, lack of work training, inadequate pension provision.
• Failure to tackle poor working conditions and oppressive management styles both of which may be predictors of early retirement.

Policy Options
• New emphasis on tackling health inequalities in the workplace (but note problems of SMEs).
• Workplace as setting for improving health and well-being (but globalization increasing pressures on workers).
• Focus upon occupational health in middle-life (though services being cut in many places).
• Specialist support for migrant workers (given complex work histories).
• Support for those balancing caring and working roles.• Different needs short and long-term unemployed.• Focus on key groups such as line managers whose attitudes
towards older workers may be crucial.
WORK, HEALTH AND WELL-BEING:
RESEARCH NETWORK
Some research questions:
• What is the role of line managers as gatekeepers facilitating return to work? What variations can be identified in terms of the impact of their in respect of mental health and musculo-skeletal issues?
• What role is played by different work environments in assisting return to work/retention etc?
• What forms of collaboration can be identified between health organisations and employers?
• What is the role of self-care? How can its effectiveness be enhanced within the workplace?

Acknowledgements
• Rowntree Foundation and Department of Work and Pensions for funding for data analysis of sections of the paper.
• Dr. Jim Ogg (Young Foundation, UK) for work on the British Household Panel Survey and English Longitudinal Survey on Ageing.

References
• Banks, J. and Tetlow, G. Extending Working Lives. In Living in the 21st Century. In: The 2006 English Longitudinal Study of Ageing (Wave 3). Institute for Fiscal Studies, 2008.
• Cappellari, L. et al. Labour market transitions among the over-50s. Department for Work and Pensions, 2005.
• Emmerson, C. and Tetlow, G. Labour Market Transitions. In: The 2004 English Longitudinal Study of Ageing. Institute for Fiscal Studies, 2006.
• Loretto, ed The Future for older workers. Policy Press, 2007
• Phillipson, C. Transitions from work to retirement. Policy Press, 2002

Selected references
• Phillipson, C and Smith, A. Extending Working life: a review of the research literature. Department for Work and Pensions, 2005.
• Phillipson, C. Extending Working Life: problems and prospects for social and public policy. In Bauld, L. et al. Social Policy Review Policy Press, 2006
• Smeaton, D. and Vegaris, S. (2009) Older people inside and outside the labour market. Research Report No. 22. EHRC
• Schmid, G.Towards a theory of transitional labour markets. In Schmid, G and Gazier (eds) The dynamics of full employment. Edward Elgar, 2002.
• Vickerstaff, S. et al. Encouraging labour market activity among 60-64 year olds. Department of Work and Employment, 2008.

Measuring Ill-health and older workers: a comparison of the US
and the UKDavid Lain
University of Brighton, [email protected]

Health and employment past 65 in the US and England
• Previous research indicates health is an important influence on employment past age 65. However, hard to measure / compare.
• More needs to be known about how the influence of health on employment is mediated through other known influences, such as education and wealth.
• Using English Longitudinal Study of Ageing 2002 and US Health and Retirement Study 2002, I will examine:
1. How can we compare health using these surveys?2. How does health interact with wealth and education to
influence employment past 65?3. How does this vary between the countries?
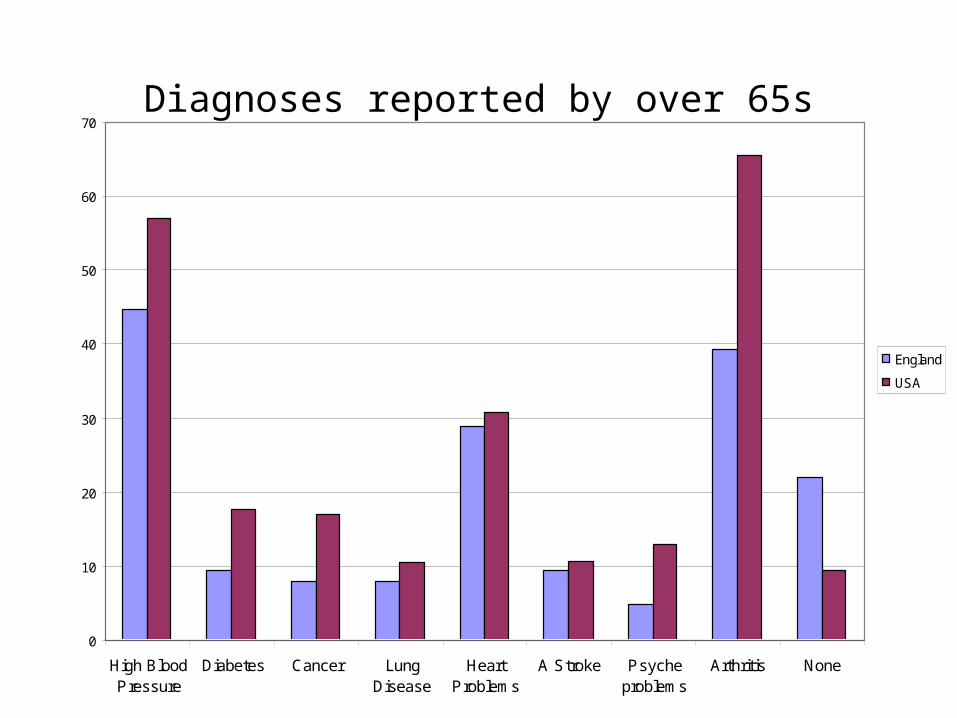
Diagnoses reported by over 65s
0
10
20
30
40
50
60
70
High BloodPressure
Diabetes Cancer LungDisease
HeartProblems
A Stroke Psycheproblems
Arthritis None
England
USA

Difficulties reported by over 65s
0
10
20
30
40
50
60
Walk
ing se
vera
l bloc
ks
Sitting
for 2
hrs
Gettin
g up
from
a ch
air
Climb
seve
ral fl
ights
of st
airs
Stoop
ing/kn
eelin
g/cro
uchin
g
Difficu
lty lif
t/car
ry 1
0 lbs
Picking
up
coin
Reach
ing/e
xtend
ing a
rms u
p
Pushin
g pu
lling
objec
tsNon
e
England
USA
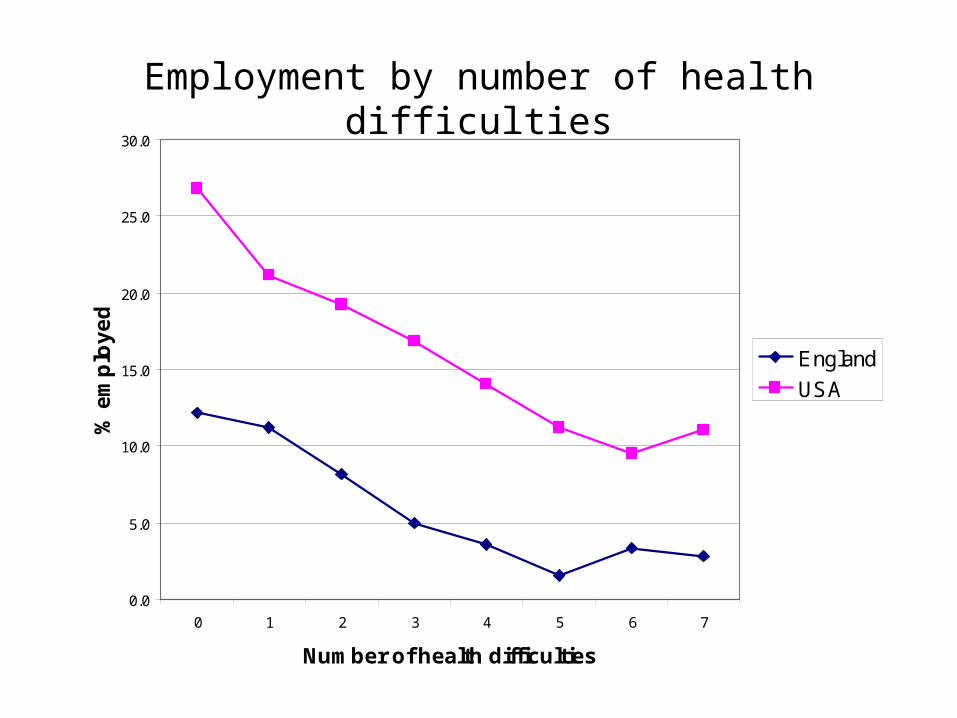
Employment by number of health difficulties
0.0
5.0
10.0
15.0
20.0
25.0
30.0
0 1 2 3 4 5 6 7
Number of health difficulties
% e
mp
loy
ed
England
USA

Employment Ratio: low : medium/high education
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4
Number of health difficulties
Em
plo
ym
en
t ra
tio
(lo
w:
me
diu
m/h
igh
ed
u)
England
USA

Employment Ratio: Bottom 2 wealth quintiles : Top 3 quintiles
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 1 2 3 4
Number of health difficulties
Em
plo
ym
en
t ra
tio
(b
ott
om
: t
op
)
England
USA

Employment past 65 by wealth quintile, 2002
• Source: Analysis of the English Longitudinal Study of Ageing and Health and Retirement Study
England USA % Ratio
1st quintile 11.5 21.7 1.9
2nd quintile 8.5 17.7 2.1
3rd quintile 6.1 18.9 3.1
4th quintile 5.2 17.4 3.3
5th quintile 2.7 12.6 4.7
Total 6.8 17.7 2.6
Base 5508 10392

Influence of wealth on employment past age 65: Odds ratios from logistic regression analysis
Model 1 (wealth + age)
Model 2 (wealth + age + health + edu)
England USA England USA
Q1 1.00 1.00 1.00 1.00
Q2 0.72* 0.76** 0.86 0.85
Q3 0.50*** 0.81** 0.66* 1.00
Q4 0.50*** 0.75*** 0.73 1.02
Q5 0.27*** 0.54*** 0.45*** 0.82*• Note:*** = p<0.001, ** = p<0.01, * = p<0.05.
Conclusions
• Comparative research can help us understand what is specific to the English situation.
• In both countries: Employment declines as health worsens (but employment higher at all health levels in US).
• In both countries: Education increases the likelihood of working for people with health difficulties.
• In England: Low levels of wealth reduce likelihood of working (except for the very healthy ‘poor’);
• Institutional explanation: means-tested benefits.• Adopted ‘difficulties’ measure of health; need to consider the
social construction of health measures.

Does an understanding of occupational identity help to explain
vocational rehabilitation outcomes for older workers?
Dr Joanne RossNHS Eastern and Coastal Kent

Vocational rehabilitation
• “a process whereby those disadvantaged by illness or disability can be enabled to access, return to, or remain in, employment, or other useful occupation.”
(British Society of Rehabilitation Medicine 2003 p1)

Current perspectives in vocational rehabilitation

Lifespan perspective
• Younger worker:– accessing employment
• Older worker: – returning to and remaining in employment

A condition-focused perspective
• A ‘medical model’ approach seeks to understand:
• the disease process
• the nature and aetiology
• the impairment or disability
• the anticipated course
• management of the condition.

A functional perspective– A functional approach seeks to understand:
• the functional implications of a medical diagnosis– physiological
– physical
– psychological status
• the functional capacity of the worker
(Ross J 2007)

A bio-psychosocial perspective
• The bio-psychosocial model seeks to understand:– the nature of the disability or condition– psychological factors– social contextual factors – eg. family
influences, environmental barriers
(Waddell G, Burton KA, Kendall N 2008)

An occupational perspective
• An occupational approach seeks to understand:– the person– the environment– the occupation
and – the interface between them
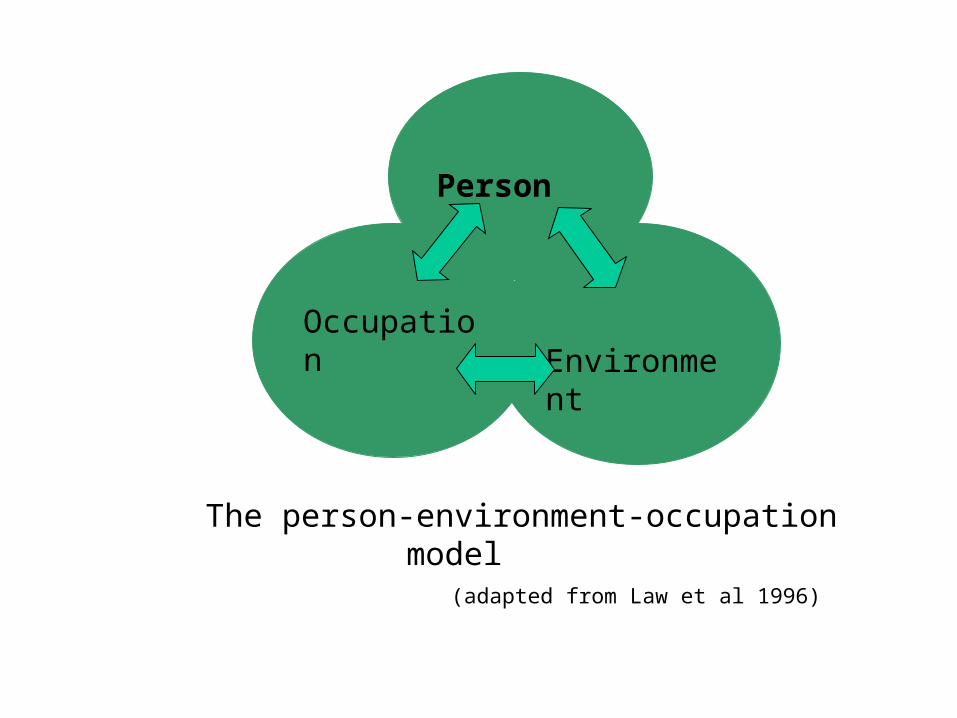
Environment
Occupation
Person
The person-environment-occupation model (adapted from Law et al 1996)

What is an ‘Occupation’?• Human occupation:
• ‘Groups of activities and tasks of everyday life, named, organized and given value and meanings by individuals and a culture. Occupation is everything people do to occupy themselves, including looking after themselves (self-care), enjoying life (leisure) and contributing to the social and economic fabric of their communities (productivity).’ (Townsend 2002 p34)
• ‘Occupation, or the ordinary and extraordinary things that people do every day, is central to the way we all live our lives – what we are, who we become and how we achieve our dreams and aspirations.’
(Watson 2004 p3)
An occupational perspective in vocational rehabilitation

Environment (Workplace)
Occupation (Work)
the nature of the illness / injury the condition experience
occupational identity
Person
The participation in work framework: the person-centred stage (Ross 2008)
The occupational identity
• ”……. if someone’s got childcare issues, I’ve had quite a number of those, childcare is not anything to do with the disability, but someone’s circumstances might of actually changed and you have to take that into consideration…. in terms of an active return to work, facilitating that return to work, you have to look at all the various components and what will actually work with someone.”
• “I emphasise sort out the social life and the recreational life first, which will give us guidance as to how you are going to function in the workplace.”

Occupational identity…..
• is underpinned by the value and meanings which an individual attaches to their daily occupations
• is made up of the unique blend of activities which make up the daily life of an individual
• includes the roles and routines which a person performs on a day-to-day basis
• the balance of occupational roles and activities contributes to an individual’s health and overall sense of well-being
• extends beyond, the person’s work life (worker identity)• is shaped by family roles and social supports• changes across the lifespan• is influenced by the nature of a health condition and the person’s
illness/injury experience.

• “I’m actually a member of a Buddhist group...... and a lot of our meetings are always in the evening anyway, so I was missing out a lot of that and that to me was quite important , so what actually happened was that (the OT) said she thought that would be beneficial as well, if we could change my shifts somehow...”

occupational identity
worker identity

Workplace (environment)
The participation in work framework: the worker identity stage
Work(occupation)
Person as a worker
feeling fear
the value attachedto work
the ‘person-work’ match
Defining the work activity
worker identity

Worker identity
– is one element of a person’s occupational identity
– Is the person’s perceptions of themself as a worker or potential worker
– Includes paid and unpaid work roles (volunteer, carer)
– includes the values and meanings which the person attaches to work
– the value attached to work is not static, it changes over time and across the lifespan
– may be altered by a significant life event.
• “….he’s a married man, his wife has had to go out and work……he was the house husband. Their roles had changed and the patterns that they’d developed, and he has a very close relationship with his wife ……she was very much reinforcing that he couldn’t work……”
• “His wife has quit work to look after him so now neither he or his wife work.”

Key implications for the older worker
• Following the onset of a health condition or disability:
– a person chooses to resume those occupations which are most highly valued
– occupational identity influences the person’s decision about a return to employment
– ‘worker identity’ may be altered
– a fear of returning to work is common
– the longer the person is away from work, the less value they may attach to it
– paid work occupations may be replaced with unpaid occupations.

References• British Society of Rehabilitation Medicine (2003). Vocational Rehabilitation – The
Way Forward. London, BSRM.• Law M et al (1996). The Person-Environment-Occupation Model: A Transactive
Approach to Occupational Performance. Canadian Journal of Occupational Therapy vol 63,1 p 9-23.
• Ross J (2007). Occupational Therapy and Vocational Rehabilitation. West Sussex. Wiley and Sons.
• Ross J (2008). The participation in work framework: an occupation-focused perspective of rehabilitation for work. Conference proceedings. Paper presented at the 8th European Congress of the Council of Occupational Therapists for the European Countries (COTEC), Hamburg, Germany. May 2008.
• Townsend E (ed) (2002). Enabling Occupation; An occupational therapy perspective. Ottawa. Canadian Association of Occupational Therapists.
• Watson R & Swartz L (Eds) (2004). Transformation through Occupation. London. Whurr Publishers.

Understanding the impact of health and health pessimism on the extending work life agenda
Sarah Vickerstaff

On the threshold of a new era?
In an era of workforce ageing and increasing life expectancy working longer may be presented as an ‘unavoidable obligation’. The Government’s urge to extend our working lives is summed up in the title of the recent OECD review of policies: Live Longer Work Longer.

Reasons for economic inactivity: by sex and age, 2008
Table 4.20
Reasons for economic inactivity: by sex and age, 20081
United Kingdom Percentages
16–24 25–34 35–49 50–59/64All aged
16–59/64Men
Long-term sick or disabled 5 40 62 49 34Looking after family or home 1 9 16 6 6Student 82 27 4 - 33Retired 0 0 1 33 13Other 10 17 12 9 11
All men (=100%) (millions)2 1.2 0.3 0.5 1.3 3.3
WomenLong-term sick or disabled 3 8 24 41 19Looking after family or home 23 72 61 27 45Student 66 10 4 1 22Retired 0 0 - 14 3Other 8 8 8 14 9
All women (=100%) (millions)2 1.3 0.9 1.4 1.1 4.7
2 Includes discouraged workers and those who are temporarily sick.1 Data are at Q2 and are not seasonally adjusted. See Appendix, Part 4: Labour Force Survey.
Source: Labour Force Survey, Office for National Statistics
Source: Social Trends, No 39, 2009 Edition, ONS.

Government’s agenda
• Target 80% employment rate• Work as the best form of welfare • Reduce numbers on Incapacity Benefit (now
Employment Support Allowance) by 1 million and keep people with health conditions in work
• Extending working life: encourage people to delay retirement and work for longer
• New Deal for Carers

Health and work
• 7% of the working age population are receiving incapacity benefits due to ill-health or disability
• 3% of the working age population are off work due to sickness at any one time
• May 2008 GB total for IB 2.6m claimants: 1.5m men and 1.1m women
• Target of 1m reduction in IB claimants by 2016

Doctors assessment of the nature of the claimants’ health problems and medical basis of the incapacity claim
Women (%) Men (%)
Mental behavioural 41 41
Musculoskeletal 22 20
Nervous system 7 6
Injury, poisoning 4 5
Respiratory 3 2
Circulation 2 5
All other 20 20
Source: DWP Figures quoted by Beatty, Fothergill, Powell, Houston and Sissons (2008),Women on Incapacity Benefits; New Survey evidence
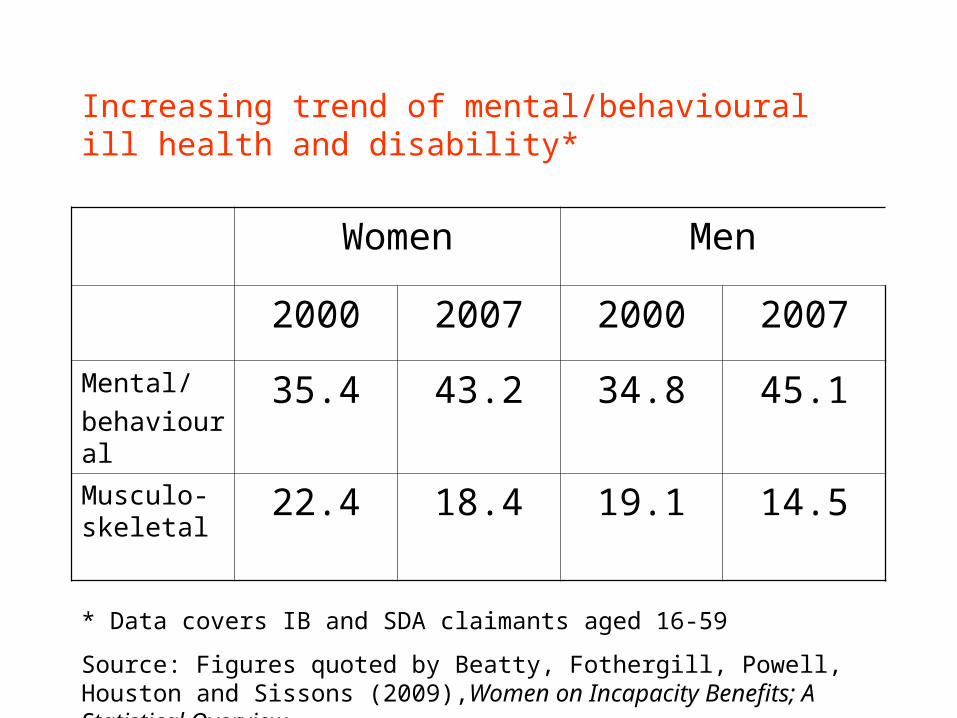
Increasing trend of mental/behavioural ill health and disability*
Women Men
2000 2007 2000 2007
Mental/
behavioural35.4 43.2 34.8 45.1
Musculo-skeletal
22.4 18.4 19.1 14.5
* Data covers IB and SDA claimants aged 16-59
Source: Figures quoted by Beatty, Fothergill, Powell, Houston and Sissons (2009),Women on Incapacity Benefits; A Statistical Overview

Qualitative research: • Commissioned by DWP
• Interviews with couples and individuals (96 people – 49 women;47 men - in total)
• Based in three areas: Edinburgh, Nottingham and Thanet
• Sample selected on the basis of age, income, labour market status, health and domestic circumstances

Profile of the sample
Income band Edinburgh Nottingham Thanet
Under 10,000 0 1 15
10,000-20,000 8 13 9
21,000-30,000 13 6 3
31,000-40,000 5 6 0
Over 41,000 2 5 1
Unassigned 5 1 3
Self-reported Household Income
Complexity of the “illness experience” and its impact on working and work transitions
- the condition itself
- the nature of the work environment
- the nature of the work
- GP, NHS responses
- the need or motivation to work
- the role of family and friends
- the individual’s resilience
Managing work and healthColin who is currently 60 had worked for the Police but retired in 1995 going on to work for British Gas for five years. In his forties he had had two heart attacks and a heart bypass at 50. His health continued to be a worry. He had also remarried in his forties and at the time of interview had three children under the age of 16. Two years ago he realised that he needed to scale down his work because of his health, although he wanted to continue working. He went back to working for the Police on the civilian side and had negotiated a job-share arrangement:
‘Obviously because of previous medical problems, I’ve got to be careful what I do, so, as I say, I’m on a job-share, so I’m OK with that because it means that because it’s a shift-system that I work, it means there’s long periods when I’m off…. Well, normally I would work until 65. But obviously with a second marriage and young children I’ve got to keep my options open and also the new age act that’s come in, it opens doors for me that would have been closed previously’.
Source: Vickerstaff et al ((2008) Encouraging Labour Market Activity Among 60-64 Year Olds, Research Report no. 531 DWP.

Colin’s illness experience
Flexible work
available
Strong push
to work
from family
Financial
motivation
Benign work
environment
Heart
problems
ongoing
Illness
experience

Forced to give up workCarol worked for over 10 years in a independently run centre for disadvantaged children, having been a respite foster carer previously. She was a day-care leader for pre-school children. The work was increasingly stressful:
I mean an example would be that, you know, I went to one particular funeral where I’d buried a mum, her baby of just over a year and her little girl of 3 years and I’d been cuddling those 2 children a few hours before this fire and had got quite a good relationship going with this mum and she finally was able to open up.
Carol had to go back to work straight after this event and soon after went on sick leave with headaches and anxiety and never returned to work.
Source: Vickerstaff et al ((2008) Encouraging Labour Market Activity Among 60-64 Year Olds, Research Report no. 531 DWP.

Carol’s illness experience
Stressful work
GP rather
passive
Children had
left home,
could cope
on benefits
Poor
management
Mental
health
Illness
experience

The prospect of ill health‘ I would like to carry on doing something for as long as I could, you know so…I always want to remain active, doing something, for as long as physically possible I suppose so I don’t know [when he might retire completely]. I find that difficult to answer directly, but…it depends on my health.’ (ES36Male)
‘Health might have an influence on that obviously [how long he might carry on working]. But things change don’t they? I mean that’s the thing and I might…Whatever I’m saying now things might happen.’(NS72Male)

Health pessimism: ‘No-one was getting any younger’
So from our point of view, we just want to enjoy it [retirement] while we’ve both got health to do it. Because there’s so many people work right to the end of their retirement, you know, whether they’re 60 or 65, and never get a good retirement, you know, for health reasons, and, well, we feel we’re fortunate we can do it now and enjoy it. (EC50F)

Actuarial statistics versus the experience of families, friends and colleagues
‘People that work downs a pit, you work under ground and you retire at 60. That’s standard. If you work on the surface you retire at 65. We had a deputy retire at the pit on the Friday and he died on the Sunday.’ (TC14Male)
‘But I can always remember when we had this round of redundancies, they also let people retire early and there was one particular chap, I had known him all my working life. He was a welder, working on the shop floor, but he’d got a passion for golf and he was quite good, and he retired two years early – say he was 63 – and on his 65th birthday he was playing golf, well he had a heart attack and died, and, you know, that’s always stuck with me for some reason.’ (NC63 Male)
Cultural view that people should not leave it too late to enjoy retirement:
‘And the one thing, just maybe to get a little bit out of it [retirement] because I’ve lost a load of friends who have died quite young, who have died not long after their retirement age and I thought “maybe it is time to get some social time to yourself”.’(ES45Female)
‘We want to retire together because neither of our parents had any retirement together so I mean my mum died at 48 and my father died at 65 and his mum died at 60. His dad did live until he was nearly 80 but on his own, you know, and so we… while we’ve got good health, touch wood, we want to enjoy it so…’ (NS75Female)
Responses to state pension deferral opportunities: carpe diem
‘Because you never know what’s round the corner.’ (EC33Female)
‘But my argument is if you’re retired and you’re older, live for the moment! .... No, because you might just, you just might not be there. Just enjoy it, use it.’(EC35Female)
‘I will retire at 65 and get what’s coming, if I can make it to 65.’ (TC14Male)
‘I think it’s a cop-out for the government honestly. It’s a way of them keeping the money, hoping you curl your toes and they keep the money!’ (NS69Female)

Conclusions• Impact of health issues on continuing or
ceasing work complex, multifaceted, need a bio psychosocial model
• Very important impact of role models; family friends, colleagues more persuasive than the ‘facts’
• Health subjectivities, health pessimism a significant factor in how older workers think about the future and retirement in particular




![Presentation to Workplace Health Champions at [Workplace Name]](https://static.fdocuments.net/doc/165x107/551bcd74550346be588b526b/presentation-to-workplace-health-champions-at-workplace-name.jpg)













