with Surgery/Endoscopy to Improve Workflow of … · Surgery/Endoscopy to Improve Workflow of...
55
Collaborating with Surgery/Endoscopy to Improve Workflow of Specimens from Electronic Order to Arrival in the Laboratory Debbie Dickman, MA MT(ASCP)SH M.A. Womack, MBA (ASCP) SBB Certified Six Sigma Black Belt “Never let a good crisis go to waste” Winston Churchill
Transcript of with Surgery/Endoscopy to Improve Workflow of … · Surgery/Endoscopy to Improve Workflow of...

Collaborating with Surgery/Endoscopy to Improve Workflow of Specimens from
Electronic Order to Arrival in the Laboratory
Debbie Dickman, MA MT(ASCP)SH
M.A. Womack, MBA (ASCP) SBBCertified Six Sigma Black Belt
“Never let a good crisis go to waste” Winston Churchill

2

3
CENTER FOR DIAGNOSTIC PATHOLOGY (CDP)

Florida Hospital’s Lean Journey• Started with Core lab and phlebotomy processes in 2002
• Next in Blood Bank in 2003 with a small team “leaning” Blood Bank processes
• Developed a system‐level QA/PI position in 2003• Expanded to department level projects, such as Microbiology projects by 2010
• Infiltrated the entire lab by 2012 (Clinical/Pathology)• Developed an Orlando based Process Improvement Manager position in 2012
4

Circle of Pathology
Accession
Gross Process
Embed
Cut
Slide/Stain
Slide Distribution
PathologistRead/Dictate
Transcribe
Review/Sign Release Print
Order
5

Pathology Volumes
6
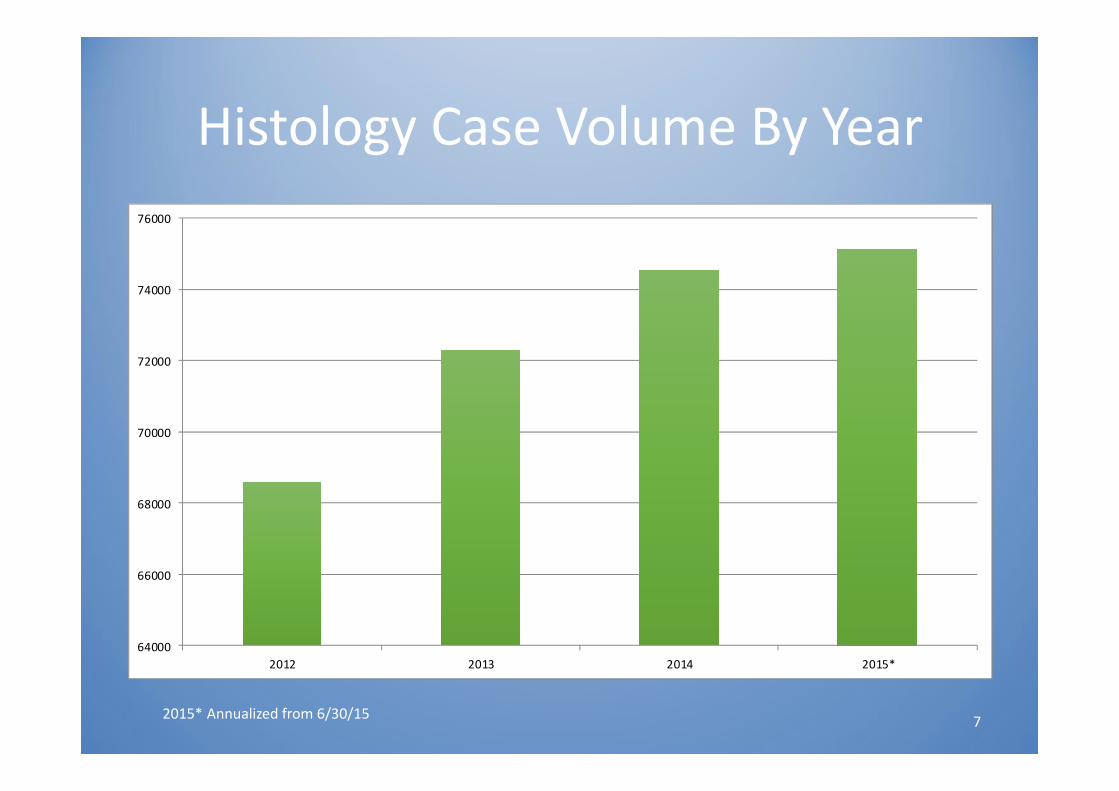
Histology Case Volume By Year
64000
66000
68000
70000
72000
74000
76000
2012 2013 2014 2015*
2015* Annualized from 6/30/15 7

• Cytology• Immunochemistry• Histology• Diagnostic Hematology
> 2100 Slides Assembled Daily
• 21 Pathologists• 8 Campus locations
Cases Distributed • For storage
• For redeployment• Continuum of care• Tumor Boards• Send out tests• Legal purposes
Slides and Tissue Blocks Returned
High‐Level Specimen Process
8
Problem StatementWhat was the crisis?
Three incidents of missing or mismatched specimens occurred in summer 2014, triggering a series of IMMEDIATE and SYSTEMATIC process changes:
1. Procedural: endoscopy specimen mismatch
2. Transport: tote carrying 15 specimens missing after courier pick‐up
3. Pathology: specimen slide mismatch at the Center for Diagnostic Pathology (CDP)
9
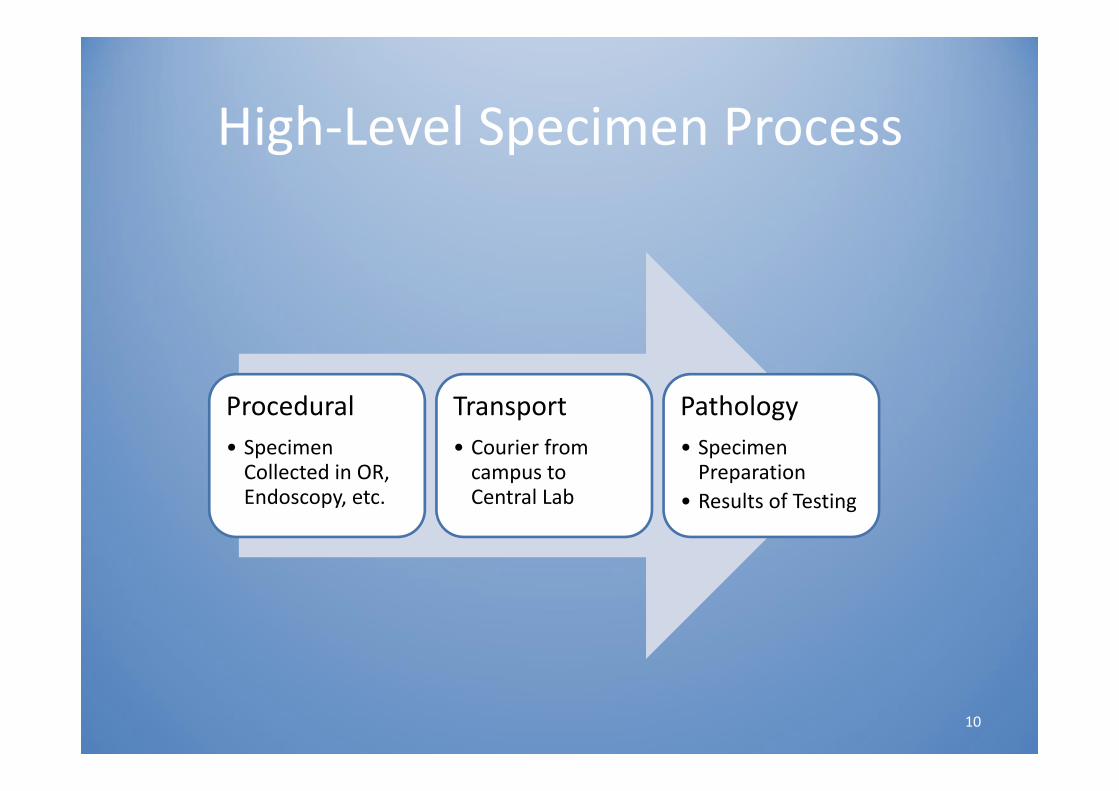
High‐Level Specimen Process
Procedural• Specimen Collected in OR, Endoscopy, etc.
Transport• Courier from campus to Central Lab
Pathology• Specimen Preparation
• Results of Testing
10

Specimen ProcessSYSTEMATIC SOLUTIONS
Procedural• No pre‐numbering, SOP update• Electronic specimen order entry• Surginet (PathSP interim)
Transport• RFID tracking of totes• Exclusive chain‐of‐custody FH
couriers• Alert for overdue specimen
Pathology• Bar‐coding for specimen slides• Dedicated slide printers• Receiving staff• Formal escalation plan
11

Objectives
• Describe development and deployment of electronic orders from procedural areas for Pathology specimens
• Outline pathology specimen tracking from point of collection until delivery in Pathology
• Address single piece flow in Pathology Accessioning, Grossing and Histology to prevent mismatch errors 12
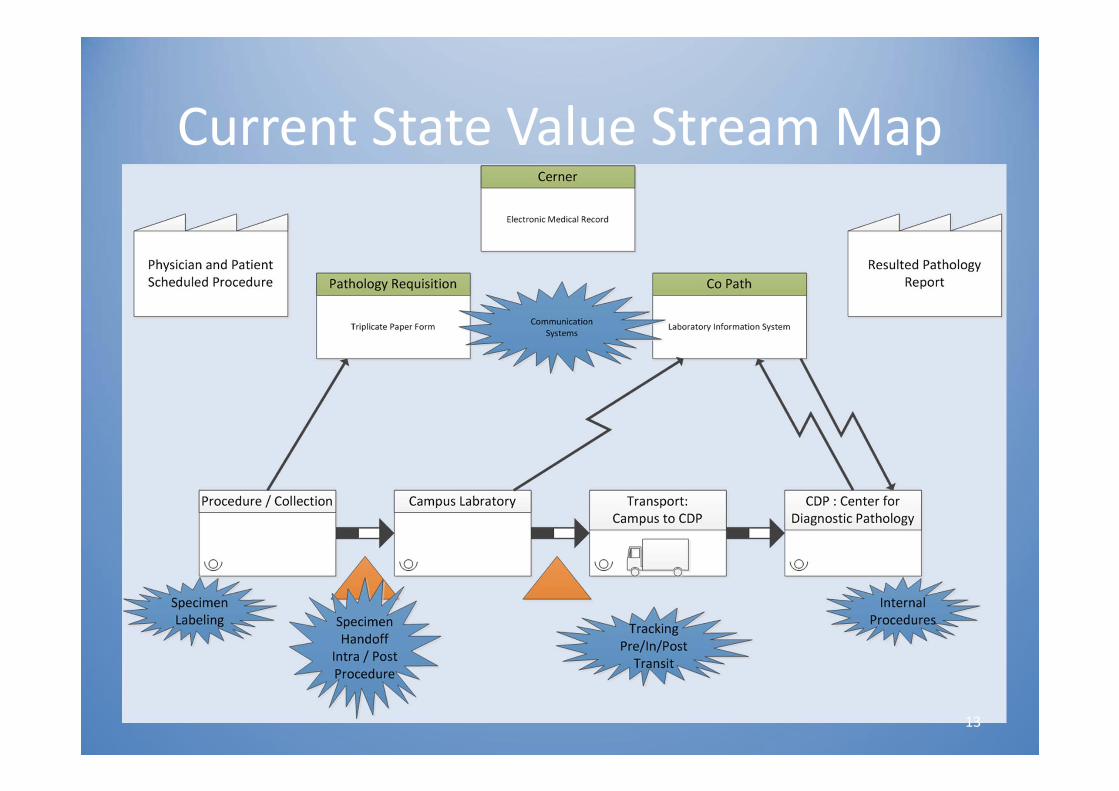
Current State Value Stream Map
13
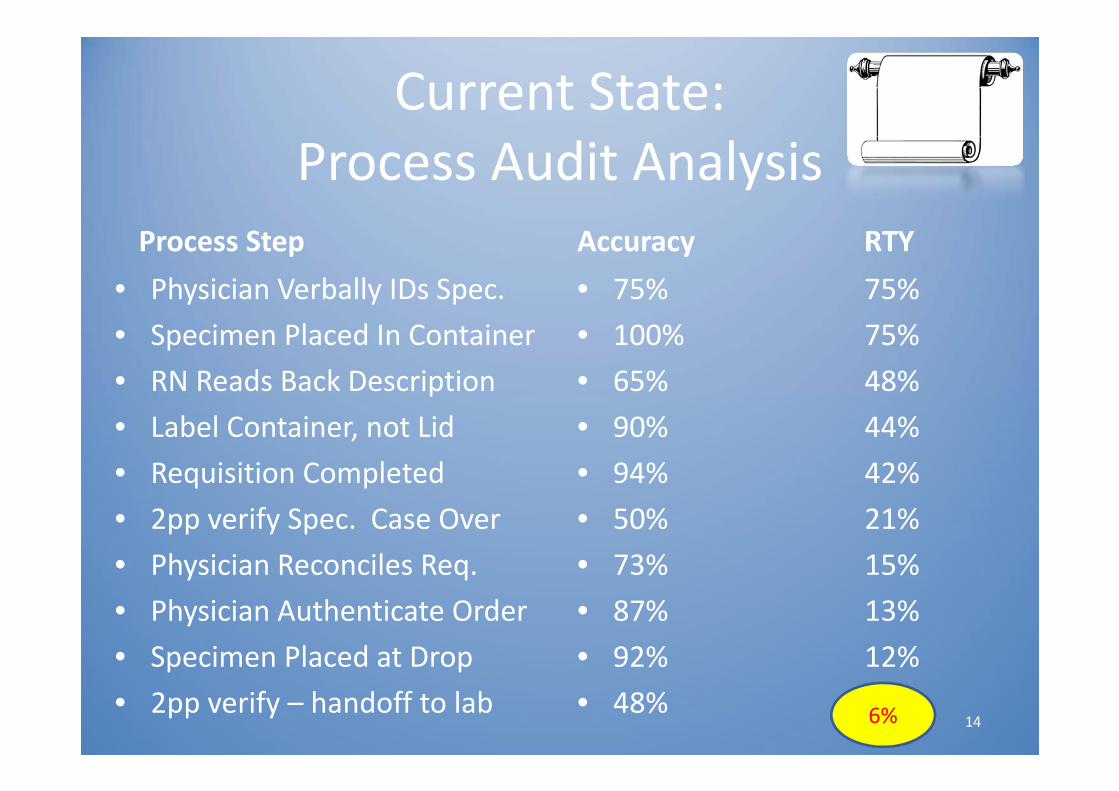
Current State: Process Audit Analysis
Process Step• Physician Verbally IDs Spec.• Specimen Placed In Container• RN Reads Back Description• Label Container, not Lid• Requisition Completed• 2pp verify Spec. Case Over• Physician Reconciles Req.• Physician Authenticate Order• Specimen Placed at Drop• 2pp verify – handoff to lab
Accuracy RTY• 75% 75%• 100% 75%• 65% 48%• 90% 44%• 94% 42%• 50% 21%• 73% 15%• 87% 13%• 92% 12%• 48% 6%6% 14

Procedure/Collection:Failure Modes
• Same case, multiple frozen specimens: requires separate lab sheets and is time consuming
• Specimen Not Always Placed in BioHazard Bag• Procedure Area Staff Comment, Time Could be Better Spent Getting Next Case Ready Instead of Transporting Specimen to Laboratory
• After Hours Procedures Are Different, Causes Error
15

Procedure/Collection:Failure Modes
• Use of Outdated Requisition Forms. Using Up Stockpile.
• New Transporters Unaware of the Handoff Procedure• Cases with 20 Specimens or More, Contamination/ Infection Control Issue if Not All Containers Used
• Pre‐Labeling of Syringe Before Drawing Sample
16

Specimen Collection Process: Campus to CDP ‐ Failure Mode
• Lack of a single identifier for a sample from the point of collection, i.e., barcode
• Multiple versions of requisition forms and therefore lab collection processes . For example separate requisitions for Radiology, L&D, OR/Endo and Corresponding paper logs
• Electronic orders in less than 10% of specimens followed
17

Specimen Collection Process: Campus to CDP ‐ Failure Mode
• Varied identifiers used during specimen hand‐off (last 4 digits of FIN, MRN)
• Batching during (Co‐Path) ordering/accessioning process: – Data entry from requisition form– Case number manually written onto requisition form– Pre‐printed labels with case numbers are affixed on the specimen container
– When more than two samples case number is manually written on the specimen container
18
Transport and CDP Processes: Failure Mode
• Log that accompanies the specimen is generated in duplicate – Copy of the Tote Log stays with the Campus Lab– Copy travels with the Tote and is completed at CDP
• The loop is not closed; the campus lab does not receive confirmation of delivery of specimens at CDP
• No consistent way to track down which samples were in a tote (In the case that a tote is missing)
• Samples may be dropped off when Histotech is away from desk without a hand‐off process
19

PathologyProcessing Steps
Accessioning Grossing Tissue Processing
EmbeddingCuttingStaining
Slide Distribution
20

Pathology Specimen Processing: Failure Mode
• Accessioning: Mismatch specimens with cassettes⁻ Batch processing of specimens and cassettes⁻ Multiple specimens and cassettes co‐located on same cart
• Cassette and specimen have the potential to be mixed up
⁻ Pink copy of requisition compiled together• Sometime forms are illegible
21

Pathology Specimen Processing: Failure Mode
• Grossing: mismatch of specimen with cassettes⁻ Co‐location of specimen and cassettes
• Matching specimens, requisitions, and cassettes⁻ Multiple cassettes for multiple specimens printing to one common cassette printer
• Pathology assistants locating specific cassettes for their case
22

Pathology Specimen Processing: Failure Mode
• Cutting: mismatch of blocks/cassettes and slides⁻ Batch processing of slides
• Blocks/cassettes may need to be re‐embedded• Slide count no longer matches number of blocks/cassette
• Loss of 1‐to‐1 ratio• Mismatch of specimen to slide
23

Pathology Specimen Processing: Failure Mode
• Slide Distribution: misplacement of slide folders⁻ Routing slip filled out incorrectly
• Wrong pathologist marked to receive slide (results in mismatched assignment in system)
⁻ Folders placed in wrong box• Slide folders sent to wrong campus or location
– Increase lead‐time for analysis of specimens
24
Proposed Solutions
25

PROPOSED SOLUTIONS Procedure Areas
• Electronic Pathology orders in Cerner to Sunquest
• Campus roll out over 6 month schedule
Tracking of Specimens from Procedure to
Resulting
• 2 person read‐back verification at bedside: Hard Stop
• Receipt at Point of Service by Lab with laptop
Specimen Verification
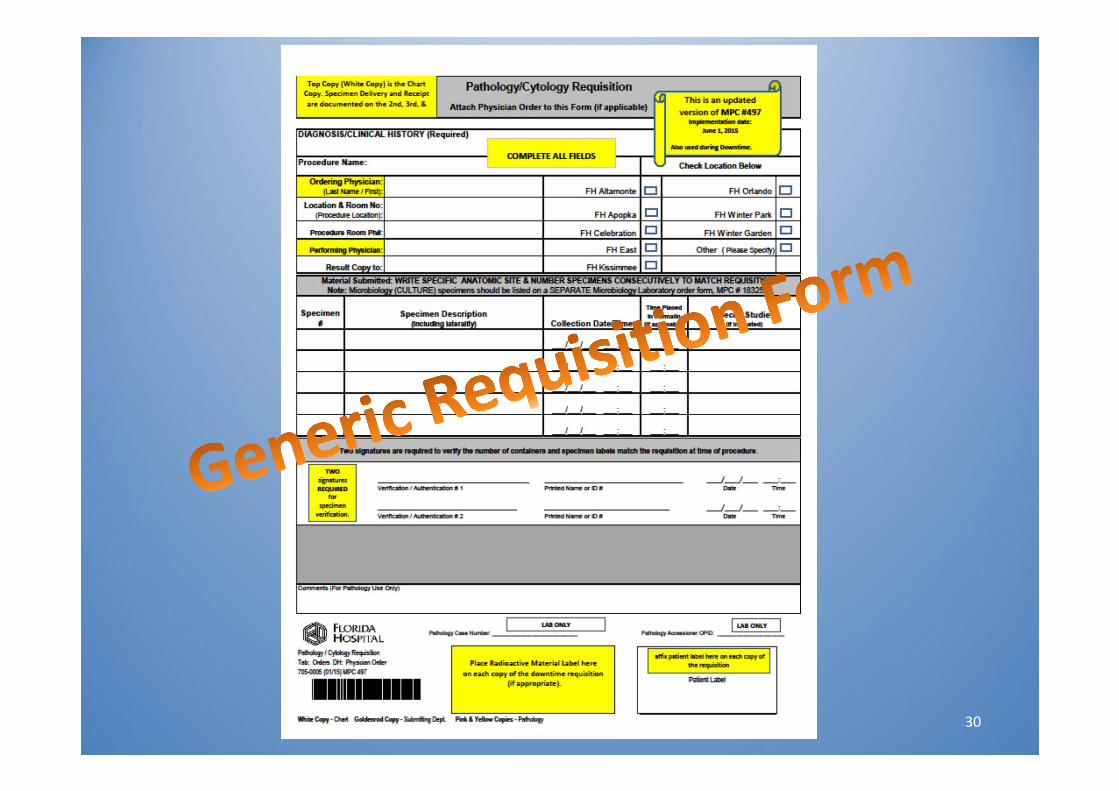
• SOP revisions: Specimen ID• One form for downtime use• Secure Specimen Locations• Tamper‐proof Containers for Endoscopy
Standardization
26

‐Fields in Yellow are Mandatory (including the Procedure Name field)‐Use Free Text to enter result for fields Procedure Name, Preop Diagnosis, Submitting Location, Copy to Physician, Path Specimen X, and Path Specm X Instructions
CERNER ORDERS
27
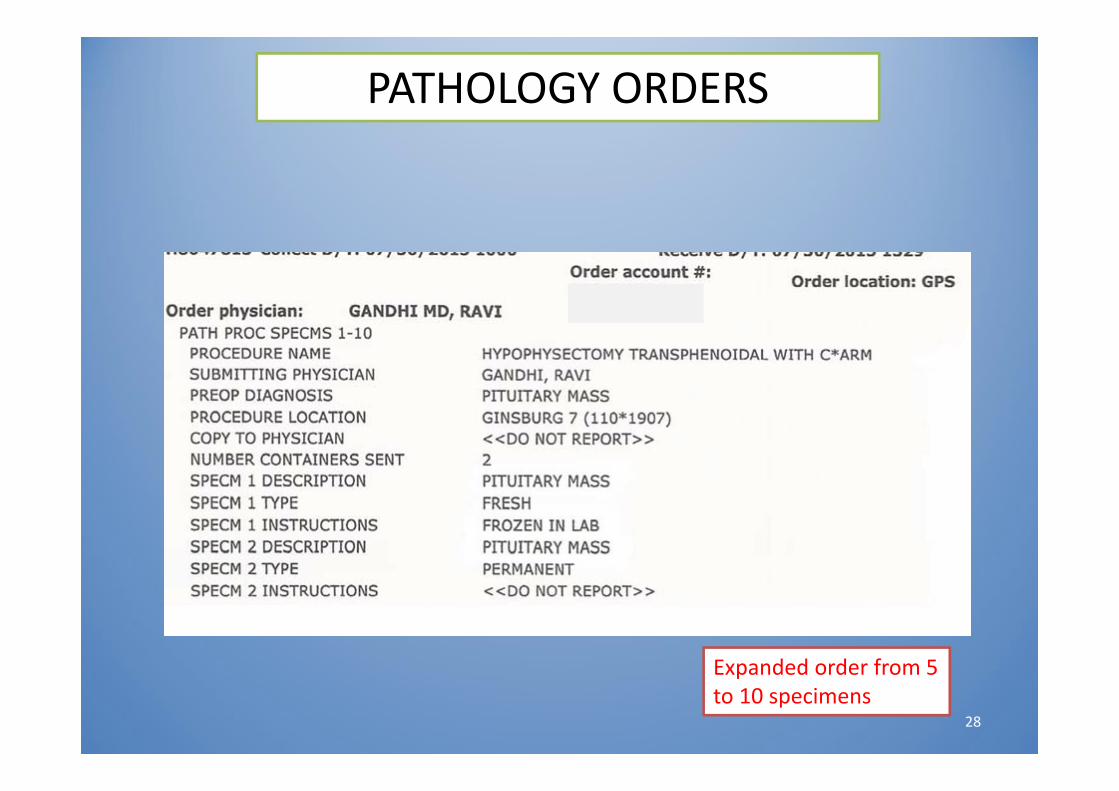
PATHOLOGY ORDERS
Expanded order from 5 to 10 specimens
28

Surgery Careset Orders Container SOURCES
Surgery Microbiology Tissue Orders
SOLID TISSUES
Soft Tissue or Bone Culture with Gram Stain (MCSBT)
Gram Stain Only (GRAMS)
Fungus Culture (MCFU)
Fungus Culture With Smear (MCFUN)
Acid Fast Bacteria with Smear (MCAFB)
Flow Cytometry Non Blood (FLOWNB)
Surgery Microbiology Foreign Body Orders
FOREIGN BODIES, SUCH AS CATH TIPS
Wound Culture Surgical with Gram Stain (MCSURG)
Gram Stain Only (GRAMS)
Fungus Culture (MCFU)
Fungus Culture With Smear (MCFUN)
Acid Fast Bacteria with Smear (MCAFB)
Surgery Microbiology Swab Orders
USE WHEN A TISSUE IS SWABBED; NOT FOR FLUIDS, SOLID TISSUES OR FOREIGN BODIES
Wound Culture Surgical with Gram Stain (MCSURG)
Gram Stain Only (GRAMS)
Fungus Culture (MCFU)
Fungus Culture With Smear (MCFUN)
Acid Fast Bacteria with Smear (MCAFB)
Surgery Microbiology/Lab Fluid Orders
ALL STERILE BODY FLUIDS (Ascites, Pleural, etc.)
Body Fluid Culture with Gram Stain (MCBF)
Gram Stain Only (GRAMS)
Fungus Culture (MCFU)
Fungus Culture With Smear (MCFUN)
Acid Fast Bacteria with Smear (MCAFB)
Glucose Level Fluid (GLUFL)
Protein Fluid (TPFL)
Flow Cytometry Non Blood (FLOWNB)
Surgery Microbiology/Lab CSF Orders
USE FOR CSF ORDERS
CSF Culture with Gram Stain (MCCSF)
Fungus Culture (MCFU)
Fungus Culture With Smear (MCFUN)
Acid Fast Bacteria with Smear (MCAFB)
Cell Count and Differential CSF (CNTCSF)
Glucose Level CSF (GLUCSF)
Protein CSF (TPCSF)
Surgery Microbiology Urine Orders
URINE ORDERSUrine Culture (tie to Suprapubic order please)
Fungus Culture With Smear (MCFUN)
Acid Fast Bacteria with Smear (MCAFB)
SURGERY MICROBIOLOGY ORDERS
30
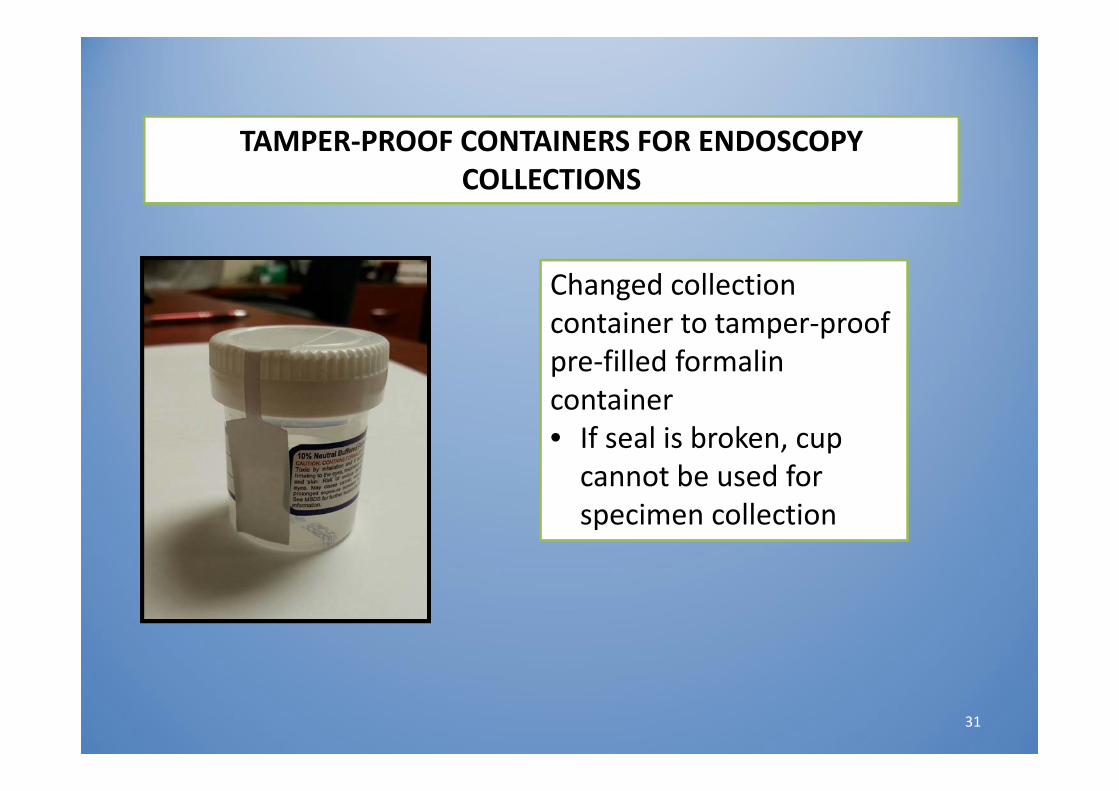
Changed collection container to tamper‐proof pre‐filled formalin container• If seal is broken, cup cannot be used for specimen collection
TAMPER‐PROOF CONTAINERS FOR ENDOSCOPY COLLECTIONS
31
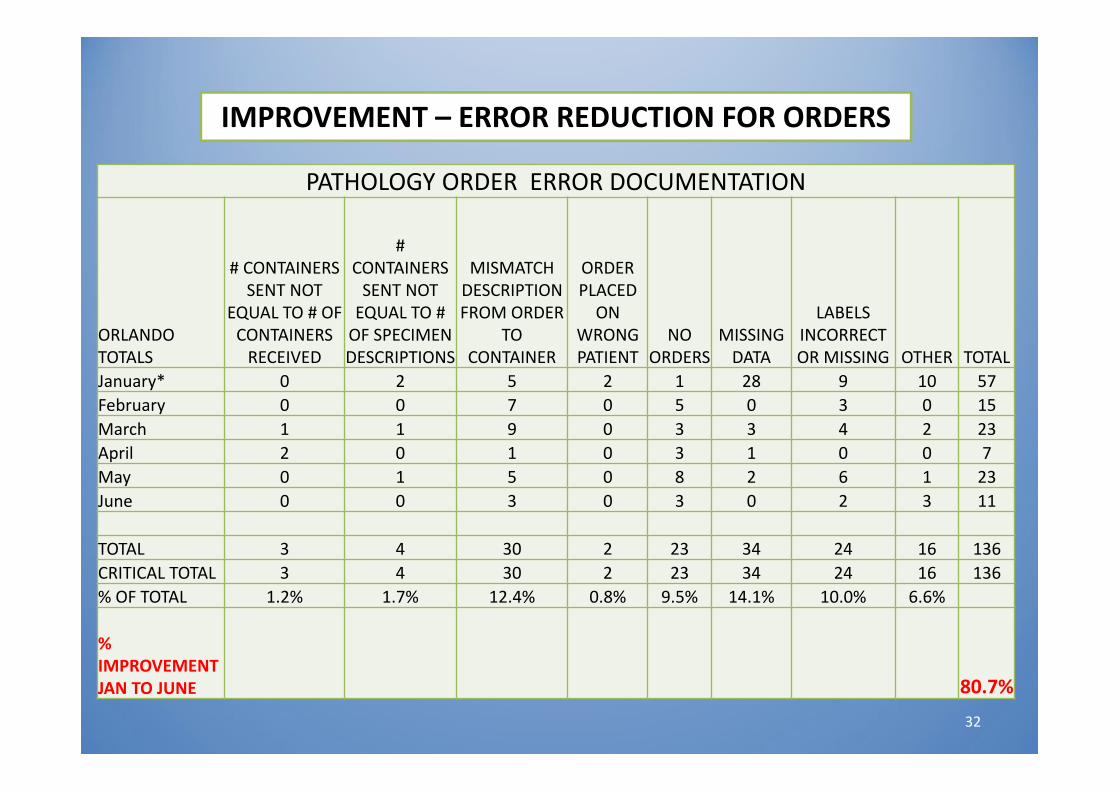
PATHOLOGY ORDER ERROR DOCUMENTATION
ORLANDO TOTALS
# CONTAINERS SENT NOT
EQUAL TO # OF CONTAINERS RECEIVED
# CONTAINERS SENT NOT EQUAL TO # OF SPECIMEN DESCRIPTIONS
MISMATCH DESCRIPTION FROM ORDER
TO CONTAINER
ORDER PLACED ON
WRONG PATIENT
NO ORDERS
MISSING DATA
LABELS INCORRECT OR MISSING OTHER TOTAL
January* 0 2 5 2 1 28 9 10 57February 0 0 7 0 5 0 3 0 15March 1 1 9 0 3 3 4 2 23April 2 0 1 0 3 1 0 0 7May 0 1 5 0 8 2 6 1 23June 0 0 3 0 3 0 2 3 11
TOTAL 3 4 30 2 23 34 24 16 136CRITICAL TOTAL 3 4 30 2 23 34 24 16 136% OF TOTAL 1.2% 1.7% 12.4% 0.8% 9.5% 14.1% 10.0% 6.6%
% IMPROVEMENT JAN TO JUNE 80.7%
IMPROVEMENT – ERROR REDUCTION FOR ORDERS
32

PROPOSED SOLUTIONSCampus Lab and Transportation to
Pathology• Insourced the couriers to be owned by the hospital • Eliminate variability• Path Lab Assistants for specimen Pickup
Own the Couriers
• Real time monitoring at campus lab & Pathology using electronic Pathology orders
• Electronic pending logOL Monitor
• Standardize totes• Add RFID tags to all totes• Add Tote tracking in Sunquest batches
Tote Tracking
33

Florida hospital “in‐sourced” couriers by adding a courier services department in Materials Management.Advantages: Florida hospital employeesAbility to share routes with pharmacy and other departments
Standardized methods for transport
OWN THE COURIERS
34

Alicia & KB, a vital part of the Path/Lab specimen pickup process at Orlando
Why pick up Pathology specimens from throughout the hospital?
Benefits: Ensures proper hand‐off
from procedural area to Lab Level‐loads incoming
specimens from collection to delivery
Allows “point‐of‐service troubleshooting” and develops good practices
Extends “goodwill” between departments and eliminates “silo’s”
Costs: FTEs for coverage
35
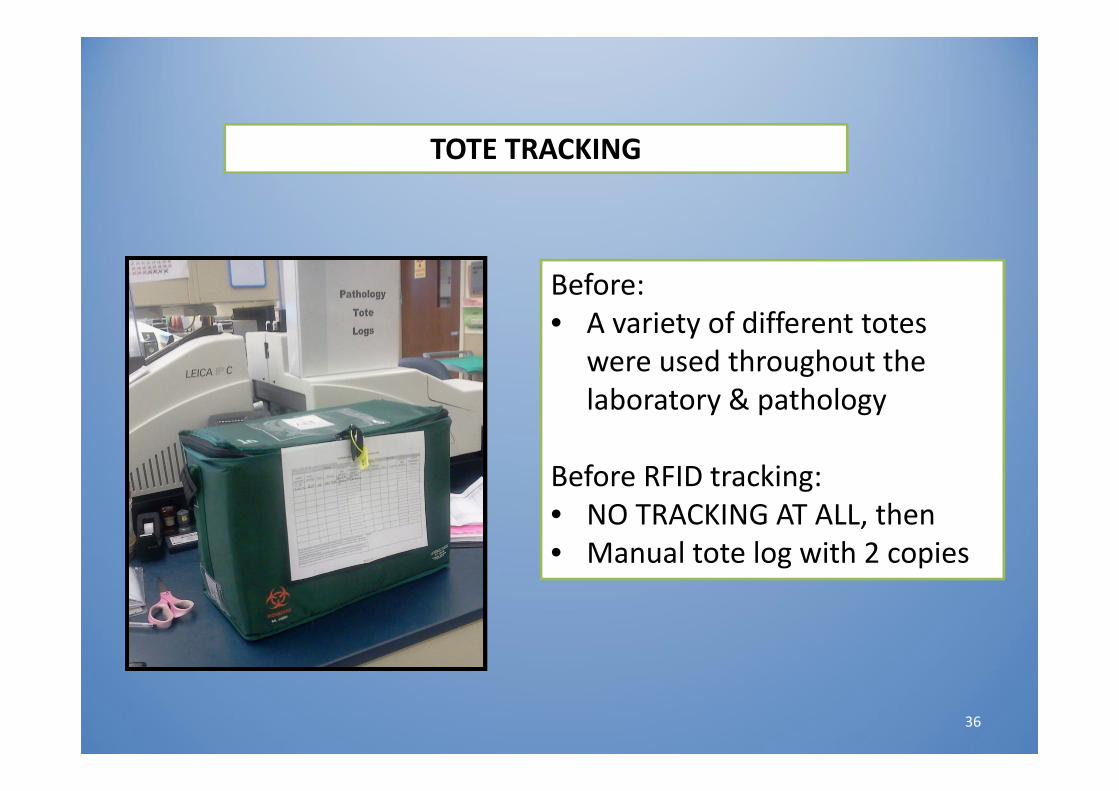
Before:• A variety of different totes
were used throughout the laboratory & pathology
Before RFID tracking:• NO TRACKING AT ALL, then• Manual tote log with 2 copies
TOTE TRACKING
36

Green Pathology tote with RFID tag attached. Staff creates “batch” in Sunquest
Scans the RFID barcode tag in Batch comments during Batch formation
This ties the specimen to the batch, the batch to the tote
RFID tag sends alert if tote out of system >4 hours
Future: add Gajema/Cerner Outreach to tie tote to courier
37
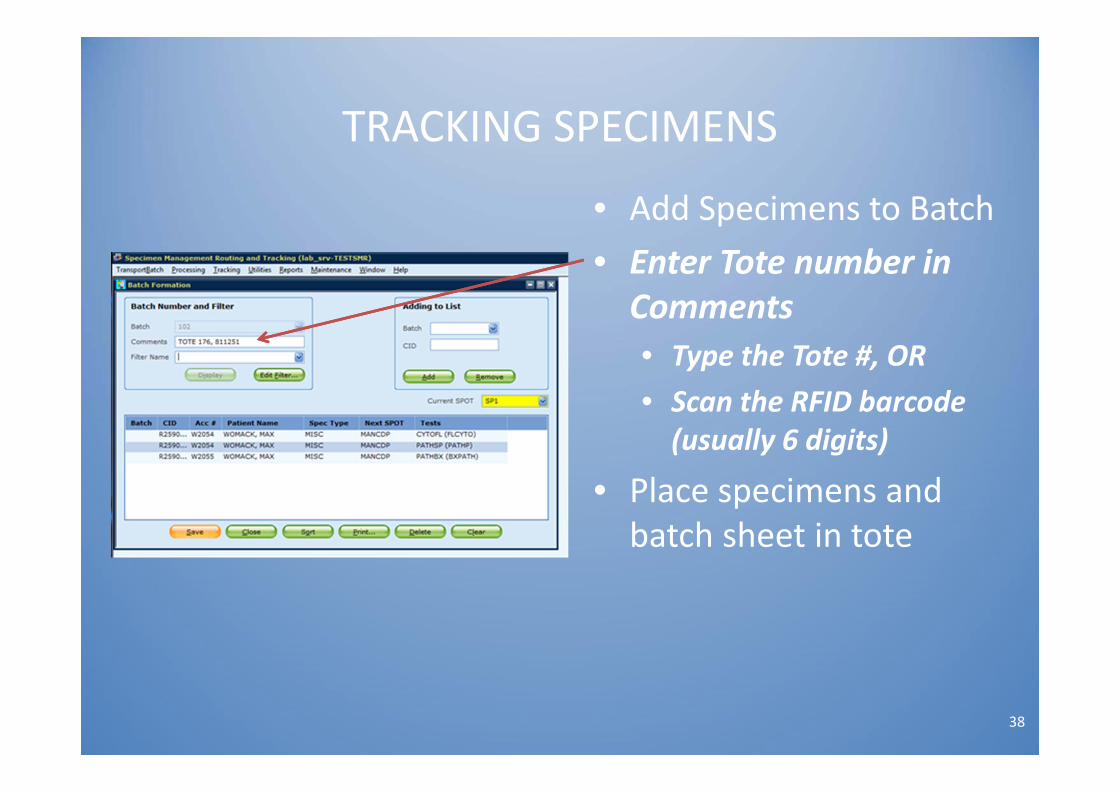
TRACKING SPECIMENS
38
• Add Specimens to Batch• Enter Tote number in Comments• Type the Tote #, OR• Scan the RFID barcode (usually 6 digits)
• Place specimens and batch sheet in tote

OL MONITOR
39
• The OL Monitor is an overdue log of pending tests.• Priority colors have been set up as follows:
» Red = > 120 minutes» Black = < 120 minutes
• Once TEST is received in Sunquest it will be removed from the OL Monitor display.
• PULL specimens • Improve TAT from collect
to receive in lab

40
OL MONITOR DISPLAY – ELECTRONIC PENDING LOG
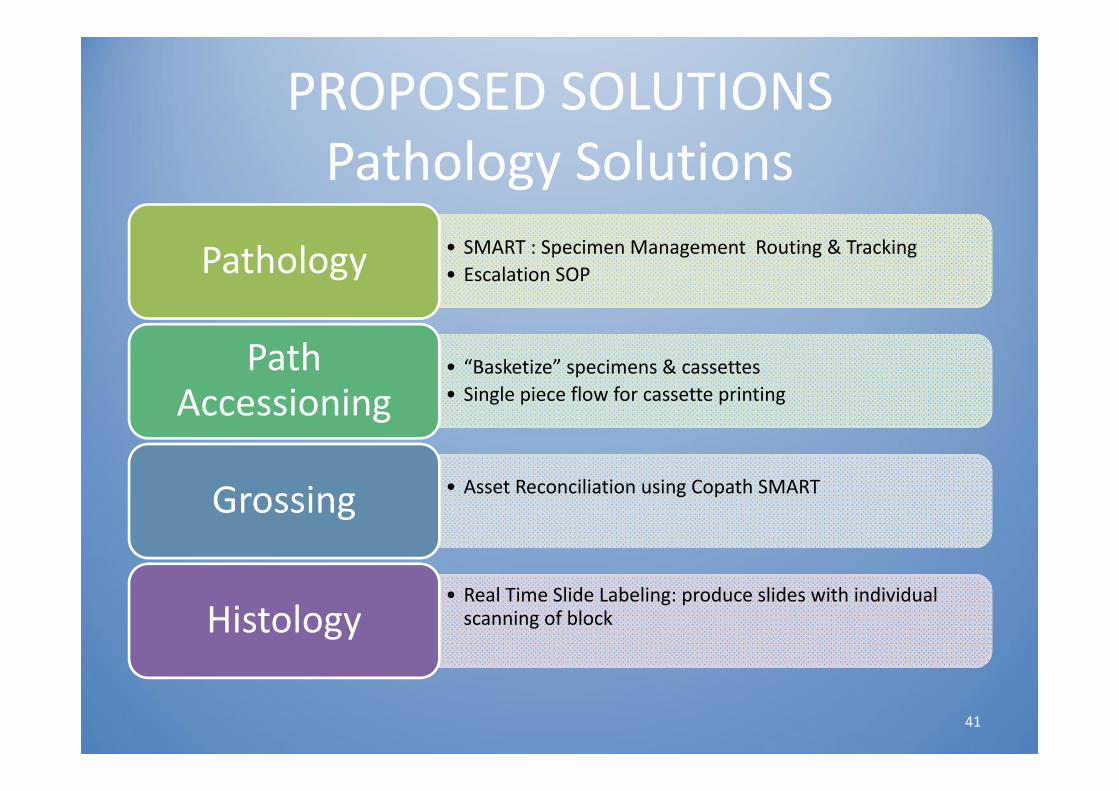
PROPOSED SOLUTIONSPathology Solutions
• SMART : Specimen Management Routing & Tracking• Escalation SOPPathology
• “Basketize” specimens & cassettes• Single piece flow for cassette printing
Path Accessioning
• Asset Reconciliation using Copath SMARTGrossing
• Real Time Slide Labeling: produce slides with individual scanning of blockHistology
41

• Allows tracking of containers, requisitions, cassettes and slides within the laboratories with 2D barcodes– Eliminates hand‐written cassettes and slides
• Creates audit trail of each “asset” (block/slide) with location & tech
• Allows timely follow up of delayed assets• Real Time Slide Labeling forces single piece flow for printing of slides from each block
• “Rule Building” through Advanced Protocols & Asset Manager
SMART ‐ Sunquest(Specimen Management Routing & Tracking)
42

Pathology Accessioning Process 1 Lab Assistant works with 1 tote at
a time Removes specimen and paper print
out from biohazard bag in tote Compares for accuracy Receives in Sunquest Creates case in Copath Prints cassettes to “local” cassette
printer (single piece flow) “Basketizes” specimens/paper &
cassettes Places baskets on cart to move to
gross room
43

GROSSING – ASSET RECONCILIATION• VERIFIES CASSETTES MATCH CONTAINER/CASE IN COPATH
44
Note: example from Copath User Guide

Histology Single Piece Flow Histotech scans block Copath prints slides programmed to
that block Eliminates slide/block mismatches
Real time slide labeling• Prevents block/slide mismatch• Creates single piece flow
45
EXAMPLES: Empty container if specimen is not easily recollected Misidentified samples discovered after results have been reported
Lost/Missing sample –if specimen is not easily recollected Erroneous results reported, such as Corrected pathology
diagnosis • Extreme delay in testing/results
Immediate notification and escalation to Administration is required for any laboratory error or event considered to be an Adverse EventStandardized the escalation process
LABORATORY ESCALATION PROCESS
46

Resource $ Amount $ Actual Spend
Capital IT Capital
FTE (s)
Laptops (18) Specimen Handoff $50,000 X
OL Monitor ( software for Toughbook)
$ 5,000 X
OL Monitor screens, hardware and software
$15,000 X
Aeroscout and Gajema Specimen and Tote Tracking system
$68,000 X
1.5 FTE’s Central Accessioning $50,000 X
Cassette Printers (3) in CDP $105,000 X
LIS interface ( Printers in CDP) $22,500 X
Operating Actual Costs $61,542
Capital Actual Costs $166,085
Total Resource *does not include FTEs
$265,500$215,500*
$227,627* 1.5FTE
*over $12,127, unexpected expense for Cassette printer licenses
PROJECT COSTS
47

SPECIMEN PATHOLOGY SCORECARD
48
Key Performance Indicators ‐ OrlandoGoal 2015 JULY AUG SEPT
Process Measures:
Collection Time to Arrival in Campus Lab < 3 hours 3 3 2.6
Arrival Campus Lab to Arrival in CDP < 6 hours 2 3.4 3.2
Collection Time to Arrival in CDP < 8 hours 6 6.3 5.7
Tote escalations to administration Zero 0 0 0
Outcome Measures:
Internal CDP mislabeling errors Zero 0 1 0
Specimen Discrepancy (Total) ‐ Non‐Lab Zero 25 21 24
Specimen Escalations to System Administration Zero 5 0 2
IDEAL STATE
• Procedural areas:– Bedside positive patient ID– Place 1 order that flows to all systems– With all required information– And produces 1 barcode label per specimen that can be tracked from point of collection to final result
49

BARRIERS TO IDEAL STATE
• Positive Patient Identification not a “hard stop” in procedural areas
• Cerner/Copath/Sunquest not truly integrated– Orders entered in Cerner and flows to Sunquest in discrete data fields
– Order is ‘rebuilt’ in Copath because Copath does not accept “discrete” data
– Too many barcode labels per specimen:• Chart label, Sunquest tracking label for each case, container label from Copath SMART
50

NEXT STEPS• Reduce specimen/order mismatch
– Hard stop by procedural areas– Reduce delays in obtaining corrections
• Improve TAT from collect to campus lab & campus lab to CDP– Optimize OL Monitor & TAT data– Review the courier schedule to minimize delays– Level load workload in Pathology
• Seek opportunity for true single piece flow from point of collection through final result
51
Conclusions ‐ Pluses• Electronic orders from procedural areas have standardized
ordering and reduced clerical errors; this has created specimen accountability (80% improvement)
• Implementation of OL monitor has prevented delays &/or missing samples
• Standardization of transportation: no lost totes• Implemented single piece flow for cassette printing• Established TAT metrics• Improved SAFETY!!• Developed trusted relationships between Surgery,
Endoscopy and Laboratory
52

Conclusions ‐ Deltas
• Inconsistent Hard Stop for Specimen ID in Procedural Areas
• Continued revisions and additions for electronic orders has created confusion
• Staff at CDP Path Accessioning – 1.5 open positions and less experienced
• Limited integration of multiple IT systems for true tracking from collect to receive– Tracking ideal is 1 barcode label per specimen to one order, from collection of specimen to final receipt
53

Learnings
• To Do:• Get feedback from front line staff
before developing any IT solutions
• Dedicate a team and assign a Project Manager to keep the momentum
• Always use your best and brightest when solving complex problems
• Not to Do:• Sweat over a few $$s when the
risk is too great!• Wait for the 3rd project to finally
fix what you knew was wrong all along
• Accept less than perfection when labeling of specimens
54

Thank You’s!• Arlene Herrin, VP of Ancillary Services, for always having the
lab’s “back”• Susana Savino, System Lab Admin Director, for supporting all
of the changes• Jeanette Bartos, System Surgery Director, for collaborating
with electronic orders• Barb Serra, Asst. Director‐Pathology, for providing all of the
“human help”• Aneet Panesar, QA Coordinator‐Pathology for helping with the
data and observations• Pathology team: Martha Hustek, Mike Sheehan, Carol Waddell
& many others!• Lynne Evans‐Williams, MIS Project Manager, deployed all of
the hardware for this project• Debra Walters, Sue Arcuri and Maxine Brown, LIS Specialists 55