
WHO:s arbete med antibiotikaresistens -vad händer? · 2011: Världshälsodagen . 6-punkts...
30
WHO:s arbete med antibiotikaresistens -vad händer?
Transcript of WHO:s arbete med antibiotikaresistens -vad händer? · 2011: Världshälsodagen . 6-punkts...

WHO:s arbete med antibiotikaresistens -vad händer?

Orphanage in Bamako, Mali ESBL colonized 100% of the children and 63%, of the adult staff studied. Tandé et al. Emerg Infect Dis. 2009 Mar;15(3):472-4.
Mumhibili hospital, Tanzania Tanzania The mortality rate from Gram-negative bloodstream infection was 43 %, more than double that of malaria.. Blomberg et al. BMC Infect Dis. 2007 May 22;7:43.
Källa: Otto Cars
”Vi blickar ut i världen”

One child is dying every five minutes because the antibiotic given is ineffective Neonatal sepsis in five countries in South Asia (India, Pakistan, Afganistan, Nepal, Bangladesh),
Zulfiqar Bhutta ReAct conference,2010 http://www.reactgroup.org/resource-centre/react-presentations/the-global-need-for-effective-antibiotics.html
Källa: Otto Cars

Sjukdomsspecifika program som behandlar resistens
Tuberkulos (2006)
Artemisinin- resistent Malaria (2011)
N. Gonorrhoea (2012)
Anti-HIV resistens (2012)
Saknas ett samlat program som tar upp resistens i “vanliga” bakterier.
2011: Världshälsodagen
6-punkts “policy package“ Ett upprop till medlemsländerna att agera
Finansierad multisektoriell nationell plan, brett samhällsengagemang
Förstärka “surveillance” och lab-kapacitet
Tillgång till nödvändiga mediciner av säker kvalitet
Rationell läkemedelsanvändning
Vårdhygien och prevention
Stimulera FoU avseende nya mediciner och andra verktyg
Presentatör
Presentationsanteckningar
WHO is aware of these challenges and is addressing them, also through strategies for combating antimicrobial resistance. The policy package launched in April 2011 highlights the essential elements of a multifaceted approach to combat AMR.

AMR surveillance roadmap: • WHO Global AMR Rapport • Behov av harmonisering • Samarbete mellan nätverk
Dec 2012
1st “Tekniska konsultationen” om global resistensövervakning

Presentatör
Presentationsanteckningar
Thank you so much for your interest and for joining us in this discussion on WHOs first global report on antimicrobial resistance, which this time has a focus on surveillance The report is based on recommendations from the first WHO technical consultation on ”Strategies for Global Surveillance of Antimicrobial Resistance” that was held in 2012, as a follow up to the world health day 2011. The consultation stressed the urgent need for data on the present situation and burden of antimicrobial resistance, particularly for bacteria causing common infections, which is where the major knowledge gaps are. http://www.who.int/drugresistance/publications/surveillance-meeting2012/en/ /

• Fokus på antibakteriell resistens (ABR) • Sammanfattningar av
• sjukdomsspecifika program: Tb, Malaria, HIV • djur/ livsmedel • candidiasis
Beskrivning av ABR surveillance i olika WHO regionerna
Nationella eller publicerade
resistensdata för 7 bakterier
(9 kombinationer)
Systematiska granskningar av
evidens för sjukdoms-och ekonomisk börda
för 5 bakterier/
resistenskombinationer
Kunskapsluckor
Antimicrobial Resistance Global Report on Surveillance 2014

Insamling av resistensdata
Officiella nationella data
Nationella och internationella
nätverk
Publikationer efter
2008
När inga data inkom

*National data means data obtained from official sources, but not that data necessarily are representative for the population or country as a whole
Tillgängliga nationella resistensdata 2013 Nio “bug/drug” kombinationer
WHO: Antimicrobial Resistance. Global report on surveillance 2014
Presentatör
Presentationsanteckningar
This map shows an overview of the responses regarding resistance data from the Member States: 129 countries responded of which 114 returned at least some data on at least one of the 9 requested bacteria–antibacterial drug combinations Long-standing international collaboration probably contributed to the high coverage in the Americas and the EU. Many responding countries had difficulties to provide data based on testing of at least 30 of isolates.
Name of bacterium/ resistance
Examples of typical diseases
No. of 194 MS providing
national data
No. of WHO regions with national reports of 50 %
resistance or more
Range of reported proportion of
resistance
Escherichia coli Urinary tract infections, blood stream infections
-vs 3rd gen. cephalosporins 84 5/6 0-82
-vs fluoroquinolones 90 5/6 3-96
Klebsiella pneumoniae
Pneumonia, blood stream infections, urinary tract infections
-vs 3rd gen. cephalosporins 85 6/6 2-82
-vs carbapenems 69 2/6 0-68
Staphylococcus aureus Wound infections, blood stream infections
-vs methicillin “MRSA” 83 5/6 0.3-90
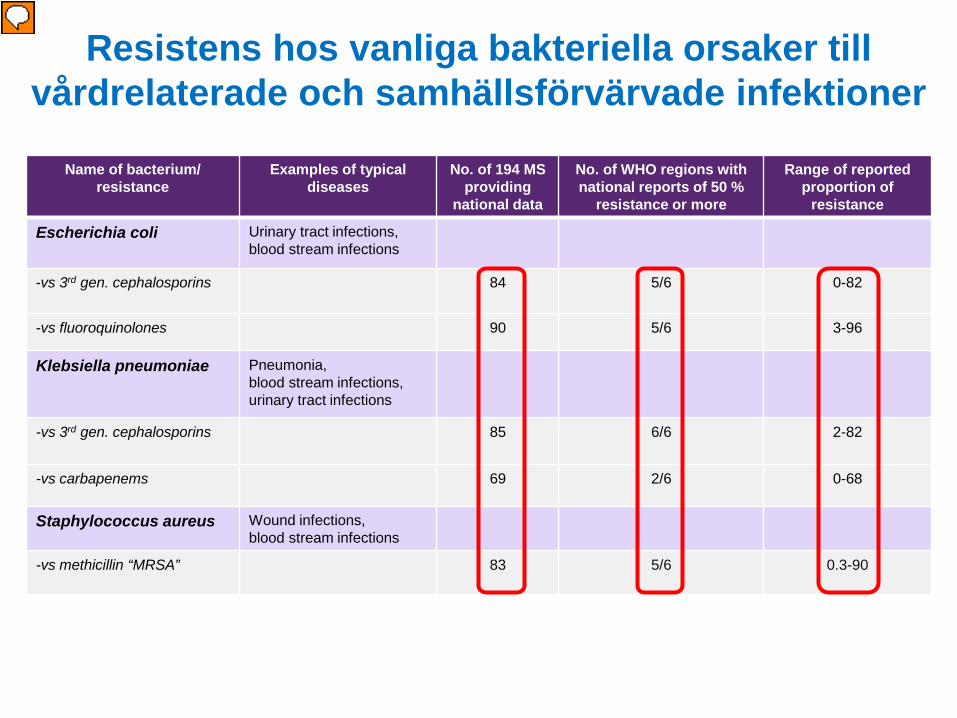
Resistens hos vanliga bakteriella orsaker till vårdrelaterade och samhällsförvärvade infektioner
Presentatör
Presentationsanteckningar
The next 2 slides give an overview of the key findings: Escherichia coli, Klebsiella pneumoniae and Staphylococcus aureus are all major causes of both community and hospital acquired infections. Infections they cause range from life-threatening blood-stream infections, to self-limiting infections of the urinary bladder or superficial wound infections. It can be seen that less than half of countries reported data on at least 30 isolates. resistance proportions exceeding 50 % were reported from at least 5/6 WHO regions for all but one �combination, It can also be seen that there is a wide variety in the proportion of resistance reported, from 0 to �more than 80% for most of the combinations In E. coli and Klebsiella pneumoniae, which are both Gram-negative bacteria normally colonizing the intestine, �high levels of resistance to 3rd generation cephalosporins, (which has been reported from most parts of the world), means that one of the most important groups of antibiotics for intravenous treatment of severe infections, typically in hospitalized patients, is lost. High resistance to fluoroquionolones in E. coli, also reported from most parts of the world, means that an important medicine for oral treatment of urinary infections and infections of the kidney is lost. Carbapenems are the most commonly available last resort for treatment of Gram-negative infections resistant to �cephalosporins. Carbapenem resistance in K. pneumoniae was discovered in the early 2000:s and has already �spread to all parts of the world; countries in 2/6 WHO regions even report resistance > 50%. This means that there are usually no treatment options left for this important cause of hospital acquired infections, typically seen in iinfections in ntensive care units and in neonates. Staphylococcus aureus is a common colonizer of the skin. MRSA was initially a major concern in hospital-�acquired infections, but is now also of growing concern in the community. High resistance to methicillin means that use of more expensive and toxic second line drugs are needed for treatment. It also means that standard prophylaxis to prevent infections in orthopaedic and other types of surgery will be �ineffective

Name of bacterium/ resistance
Examples of typical diseases
No. of 194 MS providing national data
No. of WHO regions with national reports of 25 % resistance or more
Range of reported proportion of
resistance
Streptococcus pneumoniae
Pneumonia, meningitis, otitis
-non-susceptible to penicillin
66 6/6 0-73
Nontyphoidal Salmonella Foodborne diarrhoea, blood stream infections
-vs fluoroquinolones 66 3/6 0-96
Shigella species Diarrhoea (“bacillary dysenteria”)
- vs fluoroquinolones 34 2/6 0-47
Neisseria gonorrhoeae Gonorrhoea
-vs 3rd gen. cephalosporins 42 3/6 0-36
Resistens hos vanliga bakteriella orsaker främst till samhällsförvärvade infektioner
Presentatör
Presentationsanteckningar
Here are examples of bacteria predominantly causing infections that are common in the community: S. Pneumoniae is the leading cause worldwide of community-acquired pneumonia, an important cause of morbidity and mortality, particularly among children and elderly people Nontyphoidal Salmonella and Shigella are two of the most important diarrhoeal pathogens, also �causing major morbidity and mortality, particularly in children. N. gonorrhoeae is the bacterium that causes gonorrhoea. Again it can be seen that: less than half of countries reported data on at least 30 isolates. resistance proportions exceeding 25 % have been reported from most parts of the world for several of �these combinations, there is a wide variety in the proportion of resistance reported for most of the combinations The implications of these findings are that Reduced susceptibility to penicillin in S. pneumoniae, which is reported from all parts of the world, means that oral penicillin treatment may be ineffective for treatment of pneumonia although most diarrheal infections caused by Salmonella are self-limited and do not benefit from �antibiotic treatment, severe infections and cases with concomitant blood-stream infections should be treated, and resistance to fluoroquionolones, means that an important treatment option is lost.�The same is true for Shigella, for which antibiotic treatment has a more prominent place Gonorrhoea, if untreated or inappropriately treated, can result in infertility. �Infection in pregnant women can result in infections in the newborn, including eye infections that �may lead to blindness. �Because of widespread resistance, older and cheaper antibacterial medicines are no longer effective �intreatment of gonorrhoea and 3rd generation cephalosporins are the last resort for treatment.
Deaths (%)
Outcome (number of studies included) Resistant Not resistant RR (95% CI)
Escherichia coli resistant to:
3rd gen. cephalosporins Bacterium attributable mortality (n=4) 23.6 12.6 2.02 (1.41 to 2.90)
Fluoroquinolones Bacterium attributable mortality (n=1) 0 0
Klebsiella pneumoniae resistant to:
3rd gen. cephalosporins Bacterium attributable mortality (n=4) 20 10.1 1.93 (1.13 to 3.31)
Carbapenems Bacterium attributable mortality (n=1) 27 13.6 1.98 (0.61 to 6.43)
Staphylococcus aureus resistant to:
Methicillin (MRSA) Bacterium attributable mortality (n=46) 26.3 16.9 1.64 (1.43 to 1.87)
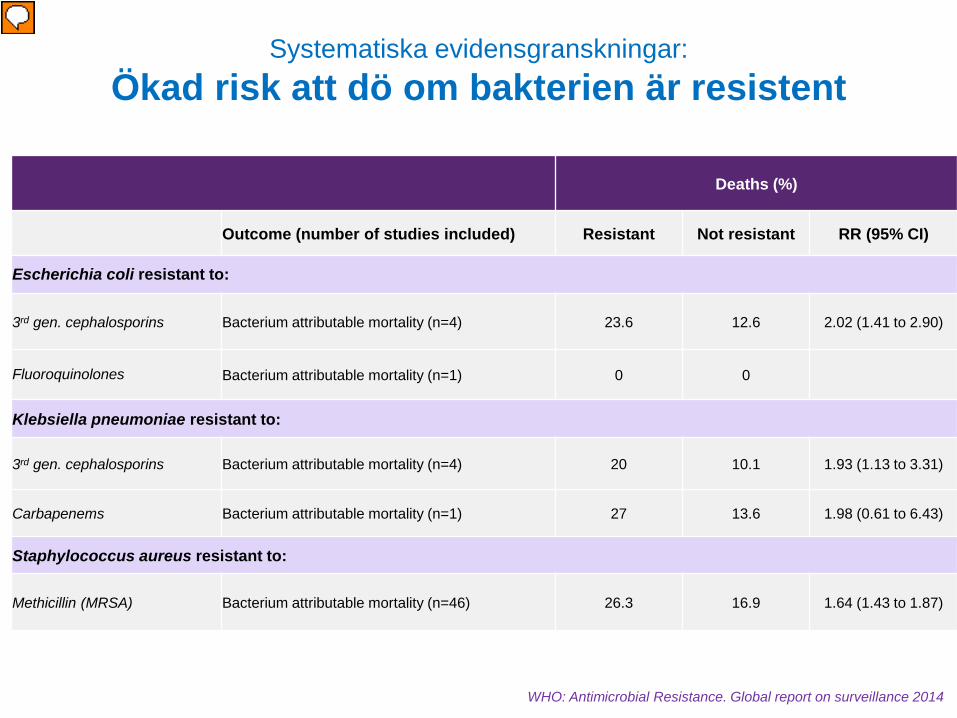
Systematiska evidensgranskningar: Ökad risk att dö om bakterien är resistent
WHO: Antimicrobial Resistance. Global report on surveillance 2014
Presentatör
Presentationsanteckningar
5 combinations of bacteria/ antibacterial resistance were reviewed �separately; This slide shows that there was a statistically significant increased risk for patients infected with a resistant strain to die from the infection in all but two combinations where there was not enough data. The additional risk to die was about 2-fold for infections with the �resistant Gram-negative bacteria, and more than 50% higher for MRSA �infections. For infections caused by E. coli resistant to fluoroquionolones, �Klebsiella pneumoniae resistant to 3rd generation cephalosporins and �Staphylococcus aureus resistant to methicillin, there was also an increased risk for progresstion to septic chock and/or �admission to intensive care unit, both of which will cause increased �health care expenditures

Antibacterial resistance Studies included in SR (n)
Studies reporting cost data (n)
Excess cost (n = studies reporting costs)
Hospitalization Antibacterial therapy Medical care Additional cost
variables
Escherichia coli resistant to:
3rd gen. cephalosporins 25 2 Yes (n=2) Yes (n=1) Yes (n=1) Yes (n=1)
Fluoroquinolones 12 0 - - - -
Klebsiella pneumoniae resistant to:
3rd gen. cephalosporins 24 0 - - - -
Carbapenems 13 0 - - - -
Staphylococcus aureus resistant to:
Methicillin 147 19 - Yes (n=6) Yes (n=6) Yes (n=9)
WHO: Antimicrobial Resistance. Global report on surveillance 2014
Systematiska evidensgranskningar: Ökad kostnad om bakterien är resistent
Presentatör
Presentationsanteckningar
This slide summarizes findings from studies designed to address potential excess in health-care costs. Only a few studies were available for E. coli resistant to 3rd generation �cephalosporins and methicillin resistant S. aureus. Still, excess costs, measured as costs for hospitalization, antibacterial therapy, medical care or other additional cost variables were higher for �infections caused by resistant strains. For instance, for E. coli, hospital costs were about 1.6-3 times higher in �infections caused by strains resistant, as opposed to sensitive, to 3rd �generation cephalosporins

1. Höga resistensiffror rapporterades i alla WHO-regioner bland vanliga bakterier som orsakar såväl vårdrdrelaterade som samhällsförvärvade infektioner
2. Resistens påverkar patienter och sjukvårdskostnader negativt
3. Behandlingsalternativen för vanliga infektioner håller på att ta slut
4. Trots begränsningar visar rapporten på storleksordningen på problemet samt kunskapsluckor
Sammanfattning I: Antibakteriell resistens

1. Kunskapsluckor störst där sjukvårdssystemen är svagast
2. Det finns ingen harmonisering av metodologi (standards ej implementerade): • Vilka prover/ vilken information som ska samlas in • Hur labtestning o resistensbestämning ska utföras • Hur data ska sammanställas och delas
3. Data vanligen som en procentsiffra per “bug/drug” utan koppling till patientinformation
4. Rapporten är en base-line för att följa förbättring av surveillance
Sammanfattning II: Övervakning av Antibakteriell resistens

Förebyggande åtgärder och vårdhygien
Världshälsoförsamlingen

Många frågor/ kritik
“STAG”-strategisk rådgivande grupp
2013
Presentatör
Presentationsanteckningar
The World Health Assembly at its 67th session adopted resolution WHA67.25 on combating antimicrobial resistance. Through this resolution, the Health Assembly has requested that the Director-General develops a draft global action plan to combat antimicrobial resistance, including antibiotic resistance, and submits a draft of that plan to the Sixty-eighth World Health Assembly in 2015. WHO will lead the development of a draft global action plan that reflects the commitment, perspectives and roles of all relevant stakeholders, and in which everyone has clear and shared ownership and responsibilities. The Health Assembly, through the resolution, has specifically requested that WHO consult Member States as well as other relevant stakeholders, especially other multilateral stakeholders such as FAO and OIE, in developing the global action plan. Such consultation is a major component of the work plan for the next 12 months.

2014
Resolution 67.25
Presentatör
Presentationsanteckningar
The World Health Assembly at its 67th session adopted resolution WHA67.25 on combating antimicrobial resistance. Through this resolution, the Health Assembly has requested that the Director-General develops a draft global action plan to combat antimicrobial resistance, including antibiotic resistance, and submits a draft of that plan to the Sixty-eighth World Health Assembly in 2015. WHO will lead the development of a draft global action plan that reflects the commitment, perspectives and roles of all relevant stakeholders, and in which everyone has clear and shared ownership and responsibilities. The Health Assembly, through the resolution, has specifically requested that WHO consult Member States as well as other relevant stakeholders, especially other multilateral stakeholders such as FAO and OIE, in developing the global action plan. Such consultation is a major component of the work plan for the next 12 months.

Förslaget till Global Action Plan “GAP”
5 vägledande principer – Hela samhället (alla sektorer) engageras – Förebygg först – “Access, not excess” – Varaktighet – Stegvis implementering, delmål
Presentatör
Presentationsanteckningar
The action plan is based on six guiding principles: Whole of society engagement. Antimicrobial resistance will affect every individual, regardless of their health or economic circumstances, lifestyles or behaviours. It will also have an impact on many sectors beyond health including food security, agriculture and animal health, development including economic development. Everyone therefore needs to be engaged in the implementation of this action plan on a personal or professional basis. Actions need to be based on best available knowledge and evidence. With scarce resources and many competing health and economic priorities, is essential that the actions and investment needed to address antimicrobial resistance are supported wherever possible by clear and compelling evidence or rationale for their benefit and cost-effectiveness. Difficult or costly actions are also too easily avoided or challenged without such evidence. However, the need for action now is clear and must not be delayed because of gaps in scientific evidence or knowledge. Prevention first. Preventing infection (without use of antimicrobial medicines) has multiple benefits. Every infection prevented is one that does not need treatment whether appropriately or inappropriately, and is also not a source of further infections. Many interventions and practices for the prevention of infection are cost effective and can be implemented in all resource settings and sectors. Access not excess. The overall goal is to preserve our ability to treat serious infections. In some contexts preserving the effectiveness of antimicrobial medicines means using less. In other settings, poor access to affordable quality assured medicines is currently compromising health outcomes. Actions to address antimicrobial resistance need to take into account the need to maintain equitable access to and appropriate use of existing and new antimicrobial medicines. Sustainability. Addressing antimicrobial resistance will require long term change and investment, and new practices may need to be maintained indefinitely. Actions are more likely to be sustainable where they are integral to health systems or practices in other sectors, and where there is evidence of continuing health and economic benefit. Incremental targets for implementation. All countries and other stakeholders need to be able to demonstrate progress towards implementation of the global action plan, whatever their current status. A step-wise approach to targets and performance indicators for implementation of the plan, based on a series of “building-blocks” will allow for different priorities and capacities among Member States and other stakeholders.

Fem strategiska målområden
Samordning & Tvärsektoriellt engagemanng
Stärka kunskaps-
läget
Optimera användninga
av antimikrobiella
läkemedel
Prevention
Utveckla “economic case” för uthållig
finansiering
Förbättra medvetenhet
och förståelse
Följa upp framsteg

Förankringsprocess
http://www.who.int/drugresistance/amr_global_action_plan/en/
Email till [email protected] Ämne: ‘SUBSCRIBE TO MAILING LIST’
Presentatör
Presentationsanteckningar
The Strategic and Technical Advisory Group (STAG) on antimicrobial resistance has been convened to advise the Director-General on the main areas of concern, priorities for action, and medium- to long-term objectives for inclusion in the draft global action plan. WHO will continue to work with its Strategic and Technical Advisory Group on Antimicrobial Resistance, to engage with a wide range of organizations and experts in order to set out the scientific and policy issues, develop proposals for targets and indicators, and review the draft action plan prior to its submission to the governing bodies in 2015. The next meeting is being planned for 16 to 17 October 2014, and a further meeting prior to the Health Assembly in 2015. http://www.who.int/drugresistance/stag/en/ June 2014: http://www.who.int/drugresistance/netherlands_meeting_june_2014/en/

WHO styrelsemöte Januari 2015
• Starkt stöd att gå vidare till WHA • 39 country statements, plus 5 NGOs
• Några önskemål om ändringar/ förtydliganden • WHO FAO OIE tripartite möte10 Feb 2015 • WHO Advisory Group “STAG” mote 24-25 Feb 2015

Möten för att understödja GAP
Juni 2014: Holland; – AMR och livsmedelsproduktion, “One Health”
Nov 2014 Norge; – Rationell användning
Dec 2014 Sverige; – Resistensövervakning inom humanmedicin
Presentatör
Presentationsanteckningar


“Outcome statement” http://www.folkhalsomyndigheten.se/documents/projektwebbar/s
ar/outcome-statement-amr-surveillance-final.pdf
“In order to improve surveillance of AMR, in alignment with resolution WHA67.25, we agree to work together with WHO to establish global surveillance for AMR, that includes:
making surveillance of AMR a national and global priority and
supporting the development of a global programme for surveillance of AMR in human health
in accordance with the WHO road map, starting with an early implementation phase of agreed standards and principles for collaboration.”


Tack!


















