
WHO guideline development for CCHF clinical management and ... · WHO guideline development for...
53
WHO guideline development for CCHF clinical management and the WHO R&D roadmap for CCHF and other actual aspects Natalia Pshenichnaya, MD, DSC., Prof. Head of Infectious Diseases Department at the Postgraduate Faculty of Physicians, Rostov State Medical University, Rostov-on-Don, Russia; Taskforce member of CCHF WHO R&D Blueprint roadmap; Member of WHO CCHF clinical management guideline development group ESCMID workshop, Bucharest, 23 March
Transcript of WHO guideline development for CCHF clinical management and ... · WHO guideline development for...

WHO guideline development for CCHF clinical management and the WHO R&D roadmap for
CCHF and other actual aspects
Natalia Pshenichnaya, MD, DSC., Prof.Head of Infectious Diseases Department at the Postgraduate Faculty of Physicians, Rostov State Medical University, Rostov-on-Don, Russia;
Taskforce member of CCHF WHO R&D Blueprint roadmap; Member of WHO CCHF clinical management guideline development group
ESCMID workshop, Bucharest, 23 March

Greece (2008)
Georgia (2009)
India (2011)
Spain (2016)
Country at risk (serological evidence + vector)
Country with low risk (presence of vector)
50 to 200 cases per year
5 to 49 cases per year
Crimean-Congo Haemorrhagic Fever Geographic Distribution
50° North limit for the geographic distribution of genus Hyalomma ticks
Pierre Formenty, et al. In Ergonul & Whitehouse, CCHF, Springer, 2007; modified
Countries where within last 10 years first case of CCHF in human was detected

Karesh WB, Lancet 2012

The Course of Infection in animals
Mild clinical symptoms
Described by Shepherd et al in 1980s.
No striking notes in recent outbreaks, since 2000
Viremia
Lasts for 7-10 days in mammals
Onder Ergonul, Berlin, Germany, 2016

CCHF case fatality rate in different countries
Keshtkar-Jahromi M et al. Antiviral Research 2013;100(1):20-8Shaikh MA et al. J Pak Med Assoc 2015;65(5):576
Nurmakhanov T, et al. IJID 2015;38:19-23Volynkina AS et al. Plague 2015: no.1
Leblebicioglu H et al. Antiviral Research 2016;126:21-34
CFR ≈ 4% - 36%
[2002-2015]
2124 cases
CFR: 4,0%
[1999-2017]

CCHF case definitionPROBLEMS:
1.There is no any standardized case definition for all countries, each country use own case
definition. This circumstance don’t allow to compare studies in different countries;
2. Cases can be missed (mild cases, cases without haemorrhagic symptoms)As example – CCHF case definition in Russia (very close to case definition in Greece and Pakistan)
Suspected case• Acute onset of illnesses with high fever (>38.0°C)• Spring-Summer season• History of tick bite or contact with tick on the endemic area• History of contact with CCHF patient during health care for patient• Occupation (agriculture of field work, cowherd, cattleman, etc.)Probable case• Acute onset of illnesses with high fever (>38.0°C)• Spring-Summer season• At least two of the following haemorrhagic manifestations: petechiae, purpuric rash, rhinorrhagia,
haemorrhage, bloody vomiting, epistaxis, hemoptysis• the absence of any known precipitating factor for haemorrhagic manifestation• absence of any known reasons of haemorrhagic manifestation• leukopenia, thrombocytopenia in bloodConfirmed case• Specific clinical and epidemiological data;• anti-CCHF Ig M titers 1:800 and more, in any IgG titers, detection of RNA of the CCHF virus.Disadvantage of case definition:
include fever only more than 38,0 C.
Mild cases with sub febrile temperature can be missed
Early autumn season is missed
History of contact with possibly infected animals including agriculture animals is missed

0
20
40
60
80
100
120
140
160
180
200
Annual dynamics of CCHF cases by
months in Russia
Number of cases
tick bites60%
unknown24%
Removing of ticks
5%Crushin
g of
ticks10%
Human-to-human
transmission1%
Way of CCHF transmission
in Russia
Volynkina A.S., Kotenev E.S., Lisitskaya Ya.V., Maletskaya O.V., Shaposhnikova L.I., Kulichenko A.N. Epidemiological Situation on Crimean Hemorrhagic Fever in the Russian Federation in 2016, and Prognosis for 2017. Problemy Osobo Opasnykh Infektsii [Problems of Particularly Dangerous Infections]. 2017; 1:24–28. (In Russ.). DOI: 10.21055/0370-1069-2017-1-24-28;ProMED-mail. Crimean-Congo haemorrhagic fever (Russia, Kazakhstan, preliminary results of 2017) ProMED-mail 2017; 03 Oct: 20180127.5589232. <http://www.promedmail.org>. Accessed 30 Jan July 2018.
Individual farm43%
Collective farm
18%
Field work18%
Outdoor recreation
16%
Pastures5%
Circumstances associated with the
contamination in Russia

Fever
Ergonul O, Lancet ID, 2006

Acute onset, fever, residence in endemic area during season of tick activity
Daily examination of thrombocytes, leucocytes, ALT,
AST
thrombocytes leucocytes
ALT, AST
Testing blood samples for CCHF virus:PCR , ELISA (IgM)
Antivirals (ribavirin) administration before receiving of PCR and ELISA results
Developing of hemorrhage without any other
preconditions
Consultation of hematologist
Acute onset, fever + epidemiological anamnesis for
CCHF (habitation, occupation, visiting nature, tick bite, contact
with tick, contact with probable or confirmed CCHF case, etc.)
Patient refer for medical aidStandard PPE for examination of all patients during first medical aid:
gloves + surgical mask and goggles (if bleeding)
Probable CCHF case;PPE: gloves + goggles + surgical mask or respirator N95 or similar (if patient is
on inhalator or ALV device)
Suspected CCHF case;PPE: gloves + surgical mask
Confirmed CCHF case: PPE and antiviralsis the same as at Probable CCHF case

CCHF in Tajikistan, 2009Cluster of 5 CCHF cases in Tursunzade
Index case
a 50 year old man (day of symptoms onset 18 July 2009,day of death - 26 July 2009) within 18-24 July the
patient was treated from ILI, acute bronchitis in out-patient department, due to
deterioration of clinical picture he was addressed to hospital
- bleeding (vomiting) started in emergency room of regional
hospital(24 July 2009)
Anti CCHF IgM “-”
Secondary case
Physician who
examined patient in
emergency hospital
PPE: tissue mask,
gloves?
(died on 6 Aug)
Anti CCHF IgM “-”
Secondary case
Wife (alive)Anti CCHF IgM “+”
Secondary case
Relative (alive)Anti CCHF IgM “+”
Secondary case
Relative (died on
5 Aug),He was involved in
bureal
Anti CCHF IgM “-”
CCHF was not verified,
Body of patient was released to
relatives for burial preparation


CCHF in Kazakhstan 2009 (1)
Index case
a 23 year old woman, who re-admitted in the maternity hospital 3 days after
childbirth with fever and bleeding on 29 June 2009 and died on 4 July 2009
Due to bleeding from uterus she was operated 3 times: first time on 29 June
and twice on 2 July 2009; Anti CCHF IgM “-”
Secondary case
Surgeon in
Turkestan hospital
(died on 10 July)Not tested for CCHF
Secondary case
Vascular surgeon
from Shymkent
(died on 9 July)
CCHF Ag “+”
in corpse
Secondary case
Assistant-
gynecologist
(alive)
Anti CCHF IgM
“+”
Secondary case
Newborn baby
(died on 3 Aug),
Not tested for
CCHF
Tertiary case
Pediatrician,
who took care of
the baby (died
on 12 July)
CCHF Ag “+”
in corpse
Secondary case
old junior
maternity nurse
(alive)
Anti CCHF IgM “+”
Cluster of 7 CCHF cases in Turkestan

Mutabor Shermetova, Turkestan, Kazakhstan, 2007

Mutabor Shermetova, Turkestan, Kazakhstan, 2007

CCHF in Southern Kazakhstan region, (Turkestan city)
Mutabor Shermetova, Turkestan, Kazakhstan, 2007

Gulzhan Abuova,, Shimkent, Kazakhstan, 2007

Mutabor Shermetova, Turkestan, Kazakhstan, 2007

Recent clinical findings
Aerosol way of CCHF transmission
CCHF transmission via sexual
contacts
Severe course of CCHF in pregnancy
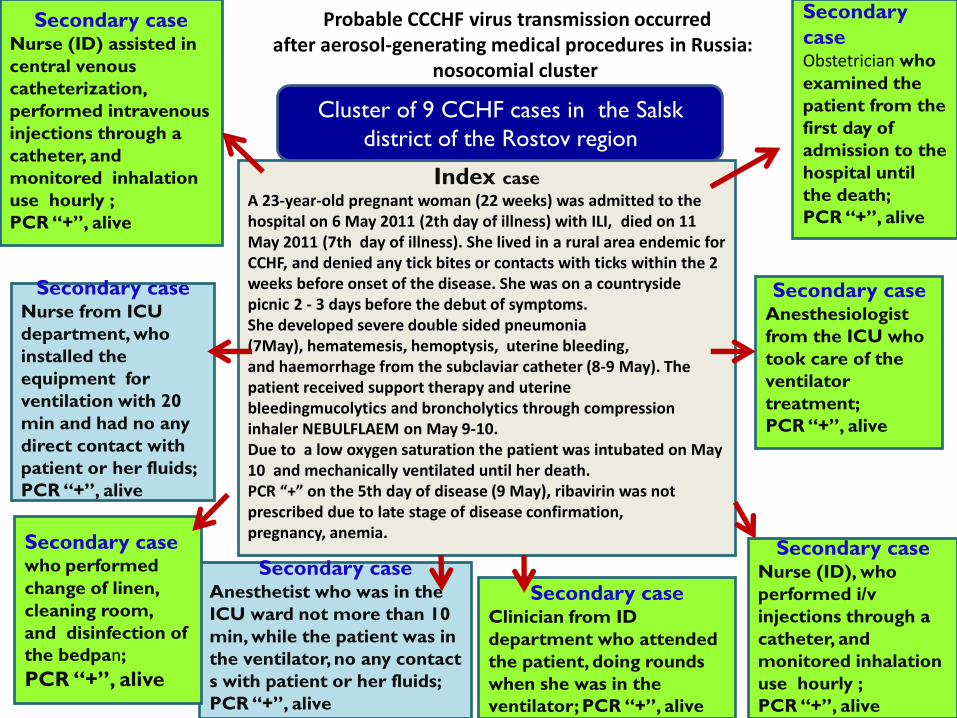
Probable CCCHF virus transmission occurred after aerosol-generating medical procedures in Russia:
nosocomial cluster
Index case
A 23-year-old pregnant woman (22 weeks) was admitted to the hospital on 6 May 2011 (2th day of illness) with ILI, died on 11 May 2011 (7th day of illness). She lived in a rural area endemic for CCHF, and denied any tick bites or contacts with ticks within the 2 weeks before onset of the disease. She was on a countryside picnic 2 - 3 days before the debut of symptoms.She developed severe double sided pneumonia (7May), hematemesis, hemoptysis, uterine bleeding, and haemorrhage from the subclaviar catheter (8-9 May). The patient received support therapy and uterine bleedingmucolytics and broncholytics through compression inhaler NEBULFLAEM on May 9-10.Due to a low oxygen saturation the patient was intubated on May 10 and mechanically ventilated until her death.PCR “+” on the 5th day of disease (9 May), ribavirin was not prescribed due to late stage of disease confirmation, pregnancy, anemia.
Secondary caseNurse (ID) assisted in
central venous
catheterization,
performed intravenous
injections through a
catheter, and
monitored inhalation
use hourly ;
PCR “+”, alive
Secondary caseNurse from ICU
department, who
installed the
equipment for
ventilation with 20
min and had no any
direct contact with
patient or her fluids;
PCR “+”, alive
Secondary caseAnesthetist who was in the
ICU ward not more than 10
min, while the patient was in
the ventilator, no any contact
s with patient or her fluids;
PCR “+”, alive
Secondary casewho performed
change of linen,
cleaning room,
and disinfection of
the bedpan;
PCR “+”, alive
Secondary caseClinician from ID
department who attended
the patient, doing rounds
when she was in the
ventilator; PCR “+”, alive
Secondary caseNurse (ID), who
performed i/v
injections through a
catheter, and
monitored inhalation
use hourly ;
PCR “+”, alive
Secondary caseAnesthesiologist
from the ICU who
took care of the
ventilator
treatment;
PCR “+”, alive
Secondary
caseObstetrician who
examined the
patient from the
first day of
admission to the
hospital until
the death;
PCR “+”, alive
Cluster of 9 CCHF cases in the Salsk
district of the Rostov region

• Should be use during certain procedures with an increased risk of infection transmission
– Ingalation via nebulazer
– aspiration or open suctioning of respiratory tract secretions
– intubation
– cardiopulmonary resuscitation
– bronchoscopy
• Appropriate PPE (gown, eye protection, gloves)
• Adequate ventilation (>12 times per 1 hour)
• Avoid unnecessary individuals in the room © WHO
Atkinson J, Chartier Y, Pessoa-Silva CL, Jensen P, Li Y, Seto W-H. Natural ventilation for infection control in health-care settings. In: WHO Publication/Guidelines. Geneva: World Health Organization; 2009 (http://www. who.int/water_sanitation_health/publications/natural_ventilation/en/index. html).
Usually standard, contact and droplet precautionsrecomended during health care for patients with CCHF
Airborne precautions should be add in specific conditions according to WHO recommendations
+

Strict Infection Control
Contact monitoring Lucille Blumberg, Tirana, Albania, 2013

2009

Administrationofribavirin,n=2 Noribavirin,n=4Lethalcasesinpregnancy 0 3Fetusdeath 0 4
Russia – 6 cases
Common mortality rate in pregnancy – 35,7%; before 20th week of pregnancy - 9%; after 20th weeks of pregnancy -48,4%
CCHF and pregnancy: systematic review and case series (42 cases totally)
Administrationofribavirin,n=13
Noribavirin,n=23 p
Lethalcasesinpregnantwomen
5(38,5±13,5%) 10(43,4±10,3%) >0,05
Fetusdeath 5(38,5±13,5%) 15(65,2±9,9%) >0,05

Mild or asymptomatic course of
disease
Subclinical infections with Crimean-Congo hemorrhagic fever virus, Turkey Emerging Infectious Diseases Volume 18, Issue 4, April 2012, Pages 640-642
The screening for IgG to CCHF virus in endemic areas showed the presence of antibodies in 10% of the population. the detection rate of IgG to CCHF increased according to the age.The researchers came to the conclusion that 88% of CCHFCases are mild or asymptomatic

Wife, 45 years old, admitted to the hospital on
the 2th day of disease (22.04.2010), on the 5th
day after tick bite (19.04).
No any hemorrhages at the day of admission,
fever 38-39 C, Hb -119 g/l, WBC - 3,4*109, PLTs -
123*103, on the 3th day of disease hemorrhages at
the places of i/v injections.
ELISA (29.04) anti CCHF IgM 1:800, IgG -negative.
1thcouple
Husband, 47 years old admitted to the hospital on
the 1th day of disease (25.04.2010), there was no
any rick factors in anamnesis, sexual contact with
wife between 20-21.04.
No hemorrhages at the day of admission, fever 39-40 C,
Hb-107 g/l, WBC- 3,2*109, PLTs - 95*103, on the 3th day
of disease gastrointestinal bleeding and massive
hemorrhages in the places of i/v injections.
ELISA (5.05 anti CCHF IgM 1:1600, IgG – negative.
2thcouple
Husband, 27 years old, the slaugther, admitted to the hospital on the 7th day of disease (23.05.2005).No any hemorrhages were detected during whole course of disease, on the first 1-2 days of illness fever was 38,0-39,0 C, next 5 days before hospitalization -32,2-37,3 C, Hb 144 g/L, WBC -3,2*109, PLTs -146*103.ELISA (30.05) anti CCHF IgM 1:800, IgG-negative.
Wife, 29 years old admitted to the hospital on the 2th
day of disease (25.05.2005), unemployed, there was no
any tick bites in anamnesis, sexual contacts with
husband between 19-22.05.
Fever 39,0 C at the day of admission, Hb-118 g/l,
leucocytes - 3,4*109, PLTs - 123*103, on the 3-4th day
of disease small hemorrhages were observed at the
places of i/v injections. CCHF confirmed by ELISA
(06.06) anti CCHF IgM 1:800, IgG – negative.
3thcouple
Husband, 55 years old, store manager,, admitted
to the hospital on the 3th day of disease
(18.06.2014), on the 5th day after tick
bite(13.06).
On the 1th day of disease fever was 37,2 C, on
the 2 and 3th days - 38-39 C, Hb 150 g/l, WBC -
4,3*109, PLTs - 128*103. No any hemorrhages
during whole course of disease were detected.
PCR (20.06) positive, ELISA (24.06) anti CCHF
IgM 1:800, IgG – negative.
Wife, 52 years old, seller, admitted to the hospital on
the 2th day of disease (21.06.2014), she had sexual
contacts with husband between 16-17.06.
Fever was 39,0 C at the day of admission, Hb-118 g/l,
WBC-2,1*109, PLTs-140*103. No any hemorrhages
during whole course of disease were detected.
PCR (22.06) positive, ELISA (30.06) anti CCHF IgM
1:6400, IgG – negative.
Primary case Secondary case
4 days
8 days
5 days
Difference between date of onset of symptoms
Transmission via sexual contacts - close contact way of CCHF transmission? (observation of 3 couples with CCHF in the Salsk district of the Rostov region of Russia, 2004-2015 )

Core factors, which are important for probable transmission via sexual
contacts:
1. All sexual partners of CCHF patient should be under
medical observation with 2-times thermometry within 14
days
1. Ribavirin preventive dose (500 mg qid 7-10 days)
should be administer for partners who had sexual
contacts with CCHF patients during disease or 1-2 days
before it.

High risk exposure
n=146
PEP Ribavirin
n=56 (38%)
Infected
n=7 (12.5%)
symptomatic
n=6 (86%)
Fatal
n=0 (0%)
Not infected
n=49 (87.5%)
no PEP
n=90 (62%)
Infected
n=87 (97%)
symptomatic
n=86 (99%)
Ribavirin <48 hrs after
symptoms
n=12
Fatal
n=0 (0%)
No ribavirin <48 hours after
symptoms
n=74
Fatal
n=32 (43%)
Not infected
n=3 (3%)
Ergonul, in press
Ribavirin in Post-Exposure Prophylaxis for CCHF

Experience from case management• If patients have not a tick bite in anamnesis:
- 30-40% of them at the pre-hemorrhagic stage of disease primary addressed for medical aid into departments of non-communicable disease and had different from CCHF diagnosis (acute diarrhea, ILI, bronchitis, hematological disease, etc.)
- 10-20% of them at hemorrhagic stage addressed to surgical, hematological, oncology, gynecology otorhinolaryngology departments)
• hypodiagnostic of CCHF and late reference for medical aid is lead to delaying of start of specific treatment (ribavirin) and supportive treatment and almost all cases of death in Russia are connected with this options (CFR 4,1%).
• Prescription of ribavirin in pre-hemorrhagic stage of CCHF ( for example, after tick bite or direct contact with confirmed CCHF case) can stop the developing of hemorrhage in 85-90% of cases

Differential diagnosis HFVs
Leptospirosis
Meningococcemia
Rickettsial diseases
Malaria
Sepsis
Influenza
Viral hepatitis
Toxic shock syndrome
Idiopathic or thrombotic thrombocytopenic purpura
Hemolytic uremic syndrome
Acute leukemia
Collagen-vascular diseases
Blumberg L et al. Manson’s Tropical Disease 2014Fisgin NT, et al. Epidemiol Infect 2010;138(1):139-44
Leblebicioglu H. UpToDate.com 2015Consider geographic distribution of diseases
68% of CCHF cases have an initial misdiagnosis of various diseases

42-yr old hunter
Not feeling well on Thursday evening
Collapsed on Friday – hypotensive, confused,
ecchymotic rash, mucosal bleeding
Constant exposure to ticks, skins wild animals
HB 10, WCC 30 000, platelets 67 000
AST 35, ALT 38
Lucille Blumberg, Tirana, Albania, 2013

42-yr old hunter
Not feeling well on Thursday evening
Collapsed on Friday – hypotensive, confused,
ecchymotic rash, mucosal bleeding
Constant exposure to ticks, skins wild animals on game
farm
HB 10, WCC 30 000, platelets 67 000
AST 35, ALT 38
CCHF NEGATIVEBLOOD CULTURE:N MENINGITIDES
Lucille Blumberg, Tirana, Albania, 2013

36yr old agriculture worker in endemic
area
• Fever, epistaxis
• WCC 18000, platelets 34 000
• AST 34, ALT 45
Lucille Blumberg, Tirana, Albania, 2013

36yr old agriculture worker in endemic
area
• Fever, epistaxis
• WCC 18000, platelets 34 000
• AST 34, ALT 45
CCHF NEGATIVELEUKEMIA
Lucille Blumberg, Tirana, Albania, 2013

TreatmentAntiviral treatment
Review 2018 – in press

Comparative studies ofribavirin treatment of CCHF in Iran
Years Route CasesRibavirin/no ribavirin
Study type Result References
1999-2001 PO 139/48 Retrospective observational
Decreased Mardani et al., 2003
1999-2004 PO 236/19 Retrospective observational
Decreased Alavi-Naini et al., 2006
2007 PO 123/0 RestrospectiveCross-sectional
Decreased/early use
Sharifi-Mood et al., 2009
Leblebicioglu H, Berlin, Germany, 2016

150
249 266
438
717
1315 1318
868
1075
796
910967
718
0
20
40
60
80
100
0
200
400
600
800
1000
1200
1400
Cases (n)
Mortality (%)
Ribavirin use (%)
%
Leblebicioglu H et al. Antiviral Research 2016;126:21-34
CCHF in Turkey between 2002-15

Difficult to interpret results of studies
• Most of them observational studies
• All of them except one retrospective studies
• Calculation of an adequate sample size is crucial
• Different study design
• Lack of randomization
• Different case definitions and case groups
• Generally small number of cases who didn’t take ribavirin in control groups
• Differences between the time from the onset of illness to treatment
• Severity of infection varies
• Viral load is not available in most studies
• Most of the studies were performed in tertiary care hospitals with more complicated patients
• Variations in medical practices
• Early diagnosis and supportive treatment may alter the clinical course of the disease
• Genetic differences between CCHFv isolates from different geographic areas
Leblebicioglu H, Berlin, Germany, 2016

Recommendations
The antiviral drug ribavirin has been used in treatment of established
CCHF infection with apparent benefit. Both oral and intravenous formulations seem to be effective
The virus is sensitive in vitro to the antiviral drug ribavirin. It has
been used in the treatment of CCHF patients reportedly with
some benefit
General supportive therapy is the keystone to success of CCHF clinical management

Supportive treatment Standard treatment is supportive therapy
Early aggressive intensive care support (plasma if hypocoagulation, Platelet
transfusion is warranted to maintain platelet count >50,000/mm3 in the setting of
bleeding and for patients with platelet count <20,000/mm3 in the absence of
bleeding).
Support of coagulation system
Careful monitoring
Oxygenation
Fluid & electrolyte balance
Blood pressure
Early use of inotropic agents (dobutamine)
Ventilation support for severe cases
Hemodialysis
Pain management
Parenteral nutrition
British Committee for Standards in Haematology Guideline. British Journal of Haematology, 2003, 122, 10–23 Leblebicioglu H, et al. Vector Borne Zoonotic Dis 2012;12(9):805-11Leblebicioglu H, et al. Vector Borne Zoonotic Dis 2012;12(9):805-11

Discharge of patients
• Relaps and reinfection after discharge were not reported
• The main criteria for discharge are resolving fever and signs and symptoms of CCHF with no longer bleeding
• Laboratory tests taken for decision of discharge in rank of order are– Platelet count (either >100.000/mm3 or 50.000-100.000/ mm3 but in a trend of
increase)– Normal internalization normalization ratio (INR), prothrombin time (PT), activated
partial thromboplastin time (apTT)– Transaminases of lower than 5 times of upper limit of normal
Leblebicioglu H, et al. J Infect 2016;72(4):500-1.
Development of WHO Guideline for Clinical Management of Crimean Congo Haemorrhagic
Fever (2016-2018) (1)
• Guideline is still in progress……
• Guideline is based on PICO questions:• Patient Problem, (or Population)
• Intervention,
• Comparison or Control
• Outcome
It includes:
• Supportive treatment (platelets, fresh frozen plasma, corticosteroids etc.)
• Directed therapeutics (ribavirin (intravenous) OR ribavirin (oral) OR favipiravir OR interferons OR immune globulin (including convalescent plasma)
• Case definition/ laboratory diagnostics (ELISA, PCR) (how case definition for CCHF (sensitivity) compared to laboratory diagnosis with RT-PCR, rapid diagnostic tests for CCHF )
• Transmission/exposure (barrier contraception for sexual contacts, breastfeeding, oral ribavirin as PEP)
• Infection prevention and control (standard PPE for VHFs )
Special attention to high risk populations (age cut-offs, comorbidities, pregnancy, obesity, etc)
Development of WHO Guideline for Clinical Management of Crimean Congo Haemorrhagic
Fever (2016-2018) (1)

EDPLN
Developing & implementing R&Droadmaps
Methodology Synopsis
High level summary of principles and concepts to
provide an overview and to be used for peer-review
publication
Methodology
CoreDocument
Outline of the information and elements to
understand roadmaps and roadmapping
development/process
Appendices
Systematic list of detailed instruction/stepsto
elaborate and to implement R&Droadmaps
CCHF has been identified as a one the WHO priority disease for which accelerated basic and applied research as well as product development would be beneficial.

CCHF R&D Blueprint roadmap (1)Main purpose
• To be able to reduce death and morbidity from CCHF through safe and affordable effective treatments informed by rapid, reliable and easily accessible diagnostics by 2023, and
• To be able to prevent or mitigate CCHF disease through deployment of safe, affordable and effective vaccines and other preventive measures by 2030.
Diagnostic• Development and validation of rapid diagnostic tests for CCHF with high sensitivity and specificity
(simple to use, sample-to-answer nucleic acid tests with high sensitivity and specificity and (ii) rapid point-of-care tests (nucleic acid or antigen detection ) with minimal requirements for biosafety precautions and staff training (2018-2024).
• By 2020, at least 2 WHO-prequalified, accessible commercial IgM and IgG serology tests available for follow-up of suspected CCHF cases, for epidemiological purposes and for pre-screening volunteers for CCHF vaccine trials.
• Investigate utility of alternative sample types (urine, oral fluid, semen etc) for CCHF diagnosis; this will also provide knowledge about CCHFV persistence in body fluids and may support non-invasive diagnostics.
• Developing «fever panel» – diagnostic tests that use a common platform to distinguish CCHF from related illnesses with similar presentation
• Continue to review the utility of next generation sequencing (especially metagenomics) for CCHF diagnostic use (including contact tracing and epidemiological approaches), particularly using portable solutions e.g. MinIon in the field.

EDPLN
CCHFtherapeuticsinterventions
● Ribavirin: systematic reviews regarding the clinical efficacy
of Ribavirin in treatment of CCHF have been published .
Both studies agree that current evidence is insufficient and
call for a large placebo-controlled trial.
● Favipiravir (T-705) good efficacy in transgenic IFNAR mouse
models.
● Intravenous immunoglobulin (IVIG), several studies in
Soviet Union, South Africa, Turkey and Bulgaria reported
but lack of evidence in absence of proper controls.
● Monoclonal antibodies (Mabs) [similar to Ebola]
● New compounds
P i e r r e F o r m e n t y , W H O , 2 n d I n t e r n a t i o n a l C o n f e r e n c e o n C r i m e a n - C o n g o
H e m o r r h a g i c F e v e r , 1 0 - 1 2 S e p t e m b e r 2 0 1 7 , T h e s s a l o n i k i , G r e e c e

Therapeutics
• By 2019, produce protocols in consultation with national regulatory authorities for dose regimen and subsequent randomized controlled trials to assess the efficacy and safety of existing therapeutic products (e.g. favipiravir), alone or in combination therapy against CCHF.
• By 2020, initiate first evaluation of the therapeutic potential of antibody therapy in a relevant preclinical model of CCHFV infection.
• By 2021, start patient enrolment to phase II trials of an existing therapeutic (e.g. favipiravir) in 2 or more countries to evaluate efficacy against CCHF disease and establish pharmacokinetic data.
• By 2023, take successful therapeutics forward to a phase III randomized controlled trial to establish full efficacy against CCHF disease.
• Development of a standardized case definition for CCHF for clinical trials
CCHF R&D Blueprint roadmap (2)

Vaccines and Vector Control
• Working with the appropriate national regulators, take at least one CCHF vaccine candidate that meets the TPP for CCHF vaccines and with proven efficacy in relevant animal models, into human phase 1 safety and early immunogenicity trails by 2019 and phase II trial by 2023.
• Prioritise and progress 5 early-stage developmental human CCHF vaccines through relevant animal models by 2025.
• By 2025, complete a proof-of-concept study of experimental Hyalomma-targeted tick vaccines and/or veterinary anti-CCHF vaccine(s) in relevant animal models.
• By 2025, identify the adaptive immune responses and protective mechanisms in humans and NHPs against CCHF disease and identify the correlates of protection for use in preclinical vaccine studies.
CCHF R&D Blueprint roadmap (3)

CCHFvaccines - candidatesFrom Dowall SD et al., 2017
Vaccine type CCHFVantigen
ImmunityProtection in
preclinical model
Clinical evidence
Antibody Tcell SafetyManufacturin
g
practicalities
Inactivated virus
(mousebrain)Whole virus Y Y ? ? No
Inactivated virus(cell
culture)Whole virus Y NT Y2 ? No
ModifiedVaccinia
Ankara(MVA)M segment Y Y Y3 Y Y
Ssegment Y Y No Y Y
DNAvaccine M segment Y NT NT Y Y
Gc, Gn andNP Y Y Y4 Y Y
Transgenicplant Glycoprotein Y NT NT ? Y
Protein Gn glycoprotein Y NT No ? Y
Gcglycoprotein Y NT No ? Y
Adenovirus M segment Y Y No Y Y
Virus-like particles Gc, Gn andNP Y Y Y5 Y Y
P i e r r e F o r m e n t y , W H O , 2 n d I n t e r n a t i o n a l C o n f e r e n c e o n C r i m e a n - C o n g o
H e m o r r h a g i c F e v e r , 1 0 - 1 2 S e p t e m b e r 2 0 1 7 , T h e s s a l o n i k i , G r e e c e
EDPLN

EDPLNCCHF R&D Blueprint, timelines
2018 2019 2021 2023
Q1-
Q2
Q2-
Q4
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Finalise CCHF R&D Baseline Assessment M1
Develop a CCHF R&D Roadmap M2
Develop CCHF Target Product Profiles M3
Prequalification review of CCHF diagnostic tests M4
CCHF therapeutics clinical trials M5
Only together we can find asolution!
Thank you for attention!

Exposure
Risk assessment
Low risk
Follow up with CBC
Normal Results in 14 days
Stop follow up
Low WBC and PLT
isolation
supportive tx
Tx with Ribavirin
High risk
PEP with ribavirin
watchfull care
Ergonul, in press
Ribavirin in Post-Exposure Prophylaxis for CCHF

42 year prison warder from endemic area
• Fever, abdominal pain
• Lives on farm in endemic area
• 7 days later: Bleeding, ARDS, renal failure
• platelets 34 000, WCC 2
• ALT 8 000, AST 6 000, LDH 30 000
• Hepatitis A and B neg. HIV neg, CCHF neg
• Died
Lucille Blumberg, Tirana, Albania, 2013

42 year prison warder from endemic
area
• Fever, abdominal pain
• Lives on farm in endemic area
• 7 days later: Bleeding, ARDS, renal failure
• platelets 34 000, WCC 2
• ALT 8 000, AST 6 000, LDH 30 000
• Hepatitis A and B neg. HIV neg, CCHF neg
• Died
HERPES HEPATITISLucille Blumberg, Tirana, Albania, 2013


















