
W.H.O gets better - thoracic.org · Objectives • Understand the various types and the WHO...
63
W.H.O gets better ? Phenotyping pulmonary hypertension: Where are we now? Rahul G Argula MBBS, MPH Assistant Professor, Division of Pulmonary, Critical Care, Allergy and Sleep Medicine Medical University of South Carolina
-
Upload
vuongtuong -
Category
Documents
-
view
214 -
download
0
Transcript of W.H.O gets better - thoracic.org · Objectives • Understand the various types and the WHO...

W.H.O gets better ?Phenotyping pulmonary hypertension:
Where are we now?
Rahul G Argula MBBS, MPHAssistant Professor,
Division of Pulmonary, Critical Care, Allergy and Sleep MedicineMedical University of South Carolina

Disclosures
• Consultant for Actelion and Gilead. • Received speaking fees from PHA for CME events. • This presentation does describe off-label use of PAH therapies in non
WHO group I patients in a research setting.

Objectives• Understand the various types and the WHO classification of
pulmonary hypertension (PH)• Review the pathophysiology of pulmonary arterial hypertension (PAH)
vs. other forms of Pulmonary hypertension (PH)• Review the treatment of pulmonary hypertension (PH) and therapies
of pulmonary arterial hypertension (PAH)• Review the current understanding of treatment of WHO groups I, II
and III pulmonary hypertension.

Age: 44 yearsHPI: Progressive dyspnea
Patient 1
Comorbidities:
• Kyphoscoliosis
• Obesity
• Obstructive Sleep Apnea
Two Women with dyspneaPatient 2
Age: 54 yearsHPI: Progressive dyspnea
Comorbidities:
• Hypertension
• Systemic sclerosis
• Mild interstitial lung disease

Patient 2
NYHA Class IV
• BP: 120/84 mm Hg
• JVP elevated
• Regular rate, rhythm
• Loud P2
• 3/6 murmur (holosystolic, left sternal border)
• 2+ leg edema
NYHA Class IV
Patient 1
• BP: 110/65 mm Hg
• JVP elevated
• Regular rate and rhythm
• Loud P2
• 2/6 murmur (holosystolic, left sternal border)
• 2+ leg edema
Two women with dyspnea

How do we manage them ?

Pulmonary hypertension: Definitions
Mean PAP ≥25 mm Hg at rest during RHCPH
Mean PAP ≥25 mm Hg plusPAWP ≤15 mm Hg plus
PVR >3 Wood units during RHCPAH
Hoeper MM et al. J Am Coll Cardiol. 2013;62:D42-D50.PAP: Pulmonary artery pressurePAWP: Pulmonary capillary wedge pressuePVR: Pulmonary vascular resistance

Right heart
Pulmonary hypertension
Lungs
Left heart
Brai
n
Live
r
Kidn
eys
Skin
MSK GI
Pulmonary arterial remodeling
Clots
Lung disease
mPAP ≥ 25 mm Hg
Left heart disease
Pulmonary artery
Pulmonary veins

1. Pulmonary arterial hypertension (PAH)1.1 Idiopathic PAH1.2 Heritable PAH
1.2.1 BMPR21.2.2 ALK1, ENG, Smad 9, CAV1, KCNK31.2.3 Unknown
1.3 Drug- and toxin-induced1.4 Associated with
1.4.1 Connective tissue disease1.4.2 HIV infection1.4.3 Portal hypertension1.4.4 Congenital heart diseases1.4.5 Schistosomiasis
1’. Pulmonary veno-occlusive disease and/orpulmonary capillary hemangiomatosis
1’’. Persistent PH of the newborn
2. PH due to left heart disease2.1 LV systolic dysfunction2.2 LV diastolic dysfunction2.3 Valvular disease2.4 Congenital/acquired left heart inflow/outflow tract
obstruction and congenital cardiomyopathies
3. PH due to lung diseases and/or hypoxia
3.1 Chronic obstructive pulmonary disease3.2 Interstitial lung disease3.3 Other pulmonary diseases with mixed restrictive
and obstructive pattern3.4 Sleep-disordered breathing3.5 Alveolar hypoventilation disorders3.6 Chronic exposure to high altitude3.7 Developmental lung diseases
4. Chronic thromboembolic PH
5. PH with unclear multifactorial mechanisms5.1 Hematological disorders: chronic hemolytic anemia,
myeloproliferative disorders, splenectomy5.2 Systemic disorders: sarcoidosis, pulmonary
histiocytosis, lymphangioleiomyomatosis, 5.3 Metabolic disorders: glycogen storage disease,
Gaucher disease, thyroid disorders5.4 Others: tumoral obstruction, fibrosing mediastinitis,
chronic renal failure, segmental PH
5th World Symposium on PH: Classification

What is the significance of pulmonary hypertension ?

*Bonferroni-adjusted p<0.05 in pairwise comparison with lowest tertile.Lam CSP et al. Circulation. 2009;119:2663-2670.
86420Time (yr)
Cum
ulat
ive
surv
ival
1.00
0.95
0.90
0.85
PASP quintile1: 15-23 mm Hg2: 24-25 mm Hg3: 26-29 mm Hg4: 30-32 mm Hg*5: 34-66 mm Hg*
86420Time (yr)
Cum
ulat
ive
surv
ival
PASP tertile1: 15-24 mm Hg2: 24-28 mm Hg3: 28-43 mm Hg*
1.000
0.975
0.950
0.925
0.900
RVSP and Survival in the community
All Participants(N=1413)
Overall Log Rank p<0.001
No Cardiopulmonary Disease (N=778)
Overall Log Rank p=0.002

Epidemiology of PH by Echocardiography• Single echocardiography lab / Australian community of 165,450/ 10,314 patients/15, 633
echocardiograms • Etiology of PH noted on echocardiogram
• N=936 with echo PASP >40 mm Hg
Strange G et al. Heart. 2012;98:1805-1811.
Miscellaneous, 2.7%
Lung disease,Sleep-related
hypoventilation,9.3%
CTEPH, 2.0%
PAH, 2.7% Unknown,
15.4%
Left heartdisease, 67.9%
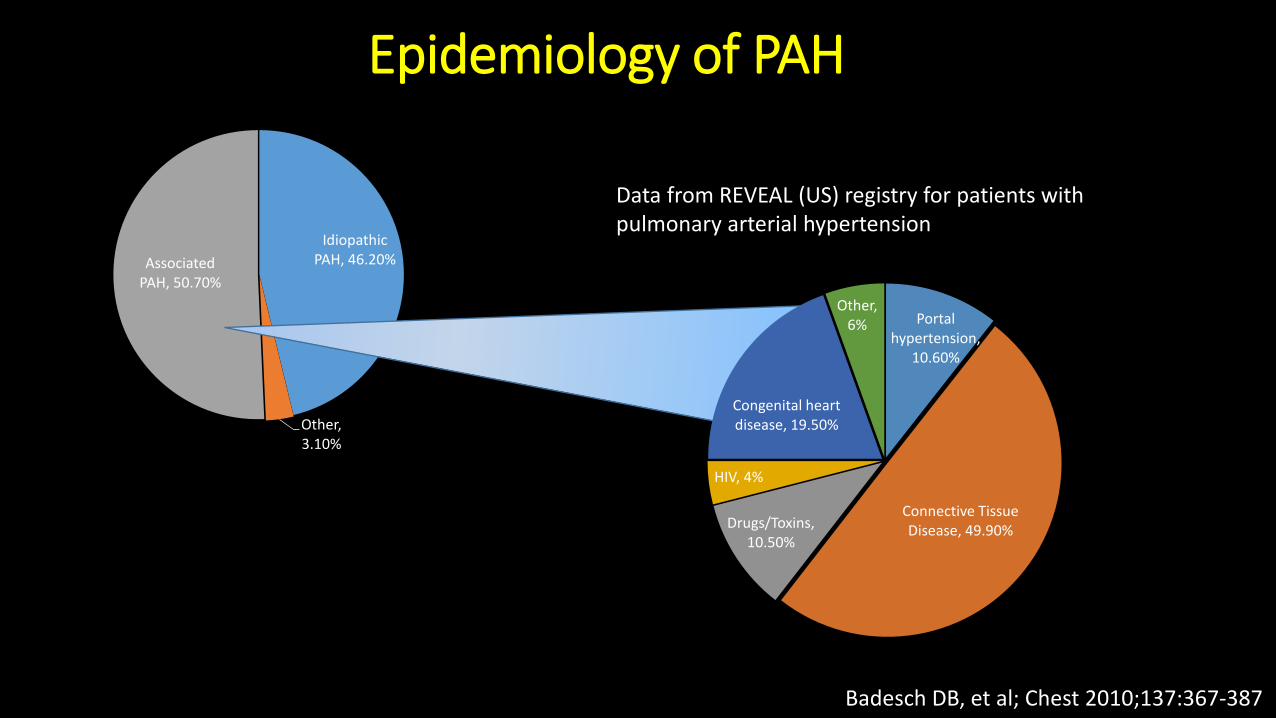
Idiopathic PAH, 46.20%
Other, 3.10%
Associated PAH, 50.70%
Epidemiology of PAH
Portal hypertension,
10.60%
Connective Tissue Disease, 49.90%Drugs/Toxins,
10.50%
HIV, 4%
Congenital heart disease, 19.50%
Other, 6%
Badesch DB, et al; Chest 2010;137:367-387
Data from REVEAL (US) registry for patients with pulmonary arterial hypertension

PH is common but PAH is rare
However, PAH is deadly!
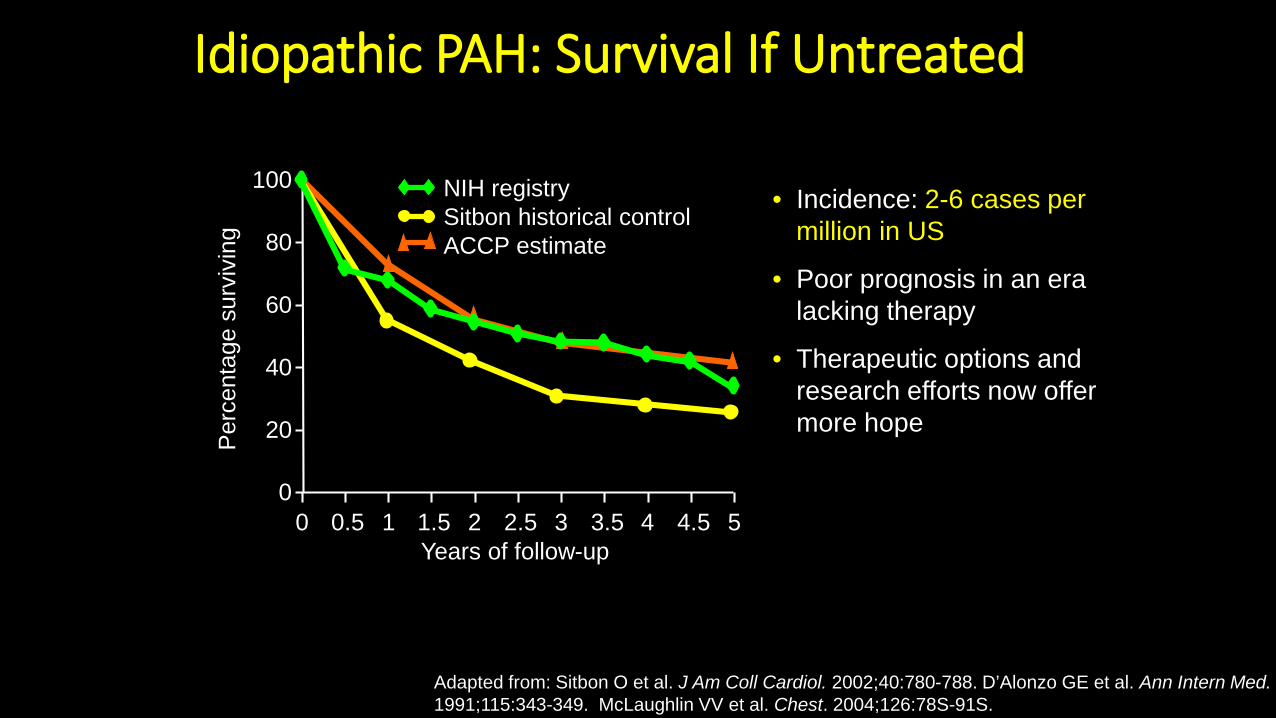
Adapted from: Sitbon O et al. J Am Coll Cardiol. 2002;40:780-788. D’Alonzo GE et al. Ann Intern Med.1991;115:343-349. McLaughlin VV et al. Chest. 2004;126:78S-91S.
Idiopathic PAH: Survival If Untreated
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 50
20
40
60
80
100
Years of follow-up
Per
cent
age
surv
ivin
gNIH registrySitbon historical controlACCP estimate
• Incidence: 2-6 cases per million in US
• Poor prognosis in an era lacking therapy
• Therapeutic options and research efforts now offer more hope

Chest. 2008;134(6):1271-1277. doi:10.1378/chest.08-1341
Pulmonary Arterial HypertensionHealthy Lung
Pathophysiology

Progression of PAH
RAP
PVR
PAP
CO
Pre-symptomatic / Compensated
Worsening symptoms
Decompensated/RV failure
Time
Adapted from: Taichman D, Mandel J, Clin Chest Med 34(2013) 619-637

How do we treat the PAH patients ?
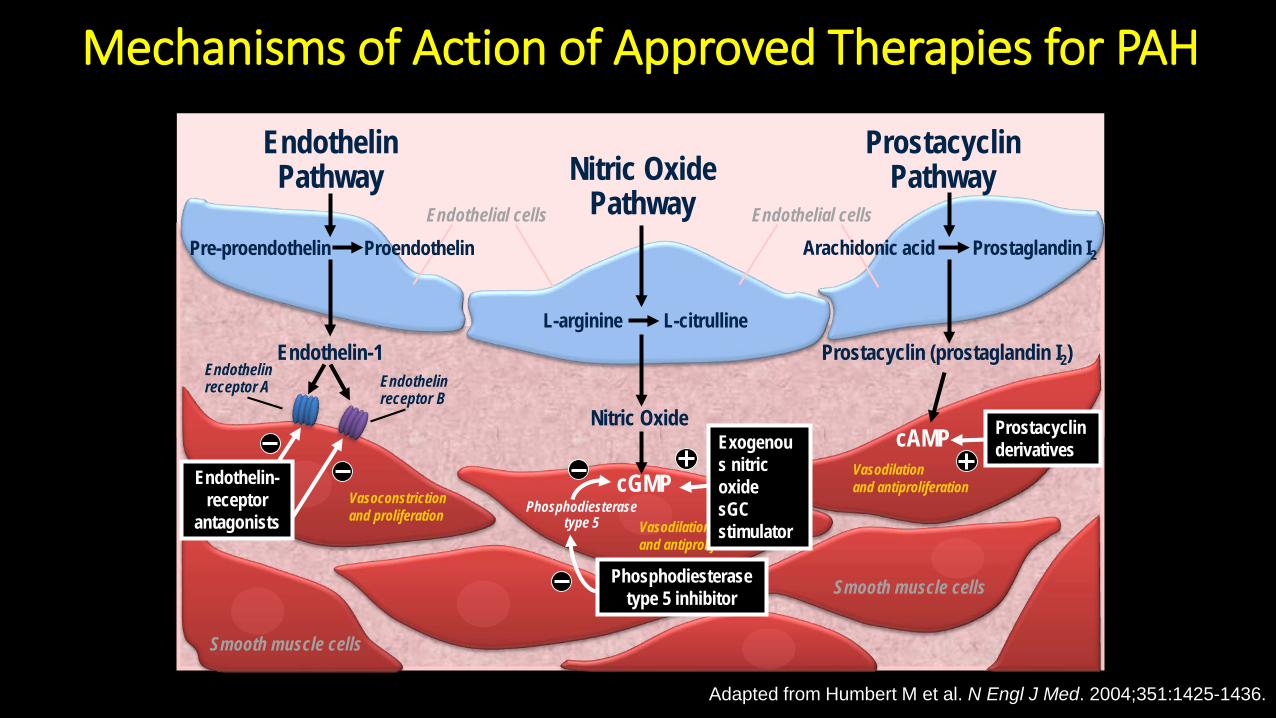
Mechanisms of Action of Approved Therapies for PAH
Adapted from Humbert M et al. N Engl J Med. 2004;351:1425-1436.
cGMP
cAMP
Vasoconstriction and proliferation
Endothelinreceptor A
Endothelin-receptor
antagonists
Endothelinreceptor B
Phosphodiesterase type 5 inhibitor
Vasodilationand antiproliferation
Phosphodiesterase type 5
Vasodilationand antiproliferation
Prostacyclin derivatives
Nitric Oxide
Endothelin-1
Pre-proendothelin
L-arginine
Prostaglandin I2
L-citrulline
Nitric OxidePathway
EndothelinPathway
ProstacyclinPathway
Endothelial cells
ProendothelinEndothelial cells
Arachidonic acid
Smooth muscle cells
Prostacyclin (prostaglandin I2)
Smooth muscle cells
Exogenous nitric oxide sGCstimulator

Pharmacotherapy of Pulmonary Arterial Hypertension
Oral Inhaled Subcutaneous IntravenousPDE5 inhibitors:- Sildenafil- Tadalafil
sGC stimulators:- Riociguat
ETR-A antagonist:- Ambrisentan
ETR- A,B antagonists:- Bosentan- Macitentan
Prostacyclin analogs:- Beraprost- Treprostinil- Selexipag
Prostacyclin analogs:- Iloprost- Treprostinil
Prostacyclin analogs:- Treprostinil
Prostacyclin analogs:- Treprostinil- Epoprostenol
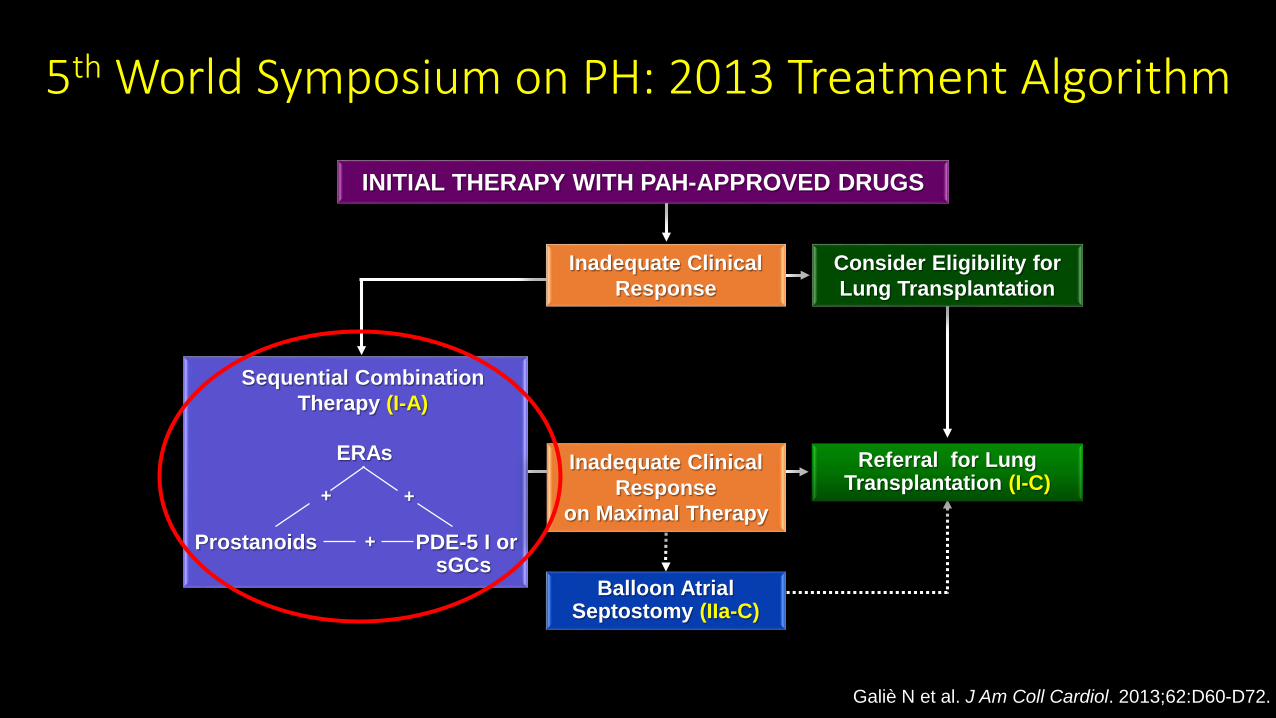
5th World Symposium on PH: 2013 Treatment Algorithm
Galiè N et al. J Am Coll Cardiol. 2013;62:D60-D72.
Sequential CombinationTherapy (I-A)
Referral for LungTransplantation (I-C)
Consider Eligibility for Lung Transplantation
Inadequate ClinicalResponse
on Maximal Therapy
INITIAL THERAPY WITH PAH-APPROVED DRUGS
PDE-5 I orsGCs
ERAs
Prostanoids
++
+
Balloon AtrialSeptostomy (IIa-C)
Inadequate ClinicalResponse

Phenotype Vs. Genotype
Phenotype: The observable attributes of an Individual
Genotype: The inherited material transmitted by gametes

Why Phenotype pulmonary hypertension?
1. Identify patients appropriate for therapy (PAH vs. PH)
2.Identify patients at risk for morbidity and mortality
3.Understand disease progression and trajectory

1965 : The origins of PH phenotyping & The Aminorex epidemic

THE W.H.O classification
First WHO classification: Geneva, 1973
Second WHO classification: Evian, 1998
Third World Symposium on PH : Venice, 2003
Fourth World Symposium on PH : Dana Point, 2008
Fifth World Symposium on PH : Nice, 2013

The first W.H.O classification of PH: 1973
1) Primary Pulmonary Hypertension (PPH): Any patient with a pulmonary artery pressure > 25mm Hg without elevation of PCWP (pulmonary capillary wedge pressure
- Pathologic Classification of PPH1. Plexogenic pulmonary arteriopathy2. Recurrent pulmonary thromboembolic disease3. Pulmonary veno-occlusive disease (PVOD)
2) Secondary Pulmonary hypertension

1. Pulmonary arterial hypertension (PAH)1.1 Idiopathic PAH1.2 Heritable PAH
1.2.1 BMPR21.2.2 ALK1, ENG, Smad 9, CAV1, KCNK31.2.3 Unknown
1.3 Drug- and toxin-induced1.4 Associated with
1.4.1 Connective tissue disease1.4.2 HIV infection1.4.3 Portal hypertension1.4.4 Congenital heart diseases1.4.5 Schistosomiasis
1’. Pulmonary veno-occlusive disease and/orpulmonary capillary hemangiomatosis
1’’. Persistent PH of the newborn
2. PH due to left heart disease2.1 LV systolic dysfunction2.2 LV diastolic dysfunction2.3 Valvular disease2.4 Congenital/acquired left heart inflow/outflow tract
obstruction and congenital cardiomyopathies
3. PH due to lung diseases and/or hypoxia
3.1 Chronic obstructive pulmonary disease3.2 Interstitial lung disease3.3 Other pulmonary diseases with mixed restrictive
and obstructive pattern3.4 Sleep-disordered breathing3.5 Alveolar hypoventilation disorders3.6 Chronic exposure to high altitude3.7 Developmental lung diseases
4. Chronic thromboembolic PH
5. PH with unclear multifactorial mechanisms5.1 Hematological disorders: chronic hemolytic anemia,
myeloproliferative disorders, splenectomy5.2 Systemic disorders: sarcoidosis, pulmonary
histiocytosis, lymphangioleiomyomatosis, 5.3 Metabolic disorders: glycogen storage disease,
Gaucher disease, thyroid disorders5.4 Others: tumoral obstruction, fibrosing mediastinitis,
chronic renal failure, segmental PH
5th World Symposium on PH: Classification

How do we manage the non WHO group I patients ?

WHO group II pulmonary hypertension

WHO group II pulmonary hypertension: Pathophysiology
Vachiery JL et al, JACC 2013;62( Suppl D): D100 – 108

Post-capillary PH
RA RV PA PVPC
LA LV Ao
mPAP ≥ 25 mm HgPCWP >15 mm HgDPG < 7 mm Hg
PVR <3 Wood units
Spectrum of PH in left heart disease
Mixed PHmPAP ≥ 25 mm HgPCWP >15 mm Hg
DPG ≥ 7 mm HgPVR ≥3 Wood units DPG: PA diastolic – PCWP gradient
Heart failure with preserved ejection fraction (HFpEF)
Heart failure with reuced ejection fraction (HFrEF)

Management of PH in left heart disease: HFpEF and HFrEF
1. Manage left heart disease
2.No currently approved therapies for HFpEF or HFrEF associated PH
3.Unique phenotypes ?

NO Pathway ERA Prostacyclin pathwayPDE5-inhibitors sGC stimulators
‘HFpEF without PH’ RELAX trial –– no benefit1
SOCRATES-PRESERVED – Vericiguatin HfPEF. No change in LA size and BNP but improved quality of life.
Most ERA studies have been in patients with heart failure alone.
The impact of ERAs on WHO II PH is unknown
IV epoprostenol in ‘HFrEF + PH’ – ‘FIRST’ trial – terminated due to increased mortality in the epoprostenol arm.
‘HFrEF + PH’ – Sildenafil improved hemodynamics and exercise performance
HFpEF + PH’ – DILATE study -Riociguat did not have significant impact on PAP but increased CI and lowered PVR.
‘HFpEF + PH’ – ‘MELODY’ trial –Macitentan in ‘HFpEF + PH’ –currently ongoing
‘HFpEF + PH’ – ‘SOUTHPAW’ trial – Oral Treprostinil in ‘HFpEF + PH’ – currently ongoing
A meta-analysis of 6 RCTs (HFrEF+ PH) - PDE5-I improved hemodynamics and exercise performance
‘HFrEF + PH’ – LEPHT study -Riociguat did not lower PAP (1o
end point), but increased CI and lowered PVR.5
Comment: From small studies, we know that ERA use in ‘HFpEF + PH’ causes significant peripheral edema7
SUMMARY: Routine use of Prostacyclin pathway analogs in WHO II PH is not approved.
PARAGON HF– results pending
‘HFpEF + PH’ – Sildenafil improved hemodynamics and exercise performance3
Comment: Riociguat could be having a systemic vasocilatory vs. cardiac effect instead of pulmonary vasodilation. SUMMARY: Routine use of ERAs in
WHO II PH is not approved. SUMMARY: Routine use of PDE5-i in WHO II PH is not approved, but may benefit a specific RV phenotpye.
SUMMARY: Routine use of sGCstimulators in WHO II PH is discouraged. May cause systemic hypotension and cardiac specific effects. Vachiery JL et al, JACC 2013;62( Suppl D): D100 – 108
WHO group II PH – clinical studies

WHO group II PH therapy : Summary
• None of the therapies for WHO group I PH (PAH) are approved for the treatment of WHO group II PH
• The NO pathway has been well studied and holds some promise in specific WHO group II phenotypes
• ERAs and Prostacyclin pathway analogs – no benefit in WHO II PH1,2
• IV Prostacyclins increase mortality in HfREF (‘FIRST’ trial)• HFpEF & PH - ERA Clincal trials underway (MELODY –macitentan)• HFpEF & PH – Prostacyclin – Clinical trial underway ( SOUTHPAW -
treprostinil)
1. Vachiery JL et al, JACC 2013;62( Suppl D): D100 – 1082. Rosenkranz S et al Int J Cardiol 2011; 154:S34-S44

WHO group III pulmonary hypertension

WHO group III pulmonary hypertension
• Second commonest cause of pulmonary hypertension (25% of all PH cases)• COPD, ILD and OSA are the commonest lung diseases associated with
pulmonary hypertension• No therapies have yet been proven to improve quality of life or survival in
patients with WHO group III pulmonary hypertension• A small subset of patients might have pulmonary hypertension that is out of
“proportion to their lung disease”• Could there be a unique “endo-phenotype” inside the WHO III population,
that could benefit from targeted therapies?

Pulmonary vasoconstriction
+ Increase in PVR
+Pulmonary vascular
remodeling
Hyperinflation
Hypercarbia
Alveolar hypoxia +
Pulmonary arterial hypoxemia
Loss of pulmonaryvascular surface
area
WHO group III pulmonary hypertension: Pathophysiology

Impact of PH in Lung disease: survivalCOPD and ILD1 COPD2
1. Leuchte HH et al, AJRCCM 2006; 173(7): 7482. Calverley P et al, COPD, 2nd Ed; 2003 (p.239)

COPD and pulmonary hypertension. Treatment with PDE5 inhibitors

Study Disease phenotype
Study design & Duration
Number of participants
(n)Outcome Results/Conclusions
Alp S, et al, 2006
COPD with moderate PH
Single arm,prospective.3-months
Sildenafil: 6 1) 6MWTD2) Hemodynamics
1) 6MWTD increased significantly2) mPAP, PVR decreased significantly
with sildenafil
Madden et al, 2006
COPD with moderate PH
Single arm,prospective.8 weeks Sildenafil: 4
1) Hemodynamics (RHC & Echo)
2) 6MWTD
1) Cardiac output increased, PVR decreased in all patients with sildenafil
2) 3 of 4 COPD patients improved 6MWTD on sildenafil
Lederer D, et al 2008
COPD without PH
Double blind randomizedcrossover trial. 4 weeks
Sildenafil:10Placebo:10
1) 6MWTD2) O2 consumption
at peak exercise
1) No change in 6MWTD2) Gas exchange worsened in sildenafil
arm3) Quality of life worsened in sildenafil
arm
Blanco I, et al, 2013
COPD with moderate PH
Double blind randomizedtrial during pulm rehab. 3 months
Sildenafil:32Placebo:31
1) Cycle endurance time
2) 6MWTD3) Quality of life
1) Cycle endurance time increased in the sildenafil arm
2) No difference in 6MWTD change between groups
3) No difference in quality of life between groups

COPD and pulmonary hypertension. Treatment with sGC stimlators and Nitric
Oxide

Study Disease phenotype
Study design & Duration
Number of participants
(n)Outcome Results/Conclusions
Ghofrani HA,et al 2015
COPD withPH (mPAP>23 and PVR>270 dynes.sec.cm-
5.
Single arm prospectivestudy
Oral Riociguat: 22 1) Hemodynamics
1) Mean PA pressure decreased2) PVRI decreased3) Cardiac output increased4) Oxygenation remained stable.5) Lung function remained stable
Vonbank K, et al, 2003
COPD with moderate PH
Double blind, placebo controlled, Randomized trial, 3-months
O2+ pulsed NO inhaled:20O2 alone: 20
1) Hemodynamics
1) Mean PA pressure decreased2) PVRI decreased3) Cardiac output increased4) Oxygenation remained stable.

COPD and pulmonary hypertension. Treatment with Endothelin Receptor
Antagonists (ERA)

Study Disease phenotype
Study design & Duration
Number of participants
(n)Outcome Results/Conclusions
Stolz D, et al 2008
Severe or very severe COPD
Double blind placebo controlled trial. 12 weeks
Bosentan:20Placebo:10
1) 6MWTD2) Quality of life3) Lung function4) Hemodynamics5) Max Oxygen
uptake
1) No change in 6MWTD2) Gas exchange worsened in Bosentan
arm3) No change in Quality of life,
hemodynamics, lung function between groups.
Valerio G, et al, 2009
COPD with moderate PH
Prospectivecohort + controls, 18 months
Bosentan: 16Controls: 16
1) Hemodynamics2) Lung function3) Dyspnea4) 6MWTD5) Quality of life
1) mPAP, PVR decreased significantly with sildenafil (more pronounced in GOLD III and IV)
2) 6MWTD improved with Bosentan3) GOLD IV patients did not improve4) GOLD II, III with severe PH showed
more improvement
Badesch D,et al, 2006
COPD with PH ARIES III, prospective.8 weeks
Ambrisentan: 24
1) 6MWTD2) BNP
1) No improvement in 6MWTD2) Significant reduction in BNP levels
from baseline.

COPD and pulmonary hypertension. Treatment with Prostacyclin pathway
agonists (PPA)

Study Disease phenotype
Study design & Duration
Number of participants
(n)Outcome Results/Conclusions
Dernaika TA,et al 2010
COPD with PH (Echo)
Single arm,prospective.Before vs. 30 min vs. 2h after iloprost (2 doses)
Iloprost : 10
1) Lung function2) Blood gases3) 6MWTD4) Hemodynamics5) Max Oxygen
uptake
1) No change in lung function2) Peak O2 consumption and CO2
production increased with iloprost3) Increase in 6MWTD with iloprost4) No changes in gas exchange, dead
space fraction and ABG.

PH in COPD: ‘Proportion’ vs ‘Out of Proportion’ to disease
1. Mild Obstructive disease and Mild PH
2. Severe Obstructive disease and Mild PH
3. Severe Obstructive disease and Severe PH
4. Mild Obstructive disease and Severe PH
Thabut G et al, Chest 2005;127(5):1535

ILD and pulmonary hypertension. Treatment with PDE5 inhibitors

Study Disease phenotype
Study design & Duration
Number of participants
(n)Outcome Results/Conclusions
Zimmerman GS, et al, 2014
ILD with PH Observational study. 6.9 + 5.8 months
Sildenafil or Tadalafil : 10 (IPF:6, HP:4)
1) Hemodynamics2) 6MWTD3) BNP
1) Hemodynamics improved (CO improved and PVR decreased from baseline)
2) No change in 6MWTD from baseline 3) No difference in BNP from baseline
Zisman DA,et al 2010(STEP IPF)
Advanced IPF
Double blind randomizedtrial. 12 weeks + 12 wks open labeled ext
Sildenafil:90Placebo:90
1) 6MWTD2) Oxygenation3) Dyspnea severity4) Quality of life
1) No between group difference in 6MWTD
2) Gas exchange stable in sildenafil arm and worsened in placebo arm
3) Quality of life and dyspnea were better in the sildenafil arm
Han MK et al, 2013
IPF patients with RV dysfunction and RV hypertrophy
Sub group analysis of STEP IPF population
Sildenafil:56Placebo:63
1) 6MWTD2) Quality of life
IPF + RV dysfunction patients had greater improvement in 6MWTD and Quality of
life (SGRQ) with sildenafil when compared to placebo.
Jackson RM, et al, 2010 Advanced IPF
Double blind randomizedtrial. 24 weeks
Sildenafil: 14Placebo: 15
1) 6MWTD2) BORG dyspnea
score
1) No between group difference in 6MWTD
2) No between group difference in BORG dyspnea score change

ILD and pulmonary hypertension. Treatment with sGC stimlators and Nitric
Oxide

Study Disease phenotype
Study design & Duration
Number of participants
(n)Outcome Results/Conclusions
Hoeper MM et al, 2013
ILD – PH (IPF, Sarcoidosis,NSIP)
Single arm prospectivestudy
Oral Riociguat: 22
1) Hemodynamics2) 6MWTD3) Arterial
oxygenation4) Mixed venous
oxygenation
1) Mean PA pressure remained same2) PVRI decreased3) Cardiac output increased4) Arterial oxygenation decreased5) Mixed venous oxygenation improved
BellerophonPPH-PF
Idiopathic ILD with & without PH
Double blind, placebo controlled, Randomized trial,
Pulsed inhaled NO
1) 6MWTD2) BNP3) Hemodynamics4) Lung function5) Dyspnea6) Quality of life
ONGOING.AWAITING IRB APPROVAL AT MUSC

ILD and pulmonary hypertension. Treatment with Endothelin Receptor
Antagonists (ERA)

Study Disease phenotype
Study design & Duration
Number of participants
(n)Outcome Results/Conclusions
Corte TJ, et al 2014BPHIT study
Fibrotic IIP patients (RHC confirmed PH)
Double blind placebo controlled (2:1) trial. 16 weeks.
Bosentan: 40Placebo: 20
1) Decrease in PVRi2) Pulmonary
hemodynamics3) Quality of life4) Lung function5) Disease
progression
1) No between group differences in PVRi
2) No between group differences in pulmonary hemodynamics, quality of life, disease progression.
Badesch D,et al, 2006ARIES III study
ILD with PH ARIES III, prospective.8 weeks
Ambrisentan: 21
1) 6MWTD2) BNP
1) No improvement in 6MWTD2) Significant reduction in BNP levels
from baseline.

ILD and pulmonary hypertension. Treatment with Prostacyclin pathway
agonists (PPA)

Study Disease phenotype
Study design & Duration
Number of participants
(n)Outcome Results/Conclusions
Saggar R et al, 2009
Advanced IPF with pulmonary hypertension
case report 1 IPF + pulmonary hypertension
1. Patient had pulmonary vascular resistance severely elevated –suggesting PH out of proportion to lung disease.
2. Patient was successfully bridged to lung transplant with IV treprostinil
INCREASE
ILD (CTD associated or idiopathic) or CPFE, with PH
Double blind, placebo controlled, Randomized trial,
Inhaledtreprostinil: vs PlaceboTotal: 314
1) 6MWTD2) BNP3) Lung function4) Dyspnea5) Quality of life
ONGOING.CURRENTLY RECRUITING AT MUSC

PH in ILD and COPD: Treatment summary
• Treat hypoxemia, hyperinflation and avoid hypercapnia. • None of the WHO group I therapies are approved for treatment of
PH associated with ILD or COPD. • PDE5 inhibitors are the best studied PA vasodilator therapies in
COPD and ILD related PH• PDE5 inhibitors have not been shown to improve quality of life or
survival in patients with ILD/COPD related pulmonary hypertension• A small subset of patients with pulmonary hypertension that is out
of “proportion to their lung disease” might be the most favorable targets for therapies in the future.

PH in Obstructive sleep apnea : Treatment• Treat OSA with CPAP or BiPAP
therapy• Pulmonary hemodynamics
usually improve with OSA therapy
• No indication for PA vasodilator therapies
• Consider treatment in : Patients with persistent pulmonary hypertension and symptoms despite OSA therapy
Sajkov D et al, AJRCCM 2002 165 (2):154

Patient 2
Labs
• ABG: PH:7.42/40/86 mm Hg (FiO2:21%)
• HcO3- = 26
• BMP:134/3.8/98/26/19/0.9
• CBC, Renal function: WNL
• CXR: Cardiomegaly, mild ILD in bases
Two Women with dyspnea
Labs
Patient 1
• ABG: pH: 7.3/78/68mm Hg (FiO2:30%)
• HCO3- = 45
• BMP:136/4.8/98/45/16/0.8
• CBC, Renal function: WNL
• CXR: Kyphoscoliosis

Patient 2
Echo
• LV: EF 58%
• Grade 1 diastolic dysfunction
• RV: ↑↑↑ size
• 3+ RV dysfunction
• PASP: 76 mm Hg
• RA: 10 mm Hg
• 2+ TR
Echo
Patient 1
• LV: EF 65%
• No diastolic dysfunction
• RV: ↑ size
• 1+ RV dysfunction
• PASP: 60 mm Hg
• RA: 10 mm Hg
• 1+ TR
Two Women with dyspnea

Patient 2
Invasive Hemodynamics• RA: 12 mm Hg
• mPAP: 41 mm Hg
• PCWP: 10 mm Hg
• CO: 2.6 L/min
• PVR: 11.9 Wood units
• BP: 93/69 mm Hg• Vasodilator challenge with iNO: non-responder
Invasive Hemodynamics
Patient 1
• RA: 8 mm Hg
• mPAP: 39 mm Hg
• PCWP: 11 mm Hg
• CO: 5.6 L/min
• PVR: 5 Wood units
• BP: 148/80 mm Hg• Vasodilator challenge with iNO: non responder
Two Women with dyspnea

Patient 2
Final Diagnosis• WHO Group I—pulmonary
arterial hypertension (PAH)
• PAH due to connective tissue disease
Final Diagnosis
Patient 1
• WHO Group III—pulmonary hypertension due to chronic alveolar hypoventilation
• Severe Obstructive sleep apnea and chest wall restriction (FVC :64% predicted)
Sleep study: Severe Sleep apnea with multiple apneic events during sleep
Sleep study: Not performed as patient had no risk factors for sleep apnea
Two Women with dyspnea
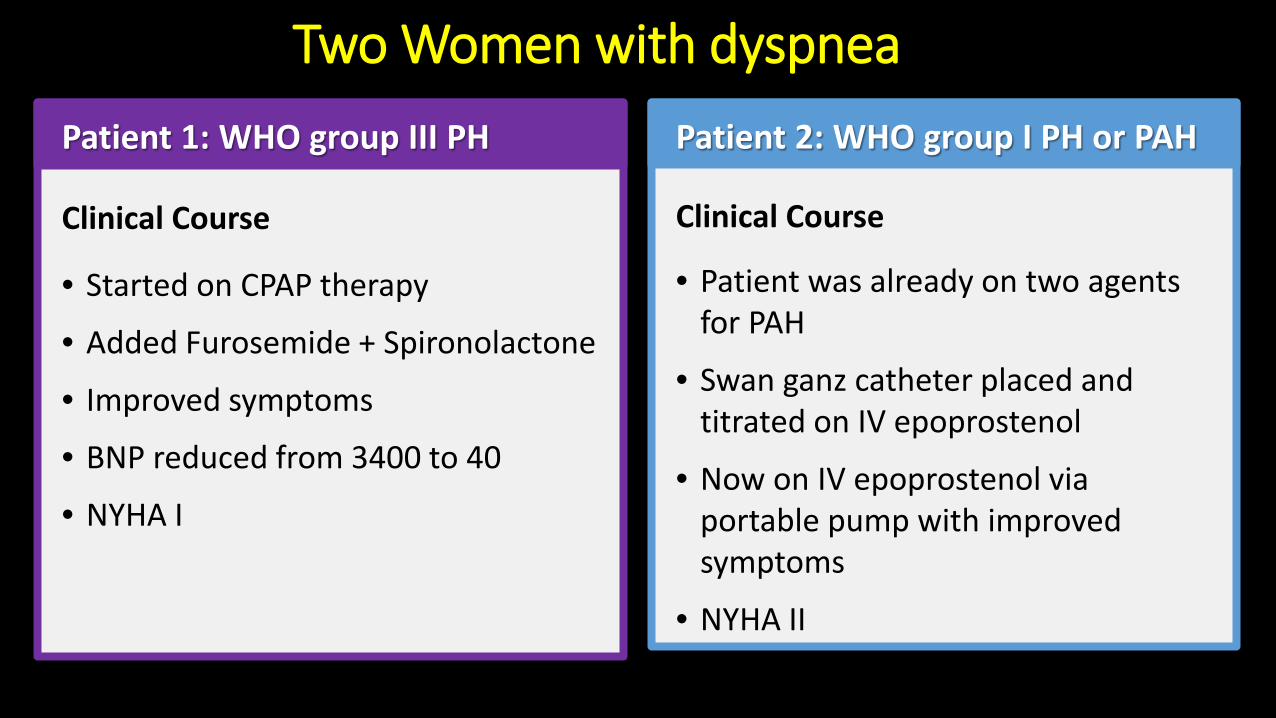
Patient 2: WHO group I PH or PAH
Clinical Course
• Patient was already on two agents for PAH
• Swan ganz catheter placed and titrated on IV epoprostenol
• Now on IV epoprostenol via portable pump with improved symptoms
• NYHA II
Clinical Course
Patient 1: WHO group III PH
• Started on CPAP therapy
• Added Furosemide + Spironolactone
• Improved symptoms
• BNP reduced from 3400 to 40
• NYHA I
Two Women with dyspnea

Summary: PH Lessons1. PH is common, but most often due to LHD or chronic lung disease:
selective pulmonary vasodilators are not proven in these patients2. PAH is rare but deadly:3. Learn to differentiate Group I PAH from other forms of PH: when in
doubt, refer to a PH center. 4. No currently approved therapies for WHO group II or left heart
disease related PH. There might be a unique RV phenotype suitable for therapy with PDE5 inhibitors.
5. No currently approved therapies for WHO group III or lung disease related PH. Among IPF patients, there might be a unique RV phenotype suitable for therapy with PDE5 inhibitors.
6. No indication for PA vasodilator use in patients with OSA associated PH.


















