
Who Gets Alcoholic Liver Disease? - ERAB · Case control studies of PNPLA3 in ALD Study Numbers...
32
Who Gets Who Gets Alcoholic lcoholic Liver iver Disease? isease? Chris Day Chris Day Newcastle University Newcastle University
Transcript of Who Gets Alcoholic Liver Disease? - ERAB · Case control studies of PNPLA3 in ALD Study Numbers...

Who Gets Who Gets AAlcoholic lcoholic LLiver iver
DDisease?isease?
Chris DayChris Day
Newcastle University Newcastle University

Fatty hepatocytes Fatty hepatocytes
Intracellular fat
deposition
Intracellular fat
deposition
Alcoholic Fatty Liver (Steatosis) Alcoholic Fatty Liver (Steatosis)

Fibrosis with necrosis Fibrosis with necrosis
Inflammation Inflammation
Fat deposits Fat deposits
Alcoholic SteatoHepatitis (ASH) Alcoholic SteatoHepatitis (ASH)
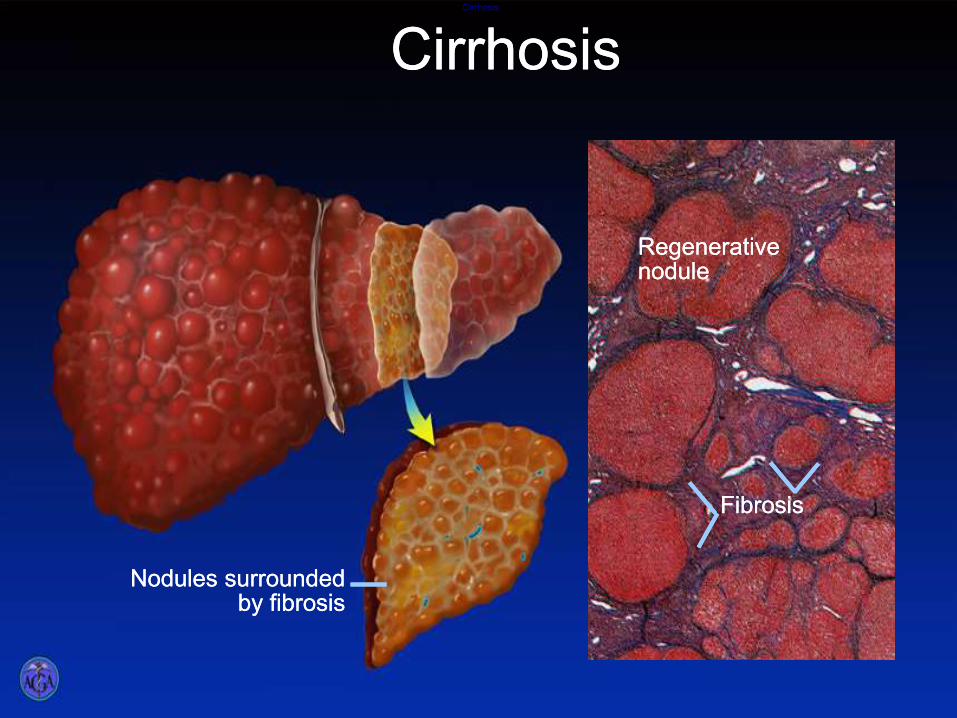
Cirrhosis Cirrhosis
Fibrosis Fibrosis
Nodules surrounded by fibrosis
Nodules surrounded by fibrosis
Regenerative nodule Regenerative nodule
CirrhosisCirrhosis

Fatty Liver
(60-100%)
Normal
(0-30%)
Cirrhosis
(<10%)
Steatohepatitis
(20-30%)
Prevalence of disease
stages in unselected
heavy drinkers
WHY??

Dose & pattern of alcohol intake Dose & pattern of alcohol intake
Dietary factorsDietary factors –– Specific nutrients?Specific nutrients?
–– General excess (obesity)General excess (obesity)
Smoking Smoking Becker 2002, Becker 2002, KlatskyKlatsky 20062006
Coffee drinkingCoffee drinking KlatskyKlatsky 20062006
Gut bacteria (the “microbiome”) ? Gut bacteria (the “microbiome”) ?
NonNon--genetic (inherited) factorsgenetic (inherited) factors

Leon et alLeon et al Lancet 2006Lancet 2006
ALD & Dose: population levelALD & Dose: population level
Cirrhosis death rate correlates
with per capita alcohol intake

ALD & Dose: individual levelALD & Dose: individual level
0
1
2
3
4
5
6
7
8
0 0.1-3 3-6 6-9 9-12 >12
Cirrhosis
Any liverdisease
% of
category
Drinks per day
Bellentani et al 1997Bellentani et al 1997

ALD risk and ALD risk and patternpattern of intakeof intake
Risk of ALD increased by:Risk of ALD increased by:
Drinking outside mealDrinking outside meal--timestimes
RiskRisk : 3.4[1.7: 3.4[1.7--6.6] 6.6] BellentaniBellentani 19971997
Drinking beer/spirits rather than wineDrinking beer/spirits rather than wine
RiskRisk : 2.5[1.7: 2.5[1.7--3.3] 3.3] Becker 2002Becker 2002
Daily versus weekend drinking Daily versus weekend drinking
RiskRisk : 2.5 [1.8: 2.5 [1.8--4.6] 4.6]
StokkelandStokkeland 20082008

Johansen, Friis, Skovenborg, Gronbaek BMJ 2006
Is wine Is wine vsvs beer effect due to beer effect due to
confounding “lifestyle” factors?confounding “lifestyle” factors?

Diet and ALD: the role of Diet and ALD: the role of
obesityobesity
0
5
10
15
20
25
30
35
Steatosis Hepatitis Cirrhosis
% o
ve
rw
eig
ht
With lesion
Withoutlesion
1604 heavy drinkers1604 heavy drinkers
Overweight = minimum Overweight = minimum
BMI>25 women, >27 men BMI>25 women, >27 men
in previous 10yrin previous 10yr
In multivariate analysis In multivariate analysis
obesity/glucose best obesity/glucose best
predictors of cirrhosis predictors of cirrhosis
(Risk (Risk > x 2> x 2 for obesity) for obesity)
Naveau et al 1997Naveau et al 1997
Raynard et al 2002Raynard et al 2002

Rates of liver cirrhosis in 1,230,662 UK women
(mean age 56yrs) followed up for mean 6.2 years
Liu Br Med J 2010

Relative risks of contributions of BMI and alcohol to liver
disease mortality (adjusted for all risk factors).
Hart Br Med J 2010
9,559 Scottish men followed up for mean 29 years

Obesity & ALD: ?explanation for Obesity & ALD: ?explanation for
associationassociation
Mechanisms of ALD & obesity related Mechanisms of ALD & obesity related
liver disease (NAFLD) very similar:liver disease (NAFLD) very similar: –– Metabolic overloadMetabolic overload
–– Oxidative, ER and cytokine mediated stressOxidative, ER and cytokine mediated stress
–– The The microbiomemicrobiome//endotoxinendotoxin
Direct Direct fibrogenicfibrogenic (scar producing) (scar producing)
effects of obesityeffects of obesity –– High Insulin/glucoseHigh Insulin/glucose
–– ““AdipokineAdipokine” profile” profile

Risk of ALD and coffee drinkingRisk of ALD and coffee drinking
Coffee intakeCoffee intake Relative Risk of ALDRelative Risk of ALD
Never/seldomNever/seldom 1.01.0
<1<1 0.7 [0.40.7 [0.4--1.1]1.1]
11--33 0.6[0.40.6[0.4--0.8], p<0.0010.8], p<0.001
≥4≥4 0.2[0.10.2[0.1--0.4], p<0.0010.4], p<0.001
Per cup/dayPer cup/day 0.8[0.70.8[0.7--0.9], p<0.0010.9], p<0.001
Adjusted for age, weight, smoking, gender, ethnicity
Klatsky 2006

Gut bacteria Gut bacteria -- the “microbiome” the “microbiome”
-- and ALD susceptibility?and ALD susceptibility?
Abundant evidence that the gut Abundant evidence that the gut
microbiomemicrobiome may be involved in ALD may be involved in ALD
pathogenesis pathogenesis PurohitPurohit 20082008
NonNon--alcoholic steatohepatitis (NASH) as alcoholic steatohepatitis (NASH) as
a transmissible disease ? a transmissible disease ? HenaoHenao--Mejia Nature 2012Mejia Nature 2012
What about ALD?What about ALD?
–– Faeces from ALD patients induce ALD in Faeces from ALD patients induce ALD in
alcohol fed mice alcohol fed mice LlopisLlopis 20132013
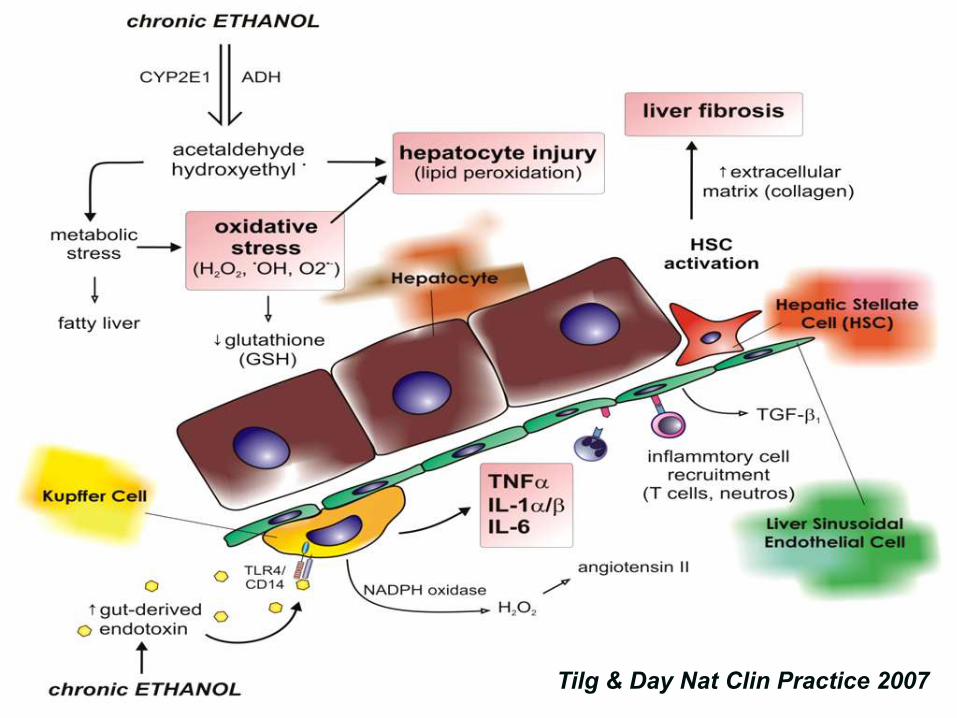
Tilg & Day Nat Clin Practice 2007

Gender and ALDGender and ALD
Females develop ALD at “lower” intakeFemales develop ALD at “lower” intake
Explanation: Explanation: blood alcohol levels for same blood alcohol levels for same dose per body weightdose per body weight VolVol distribution distribution Marshall 1983Marshall 1983
EstrogenEstrogen sensitises the liver (sensitises the liver (KupfferKupffer cells) to cells) to bacterial (bacterial (endoendo) toxins) toxins –– gut permeability to gut permeability to endotoxinendotoxin
–– Endotoxin receptors (CD14) & release of Endotoxin receptors (CD14) & release of inflammatory mediators from liver inflammatory inflammatory mediators from liver inflammatory cells (cells (egeg. . TNFTNFaa)) Thurman et al 1999Thurman et al 1999

Tilg & Day Nat Clin Practice 2007

Are genes importantAre genes important??
Concordance rates (%) among 15 924 male twin
pairs age 67-77. Alcoholism and cirrhosis ↑ 25%.
Alcoholism genetic
ALD genetic
Risk “over-and-above” the risk of
alcoholism
Hrubec 1981
MZ DZ
Alcoholism 26.3 11.9
Cirrhosis 14.6 5.4
MZ DZ
Alcoholism 26.7 12.2
Cirrhosis 16.9 5.3
1981 1996
Alcoholism genetic
ALD risk now shared with alcoholism
No longer a significant independent
genetic risk for ALD
Reed 1996
Ethnic variation in susceptibility Ethnic variation in susceptibility
Caetano & Clark 1998, Stinson 2001, Caetano & Clark 1998, Stinson 2001,
KlatskyKlatsky 2006 2006

Finding the genesFinding the genes
HypothesisHypothesis--drivendriven
–– Candidate gene caseCandidate gene case--control studiescontrol studies All studies in ALD thus farAll studies in ALD thus far
Almost all underpowered (too small)Almost all underpowered (too small)
HypothesisHypothesis--free (generating)free (generating)
–– “Whole” genome scanning “Whole” genome scanning None in ALD as yet (underway) None in ALD as yet (underway) –– BUT:BUT:
Clues from studies in NAFLDClues from studies in NAFLD

• USA Study population: (Black n=1032, White n=636, Hispanic n=383).
• 9229 non-synonymous exonic SNPs.
• Steatosis defined non-invasively by 1H-MRS.
Figure 2.
Association between a sequence variant in PNPLA3 (I148M) and hepatic triglyceride (TG)
content. (a) PNPLA3 is a 481 residue protein that contains a patatin-like domain at the N
terminus (residues 10-179, UniProt http://pir.uniprot.org/uniprot/ ) with consensus sequences
for a Ser-Asp catalytic dyad (Gly-X-Ser-X-Gly and Asp-X-Gly/Ala)14. The I148M substitution
(rs738409) is located between the consensus sequences for the catalytic dyad and is highly
conserved. (b) Median hepatic TG content, body mass index (BMI), homeostatic model
assessment of insulin resistance (HOMA-IR) and plasma TG levels in the Dallas Heart Study.
Values for hepatic fat content were compared using ANOVA. Age, gender, BMI, diabetes
status, ethanol use and global ancestry were included as covariates in the model. ( c) Median
Romeo et al. Page 9
Nat Genet. Author manuscript; available in PMC 2009 June 1.
NIH
-PA
Auth
or M
anu
scrip
tN
IH-P
A A
uth
or M
an
uscrip
tN
IH-P
A A
uth
or M
an
uscrip
t
Figure 2.
Association between a sequence variant in PNPLA3 (I148M) and hepatic triglyceride (TG)
content. (a) PNPLA3 is a 481 residue protein that contains a patatin-like domain at the N
terminus (residues 10-179, UniProt http://pir.uniprot.org/uniprot/ ) with consensus sequences
for a Ser-Asp catalytic dyad (Gly-X-Ser-X-Gly and Asp-X-Gly/Ala)14. The I148M substitution
(rs738409) is located between the consensus sequences for the catalytic dyad and is highly
conserved. (b) Median hepatic TG content, body mass index (BMI), homeostatic model
assessment of insulin resistance (HOMA-IR) and plasma TG levels in the Dallas Heart Study.
Values for hepatic fat content were compared using ANOVA. Age, gender, BMI, diabetes
status, ethanol use and global ancestry were included as covariates in the model. ( c) Median
Romeo et al. Page 9
Nat Genet. Author manuscript; available in PMC 2009 June 1.
NIH
-PA
Auth
or M
anu
scrip
tN
IH-P
A A
uth
or M
an
uscrip
tN
IH-P
A A
uth
or M
an
uscrip
t
PNPLA3 (I148M) – Carriage of G allele associated with increased steatosis (p=5.9 x 10-10)

Presence of NASH
OR 1.5 (1.12-2.04)
Fibrosis >F1
OR 1.5 (1.09-2.12)
N=591

PNPLA3 PNPLA3 -- AdiponutrinAdiponutrin
Anstee et al, 2013
He et al, 2010 Huang et al, 2010 Huang et al, 2011 Pirazzi et al, 2012
But why the link with NASH & scarring?

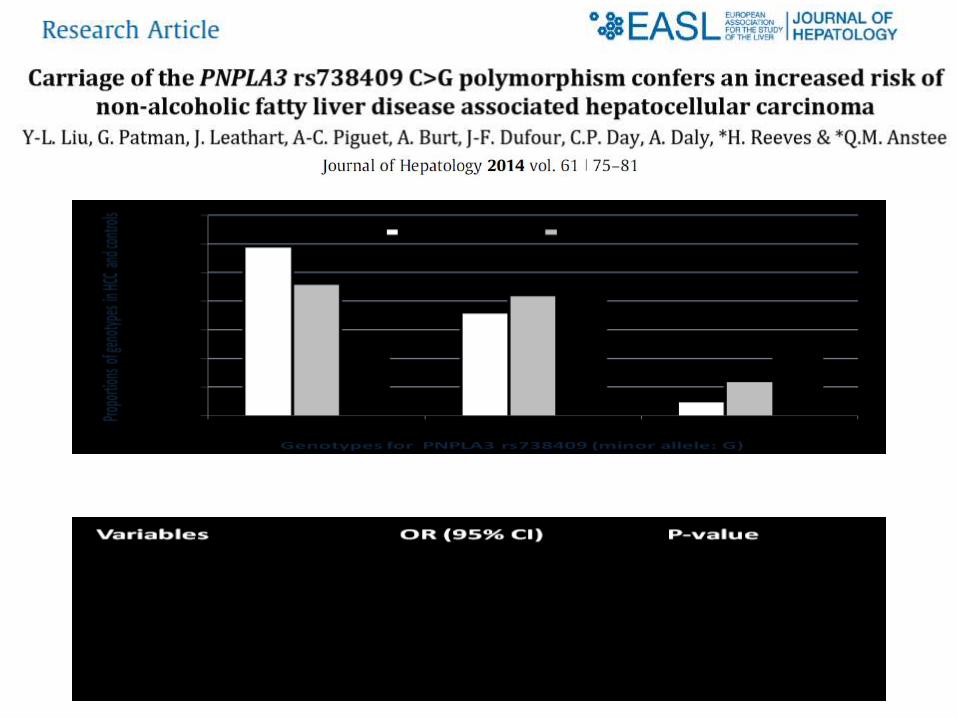

Case control studies of PNPLA3 Case control studies of PNPLA3
in ALD in ALD
Study Numbers Ethnicity Associated
phenotype
Tian, 2010 1,221 Mexican-
European
Risk of ALD and
cirrhosis
Seth, 2010 548 UK Risk of ALD and
cirrhosis
Stickel , 2010 1,043/376 German Risk of ALD and
cirrhosis
Trepo, 2011 658 Belgian Risk of ALD and
cirrhosis
Trepo 2012 571 Belgian and
French
Risk of HCC
Nischalke 2011 160 Germany Risk of HCC

TM6SF2 (E167K) – Carriage of minor allele associated with increased steatosis (p=5.7 x 10-8)
See also: Holmen et al, Nature Genetics, 2014
– Carriage of major allele increased cholesterol and cardiovascular disease

Multivariate analysis (additive model) incorporating Age, Gender, BMI, T2DM and PNPLA3 rs738409 genotype.
i.e. OR per copy of the minor allele carried
Nature Communications, 2014; 10.1038/ncomms5309.

↑ IHTG
↑Steatosis
↑ Fibrosis
? ↑ NASH ↑ Cardiovascular Disease
↓ LDL-C ↓ TG
T-allele Lys167 (E167K)
↓ Hepatic VLDL Excretion
C-allele Glu167 (E167K)
↑ Total Chol ↑ LDL ↑ TG
↑ Hepatic VLDL Excretion
↑ Intrahepatic Fatty Acid Flux
Obesity Alcohol T2DM
TM6SF2 rs58542926
Does TM6SF2 genotype determine the CAUSE of death in
NAFLD/ALD?

TM6SF2 gene variant determines TM6SF2 gene variant determines
risk of liver and heart disease risk of liver and heart disease
Dongiovanni 2014

ConclusionsConclusions
ALD is a typical “complex” disease with susceptibility ALD is a typical “complex” disease with susceptibility likely due to a combination of genetic/environmental likely due to a combination of genetic/environmental factorsfactors
Several modifiable environmental risk factors such Several modifiable environmental risk factors such as diet/coffee drinking identifiedas diet/coffee drinking identified
Role of the Role of the microbiomemicrobiome as a modifiable and as a modifiable and ?transmissible risk factor worthy of further study?transmissible risk factor worthy of further study
PNPLA3 is the only robust genetic association PNPLA3 is the only robust genetic association reported thus far and is also associated with HCCreported thus far and is also associated with HCC
Genetic factors may explain CAUSE of death in Genetic factors may explain CAUSE of death in heavy drinkersheavy drinkers
GGenome wide scans are awaited with interestenome wide scans are awaited with interest


















