
Whiplash Associated Disorders J. Scott Bainbridge, MD Denver Back Pain Specialists .
60
Whiplash Associated Whiplash Associated Disorders Disorders J. Scott Bainbridge, MD Denver Back Pain Specialists www.denverbackpainspecial ists.com
-
Upload
charla-barber -
Category
Documents
-
view
223 -
download
1
Transcript of Whiplash Associated Disorders J. Scott Bainbridge, MD Denver Back Pain Specialists .

Whiplash Associated DisordersWhiplash Associated Disorders
J. Scott Bainbridge, MD
Denver Back Pain Specialists
www.denverbackpainspecialists.com
DefinitionDefinition
Quebec Task Force on Whiplash-Associated-Disorders redefined the term in 1995 as “an acceleration-deceleration mechanism of energy transfer to the neck which may result from rear-end or side impact, predominately in MVAs, and from other mishaps.

DefinitionDefinition
The energy transfer may result in bony or soft tissue injuries (whiplash injury), which may in turn lead to a wide variety of clinical manifestations (whiplash Associated Disorders)”.

WAD – Scope of ProblemWAD – Scope of Problem
Yearly Incidence 4/1,000 (.8-8)$3.9 billion/yr in USA, $29 b w litigation4-42% of pts w MVA related neck injuries
with sx several yrs later

Quebec ClassificationQuebec Classification
Grade 0: No neck c/o or PE signsGrade I: Neck c/o pain, stiffness or
tenderness but no PE signsGrade II: Neck c/o AND mskl signsGrade III: Neck c/o AND neuro signsGrade IV: Neck c/o AND fracture or
dislocation

MVA – Spectrum Beyond MVA – Spectrum Beyond WADWAD
Cervicothoracic Other MusculoskeletalBrain Injury, Post Concussive SyndromeOther NeurologicalVestibular DysfunctionPsychologicalSocial/Economic/Litigation

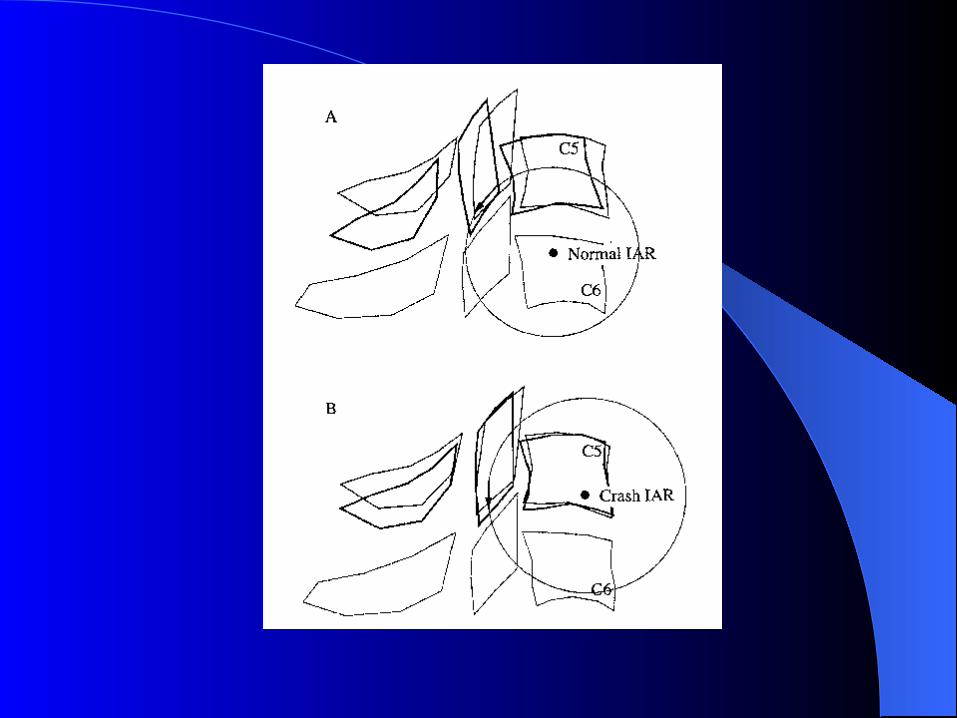
Motion Analysis of C-Spine Motion Analysis of C-Spine During Whiplash LoadingDuring Whiplash Loading
Kaneoka, et al; Spine 24:8 pp 763-77010 males – sled glided back into damper at
4 km/hrCineradiography of C-spineEach vertebra’s rotational angle and C5-6
instantaneous axes of rotation quantifiedSEMG of SCM and C-paraspinals

Pathological ForcesPathological Forces
8 km/hr 5 mph135 N

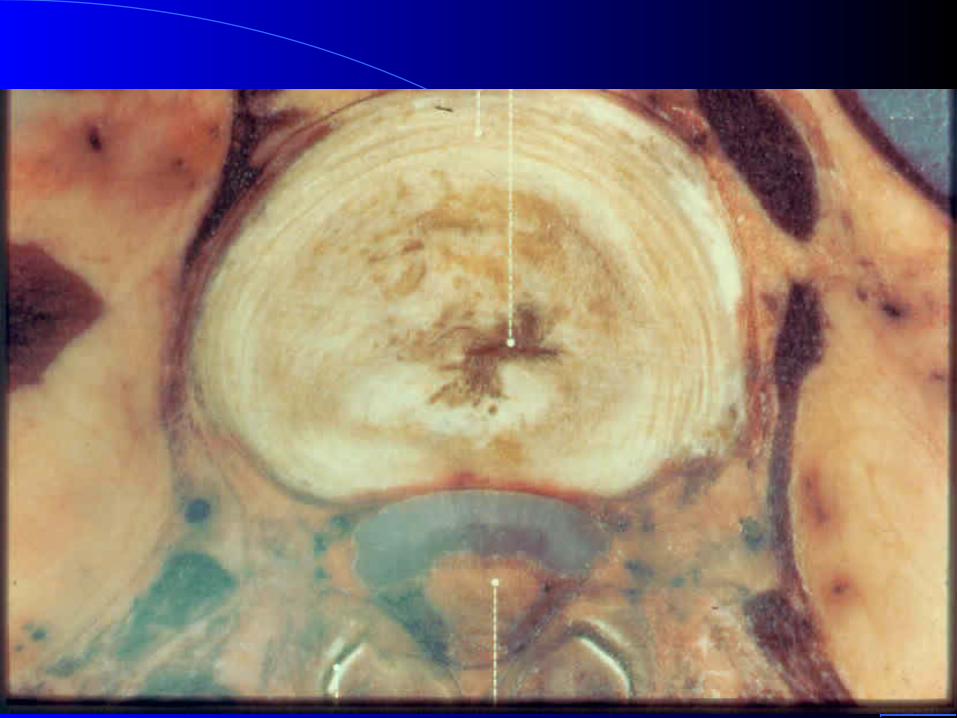
PathologyPathology
Facet: synovial fold (meniscoid) impingement, facet capsular subcatastrophic failure, capsular failure w/wo fracture or subluxation, microfracture – cart/bone
Disc rim lesions/herniation, anterior vs. posterior Neural Muscular Start or speed degenerative cascade
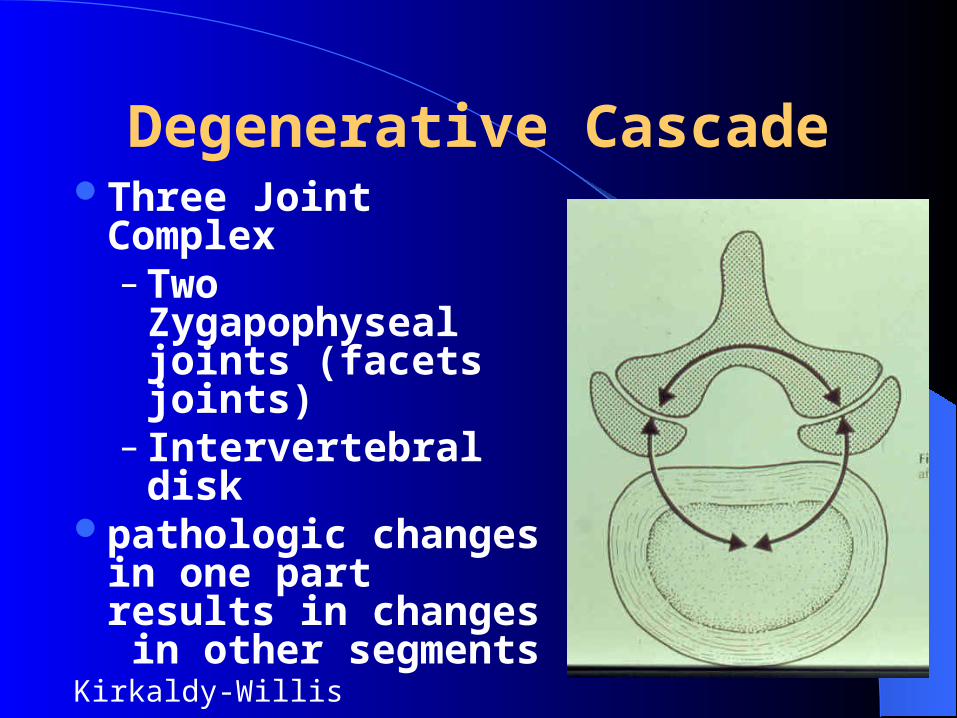
Degenerative CascadeThree Joint Complex
– Two Zygapophyseal joints (facets joints)
– Intervertebral diskpathologic changes in
one part results in changes in other segments
Kirkaldy-Willis

Degenerative Cascade – Segmental Dysfunction
reactive z-joint synovitis– Inflammation &
joint pain

Degenerative Cascade – Degenerative Cascade – Segmental DysfunctionSegmental Dysfunction
articular cartilage z-joint degeneration

Subchondral Sclerosis

Cartilage Degeneration

Degenerative Cascade – Degenerative Cascade – Instability PhaseInstability Phase
Annular fibers less competent
Disc protrusions

Uncovertebral Joints - Joints of LuschkaUncovertebral Joints - Joints of Luschka
Uncinate processes hook posterolaterally between one vertebra & the base of the next
With shearing stresses to anular tissue, degenerative spurs begin to develop in teenage years
Spurring can cause foraminal stenosis

Degenerative Cascade – Degenerative Cascade – Instability PhaseInstability Phase
Normal Foraminal narrowing
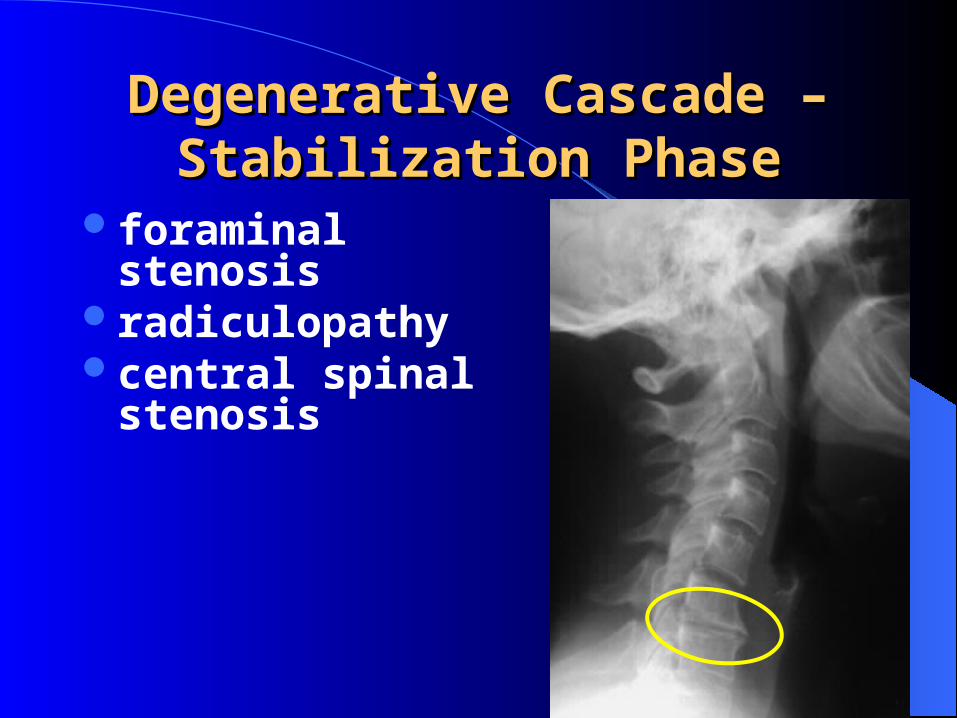
Degenerative Cascade – Degenerative Cascade – Stabilization PhaseStabilization Phase
foraminal stenosisradiculopathycentral spinal
stenosis

Degenerative Cascade – Degenerative Cascade – Stabilization PhaseStabilization Phase
ankylosis of motion segment
multilevel degenerative changes & spondylosis

Degenerative Cascade – Degenerative Cascade – Stabilization PhaseStabilization Phase
ankylosis of motion segment

Cervical Z Joint PainPrevalence of chronic cervical z-joint
pain after whiplash injuries: 60% (Lord, Spine, 1996)
Z Joint pain referral patterns characterized with provocative injections (Dwyer)
Imaging is unremarkableConfirm suspicions with dx intra-
articular z-jt injections or medial branch blockade


DwyerZ-joint Referral Patterns Spine1990

FukuiThoracic Z-joint Referral Patterns
RegionalAnesthesia1997

Spinalcord
HNP
duraLig.flavum

“Annular fibers restrict axial rotation more than the facet joints.” (Krismer 1996)

Normal disc
Posterior Tearwith epiduralleak

Grubb, Kelly.Spine 25:1382-1389, 2000Cervical DiscographyPain Referral Patterns173 discograms, 404 positivediscs>50% with >3 positive discs
C2-3 C3-4C4-5
C5-6 C6-7

Provocative Cervical
Discography
Slipman NASS 2002
C2-3
C3-4
C4-5

C5-6
C6-7
C7-T1
Provocative Cervical
Discography
Slipman NASS 2002


Treatment - AcuteTreatment - Acute
Oral Steroids?NSAIDs?Immobilize?Early Therapy?

TreatmentTreatment
Facet Joints

Treatment of Facet InjuryTreatment of Facet Injury
Manual TherapyPostural EducationNeuromuscular Reeducation/Stability Cervical TractionSpinal InjectionsSurgical Stabilization

Manual TherapyManual Therapy
Grade 1: Small amplitude, beginning rangeGrade 2: Large amp, resistance freeGrade 3: Large amp into resistance (MET)Grade 4: Small amp well into resis (HVLA)Grade 5: Past end-range

Spinal Injection/Nerve Spinal Injection/Nerve AblationAblation
Intraarticular CorticosteroidFacet Denervation (Lord,et al; NEJM 1996;
335:1721-6)

Treatment of Disk DisordersTreatment of Disk Disorders
Posture/ Spine Stability TrainingCervical TractionTreat Assoc Muscle/Facet DisordersSpinal InjectionsSurgical (ACDF, other); Treatment for axial
neck pain?
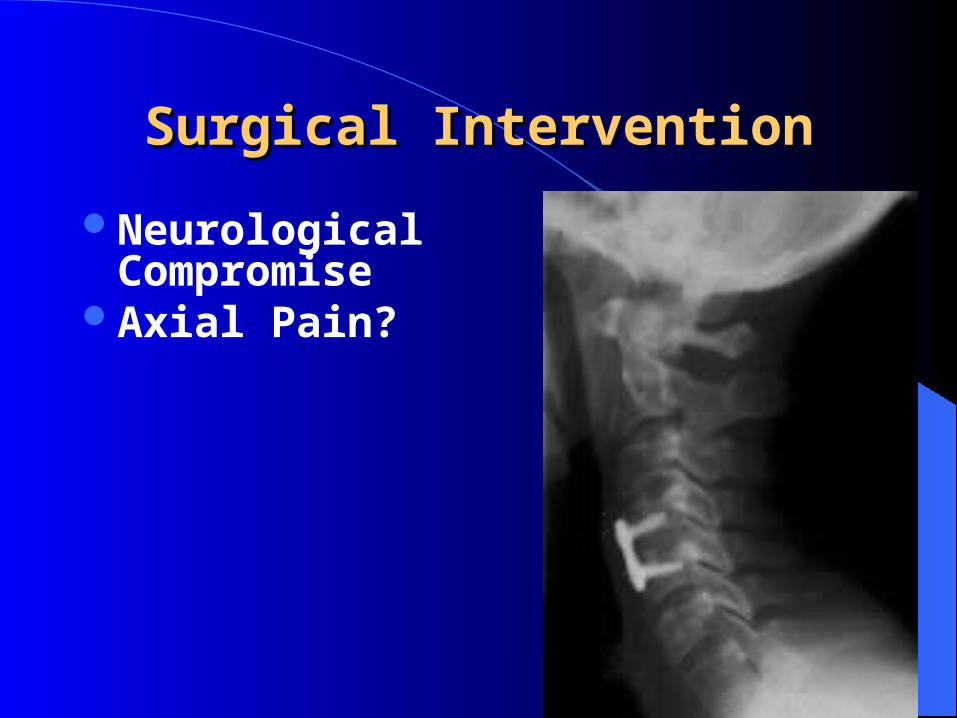
Surgical InterventionSurgical Intervention
Neurological Compromise
Axial Pain?
Treatment of Muscle Treatment of Muscle DisordersDisorders
Massage: CMT, self, theracanePostural EducNeuromuscular Reeducation/StabilityBiofeedbackTrigger Point Injections/AcupunctureBotulinum Toxin: Botox/Myoblock

Movement Movement Dysfunction Dysfunction
Dynamic StabilityDynamic Stabilityand Muscle Balanceand Muscle Balanceof the Cervical Spineof the Cervical Spine

Segmental Dysfunction

Movement DysfunctionMovement Dysfunction
pain patholog y
dysfunctio n
abnorm al stress or strain
uncontrolled m ovem en t
loss of local or global control

Local stability segmental Local stability segmental controlcontrol
The segmental stability of the spine is dependent on recruitment of the deep local stability muscles
The spine will fail if local activity is insufficient even if the global muscles work strongly
1 –3 % MVC muscle stiffness significantly increases stability
25% MVC = optimal stiffness & stability(Cholewicki & McGill 1996, Crisco & Panjabi 1991,
Hoffer & Andreasson 1981)

InhibitionInhibition
Inhibition: failure of normal recruitment– poor recruitment under low threshold stimulus– delayed recruitment timing– altered recruitment sequencing
Inhibition ‘off’

Afferent Input & Recruitment Afferent Input & Recruitment
Recruitment is partially due to the influence of proprioceptive activity
Proprioceptive afferent (γ loop) input is essential for tonic (low threshold) recruitment
Sensation of effort is linked to recruitment• (Eccles et al. 1957, Grimby & Hannerz 1976)

Proprioception and PathologyProprioception and Pathology
Whiplash patients have significant in ability to reposition head after movement– worse with mid range movement than end range – worse in direction of injury mechanism (flex/ext)
Kinesthetic accuracy improves with specific proprioceptive exercise
(Loudow et al 1997, Revel et al 1991 1994, Heikkla & Astrom 1996)
Evidence of Local DysfunctionEvidence of Local Dysfunction
Uncontrolled segmental translation
Segmental change within cross-sectional area
Altered pattern of low threshold recruitment
Motor recruitment timing deficit• (review: Comerford & Mottram 2001)

I.I. Control of NeutralControl of Neutrallow load recruitment in low load recruitment in
neutralneutral
Test for ability of anterior local stability muscles to control neutral (longus & RCAnt)

Deep cervical flexor Deep cervical flexor dysfunctiondysfunction
Control Can control greater
range of 2mm Hg increments (up to 28 from baseline of 20) than WAD
Less superficial muscle activity
WAD Can only control low
increments (from baseline of 20 up to 23)
Less consistent duration of hold
More superficial muscle activity
Jull 2000

Deep cervical flexor Deep cervical flexor dysfunctiondysfunction
identified in different pathological situations– Whiplash Associated Disorder (Jull 2000)
– Post-concussional headache (Treleaven et al 1994)
– Cervical headache (Watson & Trott 1993,Jull et al 1999)
– Mechanical neck pain (Silverman et al 1991, White & Sahrmann 1994, Jull 1998)

Dysfunction inDysfunction inGlobal Mobility SystemGlobal Mobility System
Myofascial shortening which limits physiological and / or accessory motion
Overactive low load or low threshold recruitment
Reacts to pain and pathology with spasm

Dysfunction related to Dysfunction related to pathologypathology
Normal Able to hold head flexed and maintain position
against light resistance
Cervical pain cervical lordosis Inability to hold head flexed in supine
– Lose position into chin poke & lordosis due to long weak longus cervicus that is compensated for by excessive scalenae and sterno-mastoid
• (White & Sahrmann 1994)
Relative Stiffness/Relative Relative Stiffness/Relative FlexibilityFlexibility
(Sahrmann 2002)
If 1 joint muscles lack ability to adequately shorten or are “weak” - they allow excessive motion
If 2 joint muscles lack extensibility or are overactive- they limit normal motion which must be compensated for elsewhere in the movement system
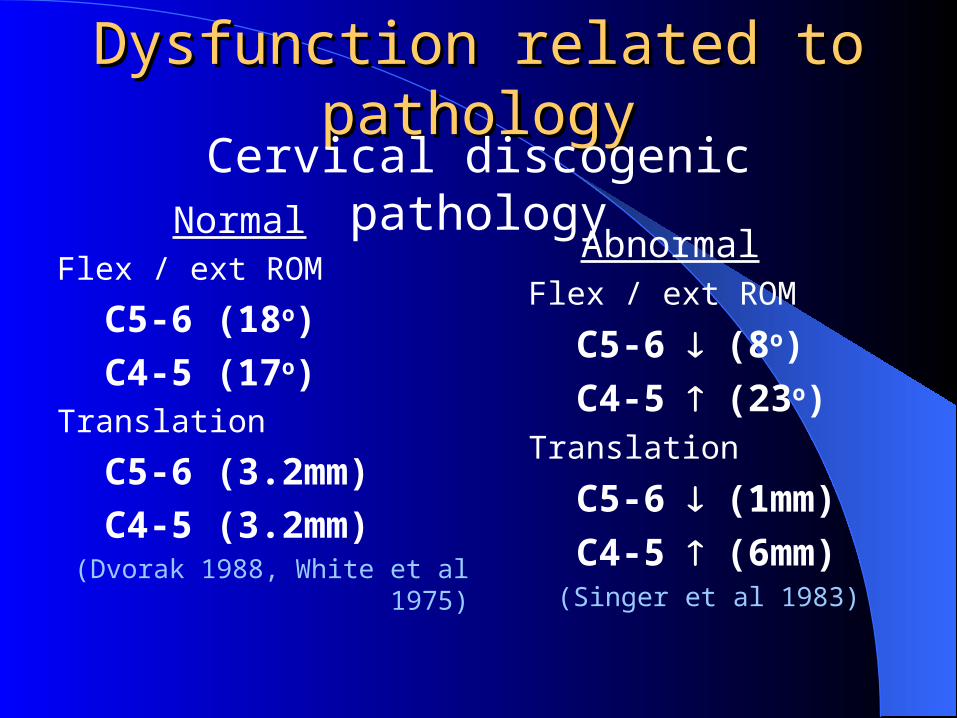
Dysfunction related to pathologyDysfunction related to pathology
NormalFlex / ext ROM
C5-6 (18o)
C4-5 (17o)Translation
C5-6 (3.2mm)
C4-5 (3.2mm)(Dvorak 1988, White et al 1975)
AbnormalFlex / ext ROM
C5-6 (8o)
C4-5 (23o)Translation
C5-6 (1mm)
C4-5 (6mm)(Singer et al 1983)
Cervical discogenic pathology

Treatment SummaryTreatment SummaryDual approach:
Treat the pathologyIdentify and correct the dynamic stability
dysfunction which may precipitate pathology Control of neutral by integration of local stabilisers
into global function Retrain dynamic control of the direction of
stability dysfunction (especially rotation) Retrain tonic, through range control of the global
stabilisers Actively regain extensibility of the global
mobilisers

‘‘Alternative’ ApproachesAlternative’ Approaches
Tai ChiAlexander techniqueYogaPilatesPhysio ball (Swiss ball)Feldenkrais
Treat Whole PersonTreat Whole Person
PsychologyWorkFamilySecondary Gain Dynamics


















