Which imaging technique should we use in the follow up of gynaecological cancer?
23
8 Which imaging technique should we use in the follow up of gynaecological cancer? Q14 Carla Antonia Testa a, * , Alessia Di Legge a , Bruna Virgilio a , Matteo Bonatti b , Riccardo Manfredi b , Mirk Paoletta c , Vittoria Rufini c a Department of Obstetrics and Gynaecology, Catholic University of the Sacred Heart, Rome, Italy b Department of Radiology, University of Verona, “G.B. Rossi” Hospital, Verona, Italy Q 1 c Institute of Nuclear Medicine, Catholic University of the Sacred Heart, Rome, Italy Keywords: gynaecological cancer recurrences imaging techniques ultrasound computed tomography magnetic resonance imaging positron emission tomography Follow-up routines after gynaecological cancer vary. The optimal approach is unknown, and no randomised-controlled trials comparing surveillance protocols have been published. In this chapter, we summarise the diagnostic performance of ultrasound, computed tomography, and magnetic resonance imaging in the follow up of women treated for ovarian or uterine cancers. Computed tomography is today the standard imaging method for the follow up of women treated for endometrial, cervical, or ovarian cancer. Six-monthly or annual follow-up examinations have not been shown to positively affect survival. Instead, a combination of transvaginal and transabdominal ultrasound examination with clinical examination might be a more cost-effective strategy for early detection of recurrence. Positron-emission tomography might play a role in women with clinical or serological suspicion of recurrence but without evidence of disease at conventional diag- nostic imaging. To create guidelines, more studies, preferably randomised-controlled trials, on follow-up strategies are needed. Ó 2014 Published by Elsevier Ltd. Introduction Despite continuing advances in surgical and non-surgical therapeutic strategies, gynaecological malignancies have a high probability (30–75%) of developing relapse and distant metastases after * Corresponding author. Tel.: þ39 (0) 630157252; Fax: þ39 (0) 630156332. Q 2 E-mail address: [email protected] (C.A. Testa). Contents lists available at ScienceDirect Best Practice & Research Clinical Obstetrics and Gynaecology journal homepage: www.elsevier.com/locate/bpobgyn 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008 1521-6934/Ó 2014 Published by Elsevier Ltd. Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 YBEOG1347_proof ■ 8 May 2014 ■ 1/23 Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the follow up of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http:// dx.doi.org/10.1016/j.bpobgyn.2014.04.008
Transcript of Which imaging technique should we use in the follow up of gynaecological cancer?

Q14
Q1
Q2
12345678910111213141516171819202122232425262728293031323334353637383940414243
Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23
YBEOG1347_proof ■ 8 May 2014 ■ 1/23
Contents lists available at ScienceDirect
Best Practice & Research ClinicalObstetrics and Gynaecology
journal homepage: www.elsevier .com/locate /bpobgyn
8
Which imaging technique should we use in thefollow up of gynaecological cancer?
Carla Antonia Testa a,*, Alessia Di Legge a, Bruna Virgilio a,Matteo Bonatti b, Riccardo Manfredi b, Mirk Paoletta c,Vittoria Rufini c
aDepartment of Obstetrics and Gynaecology, Catholic University of the Sacred Heart, Rome, ItalybDepartment of Radiology, University of Verona, “G.B. Rossi” Hospital, Verona, Italyc Institute of Nuclear Medicine, Catholic University of the Sacred Heart, Rome, Italy
Keywords:gynaecological cancer recurrencesimaging techniquesultrasoundcomputed tomographymagnetic resonance imagingpositron emission tomography
* Corresponding author. Tel.: þ39 (0) 630157252E-mail address: [email protected] (C.A.
http://dx.doi.org/10.1016/j.bpobgyn.2014.04.0081521-6934/� 2014 Published by Elsevier Ltd.
Please cite this article in press as: Testa CAup of gynaecological cancer?, Best Practicedx.doi.org/10.1016/j.bpobgyn.2014.04.008
Follow-up routines after gynaecological cancer vary. The optimalapproach is unknown, and no randomised-controlled trialscomparing surveillance protocols have been published. In thischapter, we summarise the diagnostic performance of ultrasound,computed tomography, and magnetic resonance imaging in thefollow up of women treated for ovarian or uterine cancers.Computed tomography is today the standard imaging method forthe follow up of women treated for endometrial, cervical, or ovariancancer. Six-monthly or annual follow-up examinations have notbeen shown to positively affect survival. Instead, a combination oftransvaginal and transabdominal ultrasound examination withclinical examination might be a more cost-effective strategy forearly detection of recurrence. Positron-emission tomographymightplay a role in women with clinical or serological suspicion ofrecurrence but without evidence of disease at conventional diag-nostic imaging. To create guidelines, more studies, preferablyrandomised-controlled trials, on follow-up strategies are needed.
� 2014 Published by Elsevier Ltd.
Introduction
Despite continuing advances in surgical and non-surgical therapeutic strategies, gynaecologicalmalignancies have a high probability (30–75%) of developing relapse and distant metastases after
; Fax: þ39 (0) 630156332.Testa).
, et al., Which imaging technique should we use in the follow& Research Clinical Obstetrics and Gynaecology (2014), http://

Q3
Q4
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–232
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 2/23
initial treatment [1]. In view of the low survival rate of women with recurrent disease, surveillanceprogrammes mainly aim at early detection of recurrence, the rationale for this being that earlierdiagnosis of relapse could be associated with lower morbidity and mortality rates. Other objectives ofroutine follow up are the identification of treatment complications and detection of second tumoursassociated with primary gynaecological cancer. How to best follow up women with gynaecologicalcancers is still unclear [2]. Published data indicate that 41–100% of all recurrences are detected throughsymptoms alone (i.e. the recurrence would have been detected regardless of follow-up strategy) [3,4].
The methods usually used for postoperative surveillance of women with gynaecological cancerinclude clinical history, pelvic examination, visual vaginal inspection with vaginal cytology, and serumtumour markers. Computed tomography, magnetic resonance imaging (MRI) and positron emissiontomography (PET) are also important tools in the follow up of gynaecological relapses [5,6]. Tumourmarkers have a limited role, because both benign gynaecological conditions and malignant non-gynaecological conditions may be associated with elevated levels of tumour markers. Moreover,elevated levels of tumour marker do not provide any information about the location of recurrence [7].Computed tomography, MRI, and positron emission tomography combined with computed tomogra-phy are too expensive to be proposed as first-line methods to detect recurrence, and they have a poorability to detect small lesions [8,9]. Surprisingly, scant data are available on the utility of trans-abdominal and transvaginal ultrasound examination in the follow up of women with gynaecologicalcancer. The wide availability and the low cost of ultrasound, as well as the rapidity of the examinationprocedure and the possibility of bed-side use of ultrasound, would justify its use for surveillance ofwomen treated for gynaecological cancer, provided that adequate diagnostic performance could bedemonstrated.
The most appropriate follow-up strategy for each type of gynaecological cancer is likely to dependon the natural history of the disease, the risk of recurrence, the most frequent site of relapse, and theappearance of the recurrent tumour at imaging (i.e. discrete solid or cystic lesions or diffusecarcinomatosis).
Ovarian cancer
Epithelial ovarian cancer is the most common cause of mortality among gynaecologic malignancies[10]. At diagnosis, most (75%) epithelial ovarian cancers have progressed to stage III or IV [11,12], and inwomen with this type of cancer, the 5-year survival rate is 15–20% [13]. Many factors are associatedwith poor prognosis (e.g. age at diagnosis younger than 50 years or 50 years or older), InternationalFederation of Gynaecology and Obstetrics (FIGO) stage, grade, histotype (serous or not serous), tumoursize, and CA125 levels at diagnosis [14]. The major determinants of outcome of these women are re-sidual tumour after the first cytoreductive surgery and platinum sensitivity [15].
Recurrent ovarian malignancy usually appears as a pelvic mass at the site of surgery or as diffuseperitoneal carcinomatosis, pleuropulmonary lesions, lymph node, or liver metastases. Frequently, re-lapses of ovarian cancer are associated with ascites or pleural effusion, and sometimes these are thefirst manifestations of recurrence. Pelvic relapse may involve the vaginal cuff, the parametria, thebladder, the ureters, bowel loops, or the rectum [16]. Ferrandina et al. [12] reported that diffuseabdominal carcinomatosis was the most common presentation of recurrence (62.1%). A single tumournodule or multiple tumour nodules were the first manifestation of recurrence in 9.9% and 26.7% ofwomen, respectively [12]. Ureteral obstruction may be caused by direct encasement of the ureter or bytumour infiltration of the bladder wall, which results in ureteral obstruction and hydronephrosis.Pelvic and para-aortic lymph nodes are also common sites of recurrence. Unusual sites of recurrenceare the spleen, gastrointestinal tract, skeleton musculo-cutaneous tissue, and central nervous system.
Cervical cancer
Cervical cancer is the second most common cancer worldwide in women, resulting in about275,000 deaths annually [17]. Primary treatment for cervical cancer (surgery or radiotherapy with orwithout chemotherapy) has a cure rate of 80–95% inwomen diagnosed with early stage disease (stage Ior II) and about 60% in women with stage III disease [18].
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 3
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 3/23
Surgico-pathologic factors that predict disease recurrence are FIGO stage, tumour volume, depth ofstromal invasion, lymph-vascular space invasion, parametrial extension at surgery or on histology,histologic type (e.g. small-cell cancer has poor prognosis), lymph-node involvement at surgery or onhistology, and status of the resection margins.
After radical surgery for early stage disease, metastases, when they occur, are typically distributedlocally (e.g. in the vaginal apex), regionally (e.g. in the pelvic sidewall), or distantly (e.g. in the lung). Ifprimary treatment involves pelvic radiation, the location of recurrences depends on the stage of thedisease at diagnosis, with a greater risk of persistent or recurrent pelvic disease in those with moreadvanced tumours [19]. The most common sites of distant recurrence are lung, para-aortic lymphnodes, abdominal cavity, and supraclavicular nodes [19]. About 90% of women who have distant re-currences will die of their disease within 5 years [20].
Several studies have focused on prognostic factors of relapse rather than on strategies for detectingrecurrence. The largest recently published study has shown that a surveillance programme based onroutine Pap smear and chest X-ray does not permit earlier detection of recurrence and does not im-proves survival [21].
Endometrial cancer
Endometrial carcinoma is the most common invasive malignancy of the female genital tract [22].Most womenwith the disease are diagnosed at FIGO stage I or II [2], have a good prognosis, and can becured with surgery. Women with advanced or recurrent disease have a worse prognosis, and resultsobtained with chemotherapy are far from impressive [23]. The risk of recurrence varies according towell-defined risk factors (e.g. grading, histotype, metastases to the ovaries, lymph-node metastasis,and degree of myometrial stroma infiltration), and ranges from 13–17% in large studies including allwomen with endometrial cancer [2].
The anatomic sites of endometrial cancer relapse are equally distributed between local (pelvic) anddistant (abdominal and chest) sites. Counselling on the symptoms of recurrence is extremely importantbecause most women with recurrences are symptomatic (i.e. vaginal bleeding, abdominal or pelvicpain, swelling of the legs, fever, and bowel obstruction) [24]. Most endometrial cancer recurrencesoccur within 3 years after the diagnosis of the primary tumour.
No rationale (e.g. examination accuracy, cost-effectiveness, or patient’s survival benefit) is availabletoday for any particular follow-up protocol in women with endometrial cancer [22]. Only physicalexamination, including pelvic-rectal examination, has shown some utility in detecting recurrence [22].
Uterine sarcoma
Leiomyosarcoma is the most frequent uterine sarcoma. It is an aggressive tumour with a tendencytowards early relapse. Survival for women with recurrent disease is poor. Endometrial stromal sar-coma, the second most common uterine sarcoma, is a more indolent malignancy, with a tendencytowards recurrence after a long latency period.
Because of the relative infrequency of both diseases, the study and standardisation of follow up andtreatment for recurrent disease is still under debate. In properly selected women, surgery and evenrepeated surgery for recurrent disease should be considered, because it improves survival [25]. Aprolonged disease-free interval and complete resection of disease are associated with better prognosisafter surgical resection of the recurrence [2].
Relapse of uterine sarcomas may be local or distant. In a study of 250 womenwith recurrent uterinesarcoma, the relapse was pelvic in 14% of cases, distant in 33%, and both pelvic and distant in 53% [26].Most distant relapses of uterine sarcomas involve the lungs and upper abdomen, whereas brain me-tastases are less common [26].
Ultrasound for follow up of women treated for gynaecological malignancy
In spite of major advances in the ultrasound technique (including colour Doppler and three-dimensional ultrasound), ultrasound is still not a standard method in the follow up of
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Q5
Q6
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–234
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 4/23
gynaecological malignancies. Only a few studies have investigated the ability of ultrasound to detectrecurrent disease. This is surprising considering the wide availability of ultrasound in gynaecologicdepartments where ultrasound could be routinely added to a clinical pelvic examination whenfollowing up women treated for neoplasms in the genital tract.
Ultrasound and detection of recurrence of gynaecological cancer
Pioneering studies [27,28] have shown a high accuracy for both transrectal (accuracy 90.5%) andtransvaginal (accuracy 91.6%, sensitivity 89.4%, specificity 100%) ultrasound for the detection of pelvicrecurrence of malignant disease. These results, however, are based on a small number of cases and amixture of ovarian and uterine neoplasms.
Transabdominal and transvaginal ultrasound examination was used to detect relapses in a pro-spective study by Testa et al. [29], who included women with previous ovarian, endometrial, cervicalcancer, or uterine sarcoma. This study included 385 women with recurrent gynaecological cancersubmitted to surgery. All the women enrolled were subjected to clinical examination, serum tumourmarker assay, transvaginal and transabdominal sonography, computed tomography scan, MRI, or both.The positive predictive value (PPV) of ultrasound was 100%, the negative predictive value (NPV) was92.7%. In the subgroup of women with positive clinical examination or abnormal tumour markers, thePPV of ultrasound was 100%, and the NPV was 22.2%. In women without clinical or serological signs oftumour recurrence, the PPV of ultrasound was 100% and the NPV was 99.6%. This prospective studyshowed that routine ultrasound examination may play a role in the follow up of gynaecologic ma-lignancies, especially among asymptomatic women. In women with clinical or serological signs ofrecurrence computed tomography might be better to localise the recurrence.
Ultrasound-guided biopsy of a lesion suspicious for malignancy is of great help if a recurrence ofcancer is suspected (Video 1).
Supplementary data related to this article can be found online at http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008.
Ultrasound appearance of recurrent gynaecological malignancy
The ultrasound appearance of abdominal and pelvic intraperitoneal recurrences of gynaecologicalmalignancies has been described as solid nodules vascularised at colour Doppler examination (Fig.1) oras carcinomatosis with miliariform or sheet-like patterns [30]. In a selected group of 27 women streated for gynaecological malignancy with small masses suspicious of being recurrent tumour locatedin the central pelvis, Doppler results differed significantly between malignant and benign lesions.
Fig. 1. Transvaginal ultrasound of a solitary recurrence of ovarian cancer located within the pelvis above the vaginal cuff. Therecurrence is solid and moderately vascularised at colour Doppler.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Q7
Fig. 2. Transvaginal ultrasound of a solitary recurrence of cervical cancer within the pelvis just above the vaginal cuff. It appears as(a) an inhomogeneous solid nodule at gray-scale ultrasound and (b) moderately vascularised at colour Doppler.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 5
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 5/23
Higher colour score (i.e. higher colour content at colour Doppler examination), lower resistance indexand higher peak systolic and time average maximum velocities in tumour vessels were found in ma-lignant compared with benign lesions [31]. In a study of 45 women with previous endometrial andcervical cancer, pelvic relapses were detected as a central pelvic lesion located on the vaginal apex in80% of cases; in 13% of cases the recurrencewas located at the pelvic side-wall and in 7% it occupied thewhole pelvis [31]. The lesions had diameters ranging from 1.0 to 6.8 cm. They appeared as a solidnodular mass in 98% of cases and as cystic mass in 2% of cases (Figs. 2 and 3). In 32 (71%) women, themass surrounding the bowel was hypoechogenic, whereas in 13 (29%), it showed inhomogeneousechotexture (Fig. 2). At colour and power Doppler examination, randomly dispersed blood vessels weredetected in all relapses (Fig. 2).
Ascites or a septated fluid collection is often found inwomenwith tumour recurrence, but may alsobe the only sonographic sign of recurrent disease, especially in women with recurrence of ovariancancer [29].
In a prospective study by Testa et al. [29] which included women with previous ovarian, endo-metrial, cervical cancer or uterine sarcoma, the recurrences appeared at ultrasound as a solitary lesionin 50.6% of women, and in 37% they were located centrally in the pelvis. Eighty-two per cent of therecurrences of ovarian cancer appeared as solid lesions. Recurrences of other gynaecological tumoursappeared as solid masses in 94% of cases.
Tumour nodules in the liver or spleen, paraaortic or visceral metastatic lymph nodes can bedetected with ultrasound as signs of gynaecological cancer recurrence [32]. Hydronephrosis can be anindirect sign of pelvic or retroperitoneal recurrent disease (Video 2).
Fig. 3. Transvaginal ultrasound of a solitary recurrence of ovarian cancer located within the pelvis between the bladder and therectum. It is a unilocular-solid cyst.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 4. Transvaginal ultrasound of a central pelvic recurrence of ovarian cancer with smooth borders. This recurrence might besuitable for surgical removal because it does not seem to infiltrate into surrounding tissue.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–236
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 6/23
Supplementary data related to this article can be found online at http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008.
Ultrasound examination can provide ‘dynamic’ information related to elasticity, mobility andtenderness of lesions suspected to be cancer recurrences. This helps to discriminate between benignand malignant lesions. A description of the lesions’ margins (smooth or irregularly infiltrating intosurrounding tissues) (Figs. 4 and 5) is important. It helps to plan optimal management for referral tochemotherapy, radiotherapy or surgery [33].
Computed tomography for follow up of women treated for gynaecological malignancy
Thanks to its wide availability, its time-effectiveness and its high spatial resolution, computed to-mography is the standard method for following up women who have been treated for gynaecological
Fig. 5. Transvaginal ultrasound of a central pelvic recurrence of endometrial cancer with irregular borders. This recurrence seems toinfiltrate surrounding tissue and might not be suitable for surgical removal.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Q8
Q9
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 7
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 7/23
malignancies. The ability of computed tomography to assess accurately the extent of tumour inwomenwith malignancies has increased after the introduction of thin section multi-detector scanners [34].Computed tomography can be used to investigate the woman’s whole body in less than 5 min: brainparenchyma, lung parenchyma, mediastinal structures, parenchymatous abdominal organs, the peri-toneum, retroperitoneal structures, and the skeleton can be examined for the presence of metastases.The main disadvantages of computed tomography are ionising radiation and the necessity to admin-ister intravenous iodinated contrast. Intravenous contrast is needed to increase tissue contrast reso-lution. Contrast, however, should be avoided in case of renal impairment, and may cause allergicreactions. Computed tomography is particularly useful for detecting distant recurrence of gynaeco-logical malignancies. It has limited ability to detect local recurrence.
Computed tomography and detection of recurrence
Computed tomography is themost frequently used imagingmethod for surveillance of women afterprimary treatment for ovarian cancer [6]. A largemeta-analysis [35] showed a pooled sensitivity of 79%and a pooled specificity of 84% for computed tomography for detection of recurrent ovarian cancer, andthe area under the receiver operating characteristic curve was 0.88. Another study [36], compared thecomputed tomography findings in 35womenwith clinical, laboratory signs of recurrent ovarian cancer,or both, with subsequent surgical data. It showed that computed tomography had a sensitivity of 58%and a specificity of 82% for identifying the precise abdominal sites of recurrence. The results of anotherstudy suggested that computed tomography can reliably predict tumour non-resectability in recurrentovarian cancer [37]. The main limitation of computed tomography for identifying recurrent ovariancancer is its poor ability to detect small peritoneal implants. The reported sensitivity of computedtomography for detecting peritoneal implants smaller than 1 cm varies from 25–50% [6,10]. It can beimproved, however, by administration of a negative oral contrast medium, in addition to the intra-venous one, to distend bowel loops and so increase the conspicuousness of solid implants [6,38].
Computed tomography is often considered the imaging modality of choice for the follow up ofwomen treated for cervical and endometrial cancer [39–41]. No reliable data on its sensitivity andspecificity in detecting recurrent cervical or endometrial cancer have recently been published.Encouraging results about the use of computed tomography for the detection of recurrent uterinecancer were published in 1989 (e.g. accuracy, specificity and sensitivity 92%, 80% and 92%, respectively).The main limits of computed tomography in the surveillance of women treated for endometrial andcervical cancer is its poor performance in identifying local recurrence. Use of computed tomographymakes it difficult to discriminate between postoperative and post-radiotherapy fibrosis and localtumour recurrence.
Computed tomography and morphological appearance of recurrence
Brain metastases are rare in gynaecologic malignancies, and are usually clinically suspected becauseof neurological symptoms [41]. Brainmetastases are usually located at thewhite–graymatter interface.In most cases, they are isodense to brain parenchyma in scans carried out before contrast injection.After contrast injection, they show variable patterns of enhancement as a consequence of blood–brainbarrier damage. Hypodensity of the adjacent white matter, representing hypoxic oedema, is usuallypresent.
Pleural effusion is the most common manifestation of thoracic involvement by ovarian cancerrelapse, and can be easily identified at computed tomography as the presence of hypodense (about0 Hounsfield Units) material occupying the dependent portion of the pleural cavity (Fig. 6). Solidpleural nodules or pleural thickenings may also be present. Pulmonary parenchyma involvement isseen as rounded solid nodules, variable in size, and usually located at the tip of vascular structures inthe dependent pulmonary regions. Calcifications may be present if the primary tumour is a serousovarian carcinoma. Enlarged round lymph nodes with loss of their fatty hilum indicates mediastinalinvolvement (Fig. 6). A less common pattern of thoracic involvement is lymphangitic carcinomatosis,resulting in irregular, nodular thickening of pulmonary parenchyma interstitial septae.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 6. Computed tomography of pleural and nodal recurrence of ovarian cancer. This axial computed tomography image (multi-planar reconstruction, 3 mm thick), acquired during the portal venous phase of the dynamic study, shows abundant right pleuraleffusion (star) in a patient follow up for ovarian carcinoma with suspicion of tumour recurrence. Moreover, a pathologically enlargedlymph node (arrow) can be seen in the right cardio-phrenic recess.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–238
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 8/23
Liver metastases are barely recognisable at computed tomography before contrast injection. In theportal venous phase after contrast administration, they appear hypodense compared with the liverparenchyma. Metastases from mucinous ovarian tumours usually appear markedly hypodense beforecontrast injection, and show a progressive peripheral rim enhancement after contrast injection. Cal-cifications may be present in liver metastases from serous ovarian carcinomas. Spleen, kidney,pancreas, and adrenal metastases are rare but can be detected at computed tomography.
Lymph-node metastases must be suspected in cases of enlarged rounded lymph nodes (more than1 cm in minimum diameter) with a loss of their fatty hilum (Fig. 7). A hypodense area (about 0–20 Hounsfield Units) representing necrosis in a lymph node has a positive predictive value of 100% formetastasis. Computed tomography cannot detect micrometastases in lymph nodes.
Peritoneal implants are seen as solid ill-defined areas of soft-tissue thickening, variable in size(Fig. 8), adhering to the peritoneal surface. They are predominantly or completely hypodense. Cysticmasses may also be seen, particularly in cases of mucinous neoplasms. Contrast administration iscrucial to detect peritoneal carcinomatosis. Implants usually enhance and become conspicuous afterintravenous contrast injection. Peritoneal implants may show calcifications, particularly in cases ofserous cystadenocarcinoma. Implants growing on the diaphragmatic peritoneum may result in scal-loping of the liver contour. They appear hypodense compared with the liver parenchyma (Fig. 8).Peritoneal implants may envelop bowel loops, infiltrate bowel walls, or both. This may result in bowelobstruction. Multiple coalescent carcinomatosis nodules involving the greater omentum may result inan ‘omental cake’. Ascites co-exists with peritoneal carcinomatosis in most cases. If ascites is detected,peritoneal nodules must be carefully searched for.
At computed tomography, pelvic recurrences are usually seen as ill-defined solid masses with avariable degree of contrast enhancement (Fig. 9), possibly with hypodense (0–20 Hounsfield Units)necrotic parts. Sometimes pelvic recurrences appear predominantly cystic with only minimal soft-tissue components. Central pelvic recurrences may extend to the ureters and the bladder wall, pos-teriorly to the rectum, or laterally to the pelvic sidewalls. Large pelvic recurrences can be easilyidentified at computed tomography, in particular if they involve adjacent structures. Small recurrencesoften remain undiagnosed because of the low tissue contrast resolution of computed tomography.Moreover, at computed tomography, the differentiation between recurrence and post-operative, post-radiotherapy fibrosis, or both, is extremely challenging.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 7. Computed tomography of recurrence of endometrial carcinoma in a lymph node. This coronal computed tomography image(multiplanar reconstruction, 4 mm thick), acquired during the portal venous phase of the dynamic study, shows the presence of apathologically enlarged lymph node (arrow) along the left common iliac vessels, adjacent to a surgical clip (arrowhead), in a patientpreviously operated on for endometrial carcinoma. The lymph node compresses the left ureter and this results in upstreamhydronephrosis (star).
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 9
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 9/23
Magnetic resonance imaging for the follow up of women treated for gynaecological malignancy
Nowadays, magnetic resonance scanners are widely available in developed countries. High-fieldmagnets associated with phase arrayed body coils and fast impulse sequences makes it possible toobtain high-quality images with high-tissue contrast and spatial resolution in relatively short scanningtimes. Moreover, the introduction of advanced MRI techniques, such as diffusion weighted imaging(DWI) and perfusion imaging, allows visualisation of macroscopic disease and also information ontissue cellularity and vascularisation. Themain limitations of MRI are high cost and the need for patientcooperation; indeed, the patient must lie completely still during all the examination, and, when
Fig. 8. Computed tomography of peritoneal recurrence of ovarian cancer. On these sagittal (a) and coronal (b) computed tomog-raphy images (multiplanar reconstruction, 1 and 3 mm thick, respectively) acquired during the portal venous phase of the dynamicstudy, discrete solid masses, representing peritoneal carcinomatosis (stars), can be seen along the greater omentum (a, b) and alongthe diaphragmatic peritoneum (b). In figure (a), many tiny nodules can be seen within the mesentery (arrows) representingmesenteric involvement, whereas in (b) peritoneal carcinomatosis infiltrates liver parenchyma (arrowheads). This results in scal-loping of the liver contour.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 9. Computed tomography images of pelvic recurrences of gynaecological malignancies. (a) The recurrence (star) is a small, welldefined nodule located on the vaginal vault in the midline in a woman previously operated on for cervical carcinoma; (b) therecurrence (star) is a solid mass with ill-defined margins and growth towards the rectum in a patient previously treated with surgeryand radiation for cervical carcinoma; and (c) the pelvic recurrence is bilateral (stars) and on the left side results in obstruction of theureter (arrows) in a woman operated on for ovarian cancer.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–2310
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 10/23
imaging the upper abdomen, she must be able to keep her breath for 20–25 s. Moreover, because of itssmall field of view, MRI is usually carried out only for the study of well-defined anatomical regions (e.g.the pelvis or the upper abdomen). Modern MRI scanners allow so-called ‘whole-body’ examinations,but these examinations are extremely time-consuming. Therefore, they are not routinely carried out ifthe woman can undergo a less time- and resource-consuming examination, such as computedtomography.
Magnetic resonance and detection of recurrence
In women treated for gynaecologic malignancies the two main indications for MRI are suspicion ofpelvic recurrence and peritoneal carcinomatosis. In 1993, Prayer et al. [42] demonstrated the superi-ority of MRI over computed tomography in detecting recurrent ovarian cancer (sensitivity of MRI 77.7%,specificity 93.3%; sensitivity of computed tomography 67.7%, specificity 93.3%). In 1996, Outwater et al.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 11
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 11/23
[43] reported that MRI had a sensitivity of 69% and a specificity of 94% in detecting recurrence ofovarian cancer (detection rate 35% for lesions of smaller than 2 cm and 82% for lesions larger than2 cm). A study published by Low et al. in 1997 [38] showed that Gadolinium-enhanced MRI might beextremely useful in identifying peritoneal recurrence of ovarian carcinoma (sensitivity, specificity andaccuracy values 91%, 87% and 90%, respectively). Kim et al. [44], confirmed the previously reportedencouraging results (sensitivity, specificity and accuracy 91%, 86% and 89%, respectively) identifyingrecurrent ovarian cancer.
Thanks to its ability to create images with excellent anatomical detail and to accurately delineatevaginal structures and pelvic floor muscles, MRI is considered by some to be the imaging modality ofchoice for the detection of recurrent cervical and endometrial cancer [40]. It was reported to detectbladder and rectum involvement by pelvic recurrences of uterine cancers with a sensitivity of 83% anda specificity of 100% [45].
Magnetic resonance and morphological appearance of recurrence
In women surgically treated for primary gynaecological cancer, central pelvic recurrence isusually seen as an ill-defined solid mass located on the top of the vaginal cuff between the bladderand the rectum. It is often best depicted on axial and sagittal scanning planes. Pelvic recurrenceusually shows intermediate signal intensity on T1-weighted images and heterogeneous hyper-intensity on T2-weighted images (Figs. 10–12) [46]. T2-hyperintensity is crucial for differentiatingrecurrence from post-treatment fibrosis, the latter usually appearing hypointense on T2-weightedimages. This differentiation, however, may be difficult in the first 6 months after radiotherapy,when T2-hyperintensity might be present because of inflammation and oedema. Areas of necrosis,appearing as markedly hyperintense foci on T2-weighted images, may be present within a solidrecurrence. In other cases, a recurrence may appear prevalently cystic with only some peripheralsolid mural thickenings (Fig. 11). After contrast administration, pelvic recurrence may show variabledegrees of enhancement, usually more marked in the peripheral portions of the mass (Fig. 10). Incase of cystic recurrences, contrast enhancement may be seen in cyst walls and mural thickenings(Fig. 11). Dynamic contrast-enhanced T1-weighted sequences may be helpful in the distinction be-tween tumour recurrence and fibrosis (sensitivity 91%, specificity 67%) [47]. Diffusion weightedsequences are useful for highlighting pelvic recurrence. Pelvic recurrences usually appear hyperin-tense on high b-value images and hypointense on apparent diffusion coefficient maps (Figs. 11 and12). This is because of their high cellularity (cystic lesions being the exception) (Fig. 12). The com-bination of DWI with T2-weighted images has a diagnostic performance similar to that of thecombination of contrast-enhanced T1-weighted images with T2-weighted images in the detection ofpelvic recurrence [47,48].
Involvement of adjacent organs by central pelvic recurrence is easily depicted onMRI. The finding ofa T2- and T1-hyperintense fatty plane between the neoplastic tissue and the adjacent structures ex-cludes the presence of infiltration. Infiltration must be suspected if the fatty plane is not clearly rec-ognisable. It is certainly present in case of a loss of the physiological hypointensity of the bladder wallor intestinal wall on T2-weighted images (Figs. 11 and 12). In more advanced cases, discrete T2-hyperintense tumour tissue can be seen within the rectal or bladder wall or protruding into their lu-mens. Fistulae between vagina, bladder and rectum can also be recognised at MRI. Fistulous tracts areseen as thin irregular T2-hyperintense/T1-hypointense lines if they contain fluid. They appear mark-edly hypointense both on T1- and T2-weighted images if they are filled with air. After contrastadministration, the walls of fistulas usually show significant contrast enhancement. If a fistula involvesthe bladder, T1- and T2-hypointense spots representing air bubbles are usually recognisable in theupper part of the bladder.
Tumour involvement of the pelvic sidewalls may be an isolated finding of tumour recurrence ormaybe the result of a direct continuation of a central pelvic recurrence. As the T2-hyperintense soft tissuemass infiltrates pelvic sidewalls, it causes a loss of the physiologic fatty cleavage plane and a change inthe signal intensity in the physiologically hypointense pelvic muscles. Bone infiltration is bestappreciated on fat-saturated T2-weighted images where tumour infiltration appears hyperintense, andon T1-weighted images where tumour infiltration appears hypointense compared with the
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 10. Magnetic resonance images of pelvic recurrence of cervical cancer. Axial turbo spin-echo T2-weighted images without (a)and with (b) fat-saturation show a heterogeneously hyperintense ill-defined solid mass (star) located on the top of vaginal cuff,representing tumour recurrence. On apparent diffusion coefficient map (c) the lesion appears markedly hypointense indicating highcellularity, and after intravenous contrast injection (d) it shows heterogeneous enhancement. The mass adheres to the sigmoid colon(arrow) that shows a complete loss of the physiological hypointensity of its walls indicating infiltration.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–2312
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 12/23
hyperintense fatty bone marrow. Ureteral involvement causes a fluid distention of the upstream ureterthat appears markedly hyperintense on T2-weighted images.
In women who have not undergone hysterectomy for cervical cancer, tumour recurrence, but alsoradiation fibrosis, may obstruct the cervical orifice resulting in hydrometra. OnMRI, the uterus appearsenlarged, and fluid secretions that appear hyperintense on T2-weighted images distend the endo-metrial cavity. On T1-weighted images, these secretions may show different signal intensitiesdepending on their protein content: hypointense in case of low protein content, very hyperintense incase of protein-rich fluid. Endometrial fluid does not show contrast enhancement nor diffusion coef-ficient restriction.
The ability of MRI to detect lymph-node metastases is limited. This is because detection relies onrounded shape and size (shortest diameter > 1 cm). It cannot detect micrometastases in normal-sizednodes. The identification of a markedly T2-hyperintense area, representing necrosis, within a pelviclymph node in a woman with a history of gynaecologic malignancy is virtually pathognomonic formetastasis. Necrotic lymph-node metastases, however, are quite uncommon: 17–27% in womenaffected by recurrent cervical cancer [49].
Peritoneal involvement can be accurately evaluated bymeans of MRI, with a sensitivity of 86% and aspecificity of 100%, according to Kim et al. [44] T2-weighted images are useful because of their high
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008
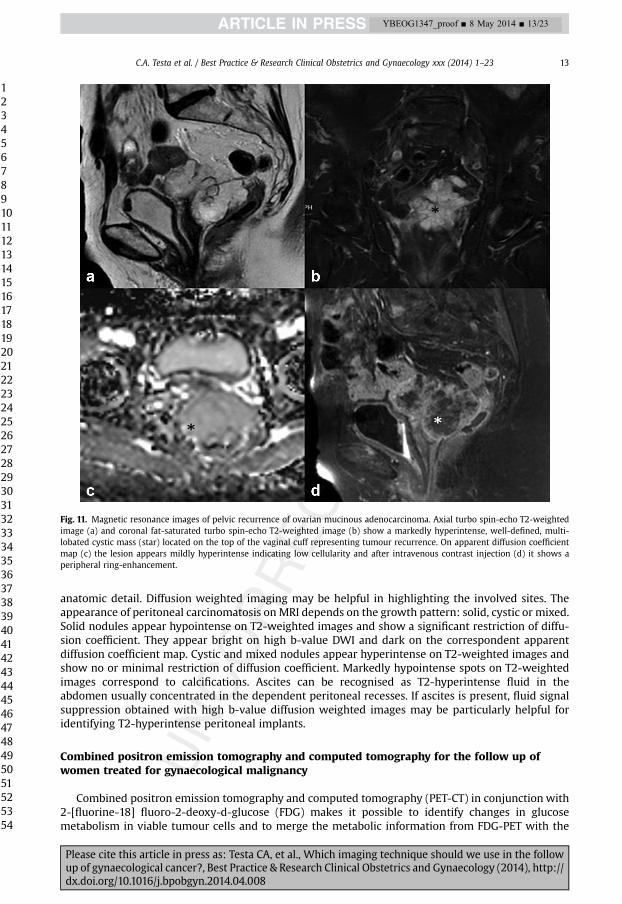
Fig. 11. Magnetic resonance images of pelvic recurrence of ovarian mucinous adenocarcinoma. Axial turbo spin-echo T2-weightedimage (a) and coronal fat-saturated turbo spin-echo T2-weighted image (b) show a markedly hyperintense, well-defined, multi-lobated cystic mass (star) located on the top of the vaginal cuff representing tumour recurrence. On apparent diffusion coefficientmap (c) the lesion appears mildly hyperintense indicating low cellularity and after intravenous contrast injection (d) it shows aperipheral ring-enhancement.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 13
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 13/23
anatomic detail. Diffusion weighted imaging may be helpful in highlighting the involved sites. Theappearance of peritoneal carcinomatosis on MRI depends on the growth pattern: solid, cystic or mixed.Solid nodules appear hypointense on T2-weighted images and show a significant restriction of diffu-sion coefficient. They appear bright on high b-value DWI and dark on the correspondent apparentdiffusion coefficient map. Cystic and mixed nodules appear hyperintense on T2-weighted images andshow no or minimal restriction of diffusion coefficient. Markedly hypointense spots on T2-weightedimages correspond to calcifications. Ascites can be recognised as T2-hyperintense fluid in theabdomen usually concentrated in the dependent peritoneal recesses. If ascites is present, fluid signalsuppression obtained with high b-value diffusion weighted images may be particularly helpful foridentifying T2-hyperintense peritoneal implants.
Combined positron emission tomography and computed tomography for the follow up ofwomen treated for gynaecological malignancy
Combined positron emission tomography and computed tomography (PET-CT) in conjunction with2-[fluorine-18] fluoro-2-deoxy-d-glucose (FDG) makes it possible to identify changes in glucosemetabolism in viable tumour cells and to merge the metabolic information from FDG-PET with the
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 12. Magnetic resonance images of pelvic recurrence of cervical carcinoma. Axial (a) and coronal (b) T2-weighted turbo spin-echo images show two ill-defined solid masses (stars) located laterally in the pelvis. The masses appear hypointense on apparentdiffusion coefficient map (c) indicating high cellularity, and show inhomogeneous contrast enhancement (d). The right mass in-filtrates an ileal loop (arrowheads), the left one infiltrates the left external iliac artery (arrow).
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–2314
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 14/23
anatomical information from computed tomography. Combined PET-CT is now established as a usefultechnique to detect local and distant recurrence (including lymph node metastases and peritonealinvolvement) of gynaecological cancers.
On PET-CT, recurrences are easily detected as abnormal areas of elevated FDG accumulation relativeto surrounding normal tissues. When evaluating gynaecological tumours, however, there are pitfalls[50,51]. These include misinterpretation of normal physiologic activity in bowel loops and bloodvessels, FDG activity in ureters and urinary bladder, and FDG activity in granulomatous tissue andactive inflammation (e.g. in regions previously treated with surgery or radiation). In addition, PET-CThas low spatial resolution (compared with other imaging techniques) and cannot detect small lesions(e.g. tiny recurrences or peritoneal implants, small metastatic lymph nodes). This is because a certainvolume of malignant tissue must be present to change the glucose metabolism. Because of theselimitations, special attention must be paid to proper patient preparation and scanning protocol.Bladder catheterisation and administration of diuretics may be needed. A standard PET-CT is carriedout 1 h after injection of FDG. Delayed imaging with an additional scan 3 h after FDG injection (so-called ‘Dual phase’ PET) has been suggested on regions suspicious for relapse to better distinguishbenign from malignant lesions [50,52].
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 15
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 15/23
Although in most institutions PET-CT is performed as a low-dose unenhanced computed tomog-raphy, the combination of PET with intravenous contrast injection and high-resolution computed to-mography (contrast-enhanced PET and computed tomography, PET and contrast enhanced computedtomography) has proven useful for increasing the accuracy of detecting recurrences in women withprevious ovarian or uterine tumours [53,54].
Whole-body magnetic resonance imaging positron emission tomography (MRI-PET) systems havebeen developed, but their diagnostic value is still under investigation. Nevertheless, the retrospectiveimage fusion of PET and MRI images, separately obtained from different scanners, might be more ac-curate than PET and contrast enhanced computed tomography or pelvic contrast-enhanced MRI indetecting recurrences of gynaecological malignancies, and may improve the diagnostic confidence ofreaders of the images [55,56].
Combined positron emission tomography and computed tomography for the detection of recurrence
Ovarian cancerSeveral studies have investigated the value of PET-CT in post-treatment surveillance of womenwith
ovarian cancer (Figs. 13–15). The reported diagnostic accuracy of PET-CT varies depending on thetechnique used (e.g. PET only or combined PET-CT; patient-based or lesion-based analysis). Moststudies report that 18F-FDG PET-CT has high accuracy in the detection of recurrent ovarian cancer: thereported sensitivity varies from 82–98.3%, the specificity from 55.6–100%, and the accuracy from 78.6–96.8% [57–63]. When PET-contrast enhanced computed tomography and PET-non-contrast-enhancedcomputed tomography were compared, sensitivity, specificity, and accuracy differed significantly, withhighest values for PET-contrast enhanced computed tomography (86.9% v 78.3%, 95.9% v 95.0%, and92.5% v 88.3%) [53]. A meta-analysis by Limei et al. [64] including 29 studies involving 1651 womenwith ovarian cancer, found pooled sensitivity and specificity for PET-CT to be 88.6% and 90.3% fordetecting recurrence of ovarian cancer [64].
Improved detection of recurrences on PET-CT can change patient management in a substantialnumber of cases. Tumour relapse was detected on PET-CT in a higher percentage of women than oncomputed tomography, and larger number of lesions were identified [59]. When PET-CT informationwas added to conventional follow-up findings, the clinical management changed in 24.7–60% of allcases [59,65–68].
In asymptomatic women suspected of ovarian cancer, FDG-PET-CT seems to be most useful becauseof increased serum levels of CA-125 antigen but negative or equivocal results of other imagingmethods. It also seems useful in women with normal cancer antigen levels but clinical symptomssuggestive of cancer recurrence [65,69–71]. Under such circumstances PET-CT had a sensitivity fordetecting intraperitoneal and retroperitoneal metastases of 93.9% and a specificity of 92.9% [69].Similar values for sensitivity and specificity were found in a meta-analysis by Havrilesky et al. [70](pooled sensitivity and specificity of PET 96% and 80%), suggesting that PET-CT has fair sensitivity todetect recurrence in women with rising CA-125 levels and normal results of conventional imaging. Itseems that active disease can be detected by PET-CT at relatively low levels of CA125, thereby facili-tating early diagnosis of recurrence [71].
Unsuspected disease in surgically inaccessible areas may be revealed by PET scans, thus changingpatient management (e.g. from surgery to chemotherapy).
Cervical cancerThe use of PET-CT in the follow up of women treated for cervical cancer is increasing (Figs. 16 and
17). The overall reported sensitivity, specificity, and accuracy in diagnosing recurrent disease is 90.3–94.7%, 81.0–92.6%, and 86.5–92.3%, respectively [59,67]. In the meta-analysis by Havrilesky et al.[70], including 25 studies (15 studies on cervical cancer, 10 studies on ovarian cancer), the pooledsensitivity and specificity of PET for detecting recurrent cervical cancer were 96% (87–99%, 95% CI)and 81% (58–94%). This is fair evidence that PET is useful for the diagnosis of recurrent cervicalcancer [70].
By carrying out a delayed PET imaging with the dual-phase technique, especially in equivocal cases,the accuracy of PET-CT in identifyingmetastatic lesions is increased, with diagnostic results reported as
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 13. Positron emission tomography and computed tomography image (PET-CT) of peritoneal carcinomatosis from recurrentovarian carcinoma. (a) Axial low-dose computed tomography image of the upper abdomen shows nodular areas of soft tissuedensity, with typical scalloping of the liver surface, as well as diffuse slight thickening along the liver capsule; (b) axial fused PET-CTimage shows multiple peri-hepatic areas of intense uptake (yellow) caused by peritoneal carcinosis; similar findings, with mildincrease of metabolic FDG uptake (orange), are seen along the caudate lobe and splenic hilum; (c) axial low dose computed to-mography image of the right iliac fossa shows asymmetric thickening of the lateral aspect of the ascending colon and a solid nodulewithin the peri-colic fat tissue, as well as an ill-defined area of increased density of fat tissue medial to the left iliac vessels. Axialfused PET-CT image corresponding to (c) shows focal areas of increased FDG uptake due to neoplastic involvement of the bowel andneoplastic nodules in mesenteric fat (d). Both in (a) and (c) nodular recurrences have been marked by superimposed light browncolour.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–2316
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 16/23
significantly superior to those of computed tomography and or MRI (sensitivity: 92% v 60%), withconsequent changes in treatment owing to PET findings in 55% of women [52]. The management of asignificant number of women with suspicion of relapse of cervical cancer can change on the basis ofPET-CT (up to 24.3%) [57,69]. A challenging situation occurs when serum squamous cell carcinomaantigen levels are increased but there are no detectable recurrent lesions on conventional imaging. In astudy by Unger et al. [75], recurrent disease was detected by PET in 66.7% of symptomatic women andin 30.8% of asymptomatic women. The PET scan had a sensitivity of 80.0% and a specificity of 100% indetecting recurrent cervix cancer in asymptomatic women. The corresponding figures in symptomaticwomen were 100% and 85.7%. In the study by Ryu et al. [76], the sensitivity of PET was high in iden-tifying recurrent cervix cancer in mediastinal, pulmonary hilum, and scalene lymph nodes, spine, andliver. The sensitivity, however, was relatively low in detecting recurrences in the lung, retrovesicallymph nodes, and para-aortic lymph nodes.
Endometrial cancerThe role of PET-CT in women suspected of having recurrence of endometrial carcinoma is not well
defined (Fig. 18). In women with primary stage III/IV endometrial cancer or suspicious or documented
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 14. Positron emission tomography and computed tomography (PET-CT) image of peritoneal carcinomatosis with involvement ofMorison’s pouch from recurrent ovarian carcinoma. (a) Axial low-dose computed tomography image of the upper abdomen showshypodense plaque-like thickening of the posterior aspect of the right liver lobe; (b) axial fused PET–CT image corresponding to (a)shows increased FDG uptake due to hypermetabolic tissue over the liver capsule; (c) sagittal low-dose CT and fused PET-CT images(d) show a linear pattern of increased uptake due to neoplastic diffusion along the posterior surface of the right liver lobe. In thefigures the increased uptake is seen as orange colour and it is marked by stars.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 17
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 17/23
recurrent endometrial cancer, the sensitivity of PETalone or FDG-PET plus MRI, computed tomography,or both, was significantly higher than that of MRI, computed tomography, or both, in detecting ma-lignant lesions [77]. In women with suspected endometrial cancer recurrence, patient-based analysisshowed that the sensitivity, specificity, and accuracy of PET-CT were all 93% [54]. On lesion analysis,PET-CT revealed only one false negative case (a missed para-aortic lymph-node metastasis measuring6 mm) and one false-positive case (a dorsal vertebral bone with degenerative changes) [54].
Uterine sarcomaBecause of the low incidence of uterine sarcomas, data on the diagnostic accuracy and clinical effect
of PET or PET-CT in the post-treatment surveillance of these tumours are limited. Metastatic diseasecan be demonstrated by PET as lesions involving mainly lungs and peritoneum, and less frequentlyliver, pancreas and breast. Published studies [78–80] agree that PET or PET-CT are highly effective indiscriminating true recurrence from benign lesions in women with suspicious findings on computedtomography, and highly sensitive in detecting recurrence in asymptomatic women undergoing followup after treatment for uterine sarcoma (sensitivity, specificity, and accuracy for PET or PET-CT: 92.9%,100%, 94.4% in women with suspected recurrence; 87.5%, 95.5%, 93.3% in women who are asymp-tomatic) [78].
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 15. Positron emission tomography and computed tomography (PET-CT) image of recurrence of ovarian cancer in lymph nodesand peritoneum. (a) Axial low-dose computed tomography image of the abdomen at the level of the kidneys shows left infra-renalpara-aortic lymphadenopathy (largest axial diameter 2 cm); (b) fused FDG-PET-CT image corresponding to (a) shows increased FDGuptake due to metastatic disease (the increased uptake is seen as orange colour and is marked with stars) (b); (b) axial low-dosecomputed tomography image shows ill-defined solid tissue in the pelvis, that is difficult to distinguish from the gastrointestinaltract; (d) fused PET-CT image corresponding to (c) shows multiple areas of increased tracer uptake in the pelvis close to a surgicalclip indicating the place of previous lymphadenectomy on the right and along the parietal peritoneum on the left due to neoplasticinvolvement of the pelvic peritoneum.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–2318
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 18/23
Combined positron emission tomography and computed tomography and morphological appearance ofrecurrence
Intraperitoneal recurrences and peritoneal implants can show varying patterns of FDG uptake onPET-CT (e.g. single nodular, multiple nodular, diffuse, and mixed FDG uptakes) within the pelvis, alongthe small and large bowel, the abdominal walls, or within the mesentery [81] (Figs. 13–15). Liversurface implants are crescent shaped, with characteristic scalloping of adjacent liver parenchyma onsimultaneous computed tomography (Fig. 13). They may also have an infiltrative growth and bedifficult to distinguish from true parenchymal metastases [35]. Early detection of liver metastases onPET-CT is limited by the physiological metabolic activity of normal liver tissue, in particular it is difficultto identify small lesions. Small metastatic lesions in lung and bone may also not be visible on PET [72].
PET-CT studies have shown that lymph nodes are a frequent site of relapse of cancer, often withsupradiaphragmatic involvement [58]. In the detection of paraaortic lymph node metastases, PET-CThas similar or better accuracy than computed tomography alone [57,70] (Figs. 15 and 16). DelayedPET scanning seems especially useful to detect malignant lymph nodes [82]. It seems that PET-CT has ahigh positive predictive value for identifying recurrent disease in retroperitoneal lymph nodes whenconventional computed tomography findings are negative or equivocal (i.e. in normal-sized nodes)[69]. It cannot, however, detect microscopic disease.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 16. Positron emission tomography and computed tomography (PET-CT) image of diffuse lymph node involvement fromrecurrent cervical carcinoma. Coronal (a) low-dose computed tomography of the abdomen shows large confluent retroperitoneallymphadenopathies extending from the iliac vessels up to the renal vessels; (b) corresponding axial fused PET–CT scan showsincreased uptake caused by metastatic lymph nodes (para-caval, para-aortic, inter-aorto-caval chains). In the figures the increaseduptake is seen as orange colour and in some areas as white colour indicating very high uptake.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 19
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 19/23
Comparison of different imaging modalities in the follow up of gynaecological cancer
It is still unclear which imaging technique should be used in the follow up of women with gynae-cological cancer, and no standardized strategies are available for universal adoption in clinical practice.
PET and contrast enhanced computed tomography seems to be the most accurate diagnosticmethod to detect relapses owing to its ability to merge metabolic and anatomical information and toprovide a whole body assessment.
In particular, in the presence of symptoms or elevated tumour markers, PET-CT (or PET and contrastenhanced CT) should be the diagnostic test to be recommended for patients in whom computed to-mography or MRI have failed to detect a recurrent lesion. It is unclear whether one should sidestepMRIand computed tomography and directly perform PET-CT. In some women, MRI or computed tomog-raphy, which are much cheaper than PET-CT, can demonstrate distant metastases or disseminatedrecurrent disease not suitable for surgery.
Fig. 17. Positron emission tomography and computed tomography (PET-CT) image of vaginal recurrence from cervical carcinoma.Axial fused PET-CT scan corresponding to (a) shows a small area of increased uptake due to vaginal recurrence (star) (b); increaseduptake is seen as orange colour and it is marked by a star. A catheter has been placed in the bladder to avoid urinary radioactivityhiding the recurrence.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Fig. 18. Positron emission tomography and computed tomography (PET-CT) image of metastatic lymph node from recurrentendometrial carcinoma. Axial low-dose computed tomography of the pelvis shows a lymph node close to the right common iliacvessels; the size criterion (short axis >1 cm indicating malignancy) does not allow assessment of the benign or malignant nature ofthis lymph node (a). Axial fused PET-CT scan corresponding to (a) shows increased metabolic activity in the metastatic lymph node(b); increased uptake is seen as orange colour.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–2320
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 20/23
How to plan the most appropriate surveillance strategy in asymptomatic women remains adilemma. A strategy with computed tomography or MRI carried out every 6 or 12 months has notshown any positive effect on survival of women with gynaecological tumours. Transvaginal andtransabdominal ultrasound combined with clinical examination during follow up might be a cost-effective strategy for detecting solitary early recurrences suitable for secondary cytoreduction.Whether such a strategy would improve patient survival is not known.
Conclusion
Follow-up guidelines for women treated for gynaecological cancer are not available. The limitedinformation in published studies does not allow evidence-based guidelines to be created. Computedtomography, MRI, ultrasound, and PET-CT are imaging methods that can be used for the surveillance ofthese women. Women who are asymptomatic can be routinely evaluated with transabdominal andtransvaginal ultrasound added to clinical and serological examinations. It is unclear when and how touse more sophisticated diagnostic imaging methods, such as computed tomography and MRI inwomen who are asymptomatic. It has not been shown that 6-monthly or annual computed tomog-raphy scans or MRI examinations have a positive effect on survival. In women with clinical or sero-logical signs of relapse but with normal results of conventional imaging, PET-CT might have a role. Itmay also have a role in women with pelvic or abdominal recurrences considered for secondarycytoreduction to exclude the presence of supradiaphragmatic lesions.
Practice points
� Ultrasound can be used as the first-line imaging method in the follow up of patients treated
for ovarian or uterine malignancies.
� Ultrasound can detect and describe pelvic and abdominal recurrences (e.g. size, mobility,
and invasion of surrounding tissues).
� Computed tomography is currently the standard imagingmethod for the follow up of women
treated for gynaecological malignancy.
� It is not clear when and how to use computed tomography or MRI in asymptomatic women
treated for ovarian or uterine malignancies.
� PET-CT can be used as a second-line diagnostic test if the results of other imaging methods
are negative or equivocal but there is a strong suspicion of recurrence because of symptoms
or elevated levels of tumour markers.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

Q13
Q10
Q11
Q12
Q15
Research agenda
� To conduct multicentre, prospective, randomised trials on the follow up for each single
gynaecological neoplasm (i.e. ovarian, endometrial, cervical cancer and uterine sarcoma) to
create evidence-based generalisable guidelines.
C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 21
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 21/23
Uncited reference
[73], [74].
References
[1] Kitajima K, Murakami K, Yamasaki E, et al. Performance of integrated FDG-PET/contrast-enhanced CT in the diagnosis ofrecurrent uterine cancer: comparison with PET and enhanced CT. Eur J Nucl Med Mol Imaging 2009;36:362–72.
[2] Sartori E, Pasinetti B, Carrara L, et al. Pattern of failure and value of follow-up procedures in endometrial and cervicalcancer patients. Gynecol Oncol 2007;107(1 Suppl 1):S241–7.
[3] Salvesen HB, Akslen LA, Iversen T, et al. Recurrence of endometrial carcinoma and the value of routine follow up. Br JObstet Gynaecol 1997;104:1302–7.
[4] Berchuck A, Anspach C, Evans AC, et al. Postsurgical surveillance of patients with FIGO stage I/II endometrial adeno-carcinoma. Gynecol Oncol 1995;59:20–4.
[5] Jeong YY, Kong HK, Chung TW, et al. Uterine cervical carcinoma after therapy: CT and MR imaging findings. Radiographics2003;23:968–81.
[6] Pannu HK, Bristow RE, Montz FJ, et al. Multidetector CT of peritoneal carcinomatosis from ovarian cancer. Radiographics2003;23:687–701.
[7] Lo SS, Khoo US, Cheng DK, et al. Role of serial markers in the surveillance for recurrence in endometrial cancer. CancerDetect Prev 1999;23:397–400.
[8] Forstner R, Hricak H, Powell CB, et al. Ovarian cancer recurrence value of MR imaging. Radiology 1995;196:715–20.[9] Reuter K, Griffin T, Hunter RE. Comparison of abdominopelvic computed tomography results and findings at second look
laparotomy in ovarian carcinoma patients. Cancer 1989;63:1123–8.[10] Tammela J, Lele S. New modalities in detection of recurrent ovarian cancer. Curr Opin Obstet Gynecol 2004;16:5–9.[11] Jemal A, Siegel R, Ward E, et al. Cancer statistics. CA Cancer J Clin 2007;2007(57):43–66.*[12] Ferrandina G, Legge F, Salutari V, et al. Impact of pattern of recurrence on clinical outcome of ovarian cancer patients:
clinical considerations. Eur J Cancer 2006;42:2296–302.[13] Greenlee RT, Hill-Harmon MB, Murray T, et al. Cancer statistics, 2001. CA Cancer J Clin 2001;51:15–36.[14] Fu Y, Wang X, Pan Z, et al. Clinical outcomes and prognostic factors of patients with epithelial ovarian cancer subjected to
first-line treatment: a retrospective study of 251 cases. Front Med 2014;8:91–5.[15] Harter P, du Bois A. The role of surgery in ovarian cancer with special emphasis on cytoreductive surgery for recurrence.
Curr Opin Oncol 2005;17:505–14.[16] Park CM, Kim SH, Kim SH, et al. Recurrent ovarian malignancy: patterns and spectrum of imaging findings. Abdom
Imaging 2003;28:404–15.[17] Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin 2005;55:74–108.[18] Petignat P, Roy M. Diagnosis and management of cervical cancer. BMJ 2007;335:765–8.[19] Perez CA, Grigsby PW, Camel HM, et al. Irradiation alone or combined with surgery in stage IB, IIA, and IIB carcinoma of
uterine cervix: update of a nonrandomized comparison. Int J Radiat Oncol Biol Phys 1995;31:703–16.[20] Hong JH, Tsai CS, Lai CH, et al. Recurrent squamous cell carcinoma of cervix after definitive radiotherapy. Int J Radiat
Oncol Biol Phys 2004;60:249–57.[21] Morice P, Deyrolle C, Rey A, et al. Value of routine follow-up procedures for patients with stage I/II cervical cancer treated
with combined surgery-radiation therapy. Ann Oncol 2004;15:218–23.[22] Sartori E, Pasinetti B, Chiudinelli F, et al. Surveillance procedures for patients treated for endometrial cancer: a review of
the literature. Int J Gynecol Cancer 2010;20:985–92.[23] Pignata S, Scambia G, Pisano C, et al., Multicentre Italian Trials in Ovarian Cancer and Gynecologic Malignancies Group.
A multicentre phase II study of carboplatin plus pegylated liposomal doxorubicin as first-line chemotherapy for patientswith advanced or recurrent endometrial carcinoma: the END-1 study of the MITO (Multicentre Italian Trials in OvarianCancer and Gynecologic Malignancies) group. Br J Cancer 2007;96:1639–43.
[24] Fung-Kee-Fung M, Dodge J, Elit L, et al., Cancer Care Ontario Program in Evidence-based Care Gynecology Cancer DiseaseSite Group. Follow-up after primary therapy for endometrial cancer: a systematic review. Gynecol Oncol 2006;101:520–9.
[25] Korets SB, Curtin JP. Surgical options for recurrent uterine sarcomas. Am Soc Clin Oncol Educ Book 2012;32:362–6.[26] Gadducci A. Prognostic factors in uterine sarcoma. Best Pract Res Clin Obstet Gynaecol 2011;25:783–95.[27] Meanwell CA, Rolfe EB, Blackledge G, et al. Recurrent female pelvic cancer: assessment with transrectal ultrasonography.
Radiology 1987;162(1 Pt 1):278–81.[28] Volpi E, Zola P, De Grandis T, et al. Transvaginal sonography in the diagnosis of pelvic malignant recurrence: integration of
sonography and needle-guided biopsy. Ultrasound Obstet Gynecol 1994;4:135–8.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–2322
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354
YBEOG1347_proof ■ 8 May 2014 ■ 22/23
*[29] Testa AC, Fruscella E, Ludovisi M, et al. The role of sonographic examination in the follow-up of gynecological neoplasms.Gynecol Oncol 2005;99:696–703.
*[30] Savelli L, Testa AC, Ferrandina G, et al. Pelvic relapses of uterine neoplasms: transvaginal sonographic and Dopplerfeatures. Gynecol Oncol 2004;93:441–5.
*[31] Testa AC, Ciampelli M, Mastromarino C, et al. Detection of central pelvic recurrent disease with transvaginal color Dopplerultrasound in women treated for gynecological malignancy. Ultrasound Obstet Gynecol 2002;19:490–5.
[32] Fischerova D. Ultrasound scanning of the pelvis and abdomen for staging of gynecological tumors: a review. UltrasoundObstet Gynecol 2011;38:246–66.
[33] Testa AC, Van Holsbeke C, Mascilini F, et al. Dynamic and interactive gynecological ultrasound examination. UltrasoundObstet Gynecol 2009;34:225–9.
[34] Pannu HK, Horton KM, Fishman EK. Thin section dual-phase multidetector-row computed tomography detection ofperitoneal metastases in gynecologic cancers. J Comput Assist Tomogr 2003;27:333–40.
[35] Gu P, Pan LL, Wu SQ, et al. CA 125, PET alone, PET-CT, CT and MRI in diagnosing recurrent ovarian carcinoma: a systematicreview and meta-analysis. Eur J Radiol 2009;71:164–74.
[36] Sala E, Kataoka M, Pandit-Taskar N, et al. Recurrent ovarian cancer: use of contrast-enhanced CT and PET/CT to accuratelylocalize tumor recurrence and to predict patients’ survival. Radiology 2010;257:125–34.
*[37] Funt SA, Hricak H, Abu-Rustum N, et al. Role of CT in the management of recurrent ovarian cancer. Am J Roentgenol 2004;182:393–8.
*[38] Low RN, Barone RM, Lacey C, et al. Peritoneal tumor: MR imaging with dilute oral barium and intravenous gadolinium-containing contrast agents compared with unenhanced MR imaging and CT. Radiology 1997;204:513–20.
[39] Patel S, Liyanage SH, Sahdev A, et al. Imaging of endometrial and cervical cancer. Insights Imaging 2010;1:309–28.[40] Jeong YY, Kang HK, Chung TW, et al. Uterine cervical carcinoma after therapy: CT and MR imaging findings. Radiographics
2003;23:969–81.*[41] Kwek JW, Iyer RB. Recurrent ovarian cancer: spectrum of imaging findings. Am J Roentgenol 2006;187:99–104.[42] Prayer L, Kainz C, Kramer J, et al. CT and MR accuracy in the detection of tumor recurrence in patients treated for ovarian
cancer. J Comput Assist Tomogr 1993;17:626–32.[43] Outwater EK, Siegelman ES, Wilson KM, et al. Benign and malignant gynecologic disease: clinical importance of fluid and
peritoneal enhancement in the pelvis at MR imaging. Radiology 1996;200:483–8.[44] Kim CK, Park BK, Choi JY, et al. Detection of recurrent ovarian cancer at MRI: comparison with integrated PET/CT.
J Comput Assist Tomogr 2007;31:868–75.[45] Kim SH, Han MC. Invasion of the urinary bladder by uterine cervical carcinoma: evaluation with MR imaging. AJR Am J
Roentgenol 1997;168:393–7.[46] Manfredi R, Baltieri S, Tognolini A, et al. Recurrent uterine cancer after surgery: magnetic resonance imaging patterns and
their changes after concomitant chemoradiation. Radiol Med 2008;113:1143–56.[47] Kinkel K, Ariche M, Tardivon AA, et al. Differentiation between recurrent tumor and benign conditions after treatment of
gynecologic pelvic carcinoma: value of dynamic contrast-enhanced subtraction MR imaging. Radiology 1997;204:55–63.[48] Nishie A, Stolpen AH, Obuchi M, et al. Evaluation of locally recurrent pelvic malignancy: performance of T2- and
diffusion-weighted MRI with image fusion. J Magn Reson Imaging 2008;28:705–13.[49] Yang WT, Lam WW, Yu MY, et al. Comparison of dynamic helical CT and dynamic MR imaging in the evaluation of pelvic
lymph nodes in cervical carcinoma. AJR Am J Roentgenol 2000;175:759–66.[50] De Gaetano AM, Calcagni ML, Rufini V, et al. Imaging of gynecologic malignancies with FDG PET-CT: case examples,
physiologic activity, and pitfalls. Abdom Imaging 2009;34:696–711.[51] Gorospe L, Jover-Díaz R, Vicente-Bártulos A. Spectrum of PET-CT pelvic pitfalls in patients with gynecologic malignancies.
Abdom Imaging 2012;37:1041–65.[52] Lai CH, Huang K, See LC, et al. Restaging of recurrent cervical carcinoma with dual-phase [18F]Fluoro-2-Deoxy-D-Glucose
positron emission tomography. Cancer 2004;100:544–52.[53] Kitajima K, Ueno Y, Suzuki K, et al. Low-dose non-enhanced CT versus full-dose contrast-enhanced CT in integrated PET/
CT scans for diagnosing ovarian cancer recurrence. Eur J Radiol 2012;81:3557–62.*[54] Kitajima K, Suzuki K, Nakamoto Y, et al. Low-dose non-enhanced CT versus full-dose contrast-enhanced CT in integrated
PET/CT studies for the diagnosis of uterine cancer recurrence. Eur J Nucl Med Mol Imaging 2010;37:1490–8.[55] Vargas HA, Burger IA, Donati OF, et al. Magnetic resonance imaging/positron emission tomography provides a roadmap
for surgical planning and serves as a predictive biomarker in patients with recurrent gynecological cancers undergoingpelvic exenteration. Int J Gynecol Cancer 2013;23:1512–9.
[56] Kitajima K, Suenaga Y, Ueno Y, et al. Value of fusion of PET and MRI in the detection of intra-pelvic recurrence of gy-necological tumor: comparison with 18F-FDG contrast-enhanced PET/CT and pelvic MRI. Ann Nucl Med 2014;28:25–32.
[57] Sala E, Kataoka M, Pandit-Taskar N, et al. Recurrent ovarian cancer: use of contrast-enhanced CT and PET/CT to accuratelylocalize tumor recurrence and to predict patients’ survival. Radiology 2010;257:125–34.
[58] Dragosavac S, Derchain S, Caserta NM, et al. Staging recurrent ovarian cancer with (18)FDG PET/CT. Oncol Lett 2013;5:593–7.
*[59] Chung HH, Kang WJ, Kim JW, et al. Role of [18F]FDG PET/CT in the assessment of suspected recurrent ovarian cancer:correlation with clinical or histological findings. Eur J Nucl Med Mol Imaging 2007;34:480–6.
[60] Antunovic L, Cimitan M, Borsatti E, et al. Revisiting the clinical value of 18F-FDG PET/CT in detection of recurrentepithelial ovarian carcinomas: correlation with histology, serum CA-125 assay, and conventional radiological modalities.Clin Nucl Med 2012;37:e184–8.
[61] Risum S, Høgdall C, Markova E, et al. Influence of 2-(18F) fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography on recurrent ovarian cancer diagnosis and on selection of patients for secondary cytoreductivesurgery. Int J Gynecol Cancer 2009;19:600–4.
[62] Fagotti A, Fanfani F, Rossitto C, et al. Oncology 2008;75:152–8.[63] Chen YM, Chen T, Zee CS, et al. Is there an impact of 18F-FDG PET/CT on the surveillance and clinical management of
recurrent ovarian cancer? Research based on a large sample in a single PET/CTcenter. Nucl Med Commun 2014;35:347–52.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008

C.A. Testa et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2014) 1–23 23
123456789101112131415161718192021222324252627282930313233
YBEOG1347_proof ■ 8 May 2014 ■ 23/23
[64] Limei Z, Yong C, Yan X, et al. Accuracy of positron emission tomography/computed tomography in the diagnosis andrestaging for recurrent ovarian cancer: a meta-analysis. Int J Gynecol Cancer 2013;23:598–607.
[65] Simcock B, Neesham D, Quinn M, et al. The impact of PET/CT in the management of recurrent ovarian cancer. GynecolOncol 2006;103:271–6.
[66] Fulham MJ, Carter J, Baldey A, et al. The impact of PET-CT in suspected recurrent ovarian cancer: a prospective multi-centre study as part of the Australian PET Data Collection Project. Gynecol Oncol 2009;112:462–8.
[67] Kitajima K, Murakami K, Yamasaki E, et al. Performance of FDG-PET/CT for diagnosis of recurrent uterine cervical cancer.Eur Radiol 2008;18:2040–7.
[68] Ebina Y, Watari H, Kaneuchi M, et al. Impact of FDG PET in optimizing patient selection for cytoreductive surgery inrecurrent ovarian cancer. Eur J Nucl Med Mol Imaging 2014;41:446–51.
[69] Murakami M, Miyamoto T, Iida T, et al. Whole-body positron emission tomography and tumor marker CA125 fordetection of recurrence in epithelial ovarian cancer. Int J Gynecol Cancer 2006;16(suppl 1):99–107.
[70] Havrilesky LJ, Kulasingam SL, Matchar DB, et al. FDG-PET for management of cervical and ovarian cancer. Gynecol Oncol2005;97:183–91.
[71] Palomar A, Nanni C, Castellucci P, et al. Value of FDG PET/CT in patients with treated ovarian cancer and raised CA125serum levels. Mol Imaging Biol 2012;14:123–9.
[72] Khan N, Oriuchi N, Yoshizaki A, et al. Diagnostic accuracy of FDG PET imaging for the detection of recurrent or metastaticgynecologic cancer. Ann Nucl Med 2005;19:137–45.
[73] Bhosale P, Peungjesada S, Wei W, et al. Clinical utility of positron emission tomography/computed tomography in theevaluation of suspected recurrent ovarian cancer in the setting of normal CA-125 levels. Int J Gynecol Cancer 2010;20:936–44.
*[74] Chang TC, Law KS, Hong JH, et al. Positron emission tomography for unexplained elevation of serum squamous cellcarcinoma antigen levels during follow-up for patients with cervical malignancies: a phase II study. Cancer 2004;101:164–71.
[75] Unger JB, Ivy JJ, Connor P, et al. Detection of recurrent cervical cancer by whole-body FDG PET scan in asymptomatic andsymptomatic women. Gynecol Oncol 2004;94:212–6.
[76] Ryu SY, Kim MH, Choi SC, et al. Detection of early recurrence with 18F-FDG PET in patients with cervical cancer. J NuclMed 2003;44:347–52.
[77] Chao A, Chang TC, Ng KK, et al. 18F-FDG PET in the management of endometrial cancer. Eur J Nucl Med Mol Imaging2006;33:36–44.
[78] Park JY, Kim EN, Kim DY, et al. Role of PET or PET/CT in the post-therapy surveillance of uterine sarcoma. Gynecol Oncol2008;109:255–62.
[79] Kao YH, Saad U, Tan AE, et al. Fluorine-18-fluorodeoxyglucose PET/CT for the evaluation of suspected recurrent uterineleiomyosarcomas. Acta Radiol 2011;52:463–6.
[80] Sharma P, Kumar R, Singh H, et al. Carcinoma endometrium: role of 18-FDG PET/CT for detection of suspected recurrence.Clin Nucl Med 2012;37:649–55.
[81] Kim HW, Won KS, Zeon SK, et al. Peritoneal carcinomatosis in patients with ovarian cancer: enhanced CT versus 18F-FDGPET/CT. Clin Nucl Med 2013;38:93–7.
[82] Ma SY, See LC, Lai CH, et al. Delayed (18)F-FDG PET for detection of paraaortic lymph node metastases in cervical cancerpatients. J Nucl Med 2003;44:1775–83.
Please cite this article in press as: Testa CA, et al., Which imaging technique should we use in the followup of gynaecological cancer?, Best Practice & Research Clinical Obstetrics and Gynaecology (2014), http://dx.doi.org/10.1016/j.bpobgyn.2014.04.008


















