What to Do With a Patient Who Smokes Steven A. Schroeder, MD Presentation courtesy of The Smoking...
79
What to Do With a Patient Who Smokes Steven A. Schroeder, MD Steven A. Schroeder, MD Presentation courtesy of Presentation courtesy of The Smoking Cessation Leadership Center The Smoking Cessation Leadership Center and Rx for Change and Rx for Change February 2007 February 2007
-
Upload
anabel-montgomery -
Category
Documents
-
view
217 -
download
0
Transcript of What to Do With a Patient Who Smokes Steven A. Schroeder, MD Presentation courtesy of The Smoking...

What to Do With a Patient
Who Smokes
Steven A. Schroeder, MDSteven A. Schroeder, MD
Presentation courtesy of Presentation courtesy of
The Smoking Cessation Leadership Center The Smoking Cessation Leadership Center
and Rx for Changeand Rx for ChangeFebruary 2007February 2007


Topics for TodayTopics for Today
Facts about smokingFacts about smoking Nicotine and dependenceNicotine and dependence Aids for cessationAids for cessation Telephone quitlinesTelephone quitlines Next stepsNext steps

JAMA Article

Tobacco’s Deadly Toll
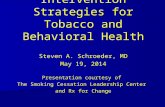
440,000 deaths in the U.S. each year440,000 deaths in the U.S. each year 4.8 million deaths world wide each year4.8 million deaths world wide each year 10 million deaths estimated by year 203010 million deaths estimated by year 2030 50,000 deaths in the U.S. due to second-50,000 deaths in the U.S. due to second-
hand smoke exposurehand smoke exposure 8.6 million disabled from tobacco in the U.S. 8.6 million disabled from tobacco in the U.S.
alonealone

*
17
81
4119 14
30
440
0
50
100
150
200
250
300
350
400
450
Comparative Causes of Annual Deaths in the United States
Nu
mb
er o
f d
eath
s (t
ho
usa
nd
s)
Source: Centers for Disease Control and Prevention
AIDS Alcohol Motor Homicide Drug Suicide Smoking Vehicle Induced
Also suffer from mental illness and/or substance abuse
*


Annual U.S. Deaths Attributable to Smoking, 1997–2001
Centers for Disease Control and Prevention. MMWR 2005;54:625–628.
31%28%23%9%8%
<1%
TOTAL: 437,902 deaths annually
Cardiovascular diseases
137,979
Lung cancer 123,836
Respiratory diseases 101,454
Second-hand smoke 38,112
Cancers other than lung
34,693
Other 1,828
Percent of all smoking-attributable deaths

Health Consequences of Smoking
U.S. Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon
General, 2004.
CancersCancers– Acute myeloid leukemia Acute myeloid leukemia – Bladder and kidneyBladder and kidney– CervicalCervical– EsophagealEsophageal– GastricGastric– LaryngealLaryngeal– LungLung– Oral cavity and pharyngealOral cavity and pharyngeal– PancreaticPancreatic
Pulmonary diseasesPulmonary diseases– Acute (e.g., pneumonia)Acute (e.g., pneumonia)– Chronic (e.g., COPD)Chronic (e.g., COPD)
Cardiovascular diseasesCardiovascular diseases– Abdominal aortic aneurysmAbdominal aortic aneurysm– Coronary heart diseaseCoronary heart disease– Cerebrovascular diseaseCerebrovascular disease– Peripheral arterial diseasePeripheral arterial disease
Reproductive effectsReproductive effects– Reduced fertility in womenReduced fertility in women– Poor pregnancy outcomes (e.g., Poor pregnancy outcomes (e.g.,
low birth weight, preterm delivery)low birth weight, preterm delivery)– Infant mortalityInfant mortality
Other effects: cataract, Other effects: cataract, osteoporosis, periodontitis, poor osteoporosis, periodontitis, poor surgical outcomessurgical outcomes

0
5
10
15
30 40 50 60
Yea
rs o
f lif
e ga
ined
Age at cessation (years)
Prospective study of 34,439 male British doctors
Mortality was monitored for 50 years (1951–2001) On average, cigarette
smokers die approximately 10 years younger than do
nonsmokers.
Among those who continue smoking, at least half will
die due to a tobacco-related disease.
Smoking Cessation: Reduced Risk of Death
Doll et al. (2004). BMJ 328(7455):1519–1527.

Reduction in cumulative risk of death from lung cancer in
men
Reprinted with permission. Peto et al. (2000). BMJ 321(7257):323–329.
Cu
mu
lati
ve r
isk
(%)
Age in years

Causal Associations with Second-hand Smoke
DevelopmentalDevelopmental– Low birthweightLow birthweight– Sudden Infant Death Sudden Infant Death
SyndromeSyndrome– Pre-term deliveryPre-term delivery
RespiratoryRespiratory– Asthma inductionAsthma induction and and
exacerbationexacerbation– Eye and nasal irritationEye and nasal irritation– Bronchitis, pneumonia, Bronchitis, pneumonia,
otitis media in childrenotitis media in children
CarcinogenicCarcinogenic– Lung cancerLung cancer– Nasal sinus cancerNasal sinus cancer– Breast cancer (younger, Breast cancer (younger,
premenopausal women)premenopausal women)
CardiovascularCardiovascular– Heart disease mortalityHeart disease mortality– Acute and chronic Acute and chronic
coronary heart disease coronary heart disease morbiditymorbidity
– Altered vascular Altered vascular propertiesproperties

Compounds in Tobacco Smoke
– Carbon monoxideCarbon monoxide– Hydrogen cyanideHydrogen cyanide– AmmoniaAmmonia– BenzeneBenzene– FormaldehydeFormaldehyde
– NicotineNicotine– NitrosaminesNitrosamines– LeadLead– CadmiumCadmium– Polonium-210Polonium-210
An estimated 4,800 compounds in tobacco smoke, including 11 proven human carcinogensGases Particles
Nicotine does NOT cause the ill health effects of tobacco.

The Real Culprit
It is the smoke, tar, and additives that It is the smoke, tar, and additives that make people sicken and die. make people sicken and die.
Nicotine is dangerous because it leads to Nicotine is dangerous because it leads to addiction, and therefore increased addiction, and therefore increased exposure tobacco constituents.exposure tobacco constituents.
Therefore, nicotine replacement therapy is Therefore, nicotine replacement therapy is helpful, not harmful. It is a “clean” form of helpful, not harmful. It is a “clean” form of nicotine.nicotine.

California15.2%
New York 20.5%
Utah11.5%
Texas 20.0%
Illinois 19.9% Kentucky
28.7%
Nevada23.1%
Centers for Disease Control and Prevention. (2006). MMWR 55:1148–1151.
Florida 21.6%
Indiana27.3%
STATE-SPECIFIC PREVALENCE of SMOKING among ADULTS, 2005

TRENDS in ADULT SMOKING, by SEX—U.S., 1955–2005Trends in cigarette current smoking among persons aged 18 or older
Graph provided by the Centers for Disease Control and Prevention. 1955 Current Population Survey; 1965–2005 NHIS. Estimates since 1992 include some-day smoking.
Per
cen
t
70% want to quit
0
10
20
30
40
50
60
1955 1959 1963 1967 1971 1975 1979 1983 1987 1991 1995 1999 2003
Male
Female 23.9%
18.1%
20.9% of adults are
current smokers
Year

TRENDS in TEEN SMOKING, by ETHNICITY—U.S., 1977–2006
Trends in cigarette smoking among 12th graders: 30-day prevalence of use
0
10
20
30
40
50
1977 1982 1987 1992 1997 2002Year
Institute for Social Research, University of Michigan, Monitoring the Future Projectwww.monitoringthefuture.org
Per
cen
t
White
Hispanic
Black

TRENDS in ADULT CIGARETTE CONSUMPTION—U.S., 1900–2005
Annual adult per capita cigarette consumption and major smoking and health events
Centers for Disease Control and Prevention. (1999). MMWR 48:986–993.Per-capita updates from U.S. Department of Agriculture, provided by the American Cancer Society.
0
1,000
2,000
3,000
4,000
5,000
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000
First SurgeonGeneral’s Report
Great Depression
End of WW II
Federal cigarettetax doubles
MasterSettlementAgreement; California first state to enact ban on smoking in bars
Broadcastad ban
Cigarette price drop
Nonsmokers’ rights movement
beginsNu
mb
er o
f ci
ga
rett
es
Year
20 states have > $1
pack tax

PREVALENCE of ADULT SMOKING,
by RACE/ETHNICITY—U.S., 2005
0% 10% 20% 30% 40% 50%
13.3% Asian*
32.0% American Indian/Alaska Native*
21.5% Black*
21.9% White*
16.2% Hispanic
Centers for Disease Control and Prevention. (2006). MMWR 55:1145–1148.
* non-Hispanic.

PREVALENCE of ADULT SMOKING,
by EDUCATION—U.S., 2005
0% 10% 20% 30% 40% 50%
10.7% Undergraduate degree
25.5% No high school diploma
43.2% GED diploma
24.6% High school graduate
22.5% Some college
7.1% Graduate degree
Centers for Disease Control and Prevention. (2006). MMWR 55:1145–1148.

Number of Smokers = New Smokers + Old Smokers -
Quitters

Number of Quitters =
Number of Quit Attempts X % of Quitters
Price
Clean indoor air
Clinician advice
Counseling
Medications
Counter Marketing

Ways to Help Smokers Quit
Raise prices (taxes)Raise prices (taxes) Clean indoor airClean indoor air Create counter-marketingCreate counter-marketing Provide cessation aids: counseling and Provide cessation aids: counseling and
pharmacotherapy, alone or in combinationpharmacotherapy, alone or in combination– Directly by clinician in individual or group Directly by clinician in individual or group
session (office or hospital)session (office or hospital)– Toll-free telephone quitlinesToll-free telephone quitlines

Reasons for Not Helping Patients Quit
1. Too busy1. Too busy
2. Lack of expertise2. Lack of expertise
3. No financial incentive3. No financial incentive
4. Most smokers can’t/won’t quit4. Most smokers can’t/won’t quit
5. Stigmatizing smokers5. Stigmatizing smokers
6. Respect for privacy6. Respect for privacy
7. Negative message might scare away 7. Negative message might scare away patientspatients
8. I smoke myself8. I smoke myself

Responses to Patient Who Smokes
Unacceptable: “I don’t have time.”Unacceptable: “I don’t have time.” AcceptableAcceptable
– Refer to a quit lineRefer to a quit line– Establish systems in your office and Establish systems in your office and
hospitalhospital– Become a cessation expertBecome a cessation expert

The 5 A’s: Review
ASK about tobacco USE
ADVISE tobacco users to QUIT
ASSESS readiness to make a QUIT attempt
ASSIST with the QUIT ATTEMPT
ARRANGE FOLLOW-UP care
Fiore et al. (2000). Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS.

Measurements of Smoking Intensity
Fagerström Test for Nicotine Fagerström Test for Nicotine DependenceDependence
BiochemicalBiochemical– Serum, urinary, or saliva cotinine testingSerum, urinary, or saliva cotinine testing– Carbon monoxide testingCarbon monoxide testing

Fagerström Test for Nicotine Dependence
Item Response Options
Points
1.1. How soon after you awaken do you smoke your first How soon after you awaken do you smoke your first cigarette?cigarette?
within 5 minuteswithin 5 minutes 6-30 minutes6-30 minutes 30-60 minutes30-60 minutes after 60 minutesafter 60 minutes
33 22 11 00
2.2. Do you find it difficult to refrain from smoking in Do you find it difficult to refrain from smoking in places where it is forbidden?places where it is forbidden?
yesyes nono
11 00
3.3. Which cigarette would you hate most to give up?Which cigarette would you hate most to give up? first one in morningfirst one in morning any otherany other
11 00
4.4. How many cigarettes per day do you smoke?How many cigarettes per day do you smoke? 10 or less10 or less 11-2011-20 21-3021-30 31 or more31 or more
00 11 22 33
5.5. Do you smoke more frequently during the first hours Do you smoke more frequently during the first hours after waking up than during the rest of the day?after waking up than during the rest of the day?
yesyes nono
11 00
6.6. Do you smoke if you are so ill that you are in bed Do you smoke if you are so ill that you are in bed most of the day?most of the day?
yesyes nono
11 00
Heatherton TF, Kozlowski LT, Frecker RC, Fagerström K-O. The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. Br J Addict 1991;86:1119–1127.

Nicotine Absorption
Absorption is pH dependent In acidic media
– Ionized poorly absorbed across membranes In alkaline media
– Non ionized well absorbed across membranes
At physiologic pH (7.3–7.5),nicotine is readily absorbed.

Nicotine Distribution
Data from Henningfield et al., Drug Alcohol Depend 1993;33:23-29. Graph reprinted with permission, Rx for Change, The Regents of the University of
California, University of Southern California, and Western University of Health Sciences.
0
10
20
30
40
50
60
70
80
0 1 2 3 4 5 6 7 8 9 10
Minutes after light-up of cigarette
Pla
sma n
icoti
ne (
ng/m
L) Arterial
Venous
Nicotine reaches the brain within 11 seconds

Metabolizedand excreted
in urine
Nicotine Metabolism
CH3N
H 10–20% excreted
unchangedin urine
Adapted and reprinted with permission. Benowitz et al. J Pharmacol Exp Ther 1994;268:296–303.
70–80% cotinine
~ 10% other
metabolites
N

Nicotine Pharmacodynamics
Central nervous systemCentral nervous system– PleasurePleasure– Arousal, enhanced vigilanceArousal, enhanced vigilance– Improved task performanceImproved task performance– Anxiety reliefAnxiety relief
OtherOther– Appetite suppressionAppetite suppression– Increased metabolic rateIncreased metabolic rate– Skeletal muscle relaxationSkeletal muscle relaxation
Cardiovascular systemCardiovascular system Heart rateHeart rate Cardiac outputCardiac output Blood pressureBlood pressure– Coronary Coronary
vasoconstrictionvasoconstriction– Cutaneous Cutaneous
vasoconstrictionvasoconstriction

Nicotine enters brain
Stimulation of nicotine receptors
Dopamine release
Dopamine Reward PathwayDopamine Reward PathwayPrefrontal
cortex
Nucleus accumbens
Ventral tegmental
area

Chronic Administration of Nicotine: Effects on the Brain
Perry et al. J Pharmacol Exp Ther 1999;289:1545–1552.
Nonsmoker Smoker
Human smokers have increased nicotine receptors in the prefrontal
cortex.
High
Low
Image courtesy of George Washington University / Dr. David C. Perry

Damage to the Insula Disrupts Damage to the Insula Disrupts Addiction to Cigarette Addiction to Cigarette
Smoking*Smoking* 19 smokers with brain damage to insula 19 smokers with brain damage to insula
region, compared with 50 smokers with region, compared with 50 smokers with brain damage elsewherebrain damage elsewhere
Smoking rates lower in insula-damaged Smoking rates lower in insula-damaged patients (odds ratio=2.94) but not patients (odds ratio=2.94) but not statistically significant (low #s)statistically significant (low #s)
But addictive cravings much lower in But addictive cravings much lower in insula damaged patients (OR=22; insula damaged patients (OR=22; p<.0005)p<.0005)
*Naqvi et al. Science 2007; 315:531-534

Depression Insomnia Irritability/frustration/anger Anxiety Difficulty concentrating Restlessness Increased appetite/weight gain Decreased heart rate Cravings*
Nicotine Pharmacodynamics: Withdrawal Effects
American Psychiatric Association. (1994). DSM-IV. Hughes et al. (1991). Arch Gen Psychiatry 48:52–59.
Hughes & Hatsukami. (1998). Tob Control 7:92–93.
Most symptoms peak 24–48 hr after quitting and subside within 2–4
weeks.
* Not considered a withdrawal symptom by DSM-IV criteria.

Nicotine Addiction Cycle
Reprinted from Med Clin N Am 76(2), Benowitz NL, Cigarette smoking and nicotine addiction, pp. 415–437, Copyright 1992, with permission from Elsevier.

Nicotine Addiction
Tobacco users maintain a minimum serum nicotine concentration in order to
– Prevent withdrawal symptoms– Maintain pleasure/arousal– Modulate mood
Users self-titrate nicotine intake by– Smoking more frequently– Smoking more intensely– Obstructing vents on low-nicotine brand
cigarettes

Cognitive Strategies for Cessation
Reframe the way a patient thinks about smoking
Review commitment to quit, focus on downsides of tobacco use
Distractive thinking Positive self-talks, “pep talks” Relaxation through imagery Mental rehearsal, visualization

Behavioral Strategies for Cessation (Avoiding Stimuli that Trigger
Smoking)
Stress – Anticipate future challenges– Develop substitutes for tobacco
Alcohol – Limit or abstain during early stages of
quitting Other tobacco users
– Stay away– Ask for cooperation from family and friends

Behavioral Strategies for Cessation (Part 2)
Oral gratification needs – Use substitutes: water, sugar-free chewing
gum or hard candies Automatic smoking routines
– Anticipate routines and develop alternative plans, e.g., with morning coffee
Weight gain after cessation – Anticipate; use gum or bupropion; exercise
Cravings – Distractive thinking; change activities

Pharmacologic Methods: First-line Therapies
Three general classes of FDA-approved drugs for smoking cessation: Nicotine replacement therapy (NRT)
– Nicotine gum, patch, lozenge, nasal spray, inhaler
Psychotropics– Sustained-release bupropion
Partial nicotinic receptor agonist– Varenicline
Currently, no medications have an FDA indication for use in spit tobacco cessation.

Nicotine Gum
Disadvantages
Gum may not be socially acceptable.
Gum is difficult to use with dentures.
Patients must use proper chewing technique to minimize adverse effects.
Advantages Gum use may satisfy
oral cravings. Gum use may delay
weight gain. Patients can titrate
therapy to manage withdrawal symptoms.

Transdermal Nicotine Patch
Disadvantages
Patients cannot titrate the dose.
Allergic reactions to adhesive may occur.
16-hr patch may lead to morning nicotine cravings.
Patients with dermatologic conditions should not use.
Advantages The patch provides
consistent nicotine levels.
The patch is easy to use and conceal.
Fewer compliance issues are associated with the patch.

Nicotine Lozenge
Disadvantages Gastrointestinal side
effects (nausea, hiccups, and heartburn) may be bothersome.
Advantages Lozenge use may
satisfy oral cravings. The lozenge is easy to
use and conceal. Patients can titrate
therapy to manage withdrawal symptoms.

Nicotine Nasal Spray
Disadvantages Nasal/throat irritation Dependence can result. Patients must wait 5
minutes before driving or operating heavy machinery.
Patients with chronic nasal disorders or severe reactive airway disease should not use the spray.
Advantages Patients can easily
titrate therapy to rapidly manage withdrawal symptoms.

Nicotine Inhaler
Disadvantages Initial throat or mouth
irritation. Can’t store cartridges
in very warm conditions or use in very cold conditions.
Patients with underlying bronchospastic disease must use with caution.
Advantages Patients can easily
titrate therapy to manage withdrawal symptoms.
The inhaler mimics hand-to-mouth ritual of smoking.

Combination NRT
Combination NRT– Long-acting formulation (patch)
Produces relatively constant levels of nicotine
PLUS– Short-acting formulation (gum, lozenge, inhaler, nasal spray)
Allows for acute dose titration as needed for withdrawal symptoms
Bupropion SR + NRT The safety and efficacy of combination of
varenicline with NRT or bupropion has not been established.Because many of the remaining smokers are very addicted, Because many of the remaining smokers are very addicted,
use of combination therapies is becoming normalized.use of combination therapies is becoming normalized.

Nicotine Agonist—VARENICLINE
Chantix, marketed by PfizerChantix, marketed by Pfizer Partial nicotinic receptor agonistPartial nicotinic receptor agonist
– Approved by the FDA May 2006, to hit the market in the Approved by the FDA May 2006, to hit the market in the fall of 2006fall of 2006
– Much DTC marketing anticipated in 2007Much DTC marketing anticipated in 2007
Early trials (JAMA) show better results than Early trials (JAMA) show better results than bupropionbupropion
Lessens withdrawal symptoms and inhibits Lessens withdrawal symptoms and inhibits the “buzz” from a smokethe “buzz” from a smoke
Main side effect is nauseaMain side effect is nausea

VARENICLINE:Mechanism of Action
Binds with high affinity and selectivity at 42 neuronal nicotinic acetylcholine receptors
– Stimulates low-level agonist activity
– Competitively inhibits binding of nicotine
Clinical effects
symptoms of nicotine withdrawal
– Blocks dopaminergic stimulation responsible for reinforcement & reward associated with smoking

VARENICLINE: Dosing
Patients should begin therapy 1 week PRIOR to their
quit date. The dose is gradually increased to minimize treatment-related nausea and
insomnia.Treatment Day Dose
Day 1 to day 3Day 1 to day 3 0.5 mg 0.5 mg qdqd
Day 4 to day 7Day 4 to day 7 0.5 mg 0.5 mg bidbid
Day 8 to end of treatment*Day 8 to end of treatment* 1 mg bid1 mg bid
Initial dose titration
* Up to 12 weeks

VARENICLINE:Adverse Effects
Common side effects (≥5% and twice the rate observed in placebo-treated patients) include:
– Nausea
– Sleep disturbances (insomnia, abnormal dreams)
– Constipation
– Flatulence
– Vomiting

VARENICLINE:Advantages and Disadvantages
DISADVANTAGES May induce nausea in up
to one third of patients.
Post-marketing surveillance data not yet available.
ADVANTAGES Varenicline is an oral
formulation with twice-a-day dosing.
Varenicline offers a new mechanism of action for persons who previously failed using other medications.
Early industry-sponsored trials suggest this agent is superior to bupropion SR.

BUPROPION SR: Mechanism of Action
Atypical antidepressant thought to affect levels of various brain neurotransmitters
– Dopamine
– Norepinephrine
Clinical effects
– craving for cigarettes
– symptoms of nicotine withdrawal

BUPROPION SR: DOSING
Initial treatment 150 mg po q AM x 3 days
Then… 150 mg po bid Duration, 7–12 weeks
Patients should begin therapy 1 to 2 weeks PRIOR
to their quit date to ensure that therapeutic plasma levels of the drug are achieved.

BUPROPION SR: Advantages and Disadvantages
Disadvantages Seizure risk is increased. Bupropion SR should be
avoided or used with caution in patients with:– History of seizures or cranial trauma– Anorexia or bulimia nervosa– Medications that lower seizure threshold– Severe hepatic cirrhosis– Concurrent use of any form of Wellbutrin,
or any MAO inhibitor in preceding 14 days
– Patients undergoing abrupt discontinuation of alcohol or sedatives
Advantages Easy to use. Bupropion SR can
be used with NRT. Might be beneficial
for patients with depression.

Combination Therapy for the Heavily Addicted Smoker—Mayo
Clinic Style
Nicotine patchNicotine patch
– Strongest dose, can use more than oneStrongest dose, can use more than one
Shorter acting nicotine replacementShorter acting nicotine replacement
Bupropion SRBupropion SR

Comparative Daily Costs of Pharmacotherapy
Cost per day, in U.S. dollars
0 2 4 6 8
Nasal spray
Patch
Varenicline
Cigarettes (1 pack/ day)
Lozenge
Bupropion SR
Gum
Inhaler $6.07
$5.81
$5.73
$5.26
$3.91
$3.67
$4.22
$4.26
Graph reprinted with permission, Rx for Change, The Regents of the University of California, University of Southern California, and Western University of Health Sciences.

Long-Term (6 month) Quit Rates for FDA-Approved Cessation
Medications
0
5
10
15
20
25
30
Nicotine gum Nicotinepatch
Nicotinelozenge
Nicotinenasal spray
Nicotineinhaler
Bupropion Varenicline
Active drugPlacebo
Data adapted from Silagy et al. (2004). Cochrane Database Syst Rev; Hughes et al., (2004). Cochrane Database Syst Rev.; Gonzales et al., (2006). JAMA and Jorenby et al., (2006). JAMA
Graph reprinted with permission, Rx for Change, The Regents of the University of California, University of Southern California, and Western University of Health Sciences.
Per
cen
t q
uit 19.5
14.6
11.5
8.6
16.4
8.8
23.9
11.8
17.1
9.1
20.0
10.2 9.4
22.5

Combination Therapy: Patch Plus Bupropion SR
15.6%
16.4%
30.3%
35.5%
0% 5% 10% 15% 20% 25% 30% 35% 40%
Placebo
Nicotine patch
Bupropion
Nicotine patchplus bupropion
Jorenby et al. N Engl J Med 1999;340(9):685–691.
Percentage of patients quit at 12 months after cessation

0
10
20
30
No clinician Self-help Non-physician clinician Physician clinician
Estimated abstinence at 5+ months
1.0 1.1(0.9,1.3)
1.7(1.3,2.1)
2.2(1.5,3.2)
n = 29 studiesType of clinician
Fiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. USDHHS, PHS, 2000.
Effects of Clinician Interventions
Compared to smokers who receive no assistance from a clinician, smokers who receive such assistance are 1.7–2.2 times as likely to quit successfully for 5 or more months.

New Medications in the Pipeline
RimonabantRimonabant– Cannabinoid receptor inhibitorCannabinoid receptor inhibitor– Blocks reinforcing effects of nicotineBlocks reinforcing effects of nicotine– Also suppresses appetiteAlso suppresses appetite– In phase III trialsIn phase III trials– Not approved for smoking cessation by FDANot approved for smoking cessation by FDA
Nicotine VaccineNicotine Vaccine– Produces antibodies to nicotineProduces antibodies to nicotine– Reduces nicotine levels in animalsReduces nicotine levels in animals
CYP246 InhibitorsCYP246 Inhibitors– CYP246 is a hepatic enzyme that metabolizes nicotineCYP246 is a hepatic enzyme that metabolizes nicotine– Higher blood nicotine levels per cigarette smokedHigher blood nicotine levels per cigarette smoked– Could also increase potency of NRTCould also increase potency of NRT

JCAHO Core Measures
Community-Acquired PneumoniaCommunity-Acquired Pneumonia Acute MIAcute MI CHFCHF PediatricsPediatrics

National Rates for AMI, Heart Failure and Pneumonia Adult Smoking Cessation Counseling
Measures
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Rat
e
AMI Heart Failure Pneumonia

Adult Smoking Cessation Counseling Adult Smoking Cessation Counseling for Acute MI Patients for Acute MI Patients
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Rat
e
JCAHO (Nat'l) UHC UCSF

Adult Smoking Cessation Counseling Adult Smoking Cessation Counseling for CHF Patients for CHF Patients
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Rat
e
JCAHO (Nat'l) UHC UCSF

Adult Smoking Cessation Counseling Adult Smoking Cessation Counseling for PN Patients for PN Patients
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Rat
e
JCAHO (Nat'l) UHC UCSF


Treating Tobacco Dependence: 2003
Providers•5 A’s Training/Education•Reimbursement •Physician Leadership
Cessation•Group Classes•Free Medications•Telephone Support•Self-Help Materials•Prov-RN
Clinics•5 A’s Training•EMR Resources•Dissemination (TAR)•Resources: Primary Care, Specialties, Pediatrics, OB/GYN
Health System•Research > $800K•Leadership: ATMCRWJF, CDC, AAHP•Formal HSI Program
Target Groups•Disease Management•PHS employees•Web-Based•Women & Children•Clinical Programs
Community•TOFCO•Oregon Quitline•Business Case
Hospital-Based•Inpatient Program•Behavioral Health/CD
Evaluation•C.O.R.E.•Utilization•Grant Writing
SMOKER(who wants to quit)

Smoking Prevalence: Providence Health Plan vs. Oregon
15%16%17%18%19%20%21%22%23%24%
'88 '89 '90 '91 '92 '93 '94 '95 '96 '97 '98 '99 2000
State of Oregon (BRFS) Providence Health Plan: Oregon

The National Quitline Card
—

Toll-free Quitline Numbers
1-800 NO BUTTS (California number)
1-800 QUIT NOW (National number)

Efficacy and Average Sample Size of Tobacco Cessation Studies
Reviewed by the Cochrane Library†
Type of Intervention Odds Ratio (95% CI*)Average Sample Size,
per trial
Nicotine Replacement Therapy (NRT, n=98*)
1.74 (1.64, 1.86) 385
Telephone Counseling (TC, n=13*)
1.56 (1.38, 1.77) 1,100
*n indicates number of studies; CI. Confidence interval.*n indicates number of studies; CI. Confidence interval.††Based on Silagy et al. (2004) and Stead et al. (2004). Based on Silagy et al. (2004) and Stead et al. (2004). The Cochrane Library.The Cochrane Library.

Knowledge of Tobacco Cessation Programs Among Knowledge of Tobacco Cessation Programs Among California SmokersCalifornia Smokers††
METHODUnaided Recall Aided Recall
% (95% CI*) % (95% CI*)
Telephone quitline 4.5 (1.1) 38.7 (2.6)
NRT 59.5 (2.5) --
Hypnosis 9.8 (1.5) --
SmokEnders 4.5 (1.1) --
Others 46.3 (2.9) --
† † Data from the California Tobacco Survey, 1999. For the unaided recall Data from the California Tobacco Survey, 1999. For the unaided recall question, survey respondents were asked, “Can you name up to 3 programs question, survey respondents were asked, “Can you name up to 3 programs that are helpful to people who are trying to quit smoking?” The aided recall that are helpful to people who are trying to quit smoking?” The aided recall question was asked only in reference to the quitline: “Have you ever heard of question was asked only in reference to the quitline: “Have you ever heard of the 1-800-NO-BUTTS (or, in Spanish, 1-800-45-NO-FUME) phone number?”the 1-800-NO-BUTTS (or, in Spanish, 1-800-45-NO-FUME) phone number?”
* CI = confidence interval.* CI = confidence interval.

Call Volume to the Quitline in response to New York City Free Patch Give-Away
Program41
182
2368
4099
558
5877
969
3010
1526
1258
1326
991
389
251
749
844
875
801
5374
1269
674
2034
1025
993
856
799
391
301
874
810
705
661
595
1984
287
894
862
636
611
2342
428
1368
910
613
613
0
50000
100000
150000
200000
250000
300000
4/2/034/9/03
4/16/034/23/03
4/30/035/7/03
5/14/03
(>425,000 calls in first 3 days!!!)

Barriers to Successful Cessation
Provider inattention/pessimism Co-dependency and mental illness No coverage for cessation medications Improper use of the medications Ignorance of toll-free tobacco quitlines

Strategies for Increasing Quit Rates
Reframe expectations of success Help businesses to help their employees
quit Focus on mental health/substance abuse
population Improved marketing of quitlines Develop new medications Create better systems Provide clinical champions

Services (short name)Services (short name) Current % receivingCurrent % receiving Additional QALYs saved if Additional QALYs saved if services nationallyservices nationally current % receiving services current % receiving services
increased to 90%increased to 90%
Tobacco Use Screening andTobacco Use Screening and 35%35% 1,300,0001,300,000
Brief InterventionBrief Intervention
Colorectal Cancer ScreeningColorectal Cancer Screening 35%35% 310,000310,000
Influenza Vaccine—AdultsInfluenza Vaccine—Adults 35% among adults 50-64 yrs35% among adults 50-64 yrs 110,000110,000
65% among adults 65+ yrs65% among adults 65+ yrs
Breast Cancer ScreeningBreast Cancer Screening 68%68% 91,00091,000
Cervical Cancer ScreeningCervical Cancer Screening 79%79% 29,00029,000
Pneumococcal Vaccine—AdultsPneumococcal Vaccine—Adults 56%56% 16,00016,000
Cholesterol ScreeningCholesterol Screening 87%87% 12,00012,000
*Priorities for America’s Health: Capitalizing on Life-Saving Cost-Effective Preventive *Priorities for America’s Health: Capitalizing on Life-Saving Cost-Effective Preventive Services.Services.
Partnership for Prevention: Additional QALYs Saved if Current % Receiving Services Increased*

Power of Intervention
⅓ to ½ of the 44.5 million smokers will die from the habit. Of the 31 million who want to quit, 10 to 15.5 million will die from smoking.
Increasing the 2.5% cessation rate to 10% would save 1.2 million additional lives.
If cessation rates rose to 15%, 1.9 million additional lives would be saved.
No other health intervention could make such a difference!