Carolinas Coast: A One-Stop Shop for Marine Observations in the Carolinas

4/4/2016
1
Patrick Coyne, MSN, ACHPN, ACNS-BC, FAAN, FPCN
What is Pain?
• A complex constellation of unpleasant sensory, perceptual and emotional experiences.
• Associated with autonomic, psychologic, emotional and behavioral responses.
• It tells you something is wrong, serves a purpose.
“Pain is whatever the person who experiences it says it is, existing whenever he/she says it does.”
Margo McCaffrey, Pain Specialist

4/4/2016
2
Physiological Effects of Pain• Increased catabolic demands: poor wound healing,
weakness, muscle breakdown
• Decreased limb movement: increased risk of DVT/PE
• Respiratory effects: shallow breathing, tachypnea, cough suppression, increasing risk of pneumonia and atelectasis
• Increased sodium and water retention
• Decreased gastrointestinal motility
• Tachycardia and elevated blood pressure
• Immunologic: decreased natural killer cell counts*
*Koga, et al. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001 Jun;91(6):654-8.
Psychological Effects of Pain
• Negative emotions: anxiety and depression
• Sleep deprivation
• Existential suffering
Barriers to Pain ControlHealth Care Professionals
• Inadequate assessment of pain and pain relief (MOST COMMON).
• Lack of understanding of the pathophysiology of pain.
• Lack of understanding of the clinical pharmacology of analgesics.
• Lack of knowledge of new methods to control pain to include adjunct drugs and neurosurgical procedures.

4/4/2016
3
Barriers to Pain ControlHealth Care Professionals, continued
• Lack of knowledge of the difference between physical dependence and addiction.
• Excessive concern about adding opioids.
• The belief that pain should be severe before patients receive opioid medication.
• The belief that patients are not good judges of the severity of their pain.
• Assignment of low priority to pain management.
• The difficult and frustrating nature of certain pain management problems
Barriers to Pain ControlThe Healthcare System
• Lack of accountability for pain management because hospitals have historically operated on an acute, disease-oriented model.
• Lack of coordination of care as patients move from one setting to another.
• Lack of contact with patients who have returned home.
• Fragmentation of care.
• Unwillingness of certain pharmacies to stock opioids because of risk of theft.
• In rural areas, resources may be limited.
Barriers to Pain ControlPatients and family members
• Lack of awareness that pain can be managed; patients may often suffer in silence.
• Fear that narcotics will lead to addiction. • Fear that use of analgesics will lead to confusion,
disorientation and/or personality changes.• Failure to report pain in a desire to be a “good
patient” and not distract physicians from treating the disease.
• Under-reporting of pain as a form of denial of disease progression or sparing family.

4/4/2016
4
Scope of the Problem• At least 50% of all cancer patients have pain.
• >70% of patients with advanced cancer have pain with pain intensity moderate to severe in 50% and excruciating in 30% .
• 50-80% of cancer patients do not obtain satisfactory pain relief.1
• Surgery: 33-88% of patients experience moderate to severe postoperative pain 2,3
1Cleeland CS et al. N Engl J Med. 1994 Mar 3;330(9):592-6.2Donovan BD. Anaesth Intensive Care. 1983 May;11(2):125-9.3 Svensson I, Siostrom G, Haliamae H. J Pain Symptom Manage 2000 Sep:20(3):193-201,
Singer 2015
4
4
4
Cancer Patients’ Beliefs about Pain Control
Belief % Agreeing
Addiction is a danger with pain meds 79
Side effects cannot be controlled. 61-85
A choice might be necessary between treating the disease and the pain
60
Pain medicine should be “saved” for when the pain is severe, otherwise it might become ineffective.
59
AHCPR Cancer Pain Guidelines; 1994
Populations at Risk for Inadequate Analgesia
• Women• Elderly• Minorities• Children• The Poor• Nursing home residents• Past/active injecting drug users• Patients with language/communication issues• Patients of a different educational/cultural or
socioeconomic background than their caregiver

4/4/2016
5
Reasons for Special Needs
• Limited verbal communication
• Lack of advocate
• Differences from health caretakers
• Stigmatization
• Differences in reactions to medications
• Physical and emotional dependence
• Inability to consent
• Lack of adequate research
Patients with Limited Communication Skills
• May give up hope after a few days of pain
• May not mention pain or demonstrate pain behaviors
• May be apathetic, listless, depressed
• Need a careful assessment
• Consider diagnostic/therapeutic trial of analgesics

4/4/2016
6
The Role of Pain / Symptom Assessments• Pain relief achieved
• Pain rhythms
• Precipitating factors
• Presence of side effects
• Constipation Nausea / vomiting
• Infection Pruritus
• Sedation Weakness
Pain Assessment
• Pain and medication history
• Location, character, intensity, frequency
• Aggravating and relieving factors
• Meaning of the pain to the person
• What pain level is tolerable?
• Type of pain: somatic, visceral, neuropathic?
Principles of Opioid Therapy: Equianalgesia
• Determine equal doses when changing opioid medications or routes of administration.
• Use of morphine equivalents helpful

4/4/2016
7
Principles of Opioid Analgesic Use in Acute and Cancer Pain (cont)
• When changing to a new opioid or different route• Use equianalgesic dosing table to estimate new dose
• Modify estimate based on clinical situation
• Recognize and treat side effects
• Be aware of potential hazards of meperidine / mixed agonist-antagonists - particularly pentazocine
• Do not use placebos to assess nature of pain
Principles of Opioid Analgesic Use in Acute and Cancer Pain (cont)
• Watch for development of:• Tolerance - treat appropriately
• Physical dependence – prevent withdrawal
• Do not label a patient psychologically depend, “addicted”, if you mean physically dependent on / tolerant to opioids
• Be alert to psychological side of patient
Principles of Opioid Therapy
• If severe pain, may need admission for IV, then may titrate quickly; patients may require 50-100% dose increases hourly, depending on drug half life. Use PCA so patient may determine.
• Once optimum dose is determined, convert to long-acting, sustained-release medication, egextended MS, Oxycodone (oxycontin) or methadone.
• Also breakthrough opioid of 10-20% of total daily scheduled dose.
• Reassess within one week.

4/4/2016
8
Principles of Opioid Therapy
• For chronic pain, use scheduled medication. PRN will cause a patient to have uneven pain relief.
• Titrate scheduled oral medication every 2-3 days. Consider sustained release or long-acting opioids such as MS Contin, Oxycontin, Methadone.
• Also provide a breakthrough dose, which should minimally equal 10-20% of the
• 24-hour opioid requirement.
Principles of Opioid Therapy:Rotation of Opioids
• Use when one opioid seems to lose its effectiveness.
• Use when adverse effects.
• Example: tremendous nausea with morphine; may need to switch to methadone or hydromorphone (Dilaudid®)
Methadone
• May be more effective in neuropathic pain syndromes than other opioids
• More potent than previously reported
• Patient may require significantly lower doses resulting in less side effects
• $ - Inexpensive

4/4/2016
9
Comparing Methadone & Morphine (Ripamonti & Bianchi 2002)
Characteristic Methadone Morphine
Oral
Bioavailability80% 35%
Half life 12- 190 hours 3-4 hours
Active
MetabolitesNO YES
Influenced by
renal disease+ +++
Influenced by
liver disease+++ +
• Good news – methadone provides another opioid for rotation, it may have benefit for neuropathic pain, it is cost-effective
• Bad news – complicated to use; long half-life, prolonged QT interval; drug-drug interactions
Good News/ Bad News
Inducers That May DecreaseMethadone Effects
• Abacavir
• Amprenavir
• Barbiturates
• Carbamazepine
• Cocaine
• Dexamethasone
• Efavirenz
• Ethanol (chronic use)
• Fusidic Acid
• Heroin
• Lopinavir+Ritonavir
• Nelfinavir
• Nevirapine
• Phenytoin
• Rifampin
• Spironolactone
• St. John’s wort
• Tobacco
• Urinary acidifiers
Leavitt (2005) Addiction Treatment Forum 3rd Ed. Methadone

4/4/2016
10
Inhibitors That May IncreaseMethadone Effects
• Cimetidine
• Ciprofloxacin
• Delavirdine
• Diazepam
• Diltiazem
• Disulfiram
• Ethanol (acute use)
• Fluconazole
• Grapefruit
• Haloperidol
• Ketoconazole
• Macrolides (erythromycin, clarithromycin)
• Metronidazole
• Omprazole
• SSRI(fluoxetine, paroxetine, nefazodone, sertraline)
• Urinary alkalinizers
• Verapamil
Leavitt (2005) Addiction Treatment Forum 3rd Ed. Methadone
Co Analgesics Commonly Used For Pain
• NSAIDS
• Acetaminophen
• Antidepressants
• Anticonvulsants
• Corticosteroids
• Neuroleptics
• Antihistamines
• Analeptics
• Benzodiazepines
• Antispasmodics
• Muscle relaxants
• Systemic local anesthetics
Adjuvant analgesics for neuropathic pain
• Anticonvulsants
• Tricyclic antidepressants
• Local anesthetics
• Corticosteroids (may also be used for other types of pain)
• Baclofen
• Capsaicin topical

4/4/2016
11
Adjuvants for pain relief include:
• Biphosphonates
• Palliative chemotherapy
Ketamine
Ketamine was developed as an anesthetic. It has weak primary analgesic properties when used by itself in smaller doses. In other circumstances and uses, however, it exerts strong adjuvant analgesic properties by inhibiting the binding of glutamate to the NMDAR, (N-methyl-D-aspartate-receptor blockade) which is probably its most critical mechanism of action. Appears to have a synergistic effect with opioids, Case reports show effectiveness when traditional and invasive techniques fail. Okon 2007
Ketamine
There is no agreement on a single, uniform best Ketamine protocol or dose. Instead, various local, idiosyncratic approaches are used. One typical, intermittent dosing schedule is 0.25-0.50 (0.60) mg/kg tid or qid. While some practitioners use the intravenous route, others prefer oral delivery . Most start at a dose of0.25–0.50 mg/kg Mercadante , Arcuri, Tirelli ,et al 2000; Kannan TR, Saxena A, Bhatnagar S,2002

4/4/2016
12
Ketamine
Some consider the routine use of a small dose of benzodiazepine or neuroleptic while initiating treatment to minimize the psychotomimetic side effects.
Ketamine
Adverse cardiovascular effects are not infrequent and include increased blood pressure and tachyarrhythmias. Neurologic adverse effects include increased intracranial pressure, and increased muscle tone. Cognitive complications are frequent and manifest as issues such as alterations in body image and mood, floating sensations, vivid dreams, hallucinations, delirium, and drowsiness.
Cocaine
• Cocaine was the first local anesthetic to be used clinically and is still used topically for minor lacerations and nasal or dermatologic procedures, due to its vasoconstrictive and pain relieving properties. Review of the literature, however, reveals that it has not been described for repeated dosing for oral or other mucosal pain. Potential side effects of mucosal administration include gingival recession and erythematous lesions. If the recommended topical doses are exceeded, liquid cocaine may be absorbed systemically causing a stimulant response or addiction. When used appropriately, this intervention can result in a dramatic improvement in quality of life and functional status.

4/4/2016
13
Topical Cocaine
• 4% applied to topical areas of pain, up to 5ml q6 prn
• Used successfully in head and neck, gyn cancers and mucusitisfrom BMT/Chemo .
Newport and Coyne 2010
Dexmedetomidine• Dexmedetomidine (Precedex) is an alpha-2 adrenergic agonist
with sedative and analgesic properties.Significantly more potent (7-8 times more alpha-2 selective) than clonidine.
• The major clinical concern associated with the use of dexmedetomidine is the potential for cardiovascular depression including hypotension and bradycardia
• This drug nay offer a bridge to effective pain management , very costly.
Coyne, Wozencraft et al 2010
Dexmedetomidine
• Dexmedetomidine (Precedex) is an alpha-2 adrenergic agonist with sedative and analgesic properties. Significantly more potent (7-8 times more alpha-2 selective) than clonidine. The major clinical concern associated with the use of dexmedetomidine is the potential for cardiovascular depression including hypotension and bradycardia
• This drug may offer a bridge to effective pain management , very costly.
Wozencraft, Coyne et al 2012, Roberts, Wozencraft ,et al AL 2011 ;Coyne, Wozencraft et al 2010

4/4/2016
14
Dexmedetomidine
Usual starting dose is 0.2mcg/kg/hour, e.g. (0.2)(70kg)=14 mcg/hour
Check vital signs pre-infusion and every 15 minutes after starting or increasing dose , if stable after 30 minutes check every 30 minutes for 3 hours, then every 4 hours for a 24 hour total.
Infusion may be increased by 0.1 mcg/kg every 30 minutes until pain is controlled.
Do NOT increase if heart rate drops below 80, systolic blood pressure drops below 100, or either decreases by > 30% of the pre-infusion baseline. Depending of goals of care a monitored bed may be appropriate. Coyne et al 2010
• Some studies demonstrate long-lasting pain relief even after drug has been stopped
• More effective in neuropathic pain but can be used for all pain syndromes.
• Starting dose 0.5mg-2 mg/kg per hr IV or SC.
• We give 100mg in 30 minutes and re evaluate.
Intravenous Lidocaine
Ferrini,Paice, 2004
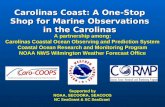
Pain
Step 1
Nonopioid
Adjuvant
Pain persisting or increasing
Step 2
Opioid for mild to moderate pain
Nonopioid Adjuvant
Pain persisting or increasing
Pain persisting or increasing
Step 3
Opioid for moderate to severe pain
Nonopioid Adjuvant
Invasive treatments
Opioid Delivery
Quality of Life
Modified WHO Analgesic Ladder
Proposed 4th Step
The WHO
Ladder
Deer, et al., 1999

4/4/2016
15
Nerve Blocks: General Outcomes
• Well-controlled studies lacking
• Variable outcome
• Type of block, pain problem, underlying medical, and neurologic condition
• Significant relief in average of 50-80% of well-selected patients
• Duration tends to average 3-6 months
• Complications
• Significant in less than 5% of well-selected patients
Celiac Plexus and Splanchnic Nerve Block• Especially for pancreatic cancer
• Associated with a high incidence of intractable pain
• Characteristically mid-epigastric - radiation to back
• Deep, peri-aortic structures
• Commonly used - effective in about 80-95% of cases
• Despite location near major organs complication rates uniformly low (usually under 1%)
• Requires radiologic control (fluoroscopy or CT)
• Some research demonstrates increased QOL/survival
• (Staats 2002)
Patients who might benefit
from implantable drug delivery systems (IDDS)
• Over 3 months to live…realistically.
• Pain scores ≥ 5
• Morphine Oral Equivalent Doses ≥ 200 mg/day• or intolerable side effects
• No active infection
• No heparin
• No barrier to CSF flow
• Oncologist and Pain Manager collaboration
• Someone can manage the IDDS after insertion

4/4/2016
16
Key Findings
Pain Reduction: 52% improvement in pain relief or 12% reduction in pain scores over CMM alone
Toxicity Reduction: 50% reduction in composite drug-related toxicity at 1 month OR 33% reduction in composite drug-related toxicity at 1 month over CMM alone.
Pain Relief Techniques
• Central technique• Alter cognitive, affective and evaluative responses to pain
• Prepatory information• Temporal and sensory
• Reduce anxiety
• Cognitive strategies• Involves mental activity to alter the evaluation of sensations
as painful, more perceived control
• Distraction, imagery (future oriented, positive self statements), hypnosis, cognitive rehearsal, systematic desensitization, relaxation
Non-Pharmacologic Techniques of Pain Control
• Utilize interdisciplinary colleagues
• Anesthesia, neurosurgery
• General surgery
• Radiation

4/4/2016
17
Essential Points About Psychological Methods
• They are not alternatives - used in conjunction with medical methods
• You use these approaches
• Used with awareness – more effective
• Most effective when used early – not as last ditch efforts after everything else fails
Non-Pharmacologic Techniques of Pain Control
• Cognitive-behavioral therapy, eg relaxation, imagery, distraction, prayer
• Physical measures: heat, cold, massage
• Complementary therapies: acupuncture and acupressure
What is Scrambler Therapy?• Substitute pain information with synthetic
"non- pain" information, created by digitally
synthesizing 16 different kinds of action
potentials with variable geometry very similar
to the endogenous kind.
• Scrambler therapy does not inhibit pain
transmission (through A-beta fiber excitation) –
can still feel sensations.
• ST may relieve pain by exciting C fibers (that
carry nocioceptive impulses) with “non-pain
information”, at energies that do not stimulate
pain impulses.
• FDA and EuroMark approved
• It is not TENS (simple on/off current, effect
disappears when off).

4/4/2016
18
What is Scrambler Therapy?
• ST delivers “non-pain” information by simulating 5 external artificial neurons with digitally synthesized action potentials assembled into packets of information strings.
• Each new packet is created with an algorithm that takes into account the previous outputs, dynamically modifying four main variables.
• type of action potential (16 different possible combinations)
• packet associated frequency (from 43 to 52 Hz) and duration 6.8-10.9 msecs
• packet time duration (0.7 - 10 sec)
• the amplitude of modulation.
• The system quickly tries different combinations until pain relief is achieved. (The technical details are described in patent number PCT/IT2007/000647.)
• The electrical charge used in Scrambler therapy is low and SAFE; at the highest setting, the amperage (A) is 3.50mA-5.50mA, and the maximum current density is only 0.0002009 Watts/cm².
• TENS uses a continuous pulse pattern with pulse width of 200 microseconds, and a pulse frequency of 80 Hz.
1. Scrambler therapy appears to work, is non-toxic, non-invasive, and relatively inexpensive.
2. Designing trials that answer the question “Does it work?” is difficult. But must be done.
3. So far, all 20 trials are positive, with no harm, an excellent safety record, and the possibility of changing the management of chronic pain.
What explains the effect of acupuncture?
• Does accupuncture work locally, at the spinal cord, at the brain, or all of the above?
• “…compromised nerve conduction in PN mainly depends on structural changes of the myelin sheaths, while the amplitude is correlated with the number of functional axons…”
• Nerve conduction velocity and amplitude was near 0 and improved in acupuncture treated patients.

4/4/2016
19
General Strategies to Control Pain• Diagnose and treat source whenever possible
• Antibiotics, chemotherapy, radiotherapy, surgery
• Immediately begin treatment of pain with analgesics
• Start with opioid for moderate to severe pain
• Individualize therapy
• Use adjuvants and nonpharmacologic modalities to supplement analgesia
• Interruption of pain transmission with nerve blocks or neurosurgery is infrequently indicated
• Provide analgesia during diagnosis and treatment of underlying disease processes
General Principles of Pharmacotherapy in Pain• Around-the-clock (ATC) administration of long-
acting opioids is preferred for chronic or persistent pain
• Short-acting analgesics are useful for intermittent pain and as supplements for breakthrough pain
• Dose of long-acting opioid should be increased if frequent rescue doses are needed
• Opioid tolerance and physical dependence do not equal addiction
• The least invasive modalities (Oral, transdermal, rectal) should be used first

4/4/2016
20
ReferencesMarineo G.Untreatable pain resulting from abdominal cancer: new hope from biophysics? JOP. 2003 Jan;4(1):1-10.
Sabato AF, Marineo G, Gatti A. Scrambler therapy. Minerva Anestesiol. 2005 Jul-Aug;71(7-8):479-82.
Smith TJ, Coyne PJ, Parker GL, Dodson P, Ramakrishnan V. Pilot Trial of a Patient-Specific Cutaneous Electrostimulation Device (MC5-A Calmare®) for Chemotherapy-Induced Peripheral Neuropathy. J Pain Symptom Manage. 2010 Dec;40(6):883-91. doi: 10.1016/j.jpainsymman.2010.03.022. PMID:20813492
Abdi S, Lakkimsetty VM, Barrera J, Candiotti K, Lubarsky D. The Use of “Scrambler Therapy” for Failed Back Surgery Syndrome. Pain Physician 2011; 14: E465-491
Guiseppe M, Vit torio I, Cristiano G, Vincenzo M, Smith TJ. MC5-A Scrambler Therapy Relieves Chronic Neuropathic Pain More Effectively Than Guideline Based Drug Management. Submitted.
Ricci M, Pirotti S, Scarpi E, Burgio M, Maltoni M, Sansoni E, Amadori D. Managing chronic pain: results from an open-label study using MC5-A Calmare® device. Support Care Cancer. 2012 Feb;20(2):405-12. Epub 2011 Mar 11.
Ghatak RK, Nandi SN, Bhakta A, Mandal GC, Bandyopadhyay M, Kumar S. Prospective study of application of biological communication (cybernatics) in management of chronic low back pain--a preliminary report. Nepal Med Coll J 2011; 13(4): 257-260 [PMID: 23016475]
Sparadeo F CK, S D'Amato. Scrambler Therapy: An Innovative and Effective Treatment for Chronic Neuropathic Pain. Journal of Life Care Planning 2012; 11(3): 3-15
Coyne PJ, Wan W, Dodson P, Swainey C, Smith TJ. A trial of scrambler therapy in the treatment of cancer pain syndromes and chronic chemotherapy-induced peripheral neuropathy. J Pain Palliat Care Pharmacother. 2013 Dec;27(4):359-64. doi: 10.3109/15360288.2013.847519. Epub 2013 Oct 21. PMID:24143893
Smith TJ, Marineo G. Treatment of Postherpetic Pain With Scrambler Therapy, a Patient-Specific Neurocutaneous Electrical Stimulation Device. The American journal of hospice & palliative care 2013 [PMID: 23838448 DOI: 10.1177/1049909113494002]
Ko YK, Lee HY, Lee WY. Clinical experiences on the effect of scrambler therapy for patients with postherpetic neuralgia. Korean J Pain. 2013 Jan;26(1):98-101. doi: 10.3344/kjp.2013.26.1.98. Epub 2013 Jan 4.
ReferencesPark HS, Sin WK, Kim HY, Moon JY, Park SY, Kim YC, Lee SC.Scrambler therapy for patients with cancer pain - case series -. Korean J Pain. 2013 Jan;26(1):65-71. doi: 10.3344/kjp.2013.26.1.65. Epub 2013 Jan 4.
Campbell T, Nimunkar AJ, Retseck J, Eickhoff JC, Backonja M, Cleary JF, Kwekkeboom KL, Yen TY. A randomized, double-blind study of “Scrambler” therapy versus sham for painful chemotherapy-induced peripheral neuropathy (CIPN). J Clin Oncol 2013; 31((suppl; abstr9635))
Pachman DR, Weisbrod BL, Seisler DK, Barton DL, Fee-Schroeder KC, Smith TJ, Lachance DH, Liu H, Shelerud RA, Cheville AL, Loprinzi CL. Pilot evaluation of Scrambler therapy for the treatment of chemotherapy-induced peripheral neuropathy. Support Care Cancer. 2015Apr;23(4):943-51. doi: 10.1007/s00520-014-2424-8. Epub 2014 Sep 24. PMID: 25245776
Sparadeo F, Kaufman C, D’Amato S. Scrambler Therapy: An Innovative and Effective Treatment for Chronic Neuropathic Pain. Journal of Life Care Planning, Vol. 11, No. 3, (3-15), 2012.
Moon JY, Kurihara C, Beckles JP, Williams KE, Jamison DE, Cohen SP. Predictive Factors Associated with Success and Failure for Calmare (Scrambler) Therapy: A Multi-Center Analysis. Clin J Pain. 2014 Sep 17. [Epub ahead of print]
Starkweather AR, Coyne P, Lyon DE, Elswick RK Jr, An K, Sturgill J. Decreased Low Back Pain Intensity and Differential Gene Expression Following Calmare®: Results From a Double-Blinded Randomized Sham-Controlled Study. Res Nurs Health. 2015 Jan 8. doi: 10.1002/nur.21632. [Epub ahead of print]
Pachman DR, Cheville AL, Shelerud RA, Linquist BM, Fee-Schroeder KC, Smith TJ, Lachance DF, Seisler DR, Loprinzi CL. Pilot Evaluation of Scrambler Therapy for the Treatment of Chronic Low Back Pain. Spine, submitted.
Notaro P,2, Dell'Agnola CA, Dell'Agnola AJ, Amatu A, Bencardino KB, Siena S. Pilot evaluation of scrambler therapy for pain induced by bone and visceral metastases and refractory to standard therapies. Support Care Cancer. 2015 Sep 26. [Epub ahead of print]
Sang Chul Lee, Keun Suk Park, Jee Youn Moon, Eun Jung Kim, Yong-Chul Kim, Hyejin Seo, Joon Kyung Sung, Da Jeong Lee. An exploratory study on the effectiveness of “Calmare therapy” in patients with cancer-related neuropathic pain: A pilot study. European Journal of Oncology Nursing 21 (2016) 1e7
Compagnone C, Tagliaferri F; Scrambler Therapy Group. Chronic pain treatment and scrambler therapy: a multicenter retrospective analysis. Acta Biomed. 2015 Sep 14;86(2):149-56.
• Burton, A.W., et al. (2011). Pain Medicine, 12, 1750-1757.
• Coyne, P.J., et al. (2010). Journal of Pain Palliative Care Pharmacotherapy, 24, 384-386.
• Coyne, P.J., et al. (2005). Clinical Journal of Oncology Nursing, 9, 581- 583.
• Ferrini R &Paice JA. Journal of Supportive Oncology, 2004; 2: 90-94
• Glare & Walsh (1991). Therap Drug Monit Gourlay. (2001). Lancet Oncology
• Kannan, et al. (2002). Journal of Pain and Symptom Management , 23: 60-65.
• Krajnik, et al. (1999). Pain
• Krotscheck U, et al. (2004). Vet Therapy, 5: 202-211
• Mercadante (2000). Journal of Pain and Symptom Management ,20:246-252.
• Newport K, and Coyne P. (2010). Journal of Pain Palliative Care Pharmacotherapy , 24:149-51.
References

4/4/2016
21
• Okon T. (2007). Pain Physician, 10: 493-500
• Paice JA, et al. (2011) Journal of Supportive Oncology, 9:129–133
• Paice JA, et al. (2008). Journal of Pain and Symptom Management, 35: 314-320
• Ribeiro, et al. (2004). Journal of Pain and Symptom Management,
• Roberts SB, et al. (2011). Journal of Palliative Medicine, 14: 371-373
• Smith TJ, et al. (2012). Journal of Pain and Symptom Management , 43: 961-966
• Smith, T., Coyne, P.J., Parker, G.L., Dodson, P.,& Ramakrishnan, V. (2010). Journal of Pain and Symptom Management
• Smith TJ, et al. (2002). Journal of Clinical Oncology, 20: 4040-4049
• Stuart-Harris, et al. (2000). British Journal of Clinical Pharmacology,
• Ward, et al. (1997). Clin Pharmacol Ther 1997
• Wilken et al. (2005). Journal of Pain Palliative Care Pharmacotherapy
• Whitcomb et al. (2002). Current Pain Headache Reports, 6:183-190
References (cont’d)


















