GESTATIONAL TROPHOBLASTIC TUMORS (GTT) GESTATIONAL TROPHOBLASTIC Disease (GTD)

© ESPEN 2003 - For personal use only. 1
ESPEN Congress Cannes2003
Organised by the Israel Society for ClinicalNutrition
Session: Dietitian Symposium: Nutrition throughout the woman life cycle
An Update in the Nutritional Management ofGestational Diabetes
Doctor Gary Frost And Doctor Anne DornhorstLondon, United Kingdom
email [email protected]
Education and Clinical Practice Programme
What is gestational diabetes?• Find definition
– WHO– This is based on risk if type 2 diabetes
• Not clear what level of glucose causes problems for thefetus– HAPO Study (hyperglycaemic adverse pregnancy outcome study)
– 25,000 pregnant women with lesser degrees of glucose tolerancewill answer this.
• Detrimental maternal effects– Type 2 diabetes– CHD

© ESPEN 2003 - For personal use only. 2
General Dietary Recommendation
• Poor evidence base– Cochrane systematic review – 4 studies reached
the quality for consideration– No relationship between dietary intervention
and final birth weight, risk of LGA infant ormethod of delivery
– Poorly designed– Small underpowered studies
General nutrition adviceapplies
• Folate• Iron• Vitamin C• Calcium and Vitamin D• Alcohol

© ESPEN 2003 - For personal use only. 3
Hyperglycaemia and the Fetus
1st trimester congenital malformations
2nd trimester fetal cell programming
3rd trimester fetal growth & stillbirth
Extra-uterine Sequelle of IntrauterineHyperglycaemia
Neonate transient hypoglycaemia; hypocalcaemia, cardiomyopathy
Adolescent obesity, IGT and insulin resistance
Adulthood obesity, type 2 DM and ?CVD

© ESPEN 2003 - For personal use only. 4
Fetal Fuels
• Metabolic changes occur throughout pregnancy to ensureoptimal fetal growth.
• Metabolic changes occur to maximise the maternal-fetaltransfer of glucose.
• Maternal glucose is the primary fetal oxidative substrateand, by late pregnancy, 17- 26g glucose are metabolisedper day.
• The maternal respiratory quotient rises during pregnancyas fetal carbohydrate metabolism increases .
Barker in reverse: High birth weightand Adult disease
• Lasting structural and functional adaptation to excess fetalnutrient supply
• Fetal insulin a key fetal growth factor, determines fat andmuscle mass at birth
• Fuel-mediated teratogenesis that effects the adipoinsularaxis, leading to insulin resistance, childhood obesity andfuture diabetes
• There is a ‘U’ shape relationship between birth weight andfuture type 2 diabetes

© ESPEN 2003 - For personal use only. 5
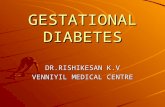
Diagnosed Type 2 Diabetes USA Prevalence Data
Per
son
s W
ith
Dia
gn
ose
dD
iab
etes
(m
illio
ns)
Diabetes Overview. October 1995 (updated 1996). NIDDK publication NIH 96-1468.Kenny SJ et al. In: Diabetes in America. 2nd ed. 1995:47-67.
Year
8
7
6
5
4
3
2
0
1
1958 1963 1968 1979 1984 1989 1994
8,000,000
5X increase
Obesity – Past and Future

© ESPEN 2003 - For personal use only. 6
Disease Risk and Body Mass
Increasing US Prevalence of Type 2 Diabetes in1990-1998
Diagnosed type 2 Diabetes È 4.9% - 6.5%
40-49 yr. È 40%
30-39 yr. È 70%
Type 2 diabetes is increasing USA teenagers
Mokdad et al, Diabetes trends in the U.S.: 1990-1998. Diabetes Care, 2000. 23: p. 1278.

© ESPEN 2003 - For personal use only. 7
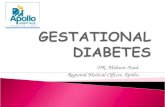
Pima Indian in Arizona
Maintained traditionallifestyle up until 1900 whenwater supply was diverted bywhite farmers and theybecome dependent on U.S.government supply of food -lard, sugar,white flour
Pima Indian Woman 1902
Pima Indiansenvironment verses genes
•The Pima Indians from Arizona have changed from a subsistence existence to Western lifestyle
•Pima Indian ancestors live in a mountainous remote undeveloped area of NW-Mexico
Ravussin et al Diabetes Care 1994 17:1067-1074

© ESPEN 2003 - For personal use only. 8
Increasing Prevalence of Type 2 DM inPima Indian Girls
0
1
2
3
4
5
6
Prav
elen
ce %
1967-1976
1977-1986
1989-1996
5-9yrs 10-14yrs 15-19yrs
5274 children examined over 30years. The prevalence hasincreased 2-3 fold over this time
Dabelea et al. J Matern-Fetal Med 2000;9:83-88
Prevalence of Type 2 DM Accordingto Maternal Diabetic Status
Dabelea et al. J Matern-Fetal Med 2000;9:83-88
0
10
20
30
40
50
60
70
80
Prav
elenc
e %
5-9. 10-14. 15-19. 20-24. 25-29. 30-34.
years
Non-DM Pre-DM DM

© ESPEN 2003 - For personal use only. 9
The Lasting Legacy of MaternalHyperglycaemia
• Maternal hyperglycaemia accounts for 40% of Type 2 DMin the Pima children <19-yrs.
• There is an increased risk of Type 2 DM in children ofType 1 mothers, and the risk appears dependent onglycaemic control in pregnancy.
• Likely to explain the higher maternal than paternal familyhistory of DM.
Obesity management
• Population based:– Obesity is a major public health problem
– To prevent GDM need to prevent obesity

© ESPEN 2003 - For personal use only. 10
-8
-6
-4
-2
0
0 1 2 3 4
Years from Randomization
Weig
ht
Ch
an
ge (
kg
)
Placebo
Metformin
Lifestyle
Mean Weight Change
The DPP Research Group, NEJM 346:393-403, 2002
0 1 2 3 4
0
10
20
30
40Placebo (n=1082)Metformin (n=1073, p<0.001 vs. Plac)Lifestyle (n=1079, p<0.001 vs. Met , p<0.001 vs. Plac )
Percent developing diabetes
All participants
All participants
Years from randomization
Cu
mu
lativ
e in
cid
en
ce (
%)
Placebo (n=1082)
Metformin (n=1073, p<0.001 vs. Placebo)Lifestyle (n=1079, p<0.001 vs. Metformin , p<0.001 vs. Placebo)
Incidence of DiabetesIncidence of Diabetes
Risk reductionRisk reduction31% by 31% by metforminmetformin58% by lifestyle58% by lifestyle
The DPP Research Group, NEJM 346:393-403, 2002

© ESPEN 2003 - For personal use only. 11
Obesity management
In pregnancy• Dutch famine (800kcal/day) thin babies, more
diabetes• Maternal ketosis effects fetal neuro-physiological
and cognative development• Moderate energy restriction 25kcal/kg/day from 24th
week, limits weight gain, LGA reduced. Womenonly gained half weight of controls (Dornhorst 1991,Knopp 1991)
Long chain polyunsaturates
Hammersmith HospitalsNHS Trust ©

© ESPEN 2003 - For personal use only. 12
Long chainpolyunsaturates (LCPs)
• Man cannot insert double bonds atthe n3 and n6 positions in fattyacids
• therefore……….
Hammersmith HospitalsNHS Trust ©
Long chainpolyunsaturates (LCPs)
• Linoleic acid (double bonds at the n6 position)
• and
• Alpha linolenic acid (double bonds at the n3 position)
• are ESSETIAL FATTY ACIDS and are the precursorsof LCPs
Hammersmith HospitalsNHS Trust ©

© ESPEN 2003 - For personal use only. 13
Long chain polyunsaturates (LCPs)
Arachidonic acid (n6) : Docosahexaenoic acid (n3)
Ratio in brain
2:1
Hammersmith HospitalsNHS Trust ©
Development of the cortex24 weeks to term
Hammersmith HospitalsNHS Trust
©

© ESPEN 2003 - For personal use only. 14
Fish oils and gestational diabetes
• Insulin resistance & altered maternal metabolismin gestational diabetes impairs arachidonic acidand DHA.– Low levels in cord blood
• Impairment of accretion may effect fetal accretionof DHA and AA
• Maternal supplements effect IQ• Low consumption in many countries is a problem
Fish consumption
• Recent evidence suggested an increasespontaneous abortion rate in low fishconsuming countries
• Is this due to DHA?• Does a maternal background of abnormal
glucose tolerance decrease levels further?• Role in hypertensive crisis? Small study
evidence.

© ESPEN 2003 - For personal use only. 15
What is What is Glycaemic Glycaemic IndexIndex
Incremental area under the bloodglucose response curve for food
Corresponding area after equi-carbohydrate portion of glucose
X 100
Glycaemic response of carbohydrates
0
2
4
6
8
10
12
0 30 60 90 120
Time (minutes)
De
lta
ch
an
ge
in
glu
co
se
(m
mo
l/l)
White Bread Wholemeal Bead White pasta Kidney beans

© ESPEN 2003 - For personal use only. 16
Glycaemic Glycaemic indexindexFOOD
White bread
Wholemeal bred
Brown rice
White rice
Boiled potato
Pasta
YamGreen banana
Sucrose
Baked beans
Chickpeas
GI100
100
81
81
98
65
7465
83
70
60
Glycaemic index
• Potential of decreasing risk of developingtype 2 diabetes
• Potential of decreasing risk of CHD• Potential effect of decreasing body weight• Mechanism
– Improving insulin sensitivity• Adipose tissue
Summerbell and Frost. Systematic Review of glyceamic index, Cochrane Reviews 2003

© ESPEN 2003 - For personal use only. 17
Feto-placental growthregulation
Rate of substrate delivery to the placental site
Release of placental growth or suppressive peptides into the umbilical circulation
Production of IGF and IGFBP by the liver and othertissues
Rate of feto-placental growth
Clapp etal 1991
Glycaemic index in GDM
• Low GI meal causes a lower post-prandialinsulin and glucose response
• Low GI diet blunt the mid and late pregancyinsulin resistance
• High GI larger infants• Low GI limited energy intake, and weight
gain in the motherClapp Proc Nutr Soc 2003

© ESPEN 2003 - For personal use only. 18
Glycaemic index in GDM
• Low blood glucose measurement• Reduction in hypos• Improved fasting blood glucose
Gestational Diabetes:Potential Relevance of Diet
A important factor fuelling the current rise inadolescent obesity & type 2 DM
We need evidence of effective interventionsPotential areas of interest are:
Fish oilsCarbohydates

© ESPEN 2003 - For personal use only. 19
The End