What Influences Patient-Therapist Interactions in ...
14
What Influences Patient-Therapist Interactions in Musculoskeletal Physical Therapy? Qualitative Systematic Review and Meta-Synthesis Mary O’Keeffe, Paul Cullinane, John Hurley, Irene Leahy, Samantha Bunzli, Peter B. O’Sullivan, Kieran O’Sullivan Background. Musculoskeletal physical therapy involves both specific and nonspecific effects. Nonspecific variables associated with the patient, therapist, and setting may influence clinical outcomes. Recent quantitative research has shown that nonspecific factors, including patient-therapist interactions, can influence treatment outcomes. It remains unclear, however, what factors influence patient-therapist interaction. Purpose. This qualitative systematic review and meta-synthesis investigated patients’ and physical therapists’ perceptions of factors that influence patient-therapist interactions. Data Sources. Eleven databases were searched independently. Study Selection. Qualitative studies examining physical therapists’ and patients’ percep- tions of factors that influence patient-therapist interactions in musculoskeletal settings were included. Data Extraction. Two reviewers independently selected articles, assessed methodolog- ical quality using the Critical Appraisal Skills Programme (CASP), and performed the 3 stages of analysis: extraction of findings, grouping of findings (codes), and abstraction of findings. Data Synthesis. Thirteen studies were included. Four themes were perceived to influ- ence patient-therapist interactions: (1) physical therapist interpersonal and communication skills (ie, presence of skills such as listening, encouragement, confidence, being empathetic and friendly, and nonverbal communication), (2) physical therapist practical skills (ie, physical therapist expertise and level of training, although the ability to provide good education was considered as important only by patients), (3) individualized patient-centered care (ie, indi- vidualizing the treatment to the patient and taking patient’s opinions into account), and (4) organizational and environmental factors (ie, time and flexibility with care and appointments). Limitations. Only studies published in English were included. Conclusions. A mix of interpersonal, clinical, and organizational factors are perceived to influence patient-therapist interactions, although research is needed to identify which of these factors actually influence patient-therapist interactions. Physical therapists’ awareness of these factors could enhance patient interactions and treatment outcomes. Mechanisms to best enhance these factors in clinical practice warrant further study. M. O’Keeffe, BScPhysio, Depart- ment of Clinical Therapies, Univer- sity of Limerick, Health Sciences Building, Limerick, Ireland. Address all correspondence to Ms O’Keefe at: [email protected]. P. Cullinane, BScPhysio, Depart- ment of Clinical Therapies, Univer- sity of Limerick. J. Hurley, BScPhysio, Department of Clinical Therapies, University of Limerick. I. Leahy, BScPhysio, Department of Clinical Therapies, University of Limerick. S. Bunzli, BScPhysio, School of Physiotherapy, Curtin University of Technology, Perth, Australia. P.B. O’Sullivan, PhD, PGDip, School of Physiotherapy, Curtin University of Technology. K. O’Sullivan, PhD, MManipTher, BPhysio, SMISCP, MISOM, Department of Clinical Therapies, University of Limerick. [O’Keeffe M, Cullinane P, Hurley J, et al. What influences patient- therapist interactions in musculo- skeletal physical therapy? Qualita- tive systematic review and meta-synthesis. Phys Ther. 2016; 96:609 – 622.] © 2016 American Physical Therapy Association Published Ahead of Print: October 1, 2015 Accepted: September 13, 2015 Submitted: April 23, 2015 Research Report Post a Rapid Response to this article at: ptjournal.apta.org May 2016 Volume 96 Number 5 Physical Therapy f 609
Transcript of What Influences Patient-Therapist Interactions in ...
What Influences Patient-TherapistInteractions in MusculoskeletalPhysical Therapy? QualitativeSystematic Review and Meta-SynthesisMary O’Keeffe, Paul Cullinane, John Hurley, Irene Leahy, Samantha Bunzli,Peter B. O’Sullivan, Kieran O’Sullivan
Background. Musculoskeletal physical therapy involves both specific and nonspecificeffects. Nonspecific variables associated with the patient, therapist, and setting may influenceclinical outcomes. Recent quantitative research has shown that nonspecific factors, includingpatient-therapist interactions, can influence treatment outcomes. It remains unclear, however,what factors influence patient-therapist interaction.
Purpose. This qualitative systematic review and meta-synthesis investigated patients’ andphysical therapists’ perceptions of factors that influence patient-therapist interactions.
Data Sources. Eleven databases were searched independently.
Study Selection. Qualitative studies examining physical therapists’ and patients’ percep-tions of factors that influence patient-therapist interactions in musculoskeletal settings wereincluded.
Data Extraction. Two reviewers independently selected articles, assessed methodolog-ical quality using the Critical Appraisal Skills Programme (CASP), and performed the 3 stagesof analysis: extraction of findings, grouping of findings (codes), and abstraction of findings.
Data Synthesis. Thirteen studies were included. Four themes were perceived to influ-ence patient-therapist interactions: (1) physical therapist interpersonal and communicationskills (ie, presence of skills such as listening, encouragement, confidence, being empatheticand friendly, and nonverbal communication), (2) physical therapist practical skills (ie, physicaltherapist expertise and level of training, although the ability to provide good education wasconsidered as important only by patients), (3) individualized patient-centered care (ie, indi-vidualizing the treatment to the patient and taking patient’s opinions into account), and (4)organizational and environmental factors (ie, time and flexibility with care and appointments).
Limitations. Only studies published in English were included.
Conclusions. A mix of interpersonal, clinical, and organizational factors are perceived toinfluence patient-therapist interactions, although research is needed to identify which of thesefactors actually influence patient-therapist interactions. Physical therapists’ awareness of thesefactors could enhance patient interactions and treatment outcomes. Mechanisms to bestenhance these factors in clinical practice warrant further study.
M. O’Keeffe, BScPhysio, Depart-ment of Clinical Therapies, Univer-sity of Limerick, Health SciencesBuilding, Limerick, Ireland.Address all correspondence to MsO’Keefe at: [email protected].
P. Cullinane, BScPhysio, Depart-ment of Clinical Therapies, Univer-sity of Limerick.
J. Hurley, BScPhysio, Departmentof Clinical Therapies, University ofLimerick.
I. Leahy, BScPhysio, Departmentof Clinical Therapies, University ofLimerick.
S. Bunzli, BScPhysio, School ofPhysiotherapy, Curtin Universityof Technology, Perth, Australia.
P.B. O’Sullivan, PhD, PGDip,School of Physiotherapy, CurtinUniversity of Technology.
K. O’Sullivan, PhD, MManipTher,BPhysio, SMISCP, MISOM,Department of Clinical Therapies,University of Limerick.
[O’Keeffe M, Cullinane P, Hurley J,et al. What influences patient-therapist interactions in musculo-skeletal physical therapy? Qualita-tive systematic review andmeta-synthesis. Phys Ther. 2016;96:609–622.]
© 2016 American Physical TherapyAssociation
Published Ahead of Print:October 1, 2015
Accepted: September 13, 2015Submitted: April 23, 2015
Research Report
Post a Rapid Response tothis article at:ptjournal.apta.org
May 2016 Volume 96 Number 5 Physical Therapy f 609

Patients with musculoskeletal painare commonly treated by physicaltherapists, yet the mechanisms by
which physical therapy interventionsinfluence clinically relevant outcomessuch as pain and disability are com-plex.1–3 Research shows that factorsassociated with the physical therapist,patient, and setting4,5 may influence clin-ical outcomes, in addition to the specificphysical interventions provided. Thesefactors make up the context and areoften described as nonspecific factors.6
Therefore, it is being increasingly recog-nized that musculoskeletal physical ther-apy involves both specific and nonspe-cific factors.6
Abundant research has focused on theimpact of the relationship betweenpatients and therapists on treatment out-come. This concept is usually referred toas the patient-therapist interaction.7 Thisinteraction is an example of a nonspe-cific factor and is fundamental to thetherapeutic process. It is defined as thesense of collaboration, warmth, and sup-port between the patient and thera-pist.2,8 The 3 main components are pro-posed to consist of: (1) patient-therapistagreement on goals, (2) patient-therapistagreement on interventions, and (3) theaffective bond between patient and ther-apist.9 Physical therapy relies on a com-plex interplay of technical skill, commu-nicative ability, and reflective capacity ofthe therapist to respond to the patient.2
Other constructs, such as trust,10 empa-thy,11 and verbal and nonverbal commu-nication, may be important prerequisitesto positive interaction.12
Evidence has emerged that positivepatient-therapist interactions in physicaltherapy settings are linked with reducedpain, reduced disability, and higher treat-ment satisfaction.2,13–17 The main sys-tematic review in this area2 providedrich quantitative data on the positiveeffect of the patient-therapist relation-ship on treatment outcome in physicaltherapy, but not specifically in a muscu-loskeletal population. No review has yetsystematically investigated physical ther-apists’ and patients’ views on factorsimportant to the patient-therapist inter-action. An investigation of the factorsthat may facilitate or hinder its develop-
ment, therefore, is appropriate. Giventhat patient-therapist interactions areunique, qualitative methods may be mostsuited to this investigation, as they wouldgather the perspectives of both physicaltherapists and patients, giving a holisticunderstanding of interaction. Therefore,the aim of this review was to systemati-cally investigate physical therapists’ andpatients’ perceptions of factors that influ-ence patient-therapist interactions inmusculoskeletal settings.
MethodData Sources and SearchesThis review has been registered in thePROSPERO database (CRD42014014336)and has been reported in accordancewith the ENTREQ guidelines.18 Theelectronic databases Academic SearchComplete, AMED, Biomedical Refer-ence Collection, CINAHL, MEDLINE,PsycARTICLES, PsycINFO, SPORTDiscus,EMBASE, Web of Science, and Scopuswere searched independently duringMarch through July 2014 by 3 authors(M.OK., P.C., I.L.). The search strategyused several combinations of the follow-ing key words: (1) qualitative research,(2) interaction, (3) pain, and (4) physicaltherapy. The complete list of key wordsis listed in Figure 1. Titles were screened
and abstracts were read where appropri-ate initially. Relevant full-text versionswere retrieved and evaluated if they ful-filled the inclusion criteria or if theabstract was insufficiently detailed todetermine eligibility. Manual searches ofreference lists of the identified studieswere also completed.
Study SelectionStudies were short-listed by 3 authors(M.OK., P.C., I.L.) independently, withany disagreements resolved by consen-sus. Studies were included if they exam-ined the opinions of patients or physicaltherapists regarding facilitators and bar-riers to a positive interaction betweenthe patient and the physical therapist.
Studies were excluded if they weresolely quantitative in nature; were notreported in English; measured only thestrength of the interaction between thepatient and the physical therapist, ratherthan the factors which influence it;examined physical therapists’ percep-tions only as part of a group of healthcare professionals; did not specificallyfocus on musculoskeletal physical ther-apy settings or conditions; examinedopinions prior to rehabilitation only; or
Figure 1.Literature search strategy.
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
610 f Physical Therapy Volume 96 Number 5 May 2016

focused on clinical reasoning decisionsonly.
Quality AssessmentTrustworthiness of the included studieswas determined by 2 authors (M.OK.,P.C.) independently using the CriticalAppraisal Skills Programme (CASP) Qual-itative Research Assessment Tool,19 withany disagreements resolved by consen-sus or consultation with another author(K.O.S.) (Appendix). This tool was cho-sen due to its extensive use in otherqualitative systematic reviews in muscu-loskeletal populations.20–22
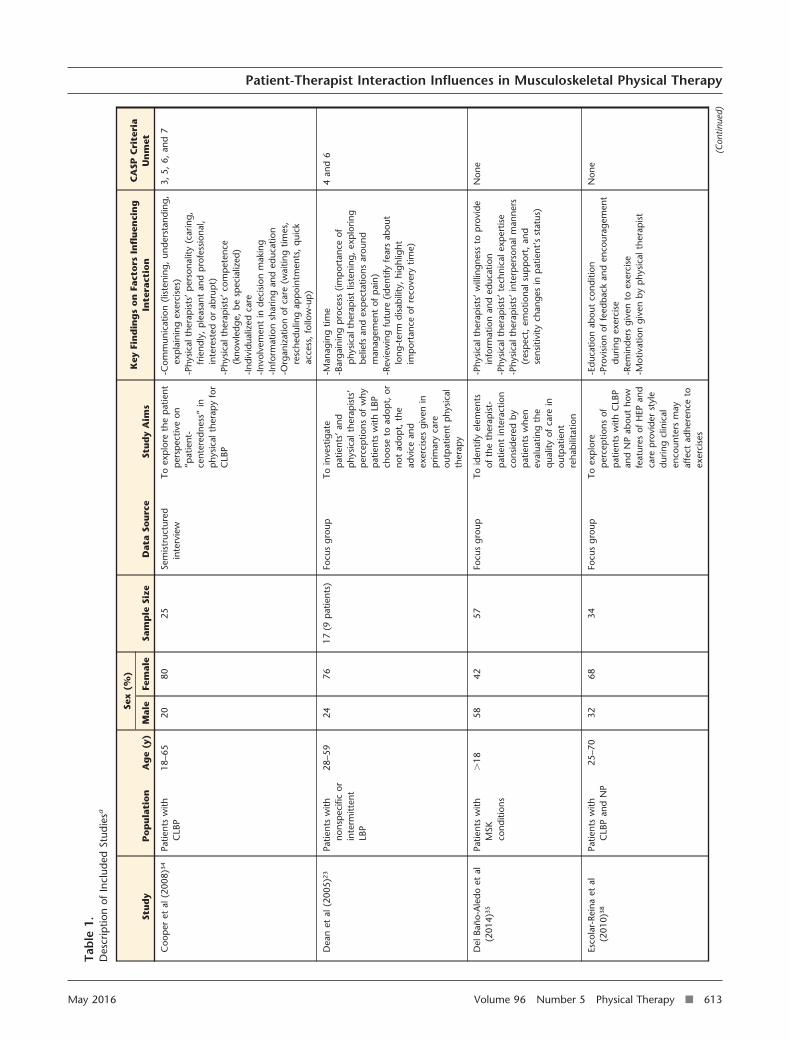
Data ExtractionData extraction was performed using apurpose-designed format by one author(M.OK.) and cross-checked by anotherauthor (J.H.) (Tab. 1). For 2 studies,23,24
the original authors were contactedto clarify information about studyparticipants.
Data Synthesis and AnalysisA thematic synthesis approach was usedto gather information and identify allthemes. It is the most appropriateapproach for qualitative meta-synthesis.The inductive analysis by Sandelowskiand Barroso25 was adapted and used 3stages: (1) extraction of findings and cod-ing of findings for each article; (2) group-ing of findings (codes) according to theirtopical similarity to determine whetherfindings confirm, extend, or refute eachother; and (3) abstraction of findings(analyzing the grouped findings to iden-tify additional patterns, overlaps, com-parisons, and redundancies to form a setof concise statements that capture thecontent of findings).
All stages were performed simultane-ously, as opposed to sequentially, as rec-ommended.25 All data under the head-ings “Results” and “Conclusions” wereread several times, line by line, to gain anidea of the topics. Relevant quotes werecopied and pasted into a Microsoft Word(Microsoft Corp, Redmond, Washington)document, and these quotes were ana-lyzed and organized into codes andgroupings. By a process of constant com-parative analysis,26 emerging groupingsfrom early codings were checked withongoing coding and used to guide later
coding. Final groupings were reviewedto ensure codings were similar in allgroups and that no potential groupingswere missed during the process. Thisprocess was simultaneously performedby 2 authors (M.OK., P.C.) indepen-dently to ensure against any biases influ-encing the analysis and coding ofthemes, with any disagreements resolvedby consensus or consultation withanother author (K.O.S.).
Consideration of SystematicReview’s TrustworthinessThe authors of this study are clinical andresearch physical therapists. Several dif-ferent authors were involved in differentstages of the review—from designing theinitial search strategy to the coding,grouping, and abstraction processes. Allauthors have experience in performingqualitative research.20
ResultsIdentification of StudiesFigure 2 summarizes study identification.A total of 7,768 journal articles wereretrieved. One article was retrieved froma reference list, and the remaining arti-cles were retrieved from the databases. Atotal of 5,651 duplicate journal articleswere removed, and 2,117 journal articles(titles and abstracts) were screened.Twenty-two journal articles wereretrieved after screening the abstracts, ofwhich 9 did not meet the inclusion cri-teria. Thirteen journal articles wereincluded in the systematic review andmeta-analysis. A total of 253 patients and78 physical therapists were interviewedin the 13 studies. The authors were con-sistent in the number of studies retrievedand included, with no disagreements tak-ing place.
Quality AssessmentThe CASP criteria of trustworthinessunmet by each study are presented inTable 1. The authors were consistent inthe scoring of the CASP criteria for eachstudy. Eight studies failed to meet crite-rion 6, for not considering theresearcher-participant relationship. Sixstudies failed to meet criterion 7, for notconsidering ethical issues. Three studiesfailed to meet criterion 4, for not justify-ing the recruitment strategy. Four studiesfailed to meet criterion 3, for not justify-
ing the research design, and another 4studies failed to meet criterion 5, for notproviding thorough information on datacollection. One study failed to meet cri-terion 8, as the data analysis was notsufficiently rigorous.
Identification of Codes/ThemesInitial coding of the eligible journal arti-cles resulted in 12 codes, which werereduced and organized into 4 themes(Tabs. 2 and 3). These themes were: (1)physical therapist interpersonal andcommunication skills, (2) physical thera-pist practical skills, (3) individualizedpatient-centered care, and (4) organiza-tional and environmental factors (Fig. 3).
Description of ResultsThere was good agreement among thestudies in this review, with similarthemes emerging. No clear contradic-tions were apparent. However, somestudies focused more on interpersonaland communication skills,27–29 whereasother studies focused more on organiza-tional and environmental factors.30,31
Theme 1: Physical TherapistInterpersonal andCommunication SkillsActive listening. One of the mostcommon aspects to emerge regardingphysical therapists’ communication skillswas active listening.24,27–34 Both physicaltherapists and patients felt that it wasimportant for physical therapists to listenand to allow patients to tell their sto-ries.24,27–34 This approach allowed abond to develop between the patientand the therapist, as the patients felt thatthey were valued.27,28,30,33 Patients wereunhappy when they were interruptedand could not tell their story.30,31,34
Patients also felt that not just listeningbut also understanding what the patientwas saying was very important.28,30,33
Some physical therapists felt that listen-ing was such an important facilitator of apositive patient-therapist interaction thatthey should be taught to improve theirlistening skills.24
Empathy. Another significant factormentioned by physical therapists andpatients as necessary to develop a posi-tive interaction was empathy.27–29,32–36
Physical therapists viewed empathy as a
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
May 2016 Volume 96 Number 5 Physical Therapy f 611

fundamental component of the patient-therapist relationship.27,29,32,37 They feltthat the treatment should take into con-sideration the pain and suffering that thepatient has endured.28,29 Patients appre-ciated when the therapist understoodwhat patients had to suffer and did notjust treat them as if the pain they had wasa minor irritation. Patients felt it wasimportant for therapists to realize howmuch of an impact pain could have ontheir lives and for therapists to empa-thize with them about this issue.27,35,36
Conversely, lack of empathy was a majorbarrier to a positive interaction, andpatients did not develop a bond withtherapists who could not empathize withthem.34
Friendliness. Patients believed thatbeing able to chat with their physicaltherapist in a friendly manner was impor-tant for positive interaction.27–30,33,35
Talking with the physical therapist in anopen way helped deepen the relation-ship between the patient and the thera-pist. Patients mentioned that a pleasantgreeting from their therapist every dayencouraged further interaction.27,30 Bothphysical therapists and patients men-tioned that having a sense of humor wasanother way to develop a positive rela-tionship.30,32 Patients found it difficult toengage with therapists when they werenot as friendly, and the interaction suf-fered as a consequence.31,35
Encouragement. Motivation andencouragement helped patients feel thatthe therapist cared about them and thatthey had a strong relationship with theirtherapist.28,33,35,38 These skills wereimportant for many reasons, as theencouragement motivated some patientsto adhere to the prescribed rehabilitationand strive to improve.27,33,35,38 The reas-
surance also provided emotional supportto patients, which further deepened thebond between the patient and the ther-apist as they shared personal feelings andexperiences.35
Confidence. Patients reported thatfeeling confident in their therapist wasan important factor and meant that theycould respect their therapist and trust hisor her opinion.27,29,30,36 Physical thera-pists stated that over time patients willbecome confident in their therapists anddevelop a sense of trust, which willenhance the interaction betweenpatients and therapists.27,29,36 However,some patients felt that their physicaltherapist was too confident and behavedin an arrogant manner, which was a sig-nificant barrier to a positive patient-therapist interaction.30
Nonverbal communication. Patientsand physical therapists acknowledgedthat nonverbal communication was avital part of communicationskills.24,30,32,36 Patients expressed thatthe therapist acting in what they felt wasan appropriate manner made them feelmore comfortable with their thera-pist.30,36 Physical contact between thepatient and therapist also enhanced thepatient-therapist interaction, accordingto both physical therapists andpatients.30 Physical therapists believedthat it was very important to pay atten-tion, not just to what the patient said, butalso to the manner and behavior of thepatient as he or she was talking.24,32
Theme 2: Physical TherapistPractical SkillsPatient education. A physical thera-pist skill that patients felt enhanced thepatient-therapist interaction was the abil-ity to provide a simple, clear explana-tion.27,29,30,32–36,38 Patients valued aneasy explanation of what their problemwas, how the physical therapist couldhelp them, and why the therapist wasprescribing certain exercises.27,32,34–36,38
Patients felt more comfortable whenthey knew what their treatment plan wasand felt interaction with their therapistwas enhanced as a result.27,34–36,38 Onthe other hand, patients did not likewhen the education given to them wastechnical and felt that this factor had a
Figure 2.PRISMA flow diagram.
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
612 f Physical Therapy Volume 96 Number 5 May 2016
Tab
le1.
Des
crip
tion
ofIn
clud
edSt
udie
sa
Stu
dy
Po
pu
lati
on
Ag
e(y
)
Sex
(%)
Sam
ple
Size
Dat
aSo
urc
eSt
ud
yA
ims
Key
Fin
din
gs
on
Fact
ors
Infl
uen
cin
gIn
tera
ctio
nC
ASP
Cri
teri
aU
nm
etM
ale
Fem
ale
Coo
per
etal
(200
8)34
Patie
nts
with
CLB
P18
–65
2080
25Se
mis
truc
ture
din
terv
iew
Toex
plo
reth
ep
atie
ntp
ersp
ectiv
eon
“pat
ient
-ce
nter
edne
ss”
inp
hysi
calt
hera
py
for
CLB
P
-Com
mun
icat
ion
(list
enin
g,un
ders
tand
ing,
exp
lain
ing
exer
cise
s)-P
hysi
calt
hera
pis
ts’
per
sona
lity
(car
ing,
frie
ndly
,p
leas
ant
and
pro
fess
iona
l,in
tere
sted
orab
rup
t)-P
hysi
calt
hera
pis
ts’
com
pet
ence
(kno
wle
dge,
besp
ecia
lized
)-I
ndiv
idua
lized
care
-Inv
olve
men
tin
deci
sion
mak
ing
-Inf
orm
atio
nsh
arin
gan
ded
ucat
ion
-Org
aniz
atio
nof
care
(wai
ting
times
,re
sche
dulin
gap
poi
ntm
ents
,q
uick
acce
ss,
follo
w-u
p)
3,5,
6,an
d7
Dea
net
al(2
005)
23
Patie
nts
with
nons
pec
ific
orin
term
itten
tLB
P
28–5
924
7617
(9p
atie
nts)
Focu
sgr
oup
Toin
vest
igat
ep
atie
nts’
and
phy
sica
lthe
rap
ists
’p
erce
ptio
nsof
why
pat
ient
sw
ithLB
Pch
oose
toad
opt,
orno
tad
opt,
the
advi
cean
dex
erci
ses
give
nin
prim
ary
care
outp
atie
ntp
hysi
cal
ther
apy
-Man
agin
gtim
e-B
arga
inin
gp
roce
ss(im
por
tanc
eof
phy
sica
lthe
rap
ist
liste
ning
,ex
plo
ring
belie
fsan
dex
pec
tatio
nsar
ound
man
agem
ent
ofp
ain)
-Rev
iew
ing
futu
re(id
entif
yfe
ars
abou
tlo
ng-t
erm
disa
bilit
y,hi
ghlig
htim
por
tanc
eof
reco
very
time)
4an
d6
Del
Bano
-Ale
doet
al(2
014)
35
Patie
nts
with
MSK
cond
ition
s
�18
5842
57Fo
cus
grou
pTo
iden
tify
elem
ents
ofth
eth
erap
ist-
pat
ient
inte
ract
ion
cons
ider
edby
pat
ient
sw
hen
eval
uatin
gth
eq
ualit
yof
care
inou
tpat
ient
reha
bilit
atio
n
-Phy
sica
lthe
rap
ists
’w
illin
gnes
sto
pro
vide
info
rmat
ion
and
educ
atio
n-P
hysi
calt
hera
pis
ts’
tech
nica
lexp
ertis
e-P
hysi
calt
hera
pis
ts’
inte
rper
sona
lman
ners
(res
pec
t,em
otio
nals
upp
ort,
and
sens
itivi
tych
ange
sin
pat
ient
’sst
atus
)
Non
e
Esco
lar-
Rein
aet
al(2
010)
38
Patie
nts
with
CLB
Pan
dN
P25
–70
3268
34Fo
cus
grou
pTo
exp
lore
per
cep
tions
ofp
atie
nts
with
CLB
Pan
dN
Pab
out
how
feat
ures
ofH
EPan
dca
rep
rovi
der
styl
edu
ring
clin
ical
enco
unte
rsm
ayaf
fect
adhe
renc
eto
exer
cise
s
-Edu
catio
nab
out
cond
ition
-Pro
visi
onof
feed
back
and
enco
urag
emen
tdu
ring
exer
cise
-Rem
inde
rsgi
ven
toex
erci
se-M
otiv
atio
ngi
ven
byp
hysi
calt
hera
pis
t
Non
e
(Con
tinue
d)
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
May 2016 Volume 96 Number 5 Physical Therapy f 613

Tab
le1.
Con
tinue
d Stu
dy
Po
pu
lati
on
Ag
e(y
)
Sex
(%)
Sam
ple
Size
Dat
aSo
urc
eSt
ud
yA
ims
Key
Fin
din
gs
on
Fact
ors
Infl
uen
cin
gIn
tera
ctio
nC
ASP
Cri
teri
aU
nm
etM
ale
Fem
ale
Gar
d(2
007)
29
Phys
ical
ther
apis
tsfo
rp
atie
nts
who
have
unde
rgon
eto
rtur
e
38–6
00
100
10Se
mis
truc
ture
din
terv
iew
Toid
entif
yfa
ctor
sim
por
tant
for
ago
odin
tera
ctio
nbe
twee
np
hysi
cal
ther
apis
tsan
dp
atie
nts
who
have
been
tort
ured
-Per
sona
lcha
ract
eris
tics
(res
pec
t,hu
mor
,em
pat
hy,
hone
sty,
flexi
bilit
y,se
lf-aw
aren
ess,
hand
lene
gativ
eem
otio
ns)
-Pro
fess
iona
land
ther
apeu
ticco
mp
eten
ce(s
eek
help
orsu
per
visi
onw
hen
req
uire
d)-L
angu
age
fact
ors
(inte
rpre
tm
eani
ng,
met
apho
rsan
dhu
mor
used
)-T
ime
and
fram
es(s
truc
ture
dtr
eatm
ent
with
adeq
uate
time)
-Cul
tura
lfac
tors
(sen
sitiv
ityto
the
pat
ient
’sne
eds,
norm
s,an
dva
lues
)-T
reat
men
tsta
ilore
dto
the
pat
ient
’sne
eds
confi
denc
ean
dtr
ust
-Rel
igio
usfa
ctor
s(r
esp
ect
belie
fs)
3,5,
6,7,
and
8
Gyl
lens
ten
etal
(199
9)3
2
Prim
ary
care
phy
sica
lth
erap
ists
44–6
210
010
Cro
ss-c
ase
anal
ysis
/in
terv
iew
Toin
vest
igat
eex
per
tp
hysi
calt
hera
pis
ts’
per
cep
tions
ofim
por
tant
fact
ors
influ
enci
ngth
eq
ualit
yof
the
inte
ract
ion
inp
hysi
calt
hera
py
trea
tmen
tin
prim
ary
care
-Pra
ctic
alp
rofe
ssio
nals
kills
and
pat
ient
exp
erie
nces
-Phy
sica
lthe
rap
yed
ucat
ion
and
theo
retic
alco
urse
sco
mp
lete
d-P
hysi
calt
hera
pis
ts’
life
exp
erie
nces
and
valu
es-P
hysi
calt
hera
pis
ts’
per
sona
lcha
ract
eris
tics
-Tea
mw
ork
-Wor
kor
gani
zatio
nan
den
viro
nmen
t-C
omm
unic
atio
nan
din
terp
erso
nals
kills
(bei
ngse
nsiti
ve,
intu
itive
,lis
teni
ng,
holis
tic,
ackn
owle
dgin
gbo
dyla
ngua
ge,
mot
ivat
ing)
-Ide
ntifi
catio
nof
pat
ient
reso
urce
s-P
atie
nted
ucat
ion
and
clea
rex
pla
natio
nsof
pro
blem
-Giv
ing
time
-Pat
ient
par
ticip
atio
nin
goal
sett
ing
3,6,
and
7
Har
man
etal
(201
1)2
4
Patie
nts
with
suba
cute
LBP
Not
stat
ed18
8244
Focu
sgr
oup
Toin
vest
igat
ecl
ient
educ
atio
np
rovi
ded
byp
hysi
cal
ther
apis
tsin
priv
ate
pra
ctic
eto
wor
kers
with
suba
cute
LBP
-Edu
catio
nab
out
pai
nan
dm
ultip
leas
pec
tsin
volv
ed-P
hysi
calt
hera
pis
ts’
taci
tkn
owle
dge
-Act
ive
liste
ning
-Rea
ssur
ance
-Ind
ivid
ualiz
edap
pro
ach
-Und
erst
andi
ngbo
dyla
ngua
ge-S
upp
ort
and
enco
urag
emen
tp
rovi
ded
-Und
erst
andi
ngof
pat
ient
need
s-I
nvol
ving
pat
ient
intr
eatm
ent
pla
n
4an
d6 (C
ontin
ued)
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
614 f Physical Therapy Volume 96 Number 5 May 2016

Tab
le1.
Con
tinue
d Stu
dy
Po
pu
lati
on
Ag
e(y
)
Sex
(%)
Sam
ple
Size
Dat
aSo
urc
eSt
ud
yA
ims
Key
Fin
din
gs
on
Fact
ors
Infl
uen
cin
gIn
tera
ctio
nC
ASP
Cri
teri
aU
nm
etM
ale
Fem
ale
Hill
san
dKi
tche
n(2
007)
31
Patie
nts
with
MSK
cond
ition
s
36–7
040
6030
Focu
sgr
oup
Toin
vest
igat
eth
efa
ctor
sth
ataf
fect
pat
ient
s’sa
tisfa
ctio
nw
ithM
SKou
tpat
ient
phy
sica
lthe
rap
yw
ithin
the
NH
Ssy
stem
ofca
rein
the
Uni
ted
King
dom
-Exp
ecta
tions
addr
esse
dor
not
addr
esse
d-P
atie
ntne
eds
met
orun
met
-Com
mun
icat
ion
and
educ
atio
nab
out
cond
ition
-Per
cep
tions
ofth
eth
erap
ist
(kno
wle
dgea
ble,
good
/poo
rco
mm
unic
ator
,em
pat
hyp
erce
ived
orno
tp
erce
ived
,en
cour
agem
ent
give
n)-T
reat
men
tp
roce
ss(c
onte
nt,
freq
uenc
yof
sess
ions
,fo
llow
-up
,w
aitin
gtim
e)
Non
e
Kidd
etal
(201
1)27
Out
pat
ient
sw
ithM
SKco
nditi
ons
20–6
850
508
Sem
istr
uctu
red
inte
rvie
wTo
inve
stig
ate
pat
ient
s’p
ersp
ectiv
esof
com
pon
ents
ofp
atie
nt-c
ente
red
phy
sica
lthe
rap
yan
dits
esse
ntia
lel
emen
ts
-Abi
lity
toco
mm
unic
ate
(list
en,
reas
sure
,ed
ucat
e)-P
hysi
calt
hera
pis
ts’
confi
denc
e-P
hysi
calt
hera
pis
ts’
know
ledg
ean
dp
rofe
ssio
nalis
m-P
hysi
calt
hera
pis
ts’
unde
rsta
ndin
gof
peo
ple
and
anab
ility
tore
late
(em
pat
hy,
enco
urag
emen
t)-T
akin
gp
atie
nts’
opin
ions
into
acco
unt
-Tra
nsp
aren
cyof
pro
gres
san
dou
tcom
e(f
ocus
onp
rogr
ess
and
mea
sure
men
t)
3,5,
6,an
d7
May
etal
(200
7)64
Patie
nts
with
LBP
29–7
741
.258
.834
Sem
istr
uctu
red
inte
rvie
wTo
inve
stig
ate
pat
ient
s’at
titud
esto
and
satis
fact
ion
with
phy
sica
lth
erap
yfo
rLB
P
-Phy
sica
lthe
rap
ists
’p
erso
nala
ndp
rofe
ssio
nalm
anne
r-E
xpla
natio
ns,
teac
hing
,an
ded
ucat
ion
pro
vide
d-P
atie
ntin
volv
emen
tin
pro
cess
-Org
aniz
atio
n(t
ime
and
acce
ssto
care
)
6an
d7
Oie
net
al(2
011)
28
1.Ph
ysic
alth
erap
ists
spec
ializ
ing
inN
PMP
44–6
817
8317
(11
pat
ient
san
d6
phy
sica
lth
erap
ists
)
Sem
istr
uctu
red
inte
rvie
w,
focu
sgr
oup
,p
erso
nal
note
s,an
dre
pea
ted
vide
ore
cord
ing
Toan
alyz
eho
wp
atie
nts
and
phy
sica
lthe
rap
ists
com
mun
icat
eve
rbal
lyan
dno
nver
bally
durin
gde
man
ding
situ
atio
ns
-Sha
red
unde
rsta
ndin
g-T
akin
gp
atie
nts’
opin
ions
into
acco
unt
-Pat
ienc
ean
dun
ders
tand
ing
nonv
erba
lac
tivity
-Phy
sica
lthe
rap
ists
’se
nsiti
vity
ofan
dab
ility
tone
gotia
teta
sks
with
pat
ient
5an
d7
2.Pa
tient
sw
ithC
LBP
orN
P22
–47
991
Peiri
set
al(2
012)
33
Patie
nts
with
MSK
cond
ition
s
60–9
216
8419
Sem
istr
uctu
red
inte
rvie
wTo
exp
lore
how
inp
atie
nts
ina
reha
bilit
atio
nse
ttin
gex
per
ienc
ep
hysi
calt
hera
py
reha
bilit
atio
n
-Em
pat
hetic
and
carin
gp
hysi
calt
hera
pis
ts(f
riend
ly,
know
ledg
eabl
e,an
dco
mp
assi
onat
e)-P
hysi
calt
hera
pis
ten
cour
agem
ent
and
mot
ivat
ion
Non
e
(Con
tinue
d)
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
May 2016 Volume 96 Number 5 Physical Therapy f 615
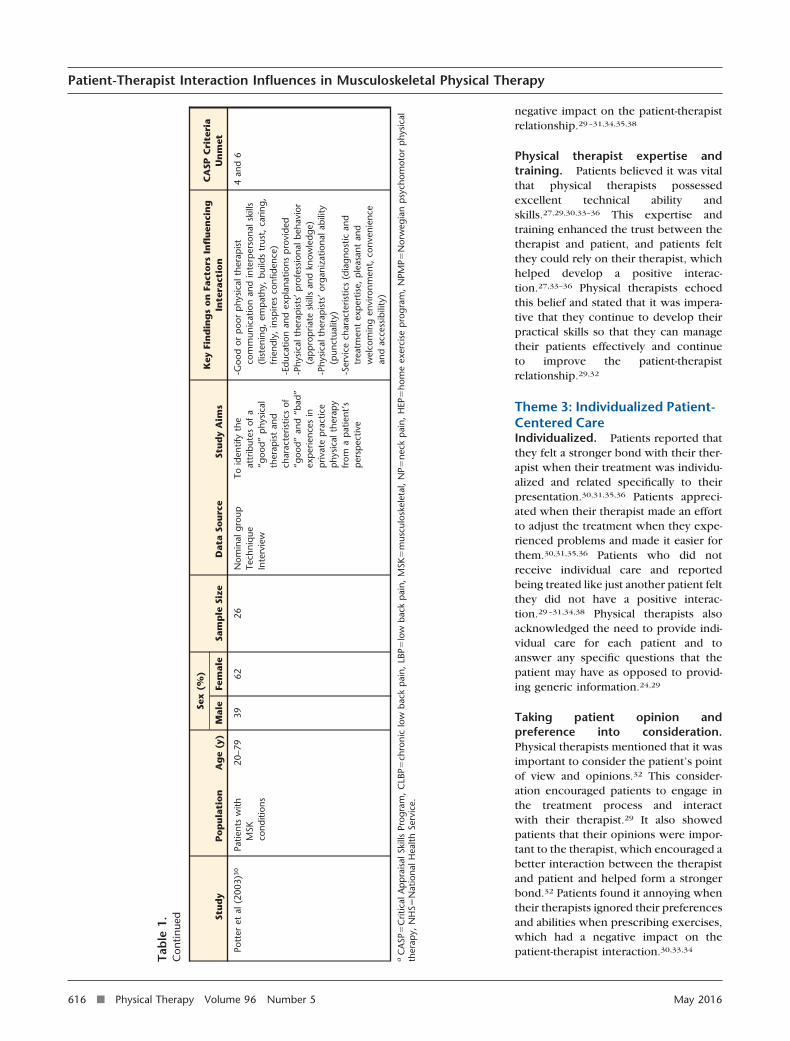
negative impact on the patient-therapistrelationship.29–31,34,35,38
Physical therapist expertise andtraining. Patients believed it was vitalthat physical therapists possessedexcellent technical ability andskills.27,29,30,33–36 This expertise andtraining enhanced the trust between thetherapist and patient, and patients feltthey could rely on their therapist, whichhelped develop a positive interac-tion.27,33–36 Physical therapists echoedthis belief and stated that it was impera-tive that they continue to develop theirpractical skills so that they can managetheir patients effectively and continueto improve the patient-therapistrelationship.29,32
Theme 3: Individualized Patient-Centered CareIndividualized. Patients reported thatthey felt a stronger bond with their ther-apist when their treatment was individu-alized and related specifically to theirpresentation.30,31,35,36 Patients appreci-ated when their therapist made an effortto adjust the treatment when they expe-rienced problems and made it easier forthem.30,31,35,36 Patients who did notreceive individual care and reportedbeing treated like just another patient feltthey did not have a positive interac-tion.29–31,34,38 Physical therapists alsoacknowledged the need to provide indi-vidual care for each patient and toanswer any specific questions that thepatient may have as opposed to provid-ing generic information.24,29
Taking patient opinion andpreference into consideration.Physical therapists mentioned that it wasimportant to consider the patient’s pointof view and opinions.32 This consider-ation encouraged patients to engage inthe treatment process and interactwith their therapist.29 It also showedpatients that their opinions were impor-tant to the therapist, which encouraged abetter interaction between the therapistand patient and helped form a strongerbond.32 Patients found it annoying whentheir therapists ignored their preferencesand abilities when prescribing exercises,which had a negative impact on thepatient-therapist interaction.30,33,34
Tab
le1.
Con
tinue
d Stu
dy
Po
pu
lati
on
Ag
e(y
)
Sex
(%)
Sam
ple
Size
Dat
aSo
urc
eSt
ud
yA
ims
Key
Fin
din
gs
on
Fact
ors
Infl
uen
cin
gIn
tera
ctio
nC
ASP
Cri
teri
aU
nm
etM
ale
Fem
ale
Pott
eret
al(2
003)
30
Patie
nts
with
MSK
cond
ition
s
20–7
939
6226
Nom
inal
grou
pTe
chni
que
Inte
rvie
w
Toid
entif
yth
eat
trib
utes
ofa
“goo
d”p
hysi
cal
ther
apis
tan
dch
arac
teris
tics
of“g
ood”
and
“bad
”ex
per
ienc
esin
priv
ate
pra
ctic
ep
hysi
calt
hera
py
from
ap
atie
nt’s
per
spec
tive
-Goo
dor
poo
rp
hysi
calt
hera
pis
tco
mm
unic
atio
nan
din
terp
erso
nals
kills
(list
enin
g,em
pat
hy,
build
str
ust,
carin
g,fr
iend
ly,
insp
ires
confi
denc
e)-E
duca
tion
and
exp
lana
tions
pro
vide
d-P
hysi
calt
hera
pis
ts’
pro
fess
iona
lbeh
avio
r(a
pp
rop
riate
skill
san
dkn
owle
dge)
-Phy
sica
lthe
rap
ists
’or
gani
zatio
nala
bilit
y(p
unct
ualit
y)-S
ervi
cech
arac
teris
tics
(dia
gnos
tican
dtr
eatm
ent
exp
ertis
e,p
leas
ant
and
wel
com
ing
envi
ronm
ent,
conv
enie
nce
and
acce
ssib
ility
)
4an
d6
aC
ASP
�C
ritic
alA
pp
rais
alSk
ills
Prog
ram
,C
LBP�
chro
nic
low
back
pai
n,LB
P�lo
wba
ckp
ain,
MSK
�m
uscu
losk
elet
al,
NP�
neck
pai
n,H
EP�
hom
eex
erci
sep
rogr
am,
NPM
P�N
orw
egia
np
sych
omot
orp
hysi
cal
ther
apy,
NH
S�N
atio
nalH
ealth
Serv
ice.
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
616 f Physical Therapy Volume 96 Number 5 May 2016

Theme 4: Organizational andEnvironmental FactorsTime. Many physical therapists per-ceived that giving their patients time todescribe their problem, and having thetime to be listened to, was an essentialfactor in positive patient-therapist inter-actions.23,29,32 Some patients did not feelthat they had enough time with the phys-ical therapist and that they had to wait along time to get an appointment.30,31
Some patients mentioned that theywould like more time with the physicaltherapist to discuss their treatment,as they were unsure about someaspects.31,34,38 Patients appreciated hav-ing the time to sit down and interactwith someone and not being rushed dur-ing appointments.23
Flexibility with patient appointmentsand care. Patients appreciated whenthe physical therapists were flexiblewhen setting up patient appoint-ments.30–32 Patients liked when theycould arrange appointments that did notdisrupt their days and felt grateful totheir therapist for accommodating theirneeds.30,31 Patients also felt that it wasvery useful being able to contact theirphysical therapists following their treat-ment and get some advice.30,31 Patientsfelt reassured that they could talk to theirtherapist when they were uncertainabout some activities, which encourageda stronger interaction between the ther-apist and patient.31
DiscussionTo our knowledge, this is the first sys-tematic review to investigate physical
therapists’ and patients’ perceptions offactors that influence patient-therapistinteractions in musculoskeletal settings.Four themes—physical therapist inter-personal and communication skills,physical therapist practical skills, individ-ualized patient-centered care, and orga-nizational and environmental aspects—were identified as the main factorsthought to influence patient-therapistinteractions. The presence or absence ofthese factors may act to positively or neg-atively influence interactions.
Physical therapists and patients bothacknowledged the importance of thephysical therapists’ communication andinterpersonal skills. Patients appreciateda physical therapist who listened andwho was empathetic, friendly, humor-ous, confident, and encouraging and hada good “bedside manner.” These findingsare in line with other qualitative studieson health care professionals’ (HCPs’)relationships with patients.3,39–41 Forexample, Laerum et al3 investigatedpatients’ opinions of medical specialistsand found that being “seen, heard, andbelieved” was crucial to the quality ofthe interaction. In particular, patientswanted professionals who expressedinterest in what they said and whoshowed signs of empathy, active listen-ing, and understanding of their problem.Similarly, Oosterhof et al,39 whoexplored factors that are associated witha successful treatment outcome inpatients with chronic pain and profes-sionals participating in a multidisci-plinary rehabilitation program, reportedthat patients wanted to be taken seri-
ously and have an open interaction withHCPs. An open interaction wasexplained as the professional having acalm, personal manner and being able tolisten well. The lack of these 2 compo-nents was reported to be associated witha failure in rehabilitation.39 In addition, aclinical ethnographic study41 revealedthat patients with chronic low back painfelt communication with HCPs wasenhanced by factors such as friendliness,empathy, respect, and a more conversa-tional and relaxed style of communica-tion (yarning). Furthermore, Strutt et al40
revealed similar themes in an osteo-pathic training clinic with patients con-sidering empathy (caring, reassuring, lis-tening, and continuity), atmosphere(friendly, relaxed, courteous), and man-ner (gentle, holistic) as crucial to theirinteraction with HCPs and their treat-ment satisfaction.
Therefore, across numerous qualitativestudies in different health care settings,communication and good interpersonalskills are perceived as vitally important tointeraction, treatment success, and satis-faction. Williams42 reported that, withinthe medical field, approximately 80% ofpatient complaints are thought to arisesecondary to a breakdown in communi-cation. Interestingly, no study in thisreview explored causes of such break-down in communication. For example,no study mentioned traits of patients thatmay prevent interaction (eg, patientsthought to be annoying or angry).20 It isno surprise that there is increasingemphasis placed on communicationskills training in physical therapy.43–45
This review shows that good communi-cation should be a fundamental part ofevery treatment encounter.
Physical therapists’ practical skills alsowere highlighted to be of importance.Patient education (what the physicaltherapist says) and expertise and training(what the physical therapist does) werethe main practical skills perceived to besignificant. The importance of patienteducation is in line with other qualitativeand quantitative literature. A recent sys-tematic review46 concluded that cogni-tive reassurance (giving knowledge) isimportant for treatment outcomes andsatisfaction in primary care settings.
Table 2.Identification of Themes From Initial Coding
Themes Codes
Physical therapist interpersonal andcommunication skills
1. Listening2. Empathy3. Friendliness4. Encouragement5. Confidence6. Nonverbal communication
Physical therapist practical skills 1. Patient education2. Physical therapist expertise and training
Individualized, patient-centered care 1. Individualized care2. Taking patient opinion and preference into consideration
Organizational and environmentalfactors
1. Time2. Flexibility with patient appointments and care
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
May 2016 Volume 96 Number 5 Physical Therapy f 617

However, although patient educationwas viewed as important by patients inthis review, physical therapists did notrefer to its importance for interaction.Similarly, Laerum et al3 found that expla-nations and knowledge were importantto patients. In particular, it was impor-tant for patients to receive an under-standable explanation of their condition.Effective education was deemed to beachieved when the patients receivedclear information in the form of simpleexplanations and metaphors. Such meth-ods have been recommended by quanti-tative data47,48 revealing the importanceof analogies and metaphors in explainingpain to patients. Oosterhof et al39 simi-larly outlined that patients appreciated athorough explanation of any assessmentsor investigations from HCPs. Patientswere satisfied when they had a similarshared understanding of their pain with
their HCPs. A clear recognizable expla-nation enabled understanding of painand the ability to explain it to others.Patients also required information abouthow to manage their pain and ways tocope to improve function. In addition, inanother study,41 patients in an osteo-pathic clinic were dissatisfied with infor-mation about their pain if it did not meettheir expectations of a good explanationor when information was provided withexcessive medical terminology. Bothwere viewed as barriers to goodcommunication.
The same studies3,39,41 revealed that edu-cation using complex medical jargon hin-dered interaction and successful rehabil-itation. Discrepancies in the explanationof factors involved in pain between pro-fessionals and patients were deemed to
be disadvantageous to interaction andoutcome. Furthermore, physical thera-pists felt that their own limited knowl-edge of pain was a barrier to providinggood patient education. Although theymentioned knowledge as a barrier tocommunication, as mentioned earlier,they did not see education as importantfor interaction. This finding may raise theissue of physical therapist role and scopeof practice and how physical therapiststhink they cannot charge for educationand need to use their skills to treat some-thing else. This area has not beenexplored enough, however, and it is dif-ficult to differentiate this area from thereview findings. Overall, given thatpatient understanding of pain is relatedto changing beliefs and better self-efficacy,49 good-quality patient educa-tion is of crucial importance.
Table 3.Frequency With Which Themes and Codes Were Identified Across the Studies Included in This Review
Themes CodesPhysical
Therapist/PatientNo. of
StatementsNo. of
Articles
Physical therapist interpersonal andcommunication skills
Listening Physical therapist 7 4
Patient 12 6
Empathy Physical therapist 6 3
Patient 7 5
Friendliness Physical therapist 4 3
Patient 8 5
Encouragement Physical therapist 0 0
Patient 9 4
Confidence Physical therapist 2 1
Patient 4 3
Nonverbal communication Physical therapist 2 2
Patient 2 2
Physical therapist practical skills Patient education Physical therapist 2 1
Patient 25 8
Physical therapist expertise and training Physical therapist 4 2
Patient 6 6
Individualized patient-centered care Individualized Physical therapist 11 2
Patient 15 6
Taking patient opinion and preference into consideration Physical therapist 3 1
Patient 0 0
Organizational and environmental factors Time Physical therapist 9 3
Patient 7 6
Flexibility with patient appointments and care Physical therapist 1 1
Patient 5 2
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
618 f Physical Therapy Volume 96 Number 5 May 2016

The finding that physical therapist train-ing and expertise are important is also inline with the literature. Peersman et al,50
who investigated patients’ priorities inoutpatient physical therapy, found thatthe physical therapists being experts intheir professional field was the mostimportant aspect for patients. Similarly,Strutt et al40 found that physical thera-pists have to be competent in their treat-ment approach and have to be thorough,knowledgeable, and dedicated. It is notpossible to differentiate from the find-ings of this review whether it is actuallygreater technical expertise and technicalskills that are needed or merely the per-ception that physical therapists are tech-nical experts that is important.
This review showed that it also wasimportant that physical therapists indi-vidualize treatment to the patient andtake patient opinions and preferencesinto account. This finding is in line withliterature showing that patients’ healthoutcomes and patients’ satisfaction ben-efit from a patient-centered approach.Laerum et al3 explored patients’ opinionsof a good consultation with medicalHCPs and found that patients appreci-ated patient-centered managementwhere the professional actively soughtthe patients’ perspective in terms ofthoughts and expectations. Similarly,
Oosterhof et al39 found that patientswere dissatisfied when they were notinvolved in the treatment planning withHCPs. Quantitative data also have shownthat identification of patient needs, goals,and expectations affects outcome.51–53
Interestingly, although physical thera-pists mentioned the importance of tak-ing patient preferences into account, nostudy in this review mentioned patientsvaluing this component. This finding iscontrary to guidelines encouragingpatient preferences for treatment in man-agement. It may indicate that patients arehappy if the treatment chosen makessense in terms of their main problemsand presentation. Some recent trialsfocusing on individualizing and tailoringtreatment to the patient presentation andneeds have shown positive findings.54–56
As quantitative and qualitative data high-light the potential importance of individ-ualizing treatment, musculoskeletalphysical therapy may benefit fromgreater emphasis on delivering an indi-vidualized approach together with goodcommunication and education.
Organizational and environmentalaspects of physical therapy also were amain theme in this review. Patients weregenerally dissatisfied about a lack of orga-nization regarding time, appointments,and appropriate resources and facilities.
This finding is in line with other litera-ture on patient-therapist interactions.3,39
For instance, Oosterhof et al39 revealedthat patients reported canceled appoint-ments, professionals arriving late, andchanges in the treatment program thatwere not implemented or explained ade-quately hindered interactions and out-comes. Similarly, Laerum et al3 foundthat patients were dissatisfied whenthere was a lack of information providedabout the layout of the treatment ses-sion. In a large survey30 of HCPs, includ-ing 2,793 physical therapists, 60%reported they did not have enough timeto “treat patients to their satisfaction.”Other patients commented that the phys-ical therapist was “rushed,” which mightbe interpreted by patients as a lack ofinterest in them.57 Patient satisfactionhas been previously related to accessibil-ity, availability, and convenience.58
Strengths and LimitationsA key strength of this review is that theresearch question is highly relevant tothe physical therapy profession. With theemerging international consensus thatmusculoskeletal pain is a multidimen-sional disorder associated with a com-plex interaction of factors across the bio-psychosocial spectrum that can beresistant to change,59,60 research isincreasingly encouraging clinicians toharness both specific and nonspecificaspects of treatment to improve out-come, with patient-therapist interactionsamong the most important of these non-specific factors. High-quality quantitativedata reveal that a positive patient-therapist interaction can positively influ-ence treatment outcomes.2,12–14 Thefindings of this review will inform phys-ical therapists about important factorsthat may need consideration whenenhancing interaction. Only studies pub-lished in English were included. Gray lit-erature was excluded from the review, aswe wanted to include only studies thathave been peer reviewed. We acknowl-edge that potentially relevant studiescould have been missed; however, wehave used this method in a similar qual-itative systematic review.20 The CASPquality assessment was not assessed forreliability; however, studies were ratedindependently, and agreement wasreached for all studies. Furthermore, as
Figure 3.Systematic review themes.
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
May 2016 Volume 96 Number 5 Physical Therapy f 619

some studies did not meet the CASP cri-teria, the credibility, transferability, anddependability of the results may havebeen affected. This review did not con-sider the specific interventions providedduring treatment, as this was not thefocus of this review. There is no sugges-tion that the specific treatment used isirrelevant, merely that the effectivenessof any specific treatment may beenhanced by better patient-therapistinteractions. It must be acknowledgedthat this review has only identified fac-tors that are perceived to be related topatient-therapist interactions. Furtherresearch is needed to examine whetherthese factors are actually related to thequality of these interactions or indeedpatient outcomes.
Clinical ImplicationsAddressing factors that are thought toinfluence patient-therapist interactionsmay enhance the experience of muscu-loskeletal physical therapy for patientsand improve adherence and outcomes.Physical therapists should be aware thatthese factors can act as facilitators of, andbarriers to, positive interaction. Eventhough it could be argued that usingthese factors effectively could be timeconsuming and thus costly in the shortterm due to longer waiting lists, adoptingthese factors could be beneficial in thelong term through promoting betteradherence and better patient outcomes.Ultimately, the responsibility lies withthe physical therapist, health care ser-vice providers, and wider society tomake time available to listen to patients’stories and provide the resources neces-sary to successfully treat patients. Giventhe higher number of patients to be seen,physical therapists may need to adoptcreative methods of dealing with longwaiting lists or organizational aspectsthat affect patient-therapist interactions.These methods could involve the use oftelephone triaging61 or the use of toolsthat assess the quality of patient-therapistinteractions, such as the Working Alli-ance Inventory and CommunicationAssessment Tool.62,63
This review revealed a disparity betweenphysical therapists’ and patients’ viewsabout the importance of education, withpatients rating it as highly important and
physical therapists failing to see its ben-efit as a determinant of interaction qual-ity. This disparity is a potential concernin management and may reveal physicaltherapists’ view of their profession (ie,that they need to deliver a particularintervention, as opposed to placing agreater emphasis on listening and edu-cating patients). Given the high impor-tance placed on education by patients,physical therapists need to prioritizeeducation in their management as a strat-egy to enhance adherence and out-comes. The provision of training coursesin the cognitive and affective domainsof patient-therapist interactions, improvingphysical therapist communicationskills, and the ability to educate andtake an individualized approach to treat-ment may enhance patient-therapistinteractions.
Further research in clinical settings isneeded to observe whether physicaltherapists account for these factors intheir interactions. It also would be inter-esting to evaluate whether training pro-grams specifically targeting the factorsidentified in this review can have aneffect on treatment delivery and out-come compared with an interventionthat does not acknowledge these factors.
In conclusion, physical therapists andpatients believe physical therapist com-munication and interpersonal skills,physical therapist practical skills, individ-ualized care, and organizational and envi-ronmental factors have a key influenceon patient-therapist interaction in mus-culoskeletal settings. The presence orabsence of any of these factors may act asa facilitator of, or barrier to, the patient-therapist interaction. Further study isneeded to examine which of these fac-tors are best related to patient-therapistinteractions and clinical outcomes. How-ever, increased emphasis on communica-tion, education, individualized care, andattention to organizational and environ-mental factors could enhance the per-ceived interaction between patients andphysical therapists.
Ms O’Keeffe, Mr Cullinane, and Dr KieranO’Sullivan provided concept/idea/researchdesign. Ms O’Keeffe, Mr Cullinane, Mr Hur-ley, Ms Bunzli, Prof Peter O’Sullivan, and Dr
Kieran O’Sullivan provided writing. MsO’Keeffe, Mr Cullinane, and Ms Leahy pro-vided data collection. Ms O’Keeffe, Mr Cul-linane, Mr Hurley, Ms Bunzli, and Dr KieranO’Sullivan provided data analysis. MsO’Keeffe and Dr Kieran O’Sullivan providedproject management. Dr Kieran O’Sullivanprovided facilities/equipment and institu-tional liaisons. Ms O’Keeffe, Mr Cullinane,Mr Hurley, Ms Bunzli, Ms Leahy, Prof PeterO’Sullivan, and Dr Kieran O’Sullivan pro-vided consultation (including review of man-uscript before submission).
Ms O’Keeffe is funded by the Irish ResearchCouncil (IRC). The IRC was not involved inany part of the design, execution, or inter-pretation of this study.
DOI: 10.2522/ptj.20150240
References1 Crow R, Gage H, Hampson S, et al. The
role of expectancies in the placebo effectand their use in the delivery of health care:a systematic review. Health TechnolAssess. 1999;3:1–96.
2 Hall AM, Ferreira PH, Maher CG, et al. Theinfluence of the therapist-patient relation-ship on treatment outcome in physicalrehabilitation: a systematic review. PhysTher. 2010;90:1099–1110.
3 Laerum E, Indahl A, Skouen J. What is “thegood back-consultation”? A combinedqualitative and quantitative study ofchronic low back pain patients’ interac-tion with and perceptions of consultationswith specialists. J Rehabil Med. 2006;38:255–262.
4 Del Re A, Fluckiger C, Horvath AO, et al.Therapist effects in the therapeutic allian-ce–outcome relationship: a restricted-maximum likelihood meta-analysis. ClinPsychol Rev. 2012;32:642–649.
5 Szybek K, Gard G, Linden J. Thephysiotherapist-patient relationship:applying a psychotherapy model. Phys-iother Theory Pract. 2000;16:181–193.
6 Miciak M, Gross DP, Joyce A. A review ofthe psychotherapeutic “common factors”model and its application in physical ther-apy: the need to consider general effectsin physical therapy practice. Scand J Car-ing Sci. 2012;26: 394–403.
7 Martin DJ, Garske JP, Davis MK. Relationof the therapeutic alliance with outcomeand other variables: a meta-analyticreview. J Consult Clin Psychol. 2000;68:438.
8 Ackerman SJ, Hilsenroth MJ. A review oftherapist characteristics and techniquespositively impacting the therapeutic alli-ance. Clin Psychol Rev. 2003;23:1–33.
9 Bordin ES. The generalizability of the psy-choanalytic concept of the working alli-ance. Psychother Theory Res Pract. 1979;16:252.
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
620 f Physical Therapy Volume 96 Number 5 May 2016

10 Hall AM, Ferreira ML, Clemson L, et al.Assessment of the therapeutic alliance inphysical rehabilitation: a RASCH analysis.Disabil Rehabil. 2012;34:257–266.
11 Mercer SW, Maxwell M, Heaney D, WattGC. The consultation and relational empa-thy (CARE) measure: development andpreliminary validation and reliability of anempathy-based consultation process mea-sure. Fam Pract. 2004;21:699–705.
12 Pinto RZ, Ferreira ML, Oliveira VC, et al.Patient-centred communication is associ-ated with positive therapeutic alliance: asystematic review. J Physiother. 2012;58:77–87.
13 Ferreira PH, Ferreira ML, Maher CG, et al.The therapeutic alliance between clini-cians and patients predicts outcome inchronic low back pain. Phys Ther. 2013;93:470–478.
14 Fuentes J, Armijo-Olivo S, Funabashi M,et al. Enhanced therapeutic alliance mod-ulates pain intensity and muscle pain sen-sitivity in patients with chronic low backpain: an experimental controlled study.Phys Ther. 2014;94:477–489.
15 Lewin S, Skea Z, Entwistle V, et al. Inter-ventions for providers to promote apatient-centred approach in clinical con-sultations. Cochrane Database Syst Rev.2001;4:CD003267.
16 Moore PM, Wilkinson SS, Rivera MercadoS. Communication skills training for healthcare professionals working with cancerpatients, their families and/or carers.Cochrane Database Syst Rev. 2004;2:CD003751.
17 McGilton KS, Boscart V, Fox M, et al. Asystematic review of the effectiveness ofcommunication interventions for healthcare providers caring for patients in resi-dential care settings. Worldviews EvidBased Nurs. 2009;6:149–159.
18 Tong A, Flemming K, McInnes E, et al.Enhancing transparency in reporting thesynthesis of qualitative research: ENTREQ.BMC Med Res Methodol. 2012;12:181.
19 Critical Appraisal Skills Programme(CASP). CASP checklists. 2013. Availableat: http://www.casp-uk.net/. AccessedApril 15, 2015.
20 Synnott A, O’Keeffe M, Bunzli S, et al.Physiotherapists may stigmatise or feelunprepared to treat people with low backpain and psychosocial factors that influ-ence recovery: a systematic review. JPhysiother. 2015;61:68–76.
21 Kelly GA, Blake C, Power CK, et al. Theassociation between chronic low backpain and sleep: a systematic review. Clin JPain. 2011;27:169-181.
22 Fullen B, Baxter G, O’Donovan B, et al.Doctors’ attitudes and beliefs regardingacute low back pain management: a sys-tematic review. Pain. 2008;136:388–396.
23 Dean SG, Smith JA, Payne S, Weinman J.Managing time: an interpretative phenom-enological analysis of patients’ and phys-iotherapists’ perceptions of adherence totherapeutic exercise for low back pain.Disabil Rehabil. 2005;27:625–636.
24 Harman K, Bassett R, Fenety A, Hoens AM.Client education: communicative interac-tion between physiotherapists and clientswith subacute low back pain in privatepractice. Physiother Can. 2011;63:212–223.
25 Sandelowski M, Barroso J. Handbook forSynthesizing Qualitative Research. NewYork, NY: Springer Publishing Co; 2007.
26 Strauss A, Corbin J. Grounded theorymethodology: an overview. In: Denzin N,Lincoln Y, eds. Handbook of QualitativeResearch. Thousand Oaks, CA: Sage; 1994:273–285.
27 Kidd MO, Bond CH, Bell ML. Patients’ per-spectives of patient-centredness as impor-tant in musculoskeletal physiotherapyinteractions: a qualitative study. Physio-therapy. 2011;97:154–162.
28 Oien AM, Steihaug S, Iversen S, Raheim M.Communication as negotiation processesin long-term physiotherapy: a qualitativestudy. Scand J Caring Sci. 2011;25:53–61.
29 Gard G. Factors important for good inter-action in physiotherapy treatment of per-sons who have undergone torture: a qual-itative study. Physiother Theory Pract.2007;23:47–55.
30 Potter M, Gordon S, Hamer P. The physio-therapy experience in private practice:the patients’ perspective. Aust J Phys-iother. 2003;49:195–202.
31 Hills R, Kitchen S. Satisfaction with outpa-tient physiotherapy: focus groups toexplore the views of patients with acuteand chronic musculoskeletal conditions.Physiother Theory Pract. 2007;23:1–20.
32 Gyllensten AL, Gard G, Salford E, Ekdahl C.Interaction between patient and physio-therapist: a qualitative study reflecting thephysiotherapist’s perspective. PhysiotherRes Int. 1999;4:89–109.
33 Peiris CL, Taylor NF, Shields N. Patientsvalue patient-therapist interactions morethan the amount or content of therapyduring inpatient rehabilitation: a qualita-tive study. J Physiother. 2012;58:261–268.
34 Cooper K, Smith BH, Hancock E. Patient-centredness in physiotherapy from theperspective of the chronic low back painpatient. Physiotherapy. 2008;94:244–252.
35 Del Bano-Aledo ME, Medina-Mirapeix F,Escolar-Reina P, et al. Relevant patient per-ceptions and experiences for evaluatingquality of interaction with physiothera-pists during outpatient rehabilitation: aqualitative study. Physiotherapy. 2014;100:73–79.
36 May SJ. Patient satisfaction with manage-ment of back pain. Physiotherapy. 2001;87:4–20.
37 Cherry-Bukowiec JR, Denchev K, Dickin-son S, et al. Prevention of catheter-relatedblood stream infection: back to basics?Surg Inf. 2011;12:27–32.
38 Escolar-Reina P, Medina-Mirapeix F,Gascon-Canovas JJ, et al. How do care-provider and home exercise programcharacteristics affect patient adherence inchronic neck and back pain: a qualitativestudy. BMC Health Serv Res. 2010;10:60.
39 Oosterhof B, Dekker J, Sloots M, et al. Suc-cess or failure of chronic pain rehabilita-tion: the importance of good interac-tion—a qualitative study under patientsand professionals. Disabil Rehabil. 2014;36:1903–1910.
40 Strutt R, Shaw Q, Leach J. Patients’ per-ceptions and satisfaction with treatment ina UK osteopathic training clinic. ManTher. 2008;13:456–467.
41 Lin I, O’Sullivan P, Coffin J, et al. “I can sitand talk to her”: aboriginal people,chronic low back pain and heathcare prac-titioner communication. Aust Fam Physi-cian. 2014;43:320.
42 Williams D. Communication Skills inPractice: A Practical Guide for HealthProfessionals. London, United Kingdom:Jessica Kingsley Publishers; 1997.
43 Parry RH, Brown K. Teaching and learningcommunication skills in physiotherapy:what is done and how should it be done?Physiotherapy. 2009;95:294–301.
44 Lonsdale C, Hall AM, Williams GC, et al.Communication style and exercise compli-ance in physiotherapy (CONNECT): a clus-ter randomized controlled trial to test atheory-based intervention to increasechronic low back pain patients’ adherenceto physiotherapists’ recommendations—study rationale, design, and methods. BMCMusculoskelet Disord. 2012;13:104.
45 Shannon R, Hillsdon M. Motivational inter-viewing in musculoskeletal care. Musculo-skeletal Care. 2007;5:206–215.
46 Pincus T, Holt N, Vogel S, et al. Cognitiveand affective reassurance and patient out-comes in primary care: a systematicreview. Pain. 2013;154:2407–2416.
47 Gallagher L, McAuley J, Moseley GL. Arandomized-controlled trial of using abook of metaphors to reconceptualizepain and decrease catastrophizing in peo-ple with chronic pain. Clin J Pain. 2013;29:20–25.
48 Stewart M. The road to pain reconceptu-alisation: do metaphors help or hinder thejourney? Pain and Rehabilitation. 2014;2014:24–31.
49 Louw A, Diener I, Butler DS, PuenteduraEJ. The effect of neuroscience educationon pain, disability, anxiety, and stress inchronic musculoskeletal pain. Arch PhysMed Rehabil. 2011;92:2041–2056.
50 Peersman W, Rooms T, Bracke N, et al.Patients’ priorities regarding outpatientphysiotherapy care: a qualitative and quan-titative study. Man Ther. 2013;18:155–164.
51 Linde K, Witt CM, Streng A, et al. Theimpact of patient expectations on out-comes in four randomized controlled trialsof acupuncture in patients with chronicpain. Pain. 2007;128:264–271.
52 Mondloch MV, Cole DC, Frank JW. Doeshow you do depend on how you thinkyou’ll do? A systematic review of the evi-dence for a relation between patients’recovery expectations and health out-comes. Can Med Assoc J. 2001;165:174–179.
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
May 2016 Volume 96 Number 5 Physical Therapy f 621

53 Verbeek J, Sengers M-J, Riemens L,Haafkens J. Patient expectations of treat-ment for back pain: a systematic review ofqualitative and quantitative studies. Spine.2004;29:2309–2318.
54 Vibe Fersum K, O’Sullivan P, Skouen J,et al. Efficacy of classification�based cog-nitive functional therapy in patients withnon-specific chronic low back pain: a ran-domized controlled trial. Eur J Pain. 2013;17:916–928.
55 Hill JC, Whitehurst DG, Lewis M, et al.Comparison of stratified primary caremanagement for low back pain with cur-rent best practice (STarT Back): a ran-domised controlled trial. Lancet. 2011;378:1560–1571.
56 Åsenlöf P, Denison E, Lindberg P. Individ-ually tailored treatment targeting activity,motor behavior, and cognition reducespain-related disability: a randomized con-trolled trial in patients with musculoskel-etal pain. J Pain. 2005;6:588–603.
57 Harrison K, Williams S. Exploring thepower balance in physiotherapy. Br J TherRehabil. 2000;7:355–361.
58 Fox JG, Storms DM. A different approachto sociodemographic predictors of satis-faction with health care. Soc Sci Med A.1981;15:557–564.
59 Karjalainen K, Malmivaara A, van TulderM, et al. Multidisciplinary rehabilitationfor fibromyalgia and musculoskeletal painin working age adults. Cochrane Data-base Syst Rev. 2000;2:CD001984.
60 Nijs J, Roussel N, van Wilgen CP, et al.Thinking beyond muscles and joints: ther-apists’ and patients’ attitudes and beliefsregarding chronic musculoskeletal painare key to applying effective treatment.Man Ther. 2013;18:96–102.
61 Taylor S, Ellis I, Gallagher M. Patient satis-faction with a new physiotherapy tele-phone service for back pain patients.Physiotherapy. 2002;88:645–657.
62 Makoul G, Krupat E, Chang C-H. Measur-ing patient views of physician communi-cation skills: development and testing ofthe Communication Assessment Tool.Patient Educ Couns. 2007;67:333–342.
63 Hatcher RL, Gillaspy JA. Development andvalidation of a revised short version of theWorking Alliance Inventory. PsychotherRes. 2006;16:12–25.
64 May S. Patients’ attitudes and beliefs aboutback pain and its management after phys-iotherapy for low back pain. PhysiotherRes Int. 2007;12:126–135.
Appendix.Critical Appraisal Skills Program (CASP) Tool
I. Was there a clear statement of the aims of the research?
II. Is a qualitative methodology appropriate?
III. Was the research design appropriate to address the aims of the research?
IV. Was the recruitment strategy appropriate to the aims of the research?
V. Were the data collected in a way that addressed the research issue?
VI. Has the relationship between researcher and participants been adequately considered?
VII. Have ethical issues been taken into consideration?
VIII. Was the data analysis sufficiently rigorous?
IX. Is there a clear statement of findings?
X. How valuable was the research?
Patient-Therapist Interaction Influences in Musculoskeletal Physical Therapy
622 f Physical Therapy Volume 96 Number 5 May 2016