What Can Government-Administered Registries Learn from Quality Registries? Marta Ebbing, MD, PhD...
40
What Can Government-Administered Registries Learn from Quality Registries? Marta Ebbing, MD, PhD Department director, Dept. of Health Registries Norwegian Institute of Public Health No conflicts of interest Thanks to all my colleagues!
-
Upload
spencer-turner -
Category
Documents
-
view
222 -
download
1
Transcript of What Can Government-Administered Registries Learn from Quality Registries? Marta Ebbing, MD, PhD...

What Can Government-Administered Registries Learn from Quality Registries?
Marta Ebbing, MD, PhDDepartment director, Dept. of Health RegistriesNorwegian Institute of Public HealthNo conflicts of interestThanks to all my colleagues!

Ebbing, NIPH 2
Outline
Register operation with quality
GARs in Norway – S & W
How to combine the best from GARs and QRs?
Summary and conclusion
2014-12-09

Ebbing, NIPH 3
Norwegian Advantages
All residents unique 11-digit personal IDAll residents access to public health careGovernment administered registries (6/17);
Cause of Death Registry (CoDR) (1951)Cancer Registry (CRN) (1955)Medical Birth Registry (MBRN) (1967)Prescription Database (NorPD) (2004)Patient Registry (NPR) (2008)Cardiovascular Disease Registry (NCVDR) (2012 )
2014-12-09
Ebbing, NIPH 4
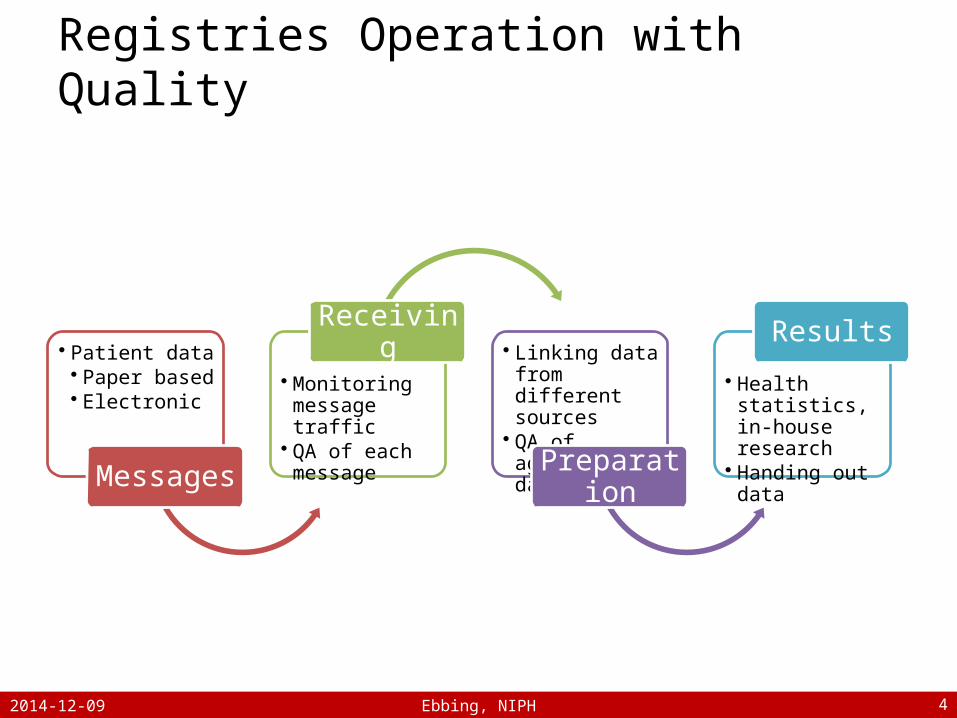
Registries Operation with Quality
• Patient data• Paper based• Electronic
Messages
• Monitoring message traffic
• QA of each message
Receiving • Linking data from different sources
• QA of aggregated data
Preparation
• Health statistics, in-house research
• Handing out data
Results
2014-12-09

Ebbing, NIPH 5
Registries Operation with Quality
• Patient data• Paper based• Electronic
Messages
• Monitoring message traffic
• QA of each message
Receiving • Linking data from different sources
• QA of aggregated data
Preparation
• Health statistics, in-house research
• Handing out data
Results
2014-12-09

Ebbing, NIPH 6
GARs – Legal Regulation
Wide purposesRelevant and sufficient information – “need no know”, not “nice to know”Personal integrity and data security
2014-12-09

Ebbing, NIPH 7
GARs in Norway – S & WStrengthts WeaknessesAll individuals or events included
Lack of detailed medical information
Governmental responsibility; funding, continuity, data security, personal privacy
Lack of genuine interest from relevant health care personnel
Many different registration systems
2014-12-09

Ebbing, NIPH 8
Two GAR Examples
Norwegian Cardiovascular Disease Registry (2012 )
Medical Birth Registry of Norway (1967 )
2014-12-09

Ebbing, NIPH 9
CVD in Norway 2012-2013Data Source Unit 2012 2013
GPs1 Consultations for CVD or related problems 1 850 954 1 814 245
Pharmacies2 Users of CVD medications (ATC: C) 1 018 877 1 039 755
Hospitals3 Patients with CVD or related diagnoses 339 155 327 845
CoDR4 Patients diseased from CVD 13 018 12 132
1Reimbursementdata from «Kontroll og utbetaling av helserefusjoner» 2Norwegian Prescription Database3Norwegian Cardiovascular Disease Registry4Cause of Death Registry
2014-12-09

Ebbing, NIPH 10
Norwegian CVD Registry
National, person identifiable, compulsory Established in 2012Combined registry (core + 8 QRs) The Norwegian Institute of Public Health responsible for data management
2014-12-09

Ebbing, NIPH 11
BMJ 2005 331;942-945
based research and those who do not, or cannot, consent. Blanket requirements for explicit consent for the use of individuals' identifiable data can bias disease registers, epidemiological studies, and health services research.PMID:
16223793[PubMed - indexed for MEDLINE]
PMCID:PMC1261192
Free PMC Article•
Images from this publication.See all images (2)Free text
Fig
1
Kaplan-Meier survival curve for death from all causes among 187 adults with brain arteriovenous malformations by their consent to participate in an observational study (consenters 2 deaths, non-consenters 12 deaths; log rank=15.8, P=0.0001)Bias from requiring explicit consent from all participants in observational research: prospective, population based studyBMJ. 2005 October 22;331(7522):942-942.
Fig
2
Kaplan-Meier analysis of time to first seizure among 187 adults with brain arteriovenous malformations by their consent to participate in an observational study (consenters 42 events, non-consenters 13 events; log rank=4.1, P=0.044)Bias from requiring explicit consent from all participants in observational research: prospective, population based studyBMJ. 2005 October 22;331(7522):942-942.PUBLICATION
TYPES, MESH
TERMSPublication Types
•Multicenter
Study•Research
Support, Non-U.S. Gov'tMeSH Terms
•Adolescent•Adult•Aged•Central Nervous
System
Vascular
Malformations/complications•Central Nervous
System
Vascular
Malformations/diagnosis*•Central Nervous
System
Vascular
Malformations/mortality•Epidemiologic
Methods•Female•Humans•Informed
Consent*•Intracranial Hemorrhages/epidemiology•Intracranial Hemorrhages/etiology•Male•Middle
Aged•Patient Selection/ethics*•Prognosis•Scotland/epidemiology•Seizures/epidemiology•Seizures/etiology•Selection
BiasLINKOUT
-
MORE
RESOURCESFull Text Sources•HighWire•Europe PubMed Central•Ovid Technologies, Inc.•PubMed Central•PubMed Central Canada
Other Literature Sources•Labome Researcher Resource - ExactAntigen/Labome•Access more work from the authors - ResearchGate
PubMed Commons homePubMed
Commons 0
comments
How to join PubMed Commons
•Supplemental ContentFULL
TEXT
LINKS
SAVE
ITEMS
Add to FavoritesView
more
options
RELATED CITATIONS IN PUBMED
•Demographic and AIDS-related characteristics of consenters to a population-based HIV-survey: results from a pilot study in Arusha, Tanzania.
[East Afr Med J. 1994]
Demographic and AIDS-related characteristics of consenters to a population-based HIV-survey: results from a pilot study in Arusha, Tanzania.Ole-King'Ori N, Klepp KI, Kissila PE, Biswalo PM, Mnyika KS. East Afr Med J. 1994 Aug; 71(8):483-9.
•Selection bias resulting from the requirement for prior consent in observational research: a community cohort of people with ischaemic heart disease.
[Heart. 2007]
Selection bias resulting from the requirement for prior consent in observational research: a community cohort of people with ischaemic heart disease.Buckley B, Murphy AW, Byrne M, Glynn L. Heart. 2007 Sep; 93(9):1116-20. Epub 2007 May 13.
•Assessing the impact of the requirement for explicit consent in a hospital-based stroke study.
[QJM. 2008]
Assessing the impact of the requirement for explicit consent in a hospital-based stroke study.Jackson C, Crossland L, Dennis M, Wardlaw J, Sudlow C. QJM. 2008 Apr; 101(4):281-9. Epub 2008 Feb 15.
• Written informed consent and selection bias in observational studies using medical records: systematic review.
[BMJ. 2009]
Review Written informed consent and selection bias in observational studies using medical records: systematic review.Kho ME, Duffett M, Willison DJ, Cook DJ, Brouwers MC. BMJ. 2009 Mar 12; 338:b866. Epub 2009 Mar 12.
• Getting meaningful informed consent from older adults: a structured literature review of empirical research.
[J Am Geriatr Soc. 1998]
Review Getting meaningful informed consent from older adults: a structured literature review of empirical research.Sugarman J, McCrory DC, Hubal RC. J Am Geriatr Soc. 1998 Apr; 46(4):517-24.
See reviews...See all...CITED BY 18 PUBMED CENTRAL ARTICLES
2014-12-09
Ebbing, NIPH 12
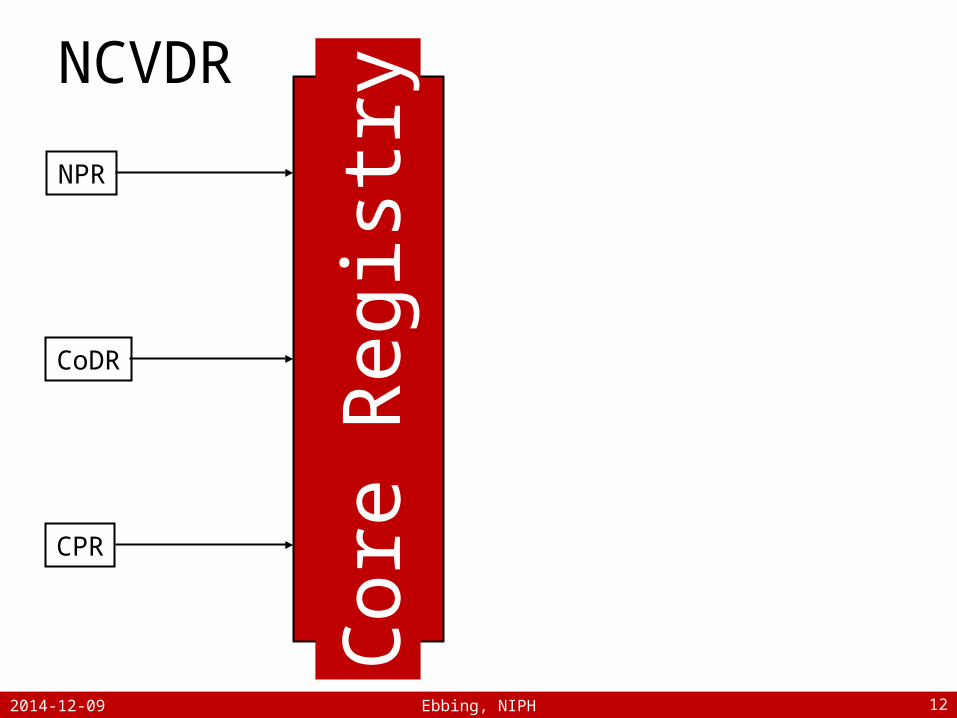
NPR
CoDR
CPR Core
Reg
istry
NCVDR
2014-12-09

Ebbing, NIPH 13
Core Data
Person informationAdministrative informationMedical information
Diagnoses from the NPR for outpatient visits and hospital stays
ICD-10 Ch. IX, codes I00-I99, ++
Procedures from the NPRNCSP/NCMP Ch. F, P ++
Cause of death from the CoDRfor persons registered with or diceased from CVD
2014-12-09

Ebbing, NIPH 14
NPR
CoDR
CPR
Stroke Registry
Heart Surgery Registry
Heart Failure Registry
Invasive Cardiology Registry
Myocardial Infarction Registry
Cardiac Arrest Registry
Vessel Surgery Registry
Pacemaker- and ICD Registry
Core
Reg
istry
NCVDR
2014-12-09

Ebbing, NIPH 15
Quality Registry Data
Known risk factors for CVDHistory of CVDCurrent CVDMedical details on current episode/procedureResults of health careFurther treatment
MedicationsOther secondary prevention efforts
Quality of life / PROMS
2014-12-09

Ebbing, NIPH 16
NCVDR Council (2012)
Regional Health Authorities, Universities/Research, QRs, QR Services, Central Health Authorities
2014-12-09

Ebbing, NIPH 17
Challenges
Legal issues – personal data actTechnical issuesQuality of data in NPR and CoDRToo much focus on datacollection, and too little on analyses?Many stakeholders, consensus necessary
2014-12-09

755 878 episodes, 327 845 pasients
575 261 episodes withmain diagnosis fromqualifying diagnoses
385 677outpatient visits
189 584hospital stays
NCVDR Core Registry 2013
2014-12-09 18Ebbing, NIPH

Ebbing, NIPH 19
Variable CR QR Coverage No. of patients with stroke1 9 730 7 260 74,6%No. of pasients with AMI2 14 485 12 336 85,2 %No. of PCIs at HUH3 1 325 1 290 97,4 %No. of CABGs4 1 926 1 919 99,6 %No. of pacemaker implantations5 3 468 3 459 99,7 %Abbreviations: CR, core registry; QR, quality registry; AMI, acute myocardial infarction; HUH, Haukeland University Hospital; CABG, coronary artery bypass grafting.1NCVDR Core Registry (main diagnosis) vs. Stroke Registry 2NCVDR Core Registry (main or seconrady diagnosis) vs. Myocardial Infarction Registry3NCVDR Core Registry vs. Invasive Cardiology Registry4NCVDR Core Registry vs. Heart Surgery Registry vs5NCVDR Core Registry vs. Pacemaker- and ICD Registry.
«Coverage» CR vs. QR in 2013
2014-12-09

Ebbing, NIPH 20
NCVDR Achievements 2012-13
Improvement of quality of health care services for patients with cardiovascular disease
Surveillance; incidence and prevalence Data for research Data for evaluation of results of health care
services – National Quality Indicators Stroke, AMI
Data for planning of health care services
2014-12-09

Ebbing, NIPH 21
NCVDR Combined Registry Model
1. Exploit existing data 2. Coordinate data capture, data
handling and analyses3. Ensure full coverage4. Ensure influence from clinical
specialists and researchers
2014-12-09

Ebbing, NIPH 22
No. of Births in Norway
2004 2005 2006 2007 2008 2009 2010 2011 2012 201353,000
54,000
55,000
56,000
57,000
58,000
59,000
60,000
61,000
62,000
63,000
2014-12-09

Ebbing, NIPH 23
No. of Maternity Units in Norway
2004 2005 2006 2007 2008 2009 2010 2011 2012 201346
48
50
52
54
56
58
60
62
64
66
68
≥ 10 BirthsAll
2014-12-09

Ebbing, NIPH 24
Medical Birth Registry of Norway
National, person identifiable, compulsory Established in 1967Combined registry (core + 1 QR) The Norwegian Institute of Public Health responsible for data management (2002)
Core data collected at birth from maternity units via MBRN system (1967)QR data collected after birth from hospitals via QR system (2006)
2014-12-09

Ebbing, NIPH 25
CPR Core
Reg
istry
MBRN
Hosp
2014-12-09

Ebbing, NIPH 26
Hosp
CPR
Norwegian Newborn Medical QR
Core
Reg
istry
MBRN
2014-12-09

Ebbing, NIPH 27
MBRN Council (2009 )
Obstetricians, midwifes, NIPH
2014-12-09

Ebbing, NIPH 28
«QR Data» in MBRN Core Registry
Details on risk factorsSmoking habits (1999)Body mass index (2005)
Details on deliveriesRobson classification, gestational age ++Progress and procedures during delivery
Details on the newbornCongenital malformationsOther conditions at birth
2014-12-09

Ebbing, NIPH 29
Statistics by Maternity Units
Since 2008, in cooperation with maternity unitsTo provide numbers for the maternity units’ evaluation on clinical practice To provide data for quality indicators published at helsenorge.noFor the care providers, health administrators and the publicHandle with care!
2014-12-09

Ebbing, NIPH 302014-12-09

Ebbing, NIPH 31
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95
AlleOUS UllevålHaukelandStavangerAhusSt. OlavØstfoldOUS Rikshosp.KristiansandVestfoldDrammenTelemarkBærumHaugesund
ÅlesundTromsøLillehammerBodøArendalLevangerElverumFørdeGjøvikRingerikeMoldeVoldaHammerfestStordHarstadVossKongsvingerKristiansundNamsosFlekkefjordRanaVesterålenKongsbergSandnessjøenNarvikKirkenes
Mor røyker ved svangerskapets begynnelse, 2013 (99 % konfidensint.)
Smok
ing
2014-12-09

Ebbing, NIPH 32
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95
AlleOUS UllevålHaukelandStavangerAhusSt. OlavØstfoldOUS Rikshosp.KristiansandVestfoldDrammenTelemarkBærumHaugesund
ÅlesundTromsøLillehammerBodøArendalLevangerElverumFørdeGjøvikRingerikeMoldeVoldaHammerfestStordHarstadVossKongsvingerKristiansundNamsosFlekkefjordRanaVesterålenKongsbergSandnessjøenNarvikKirkenes
Mor har overvekt eller fedme før svangerskapet, 2013 (99 % konfidensint.)
Ove
rwei
ght &
Obe
sity
2014-12-09

Ebbing, NIPH 332014-12-09

Ebbing, NIPH 342014-12-09

0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95
AlleOUS UllevålHaukelandStavangerAhusSt. OlavØstfoldOUS Rikshosp.KristiansandVestfoldDrammenTelemarkBærumHaugesund
ÅlesundTromsøLillehammerBodøArendalLevangerElverumFørdeGjøvikRingerikeMoldeVoldaHammerfestStordHarstadVossKongsvingerKristiansundNamsosFlekkefjordRanaVesterålenKongsbergSandnessjøenNarvikKirkenes
Keisersnitt blant alle fødsler, 2013 (99 % konfidensint.)
Caes
area
n, A
ll D
eliv
erie
s
2014-12-09 35Ebbing, NIPH
Ebbing, NIPH 36
helsenorge●no
“Several studies have shown variations in the incidence of caesarean sections at otherwise comparable maternity wards in Norway. The variations can not be explained only from patient composition of mothers and percentage of women wanting a caesarean section. The optimal level of deliveries by caesarean is not known.”
https://helsenorge.no/Kvalitetsindikatorer/graviditet-og-fodsel/kvalitetsindikator-keisersnitt
2014-12-09

0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95
AlleOUS UllevålHaukelandStavangerAhusSt. OlavØstfoldOUS Rikshosp.KristiansandVestfoldDrammenTelemarkBærumHaugesund
ÅlesundTromsøLillehammerBodøArendalLevangerElverumFørdeGjøvikRingerikeMoldeVoldaHammerfestStordHarstadVossKongsvingerKristiansundNamsosFlekkefjordRanaVesterålenKongsbergSandnessjøenNarvikKirkenes
Keisersnitt innen Robson-gruppe 1, 2013 (99 % konfidensint.)
Cae
saer
ean
in R
obso
n 1
2014-12-09 37Ebbing, NIPH

0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95
AlleOUS UllevålHaukelandStavangerAhusSt. OlavØstfoldOUS Rikshosp.KristiansandVestfoldDrammenTelemarkBærumHaugesund
ÅlesundTromsøLillehammerBodøArendalLevangerElverumFørdeGjøvikRingerikeMoldeVoldaHammerfestStordHarstadVossKongsvingerKristiansundNamsosFlekkefjordRanaVesterålenKongsbergSandnessjøenNarvikKirkenes
Keisersnitt innen Robson-gruppe 3, 2013 (99 % konfidensint.)
Cae
saer
ean
in R
obso
n 3
2014-12-09 38Ebbing, NIPH

Ebbing, NIPH 39
Summary & Conclusion
GARs – some of them with QR qualities
We must reduce the burden of reporting!
Cooperation and concensus – and linking!
Combined registries – the way to proceed?
2014-12-09

Ebbing, NIPH 402014-12-09